#cass report
Text
"Sex is biological fact, NHS declares."
Fuckin FINALLY.
The article's behind a paywall, so I had to grab a screenshot fast. It's not the clearest picture, and I may have cut some off.
Here's the article, if you can get around the paywall.


From BBC News via Yahoo News:
NHS England charter to stress biological sex when placing patients in wards
Transgender women should not be put on single-sex female NHS wards, the government is proposing.
The measure is part of a raft of changes to the NHS Constitution for England, the charter of rights for patients.
The proposals stress the importance of biological sex for the first time when it comes to same-sex accommodation and intimate care.
In both cases, the rights are available only where possible.
For example, same-sex accommodation rights, which have existed for years, can and are breached where there is a clinically urgent need to admit and treat a patient and do not extend to areas such as critical care or accident and emergency.
The guidance also means that trans men should not be housed on single-sex male wards.
Under the proposals:
transgender people, whose gender identity differs from their biological sex, may be provided single rooms, where appropriate
patients will have the right to request a person of the same biological sex delivers any intimate care
Health Secretary Victoria Atkins said it was about making it clear that "sex matters".
"We want to make it abundantly clear that if a patient wants same-sex care, they should have access to it wherever reasonably possible," she said.
"By putting this in the NHS Constitution, we're highlighting the importance of balancing the rights and needs of all patients, to make a healthcare system that is faster, simpler and fairer to all."
'Trampled over'
Maya Forstater, of the Sex Matters campaign group, said the changes were "excellent news".
"The confusion between 'sex' and 'gender' in official policies like the NHS Constitution is what has enabled women's rights to be trampled over in the name of transgender identities," she said.
But Cleo Madeleine, of Gendered Intelligence, said robust policies were already in place and the government had its priorities wrong.
"After 14 years of austerity, medical professionals are crying out for more funding, more resources, and better conditions for staff and patients," she said.
"The government seems hell-bent on pursuing its obsession with the transgender community instead of addressing these longstanding needs."
'Martha's rule'
The changes are part of a wider review of the NHS Constitution, which the government must complete every 10 years.
They also include a plan to embed patients and their loved ones' right to access a rapid review from outside the care team if the patient is deteriorating.
This is the right behind "Martha's rule", which is being introduced in the NHS, to ensure patients know they can ask for a second opinion, with the government providing funding to hospitals for posters and leaflets informing patients and their families.
Martha Mills died aged 13, after being admitted to King's College Hospital, south London, in 2021, having injured her pancreas slipping on to the handlebars of her bike while cycling.
She later developed sepsis - but with better care, could have survived, an inquest found.
All the changes will be consulted on over the next eight weeks, before the constitution is updated later this year.
Labour's shadow health secretary Wes Streeting said: "Rights on paper are worthless unless they are delivered in practice.
"The NHS constitution already pledges that no patient will have to share an overnight ward with patients of the opposite sex, but that is not the case for too many patients."
#sex is fact#sex not gender#Cass report#Cass review#WPATH#gender critical#NHS#the tide is turning#the telegraph#the daily telegraph#BBC news
261 notes
·
View notes
Text
This is what happen when people take the 'your brain doesn't mature till 25' pop-sci too literally and just ran with it, also transphobia
#england#britain#rishi sunak#trans#lgbt#lgbtqia+#natalie wynn#contrapoints#queer#trans rights#cass review#cass report
8K notes
·
View notes
Text
"They shouldn't socially transition until after 25"
So trans people magically aren't adults at 18 like cis people!?!?!????
[sarcasm] Wow yeah that sounds good and like something a normal government would say. Hope this isn't a dangerous precedent that will be used to repeal rights from other minority groups
6K notes
·
View notes
Text
My favourite part of the Cass Report is where she goes: “Florence Ashley and others have shown that gatekeeping doesn’t work and should be abandoned. We disagree, not based on any evidence but because it’s incompatible with the way we’ve already decided we wanted to do things.”
#transgender#lgbtq#trans#queer#lgbtqia#lesbian#gay#lgbt#books#trans lit#cass review#cass report#gender affirming care#gender affirming healthcare#trans healthcare
1K notes
·
View notes
Text



Yeah so fuck the cass report
#cass report#cass review#transgender#trans in the uk#UK#trans ftm#trans mtf#trans teen#ppg#ace copular#ace ppg#gangreen gang#gangreen gang ppg
753 notes
·
View notes
Text
UK petition: Sandyford Clinic [Scotland] to immediately continue to prescribe trans kids hormone blockers
[ Sign here ]
Following the Cass Review, trans kids are no longer able to receive puberty blocker prescriptions from Sandyford, Scotland's only gender identity clinic for under 18s.
This is devastating news for trans kids who will now see their bodies change in ways that will trigger dysphoria. It will ultimately cost lives as trans kids are driven to suicide. All this will happen because of some despicable, manufactured "trans debate", where trans kids, and adults, are being used as a scapegoat for society's problems.
Trans charities and advocate groups are condemning the awful Cass Review all over the country. The only groups celebrating this dreadful document are anti-trans ones.
Hormone blockers have been used for decades safely, and the vast majority of trans kids that go on to transition are happy.
A common argument against blockers is that trans kids are not old enough to make such decisions. This is exactly what puberty blockers are for; to hit the pause button on any irreversible changes; to give trans kids time to make these decisions.
We urge Sandyford clinic to immediately resume providing trans kids with their life-saving puberty blockers.
[ Sign here ]
#petition#UK#projects#cass review#cass report#armchair activism#puberty blockers#sandyford clinic#scotland#trans
566 notes
·
View notes
Text
The Cass Report demonstrates a truly ridiculous ignorance of literally *anything* to do with not only trans lives, but basic medical treatment protocols.
You *cannot* do double-blind tests where an intervention very clearly has distinct observable effects. Medicine also frequently does not do double-blind tests when doing so would be a) basically impossible, and b) inhumane. It’s particularly common to measure efficacy of an intervention by follow-up and statistical analysis where children and young people are concerned because experimenting on kids is so fucking unethical.
The report is treating reports following established medical protocols as though they are some kind of pseudoscience. Literally the only reasons for this are either a) an ignorance of basic medical and research procedures so profound as to show an utter unsuitability to be involved in reporting on anything to do with healthcare or b) blatant disingenuousness to find an excuse to discard the results they don’t want to acknowledge. Which also renders them deeply unsuitable to report on anything to do with healthcare.
They have used to existence of nonbinary people as an excuse to deny under-25s transition care, treating our entire identity as some sort of adolescent identity crisis. As a 40-year old nonbinary person, I can only say how *utterly* this betrays a profound ignorance of trans culture and identity and/or a commitment to patriarchal and colonial gender norms so profound they are utterly unwilling to dive into the easily-available evidence of adults all over the world with nonbibary identities today, and the anthropological and historical evidence of cultures all over the world with an understanding of gender outside the binary.
And the recommendation that transition should be forbidden to people with mental illness or neurodivergence only betrays how deeply and profoundly transphobia is entwined with disableism. There is a line which literally says “transition did not affect manifestation of symptoms of autism spectrum disorder”. As if this was remotely relevant to anything other than pathologising both transness and neurodivergence.
It of course also attempts to ignore the reality that millions of British adults are seeking neurodivergence diagnoses through the NHS and being turned down or stuck on waiting lists that can easily be *seven* years long.
I am sick with fury and fear, and trying to mute my own reactions because I have a dissertation draft due in tomorrow I *need* to work on.
#cass report#transphobia#institutional transphobia#disableism#ableism#profound and probably wilful ignorance of basic medical testing protocols#terf island#autistic adult
333 notes
·
View notes
Text
The whole “your brain doesn’t finish developing until 25” spiel has fucking ruined society I swear. It’s such a gross misunderstanding of the original study it’s laughable, and yet people use it as scientific evidence that infantilising young adults (usually women or people perceived to be women lbr) is ethical actually.
YOUR BRAIN IS CONSTANTLY CHANGING AND DEVELOPING YOUR ENTIRE LIFE. YOU DON’T SUDDENLY WAKE UP ON YOUR 25TH BIRTHDAY WITH ALL THE MATURITY AND KNOWLEDGE YOU NEVER PREVIOUSLY POSSESSED. STOP SPREADING THIS NONSENSE
#Inspired by the Cass report and the fact it’s also spreading this bs and using it to deny trans healthcare#pseudoscience#neuroscience#infantilization#brain development#cass review#cass report#transphobia#trans rights#rant#vent#psychology#psychiatry
389 notes
·
View notes
Text
By: Andy L.
Published: Apr 14, 2024
It has now been just little under a week since the publication of the long anticipated NHS independent review of gender identity services for children and young people, the Cass Review.
The review recommends sweeping changes to child services in the NHS, not least the abandonment of what is known as the “affirmation model” and the associated use of puberty blockers and, later, cross-sex hormones. The evidence base could not support the use of such drastic treatments, and this approach was failing to address the complexities of health problems in such children.
Many trans advocacy groups appear to be cautiously welcoming these recommendations. However, there are many who are not and have quickly tried to condemn the review. Within almost hours, “press releases“, tweets and commentaries tried to rubbish the report and included statements that were simply not true. An angry letter from many “academics”, including Andrew Wakefield, has been published. These myths have been subsequently spreading like wildfire.
Here I wish to tackle some of those myths and misrepresentations.
-
Myth 1: 98% of all studies in this area were ignored
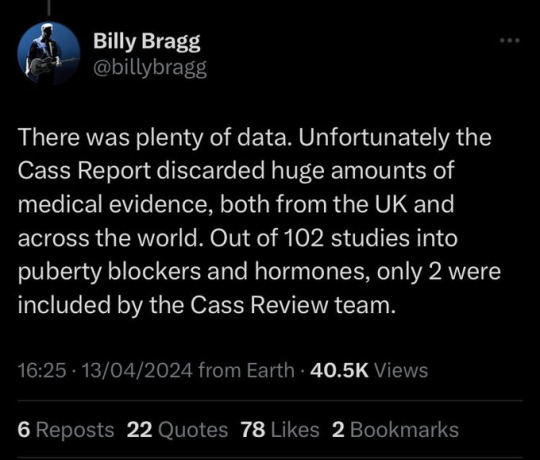
Fact
A comprehensive search was performed for all studies addressing the clinical questions under investigation, and over 100 were discovered. All these studies were evaluated for their quality and risk of bias. Only 2% of the studies met the criteria for the highest quality rating, but all high and medium quality (50%+) studies were further analysed to synthesise overall conclusions.
Explanation
The Cass Review aimed to base its recommendations on the comprehensive body of evidence available. While individual studies may demonstrate positive outcomes for the use of puberty blockers and cross-sex hormones in children, the quality of these studies may vary. Therefore, the review sought to assess not only the findings of each study but also the reliability of those findings.
Studies exhibit variability in quality. Quality impacts the reliability of any conclusions that can be drawn. Some may have small sample sizes, while others may involve cohorts that differ from the target patient population. For instance, if a study primarily involves men in their 30s, their experiences may differ significantly from those of teenage girls, who constitute the a primary patient group of interest. Numerous factors can contribute to poor study quality.
Bias is also a big factor. Many people view claims of a biased study as meaning the researchers had ideological or predetermined goals and so might misrepresent their work. That may be true. But that is not what bias means when we evaluate medical trials.
In this case we are interested in statistical bias. This is where the numbers can mislead us in some way. For example, if your study started with lots of patients but many dropped out then statistical bias may creep in as your drop-outs might be the ones with the worst experiences. Your study patients are not on average like all the possible patients.
If then we want to look at a lot papers to find out if a treatment works, we want to be sure that we pay much more attention to those papers that look like they may have less risk of bias or quality issues. The poor quality papers may have positive results that are due to poor study design or execution and not because the treatment works.
The Cass Review team commissioned researchers at York University to search for all relevant papers on childhood use of puberty blockers and cross-sex hormones for treating “gender dysphoria”. The researchers then graded each paper by established methods to determine quality, and then disregarded all low quality papers to help ensure they did not mislead.
The Review states,
The systematic review on interventions to suppress puberty (Taylor et al: Puberty suppression) provides an update to the NICE review (2020a). It identified 50 studies looking at different aspects of gender-related, psychosocial, physiological and cognitive outcomes of puberty suppression. Quality was assessed on a standardised scale. There was one high quality study, 25 moderate quality studies and 24 low quality studies. The low quality studies were excluded from the synthesis of results.
As can be seen, the conclusions that were based on the synthesis of studies only rejected 24 out of 50 studies – less than half. The myth has arisen that the synthesis only included the one high quality study. That is simply untrue.
There were two such literature reviews: the other was for cross-sex hormones. This study found 19 out of 53 studies were low quality and so were not used in synthesis. Only one study was classed as high quality – the rest medium quality and so were used in the analysis.
12 cohort, 9 cross-sectional and 32 pre–post studies were included (n=53). One cohort study was high-quality. Other studies were moderate (n=33) and low-quality (n=19). Synthesis of high and moderate-quality studies showed consistent evidence demonstrating induction of puberty, although with varying feminising/masculinising effects. There was limited evidence regarding gender dysphoria, body satisfaction, psychosocial and cognitive outcomes, and fertility.
Again, it is myth that 98% of studies were discarded. The truth is that over a hundred studies were read and appraised. About half of them were graded to be of too poor quality to reliably include in a synthesis of all the evidence. if you include low quality evidence, your over-all conclusions can be at risk from results that are very unreliable. As they say – GIGO – Garbage In Garbage Out.
Nonetheless, despite analysing the higher quality studies, there was no clear evidence that emerged that puberty blockers and cross-sex hormones were safe and effective. The BMJ editorial summed this up perfectly,
One emerging criticism of the Cass review is that it set the methodological bar too high for research to be included in its analysis and discarded too many studies on the basis of quality. In fact, the reality is different: studies in gender medicine fall woefully short in terms of methodological rigour; the methodological bar for gender medicine studies was set too low, generating research findings that are therefore hard to interpret. The methodological quality of research matters because a drug efficacy study in humans with an inappropriate or no control group is a potential breach of research ethics. Offering treatments without an adequate understanding of benefits and harms is unethical. All of this matters even more when the treatments are not trivial; puberty blockers and hormone therapies are major, life altering interventions. Yet this inconclusive and unacceptable evidence base was used to inform influential clinical guidelines, such as those of the World Professional Association for Transgender Health (WPATH), which themselves were cascaded into the development of subsequent guidelines internationally.
-
Myth 2: Cass recommended no Trans Healthcare for Under 25s
Fact
The Cass Review does not contain any recommendation or suggestion advocating for the withholding of transgender healthcare until the age of 25, nor does it propose a prohibition on individuals transitioning.
Explanation
This myth appears to be a misreading of one of the recommendations.
The Cass Review expressed concerns regarding the necessity for children to transition to adult service provision at the age of 18, a critical phase in their development and potential treatment. Children were deemed particularly vulnerable during this period, facing potential discontinuity of care as they transitioned to other clinics and care providers. Furthermore, the transition made follow-up of patients more challenging.
Cass then says,
Taking account of all the above issues, a follow-through service continuing up to age 25 would remove the need for transition at this vulnerable time and benefit both this younger population and the adult population. This will have the added benefit in the longer-term of also increasing the capacity of adult provision across the country as more gender services are established.
Cass want to set up continuity of service provision by ensure they remain within the same clinical setting and with the same care providers until they are 25. This says nothing about withdrawing any form of treatment that may be appropriate in the adult care pathway. Cass is explicit in saying her report is making no recommendations as to what that care should look like for over 18s.
It looks the myth has arisen from a bizarre misreading of the phrase “remove the need for transition”. Activists appear to think this means that there should be no “gender transition” whereas it is obvious this is referring to “care transition”.
-
Myth 3: Cass is demanding only Double Blind Randomised Controlled Trials be used as evidence in “Trans Healthcare”
Fact
While it is acknowledged that conducting double-blind randomized controlled trials (DBRCT) for puberty blockers in children would present significant ethical and practical challenges, the Cass Review does not advocate solely for the use of DBRCT trials in making treatment recommendations, nor does it mandate that future trials adhere strictly to such protocols. Rather, the review extensively discusses the necessity for appropriate trial designs that are both ethical and practical, emphasizing the importance of maintaining high methodological quality.
Explanation
Cass goes into great detail explaining the nature of clinical evidence and how that can vary in quality depending on the trial design and how it is implemented and analysed. She sets out why Double Blind Randomised Controlled Trials are the ‘gold standard’ as they minimise the risks of confounding factors misleading you and helping to understand cause and effect, for example. (See Explanatory Box 1 in the Report).
Doctors rely on evidence to guide treatment decisions, which can be discussed with patients to facilitate informed choices considering the known benefits and risks of proposed treatments.
Evidence can range from a doctor’s personal experience to more formal sources. For instance, a doctor may draw on their own extensive experience treating patients, known as ‘Expert Opinion.’ While valuable, this method isn’t foolproof, as historical inaccuracies in medical beliefs have shown.
Consulting other doctors’ experiences, especially if documented in published case reports, can offer additional insight. However, these reports have limitations, such as their inability to establish causality between treatment and outcome. For example, if a patient with a bad back improves after swimming, it’s uncertain whether swimming directly caused the improvement or if the back would have healed naturally.
Further up the hierarchy of clinical evidence are papers that examine cohorts of patients, typically involving multiple case studies with statistical analysis. While offering better evidence, they still have potential biases and limitations.
This illustrates the ‘pyramid of clinical evidence,’ which categorises different types of evidence based on their quality and reliability in informing treatment decisions

The above diagram is published in the Cass Review as part of Explanatory Box 1.
We can see from the report and papers that Cass did not insist that only randomised controlled trials were used to assess the evidence. The York team that conducted the analyses chose a method to asses the quality of studies called the Newcastle Ottawa Scale. This is a method best suited for non RCT trials. Cass has selected an assessment method best suited for the nature of the available evidence rather than taken a dogmatic approach on the need for DBRCTs. The results of this method were discussed about countering Myth 1.
Explainer on the Newcastle Ottawa Scale
The Newcastle-Ottawa Scale (NOS) is a tool designed to assess the quality of non-randomized studies, particularly observational studies such as cohort and case-control studies. It provides a structured method for evaluating the risk of bias in these types of studies and has become widely used in systematic reviews and meta-analyses.
The NOS consists of a set of criteria grouped into three main categories: selection of study groups, comparability of groups, and ascertainment of either the exposure or outcome of interest. Each category contains several items, and each item is scored based on predefined criteria. The total score indicates the overall quality of the study, with higher scores indicating lower risk of bias.
This scale is best applied when conducting systematic reviews or meta-analyses that include non-randomized studies. By using the NOS, researchers can objectively assess the quality of each study included in their review, allowing them to weigh the evidence appropriately and draw more reliable conclusions.
One of the strengths of the NOS is its flexibility and simplicity. It provides a standardized framework for evaluating study quality, yet it can be adapted to different study designs and research questions. Additionally, the NOS emphasizes key methodological aspects that are crucial for reducing bias in observational studies, such as appropriate selection of study participants and controlling for confounding factors.
Another advantage of the NOS is its widespread use and acceptance in the research community. Many systematic reviews and meta-analyses rely on the NOS to assess the quality of included studies, making it easier for researchers to compare and interpret findings across different studies.
As for future studies, Cass makes no demand only DBRCTs are conducted. What is highlighted is at the very least that service providers build a research capacity to fill in the evidence gaps.
The national infrastructure should be put in place to manage data collection and audit and this should be used to drive continuous quality improvement and research in an active learning environment.
-
Myth 4: There were less than 10 detransitioners out of 3499 patients in the Cass study.

Fact
Cass was unable to determine the detransition rate. Although the GIDS audit study recorded fewer than 10 detransitioners, clinics declined to provide information to the review that would have enabled linking a child’s treatment to their adult outcome. The low recorded rates must be due in part to insufficient data availability.
Explanation
Cass says, “The percentage of people treated with hormones who subsequently detransition remains unknown due to the lack of long-term follow-up studies, although there is suggestion that numbers are increasing.”
The reported number are going to be low for a number of reasons, as Cass describes:
Estimates of the percentage of individuals who embark on a medical pathway and subsequently have regrets or detransition are hard to determine from GDC clinic data alone.
There are several reasons for this:
Damningly, Cass describes the attempt by the review to establish “data linkage’ between records at the childhood gender clinics and adult services to look at longer term detransition and the clinics refused to cooperate with the Independent Review. The report notes the “…attempts to improve the evidence base have been thwarted by a lack of cooperation from the adult gender services”.
We know from other analyses of the data on detransitioning that the quality of data is exceptionally poor and the actual rates of detransition and regret are unknown. This is especially worrying when older data, such as reported in WPATH 7, suggest natural rates of decrease in dysphoria without treatment are very high.
Gender dysphoria during childhood does not inevitably continue into adulthood. Rather, in follow-up studies of prepubertal children (mainly boys) who were referred to clinics for assessment of gender dysphoria, the dysphoria persisted into adulthood for only 6–23% of children.
This suggests that active affirmative treatment may be locking in a trans identity into the majority of children who would otherwise desist with trans ideation and live unmedicated lives.
I shall add more myths as they become spread.
==
It's not so much "myths and misconceptions" as deliberate misinformation. Genderists are scrambling to prop up their faith-based beliefs the same way homeopaths do. Both are fraudulent.
#Andy L.#Cass Review#Cass Report#Dr. Hilary Cass#Hilary Cass#misinformation#myths#misconceptions#detrans#detransition#gender affirming healthcare#gender affirming care#gender affirmation#affirmation model#medical corruption#medical malpractice#medical scandal#systematic review#religion is a mental illness
338 notes
·
View notes
Text
I'm really panicked about the Cass Report sitch in the UK right now. I just have this horrible, sickened feeling. the articles proclaiming about the 'puberty blocker scandal' as if the report said that puberty blockers had been proven harmful, and not just that the report reoghtfully claimed that there hadn't been enough research.... which is basically the exact same situation as such medications as SSRIs, birth control in the NHS and yet those situations won't be used to bolster and reaffirm a hateful congregation of idiotic transphobes with too much power into dragging trans rights and healthcare in the UK through subsequent decades of incredibly harmful stagnation, fearmongering, and outright harm.
the Cass Report seems to me only to confirm what we know about almost every other sector of the NHS: that it's broken, underfunded, bogged down in failing beurocracy and not interested in preventative care as its mainline strategy. that's a position where the blame should be laid at the feet of the Conservative party, not at the feet of people who believe trans people should have adequate care which as at least a first line BELIEVES THEM
calling this a 'watershed' moment as if giving trans individuals gender affirming care is evil, while everyday within the NHS racism, medical misogyny, regional disparities between the North (edited add wales also) and Souths standards of healthcare which cause life expectancy to be lower, a mental health sector which is so utterly broken it can't actually help anyone. ..... etc etc etc are happening. its transphobia. its just hateful transphobia. transphobia which is now seen to be validated by idiots
I feel so sick and scared
345 notes
·
View notes
Text
Why on earth is anyone taking this shoddy cass review seriously?
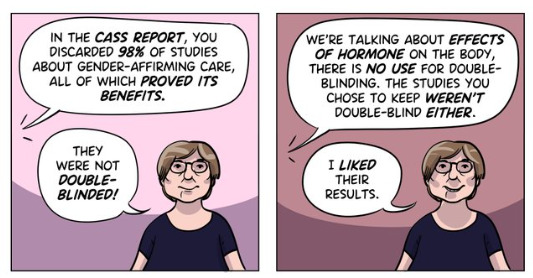
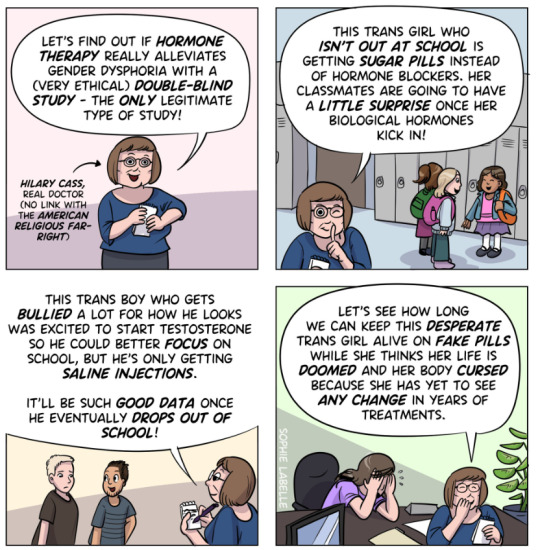
I'm sorry but it's baffling how an actual government is uncritically taking this review at face value. It literally only comes to the conclusion it does because it ignore literally all other evidence. They excluded a shit ton of studies because they didn't have enough controls, which sounds reasonable but in order to have those controls they'd have to unknowingly give patients placebos instead of the hormonal therapy and puberty blockers they asked for.
That would be an extremely unethical thing to do, and would achieve nothing because the effects of hormonal therapy and puberty blockers are extremely obvious.
Just let that sit with you for a moment. All that clinical evidence completely thrown out the window because they didn't do a horrific and unethical test on their patients. All that clinical evidence ignored because the study was ethical. This is an extreme oversight at BEST and deliberate misinformation at worst. Either way, it makes the review extremely unreliable.
That's just one issue. But the fact that the vast, VAST majority of research was completely ignored due to a ridiculous and unethical requirement should be enough for you to oppose anyone using this as evidence for anything other than why queer people need to be included in scientific discussions about our communities. Because this review is being used to roll back LGBT rights.
#cass review#cass report#queer#queerphobia#transphobia#trans#transgender#nhs england#trans rights#lgbt rights#transgender rights#lgbtq#lgbt#lgbtqia#lgbtq community#queer community#pseudoscience#bad science#feminism#feminist#intersectional feminism#uk#britain#england
173 notes
·
View notes
Text
The methodology for the Cass review was established by a team from the University of York including Tilly Langdon, who has previously been involved in promoting Gender Exploratory Therapy – an approach which, despite its neutral-sounding name, discourages children from identifying as trans and has been likened to conversion therapy. Her approach included setting a very high bar for evidence to be considered in the review, ruling out 100 of the existing 103 studies into the use of puberty blockers and hormones to treat trans children.
The reason given for excluding all these studies was that they did not incorporate a double blind approach – in other words, they did not involve giving puberty blockers to some patients and placebos to others. This might sound like a reasonable objection on the face of it – until one considers that puberty is a dramatic physical and psychological process, and people can easily tell when it’s happening to them, so a double blind simply wouldn’t work in practice.
The Cass review called for more research and, again, few would disagree with this. The suggestion that treatment should be withheld in the process, however, is not neutral. It presupposes that the harm done by puberty blockers (demineralisation of bones, which is usually temporary in the short-term treatment recommended and is similar to what occurs in pregnancy) is more severe than the harm done to a trans child by going through the wrong sort of puberty. The latter is linked to high rates of self-harm and suicidal ideation, together with the need, in many cases, for extensive surgical procedures.
Confusingly, the review states that children taking puberty blockers showed “no changes in gender dysphoria or body satisfaction”, which suggests that the author didn’t actually understand what puberty blockers do at all. They don’t make children feel better – they just delay a process that makes them feel worse.
This is one of several oddities in a report that lacks internal consistency. It states that there is no established definition of social transition, for instance, and does not offer one, but goes on to talk about it as if there were. It also talks about autistic ‘girls’ identifying as trans in increasing numbers, treating this as mysterious and as cause for concern, despite acknowledging elsewhere that more and more girls are being diagnosed as autistic, so one would expect more diagnoses to be present within any subsection of the young female-assigned population.
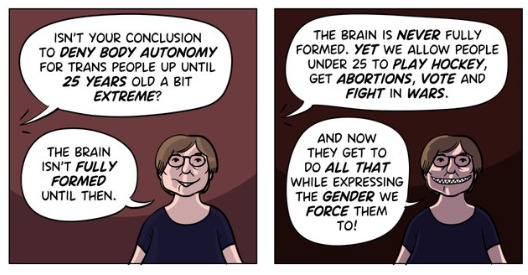
Perhaps the most worrying of the review’s conclusions – which should concern people far beyond the trans community – is the suggestion that as far as NHS treatment is concerned, trans people should be treated as children until they are 25. The rational for this is that 25 is the age when (on average) the brain stops developing. As any neurologist will tell you, the brain is in fact never static, and within ten years or so of that age, it begins to shrink. Deciding who has the capacity to make decisions based on brain age could have unintended consequences for the likes of Cass (64).
That aside, what would setting the age of true adulthood at 25 mean for everybody else? If we couldn’t allow people to consent to medical treatment at 24, should we ask them to risk dying for us? If not, then at a stroke we could lose a quarter of our armed forces. Likewise, we would have to give serious thought to what to do about a third of parents who might not be considered competent to look after their newborn children.
And then there are issues like contraception. Right-wingers have long contended, on one pretext or another, that teenage girls shouldn’t have the right to take the pill without their parents’ consent. This is where the review’s suggestion starts to look less like a double standard and more like the thin end of a very nasty wedge.
283 notes
·
View notes
Text
Fuck the Cass report
Fuck the Tories
Fuck Labour
Fuck TERFs
242 notes
·
View notes
Text
i am so sorry for the trans folk living in the uk. no matter if you’re fully transitioned, an adult, a minor, this has affected you and i am so so sorry. i know how scary it is right now and this shit has not made it any better.
trans people all around the world see you and hear you. in fact, even non-trans people, allies, professionals, people out of the community, all see you and know how wrong this is.
The world is not all against you. Please believe that there is hope. Because there is. Please keep yourself safe and please take care of yourself to the best of your abilities. You breathing is proof that you deserve to be here. You deserve to be here. You truly do.
Please. Be as okay as you can be right now.
#this post is meant to be a reminder to stay as safe as people can#I don’t know who this will reach. or if it will do anything at all#but i hope it reaches someone:)#I also tried to use the least triggering language possible but if it comes off as anything please tell me /srs#transphobia#tw transphobia#cass review#cass report#trans#trans rights#<- I don’t want to flood with negativity. but I’ve seen stuff being tagged like this so I will
211 notes
·
View notes
Text
The Be Kind Brigade strikes again.
97 notes
·
View notes
Text
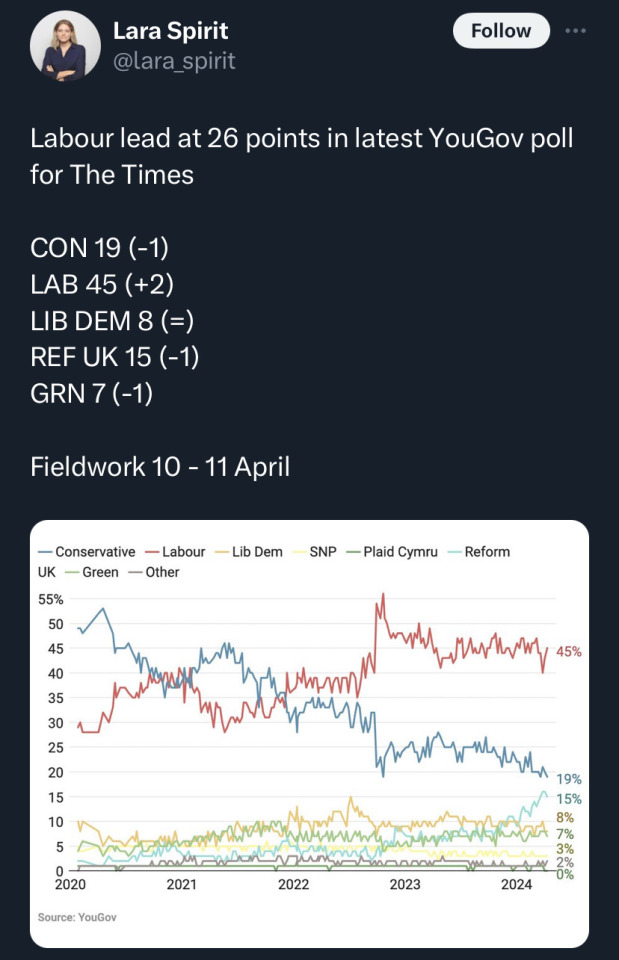
Labour are on track to win a landslide victory,
you can vote green and know you aren’t enabling a Tory back door victory, I myself am planning to vote snp as a voter in Scotland
the tories will have been in power for 14 years next month their time in power is done everyone in Westminster knows it’s why the tories are in burn mode,
it’s going to be a starmer coronation so it’s important that it’s tempered by a left wing since he’s forced all the Labour left out
#tories out#british politics#conservative party#tory party#uk politics#politics#vote#keir starmer#labour party#green party#cass report#election watch 2024
91 notes
·
View notes
Last Seen Blogs

maggieparson
uh huh honey.

karniss-bg3
Kar'niss: The Broken Beauty

askinsanewheatley
I am not a moron. You'll see.

torsamors
We Only Part To Meet Again

poisonangelmuse
This is my kingdom come