#people are people at the end of the day not diagnostic criteria
Text
‘they didn’t have the concept of mental illness back in the day so that’s why so many people claimed they could talk to god/had life altering visions/believed in witchcraft’ have you considered that maybe the lack of current magic in our world is due to the psychiatric system’s well-meaning inability to differentiate between life-threatening delusions & whimsy/possible spiritual insight
#idk abt this one. i never know if i’m religious or have mild psychosis. i think it’s pretty easy to tell the difference generally cause one#time i thought i was god & had total control over our world and that was a hashtag crazy mental illness moment & i’ve always had vague#feelings that i can control the world via cheat codes like closing doors in certain ways or punching walls but these days i mostly#understand that that is. ocd.#ocd tendencies we shall say actually since i lack a diagnosis or certainty of any kind of except for the knowledge that my brains#silly sometimes.#but also i do like have a genuine spirituality to me sorry that that makes me crazy or whatever & i believe in some god adjacent thing & for#want of a better word sort of in ‘magic’. by a modern sensibility this makes me crazy#but. Like.#anti psychiatry#<- to an extent. i have no proper full formed opinions on the matter & am sure it is very helpful sometimes But.#people are people at the end of the day not diagnostic criteria#and i find it silly when anything predisposes that there is no magic or religion in our world#oliver talks
9 notes
·
View notes
Text
Does anyone realize that the "everyone is valid" thing has actual diagnostic implications?
Yes, every case of DID will have differences from another. But all DID cases must meet diagnostic criteria in order to actually be DID. You can't say "everyone is valid" and "DID can look like anything" because really, it can't. At the end of the day, there are still diagnostic criteria that must be met. If anything goes and anything is valid and anything can be DID, then DID is nothing and we might as well not even classify it as a disorder at all.
Same thing as people who say that "everyone has a little bit of DID" or "everyone has parts". Yes, you act differently at work than you do at home. This does not mean that you have dissociated parts of a fragmented self, and if it did, then DID would be a redundant diagnosis and there would be no need to have it in the ICD or DSM if "everyone" had it.
#actually did#actually dissociative#ramcoa#ramcoa survivor#did osdd#did system#dissociation#dissociative identity disorder#dissociative system#osddid
506 notes
·
View notes
Text
we are about an hour into rare disease day in my timezone! (it's always the last day of february, whether that's the 28th or the 29th.) the true prevalence of mast cell disorders is unknown, as they are often misdiagnosed or ignored. and mast cell activation syndrome, the most prevalent kind of mast cell disorder, only had diagnostic criteria laid out for the first time in 2010. so whether or not it's truly rare is really up in the air!
(personally I suspect it is just aggressively underdiagnosed but I'm not a research scientist or diagnostician right now. and even if it is rare, it's gonna be a lot less so than it was 5 years ago as certain respiratory infections are known to trigger it into visibility. that's what happened to me when I got mono at the end of 2015, further compounded when I got covid in 2022.)
all chronically ill people face a lot of hurdles when it comes to seeking diagnosis, accommodation, and treatment (all of which can be severely complicated by any intersecting marginalities), but rare diseases present a special challenge.
for example, I have an immune disorder. my immune system does not like being alive, my mast cells are way too jumpy and throw a tantrum over every little thing. you'd think an immunologist would be the one to treat me, right?
I've had 6 immunology referrals rejected in the past 9 months alone. multiple major immunology clinics in my major city tied to a major research university outright refuse to see patients with "mcas" written anywhere in their chart.
after 8 years of being debilitatingly ill, and suspecting it was immune mediated for 6, and getting it confirmed beyond a shadow of a doubt by the bone marrow biopsy last month, I will have my second ever appointment with an immunologist. another 2 1/2 months from now. the first immunologist lied to me about the reliability of the one available blood test, when I first came up with the hypothesis by myself 6 years ago, and forced me to abandon my (correct!!! now proven!!!) hypothesis for 3 entire years while we wandered around lost and got nowhere other than even more thorough process of elimination.
okay, well if my immune system is attacking me, maybe it's technically autoimmune? that's the rheumatologists instead of the immunologists, what do they have to say? dick all my dude, I don't have rheumatoid arthritis so they just shrug at me and go "idk, fibro? I don't know why you're here" and send me home with nothing. (I literally had a rheumatologist say to me, verbatim, "I don't know why you're here." buddy it's your job to read the chart and decide if I get seen or not, you tell me. at least he had a snazzy outfit.)
being chronically ill can be a terrible struggle no matter what, but a disease that is perceived as rare, accurate or not, adds a whole new layer of bullshit. (and of course there are much much rarer diseases out there, with even more hoops and dead ends and struggles and all-new layers of bullshit that even I don't have to deal with!)
anyway I'm having a shit time and using this awareness day as an excuse to productively bitch about it 👍
#it is okay to reblog this btw!#I know sometimes ppl get skittish when posts seem personal#(but I also know a wall of text is not Aesthetique™️ which like fair it's your blog yknow?)#kirby#swearing#long post#daily kirby#my art#digital#hal laboratory#nintendo#rare disease day#mcas#mast cell activation disorder#one time my wife took me to a gathering with her (at the time future-)doctor friends#and they were asking me about what I do and stuff and I was like 'oh I'm disabled'#so of course they're like 'oh with what?' basically#so I had to explain that we didn't know#and *why* we didn't know#and they seemed deeply disquieted that it could take even that long to find answers.#(this was coincidentally 6 years ago.)#it's a good lesson for them to learn early.
125 notes
·
View notes
Text
NagiReo in Blue Lock and Episode Nagi through a BPD4BPD Lens
For this analysis we will be using the diagnostic criteria for Borderline Personality Disorder from the DSM-5, below, which was last updated in 2013.
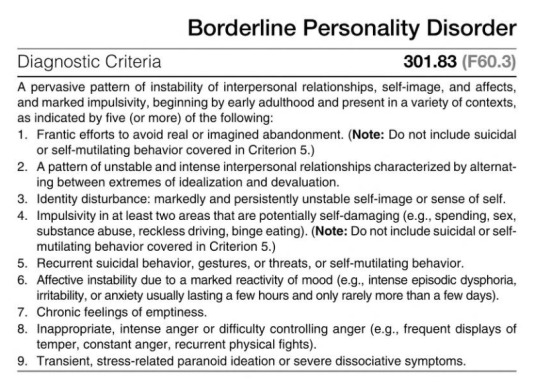
We'll be taking a look at Nagi and Reo's behavior in both Blue Lock and Episode Nagi, as well as the trivia included in the Egoist Bible. We will be going through at least five different diagnostic criteria for each of them, before talking about BPD4BPD relationships and the way Nagi and Reo interact as each other's FP's.
Chronic Feelings of Emptiness
First, lets's take a look at Blue Lock.
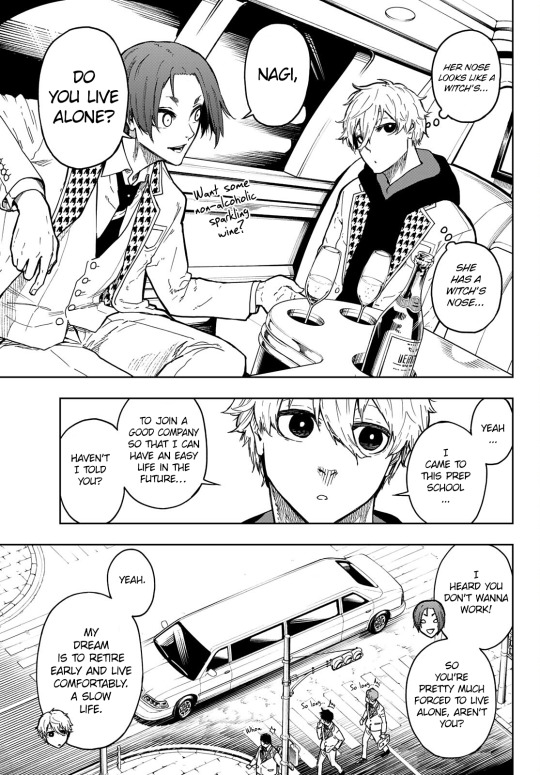
From his very first appearance, Nagi displays a boredom with day to day tasks and relies on Reo heavily.

Here's a little collage of Nagi's apathy in early Blue Lock.

Meanwhile, Reo is shown to have been chronically bored with life since childhood. He is "easily bored, [] seek[ing] something to do," which he finds in his goal to win the world cup.

Now let's look into Episode Nagi.
Nagi demonstrates a persistent low energy/fatigue. He's bored by self-care activities and taking care of basic needs.
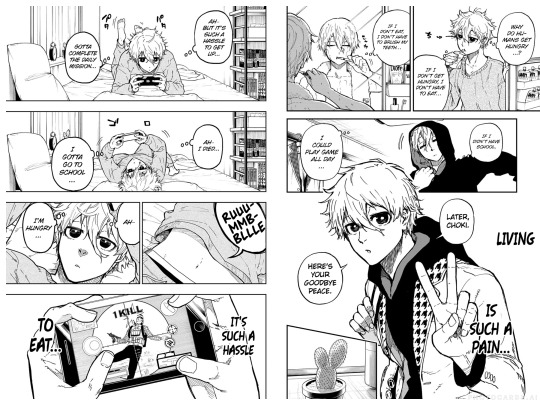
He originally doesn't want to join Blue Lock because of this chronic emptiness/boredom.

Now we move onto the Egoist Bible.
Nagi describes his weakness as "Tend[ing] to find many things bothersome," which is backed up by the panels we looked at earlier.
Reo considers his his weakness to be, "I can do anything and get bored easily." When he describes a day in his life at Blue Lock he says, "When I asked Nagi, "Let's play games," he refused. "Because if you improve quickly, you'll get bored easily," he said. You really know me, I thought, but that made me a bit sad." His boredom is a weakness for him, that both he and others, like Nagi, pick up on.
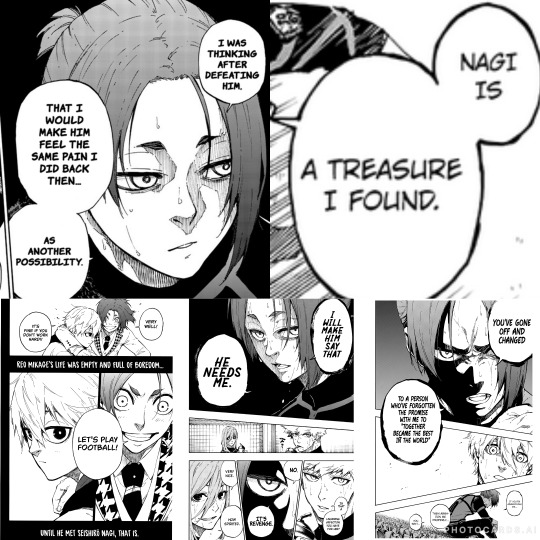
A Pattern of Unstable and Intense Interpersonal Relationships Characterized by Alternating Between Extremes of Idealization and Devaluation
Here, I'll note the DSM-5's notes from the Diagnostic Features section: "They may idealize potential caregivers or lovers at the first or second meeting, demand to spend a lot of time together, and share the most intimate details early in a relationship. However, they may switch quickly from idealizing other people to devaluing them, feeling that the other person does not care enough, does not give enough, or is not “there” enough. These individuals can empathize with and nurture other people, but only with the expectation that the other person will “be there” in return to meet their own needs on demand. These individuals are prone to sudden and dramatic shifts in their view of others, who may alternatively be seen as beneficent supports or as cruelly punitive. Such shifts often reflect disillusionment with a caregiver whose nurturing qualities had been idealized or whose rejection or abandonment is expected."
Again, we first look at Blue Lock.
Nagi demonstrates a positive attitude towards Reo. He looks up to him and is often praising him and mentioning him even when Reo isn't around. However he ends up harshly speaking to Reo after their argument directly after their 3v3 match, showing a rapid switch in emotions triggered by feelings of Reo not caring about their promise.

Reo shows a lot of negative emotions easily. He feels rejected and spiteful because of Nagi leaving him during the second selection. This makes him think of plans to make Nagi take him back, experience the same pain, etc. He continues to describe Nagi as a treasure he found, however, as a person who made his life stop being boring.
Now let's move onto Episode Nagi.
Nagi and Reo share with each other the details of their personal lives very quickly after meeting each other, something mentioned in the DSM-5 as: "shar[ing] the most intimate details early in a relationship." Reo especially does this, but both do.
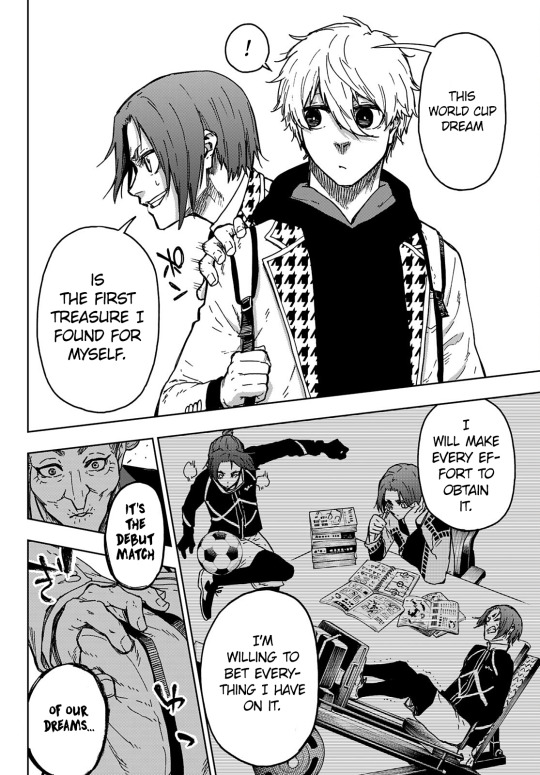
Reo is also stuck on the idealized idea of playing soccer with Nagi. He makes every effort to make this into a reality, even with the later devaluation he experiences during Blue Lock.

Identity Disturbance: Markedly and Persistently Unstable Self-Image or Sense of Self
The Diagnostic Criteria of the DSM-5 says this: "There are sudden and dramatic shifts in self-image, characterized by shifting goals, values, and vocational aspirations. There may be sudden changes in opinions and plans about career, sexual identity, values, and types of friends. These individuals may suddenly change from the role of a needy supplicant for help to that of a righteous avenger of past mistreatment. Although they usually have a selfimage that is based on being bad or evil, individuals with this disorder may at times have feelings that they do not exist at all. Such experiences usually occur in situations in which the individual feels a lack of a meaningful relationship, nurturing, and support. These individuals may show worse performance in unstructured work or school situations," in regards to this criteria.
First, we will take a look at Blue Lock, once again.
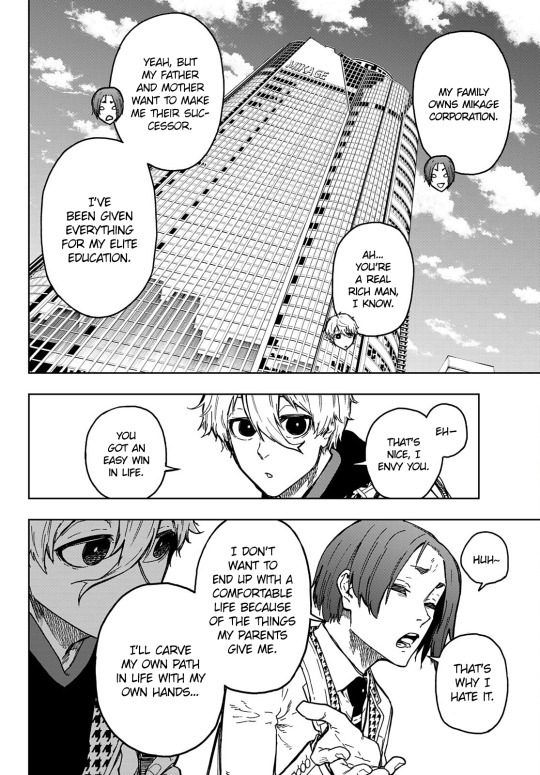
Nagi doesn't have a solid identity in football or a goal. He plays depending on Reo. His ego revolves around Reo's and he doesn't have a sense of his own. Nagi cares about Reo deeply and because he started playing football for Reo, he has a hard time developing an identity within football outside of Reo.

Reo has a conflicting set of ideals. He flickers between wanting to be independent and rely on no one and wanting to play with Nagi. This is partially because Nagi is the object of his affection and therefore the center of both his black and white thinking and fear of rejection.

Reo also experiences a disjointed sense of identity within his personal opinion of himself. When faced with Nagi's rejection, Reo's opinion of himself drops exponentially.

Moving on to Episode Nagi.
Nagi is unsure of his identity and stands on shaky ground regarding his worth.
Meanwhile Reo, in contrast to Blue Lock, is confident and happy because of his idealization of Nagi and his dream, showing the instability and fluctuation of his identity.
Finally, let's take a look at the Egoist Bible.
Reo answers that what makes him happy is "Due recognition" and what makes him sad is "preconceived views" showing the way he is influenced by others in his view of himself and his identity.
Frantic Efforts to Avoid Real or Imagined Abandonment
"The perception of impending separation or rejection, or the loss of external structure, can lead to profound changes in self-image, affect, cognition, and behavior. These individuals are very sensitive to environmental circumstances. They experience intense abandonment fears and inappropriate anger even when faced with a realistic time-limited separation or when there are unavoidable changes in plans (e.g., sudden despair in reaction to a clinician’s announcing the end of the hour; panic or fury when someone important to them is just a few minutes late or must cancel an appointment). They may believe that this “abandonment” implies they are “bad.” These abandonment fears are related to an intolerance of being alone and a need to have other people with them."
Let's look at Blue Lock.
Nagi does everything throughout Blue Lock to keep his promise to Reo. This promise is important because it represents their partnership and implies that Reo will stay with him. During the Neo Egoist League, Nagi struggles to convince Reo to play with him again, trying to avoid the rejection of losing Reo as a partner, which would make him feel purposeless.

Meanwhile, Reo often tries to avoid rejection. To him rejection is one of the worst things that could happen. He's always thinking about rejection, about being chosen, about what happens if he isn't chosen.

Now let's look at Episode Nagi.
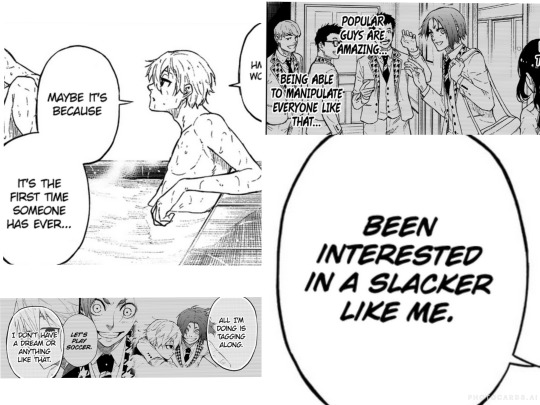
In Episode Nagi, Nagi's fear of rejection is a little bit clearer. We can go back to the panels showing his sense of self to take a look at his thoughts of just being the tag along or a slacker to see this. He also is determined to stay with Reo in Blue Lock, despite his laziness and lack of motivation because of their promise. When he's insulted he instates himself as Reo's partner and part of a set.

Meanwhile, Reo notices rejection in small things like offhand comments. For example when Nagi passes to Zantetsu and comments on his dream being the same.

Inappropriate, Intense Anger or Difficulty Controlling Anger
The DSM-5 says: "They may display extreme sarcasm, enduring bitterness, or verbal outbursts. The anger is often elicited when a caregiver or lover is seen as neglectful, withholding, uncaring, or abandoning. Such expressions of anger are often followed by shame and guilt and contribute to the feeling they have of being evil."
Let's look at Blue Lock for a final time.
Nagi expresses anger towards Isagi when he brings up Reo, because he recently experienced separation from him.
Reo resorts to physical violence on the field when Nagi is brought up in insults.


Now, for Episode Nagi.
Reo has to stop Nagi from getting into a verbal altercation with Barou that would most likely devolve into a physical fight. This started because of Reo being brought up in an insult.

BPD4BPD

This BPD4BPD flag was made by @gender-mailman
BPD4BPD is a label for pwBPD who want to date pwBPD. To me this is an incredibly interesting lens to view NagiReo through because I find that it makes them click as people who understand each other in this specific way of their BPD and yet, because of their clumsy teenage inexperience and because of their independent struggles with it, keep on hurting each other.
I feel like with NagiReo, the way their relationship has developed throughout Blue Lock up until the Neo Egoist League, it's lacking communication. They're both hurting each other in ways that are typical for how they react to rejection and they get stuck in cycles of miscommunication because of it. They both deeply care about each other and I think because they're teenagers who don't really know what they're doing with their friendship or tentative romance or whatever you choose to interpret their relationship as it is turning out exactly as one would expect. I think there's a positive outlook for them which is very exciting to see for two characters who fall so closely within the lines of BPD coding and have such a close and interesting relationship, a BPD4BPD relationship that's really rare to see in media.
In fandom, I see a lot of casual ableism towards Reo especially, perhaps because his coding is more overt, especially in the department of expressing feelings of rejection, which is bleak, but honestly that is something we can work on as a fandom.
Also, please feel free to add to this post if there's anything I missed, especially since my manga reading website is a little bit behind both on Episode Nagi and on Blue Lock, or if there's anything interesting you have to add!
Remember to be kind to your local pwBPD and just all pwPDs and I hope you enjoyed this little dive into NagiReo's theoretical psychology!
#seabirds.txt#blue lock#bllk#nagireo#nagi seishiro#mikage reo#blue lock analysis#blue lock theory#i dont really know if this is anything. i havent made a post with analysis like this before and i feel like its kind of. Bad. but we'll see#wild geese series.
49 notes
·
View notes
Text
Trans Floridians: "Informed Consent" guidelines are shaping up to be worse than the Harry Benjamin days
The Florida Board of Medicine is discussing the "informed consent" standards today. These will affect trans people, including adults, who are both starting and continuing care.
In short, the guidelines require a prohibitively expensive and difficult to access number of regular assessments for the life of "treatment". (Which, for most of us on HRT is the rest of our lives.) The guidelines look for any opportunity to deny care, from lack of social support to "co-morbidities" that are likely targeting autism, depression, etc.
The specific requirements for you to receive and continue HRT treatment include the following:
1. Meets the current DSM or ICD criteria for gender dysphoria;
2. Mental health and physical conditions that could negatively impact the outcome of treatment have been assessed, with risks and benefits discussed
3. Gender dysphoria is marked and sustained;
4. Demonstrates capacity to consent for the specific gender dysphoria hormone treatment;
5. Does not suffer from psychiatric comorbidity that interferes with the diagnostic work- up or treatment;
6. Has adequate psychological and social support during treatment;
7. Demonstrates knowledge and understanding of the risks, benefits, and expected outcomes of HRT as well as the medical and social risks and benefits of sex reassignment surgery;
8. Understands the effect of gender-affirming hormone treatment on reproduction and they have explored reproductive options;
9. Undergoes an evaluation by the prescribing physician at least every 3 months
10. Undergoes a suicide risk assessment by a licensed mental health care professional at least every 3 months;
11. Undergoes laboratory testing, including blood tests, at least every 6 months;
12. Bone (DEXA) scan once a year to allow monitoring of your bone density (bone strength) during treatment, which can be altered by HRT;
13. Annual mental health assessments by a board-certified Florida licensed psychiatrist or psychologist; and
14. Continued counseling with a licensed mental health care professional during the treatment period, with the frequency recommended by the licensed mental health care professional.
Erin covers here:
From Representative Anna V. Eskamani:
Beginning on page 264 of the meeting packet is the draft informed consent forms for tomorrow's meeting. In part it reads -- "Before beginning or continuing HRT, the individual needs to undergo a thorough psychological and social evaluation performed by a Florida licensed board-certified psychiatrist or a Florida licensed psychologist. The psychiatrist or psychologist must submit a letter to the prescribing physician confirming this."
https://ww10.doh.state.fl.us/.../06232023_JRL_Publicbook.pdf
Licensed mental health counselors and licensed social workers are trained to write evaluation letters. They know most providers have an LCSW or mental health on staff. This is cruel for the sake of bring cruel and designed to make access more difficult.
I experienced the gatekeeping during the Harry Benjamin days, including the mandatory one year "real life test" where you have to live as your gender in all aspects of your life without the benefits of HRT. It was a very stressful and dangerous practice that was designed to crush us.
This is so much worse. Even with my current salary, health benefits, and work from home schedule, I don't see how I could afford the time and money for all the assessments, nevermind how insulting and discriminatory they are.
Trans Floridians should watch this story closely as the Board of Medicine discusses and finalizes these requirements. As of today, these are not final, but in the current state, would mean the end of informed consent in Florida, and all but bans care entirely.
106 notes
·
View notes
Text
Just saw someone say radfems advocate for the genocide of disabled people… exuse me? I’ve seen so many disabled radfems who were radicalised because of how they’re treated as disabled women.
So many health conditions that only effect FEMALES aren’t recognised as disabilities because of medical misogyny. Endometriosis can cause women to be bedridden. Some women go through their lives in constant agony with doctors simply just prescribing birth control or weight loss, only for pathologists to find endometriosis tissue on spines, in lungs, even on brains. Symptoms for many disabilities differ between men and women, and guess who’s symptoms they value more? Most diagnostic criteria for disabilities are based off mostly male experiences. Conditions that effect women only are extremely under researched, under diagnosed, and mistreated.
Disabilities can also be caused by other feminist issues like sex work and kink culture. Women often go into sex work because of their disabilities and chronic illness. They aren’t able to stand for too long, they can’t work 5+ days a week, they can’t work long hours. This isn’t to say that sex work is easy - it’s just very flexible and often the only option when no other job can be bothered to accommodate you. Women have ended up with colonoscopy bags after being pressured into rough anal sex. Women have had permanent vaginal tearing and scarring after rough sex where male partners didn’t care for foreplay. Women have died, suffered brain damage, had strokes because of male partners choking them.
Homeless and disabled women are among the most vulnerable of us. No actual radical feminist could exclude or be aggressive towards them without going against her own beliefs. It makes no sense. People will just say anything to demonise radical feminism and scare women away because radicalised women are a threat to the patriarchy.
#radical feminists do touch#anti sex industry#anti sex trafficking#radblr#radical feminist safe#radical feminists do interact#terfblr#terfism#terfsafe#lgb drop the t#medical misogyny#radical feminism#radical feminst#misandry
16 notes
·
View notes
Text
Ways LTC is super ASPD/sociopath coded as heck!
has a strong background in mental issues a la a very abusive homelife
has one particular traumatic incident that starts as the turning point for his personality (hammer + murder-homocide by proxy), this incident also involves a severe loss of stability via a parental figure/adult which is very common in the early trauma of people with ASPD
normally it's torturing or murdering small animals in childhood as the diagnostic criteria but it was probably people for LTC (though we don't know about any earlier instances of torturing specifically besides LG)
LTC mentions not caring about the murders he's commited as long as he has fun, which scans because people with ASPD often struggle feeling anything at all and end up chasing intense highs just to meet that need (hence why they often have high risk-taking behaviour and serious addiciton issues)
speaking of risk taking behaviour, LTC had no problem going into the police station in his real body just to perform a subsequent kidnapping in said police station all while very calm and collected, like it was a literal walk in the park
LTC seems to have a value system about right and wrong that's very different from social norms e.g. gossiping is just as bad as beating your wife. I'm sure this child-trauma-jibberish logic really helps with that lack of empathy.
I was gonna have a whole bulletpoint about Clash's lyrics, but turns out I MISHEARD A BUNCH OF THEM, but I do think the line "Become the person that I wished for that day" line feels very LTC.
He got talked into doing some extreme shit as a kid that fucked him up. And now he keeps repeating and refining his aggressive and destructive behaviour, because in the end it WAS so important for him and LTX getting a better life. Though that's more LTC character analysis than anything ASPD.
#link click#link click season 2#link click spoilers#li tianchen#shiguang daili ren#link click analysis#i love this mentally ill little skrunkle#HE DESERVED BETTER#THEY BOTH DESEREVED SO MUCH BETTER
28 notes
·
View notes
Text
Fought with my partner today about holiday plans, honestly caused by communication deficiency + bpd abandonment avoidance bullshit + meltdown.
I kept saying I don’t want to go with him to his family’s holiday meal unless he actively wants me to go (turns out just desperately tying to feel wanted, just bpd diagnostic criteria #1, something neither of us realized at the time) so he kept insisting he didn’t care one way or the other (with good intention, so that I wouldn’t feel obligated to do something overwhelming)
Anyway this man is so good to me, we were angry and yelling at each other but he didn’t wanna leave me home alone while I was that upset so he called and told his mom he wasn’t coming. And I know he wasn’t really dying to do the whole holiday family ordeal, but I still feel so awful.
He is so understanding and puts up with my horrific behavior and chronic/mental illness nonsense and as a thanks I ruin his day. His day off. We worked it out, things ended up good, but now he has to end his day early, mentally and emotionally exhausted, and then get up to work all day tomorrow so he can support both of us because my psychotic ass is too disabled to hold a job or any worthwhile income. And then he gets to come home to a messy house because I’m too dysfunctional to maintain our home properly. And I can’t believe he puts up with this and has for years and years. I’ve never felt so unconditionally loved.
I feel guilty for the obvious but then exponentially guilty that I don’t consistently act more grateful or even just affectionate. But whenever I try to express affection or gratitude or remorse, this panic alarm goes off in my brain that I’m about to give up allll my power and therefore ensure eternal suffering and oppression for myself. Which is just cptsd-brain lying to me, I know. But even knowing that logically, affection and gratitude still feel near impossible to express. I feel them sooooososooosos deeply……. I just wish I could let people know without vibrating violently and tensing up all my muscles involuntarily to the point of catatonia. Getting pretty close just writing this post tbh
Anyway I’ve been doing a lot of self-worth exercises and DBT work on my own and I know things will get better. I just want to be able to give the people I love all the thanks they deserve for all of the endless things they’ve done for me. I just want people to know how grateful I am and how sometimes it feels like my heart is overflowing so much I’m drowning in it. I just want to be able to express that to anyone that deserves to hear it.
#rants & reflections#cptsd healing#cptsd recovery#abandoment issues#bpd meltdown#audhd#bpd relationships#bpd love#trauma recovery#trauma brain#borderline vent#borderline personality disorder#late diagnosed autistic#neurodiversity
16 notes
·
View notes
Text
Truama is subjective.
What was intensely traumatic for me might not be traumatic to you, and it might not have even been traumatic in the moment.
We have did comorbid with autism adhd and anxiety, things that may not have been upsetting in the moment can become upsetting later. Our mother thinks our childhood was good and cool, we remember very little of it and in the past the only bits we remembered with any clarity were traumatic things.
This is why I personally don’t think endos exist, and that’s not me siding with anti endos either. I think that trauma is subjective, covert, and easy to miss, and that everyone has it. Some people are more susceptible to letting it cause problems.
Trauma is not a requirement for did. ptsd and cptsd are not requirements for did. They are commonly found with did, but they are not diagnostic criteria.
I do not have ptsd symptoms (as far as I’m aware)
I have had experiences with alters since i was 13 or 14, I have had a therapist clock it without me asking about it, and I’ve talked to my current therapist about it.
My trauma is not terribly bad, I was bullied as a kid, I had undiagnosed autism and anxiety, emotional neglect (minor), health trauma related to both of my parents having chronic illnesses, and some general being raised in the 2010s trauma shit like having too much access to the internet.
I still have alters, I still lose time, I still have a seemingly ever changing internal image.
I also just don’t think it matters that much. If your playing trauma Olympics what are you doing with your life. Be happy that someone didn’t have as shitty of a life.
ALSO, as an end note to anyone that picked up on the fact that I am young, I only found out I have did because of a coincidence. If I had not met the people I did that day I likely would have gone many many years without figuring it out. DID in the past was assisted in its obfuscation by the lack of easy education, there is a wealth of info now and it is very easy to find stuff out.
-Tara
#endo safe#endo friendly#did system#disociative identity disorder#traumagenic system#syscourse#autism#adhd#disociation#trauma#did community#do not attack#I am open to discussion but I am not willing to have a fight over this.#my therapist agrees with me on this shit#my therapist is so cool#love her#very helpful#also if your sitting there asking about amnesia#I experience amnesia#I have bilipped a whole week before and regularly have bits of time disappear
7 notes
·
View notes
Note
Thoughts on the, Phil is autistic discourse?
Simple answer: yes, yes he is, and I've been collecting stuff in my 'tism' tag for the same
To get more serious tho: neurodivergence is a massive spectrum of symptoms, and a lot of diagnostic criteria we uphold as watertight categories are actually quite arbitrary very often. Now I'm someone who, like much of the autistic community, do not see it as a 'disorder'(ie, I do not see it as needing a cure/something being wrong, I do understand that it is a disability and I find it to be so myself for many of the symptoms) but a neurodivergence. And a key part of the neurodivergence movement is to reject psychiatric categories and accept "symptoms" as just traits, ways in which different people's minds work and different ways in which people process trauma and different sensory experiences since all sensory experience is neurological and therefore inherently subjective etc etc. It's an alternative to the pathologising medical model of psychiatry. That being said, autistic people have particular kinds of shared experiences, not everyone will have them the same way it's a broad range of traits, but we are able to recognise, let's say, "one of our kind" very often. That's how I found out I'm autistic too, by talking to other autistic people who helped me figure out this part of my neurodivergence amongst other stuff. I think people who don't go for diagnosing - whether "professionally" or through self-identification - are completely valid for doing so, it's really just a matter of whether or not you're trying to put a word to your experiences, and if you aren't then you aren't. I will say that so many autistic people here talking about how they have shared experiences as autistic people with Phil probably indicates that he is one of us, but whether he chooses to use that as a label or no is up to him of course, and at the end of the day "is xyz autistic" will come down to "does xyz wish to use the label of being autistic to put a name to their neurodivergent experiences". Can a lot of what is considered strange and random behaviour on Phil's part be explained when you look at it from the lens of autism though? Yes definitely. It's all about people finding people they relate to and going [leonardo di caprio pointing meme]
12 notes
·
View notes
Text
I got really sick for about ten days and have been otherwise out of it somewhat. I had a few asks from people checking in so I wanted to just address things in a post.
Under a read more to not clog anyone's dashboard.
Thank you to everyone who checked in and left kind messages. I have good news in that I don't have to find a new place to live and things haven't ended in my relationship. Things have been sorted out but it was definitely rocky for a bit.
As folks know, I have a history of mental illness issues to the point of benefitting from a service dog to assist with panic attacks, sensory overload, and grounding me during dissociation. It was becoming apparent that my mental health was getting worse and that there was likely something beyond my current diagnoses. My last therapist wasn't helping and was ignoring some of my most troubling symptoms. So I changed therapists and they have come to agree after only a few sessions that I meet a diagnosis for one of the "scary" mental health disorders. It's not officially diagnosed but the therapist has basically said "you have this I just haven't done all the diagnostic work yet".
Unfortunately, my partner had a lot of trouble with this and had a big panic over this. She was absolutely not able to handle the idea of this and it caused a lot of issues. After speaking with my therapist and learning a bit more about the diagnosis, she still has feelings about this but has worked through the worst of it and has apologized for her reaction. She still has some feelings about this but we are doing much much better. She is still working to understand what this diagnosis means but shes managing. The bright side is the diagnosis explains a lot of behaviors that have utterly confused her. So that is helping her understand me better and how I react to things. It still feels a bit fake that I meet the criteria for this diagnosis hence why I'm being vague. It feels like I'm probably just making shit up. So it's been a lot for me as well.
So thank you for everyone being kind and supportive. This is a lot to manage but slowly getting there. Here is a cute photo of Tzapo being so very eepy as thanks for reading through this.

19 notes
·
View notes
Text
TWs: Talk of pedophillia, child abuse, and my frustration with the internet, purity culture, and stigma.
Please do me a favour also, and read the post to the end before saying anything to me about it. For our mutual sanity.
I am going to combust if I see another kill all pedophiles post.
Pedophile is a diagnosis that requires you to experience significant distress about your attraction. Or to have actively found a child desirable and acted on that desire. (The latter is extremely likely to be a minority but due to the stigma few are willing to voluntarily come forward to be studied)
If you think it is okay to find fictional minors attractive, but do not have interest in them irl, (ie people who consume loli/sho) you would not classify as a pedophile.
Assaulting a child you do not find attractive does not make someone a pedophile, it makes them an abuser.
Alas, purity culture has once again moved the focus away from the actual abusers and onto predominantly innocent people who genuinely do not want to harm anyone.
If you’re queer or poc or mentally ill or marginalized in any way that should sound horribly familiar.
Please for the love of god, if you’re someone who says all pedophiles deserve to die. Read the diagnostic criteria and if you still think that after you have, block me, please. Because at that point you are knowingly saying a lot of innocent people should die, as the actual abusers rarely turn out to be pedophiles.
Here, I’ll even save you the effort of finding it. This article cites the DSM directly and saves skimming the incredibly dense book that is the DSM
I can’t link it directly because that’s illegal but there’s a full copy of the DSM-5 if you search “DSM-5 Reddit” and use the top link. As of posting this the link works, if that changes let me know and I’ll update this accordingly.
Pages 697-700 for those interested in reading the full piece.
I’m not typically one to talk about my opinion of this in public because I know for a fact there’s going to be a mass of people who will do exactly what they’ve been trained by purity culture to do. React with outright disgust and horror without being willing to consider that they’ve been manipulated so that child abusers can continue to abuse children while their victims burn anyone who dares question them.
But I’m tired.
I have a lot of experience with heavily stigmatized disorders. I’m schizophrenic, autistic, and have SCPD. I’m also visibly queer + trans in a heavily conservative area. So the the idea that person with X disorder is a threat to children is very, very familiar.
I’m also a CSA victim, and it’s… Sad, watching other victims allow abusers to continue existing in the shadows while perpetuating the stigma that keeps said abusers hidden. I’m aware of my privilege as someone who is educated on the manner and as someone with the resources at my disposal along with the knowledge of how to take advantage of said resources.
I suppose that’s why I decided to actually write this out publicly. That way people who may not have otherwise known can educate themselves and form a stronger community that evicts actual abusers and not predominantly innocent people trying to recover from one of the most stigmatized disorders someone can have, or people with questionable taste in porn when more often than not said porn is harmless.
Here’s another article, this one talks in depth about whether or not fictional loli/sho nsfw actually encourages pedophillic behaviour and urges from a sociology perspective. With papers and stats to back up it’s points.
It also talks about whether or not loli/sho can even be considered pedophillic at all, along with the general impact of porn on sexual violence. It’s a very good and informative read if you have the time.
It ALSO acknowledges bias in the studies it cites, and how that makes the opinion drawn from the study less valuable.
Gods this is long, take a snack, and have the day you deserve /neutral
🍮🍪🍩🍎🍟
16 notes
·
View notes
Text
Random psychology disorder (somewhat) explained #2 (Borderline personality disorder)
Diagnostic Criteria
A pervasive pattern of instability of interpersonal relationships, self-image, and affects, and marked impulsivity, beginning by early adulthood and present in a variety of contexts, as indicated by five (or more) of the following:
1. Frantic efforts to avoid real or imagined abandonment. (Note: Do not include suicidal or self-mutilating behavior covered in Criterion 5.)
2. A pattern of unstable and intense interpersonal relationships characterized by alternating between extremes of idealization and devastation.
3. Identity disturbance: markedly and persistently unstable self-image or sense of self.
4. Impulsivity in at least two areas that are potentially self-damaging (e.g., spending, sex, substance abuse, reckless driving, binge eating). (Note: Do not include suicidal or self-mutilating behavior covered in Criterion 5.)
5. Recurrent suicidal behavior, gestures, or threats, or self-mutilating behavior.
6. Affective instability due to a marked reactivity of mood (e.g., intense episodic dysphoria, irritability, or anxiety usually lasting a few hours and only rarely more than a few days).
7. Chronic feelings of emptiness.
8. Inappropriate, intense anger or difficulty controlling anger (e.g., frequent displays of temper, constant anger, recurrent physical fights).
9. Transient, stress-related paranoia ideation or severe dissociative symptoms.
Diagnostic Features
The essential feature of borderline personality disorder is a pervasive pattern of instability of interpersonal relationships, self-image, and affects, and marked impulsivity that begins by early adulthood and is present in a variety of contexts.
Individuals with borderline personality disorder make frantic efforts to avoid real or imagined abandonment (Criterion 1).
The perception of impending separation or rejection, or the loss of external structure, can lead to profound changes in self-image, affect, cognition, and behavior.
These individuals are very sensitive to environmental circumstances.
They experience intense abandonment fears and inappropriate anger even when faced with a realistic time-limited separation or when there are unavoidable changes in plans (e.g., sudden despair in reaction to a clinician's announcing the end of the hour; panic or fury when someone important to them is just a few minutes late or must cancel an appointment).
They may believe that this "abandonment" implies they are "bad."
These abandonment fears are related to an intolerance of being alone and a need to have other people with them.
Their frantic efforts to avoid abandonment may include impulsive actions such as self-mutilating or suicidal behaviors, which are described separately in Criterion 5 (see also "Association With Suicidal Thoughts or Behavior").
Individuals with borderline personality disorder have a pattern of unstable and intense relationships (Criterion 2).
They may idealize potential caregivers or lovers at the first or second meeting, demand to spend a lot of time together, and share the most intimate details early in a relationship.
However, they may switch quickly from idealizing other people to devaluing them, feeling that the other person does not care enough, does not give enough, or is not "there" enough.
These individuals can empathize with and nurture other people, but only with the expectation that the other person will "be there" in return to meet their own needs on demand.
These individuals are prone to sudden and dramatic shifts in their view of others, who may alternatively be seen as beneficent supports or as cruelly punitive.
Such shifts often reflect disillusionment with a caregiver whose nurturing qualities had been idealized or whose rejection or abandonment is expected.
There may be an identity disturbance characterized by markedly and persistently unstable self-image or sense of self (Criterion 3).
There are sudden and dramatic shifts in self-image (e.g., suddenly changing from the role of a needy supplicant for help to that of a righteous avenger of past mistreatment).
Although they usually have a self-image that is based on the feeling of being bad or evil, individuals with this disorder may at times have feelings that they do not exist at all.
This can be both painful and frightening to those with this disorder.
Such experiences usually occur in situations in which the individual feels a lack of a meaningful relationship, nurturing, and support.
These individuals may show worse performance in unstructured work or school situations.
This lack of a full and enduring identity makes it difficult for the individual with borderline personality disorder to identify maladaptive patterns of behavior and can lead to repetitive patterns of troubled relationships.
Individuals with borderline personality disorder display impulsivity in at least two areas are potentially self-damaging (Criterion 4).
They may gamble, spend money irresponsibly, binge eat, abuse substances, engage in unsafe sex, or drive recklessly.
Individuals with this disorder display recurrent suicidal behavior, gestures, or threats, or self-mutilating behavior (Criterion 5).
Recurrent suicidal thoughts or behavior are often the reason that these individuals present for help.
These self-destructive acts are usually precipitated by threats of separation or rejection or by expectations that the individual assume increased responsibility.
Self-mutilative acts (e.g., cutting or burning) are very common and may occur during periods in which the individual is experiencing dissociative symptoms.
These acts often bring relief by reaffirming the individual's ability to feel or by expiating the individual's sense of being evil.
Individuals with borderline personality disorder may display affective instability that is due to a marked reactivity of mood (e.g., intense episodic dysphoria, irritability, or anxiety usually lasting a few hours and only rarely more than a few days) (Criterion 6).
The basic dysphoric mood of those with borderline personality disorder is often disrupted by periods of anger, panic, or despair and is rarely relieved by periods of well-being or satisfaction.
These episodes may reflect the individual's extreme reactivity to interpersonal stresses.
Individuals with borderline personality disorder may be troubled by chronic feelings of emptiness, which can co-occur with painful feelings of aloneness (Criterion 7).
Easily bored, they may frequently seek excitement to avoid their feelings of emptiness.
Individuals with this disorder frequently express inappropriate, intense anger or have difficulty controlling their anger (Criterion 8).
They may display extreme sarcasm, enduring bitterness, or verbal outbursts.
The anger is often elicited when a caregiver or lover is seen as neglectful, withholding, uncaring, or abandoning.
Such expressions of anger are often followed by shame and guilt and contribute to the feeling they have of being evil.
During periods of extreme stress, transient paranoid ideation or dissociative symptoms (e.g., depersonalization) may occur (Criterion 9), but these are generally of insufficient severity or duration to warrant an additional diagnosis.
These episodes occur most frequently in response to a real or imagined abandonment.
Symptoms tend to be transient, lasting minutes or hours.
The real or perceived return of the caregiver's nurturance may result in a remission of symptoms.
Associated Features
Individuals with borderline personality disorder may have a pattern of undermining themselves at the moment a goal is about to be realized (e.g, dropping out of school just before graduation; regressing severely after a discussion of how well therapy is going; destroying a good relationship just when it is clear that the relationship could last).
Some individuals develop psychotic-like symptoms (e.g., hallucinations, body-image distortions, ideas of reference, hypnagogic phenomena) during times of stress.
Individuals with this disorder may feel more secure with transitional objects (i.e., a pet or inanimate possession) than in interpersonal relationships.
Premature death from suicide may occur in individuals with borderline personality disorder, especially in those with co-occurring depressive disorders or substance use disorders.
However, deaths from other causes. such as accidents or illness, are more than twice as common as deaths by suicide in individuals with borderline personality disorder.
Physical handicaps may result from self-inflicted abuse behaviors or failed suicide attempts.
Recurrent job losses, interrupted education, and separation or divorce are common.
Physical and sexual abuse, neglect, hostile conflict, and early parental loss are more common in the childhood histories of those with borderline personality disorder.
Differential Diagnosis
Depressive and bipolar disorders. Borderline personality disorder often co-occurs with depressive or bipolar disorders, and when criteria for both are met, both should be diagnosed.
Because the cross-sectional presentation of borderline personality disorder can be mimicked by an episode of depressive or bipolar disorder, the clinician should avoid giving an additional diagnosis of borderline personality disorder based only on cross-sectional presentation without having documented that the pattern of behavior had an early onset and a long-standing course.
Separation anxiety disorder in adults. Separation anxiety disorder and borderline personality disorder are characterized by fear of abandonment by loved ones, but problems in identity, self-direction, interpersonal functioning, and impulsivity are additionally central to borderline personality disorder.
Other personality disorders. Other personality disorders may be confused with borderline personality disorder because they have certain features in common.
It is therefore important to distinguish among these disorders based on differences in their characteristic features.
However, if an individual has personality features that meet criteria for one or more personality disorders in addition to borderline personality disorder, all can be diagnosed.
Although histrionic personality disorder can also be characterized by attention seeking, manipulative behavior, and rapidly shifting emotions, borderline personality disorder is distinguished by self-destructiveness, angry disruptions in close relationships, and chronic feelings of deep emptiness and loneliness.
Paranoid ideas or illusions may be present in both borderline personality disorder and schizotypal personality disorder, but these symptoms are more transient, interpersonally reactive, and responsive to external structuring in borderline personality disorder.
Although paranoid personality disorder and narcissistic personality disorder may also be characterized by an angry reaction to minor stimuli, the relative stability of self-image, as well as the relative lack of physical self-destructiveness, repetitive impulsivity, and profound abandonment concerns, distinguishes these disorders from borderline personality disorder.
Although antisocial personality disorder and borderline personality disorder are both characterized by manipulative behavior, individuals with antisocial personality disorder are manipulative to gain profit, power, or some other material gratification, whereas the goal in borderline personality disorder is directed more toward gaining the concern of caretakers.
Both dependent personality disorder and borderline personality disorder are characterized by fear of abandonment; however, the individual with borderline personality disorder reacts to abandonment with feelings of emotional emptiness, rage, and demands, whereas the individual with dependent personality disorder reacts with increasing appeasement and submissiveness and urgently seeks a replacement relationship to provide caregiving and support.
Borderline personality disorder can farther be distinguished from dependent personality disorder by the typical pattern of unstable and intense relationships.
Personality change due to another medical condition. Borderline personality disorder must be distinguished from personality change due to another medical condition, in which the traits that emerge are a direct physiological consequence of another medical condition.
Substance use disorders. Borderline personality disorder must also be distinguished from symptoms that may develop in association with persistent substance use.
Identity problems. Borderline personality disorder should be distinguished from an identity problem, which is reserved for identity concerns related to a developmental phase (e.g., adolescence) and does not qualify as a mental disorder.
Adolescents and young adults with identity problems (especially when accompanied by substance use) may transiently display behaviors that misleadingly give the impression of borderline personality disorder.
Such situations are characterized by emotional instability, existential dilemmas, uncertainty, anxiety-provoking choices, conflicts about sexual orientation, and competing social pressures to decide on careers.
Comorbidity
Common co-occurring disorders include depressive and bipolar disorders, substance use disorders, anxiety disorders (particularly panic disorder and social anxiety disorder), eating disorders (notably bulimia nervosa and binge-eating disorder), post-traumatic stress disorder, and attention-deficit/hyperactivity disorder.
Borderline personality disorder also frequently co-occurs with the other personality disorders.
#borderline personality disorder#borderline pd#personality disorder#long post#psychology#mentalheathawareness#dsm 5#mental heath support#mental illness#mental health#I love you BPD bitches#cluster b#cluster b personality disorder
5 notes
·
View notes
Text
Why Palpatine is autistic (headcanon)
Listen if I was diagnosed as autistic in 15 minutes without diagnostic assessment and by answering "eh, kind of" to 2/10 questions, then this man should be diagnosed ten times over
You can only disagree with me once you've read the whole thing <3
Part 1: DSM-5 official diagnostic criteria
Deficits in social-emotional reciprocity, ranging, for example, from abnormal social approach and failure of normal back-and-forth conversation; to reduced sharing of interests, emotions, or affect; to failure to initiate or respond to social interactions.
This criterium can include a lack of affective/emotional empathy. Also, when is Palpatine interested in the emotions of others beyond how it serves him?
Yes, he does seem socially adept. But this is something you can learn, literally. He's had a lot of training in how politicians act, how to convince people, etc. It's all an act. It's just a more severe form of masking.
And let's not forget: how much easier is social interaction when you can sense the other person's thoughts and feelings through the Force? No need to read their body language at all. You can feel what's going on and what they want to hear
Deficits in nonverbal communicative behaviors used for social interaction, ranging, for example, from poorly integrated verbal and nonverbal communication; to abnormalities in eye contact and body language or deficits in understanding and use of gestures; to a total lack of facial expressions and nonverbal communication.
Masking!! There are many moments with Palpatine where I'm like "ah, that there is very much a conscious expression, deliberately pulling those precise facial muscles, rather than something naturally happening". Same with a lot of moments of intonation.
Also, how often do you see him talk with his hands? When talking, his arms are usually rigidly at his side (or in T-Rex position).

Deficits in developing, maintaining, and understanding relationships, ranging, for example, from difficulties adjusting behavior to suit various social contexts; to difficulties in sharing imaginative play or in making friends; to absence of interest in peers.
This is specifically about equal peer relationships. Yes, Palpatine knows how to do official/business relations. You can learn that in political school or by copying others. There are rules & tactics & etiquette/protocols. But close, personal relationships?
You often see autistics in relationships with power differences, like master-apprentice/dom-sub relationships (in either role). That's a lot easier to navigate than equal peer relationships, which are a lot muddier.
Also, "absence of interest in peers". When have we seen him yearning for close personal relationships?
Stereotyped or repetitive motor movements, use of objects, or speech (e.g., simple motor stereotypes, lining up toys or flipping objects, echolalia, idiosyncratic phrases).
Palpatine does have some frequent finger tapping going on and he "worm walks" (swaying with either legs or upper body, unless focusing on walking straight and/or looking at the ground, like in the third image).

Insistence on sameness, inflexible adherence to routines, or ritualized patterns of verbal or nonverbal behavior (e.g., extreme distress at small changes, difficulties with transitions, rigid thinking patterns, greeting rituals, need to take same route or eat same food every day).
I don't think he has this one.
Highly restricted, fixated interests that are abnormal in intensity or focus (e.g., strong attachment to or preoccupation with unusual objects, excessively circumscribed or perseverative interests).
This is the big one. What neurotypical person would be able to spend every waking moment working on one singular interest (Sith Grand Plan/Dark Side), forsaking social relationships and such? Even passionate allistics wouldn't be so entirely consumed by one thing for years on end.
Palpatine also collects objects related to that interest (the Sith artifacts/artworks).
Once he's emperor he doesn't show himself much anymore but instead spends all day alone studying his special interest.
Hyper- or hyporeactivity to sensory input or unusual interest in sensory aspects of the environment (e.g. apparent indifference to pain/temperature, adverse response to specific sounds or textures, excessive smelling or touching of objects, visual fascination with lights or movement).
First of all, the depression robes from the original trilogy. That's all.
Second, I think in the Star Wars universe "sensory aspects of the environment" could apply to the Force too, in line with hyper-empathy & hypersensitivity. And guess who was born super sensitive to the Force?
Third, no neurotypical person has that kind of interior design. I'm talking about all the red. My guess is chronic under-stimulation, thus needing to be surrounded by a bright color.
Part 2: Miscellaneous/Non-diagnostic autistic traits
Gender non-conformity (always wears dresses and gives off such princess energy)
He often has T-Rex arms and when he doesn't, his arms are stiff by his side (stiff posture in general). When relaxed, the T-Rex comes out.
His father thought he was different from birth, something about Palpatine didn't appear "normal" to him
Autism & pattern recognition + seeing the inner mechanics of systems. This includes social/societal structures. Add in years of analyzing humans and their behavior/psychology. It makes it possible to see relations, predict actions, etc., either on an individual scale or a larger one.
In the same vein, good at analyzing (situations & people)
His father was said to be cruel and violent (in this house the Darth Plagueis novel is still canon, fight me). Autism + childhood trauma can turn quite intense, to put it mildly. In this case: no empathy + no attachment to other humans + learning to read people and situations very well to stay safe + tendency to rigid thinking/intense preoccupation + seeing everyone as an enemy + special interest that involves hurting others, combined with running into a Sith Lord during his formative years? Yeah, all the pieces are there.
Anyway, this headcanon is locked into my brain now and I simply can't unsee it anymore.
#autistic palpatine#sheev palpatine#autism#palpatine#darth sidious#sheevposting#chancellor palpatine#actually autistic#autistic#emperor palpatine#star wars
42 notes
·
View notes
Note
i want to chime in as another person- my mind was changed on NPD years ago but it was only because of like, real human people talking about their actual experiences that helped me realize it was not The Evil Disorder (TM) in the same way that I realized ASPD wasn't THe Evil Disorder (TM). I guess I was maybe more likely to realize something was up because i also hit a bunch of the diagnostic criteria for it but like, when literally all you hear is "narcissist just means someone is a self centered asshole" it's hard to realize that that's not actually what it is at all.
and they for real taught us that shit in school. we had a whole discussion about the myth of narcissus and how obviously that hurt ~everyone else~ more than narcissus, even though he literally starved to death and turned into a flower. it took me until i was like 17 and someone else went "hey thats kind of fucked up" before i was like oh yeah. that was probably not something he did for fun huh
idk where i'm going with this but i respect the hell out of you being willing to brave the internet goblins and be like "stop being an asshole about ppl with npd" because its gotta hurt way more when people are being an asshole about something you actually got. i made like one or two posts ages ago about the "narc abuse" ableist bullshit and i remember it being enough of a headache even when it completely and totally was not personal for me bc i do not have it
oh uh idk im sure you know this but for the people in the back sitting around, aspd is antisocial personality disorder and people with aspd are also not evil malicious serial killers in waiting or whatever the ~common interpretation~ is and people with aspd are just as capable of being good friends and normal ass people who don't run around cackling evilly or whatever and kicking puppies, just like anyone else. but buying into ableist mythology about people's diagnoses is absolutely going to cut you off from other regular people who are just living their lives and is also associated with higher rates of violence against other people :,) bigots kill
To be honest, a large chunk of the reason I get so vocal about NPD is because of how bad the ableism has wormed its way into my head. It's pretty much a daily occurrence that my housemates have to remind me that asking for help isn't manipulative and that I'm not being an evil little monster just for needing reassurance. Anti-cluster-B ableism curls up in your head and feeds on all your insecurities and struggles and it's so, so goddamn hard to deal with.
I can't ask for help getting out of bed on high pain days without getting paranoid that I've somehow manipulated my husband into being my reluctant servant. Doesn't matter how many times he reminds me that he's here because he loves me, and how helping me out of bed is an expression of that love. The internalized ableism still makes me so deeply fucking afraid that I'm the shitty one.
I have a daffodil tattooed on my head as part of my big floral scalp piece, and it's for Narcissus. Ovid's version of the story is the one that's always stuck with me the most, where Narcissus is tricked into his downfall by Nemesis. His worst crimes were "rejecting proposals from people who felt entitled to his body" and "being kind of an asshole, which is something that literally everyone is guilty of at times."
In the end, Narcissus didn't waste away because he was too self-absorbed for anything else, it happened because he was treated with trickery instead of compassion.
97 notes
·
View notes
Text
learned that the issue i have where i "go insane" and feel like my body and brain is on fire and can't sleep/ dissociate/become agoraphobic/ feel like I'm being tortured to the point that I have to boil my skin off in a bath or apply ice everywhere and scream/hit/claw myself/drive all night and sleep in my car to get a sliver of relief is because of something called Akathesia that is known to be triggered by tons of antipsychotics and bipolar meds as well as certain antibiotics and steroids.
the symptoms vary and the syndrome is notoriously hard to describe in words, but the one common description patients give is that they feel like they're being mentally and physically tortured. After Cipro last year I was so desperate I ended up soaking my feet in Epsom salts for 8 hours a day (magnesium definitely helps tamp down symptoms), and when I last had prednisone I by all definitions went totally insane the entire course and a while after the course was over. I dealt with this for years straight in high school, probably bc of antibiotics (varying intensity but often completely unbearable, i ended up suicidal and homicidal (typical for the syndrome)) and the most fucked up part is that I've been keeping bipolar meds on the table in case the mania comes back, but an estimated 20% of people end up with Akathesia from bipolar meds, and some never come back from it even after quitting meds. Antipsychotics are even worse, studies show 40-60% of patients on antipsychotics met the diagnostic criteria. and the symptoms just look like insane person shit, so basically zero chance your psychiatrist will work with you to quit them, they'll just up your dose or switch to a med that does the same thing. withdrawal actually makes the symptoms worse, so even if you do manage to quit, you'll probably end up with a prescription again
overall I had maybe 3 years since puberty where I primarily got only nighttime symptoms and only 1 year of no symptoms at all. looking back the Cipro+Prednisone I took 3 years ago for chronic ear infections probably triggered this resurgence, and I had to take Cipro AGAIN 2 months ago for a UTI (amplifying the episode frequency once more). I'm going to keep having those types of risk exposure my whole life and I already spend a good 1/5 of my time actively in an episode. I don't want to add to that
Bonus being I only discovered this bc I've been frequenting antipsych and anti therapy forums. Doctors do not care about people and want the mentally ill and other "problem patients" to die
I also wonder how many people w "slam your head into the wall" style autism are dealing with this. one of the most common presentations is a need for continual movement. I read a South African study a while back showing that therapeutic doses of magnesium+potassium (important to have both bc one uses up the other or smth in periods of stress, don't feel like looking it up rn) significantly reduced repetitive stress behaviors in autistic kids. But magnesium and potassium aren't profitable so why would the industry recommend them.
7 notes
·
View notes
Last Seen Blogs

bl-nk7
ralita

rachel-fanshun
Rachel Machinery Channel-- Fanshun

theemilyscott-blog1
Emily Scott

the-north-will-never-forget
∞ Valar Morghulis ∞
