#Hilary Cass
Text
By: Andy L.
Published: Apr 14, 2024
It has now been just little under a week since the publication of the long anticipated NHS independent review of gender identity services for children and young people, the Cass Review.
The review recommends sweeping changes to child services in the NHS, not least the abandonment of what is known as the “affirmation model” and the associated use of puberty blockers and, later, cross-sex hormones. The evidence base could not support the use of such drastic treatments, and this approach was failing to address the complexities of health problems in such children.
Many trans advocacy groups appear to be cautiously welcoming these recommendations. However, there are many who are not and have quickly tried to condemn the review. Within almost hours, “press releases“, tweets and commentaries tried to rubbish the report and included statements that were simply not true. An angry letter from many “academics”, including Andrew Wakefield, has been published. These myths have been subsequently spreading like wildfire.
Here I wish to tackle some of those myths and misrepresentations.
-
Myth 1: 98% of all studies in this area were ignored
Fact
A comprehensive search was performed for all studies addressing the clinical questions under investigation, and over 100 were discovered. All these studies were evaluated for their quality and risk of bias. Only 2% of the studies met the criteria for the highest quality rating, but all high and medium quality (50%+) studies were further analysed to synthesise overall conclusions.
Explanation
The Cass Review aimed to base its recommendations on the comprehensive body of evidence available. While individual studies may demonstrate positive outcomes for the use of puberty blockers and cross-sex hormones in children, the quality of these studies may vary. Therefore, the review sought to assess not only the findings of each study but also the reliability of those findings.
Studies exhibit variability in quality. Quality impacts the reliability of any conclusions that can be drawn. Some may have small sample sizes, while others may involve cohorts that differ from the target patient population. For instance, if a study primarily involves men in their 30s, their experiences may differ significantly from those of teenage girls, who constitute the a primary patient group of interest. Numerous factors can contribute to poor study quality.
Bias is also a big factor. Many people view claims of a biased study as meaning the researchers had ideological or predetermined goals and so might misrepresent their work. That may be true. But that is not what bias means when we evaluate medical trials.
In this case we are interested in statistical bias. This is where the numbers can mislead us in some way. For example, if your study started with lots of patients but many dropped out then statistical bias may creep in as your drop-outs might be the ones with the worst experiences. Your study patients are not on average like all the possible patients.
If then we want to look at a lot papers to find out if a treatment works, we want to be sure that we pay much more attention to those papers that look like they may have less risk of bias or quality issues. The poor quality papers may have positive results that are due to poor study design or execution and not because the treatment works.
The Cass Review team commissioned researchers at York University to search for all relevant papers on childhood use of puberty blockers and cross-sex hormones for treating “gender dysphoria”. The researchers then graded each paper by established methods to determine quality, and then disregarded all low quality papers to help ensure they did not mislead.
The Review states,
The systematic review on interventions to suppress puberty (Taylor et al: Puberty suppression) provides an update to the NICE review (2020a). It identified 50 studies looking at different aspects of gender-related, psychosocial, physiological and cognitive outcomes of puberty suppression. Quality was assessed on a standardised scale. There was one high quality study, 25 moderate quality studies and 24 low quality studies. The low quality studies were excluded from the synthesis of results.
As can be seen, the conclusions that were based on the synthesis of studies only rejected 24 out of 50 studies – less than half. The myth has arisen that the synthesis only included the one high quality study. That is simply untrue.
There were two such literature reviews: the other was for cross-sex hormones. This study found 19 out of 53 studies were low quality and so were not used in synthesis. Only one study was classed as high quality – the rest medium quality and so were used in the analysis.
12 cohort, 9 cross-sectional and 32 pre–post studies were included (n=53). One cohort study was high-quality. Other studies were moderate (n=33) and low-quality (n=19). Synthesis of high and moderate-quality studies showed consistent evidence demonstrating induction of puberty, although with varying feminising/masculinising effects. There was limited evidence regarding gender dysphoria, body satisfaction, psychosocial and cognitive outcomes, and fertility.
Again, it is myth that 98% of studies were discarded. The truth is that over a hundred studies were read and appraised. About half of them were graded to be of too poor quality to reliably include in a synthesis of all the evidence. if you include low quality evidence, your over-all conclusions can be at risk from results that are very unreliable. As they say – GIGO – Garbage In Garbage Out.
Nonetheless, despite analysing the higher quality studies, there was no clear evidence that emerged that puberty blockers and cross-sex hormones were safe and effective. The BMJ editorial summed this up perfectly,
One emerging criticism of the Cass review is that it set the methodological bar too high for research to be included in its analysis and discarded too many studies on the basis of quality. In fact, the reality is different: studies in gender medicine fall woefully short in terms of methodological rigour; the methodological bar for gender medicine studies was set too low, generating research findings that are therefore hard to interpret. The methodological quality of research matters because a drug efficacy study in humans with an inappropriate or no control group is a potential breach of research ethics. Offering treatments without an adequate understanding of benefits and harms is unethical. All of this matters even more when the treatments are not trivial; puberty blockers and hormone therapies are major, life altering interventions. Yet this inconclusive and unacceptable evidence base was used to inform influential clinical guidelines, such as those of the World Professional Association for Transgender Health (WPATH), which themselves were cascaded into the development of subsequent guidelines internationally.
-
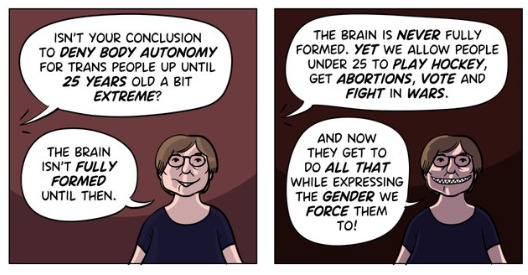
Myth 2: Cass recommended no Trans Healthcare for Under 25s
Fact
The Cass Review does not contain any recommendation or suggestion advocating for the withholding of transgender healthcare until the age of 25, nor does it propose a prohibition on individuals transitioning.
Explanation
This myth appears to be a misreading of one of the recommendations.
The Cass Review expressed concerns regarding the necessity for children to transition to adult service provision at the age of 18, a critical phase in their development and potential treatment. Children were deemed particularly vulnerable during this period, facing potential discontinuity of care as they transitioned to other clinics and care providers. Furthermore, the transition made follow-up of patients more challenging.
Cass then says,
Taking account of all the above issues, a follow-through service continuing up to age 25 would remove the need for transition at this vulnerable time and benefit both this younger population and the adult population. This will have the added benefit in the longer-term of also increasing the capacity of adult provision across the country as more gender services are established.
Cass want to set up continuity of service provision by ensure they remain within the same clinical setting and with the same care providers until they are 25. This says nothing about withdrawing any form of treatment that may be appropriate in the adult care pathway. Cass is explicit in saying her report is making no recommendations as to what that care should look like for over 18s.
It looks the myth has arisen from a bizarre misreading of the phrase “remove the need for transition”. Activists appear to think this means that there should be no “gender transition” whereas it is obvious this is referring to “care transition”.
-
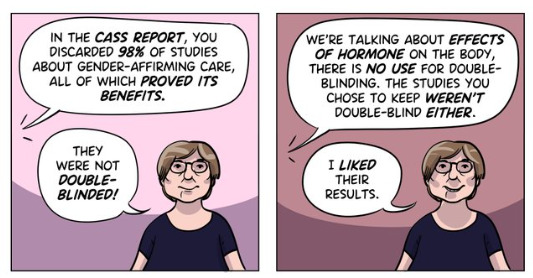
Myth 3: Cass is demanding only Double Blind Randomised Controlled Trials be used as evidence in “Trans Healthcare”
Fact
While it is acknowledged that conducting double-blind randomized controlled trials (DBRCT) for puberty blockers in children would present significant ethical and practical challenges, the Cass Review does not advocate solely for the use of DBRCT trials in making treatment recommendations, nor does it mandate that future trials adhere strictly to such protocols. Rather, the review extensively discusses the necessity for appropriate trial designs that are both ethical and practical, emphasizing the importance of maintaining high methodological quality.
Explanation
Cass goes into great detail explaining the nature of clinical evidence and how that can vary in quality depending on the trial design and how it is implemented and analysed. She sets out why Double Blind Randomised Controlled Trials are the ‘gold standard’ as they minimise the risks of confounding factors misleading you and helping to understand cause and effect, for example. (See Explanatory Box 1 in the Report).
Doctors rely on evidence to guide treatment decisions, which can be discussed with patients to facilitate informed choices considering the known benefits and risks of proposed treatments.
Evidence can range from a doctor’s personal experience to more formal sources. For instance, a doctor may draw on their own extensive experience treating patients, known as ‘Expert Opinion.’ While valuable, this method isn’t foolproof, as historical inaccuracies in medical beliefs have shown.
Consulting other doctors’ experiences, especially if documented in published case reports, can offer additional insight. However, these reports have limitations, such as their inability to establish causality between treatment and outcome. For example, if a patient with a bad back improves after swimming, it’s uncertain whether swimming directly caused the improvement or if the back would have healed naturally.
Further up the hierarchy of clinical evidence are papers that examine cohorts of patients, typically involving multiple case studies with statistical analysis. While offering better evidence, they still have potential biases and limitations.
This illustrates the ‘pyramid of clinical evidence,’ which categorises different types of evidence based on their quality and reliability in informing treatment decisions

The above diagram is published in the Cass Review as part of Explanatory Box 1.
We can see from the report and papers that Cass did not insist that only randomised controlled trials were used to assess the evidence. The York team that conducted the analyses chose a method to asses the quality of studies called the Newcastle Ottawa Scale. This is a method best suited for non RCT trials. Cass has selected an assessment method best suited for the nature of the available evidence rather than taken a dogmatic approach on the need for DBRCTs. The results of this method were discussed about countering Myth 1.
Explainer on the Newcastle Ottawa Scale
The Newcastle-Ottawa Scale (NOS) is a tool designed to assess the quality of non-randomized studies, particularly observational studies such as cohort and case-control studies. It provides a structured method for evaluating the risk of bias in these types of studies and has become widely used in systematic reviews and meta-analyses.
The NOS consists of a set of criteria grouped into three main categories: selection of study groups, comparability of groups, and ascertainment of either the exposure or outcome of interest. Each category contains several items, and each item is scored based on predefined criteria. The total score indicates the overall quality of the study, with higher scores indicating lower risk of bias.
This scale is best applied when conducting systematic reviews or meta-analyses that include non-randomized studies. By using the NOS, researchers can objectively assess the quality of each study included in their review, allowing them to weigh the evidence appropriately and draw more reliable conclusions.
One of the strengths of the NOS is its flexibility and simplicity. It provides a standardized framework for evaluating study quality, yet it can be adapted to different study designs and research questions. Additionally, the NOS emphasizes key methodological aspects that are crucial for reducing bias in observational studies, such as appropriate selection of study participants and controlling for confounding factors.
Another advantage of the NOS is its widespread use and acceptance in the research community. Many systematic reviews and meta-analyses rely on the NOS to assess the quality of included studies, making it easier for researchers to compare and interpret findings across different studies.
As for future studies, Cass makes no demand only DBRCTs are conducted. What is highlighted is at the very least that service providers build a research capacity to fill in the evidence gaps.
The national infrastructure should be put in place to manage data collection and audit and this should be used to drive continuous quality improvement and research in an active learning environment.
-
Myth 4: There were less than 10 detransitioners out of 3499 patients in the Cass study.

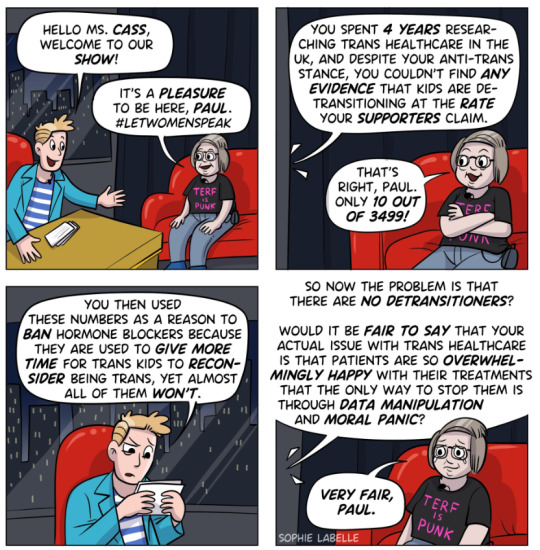
Fact
Cass was unable to determine the detransition rate. Although the GIDS audit study recorded fewer than 10 detransitioners, clinics declined to provide information to the review that would have enabled linking a child’s treatment to their adult outcome. The low recorded rates must be due in part to insufficient data availability.
Explanation
Cass says, “The percentage of people treated with hormones who subsequently detransition remains unknown due to the lack of long-term follow-up studies, although there is suggestion that numbers are increasing.”
The reported number are going to be low for a number of reasons, as Cass describes:
Estimates of the percentage of individuals who embark on a medical pathway and subsequently have regrets or detransition are hard to determine from GDC clinic data alone.
There are several reasons for this:
Damningly, Cass describes the attempt by the review to establish “data linkage’ between records at the childhood gender clinics and adult services to look at longer term detransition and the clinics refused to cooperate with the Independent Review. The report notes the “…attempts to improve the evidence base have been thwarted by a lack of cooperation from the adult gender services”.
We know from other analyses of the data on detransitioning that the quality of data is exceptionally poor and the actual rates of detransition and regret are unknown. This is especially worrying when older data, such as reported in WPATH 7, suggest natural rates of decrease in dysphoria without treatment are very high.
Gender dysphoria during childhood does not inevitably continue into adulthood. Rather, in follow-up studies of prepubertal children (mainly boys) who were referred to clinics for assessment of gender dysphoria, the dysphoria persisted into adulthood for only 6–23% of children.
This suggests that active affirmative treatment may be locking in a trans identity into the majority of children who would otherwise desist with trans ideation and live unmedicated lives.
I shall add more myths as they become spread.
==
It's not so much "myths and misconceptions" as deliberate misinformation. Genderists are scrambling to prop up their faith-based beliefs the same way homeopaths do. Both are fraudulent.
#Andy L.#Cass Review#Cass Report#Dr. Hilary Cass#Hilary Cass#misinformation#myths#misconceptions#detrans#detransition#gender affirming healthcare#gender affirming care#gender affirmation#affirmation model#medical corruption#medical malpractice#medical scandal#systematic review#religion is a mental illness
336 notes
·
View notes
Text
The Be Kind Brigade strikes again.
97 notes
·
View notes
Text


x
21 notes
·
View notes
Text
watching a tag about something likely to remove a couple basic rights and decencies from some of my friends and watching it swiftly turn into a blocklist.
there are real people's lives at play, and y'all can't stop and think about who could be The Next One to lose rights and be called subhuman trash, and made illegal within a matter of years?
8 notes
·
View notes
Text
The October 28, 2022 joint hearing of the Board of Medicine and Board of Osteopathic Medicine featured a public comment period that suspiciously began with testimony from nine anti-trans detransitioners in a row. Following the hearing, BOM member Zachariah P. Zachariah told the press that he had called these names in an order given by the Department of Health. The newly filed exhibits show that FLDOH was provided with a list of detransitioners and anti-trans parents by attorney Vernadette Broyles, president of the anti-trans Child & Parental Rights Campaign. Broyles is a prolific anti-trans activist and religious zealot who believes trans youth are the property of her deity, as she explained in a January 2020 email to a private working group of anti-trans legislators and advocacy groups.
Read more
#trans#transphobia#Florida#SB 254#trans care ban#Doe v. Ladapo#Hilary Cass#Genspect#Stella O'Malley#Joe Burgo#Vernadette Broyles#DeSantis administration#tw transphobia
10 notes
·
View notes
Text
Erin Reed at Erin In The Morning:
The anti-trans frenzy is peaking in England this week following the release of a much-anticipated review by Dr. Hillary Cass on transgender care. Many anticipated that the report would serve as a pretext to ban transgender care in England, and it appears to have been crafted to provide just such a rationale. Nations already enacting restrictive laws against transgender individuals will likely use it as justification for further discrimination. In the United States, far-right Christian nationalist groups, including Heritage Foundation (retweeted), Association of Christian Schools International, and the Alliance Defending Freedom, have cited it to support anti-trans legislation they are involved in drafting or lobbying. The Cass Review is an exercise in politics with predetermined conclusions, not science and medicine, and health authorities worldwide should reject its findings.
For those unaware of the Cass Review, and the general situation in England for transgender people, that’s understandable. Transgender people have been struggling to raise alarms there for some time after wait lists to obtain gender affirming care have ballooned in excess of 5 years, which is often prohibitive in obtaining care. After a series of political attacks on transgender people and rising anti-trans sentiment in the country, the NHS commissioned a review and tapped Dr. Hillary Cass, a pediatrician whose list of follows on social media include extremist anti-trans sources such as Transgender Trend (which argues, as is obvious, that being transgender is a “trend”), the LGB Alliance (a LGB group that believes in “dropping the T,” or transgender people), and Graham Linehan (an anti-trans activist and comedian), along with many other noted anti-trans voices. From the outset, there were concerns about her ability to conduct a study neutrally.
Over the course of the review, these concerns intensified. On one occasion, Cass met privately with medical board members selected by Governor Ron DeSantis in Florida to ban transgender care through the Florida Medical Board and appeared to collaborate via email. This only came to light during a contentious trial that revealed the board's intention to ban transgender care from the outset, prior to any review. Cass's involvement in what was essentially a predetermined strike by DeSantis against transgender people raised red flags. On another occasion, her team enlisted a researcher with a history of promoting conversion therapy as a viable option for transgender individuals to handle reviews of evidence on which the report would be based.
Now that the final report is out, it is evident that it was crafted with a predetermined conclusion in mind. The review, highly susceptible to subjectivity, disregarded the body of research on transgender care as not "high quality," a subjective judgment that cannot be trusted as politically unbiased given prior concerns. The Cass Review lends credence to claims that being transgender is "contagious" and that it can influence others around them, claims that have been debunked by dozens of medical organizations. It cites Youtube propagandists that share material from “Gays Against Groomers,” a Republican-aligned anti-transgender organization in the United States. It fearmongers that being transgender might be caused by depression, anxiety, and autism, claims that the American Psychological Association, the world's largest psychological organization, has rejected in a recent policy resolution. It asserts that rates of detransition or desistance are high, citing outdated studies from conversion therapists like Ken Zucker, who reportedly used methods such as withholding wrongly gendered toys in an attempt to "treat" transgender youth. These purportedly high rates of "detransition" or "desistance" are challenged not only by external fact checks but also data within Cass’ own review.
The review cites heavily studies that have been misleadingly used to claim that being trans may be caused by being friends with other trans people. For instance, immediately after making social contagion claims, it references a study of "2,772 adolescents" that purportedly links the question "I wish to be of the opposite sex" to "poor self-concept" and "same-sex attraction." Cass uses this to essentialy claim that many transgender individuals do not know who they are, suggesting that trans individuals may actually just be gay people influenced into being trans by being friends with other trans people—a claim without evidence, often perpetuated by those opposed to trans care. It is important to note that the study Cass cites does not concern trans people; rather, it focuses on cisgender individuals who occasionally wish they were the opposite sex for any reason, including tomboys, feminine gay boys, people experiencing sexism, and more. In that particular study, 19% of participants responded this way, a rate magnitudes higher than the often-estimated 0.5% of transgender individuals. Nevertheless, Cass includes this study as though it applies to transgender individuals, whose desire is not "occasional" but enduring.
Erin Reed's analysis on the transphobic Cass Review is spot-on.
The Cass Review, conducted by "Dr." Hilary Cass, is full of anti-trans junk science.
The report serves as a justification to further restrict trans healthcare in the United Kingdom and worldwide.
#Cass Review#Transphobia#Gender Affirming Healthcare#England#United Kingdom#Transgender Health#Hilary Cass#Social Contagion Myth#LGBTQ+#Transgender Youth
2 notes
·
View notes
Text
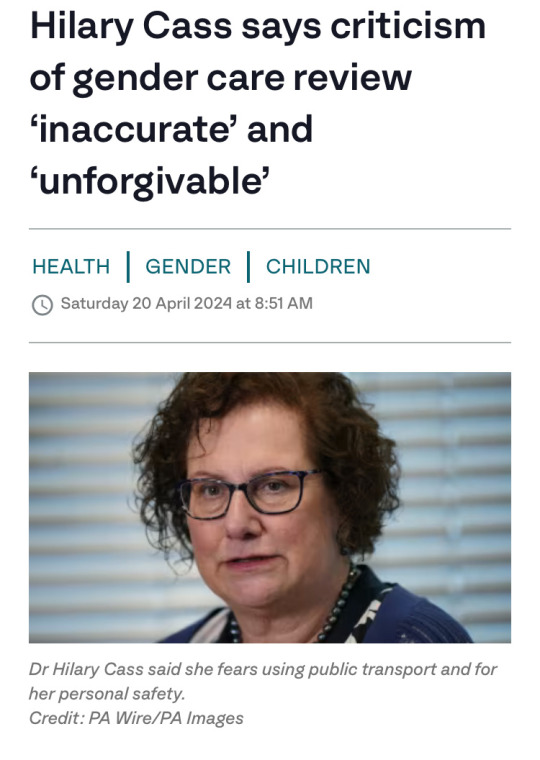
“There are few other areas of healthcare where professionals are so afraid to openly discuss their views, where people are vilified on social media, and where name-calling echoes the worst bullying behaviour. This must stop.”
#transgender#transsexual#gender identity#gender equality#Hilary Cass#puberty blockers#gender affirming care
2 notes
·
View notes
Text
An Over Written Post About Hilary Cass
Hey, so chances are, you folks have probably heard about something in the UK that cam out recently called the Cass Report. Named after the woman behind it, Hilary Cass, the report purports to provide a thorough, impartial evaluation of trans healthcare in the UK, with the intention of being used a guidance going forward.
Now, if you've already heard about the report, you've probably also heard how this this thing has more holes than swiss cheese and seems to be held together by spit, safety pins and seething hatred for us uppity queers. For example, you probably heard how Cass chose to disregard 50 out of 51 studies that support the current model of trans health care, on the grounds that they didn't utilize a "Double Blind study group", something that is recognised by medical professionals to both unethical and untenable in this situation, whilst accepting as evidence four studied that suggested trans healthcare had negligible results, all four of which ALSO did not make use of a double blind.
She also believes the toys children play with are biologically pre-determined. Seriously. Boys like trucks, girls like dollies, basic biology, simple as.
But this overly long post isn't about the report, it's about Hilary Cass the person. Who is this totally impartial, fair and balanced individual?
Well, this exact same Hilary Cass has personally warned the Conservative Minister for Equalities (this is actually very funny, trust me), Kemi Badenoch, of the "risks" of any kind of ban on conversion therapy.
In addition, Hilary Cass is a follower and supporter of far-right anti trans hate group, "Transgender Trend", an astroturfed UK group that was one of many found to have been the receipient of vast amounts of dark money from US Conservative groups such as the Heritage Foundation and Alliance Defending Freedom.

"But wait Neko!" I hear you cry, "Us poor Yanks are feeling all left out, is there anything she's done over on our side of the pond?" Well, my hypothetical American reader, there is, how astute of you.
Cass has also worked very closely with Patrick Hunter of the Catholic Medical Association as a consultant on potential anti-trans and anti-LGBT legislation to be implemented by Govenor Ron DeSantis. The CMA is an overtly anti-LGBT organisation and Hunter himself is purportedly part of a group of anti-trans activists working across the United States to undermine and undo LGBT rights, for which he was hand picked by Ron DeSantis for his role in the "Florida Review".
So yeah.
Hilary Cass: A fair, balanced, impartial, hate group following, conversion therapy supporting, fascist policy advising writer of the Cass Report.
#lgbtq#transgender#trans#lgbt pride#lesbian#gay#bisexual#uk#current events#cass report#hilary cass#this post was brought to you by a pissed off tranny dyke with too much time and anger on her hands
1 note
·
View note
Text

Following publication of the final report there have been a number of questions and points for clarification about the findings and recommendations. We have collated those questions, along with our answers, on this page.
-
Did the Review set a higher bar for evidence than would normally be expected?
No, the approach to the assessment of study quality was the same as would be applied to other areas of clinical practice – the bar was not set higher for this Review.
Clarification:
The same level of rigour should be expected when looking at the best treatment approaches for this population as for any other population so as not to perpetuate the disadvantaged position this group have been placed in when looking for information on treatment options.
The systematic reviews undertaken by the University of York as part of the Review’s independent research programme are the largest and most comprehensive to date. They looked at 237 papers from 18 countries, providing information on a total of 113,269 children and adolescents.
All of the University of York’s systematic review research papers were subject to peer review, a cornerstone of academic rigour and integrity to ensure that the methods, findings, and interpretation of the findings met the highest standards of quality, validity and impartiality.
-
Did the Review reject studies that were not double blind randomised control trials in its systematic review of evidence for puberty blockers and masculinising / feminising hormones?
No. There were no randomised control studies identified in the systematic reviews, but other types of studies were included if they were well designed and conducted.
Clarification:
The Review commissioned the University of York to undertake an independent research programme to ensure the work of the Review and its recommendations were informed by the most robust existing evidence. This included a series of systematic reviews which brought together, analysed and evaluated existing evidence on a range of issues relating to the care of gender-questioning children and young people, including epidemiology, treatment approaches and international models of current practice.
Randomised control trials are considered the gold standard in relation to research, but there are many other study designs that can give valuable information. Explanatory Box 1 (pages 49-51 of the final report) discusses in more detail the different kinds of studies that can be used, and how to decide if a study is poorly designed or biased.
Blinding is a separate issue. It means that either the patient or the researcher does not know if the patient is getting an active treatment or a ‘control’ (which might be another treatment or a placebo). Patients cannot be blinded as to whether or not they are receiving puberty blockers or masculinising / feminising hormones, because the effects would rapidly become obvious. Good RCTs can be conducted without blinding.
The University of York’s systematic review search did not identify any RCTs, blinded or otherwise, but many other studies were included. Most of the studies included were called ‘cohort studies’. Well-designed and executed high quality cohort studies are used in other areas of medicine, and the bar was not set higher for this review; even so the quality of the studies was mostly only assessed as moderate.
-
Did the Review reject 98% of papers demonstrating the benefits of affirmative care?
No. Studies were identified for inclusion in the synthesis (conclusions) of the systematic reviews on puberty blockers and masculinising/feminising hormones on the basis of their quality. This was assessed using a standard quality assessment tool appropriate to the types of study identified. All high quality and moderate quality reviews were included in the synthesis of results. This totalled 58% of the 103 papers.
Clarification:
The Newcastle-Ottawa scale (a standard appraisal tool) was used to compare the studies. This scores items such as participant selection, comparability of groups (how alike they are), the outcomes of the studies and how these were assessed (data provided and whether it is representative of those studied). High quality studies (scoring >75%) would score well on most of these items; moderate quality studies (scoring >50% – 75%) would miss some elements (which could affect outcomes); and low-quality studies would score 50% or less on the items the scale looked at. A major weakness of the studies was that they did not have adequate follow-up – in many cases they did not follow young people for long enough for the long-term outcomes to be understood.
Because the ranking was based on how the studies were undertaken (their quality and execution), low quality research was removed before the results were analysed as the findings could not be completely trusted. Had an RCT been available it would also have been excluded from the systematic review if it was deemed to be of poor quality.
The puberty blocker systematic review included 50 studies. One was high quality, 25 were moderate quality and 24 were low quality. The systematic review of masculinising/feminising hormones included 53 studies. One was high quality, 33 were moderate quality and 19 were low quality.
All high quality and moderate quality reviews were included, however as only two of the studies across these two systematic reviews were identified as being of high quality, this has been misinterpreted by some to mean that only two studies were considered and the rest were discarded. In reality, conclusions were based on the high quality and moderate quality studies (i.e. 58% of the total studies based on the quality assessment). More information about this process in included in Box 2 (pages 54-56 of the final report)
-
Has the Review recommended that no one should transition before the age of 25 and that Gillick competence should be overturned.
No. The Review has not commented on the use of masculinising/feminising hormones on people over the age of 18. This is outside of the scope of the Review. The Review has not stated that Gillick competence should be overturned.
The Review has recommended that:
“NHS England should ensure that each Regional Centre has a follow through service for 17-25-year-olds; either by extending the range of the regional children and young people’s service or through linked services, to ensure continuity of care and support at a potentially vulnerable stage in their journey. This will also allow clinical, and research follow-up data to be collected.”
This recommendation only relates to people referred into the children and young people’s service before the age of 17 to enable their care to be continued within the follow-through service up to the age of 25.
Clarification:
Currently, young people are discharged from the young people’s service at the age of 17, often to an adult gender clinic. Some of these young people have been receiving direct care from the NHS gender service (GIDS as was) and others have not yet reached the top of the waiting list and have “aged out” of the young people’s service before being seen.
The Review understands that this is a particularly vulnerable time for young people. A follow-through service continuing up to age 25, would remove the need for transition (that is, transfer) to adult services and support continuity of care and continued access to a broader multi-disciplinary team. This would be consistent with other service areas supporting young people that are selectively moving to a ‘0-25 years’ service to improve continuity of care.
The follow-through service would also benefit those seeking support from adult gender services, as these young people would not be added to the waiting list for adult services and, in the longer-term, as more gender services are established, capacity of adult provision across the country would be increased.
People aged 18 and over, who had not been referred to the NHS children and young people’s gender service, would still be referred directly to adult clinics.
-
Is the Review recommending that puberty blockers should be banned?
No. Puberty blocker medications are used to address a number of different conditions. The Review has considered the evidence in relation to safety and efficacy (clinical benefit) of the medications for use in young people with gender incongruence/gender dysphoria.
The Review found that not enough is known about the longer-term impacts of puberty blockers for children and young people with gender incongruence to know whether they are safe or not, nor which children might benefit from their use.
Ahead of publication of the final report NHS England took the decision to stop the routine use of puberty blockers for gender incongruence / gender dysphoria in children. NHS England and National Institute for Health and Care Research (NIHR) are establishing a clinical trial to ensure the effects of puberty blockers can be safely monitored. Within this trial, puberty blockers will be available for children with gender incongruence/ dysphoria where there is clinical agreement that the individual may benefit from taking them.
Clarification:
Puberty blockers have been used to suppress puberty in children and young people who start puberty much too early (precocious puberty). They have undergone extensive testing for use in precocious puberty (a very different indication from use in gender dysphoria) and have met strict safety requirements to be approved for this condition. This is because the puberty blockers are suppressing hormone levels that are abnormally high for the age of the child.
This is different to stopping the normal surge of hormones that occur in puberty. Pubertal hormones are needed for psychological, psychosexual and brain development, and there is not yet enough information on the risks of stopping the influence of pubertal hormones at this critical life stage.
When deciding if certain treatments should be routinely available through the NHS it is not enough to demonstrate that a medication doesn’t cause harm, it needs to be demonstrated that it will deliver clinical benefit in a defined group of patients.
Over the past few years, the most common age that young people have been receiving puberty blockers in England has been 15 when most young people are already well advanced in their puberty. The new services will be looking at the best approaches to support young people through this period when they are still making decisions about longer-term options.
-
Has the Review recommended that social transition should only be undertaken under medical guidance?
The Review has advised that a more cautious approach around social transition needs to be taken for pre-pubertal children than for adolescents and has recommended that:
“When families/carers are making decisions about social transition of pre-pubertal children, services should ensure that they can be seen as early as possible by a clinical professional with relevant experience.”
Parents are encouraged to seek clinical help and advice in deciding how to support a child with gender incongruence and should be prioritised on the waiting list for early consultation on this issue. This should include discussion of the risks and benefits and the voice of the child should be heard. It will be important that flexibility is maintained, and options remain open.
Clarification:
Although the University of York’s systematic review found that there is no clear evidence that social transition in childhood has positive or negative mental health outcomes, there are studies demonstrating that for a majority of young children presenting with gender incongruence, this resolves through puberty. There is also evidence from studies of young people with differences of sex development (DSD) that sex of rearing seems to have some influence on eventual gender outcome, and it is possible that social transition in childhood may change the trajectory of gender identity development for children with early gender incongruence. Living in stealth from early childhood may also lead to stress, particularly as puberty approaches.
There is relatively weak evidence for any effect of social transition in adolescence. The Review recognises that for adolescents, exploration is a normal process, and rigid binary gender stereotypes can be unhelpful. Many adolescents will go through a period of gender non-conformity in terms of outward expressions (e.g. hairstyle, make-up, clothing and behaviours). They also have greater agency in how they present themselves and in their decision-making.
Young people and young adults have spoken positively about how social transition helped to reduce their gender dysphoria and feel more comfortable in themselves. They identified that space to talk about socially transitioning and how to handle conversations with parents/carers and others would be helpful. The Review has therefore advised that it is important to try and ensure that those already actively involved in the young person’s welfare provide support in decision making and that plans are in place to ensure that the young person is protected from bullying and has a trusted source of support.
Further detail can be found in Chapter 12 of the Final Report.
-
Did the Review speak to any gender-questioning and trans people when developing its recommendations?
Yes, the Review has been underpinned by an extensive programme of proactive engagement, which is described in Chapter 1 of the report. The Review has met with over 1000 individuals and organisations across the breadth of opinion on this subject but prioritised two categories of stakeholders:
People with relevant lived experience (direct or as a parent/carer) and organisations working with LGBTQ+ children and young people generally.
Clinicians and other relevant professionals with experience of and/ or responsibility for providing care and support to children and young people within specialist gender services and beyond.
A mixed-methods approach was taken, which included weekly listening sessions with people with lived experience, 6-weekly meetings with support and advocacy groups throughout the course of the Review, and focus groups with young people and young adults.
Reports from the focus groups with young people with lived experience are published on the Review’s website and the learning from these sessions and the listening sessions are represented in the final report.
The Review also commissioned qualitative research from the University of York, who conducted interviews with young people, young adults, parents and clinicians. A summary of the findings from this research is included as appendix 3 of the final report.
-
What is the Review’s position on conversion therapy?
Whilst the Review’s terms of reference do not include consideration of the proposed legislation to ban conversion practices, it believes that no LGBTQ+ group should be subjected to conversion practice. It also maintains the position that children and young people with gender dysphoria may have a range of complex psychosocial challenges and/or mental health problems impacting on their gender-related distress. Exploration of these issues is essential to provide diagnosis, clinical support and appropriate intervention.
The intent of psychological intervention is not to change the person’s perception of who they are but to work with them to explore their concerns and experiences and help alleviate their distress, regardless of whether they pursue a medical pathway or not. It is harmful to equate this approach to conversion therapy as it may prevent young people from getting the emotional support they deserve and make clinicians fearful of providing this group of children and young people the same care as is afforded to other children and young people.
No formal science-based training in psychotherapy, psychology or psychiatry teaches or advocates conversion therapy. If an individual were to carry out such practices they would be acting outside of professional guidance, and this would be a matter for the relevant regulator.
==
Like any religious fanatics, pathological liars like "Erin" Reed and "Alejandra" Carballo still won't stop lying, since it's all they have. But their disciples should really be noticing how they've been directly refuted.
#Cass review#Cass report#Hilary Cass#Dr. Hilary Cass#disinformation#misinformation#pathological liars#Erin Reed#Alejandra Carabello#Michael Hobbes#medical scandal#medical corruption#medical malpractice#gender affirming care#gender affirming healthcare#gender affirmation#compulsive liars#gender fanatics#gender cult#gender ideology#gender identity ideology#queer theory#intersectional feminism#puberty blockers#cross sex hormones#wrong sex hormones#religion is a mental illness
35 notes
·
View notes
Text



#Don't tell me anything. I'm trying to reborn my exhausted brain.#tapadoodles#Cass over here started a f***ing war#On three fronts#Listen to me#RUN.#I mean I will stay#But you better run#meteorites literally from all over#and Cass just hilariously laughing from above#Let me go free I wanna in this chaos please
2K notes
·
View notes
Text
19 notes
·
View notes
Text
Bruce is the only member of the batfam that has no tolerance for spice. Dick grew up in a travelling circus, he has had food from all over the world. Jason grew up on the street, he ate what he could get. Tim's parents went all around the world, and had food and recipes from all around the world, whenever they were home Janet would make exotic meals. Damian grew up with Talia, he grew up on middle eastern food. But Bruce? He grew up on Alfred's British ass cooking, he thinks pepper has 'a little kick'.
#needless to say the kids find this hilarious#also. Dick would make spicy food for them all#Dick and Jason would have competitions for who can eat more spice#Dick won everytime#Some may say that Tim also has no spice tolerance... and they may be right... But I think its funnier if its just Bruce#I would add cass but idk her well enough#btw that pepper comment is something my dad has actually said#tim drake#batfam#jason todd#dick grayson#bruce wayne#damian wayne#batfamily#batbros#batgang#batboys#dcu#dc#should I add their hero names?#ehhhhh#why not#batman#nightwing#red hood#red robin#robin
8K notes
·
View notes
Text
donna’s route: in summary



#resident lover#donna beneviento#cassandra dimitrescu#the fact cass just kept wiggling her way into donna’s route is hilarious#resident lover memes
405 notes
·
View notes
Text
The tide is turning for the TQ+. And they have no one to blame but themselves
Wes Streeting last night admitted he had been wrong to say that “trans women are women” amid a major Labour row over the Cass review into NHS gender care.
The shadow health secretary said the controversial LGBT rights group Stonewall – where he used to work – had got it wrong with its slogan.
In a major about-turn for the party, he told The Sun that he now admitted “there are lots of complexities” on the trans issue but that he was prepared to take criticism “on the chin”.
It came as Labour became embroiled in another trans row after Mr Streeting welcomed the review and pledged to implement it in full.
The shadow health secretary said the report raised “some serious concerns that are pretty scandalous”.

But Rosie Duffield, a Labour MP placed under investigation by the party last year for campaigning against gender ideology, pointed out that women who had exposed the scandal had been “blanked, sidelined and dismissed” by male leaders simply for speaking up.
Last night Mr Streeting was asked on The Sun’s Never Mind The Ballots programme whether he stood by Stonewall’s claim that “trans women are women, get over it”, he admitted: “No.”
He added: “To the extent that – and I say this with some self-criticism and reflection – if you’d asked me a few years ago, on this topic, I would have said trans men are men, trans women are women. Some people are trans, get over it. Let’s move on. This is all blown out of proportion.
“And now I sort of sit and reflect and think actually, there are lots of complexities.”
He went on: “I take the criticism on the chin. And at the same time, I also think that there’s been some absolutely ugly rhetoric directed towards trans people who are at the wrong end of all of statistics on hate crime, on self harm, suicide, mental health.”
Labour has long been divided on trans issues and has been accused of flip-flopping on its stance in recent years.
The party no longer has plans to bring in self-ID for trans people, and Sir Keir Starmer, the Labour leader, has rowed back from saying “trans women are women”, and now states that a woman is an “adult female” and that 99.9 per cent of them do not have a penis.
Mr Streeting’s comments angered the Labour Left. The Corbynite group Momentum tweeted: “The Cass review ignored dozens of scientific studies, coming to a harmful conclusion of limiting access to gender-affirming care for trans youth.
“Anti-trans campaigners have celebrated it. So it’s highly disappointing that Labour’s leadership is welcoming it unreservedly.”
Yesterday, feminist Julie Bindel demanded an apology from Mr Streeting for failing to support her gender-critical views when he was president of the National Union of Students.
Earlier this year, the party dropped a year-long investigation into a complaint that Ms Duffield had been transphobic for liking a tweet by Father Ted creator Graham Linehan, who is now a gender-critical campaigner.
However, despite the changes, critics of the Labour leadership say gender-critical women in the party continue to be sidelined or not selected.

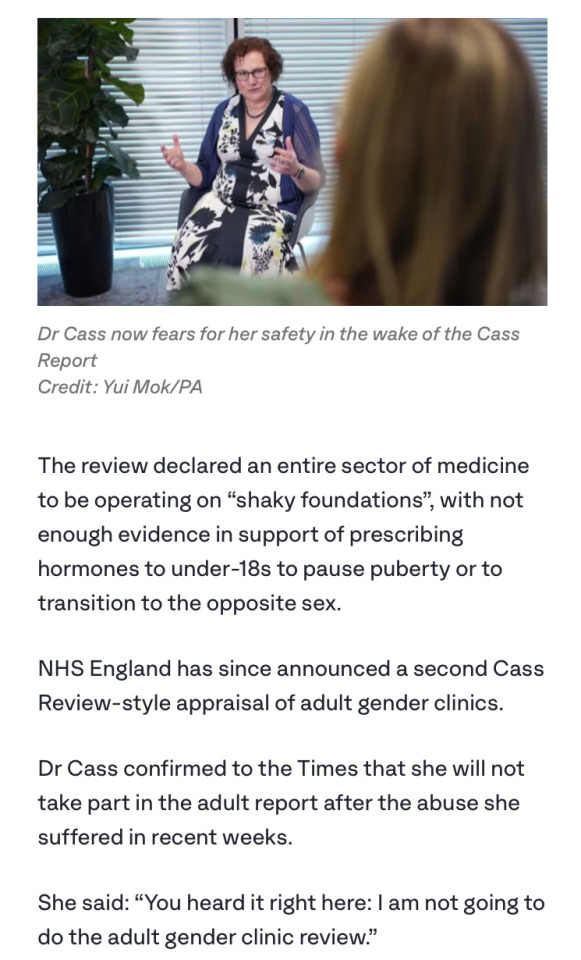
Wes Streeting says the Cass report raised 'some serious concerns that are pretty scandalous' CREDIT: Jay Williams
The Cass review, published on Wednesday, said much of the evidence for gender medicine was flimsy and that drugs such as puberty blockers should be used with extreme caution as children who think they are trans may have mental health problems.
Dr Hilary Cass, the paediatrician behind the report, said some NHS gender clinics refused to comment on requests for information.
On Never Mind the Ballots, Mr Streeting said: “I think we’ve got to ask ourselves why is it that we’ve seen medical interventions that have been given on the basis of very weak evidence?
“How is it that clinicians have been silenced or afraid to come forward? Why is it that a group of young people who are extremely vulnerable are waiting years to access treatment?
“I think there’s plenty of blame to go around. I’m pretty angry actually that despite this review having been commissioned there are some NHS trusts that refused to co-operate.
“And I want to send a clear message to them that under a Labour government there’ll be accountability for that, you’re not going to get away with it. And I want to work constructively with the Government to try to get this right.”
Earlier, he had tweeted: “Children’s healthcare should always be led by evidence and children’s welfare, free from culture wars…
“The Government must now immediately act, but if they do not, the next Labour government will work to implement the expert recommendations of the Cass review, to ensure that young people are receiving appropriate and high-quality care.”
This prompted Ms Duffield to retweet the statement, with the message: “To the many women blanked, sidelined, dismissed by male leaders when speaking up and exposing this for years.”

And Ms Bindel, a former Labour Party member, wrote: “Glad to see you are now openly critical of the gender ideology that led to the atrocities against children outlined in the Cass report.
“I am open to accepting an apology from you. In 2008, when you were NUS president, I was no-platformed alongside five fascist groups for ‘transphobia’.
“I contacted you and asked for your help. You gave none. I asked you to condemn those that had orchestrated the no-platforming, and you refused.
“Have you any idea of the reputational damage this caused me? How it gave others permission to no-platform, denounce and defame me?
“How it meant that I could be slandered by other organisations, and so many, many universities around the UK and elsewhere? If this sounds bitter then good, because I am.”
To this message, Ms Duffield said: “Thank you for leading us all here Julie. Without you, most of us wouldn’t have had a clue what had been happening to children who were far too young to have the critical faculties or agency to consent.”
Addressing Ms Bindel’s accusation, Mr Streeting replied: “From memory (16 years on, so correct me if I’m wrong!) I replied to confirm that you weren’t on NUS’ no platform policy and as this was in relation to a motion passed by the autonomous women’s campaign I was not empowered to overturn it (not least as a male president!).”
#Trans women are men#Labour Party#NHS gender care#Wes Streeting is a rare man that can admit that he was wrong#Rosie Duffield is speaking the truth#Sir Keir Starmer finally admits that women don't have penises#Men seeing the light after women have suffered from stating the obvious#Cass review#Dr Hilary Cass urges caution when gives children life altering drugs and treatments
93 notes
·
View notes
Text
Dc x dp idea 19
Danny outs himself and Vlad to Bruce Wayne at a gala. Why because he thinks Bruce is Batman’s sugar daddy. Best way to get a message to him obviously. Turns out he didn’t have to Jazz was at the gala and punched Vlad straight in the face.
So vlad finally gives up on Maddie. Maybe she found out he was half ghost and tried to kill him not really too important. Vlad is a sore loser
Meaning he kills Maddie, jack, and Danny’s friends to isolate him. Jazz is away at Gotham U and Vlad doesn’t bother to check that everyone was there when he killed them.
Danny is trapped at vlad manors like how sam was with the tiara. Anyone who may not know or recall the episode a bs princess contest was hosted sam won, weirdo with a castle (much like vlad) decided to trap her with a magic crown. She just couldn’t leave the castle (now like Danny)
Jazz thinks Danny died in the explosion. Vlad paid the custody lawyers and cops hush money as to not alert anyone Danny was alive. He needed to keep his little badger “safe”.
Vlad now has no one to stop him and has his perfect son in his grasps. He turns to world domination.
Time passes and word of Vlads adoptive son gets out. Both get invited to many galas. Danny has no say in anything and is just trying to get the damn watch off. Vlad only agree to go to the Wayne’s gala as he had never been invited before.
After a few safety precautions. Sending his ghost animals ahead to essentially hold the rich hostage. Danny would behave if it meant keep others safe after all. So the watch gets taken off for a shocker and way to prevent him from using his powers for the trip to Gotham.
Danny is just thinking of Tucker’s theory that Bruce is Batman’s sugar daddy. Sam just thought he was Batman.
So Danny writes a note addressed to Bruce.
Basically says hey vlad is plasmius. He’s a fruitloop killed my family and friends to adopt me. Please help. Btw vlad rigged the gala with ghost in case i tried anything. He has me and them connected to the totally secret remote in his front pocket. Shocks me and makes the animals attack. Don’t be mean to them. He experimented on my animal friends. So like don’t be suspicious and please pass this on to batman. Pretty sure your his sugar daddy Hence the note to you.
He does manage to pass the note on. Bruce and his kids all kinda look at him in shock.
Only then does jazz walk in with some dude with a white streak. She looked at him then vlad. Then him again. Vlad was sweating. Danny was grinning.
She then immediately decks him and tackels vlad. All while Bruce reads the note.
Dick and Jason are now involved. Danny is yelling about the remote. It goes flying Damian catches it. The ghost animals appear. Danny tells which button to click. Damian frees the ghost animals and danny from there collars or in Danny’s case watch.
#danny fenton#danny phantom#dc x dp#dp x dc#dp dc crossover#dp x dc prompt#dp x dc crossover#vlad is not a good guy#jazz and Jason are cute together#they saw her moun Danny hence there shock#Danny had been to busy trying to escape to process his emotions#jazz is older in this#the bat kids find it hilarious when they find out Danny thought Bruce was a sugar daddy#Bruce is reading the letter just like wtf#before he can do anything the Chaos was too much for him to salvage#Jason is down for a smack down#dick is trying to not cause anymore of a scene#Damian befriends the ghost animals after he fried them#cass actually came down from the roof#vlad gets arrested#jazz was mourning his human life#she new he’s be a full ghost#when vlad went nuts she assumed he had her brothers ghost#she was the one who hinted that they should invite vlad#she wasn’t gonna out him. what if he hurt Danny#jazz is a good sister#Danny’s rouges come to check in him once they can feel his signature#cujo is the first one#cujo likes Damian and Damian wants to steal cujo#jazz calls vlad out for making her think her only brother was dead immediately after she tackles him
488 notes
·
View notes
Text

“Most of all, he listened for Jyn. He listened for her struggles. He listened for her voice. He tried to determine which steady tread on the sand was hers.
For all Cassian heard, she might have vanished from the face of Jedha.
She dominated his thinking nonetheless. Cassian believed neither pity nor pragmatism explained it.”
-Rogue One Novelisation by Alexander Freed
#i went through like 4 different quotes for this one#BUT THIS ONE!!!#HE LISTENED FOR JYN!!#SHE DOMINATED HIS THINKING!!!#NEITHER PITY NOR PRAGMATISM EXPLAINED IT!!!#mind you he has known her for all of like 5 hours at this point. cass ur crush is showinggggg#alexander freed what was the meaning of this#you write this ans expect me to NOT lose my mind???#anyways i love that cassian is walking normally and jyn is taking huge steps to keep in step with him. hilarious#rogue one#jyn erso#cassian andor
294 notes
·
View notes
Last Seen Blogs

schou04powers
无标题
tarottsi
˚✦.some thoughts of mine.✦˚

julifun
Juli Fun :'3

buildowk922
챔피언게임 광고문의주세요 0502

nonton21yuk
Untitled