#WPATH
Text
J.K. Rowling has been proven right!
"The Cass Review is a damning indictment of what the NHS has been doing to children.
"Dr Hilary Cass has submitted her final report and recommendations to NHS England in her role as Chair of the Independent Review of gender identity services for children and young people.
"Hilary Cass’s report demolishes the entire basis for the current model of treating gender-distressed children. Its publication is a shameful day for NHS England, which for too long gave vulnerable children harmful treatments for which there was no evidence base. It’s now clear to all that this was quack medicine from the start.
"Dr Cass delivers stinging criticisms of NHS gender clinics, both adult and child, and her description of the Gender Identity Development Service is absolutely damning. It is disgraceful that GIDS, alongside the adult clinics, did not cooperate with her attempt to survey its practice, or to carry out a high-quality, long-term follow-up study on the treatment of children as part of the review, which would have been a global first."

You can read the entire review here. (pdf)

"Glinner" is Graham Linehan, a writer, screenwriter, and comedian who's been fighting against transitioning minors for years, losing friends, his job, and his agent along the way. But he's kept on fighting.

,
;

.

.

The tide has turned in the UK and in Europe. When will American media finally begin reporting on the closing of "gender clinics" and the bans on puberty blockers for children? I figure nothing will happen here in the U.S. until the lawsuits start flooding in. It's already begun. And with proof like the Cass Review and the WPATH files, it's going to be very, very difficult for clinics, doctors, and therapists to continue lying about how transitioning does no permanent and irreversible physical and psychological harm.
#Cass Review#transing kids#JK Rowling#I stand with JK Rowling#Graham Linehan#trans lies#WPATH#WPATH files#gender critical#gender clinics#health#medicine#the tide has turned#David Tennant
464 notes
·
View notes
Text
Fact Check: Fact Check: 216 Instances Of Factual Errors Found In Right-Wing "WPATH Files" Document

In response to the WPATH files being dropped, transgender activist Erin Reed made a response, fact checking the claims made in the editorial of the original document, written by Mia Hughes. Reed claims that there are 216 “instances of factual inaccuracies, erroneous citations, misinterpretations of what is “leaked,” and purposeful omissions contradicting the authors central editorialized claims.”
The introduction is spent discrediting the organizations involved as “right wing” and “anti trans.” Reed alleges that the quick rate at which the files were spread was a “coordinated and organized embargo campaign, leaving those in support of care with scant time to review the voluminous documents and respond.”
The first claim that Reed alleges to be false is the claim that the Beyond WPATH declaration was signed by many people who were not doctors, pointing out signatures with occupations such as “DJ” and “yoga instructor” as well as comments like “concerned parent.” The original document does not claim that all signatures were from doctors, with the exact quote stating that it was “now signed by over 2,000 concerned individuals, many of whom are clinicians working with gender diverse young people.” (bold text mine). Nowhere does it imply that only doctors were able to sign it, it simply acknowledges that many people who signed the petition were doctors. One important thing to note is that the creator of the petition, Dr. Joseph Burgo, alleges that the petition was hijacked by trans activists adding fake signatures. (timestamp: 16 min)
Here is a screenshot of the top signers of the petition. Highlighted are all medical professionals.

Note that one of the signers, Stephen B. Levine, was a former president of WPATH who left due to the organization becoming less evidence based and more focused on activists.
Next, Reed criticizes the quality of the citations, stating, "When addressing supposedly "scientific" citations, the report's performance is equally lacking." One example given is an article from The Guardian from 2004, and another being “a conservative site called "The New Atlantis, " Upon visiting the link to the New Atlantis’s “about” page, they explicitly state they are a nonpartisan organization. That being said, other sources do allege this particular publication is right wing. However, this attempt to frame any opposing source as "right wing" or "conservative" is a significant part of Reed's argument on why the information is unreliable.
Reed accuses many of the studies cited to be misrepresented. One study cited in the WPATH files is a Swedish study which is quoted as finding, “rates of completed suicide post-surgical transition to be greatly elevated over the general population.”
Reed links to an article from a site called Trans Advocate, which contains an interview with the author of the Swedish study on how her work has been misinterpreted. In this article, the study is quoted as saying, “no inferences can be drawn as to the effectiveness of sex reassignment as a treatment for transsexualism. In other words, the results should not be interpreted such as sex reassignment per se increases morbidity and mortality.” The study does not conclude that sex reassignment surgery works, but there is also no reason to suggest it causes people to be more suicidal than they were pre-transition. Hughes does imply that suicide risk can increase after transition in cases where certain mental health conditions such as BPD are left untreated, and the patient comes to regret transition later, but this is not cited as scientific fact (42).
On the page before the Swedish study is referenced (42), Hughes discusses the mental health issues commonly found in trans-identified youth and how those issues may account for the higher rate of suicidality. Reed fails to acknowledge the Amsterdam study that concluded “the suicide risk in transgender people is higher than in the general population and seems to occur at every stage of transitioning.” While some parts of the Swedish study may have been misinterpreted, there are other studies with similar findings. The point is not that suicidality increases after transition, but rather that there is little evidence to suggest that transition has a long-term benefit on a person's other mental health issues.
Reed links to three studies disputing both the 2009 study and the Swedish study, implying that all of this “much newer research from peer-reviewed articles,” completely invalidates the findings of the other studies. The first study that Reed gives as a rebuttal does not actually come to the conclusion that there is a “substantial improvement in the quality of life for transgender individuals.” This 2017 study concludes that, “Our results show that transgender women generally have a lower QoL compared to the general population. GRS leads to an improvement in general well-being as a trend but over the long-term, QoL decreases slightly in line with that of the comparison group.” Basically, it claims that quality of life increases shortly after surgery, but later declines after about 5 years. They acknowledge that this is the case in the general population as well, and they state that there is still little consensus on trans identified people’s quality of life.
The second study Reed cites looks at the quality of life of patients who have received phalloplasties. Only 32 patients were part of this study, and they found that “88% of our patients were very satisfied with the aesthetic result, 75% have had sex after surgery, and 72% were very satisfied with sexual function after GAS. Eighty-one percent had a strong improvement of QOL, and 91% would undergo the same treatment again.” However, there is more evidence that phalloplasty is a dangerous procedure, and Reed fails to acknowledge any of those studies, such as this study of 1731 phalloplasty patients, finding that the "Overall complication rate was high at 76.5%"
The third study was a survey of 27,715 trans identified adults from 2015. The introduction of the study admits that “Mental health effects of gender-affirming surgery thus remain controversial.” In this survey, only 25% of participants had undergone surgery. This study was only a secondary analysis of these survey responses, comparing results of those who did not undergo surgery with those who had.
Reed implies that the 2% fatality rate of the vaginoplasty performed on males who had previously been on puberty blockers is irrelevant because the death “occurred from a wound infection, a potential complication for any surgery.” Hughes acknowledges that the patient died of necrotizing fasciitis, (19) and the case report that Reed links states that the patient, “developed septic shock and multiple organ failure on the basis of an extended-spectrum β-lactamase-producing Escherichia coli. A severe progression of the necrotizing fasciitis was lethal, despite repeated surgical debridement, intravenous antibiotic use, and supportive care at the intensive care unit.” The study that Reed then links to prove this treatment is successful contains extremely graphic images detailing the surgery without any warning. This does not discredit the study, but for that reason I cannot really look at it.
Reed attempts to debunk the accusation that those who took puberty blockers cannot orgasm, by alluding to there being two studies disproving this. However, it appears that Reed linked the same study twice within this quote, "To ensure factual accuracy, studies have shown that those who took puberty blockers are capable of orgasm" Only the abstract is available to me for this study. Because this study is behind a paywall, it is difficult for me to verify Reed’s claims about their results. The study is a survey of group of 31 primary total laparoscopic intestinal vaginoplasty patients, and is a survey about general quality of life one year after the surgery. It states that the group was “relatively young,” and states that the, “median age at time of surgery = 19.1 years, range = 18.3–45.0.” However, it gives no indication of when the patients began transition. It does imply that patients were on "Puberty-suppressing hormonal treatment”, but does not make any mention of when the patients started puberty blockers. Marci Bowers, head of WPATH, has explicitly stated that “I’m unaware of an individual claiming ability to orgasm when they were blocked at Tanner Stage 2.” Tanner Stage 2 is around the age of 11. It is possible these patients began blockers later on, but that evidence is not available to me either way. Another important thing to note is that the conclusion of the second study states, “This group of relatively young transgender women reported satisfactory functional and esthetic results of the neovagina and a good quality of life, despite low Female Sexual Function Index scores.” (bold text mine) “The mean Female Sexual Function Index total score of sexually active transgender women was 26.0 ± 6.8.”
This study is a survey relying on patients to self report their satisfaction, and Hughes does acknowledge the flaws of self reported studies on page 33, stating that measurable studies showed less positive results than surveys. Many of the studies Reed cites as rebuttals rely on self report.
Finally, Reed criticizes the idea that gender dysphoric youth would eventually desist post-puberty. One of the links provided as evidence against this claim leads to another article of Reed's. The criticism of Kenneth Zucker's research from the 90s appears to be that it classifies children with "gender identity disorder" as those who are simply gender non-conforming. The article uses this graphic to illustrate the difference between gender identity disorder and the current DSM-5 diagnosis of gender dysphoria, implying that the latter has stricter requirements.

Reed dismisses any correlation between social transition and desistance rates and accuses Hughes of implying that, “social transition prevents this “natural” desistance, a hypothesis that has not been validated.” While there may have been some flaws in Zunker's original study, this massive difference between then and now certainly raises questions on how the impact of social transition affects a child.
In the next section, Reed claims that the “leaked material” is frequently misrepresented, yet only provides three examples of this occurring. It does appear that Hughes left out the part about the orgasm in the first example, which would have been important context to include (28). In the second example, Reed accuses Hughes of leaving out the fact that it was a detransitioner who used the phrase “gender journey” and not a clinician. In reality, Hughes does not specify who said this, simply stating “There is talk about detransition being just another step in a patient’s “gender journey.” (31) However, we only have the clinicians word to go off to prove that the patient used that phrase, and there is evidence of another clinician pushing patients to identify with their language. This doctor decided to label a patient as “eunuch identified,” despite him not claiming that label himself (51). The third example of a misrepresentation consists of a patient developing a hepatic adenoma (liver mass) after taking testosterone. Reed is correct that hepatic adenomas are benign and that they are linked to both contraceptives and hormones. However, Reed accuses the document of leaving out the fact that the patient was on both oral contraceptives and testosterone. Hughes does in fact state that the patient was on norethindrone acetate, which is a contraceptive. In the WPATH document, the doctor specifically suspects that the hormones are the cause of the liver masses as opposed to the contraceptive.
Reed alleges that Stella O’Malley and Genspect “teased a young trans girl testifying in front of a school board.” The linked tweet reads: “US-UTAH: 11 yr old “Alison” came out as trans at 8 after having a vision of wearing a long white dress in a field. Dad says his “daughter” must be “validated in who she is” & allowed to use girls spaces bc many trans-identified people consider suicide.”
Overall, Reed’s fact checking only provides a few examples, nowhere near the 216 claimed. Many of the studies linked as rebuttals do not come to the same conclusions as Reed implies. In my opinion, it appears that Reed did not expect the audience of this article to go and read the WPATH files for themselves, or for that matter, even check the links thoroughly. The few good points that are made here do not discredit the entirety of the report, and Reed fails to address the main claims in the report; such as WPATH members admitting that children do not have the capacity to consent, their disregard of proper scientific protocol, the experimental approach to healthcare, disregard of patients' other mental health issues, and lack of ethics.
If anyone wants to add things to this or expand on anything, please feel free to do so. There were a couple sections where my understanding was a bit limited, such as the limitations of the trans youth desistance study, and the puberty blockers/vaginoplasty study.
Edit: Moving this disclaimer down here because a TRA quit reading immediately after they saw this. I would like to acknowledge that I am not a doctor or any type of medical professional (neither is Reed) and some scientific studies may be difficult for me to interpret.
Edit 2: Removed the part about the New Atlantis because I have seen mixed info on it's political leanings.
#wpath#wpath files#transgender#trans#gender critical#erin reed#terfblr#radfem#radical feminism#radical feminists do interact#trans activism
68 notes
·
View notes
Text

By: Gerald Posner
Published: Mar 4, 2024
Newly leaked files from the world’s leading transgender health-care organization reveal it is pushing hormonal and surgical transitions for minors, including stomach-wrenching experimental procedures designed to create sexless bodies that resemble department-store mannequins.
The World Professional Association for Transgender Health documents demonstrate it’s controlled by gender ideologues who push aside concerns about whether children and adolescents can consent to medical treatments that WPATH members privately acknowledge often have devastating and permanent side effects.
Yet the US government, American doctors and prominent organizations nonetheless rely on WPATH guidelines for advice on treating our youth.
The files — jaw-dropping conversations from a WPATH internal messaging board and a video of an Identity Evolution Workshop panel — were provided to journalist Michael Shellenberger, who shared the documents with me.
Shellenberger’s nonprofit Environmental Progress will release a scathing summary report, comparing the WPATH promotion of “the pseudoscientific surgical destruction of healthy genitals in vulnerable people” to the mid-20th-century use of lobotomies, “the pseudoscientific surgical destruction of healthy brains.”
‘Arbitrary’ age limits
The comparison to one of history’s greatest medical scandals is not hyperbole.
It is particularly true, as the files show repeatedly, when it involves WPATH’s radical approach to minors.
When the organization adopted in 2022 its current Standards of Care — relied on by the National Institutes of Health, the World Health Organization and every major American medical and psychiatric association — it scrapped a draft chapter about ethics and removed minimum-age requirements for children starting puberty blockers or undergoing sexual-modification surgeries.
It had previously recommended 16 to start hormones and 17 for surgery.
Not surprisingly, age comes up frequently in the WPATH files, from concerns about whether a developmentally delayed 13-year-old can start on puberty blockers to whether the growth of a 10-year-old girl will be stunted by hormones.
During one conversation, a member asked for advice about a 14-year-old patient, a boy who identified as a girl and had begun transitioning at 4.
The child insisted on a vaginoplasty, a surgery that removes the penis, testicles and scrotum and repositions tissue to create a nonfunctioning pseudo-vagina. It requires a lifetime of dilation. Was he too young at 14?
Marci Bowers, WPATH’s president and a California-based pelvic and gynecologic surgeon who is herself transgender, said she considered any age limit “arbitrary.”
But she would not do it. Why?
“The tissue is too immature, dilation routine too critical.”
In lay terms, that means boys who are too young do not have enough penal tissue for the surgery and the surgeon must harvest intestinal lining to build the faux vagina. Even Bowers admits that can lead to “problematic surgical outcomes.”
She would know since she has performed more than 2,000 vaginoplasties. Her highest-profile patient is 17-year-old Jazz Jennings, the transgender star of reality TV show “I Am Jazz.”
Three corrective surgeries were required to fix problems from the original vaginoplasty.
“She had a very difficult surgical course,” Bowers admitted in a 2022 appearance on the show. “We knew it would be tough — it turned out tougher than any of us imagined.”
Still, Bowers told her colleagues in the internal discussion forum of the best age for an adolescent to undergo surgery: “sometime before the end of high school does make some sense in that they are under the watch of parents in the home they grew up in.”
Christine McGinn, a Pennsylvania plastic surgeon and herself transgender, agreed. McGinn has performed “about 20 vaginoplasties in patients under 18” and thinks the “ideal time in the U.S. is surgery the summer before the last year of high school. I have heard many other surgeons echo this.”
Waiting until teens are older than 18 and in college is problematic, she said: “there are too many stressors in college that limit patients’ ability to dilate.”
Dangers downplayed
WPATH assures patients that surgical and hormonal interventions are tested and safe. It is a different matter in private.
President Bowers, for instance, said publicly in 2022 that puberty blockers are “completely reversible,” although in the internal forum she conceded it is “in its infancy.”
What about children who are infertile for life since they started hormone blockers before they reached puberty?
Bowers told her colleagues the “fertility question has no research.”
At other stages, members talk frankly about the complications for the transition surgery for girls, a phalloplasty in which a nonfunctioning pseudo-penis is fashioned from either forearm or thigh tissue.
It requires a full hysterectomy and surgical removal of the vagina. They also discuss other serious consequences, including pelvic inflammatory disease, vaginal atrophy, abnormal pap tests and incontinence.
A 16-year-old girl who had been on puberty blockers for several years before she was put on testosterone for a year had developed two liver tumors that an oncologist concluded the hormones had caused. Another member described “a young patient on testosterone for 3 years” who had developed “vaginal/pelvic pain/spotting . . . [and] atrophy with the persistent yellow discharge.”
Several colleagues described patients with similar conditions, some with debilitating bowel problems or bleeding and excruciating pain during sex (“feeling like broken glass”).
Vaginal estrogen creams and moisturizers as well as hyaluronic acid suppositories “can be helpful.”
One WPATH member seemed surprised: “The transgender people under my surveillance do not complain about this matter. However, I confess that I have never asked them about it.”
Rise of ‘de-gender’ surgery
The litany of transition surgery’s side effects did not stop WPATH from endorsing far more radical “nullification” surgeries for patients who do not feel either male or female and identify only as nonbinary.
Several dozen so-called “de-gendering” surgeries are designed to create a sexless, smooth cosmetic appearance that is unknown in nature. There is even an experimental “bi-genital” surgery that attempts to construct a second set of genitals.
In 2017, when tabloids reported a 22-year-old man had spent $50,000 to surgically remove his sex organs so he could “transform into a genderless extra-terrestrial,” it seemed a one-off oddity.
But WPATH has enshrined that concept in its Standard of Care — the same document in which the group endorsed for the time first time chemical or surgical castration for patients who identify as eunuchs. (WPATH even linked to the Eunuch Archives, where men anonymously share castration fetishes.)
These science-fiction-like surgeries are not only reserved for adults.
“How do we come up with appropriate standards for non-binary patients?” asked Thomas Satterwhite, a San Francisco-based plastic surgeon who has operated on dozens of patients younger than 18 since 2014. “I’ve found more and more patients recently requesting ‘non-standard’ procedures.”
What are nonstandard procedures? They include “non-binary top surgery,” a mastectomy without nipples. There are brutal procedures for girls that eliminate all or part of the vagina and for boys that amputate the penis, scrotum and testicles.
The goal, as one San Francisco surgical clinic proclaims on its website, “is a smooth, neutral body that is cosmetically free of sexual identification.” On TikTok the trend is called a “flat front.”
‘Too young to understand‘
A particularly intense subject of discussion was whether minors could understand the lifelong consequences of their gender treatments. Minors are presumed by law to be incapable of making an informed decision about having a vasectomy or tubal ligation.
Gender surgeries are an exception, however.
WPATH’s Standard of Care allows all procedures so long as the minor “demonstrates the emotional and cognitive maturity required to provide informed consent/assent for the treatment.”
In a May 2022 internal workshop, “Identity Evolution,” WPATH members conceded that was all but impossible.
Daniel Metzger, the British Columbia endocrinologist who cowrote the Canadian Pediatric Society’s position paper on health care for trans minors, said, “I think the thing you have to remember about kids is that we’re often explaining these sorts of things to people who haven’t even had biology in high school yet.”
Metzger noted adolescents are incapable of appreciating the lifelong consequence of infertility. “It’s always a good theory that you talk about fertility preservation with a 14-year-old,” he said, “but I know I’m talking to a blank wall. They’d be like, ‘ew, kids, babies, gross.’ Or, the usual answer is, ‘I’m just going to adopt.’ And then you ask them, ‘Well, what does that involve? Like, how much does it cost?’ ‘Oh, I thought you just like went to the orphanage, and they gave you a baby.’ . . . I think now that I follow a lot of kids into their mid-twenties, I’m always like, ‘Oh, the dog isn’t doing it for you, right?’”
There is extensive research showing adolescent brains are wired to have little control over rash behavior and are not capable of grasping the magnitude of decisions with lifelong consequences. It is why society doesn’t allow teens to get tattoos or buy guns. Car-rental agencies set 25 as the minimum age for renting a car, and Sweden sets the same limit for deciding on sterilization.
Detransitioners ignored, shunned
Although many WPATH members privately doubt that adolescents can give truly informed consent to life-altering procedures, they must affirm whatever children say about their gender.
Unless, the WPATH files disclose, the patient wants to reverse course and become a so-called detransitioner.
WPATH members mostly dismiss those cases as insignificant or overblown by the media and question whether minors who want to revert to their birth sex really understand what they are doing.
It’s a question that would never be asked for minors who declared themselves to be gender dysphoric.
One case involved a 17-year-old boy, just graduated from high school, who had been on testosterone for two years. He was reported to be “very distraught and angry. He reports he feels he was brainwashed and is upset by the permanent changes to his body.”
A self-described “queer therapist” did not believe any young person could be brainwashed. “In my experience, those stories come from people who have an active agenda against the rights of trans people.”
WPATH President Bowers said that “I do see talk of the phenomenon [detransitioners] as distracting from the many challenges we face.”
‘Frankenstein files’
The leaked files put a spotlight on the danger of mixing ideological activism with medicine and science. They should serve as an urgent wakeup call for the medical associations and government agencies that rely on WPATH guidance for transgender health.
The files might even prompt investigations into how those with distorted personal agendas seized control of the organization at the expense of science and patients.
Investigating what has gone wrong at WPATH might prove uncomfortable for some gender progressives in the Biden administration, none more so than Adm. Rachel Levine, the assistant secretary for health. Levine, the first transgender four-star military officer, is a WPATH member and has lavished praise on the organization.
She says it “assesses the full state of the science and provides substantive, rigorously analyzed, peer-reviewed recommendations to the medical community on how best to care for patients who are transgender or gender non-binary. It is free of any agenda other than to ensure that medical decisions are informed by science.”
Either Levine is unaware of the hormonal and surgical experimentation the group promotes or refuses to acknowledge it.
“The Frankenstein files.”
That is how a pediatrician described the leaked documents after I shared them with her.
Unfortunately, this is no horror novel.
It is a medical travesty playing out in real time, and the casualties are our children.
#Gerald Posner#Michael Shellenberger#WPATH#World Professional Association for Transgender Health#Mia Hughes#WPATH Files#The WPATH Files#medical corruption#medical malpractice#medical scandal#unethical#gender ideology#gender identity ideology#queer theory#first do no harm#religion is a mental illness
27 notes
·
View notes
Text
Erin Reed at Erin In The Morning:
On Tuesday, Gov. Janet Mills of Maine signed LD 227, a sanctuary bill that protects transgender and abortion providers and patients from out-of-state prosecution, into law. With this action, Maine becomes the 16th state to explicitly protect transgender and abortion care in state law from prosecution. This follows several bomb threats targeting state legislators after social media attacks from far-right anti-trans influencers such as Riley Gaines and Chaya Raichik of Libs of TikTok. An earlier version of the bill failed in committee after similar attacks in January. Undeterred, Democrats reconvened and added additional protections to the bill before it was passed into law.
The law is extensive. It asserts that gender-affirming care and reproductive health care are "legal rights" in Maine. It states that criminal and civil actions against providers and patients are not enforceable if the provision or access to that care occurred within Maine’s borders, asserting jurisdiction over those matters. It bars cooperation with out-of-state subpoenas and arrest warrants for gender-affirming care and abortion that happen within the state. It even protects doctors who provide gender-affirming care and abortion from certain adverse actions by medical boards, malpractice insurance, and other regulating entities, shielding those providers from attempts to economically harm them through out-of-state legislation designed to dissuade them from providing care.
The bill also explicitly enshrines the World Professional Association of Transgender Health’s Standards of Care, which have been the target of right-wing disinformation campaigns, into state law for the coverage of transgender healthcare.
The bill is said to be necessary due to attempts to prosecute doctors and seek information from patients across state lines. In recent months, attorneys general in other states have attempted to obtain health care data on transgender patients who traveled to obtain care. According to the United States Senate Finance Committee, attorneys general in Tennessee, Indiana, Missouri, and Texas attempted to obtain detailed medical records "to terrorize transgender teens in their states… opening the door to criminalizing women’s private reproductive health care choices."
The most blatant of these attempts was from the Attorney General of Texas, who, according to the Senate Finance Committee, "sent demands to at least two non-Texas entities."
[...]
Despite these threats, legislators strengthened both the abortion and gender-affirming care provisions and pressed forward, passing the bill into law. Provisions found in the new bill include protecting people who "aid and assist" gender-affirming care and abortion, protections against court orders from other states for care obtained in Maine, and even protections against adverse actions by health insurance and malpractice insurance providers, which have been recent targets of out-of-state legislation aimed at financially discouraging doctors from providing gender-affirming care and abortion care even in states where it is legal.
Maine Gov. Janet Mills (D) signs gender-affirming care and abortion sanctuary state bill LD227 into law despite the best efforts of right-wing anti-trans extremists such as Riley Gaines, Courage Is A Habit, and Libs of TikTok who sought to thwart its passage and signature into law.
#Maine LD227#Maine#Janet Mills#Transgender Safe Refuge#Transgender Sanctuary State#Abortion Sanctuary State#Abortion#Gender Affirming Healthcare#LGBTQ+#Transgender Health#Transgender#WPATH
27 notes
·
View notes
Text
Newly leaked files from within the leading global transgender healthcare body have revealed that the clinicians who shape how “gender medicine” is regulated and practiced around the world consistently violate medical ethics and informed consent. The files, which were leaked from within the World Professional Association for Transgender Health (WPATH), were published today by the US-based think tank Environmental Progress.
#gender critical#sex is not gender#gender stereotypes#gender is a social construct#gender ideology#transgender ideology#transgender#medical maltreatment#medical malpractice#wpath
11 notes
·
View notes
Text
The medical transitioning of children has become one of the most controversial and polarising issues of our time. For some, it is a medical scandal. For others, life-saving treatment.
So, when hundreds of messages were leaked from an internal forum of doctors and mental health workers from the World Professional Association for Transgender Health, it was bound to spark interest. WPATH describes itself as an “interdisciplinary professional and educational organisation devoted to transgender health”. Most significantly, it produces standards of care (SOC) which, it claims, articulate “professional consensus” about how best to help people with gender dysphoria.
Despite its grand title, WPATH is neither solely a professional body – a significant proportion of its membership are activists – nor does it represent the “world” view on how to care for this group of people. There is no global agreement on best practice. The leaked messages (and the odd recording) – dubbed the WPATH files – are disturbing. In one video, doctors acknowledge that patients are sometimes too young to fully understand the consequences of puberty blockers and hormones for their fertility. “It’s always a good theory that you talk about fertility preservation with a 14-year-old, but I know I’m talking to a blank wall,” one Canadian endocrinologist says.
WPATH’s president, Dr Marci Bowers, comments on the impact of early blocking of puberty on sexual function in adulthood. “To date,” she writes, “I’m unaware of an individual claiming ability to orgasm when they were blocked at Tanner 2.” Tanner stage 2 is the beginning of puberty. It can be as young as nine in girls.
Elsewhere, there are extraordinary discussions on how to manage “trans clients” with dissociative identity disorder (what used to be called multiple personality disorder) when “not all the alters have the same gender identity”. Surgeons talk about procedures that result in bodies that don’t exist in nature: those with both sets of genitals – the “phallus-preserving vaginoplasty”; double mastectomies that don’t have nipples; “nullification” surgery, where there are no genitals at all, just smooth skin. And doctors discuss the possibility that 16-year-old patients have liver cancer as the result of taking hormones. The problem is not necessarily the discussions themselves, but that the organisation is not so open when speaking publicly.
The views of WPATH matter to the UK. For years, the organisation and its SOC have been cited as a source of “best practice” for trans healthcare by numerous medical bodies, including the British Medical Association and the General Medical Council – and still is. The Royal College of Psychiatrists refers to WPATH in its own recommendations for care.
Most relevant is that WPATH is cited as “good practice” in the current service specifications underpinning youth and adult gender clinics in England and Scotland, albeit in both cases it is WPATH’s previous SOC that is mentioned. The most recent version does away with all age limits from the beginning of puberty for hormones and surgical interventions, other than female to male genital surgery, and contains a chapter on eunuchs.
Several staff at England’s NHS adult gender clinics are not just members of WPATH (one is the former president), but authors of that current SOC. So too was Susie Green, the former boss of the young people’s charity Mermaids; a lack of medical expertise does not exclude either membership of WPATH or the power to influence policy.
England’s only NHS children’s gender clinic – the Gender Identity Development Service (Gids) at London’s Tavistock and Portman NHS Foundation Trust – will close its doors at the end of March, having been earmarked for closure since July 2022. But the 2016 service specification still underpinning Gids states that “the service will be delivered in line with” WPATH 7. While Gids was generally more cautious than other WPATH practitioners, clinicians I spoke to for my book, Time to Think, also relayed how young people claiming to have multiple personalities, or who identified with another race, could be referred for puberty blockers.
Gids staff have also presented at WPATH conferences for the past decade, including the most recent, held in 2022. This doesn’t imply agreement with WPATH’s principles, but association with the group becomes harder to justify as its views become more extreme.
It is difficult to see how the Department of Health’s assertion that NHS England “moved away from WPATH guidelines more than five years ago” holds.
What is true is that there is no mention of WPATH in updated guidance that will underpin the new youth gender services opening on 1 April. What’s more, NHS England has made it clear that WPATH’s views are irrelevant to its core recommendation that puberty blockers will no longer be available as part of routine clinical practice.
There is a battle raging over how best to care for children and young people struggling with their gender identity, with ever increasing numbers of European countries choosing to take a more cautious, less medical, approach after finding the evidence base underpinning those treatments to be wanting. NHS England insists that new services will operate in accordance with recommendations of the independent Cass review, and that it is well placed to develop policies “in line with clinical evidence and expertise”. But it won’t be easy. There is already discussion among professionals working in gender services planning a pushback against Cass’s as yet unpublished final recommendations.
It was difficult for Gids to stand up to external pressures, allowing the care it offered to suffer. At the same time, NHS England failed in its duty to provide proper oversight. Both they and those in charge of the new services must do better if they are to avoid the mistakes of the past. Without proper, evidence-based guidance on what good practice looks like, organisations like WPATH will continue to have influence.
9 notes
·
View notes
Text
"WPATH Files" Authors Upset Over How “Suspiciously” Happy Trans People Are
“WPATH Files” Authors Upset Over How “Suspiciously” Happy Trans People Are
The error-ridden “WPATH Files” spend 37,000 words telling you what to think. Nowhere is this more obvious than where the authors experience dismay over “suspicious” happiness of trans people.
View On WordPress
5 notes
·
View notes
Text
can't wait to get my wpath assessment certificate for top surgery

9 notes
·
View notes
Photo




[ Link: https://www.tandfonline.com/doi/pdf/10.1080/26895269.2022.2100644 ]
[ Correction: https://www.tandfonline.com/doi/full/10.1080/26895269.2022.2125695 ]

They have no idea how many or why people detransition. The claim that it’s a tiny minority is completely baseless.
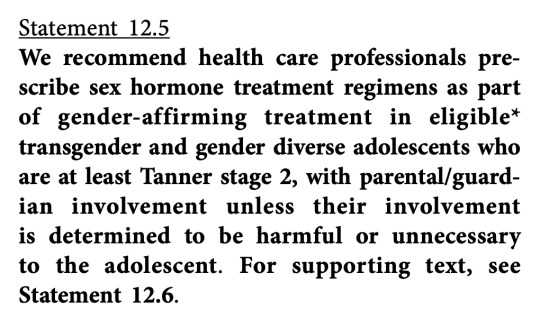
Tanner Stage 2 occurs on average at about 10 years of age in girls, as early as 8, and on average at about 12 years of age in boys, as early as 9. So WPATH is proposing that if a 10 year old girl wants puberty blockers or cross-sex hormones - note that this is about hormones, not just blocking puberty - but her parents are dubious, members complying with WPATH standards will simply administer them anyway.

That is, there are more controls for detransitioning than transitioning. This is how cults work.
Except, who’s going to go back to the doctor who mutilated them? The Tavistock said that they have no idea what proportion of their, ahem, “patients” desisted or detransitioned, because they never followed them up. They never heard back from them, and that was it. This is suggesting that they will follow up, but it’ll be like an army of Jehovah’s Witnesses at your door with “additional viewpoints.” That is, they’ll only challenge the motives of a detransitioner, not someone seeking transition.
“There's kind of like this attitude in the trans community that if you question your transition, that makes you insane.”
-- Helena Kerschner
The paper repeatedly cites Jack Turban, who is a known liar.
It’s hard to tell if they’re now extremely confident now that this ideology has attained cultural supremacy and institutional domination and have dropped the mask of what they’re up to, or they’re in panic mode, making a last-ditch grab before it all comes crashing down.
Believe them when they tell you what they’re up to.
#James Esses#queer theory#gender ideology#WPATH#defund WPATH#World Professional Association for Transgender Health#ideological capture#ideological corruption#gender cult#medical malpractice#unethical#medical scandal#medical corruption#medical transition#detransition#detrans#wokeness as religion#cult of woke#woke activism#wokeism#woke#religion is a mental illness
479 notes
·
View notes
Text
Publication of the leaked WPATH files.
Via Environmental Progress.

The written WPATH Files come from WPATH’s member discussion forum, which runs on software provided by DocMatter. Ninety seconds of the 82-minute video was made public last year. We are making the full video available for the first time. One or more people gave me the WPATH Files, and my colleagues and I attempted to summarize them as a series of articles. We quickly realized the topic was too sensitive, complex, and large to be dealt with as a work of journalism, and we moved the project to the research institute I founded seven years ago, Environmental Progress (EP). The Files are authentic. We redacted most names and left only those individuals who are leading gender medicine practitioners to whom we sent “right-of-reply” emails. We know WPATH members discussed our emails internally. No WPATH leader or member has denied that the Files are anything other than what they appear to be. EP is publishing a 70-page report to provide context for the 170 pages of WPATH Files. Mia Hughes is the author of the report. It and accompanying summary materials can be downloaded at the link below. That link also provides a link to the full WPATH video. What follows are simply a few highlights. People with a serious interest in the topic should read the report and all the files."


READ: THE WPATH FILES AND REPORT
#gender critical#gc#WPATH#World Professional Association of Transgender Health#medical experimentation#gender medicine#pseudoscientific surgical and hormonal experiments on children#trans madness#gender madness#leave those kids alone#video#feminist#radfem
3 notes
·
View notes
Text
#gender critical#gender is a social construct#gender#gender stereotypes#gender identity#gender ideology#wpath#transgender ideology#transgender
4 notes
·
View notes
Text
So you know about the "WPATH Files", that collection of screenshotted posts taken from the WPATH forum, which supposedly expose how WPATH doctors are evil and out to get your children? You'd be surprised about how the claims anti-trans activists make about those posts are not supported by the posts themselves. Don't believe me? Then let's look at the NY Post article about the document. Specifically, let's look at what the article claims versus the actual reality of what is shown in those posts.
TL;dr:
WPATH doesn't authorize medical transition procedures for immature patient. They actually verify that the patient is mature enough, before allowing the procedure. They also need parental consent.
WPATH doesn't ignore the risks of gender-affirming care. They explain them to both patient and parents, in detail. And if issues do show up, they try to fix them instead of sweeping them under the rug.
WPATH isn't trying to "desex (sterilize) children". That's just the same, old, tired "they're coming for your children!" narrative used against Jewish people, gay people etc etc.
WPATH doesn't disbelieve detransitioners, they support them.
CLAIM: Not surprisingly, age comes up frequently in the WPATH files, from concerns about whether a developmentally delayed 13-year-old can start on puberty blockers to whether the growth of a 10-year-old girl will be stunted by hormones. (The article implies that WPATH doctors are pushing medical procedures on patients who are too young to understand them)
REALITY: The first case (section 21-A "ETHICAL GUIDELINES TO ADOLESCENT CARE - WPATH members discuss the Standards of Care (SOC) ethics for treating adevelopmentally delayed, 13-year-old") is about a 13yo who is already on puberty blockers. Specifically, patients who want hormone therapy need to reach enough emotional/cognitive maturity to provide informed consent to the treatment; but the specific patient in question will reach that maturity either way later than normal, or never at all. The poster asks what to do. Other users suggest a psychiatric evaluation to check whether the patient is capable of consenting or not, weighing the risks of continuing the blockers with the risks of stopping them, etc.
There is no evidence that the doctors gave hormones to that 13yo. Keep in mind that the NYP was complaining about the possibility of that 13yo getting hormones. The NYP had no complaint about the usage of puberty blockers, since the patient was effectively mature enough to get those, and the parents and doctors gave authorization.
Also, one of the posters point out that this kind of discussion also happens with cis (aka non-trans) kids with mental development issues who need access to surgeries. The normal approach is for the doctor, the parents and the patient to discuss together to reach a consensus: in order to approve the medical procedure, the doctor must believe that the procedure will be medically beneficial, the parents must provide full informed consent, and the patient must provide as much consent as possible. There are limit cases where one side can be overridden, like when a patient will never reach a sufficient level of mental maturity, and the doctor and parents are forced to evaluate the risk/benefits of each option. My point is that the NYP has no problems when this approach is applied to cis kids; it complains only when trans kids might get access to medical procedures.
The second case (section 5-A "PUBERTY SUPPRESSION TACTICS - A WPATH member questions the effects of puberty blockers on total height achievement for a 10-year-old patient") is about a patient who asked questions about puberty blockers. The 10yo patient in question was NOT on puberty blockers, nor he was given any - unlike what the NYP tries to imply.
CLAIM: During one conversation, a member asked for advice about a 14-year-old patient, a boy who identified as a girl and had begun transitioning at 4. The child insisted on a vaginoplasty...
REALITY: This is false. The original poster (section 1-A "GENDER AFFIRMING SURGERY FOR MINORS - WPATH members discuss transition surgery for a 14-year-old") only talks about "Gender Affirming Surgery MtF". Christine N. McGinn talks about vaginoplasties she performed on minors, noting that they didn't have any more issues than adult patients: most of them went fantastic, a few of them got issue (mostly because they didn't follow the dilation schedule), and none of them regretted the surgery.
It should also be mentioned that multiple users agreed that 14 was too young. Which shoots a hole in the NYP's "WPATH tried to push vaginoplasty on a 14yo kid" narrative. Whoops.
CLAIM: President Bowers, for instance, said publicly in 2022 that puberty blockers are “completely reversible,” although in the internal forum she conceded it is “in its infancy.”
REALITY: The two quotes don't contradict each other. In the first quote, Bowers claims that blockers AS THEY ARE USED IN GENDER-AFFIRMING CARE (aka for maximum 1 year) are reversible - meaning that if you stop taking them, the effects should reverse themselves. But the second quote (in section 5-B "PUBERTY SUPPRESSION TACTICS - WPATH members discuss how puberty blockers preclude fertility options for trans patients") talks about what happens when puberty is blocked indefinitely. Two very different things.
CLAIM: What about children who are infertile for life since they started hormone blockers before they reached puberty? Bowers told her colleagues the “fertility question has no research.”
REALITY: The Bowers quote doesn't exist in any of the screenshotted posts. The NYP made that up.
CLAIM: At other stages, members talk frankly about the complications for the transition surgery for girls, a phalloplasty in which a nonfunctioning pseudo-penis is fashioned from either forearm or thigh tissue. It requires a full hysterectomy and surgical removal of the vagina. They also discuss other serious consequences, including pelvic inflammatory disease, vaginal atrophy, abnormal pap tests and incontinence.
REALITY: I can't find the screenshotted posts in question. But let's assume for a second that the NYP is telling the truth here; it doesn't actually explain why "WPATH doctors discuss the complications for transition surgery" is bad. As usual, anti-trans activists only focus on the negative effects and risks of any form of medical transition, while completely ignoring any possible positive effect - like, say, alleviating the patient's gender dysphoria.
As far as I can tell, the NYP is trying to imply that these doctors hide these risks from their patients. Which... isn't true. Like, at all. In fact, the fact that they talk about the negative effects so much on a web forum that anyone can access just by paying a fee should clue the reader that these doctors are NOT trying to hide these effects/risks from their patients.
CLAIM: A 16-year-old girl who had been on puberty blockers for several years before she was put on testosterone for a year had developed two liver tumors that an oncologist concluded the hormones had caused.
REALITY: Looking at the posts (section 3-B "SURGICAL OR HEALTHCARE COMPLICATIONS - A WPATH member discusses the development of hepatic adenomas on a client taking testosterone/estrogen"), it turns out that the patient was using both testosterone and oral contraceptives. Hepatic adenomas, also called hepatocellular adenomas, are rare but benign epithelial tumors of the liver frequently associated with oral contraceptive pill use. Meanwhile, there is no evidence that transmasculine people who use hormones are at risk of liver cancer. (Sources: 1, 2.)
CLAIM: Another member described “a young patient on testosterone for 3 years” who had developed “vaginal/pelvic pain/spotting . . . [and] atrophy with the persistent yellow discharge.” Several colleagues described patients with similar conditions, some with debilitating bowel problems or bleeding and excruciating pain during sex (“feeling like broken glass”). Vaginal estrogen creams and moisturizers as well as hyaluronic acid suppositories “can be helpful.” One WPATH member seemed surprised: “The transgender people under my surveillance do not complain about this matter. However, I confess that I have never asked them about it.”
REALITY: This part of the NYP article repeatedly jumps between section 3-C "SURGICAL OR HEALTHCARE COMPLICATIONS - A WPATH member reports their young patient is experiencing vaginal pain on testosterone"; and section 3-D "SURGICAL OR HEALTHCARE COMPLICATIONS - WPATH members discuss erection pain in a patient on estrogen". So there's some confusion here. The general gist of both discussions is: the original poster brings up an issue that their patient has, other users discuss similar cases, provide additional information, and offer possible solutions.
Again: this is a case where a patient got some negative side effects from the treatment, and doctors are trying to solve them. Cases like these happen all the time. There is no evidence that the patient wasn't properly informed before being allowed to get the treatment. The doctors are trying to fix the problem. So what, exactly, is the NYP complaining about? Because if ONE single case of negative effects is enough to condemn a medical treatment, then the NYP should condemn every single medical treatment ever. But no, instead they only focus the blame on treatments that are primarily used by trans people. I wonder why [#sarcasm].
CLAIM: “How do we come up with appropriate standards for non-binary patients?” asked Thomas Satterwhite, a San Francisco-based plastic surgeon who has operated on dozens of patients younger than 18 since 2014. “I’ve found more and more patients recently requesting ‘non-standard’ procedures.” What are nonstandard procedures? They include “non-binary top surgery,” a mastectomy without nipples. There are brutal procedures for girls that eliminate all or part of the vagina and for boys that amputate the penis, scrotum and testicles.
REALITY: Satterwhite did, in fact, ask information about standards for non-binary patients (section 12-A "NON-STANDARD MEDICAL PROCEDURES - WPATH members discuss appropriate standards of care for nonbinary patients, particularly when they request non-standard procedures"). However, you can notice a thing. The NYP made sure to explicitly talk about "de-gendering" surgeries in the most scary and shocking way possible; then they mentioned that Satterwhite operated on dozens of patients younger than 18; then mentioned his quote about non-standard surgeries; and then proceeded to once again describe said surgeries in scary terms, saying that they're performed on "girls" and "boys". So you would think that Satterwhite is performing these horrible surgeries on children, right?
Well, turns out that in the screenshotted posts, Satterwhite made absolutely no mention of underage patients. His question was about non-binary patients in general.
Also, fun fact that the NYP doesn't mention: in trans healthcare, practically all genital surgeries are performed on adult patients. The very few exceptions are performed on 17yo patients, but ONLY in cases where waiting until the patient becomes 18 would make the surgery significantly harder to perform, to the point of having an increased risk of killing the patient. And even then, you need a metric ton of medical requirements.
CLAIM: A particularly intense subject of discussion was whether minors could understand the lifelong consequences of their gender treatments. Minors are presumed by law to be incapable of making an informed decision about having a vasectomy or tubal ligation. Gender surgeries are an exception, however. WPATH’s Standard of Care allows all procedures so long as the minor “demonstrates the emotional and cognitive maturity required to provide informed consent/assent for the treatment.”
REALITY: The NYP is lying. For starters, it forgets to mention that, in various states, minors CAN get certain surgical procedures as long as they pass certain prerequisites, such as a minimum age (like 16). Why? Because it's acknowledged that children mature over time, and become more and more capable of understanding - and by extension consenting to - more complex things, like surgeries.
Another thing that the NYP omits is that minors can get invasive medical treatments even if they don't reach the minimum consent age, as long as the doctor can provide reasonable medical reason to do so; the parents provide fully informed consent to the procedure; and the underage patient provides a sufficient amount of consent, which varies depending on the procedure requested. The latter is what “demonstrates the emotional and cognitive maturity required to provide informed consent/assent for the treatment” refers to.
The main difference is that WPATH doesn't decide that patients above a certain age are automatically mature enough to consent to a specific procedure; instead, WPATH doctors actually verify whether or not the patient is mature enough to consent to that specific procedure.
CLAIM: In a May 2022 internal workshop, “Identity Evolution,” WPATH members conceded that was all but impossible. Daniel Metzger, the British Columbia endocrinologist who cowrote the Canadian Pediatric Society’s position paper on health care for trans minors, said, “I think the thing you have to remember about kids is that we’re often explaining these sorts of things to people who haven’t even had biology in high school yet.”
The quote is from the transcript of the "Identity Evolution Workshop", Clip 1. It also completely fails to prove the NYP's point. Remember: the NYP is trying to claim that children cannot, under any circumstance, consent to surgeries - implying that this means that they shouldn't have access to surgeries. This is false.
Also, the transcript shows Metzger saying that they should improve the way doctors explain medical procedures to patients and parents, because if they don't understand these procedures, they can't provide informed consent, and therefore they can't have access to said procedures. Metzger is NOT proposing to provide medical procedures to people who don't provide informed consent.
CLAIM: Although many WPATH members privately doubt that adolescents can give truly informed consent to life-altering procedures, they must affirm whatever children say about their gender.Unless, the WPATH files disclose, the patient wants to reverse course and become a so-called detransitioner.WPATH members mostly dismiss those cases as insignificant or overblown by the media and question whether minors who want to revert to their birth sex really understand what they are doing.It’s a question that would never be asked for minors who declared themselves to be gender dysphoric. One case involved a 17-year-old boy, just graduated from high school, who had been on testosterone for two years. He was reported to be “very distraught and angry. He reports he feels he was brainwashed and is upset by the permanent changes to his body.”A self-described “queer therapist” did not believe any young person could be brainwashed. “In my experience, those stories come from people who have an active agenda against the rights of trans people.”
REALITY: The NYP is dishonestly mixing together multiple different contexts.
When a patient goes to a WPATH doctor and claims to be trans, the doctor accepts it. When a patient claims to not be trans anymore, the doctor still accepts it.
When a patient declares themselves to be gender dysphoric, the doctor DOES, in fact, verify whether the assertion is true, through psychological examination, exploring whether the dysphoria is innate or caused by issues like mistakenly believing that being feminine means that you must be a girl and therefore have "female" biology and so on. After that is verified, however, the doctor accepts that the patient is right.
When discussing how the media and public claim that there is an epidemic of detransitioners, THAT is when WPATH doctors will say that the issue is overblown. Because the reality is that the amount of detransitioners - and specifically people who got through medical transition and then detransitioned afterwards - is incredibly small, unlike what anti-trans activists would make you believe.
All of that can be clearly seen in the discussion in section 4-A "DETRANSITION CONCERNS - A WPATH member reports a patient who reports feeling “brainwashed” into transition".
SO, TO RECAP:
The NYP complains that the WPATH uses ‘arbitrary’ age limits, implying imply that WPATH is trying to pressure forcibly trans young kids before they were ready. The reality, however, is that WPATH is doing what every other medical field does when a patient is a minor: they approve the treatment only if the doctor reasonably believes that it will be overall beneficial, the parents give informed consent, and the patient itself gives consent as much as possible. Checking whether or not a kid is mentally mature enough to at least understand somewhat the procedure falls under the third point; checking the kid's physical maturity falls under the first point, because it impacts whether or not the therapy will be overall beneficial.
(BTW, the NYP says that, when making the new Standards of Care, WPATH "scrapped a draft chapter about ethics and removed minimum-age requirements for children starting puberty blockers or undergoing sexual-modification surgeries." What the NYP doesn't say is that the guidelines ARE the ethics of the practice; and that WPATH replaced minimum-age requirements with evidence-based requirements. For example: instead of assuming that all 16yo patients are automatically mature enough to get hormones, the new guidelines require doctors to actually verify whether the patient is mature enough (both physically and mentally) or not. Why this change? Because there were several cases where 16yo-or-older patients were allowed to get hormones when they weren't ready.)
The NYP claims that WPATH doctors downplayed the dangers of gender-affirming care. They did not. The post themselves demonstrate that they amply and truthfully discuss these dangers - and inform their patients about them. And when negative issues do show up, WPATH doctors try to fix them.
The NYP implies that WPATH doctors are trying to de-sex children. They did not. The posts only talk about performing non-standard procedures on non-binary patients - but they make absolutely no mention of minors.
The NYP claims that WPATH doctors are dismissing and disbelieving detransitioners. They did not. WPATH doctors support detransitioning patients, direct them towards support groups, research solutions for the physical issues caused by the regretted procedures, and so on and so forth. WPATH doctors also denounce the whole "there's an epidemic of people who go through medical transition and then later detransition and regret it, because it's way too easy for children to get brainwashed into being trans and to get medical transition" narrative as false because it IS false.
4 notes
·
View notes




