#World Professional Association of Transgender Health
Text
By: Michael Shermer
Published: Mar 8, 2024
Leaked documents from World Professional Association for Transgender Health practitioners reveal a medical profession in the grips of an ideology-driven social contagion
In an early study of crowd psychology, Extraordinary Popular Delusions and the Madness of Crowds (originally published in 1841 and still in print), the Scottish journalist Charles Mackay documented such delusions as alchemy, fortune-telling, haunted houses, magnetizers, religious relics, and prophecies, and the mad crowds that fell for economic bubbles like the Dutch tulip mania, the Railway Mania, witch crazes, and the South Sea Bubble. “Men, it has been well said, think in herds; it will be seen that they go mad in herds,” Mackay observed, “while they only recover their senses slowly, one by one.”
The redux of my title includes such such popular delusions of the past half century as the Subliminal Messages scare, the Satanic Panic, the Recovered Memory mania, the Self-Esteem movement, the Multiple Personality craze, the Left-Brain/Right-Brain fad, the Mozart Effect mania, the Vaccine-Autism furor, the Super-predators fear, the Drug Abuse Resistance Education (DARE) program that increased teen drug use, the Scared Straight program that made adolescents more likely to offend, the Critical Incident Stress Debriefing (CISD) programmed that worsened anxiety and symptoms of post-traumatic stress disorder (PTSD), and many more that have plagued psychology and psychiatry.
The latest of what is likely to be added to this pantheon of popular delusions embraced by mad crowds is the trans movement as a whole and Rapid Onset Gender Dysphoria in particular, as revealed on Tuesday March 5, 2024 by Michael Shellenberger, Mia Hughes, and their colleagues at Environmental Progress in a 242-page document titled The WPATH Files: Pseudoscientific Surgical and Hormonal Experiments on Children, Adolescents, and Vulnerable Adults. “The World Professional Association for Transgender Health (WPATH) enjoys the reputation of being the leading scientific and medical organization devoted to transgender healthcare,” the authors note. However, after reviewing hundreds of leaked internal documents revealing shocking levels of uncertainty, ignorance, and devotion to outdated and debunked pseudoscientific theories, therapies, and practices, the report’s authors conclude that the opposite is true:
Newly released files from WPATH’s internal messaging forum, as well as a leaked internal panel discussion, demonstrate that the world-leading transgender healthcare group is neither scientific nor advocating for ethical medical care. These internal communications reveal that WPATH advocates for many arbitrary medical practices, including hormonal and surgical experimentation on minors and vulnerable adults. Its approach to medicine is consumer-driven and pseudoscientific, and its members appear to be engaged in political activism, not science.
We devoted an issue of Skeptic to “Trans Matters” (Vol. 27, No. 1) that included an especially thoughtful, sensitive, and deeply-researched cover story by Lisa Selin Davis, “An Overview of the Debate, Research, and Policies”, documenting the massive spike in patients reporting gender dysphoria over the past decade (this data is from a gender clinic in British Columbia but rates are comparable elsewhere). Before 2015, most trans were young boys who identified as female; after 2015 most trans were adolescent girls identifying as males.
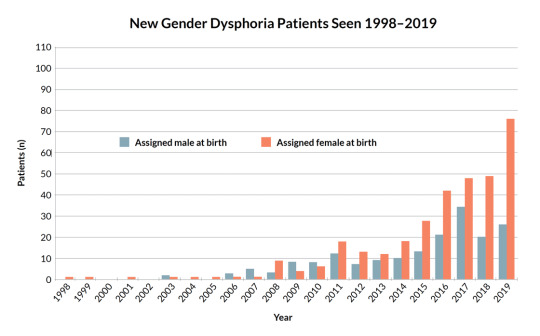
As I read the research, the Before Time (pre-2015) was very likely recording real instances of gender dysphoria (GD) in very young children and at a vanishingly rare rate well below 1%; the After Time (post-2015 to today) is very likely a phenomenon called rapid-onset gender dysphoria (ROGD), a label coined by the physician and public health researcher Lisa Littman, after she discovered in her exploratory study based on parental reports that entire peer groups of adolescents and teens were declaring themselves to be transgender, after immersion in social media or exposure in classrooms in which sizable proportions of students identified as anything but cisgender and straight. With watchful waiting and compassionate support for these adolescents, and dealing with their underlying issues of body dysphoria from puberty, autism, anorexia, and normal teen anxiety, sadness, and stress, the vast majority grow out of their self-identity of “being in the wrong body” and/or realize that, in fact, they are gay or lesbian.
Unfortunately, watchful waiting and compassionate support is not a practice that WPATH appears to recommend to medical and psychological practitioners; instead, “gender affirming care” calls for them to go along with whatever their (almost always) underage patients tell them that they want, which is often invasive, irreversible, and life-changing Hormone Replacement Therapy (HRT) and/or surgery, including the amputation of healthy breasts in females (a double mastectomy, or “top surgery”) and the surgical removal of otherwise healthy genitals and reproductive systems that will never again function normally (“bottom surgery”). Detransitioners—those who transitioned then changed their minds and sought to return to their “assigned at birth” sex (a number that is growing by the month)—are discovering that they can never have biological children (they’re told “don’t worry, you can always adopt”), can never breast feed (they’re told they can “strap on” milk-delivering faux-breasts and become “chest feeders”), and can never experience the full range of normal sexual functioning, including orgasms, not to mention numerous drug side-effects, surgical complications, infections, mounting medical bills not covered by insurance, and the like. As the authors of the WPATH Files note:
This report will show that this is a violation of medical ethics and, as is revealed by its own internal communications, WPATH does not meet the standards of evidence-based medicine. It will further show that the ethical requirement to obtain informed consent is being violated, with members admitting that children and adolescents cannot comprehend the lifelong consequences of sex-trait modification interventions, and in some cases, due to poor health literacy, neither can their parents.
Before I review some of these documents, let me note that I have covered this topic before in this column, for example, answering the question “What is a Woman, Anyway?”, on the trans swimmer Lia Thomas in particular, and on trans athletes in female sports in general. I personally know two (MTF) trans adults who transitioned well into adulthood and are happy they did so, I recognize that there are people who genuinely experience GD (which is different from ROGD), and I stand by my statement in the last column that:
Of course we should support trans rights for the same reason we support the rights of people of color, women, and gays: it is immoral (and in many cases illegal) to discriminate against someone based on such immutable characteristics as skin color, gender, and sexual preference, so gender identity should be included in our ever-expanding moral circle and our ever-bending moral arc. The problem arises when there are conflicting rights claims.
In the WPATH Files what we see is the rights of underage adolescents and vulnerable adults being violated by the very people tasked with protecting them, so I agree with the authors’ call for “the U.S. government to oversee a bipartisan national inquiry to investigate how activists with little respect for the Hippocratic Oath could have risen to such prominence as to set the Standards of Care for an entire field of medicine, leading to the medical abuse of minors and vulnerable adults.”
What follows are some of the more revealing—and in many cases egregious—examples of uncertainty, ignorance, and embrace of pseudoscientific ideas revealed in the “semi-private conversations inside WPATH’s internal online forum for discussing specific medical cases,” along with my comments (below each screen shot)
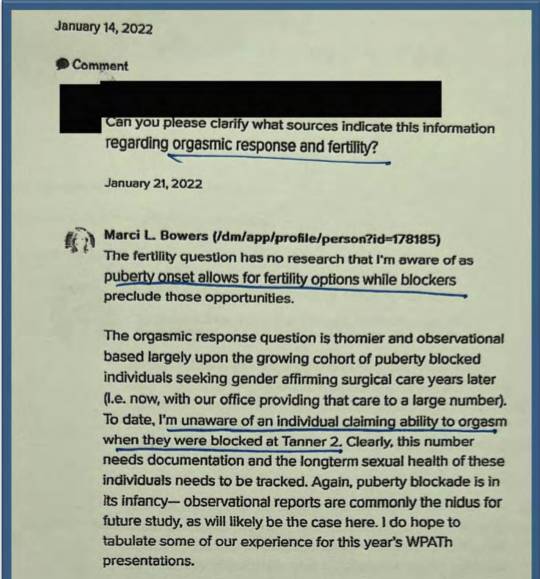
Note that this post is from Marci Bowers, often tagged as “the world’s preeminent ‘gender-reassignment’ surgeon” and who self-identifies as “a woman with a trans history” (i.e., a Male-to-Female [MTF] trans), revealing that medical professionals had no idea of the consequences of transitioning youth. The correspondent inquires about the consequences for fertility and orgasmic response post transition. “The fertility question has no research that I’m aware of,” Bowers admits, but suggesting that puberty blockers will “preclude those opportunities.” Oh is that all? What about orgasms? Again, Bowers is “unaware of an individual claiming ability to orgasm” after puberty blockers. Say again?
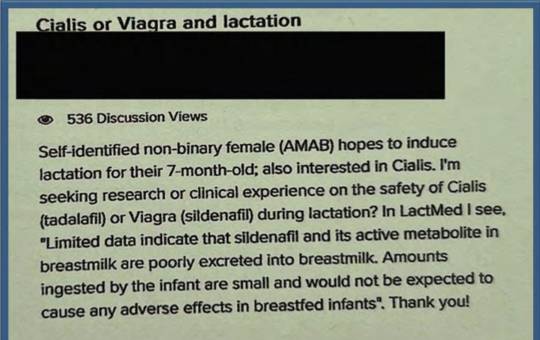
Here is a man (AMAB = Assigned Male at Birth) who self-identifies as a non-binary female who is taking Cialis/Viagra (presumably to enhance his—sorry, her—erections) who wonders if they breast feed their 7-month old will the meds get into the infant’s system. Apparently the amounts would be so small that the infant would not experience “any adverse effects” such as, what, erections?

Here's a therapist who practices EMDR (Eye Movement Desensitization and Reprocessing), the long discredited treatment for PTSD/trauma. These people are years behind the science. A 2022 literature review, for example, concluded: “Taken as a whole, this small body of work suggests that eye movements do not reliably affect susceptibility to misinformation, nor do they appear to enhance memory, but they do seem to increase spontaneous false memories.” False Memory Syndrome is the correct interpretation of what was happening in the 1990’s Recovered Memory Movement in which adult patients in psychotherapy were convinced by quack therapists that they had been sexually molested as children, even though the patients had no memory whatsoever of such abuse, nor was there any corroborating evidence such crimes ever occurred. Astonishingly, there were cases of aging parents who were tried, convicted, and imprisoned for sexual molestation based on nothing more than bogus “recovered memories,” a mass hysteria that came to an abrupt end when lawyers sued therapists for malpractice. See Carol Tavris’s account of this madness here.


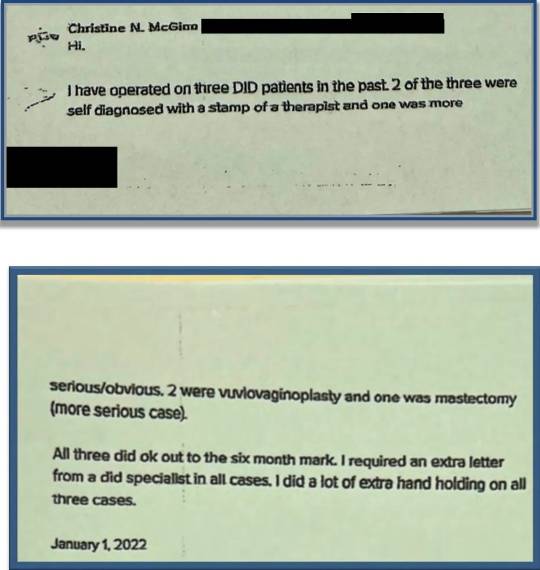
Here is a discussion of Dissociative Identity Disorder (DID), previously known as Multiple Personality Disorder (MPD), explaining that consent for transitioning must be obtained from each "alter" (alternative personality). DID and MPD is a bogus diagnosis. There is no such thing as multiple personalities, so there can be no "alternate" personalities to give consent. The entire diagnosis was founded on two famous cases that turned out to be fraudulent: Sybil and Eve (as in The Three Faces of Eve). The real Sybil—Shirley Mason (played by Sally Field in the film version)—admitted she made it all up: "I do not really have any multiple personalities. I do not even have a 'double.' ... I am all of them. I have been lying in my pretense of them." As for Eve, the real woman was Chris Costner Sizemore (played by Joanne Woodward in the film rendition), and her three faces eventually transmogrified into over 20, until a book revealed that the psychiatrist who diagnosed her was sexually and financially abusing her. Nevertheless, such quack diagnoses didn’t stop this surgeon from cutting off the healthy breasts of a DID woman, or carving out fake vaginas in two DID men:
For a complete debunking of these and additional bogus psychological theories, therapies, and treatments, see 50 Great Myths About Popular Psychology by the late Scott Lilienfeld and colleagues, and his more scholarly debunking in Science and Pseudoscience in Clinical Psychology. Skeptic’s own columnist Carol Tavris has debunked these and more quack psychology in our pages (for example, see her article on trans issues here).

This post-op trans woman (a man) later "discovered that I was not suffering from any actual pathology related to being trans.” Yet, she claims to still experience cPTSD, ADHD, anxiety, and depression. O-kay.
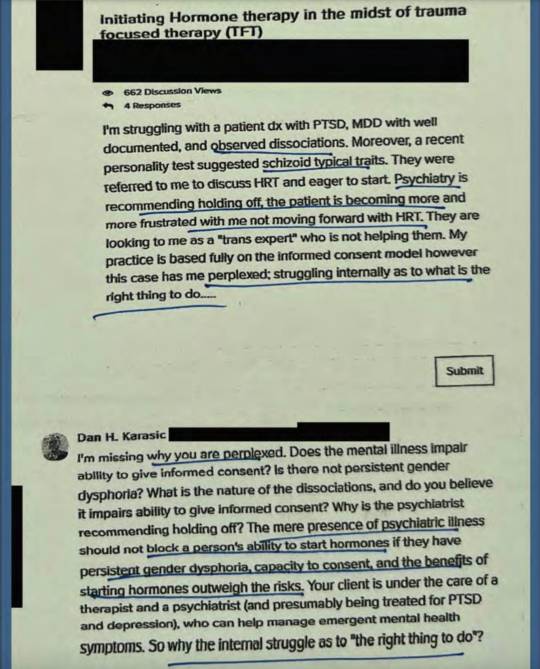
This exchange shows a practitioner reasonably conflicted about starting a patient on HRT (Hormone Replacement Therapy) with so many problems, but is nevertheless told it’s “the right thing to do”!
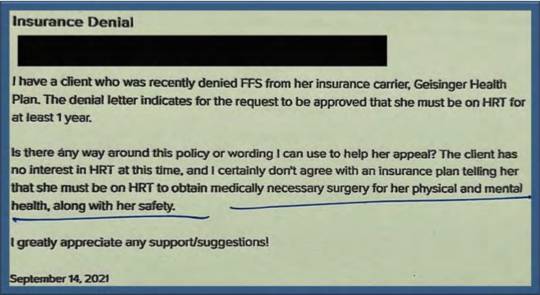
Here a WPATH member complains that their client was denied insurance coverage for surgery until completing a year of HRT, stating that they think the patient needs surgery “for her physical and mental health, along with her safety.” Safety?
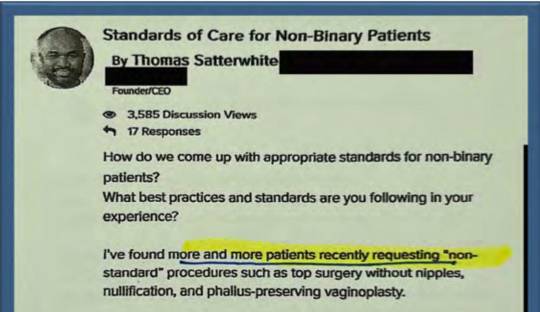
This surgeon isn’t sure how to handle patients requesting “non-standard” procedures, such as top surgery without nipples (“non-binary” means “non-nipples”?) and “phallus-preserving vaginoplasty.” The latter is non-standard indeed, inasmuch as normal vaginoplasty involves removing the penis, testicles and scrotum. This patient apparently wants both. In a follow-up missive Dr. Satterwhite explains: “With every patient I operate on, I always take a patient-centric approach and I let my patient lead the journey (not me).” Therein lies the problem when you’re dealing with underage patients who are otherwise not allowed to drive, drink, smoke, vote, serve in the military, get tattoos, and more. Why would anyone—much less medical professionals—think that adolescents could make adult decisions about such life-altering treatments?
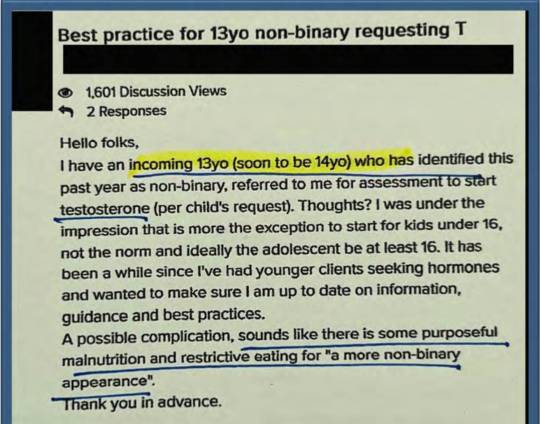
Note not only the age of onset of this condition (non-binary), 13, or that the testosterone request comes from the child and not a parent, guardian or medical professional, but that on top of all that this kid is purposefully starving themselves to look “more non-binary”. Presumably this means anorexia. Whatever this youngster is experiencing it is not going to be ameliorated by transgender medical treatments. This is medical malpractice, pure and simple, and it has to stop.
I could go on and on with dozens more such revelatory correspondence from the WPATH Files, so let me close with this observation from John Mackay, who presciently put his finger on the problem we are experiencing today: “We find that whole communities suddenly fix their minds upon one object, and go mad in its pursuit; that millions of people become simultaneously impressed with one delusion, and run after it, till their attention is caught by some new folly more captivating than the first.”
I have little doubt that when the ROGD trans social contagion runs its course it will be replaced by something else, but without politicians or attorneys intervening in the meantime I am not at all confident that the WPATH community is capable of self-regulation and course-correction away from the flagitious path they’ve been on. Still, in the long run, optimist that I am, I hope lessons will be learned from this episode, as they were with the aforementioned previous popular delusions; and with that hope I will give the last word to Mackay:
Let us not, in the pride of our superior knowledge, turn with contempt from the follies of our predecessors. The study of the errors into which great minds have fallen in the pursuit of truth can never be uninstructive. As the man looks back to the days of his childhood and his youth, and recalls to his mind the strange notions and false opinions that swayed his actions at the time, that he may wonder at them; so should society, for its edification, look back to the opinions which governed ages that fled.
Amen, brother.
#Michael Shermer#social contagion#WPATH#The WPATH Files#World Professional Association of Transgender Health#medical corruption#medical malpractice#medical scandal
8 notes
·
View notes
Text
Publication of the leaked WPATH files.
Via Environmental Progress.

The written WPATH Files come from WPATH’s member discussion forum, which runs on software provided by DocMatter. Ninety seconds of the 82-minute video was made public last year. We are making the full video available for the first time. One or more people gave me the WPATH Files, and my colleagues and I attempted to summarize them as a series of articles. We quickly realized the topic was too sensitive, complex, and large to be dealt with as a work of journalism, and we moved the project to the research institute I founded seven years ago, Environmental Progress (EP). The Files are authentic. We redacted most names and left only those individuals who are leading gender medicine practitioners to whom we sent “right-of-reply” emails. We know WPATH members discussed our emails internally. No WPATH leader or member has denied that the Files are anything other than what they appear to be. EP is publishing a 70-page report to provide context for the 170 pages of WPATH Files. Mia Hughes is the author of the report. It and accompanying summary materials can be downloaded at the link below. That link also provides a link to the full WPATH video. What follows are simply a few highlights. People with a serious interest in the topic should read the report and all the files."


READ: THE WPATH FILES AND REPORT
#gender critical#gc#WPATH#World Professional Association of Transgender Health#medical experimentation#gender medicine#pseudoscientific surgical and hormonal experiments on children#trans madness#gender madness#leave those kids alone#video#feminist#radfem
3 notes
·
View notes
Text

In 2017 I interviewed Bernadette Wren, then head of psychology at the Tavistock Gids clinic, and asked what effect puberty blocking drugs have on the adolescent brain. Looking highly uncomfortable, she replied that the evidence so far was only anecdotal but that the clinic would study its patients “well into their adult lives so that we can see”.
Even back then, before whistleblowers had exposed the rush to medically transition children, it was alarming to hear that heavy-duty GnRH agonists such as triptorelin — used to treat advanced prostate cancer and “chemically castrate” sex offenders — were being prescribed to arrest puberty in hundreds of children as young as 11.
Moreover, they were being used “off-label” before any clinical trials. And the long-term study Wren promised never materialised: Gids (the Gender Identity Development Service) routinely lost touch with patients, and the 44 it did follow reported little long-term mental health improvement.
This shocking chapter in medical history, where the ideological objectives of trans rights campaigners trumped the welfare of disturbed children, is coming to an end worldwide. The decision by NHS England effectively to ban the prescription of puberty blockers comes after the Cass review noted these drugs could “permanently disrupt” brain development, reduce bone density and lock children into a regime of cross-sex hormones requiring life-long patienthood.
NHS England unites with other national health services including those in Finland, France, Sweden and, most notably, the Netherlands — where the “Dutch protocol”, a regime of early blockers then hormones, was devised in 1998 — in pulling back from prescribing them.
Even in the United States, where a toxic combination of extreme activism and medical capitalism has pushed child gender medicine to grotesque extremes, with double mastectomies performed on 14-year-old girls, there is some retrenchment.
Leaks from the World Professional Association for Transgender Health, the body which formulates guidance on “trans healthcare”, reveal doctors perplexed at how they should explain to an 11-year-old child that drugs will render them infertile. Crucially, liberal media such as The New York Times are now reporting grave medical misgivings about child transition, once dismissed as a culture-war issue for the Republican right.
Yet the question remains: how was this ever allowed to happen? For years, puberty blockers were cheerily billed as a mere “pause button”. In 2014, Dr Polly Carmichael, the last head of Gids before the Cass review ordered its closure, went on CBBC in a show called I Am Leo, saying of blockers: “The good thing is, if you stop the injections, it’s like pressing ‘start’ and the body carries on developing as it would if you hadn’t started.”
The BBC permitted her to make this unevidenced claim to an impressionable audience of six to 12-year-olds. Imagine hearing this as a developing girl, freaked out by your new breasts and periods. No wonder Gids referrals subsequently rocketed.
Carmichael failed to mention that she did not know if pressing “restart” on puberty is always medically possible — it is not — and in fact, almost every child Gids put on blockers went on to irreversible cross-sex hormones.
After years in a Peter Pan state while their peers developed, they understandably felt there was no way back and forged on with treatment. Yet if allowed to experience natural puberty, almost 85 per cent of gender dysphoria cases resolve themselves.
Nor did Carmichael tell CBBC kids that the blockers-hormones combination, if taken early enough, not only results in sterility but kills the libido so that a young person will never experience an orgasm.
At the 2020 judicial review brought by a former Tavistock clinician and Keira Bell, the brave young detransitioner rushed onto hormones by Gids, judges expressed astonishment at Gids’s lack of an evidence base.
Reporting on this issue for seven years, I too have been struck by a complete clinical incuriosity. Not only was data not collected, but those who queried treatments or pressed for evidence faced angry condemnation. Perhaps activists knew what research might find because one long-term Finnish study, recently reported in the BMJ, destroyed the myth used to justify blockers: that a child will commit suicide if denied them.
The Finns found that “gender-affirming care” does not make a dysphoric child less suicidal. Rather, such children had the same suicide risk as others with severe psychiatric issues. In other words, changing bodies does not fix troubled minds.
Yet even after NHS England’s announcement, activists refuse to heed the now-overwhelming evidence. In its response, Stonewall persists with the myth that puberty blockers “give a young person extra time to evaluate their next steps”.
Many questions remain unanswered: will private clinics still be permitted to prescribe puberty blockers; and is Scotland’s Sandyford child gender clinic still determined to close its ears to all evidence? Plus, we have few details on how the NHS’s new “holistic” treatment for gender-questioning children will operate when it opens next month.
This repellent experiment — in which girls who like trucks or little boys who dress as princesses, and who invariably grow up to be gay, are corralled inexorably down a road towards life-changing treatments — belongs in the book of medical disgraces. As do the cheerleaders who raised money for Mermaids and those who persecuted whistleblowers or damned journalists asking questions as transphobic.
In 50 years, chemically freezing the puberty of healthy children with troubled minds will be regarded with the same horrified fascination as lobotomies — which, never forget, won the Portuguese neurologist Antonio Egas Moniz the 1949 Nobel prize.
--------------------
{Article source (behind paywall)}
233 notes
·
View notes
Text
His work through EEF was crucial to improving the lives of countless trans people. In addition to funding many of the earliest research projects, his two main contributions were the financial support he gave to the Harry Benjamin Foundation and the first North American gender clinic at Johns Hopkins Hospital in Baltimore, Maryland.
Erickson funded international conferences on trans topics in 1969 (cosponsored by the Albany Trust of London), 1971, and 1973. Later conferences were organized by the Harry Benjamin International Gender Dysphoria Association (HBIGDA) founded in 1979. It changed its name to the World Professional Association for Transgender Health (WPATH) in 2007.
EEF made major contributions to growing public awareness, too, through funding lectures, educational films, newspaper articles, radio, and television programs, and books including Money and Green’s Transsexualism and Sex Reassignment, 1969, and Money and Ehrhardt’s Man, Woman, Boy, Girl, 1972. [...]
After learning about Los Angeles-based gay and lesbian rights group ONE, Inc., which published the highly influential ONE magazine, in 1964, Erickson began giving them money after convincing them to form the nonprofit, tax-exempt Institute for the Study of Human Resources.
With the huge amounts of money he gave them over the years that other gay groups at the time could barely dream of (some $1.5 million in today’s dollars), they published a two-volume Annotated Bibliography of Homosexuality and created a variety of unprecedented gay equality focused research and education programs including lectures, and, ultimately, accreditation in 1981 by the state of California as a graduate degree-granting institution.
1K notes
·
View notes
Text
Ho boy I just got hit with a wave of HRT related asks.
I'll respond to them to the best of my ability, but imma make a copy/paste disclaimer here:
I AM NOT A MEDICAL PROFESSIONAL. I have a very, VERY marginal ability to interpret medical data over the average person due to my bio background, but it's far less than people think- hell I just said something wrong about insurance that someone had to correct.
Unfortunately, however, the nature of trans healthcare being under constant political threat worldwide means that everyone should prepare to diy, and know the basics of how they would pull that off. That's why I'm answering these questions, more info out there is always better. HOWEVER, you would better be served by other sources, like:
Anything I say directly about medical care will be an interpretation or regurgitation of something that is likely in these sources, plus a dash of personal experience. My bio knowledge and interpretation is not going to kick in here, it's gonna be too far deep in the weeds of cellular mechanisms that it's not directly relevant.
82 notes
·
View notes
Text
(1) Arkansas ban on gender-affirming care for minors ruled unconstitutional
While Moody’s ultimate ruling in the case and legal conclusions obviously matter, his findings of fact issued Tuesday could be the most important aspect of his decision. Because trial judges are able to review the evidence and are closest to the case at trial, their findings of fact are accepted on appeal unless the appeals court finds that the those findings constitute an “clear error,” a deferential standard.
After detailing the evidence presented by the parties regarding the World Professional Association for Transgender Health (WPATH) Standards of Care and Endocrine Society’s guidelines for care, Moody — an Obama appointee who has been on the bench since 2014 — found as a fact: “Transgender care is not experimental care."
#Arkansas#Gender affirming care#Trans#Transgender#Lgbtqia#lgbtq youth#protect trans lives#protect trans youth
312 notes
·
View notes
Text
The 388-page report featured 32 recommendations on how transgender care should be conducted within NHS England. It incorrectly claims that there is “no good evidence” supporting transgender care and calls for restrictions on trans care for individuals under the age of 18, although it does not advocate for an outright ban. The report endorses the idea that being transgender may be caused by anxiety, depression, and OCD issues, despite the American Psychological Association, the largest psychological association in the world, rebutting this as lacking evidence. It also claims that transgender individuals can be “influenced” into being trans, a nod to the discredited theory of social contagion and rapid onset gender dysphoria, rejected by over 60 mental health organizations. Lastly, it seemingly endorses restrictions on transgender people under the age of 25, stating that they should not be allowed to progress into adult care clinics.
To support these recommendations, the report was released alongside “reviews” of the evidence surrounding transgender care, using these reviews to assert that there is "no good evidence" for gender-affirming care. A closer inspection of the reviews released alongside the Cass report reveals that 101 out of 103 studies on gender-affirming care were dismissed for not being of "sufficiently high quality," based on the Newcastle-Ottawa Scale—a subjective scale criticized for its flaws and potential unreliability due to a high risk of bias. This critique is particularly significant given the contentious political nature of the subject and connections between reviewers, Cass, and anti-trans organizations.
[...]
Immediately after the release of the Cass Review, experts in transgender healthcare from around the world voiced their opposition to its findings. Dr. Portia Predny, Vice President of the Australian Professional Association for Trans Health, criticized the findings and recommendations as “at odds with the current evidence base, expert consensus, and the majority of clinical guidelines worldwide.” Similarly, a statement from the Professional Association for Transgender Health Aotearoa condemned the review, noting, “The Review commissioned several systematic reviews into gender-affirming care by the University of York, but appears to have ignored a significant number of studies demonstrating the benefits of gender-affirming care. In one review, 101 out of 103 studies were dismissed.”
It is important to note that gender affirming care saves lives, and there is plenty of evidence to show for it. Numerous studies have demonstrated that gender-affirming care significantly reduces suicidality, with some showing a decrease in suicidality by up to 73%. A review compiled by Cornell University, which compiled over 50 journal articles on the topic, shows the efficacy of transgender care. These findings were echoed recently in an article published by the Journal of Adolescent Health, which found that puberty blockers dramatically lowered depression and anxiety. All of these studies and more have led to The Lancet, a medical journal with international acclaim, to publish a letter stating that gender affirming care is lifesaving preventative care. The largest and most influential medical organizations support trans care. A recent and historic policy resolution passed overwhelmingly by the American Psychological Association, the largest psychological organization in the world, states that gender affirming care is a medical necessity and that being trans is not “caused” by things like autism and PTSD.
48 notes
·
View notes
Text
The new hateful anti-transgender regulations of Missouri show us that it was never about the kids

New regulations make it practically impossible for transgender people to get gender affirming medical support in Missouri.
Republicans have for a long time covered their transphobia under concern for the kids. In accordance with this a lot of their anti-trans laws and regulations have been there to “protect the kids”.
For sure , the bathroom laws and the attacks on trans participation in sports have proven that their ultimate goal is to exclude trans people from society, but they could always hide behind the idea that trans people would still be allowed to be trans people.
Missouri directive proves that the end goal is the eradication of trans people
The new emergency regulations in Missouri prove beyond doubt that this is no longer the case. Sure, it presents a set of regulations that on paper contain some loopholes that might, theoretically, allow for sanctioned hormone replacement therapy and corrective surgery. Still, there are so many barriers that this is practically impossible.
The underlying logic is the old medical paradigm of gatekeeping (psychiatric therapy, long waiting periods, constant review ensuring that you are living up to the standards of a conservative society). However, they are taking this to a new level.
So, if you are suffering from anxiety and depression (most likely caused by transphobia), that would stop you from getting relevant health care. If they can document that you are affected by “social media addiction” or “social contagion”, that will be used against you. Following Transgender World is probably enough.
So this is really about stopping trans people from showing the world that they are trans. Trans people who have already transitioned can no longer get hormones in Missouri. They will have to detransition or move to a sane state.
Note that the Missouri attorney general issued this new state directive citing a consumer protection law normally used to prosecute fraudulent business practices. These regulations have not even been discussed by lawmakers.
Misleading presentations of science
In the regulations the Republicans have the audacity to cite the World Professional Association for Transgender Health in support of their policy. WPATH is totally against this kind of transphobia. The text is full of biased and selective misrepresentations of relevant research.
The Republicans try to make people believe that transitioning medically is a risky procedure. So keep in mind that the regret rate for trans people who have transitioned using hormones and surgery is less than 1 percent.
The use of puberty blockers is not “experimental”. Drugs in the class have been FDA approved since the 1990s to treat early puberty
Most of the negative findings associated with trans people is caused by lack of proper health care and the rhetoric of Republicans and other transphobes. The Republicans are basically creating the conditions that lead to the suffering they use as an excuse to persecute trans people.
These are the requirements of the transphobic regulations
Any person or health organization that provide a covered gender transition intervention to a patient will have to:
Assess (at least annually) whether the patient continues to have gender dysphoria.
Disclose conspicuously—on its website, physically in writing, and orally in person by the prescribing provider—to the patient and (if the patient is a minor) to the patient’s parents or legal guardians, [anti-trans propaganda arguments listed in the regulation].
Ensure that for at least the 3 most recent consecutive years, the patient has exhibited a medically documented, long-lasting, persistent and intense pattern of gender dysphoria.
Ensure that the patient has received a full psychological or psychiatric assessment, consisting of not fewer than 15 separate, hourly sessions (at least 10 of which must be with the same therapist) over the course of not fewer than 18 months to explore the developmental influences on the patient’s current gender identity and to determine, among other things, whether the person has any mental health comorbidities.
Ensure that any psychiatric symptoms from existing mental health comorbidities of the patient have been treated and resolved.
Ensure that the patient has received a comprehensive screening to determine whether the patient has autism.
Ensure that the patient has received a comprehensive screening (at least annually) for social media addiction or compulsion and has not, for at least the six months prior to beginning any intervention, suffered from social media addiction or compulsion.
Ensure (at least annually) that the patient is not experiencing social contagion with respect to the patient’s gender identity.
Track all adverse effects (both expected and unexpected) that arise from any course of covered gender transition intervention for all patients beginning the first day of intervention and continuing for a period of not fewer than 15 years.
Maintain data about adverse effects in a form that can be accessed readily for systematic study.
Obtain and keep on file informed written consent from the patient and (if the patient is a minor) from all parents or guardians who have authority to consent to medical intervention, as to each requirement [listed in this section of the regulation9. Such written consent shall be obtained for each intervention.
For medical personnel these restrictions are so wide that trying to help trans people will lead to a too high risk for legal persecution. We would guess this means an end of gender affirming medical healthcare in Missouri.
The rules take effect April 27.
Missouri rules part of rapid push to limit trans health care
Missouri to Restrict Medical Care for Transgender Adults, Citing Consumer Protection Law
Below, Video by the Young Turks on Missouri Attorney General Bans Gender-Affirming Care by "Emergency Rule"
youtube
Photo: Protester wearing a transgender pride flag at the Missouri State House. From the New York Times, Charlie Riedel, Associated Press
243 notes
·
View notes
Note
I am one of those 'kids who can't consent'. I can consent. But because of radfems allying with the conservative right, you are forcing me through irreparable changes. Every day I wake up and my body is more and more disgusting. But, because of you, I keep getting gaslit by GPs that I'm not trans, that I will learn to love my body, when the reality is it's wrong. Radfems do want to kill trans people, and they want kids to stay sexually available to them. I've lost count of the amount of lesbians telling me that I shouldn't "mutilate" my body because they lose out on another butch. You're disgusting and why I may be attracted to girls but will never date them.
Killing trans people is your end goal and that's why people think you're evil. 56% increase in hate crimes in the UK, thanks for that.
No, actually, you can't consent and if you don't understand the dangerous precedent this sets (for full grown adults with agendas to tell you can consent,) I'll explain it to you.
Within the trans community there's an idea that the sooner you can get a kid to transition, socially or medically, the sooner this can be seen as normal. The normalization of transitioning children is important, it pushes the idea that they could be born in the wrong body and normalizes the idea that a child knows what is medically best for them.
Child predators will try to find a way to have access to children by any means, now imagine how much easier it would be for them to have access to vulnerable children if they just claim to understand and support their gender identity issues.
The idea that children can consent would mean parents have no right over their children when it comes to their health and protections. I'm not saying children shouldn't speak up for themselves but we need to acknowledge that many children can be coached or groomed into saying or thinking things that may not benefit them or their safety.
The people that would love it for the law to 'recognize' that kids can consent doesn't stop at transgender rights advocates. It extends to pedophiles/child molesters that would love to get off the sex registry(something Jacob Breslow thinks it shouldn't exist to begin with) & pedophiles in position of power; informing and creating guidelines regarding childrens health & gender identity issues/transgenderism.
Pedophile sympathizer Jacob Breslow advocates for the rights of pedophiles, he thinks people are too mean to them. He thinks minors can consent too.
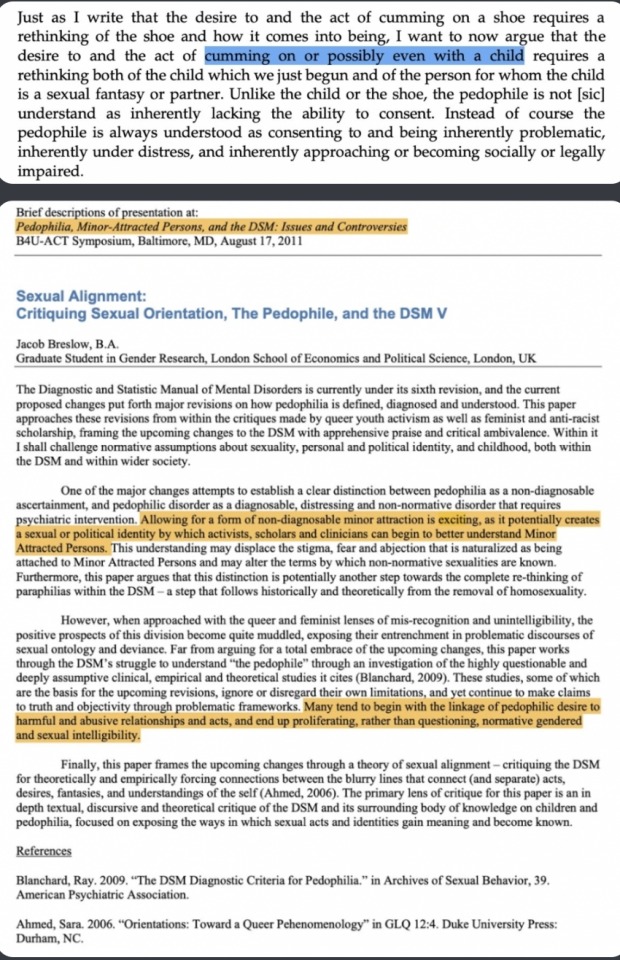
In his book Ambivalent Childhoods, Chapter 3 Desiring the Child: Queerness, Motherhood, and the Analyst, he writes:
[a description of a 12-year-old child dancing and mimicking sex acts to a crowd of adults.]
“As his movements transition from those that mimic break-dancers to those that mimic sex acts, repeating the easily citational gesticulations of pelvic thrusts … I find myself caught up in exhilarating waves of memory, identification, and desire … a desire for him himself,”
Why am I talking about Jacob Breslow? You should know him right? He was a Mermaids charity trustee until all of this came out, the pedophile sympathizing and all that.
Breslow also cited as an inspiration for his own writing Judith Levine’s 2002 book Harmful To Minors: The Perils Of Protecting Children From Sex in which she wrote that “sex is not in itself harmful to minors” and argued for the lowering of the age of consent to twelve.
He also was a guest speaker for a Pro-Pedophile B4U-ACT conference, an organization set up by a convicted child molester to destigmatize pedophiles and rebrand then as MAPs or Minor attracted person.
He's just one person tho, right? Not like there are more pedophile sympathizers in position of power when it comes to the transgender movement-
Anyways, all that to say;
Kids cannot consent because they don't have the cognitive or emotional maturity to understand long-term ramifications of such things.
>forcing irreparable changes
Going through puberty is normal. You've been convinced it's not but i promise you, you can still transition as soon as you turn 18 or whatever if that's what you want and you'll be fine.
Radfems don't align themselves with the conservative right but i can understand how you'd come to think that's what's happening when certain radfems talk on conservative platforms. I think there's a lack of understanding that they have no where else to speak on, especially when leftist first action is to label them as terfs and often don't give them the opportunity to have a conversation lest they be cancelled for even giving them the time of day.
Your body isn't disgusting. I'm sorry you feel that way and I'm sorry there are certain people that have convinced you to hate your body. I won't tell you you can learn to love yourself, it's taken me decades to learn to love myself and stop hating myself so much for things that happened to me that were out of my control and made me resent being a woman. Learning about radical feminism has definitely helped. I hope you can find something that will help you you as well that won't cause irreversible damage.
Radfems don't want to kill transpeople, I've already explained this in a different ask. Radfems don't want kids to be sexually available to them either, that's disgusting.
Hey, it sounds like you're dealing with a lot, including internalized homophobia, maybe some trauma. I truly hope you get an actual therapist that can listen and validate your concerns. My end goal isn't to kill transpeople tho I'd definitely would like to know where you're getting that from.
442 notes
·
View notes
Text

Mia Hughes: It's the part that enraged me the most. The way they talk about detransition. So, especially because you know that these are the very people who endlessly campaigned to remove all the guardrails. Gatekeeping is transphobic.
So, they did away with all the protections, they advocate for the most vulnerable people in society to be placed onto this reckless experimental medical conveyor belt. And then they do no follow up to see what became of them.
And then in the file you see them talking about detransitioners, just trivializing the experience, downplaying it, blaming the victim.
So, they will say things like, you know, detransitioners have to own and take responsibility for their decisions, especially if it's a permanent medical decision, completely oblivious to the fact that the blame lies entirely 100% on the doctors and the WPATH members who have done this to these vulnerable people.
They will say things like, you know, we need to frame, well, we've talked about the "gender journey." We need to frame detransition as another step on the "gender journey."
And they're all little activists as well. There's Marci Bowers is in there. He's the one who says you have to take responsibility. But then there's a whole bunch of little activists in there saying, we've got to find a way to allow people to make the decisions that they want to make but recognizing that gender is ever shifting and whatever.
And it's like, you're trying to do the impossible. You can't do that. You can't allow people to permanently alter their bodies while at the same time recognizing that gender is changeable and in a state of flux, the simply impossible.
And they've lost complete sight. Well, I don't think they can possibly see the harm. They see themselves as saving lives, on the right track, they're on the right side of history.
Because detransitioners create such cognitive dissonance, they absolutely have to deny that it happens. But when they come face to face with the fact that it does happen, they downplay it and trivialize it.
It makes me absolutely livid.
==
It's the same with any cult. You have to rationalize away and blame the apostates otherwise your ideology could be falsified.
#Mia Hughes#WPATH#The WPATH Files#WPATH Files#World Professional Association of Transgender Health#medical corruption#detrans#detransitioners#detransition#gender journey#gender identity ideology#gender ideology#queer theory#medical scandal#medical malpractice#cognitive dissonance#gender is fluid#genderfluid#medical mutilation#safeguarding#religion is a mental illness
9 notes
·
View notes
Text
Erin Reed at Erin In The Morning:
On Tuesday, Gov. Janet Mills of Maine signed LD 227, a sanctuary bill that protects transgender and abortion providers and patients from out-of-state prosecution, into law. With this action, Maine becomes the 16th state to explicitly protect transgender and abortion care in state law from prosecution. This follows several bomb threats targeting state legislators after social media attacks from far-right anti-trans influencers such as Riley Gaines and Chaya Raichik of Libs of TikTok. An earlier version of the bill failed in committee after similar attacks in January. Undeterred, Democrats reconvened and added additional protections to the bill before it was passed into law.
The law is extensive. It asserts that gender-affirming care and reproductive health care are "legal rights" in Maine. It states that criminal and civil actions against providers and patients are not enforceable if the provision or access to that care occurred within Maine’s borders, asserting jurisdiction over those matters. It bars cooperation with out-of-state subpoenas and arrest warrants for gender-affirming care and abortion that happen within the state. It even protects doctors who provide gender-affirming care and abortion from certain adverse actions by medical boards, malpractice insurance, and other regulating entities, shielding those providers from attempts to economically harm them through out-of-state legislation designed to dissuade them from providing care.
The bill also explicitly enshrines the World Professional Association of Transgender Health’s Standards of Care, which have been the target of right-wing disinformation campaigns, into state law for the coverage of transgender healthcare.
The bill is said to be necessary due to attempts to prosecute doctors and seek information from patients across state lines. In recent months, attorneys general in other states have attempted to obtain health care data on transgender patients who traveled to obtain care. According to the United States Senate Finance Committee, attorneys general in Tennessee, Indiana, Missouri, and Texas attempted to obtain detailed medical records "to terrorize transgender teens in their states… opening the door to criminalizing women’s private reproductive health care choices."
The most blatant of these attempts was from the Attorney General of Texas, who, according to the Senate Finance Committee, "sent demands to at least two non-Texas entities."
[...]
Despite these threats, legislators strengthened both the abortion and gender-affirming care provisions and pressed forward, passing the bill into law. Provisions found in the new bill include protecting people who "aid and assist" gender-affirming care and abortion, protections against court orders from other states for care obtained in Maine, and even protections against adverse actions by health insurance and malpractice insurance providers, which have been recent targets of out-of-state legislation aimed at financially discouraging doctors from providing gender-affirming care and abortion care even in states where it is legal.
Maine Gov. Janet Mills (D) signs gender-affirming care and abortion sanctuary state bill LD227 into law despite the best efforts of right-wing anti-trans extremists such as Riley Gaines, Courage Is A Habit, and Libs of TikTok who sought to thwart its passage and signature into law.
#Maine LD227#Maine#Janet Mills#Transgender Safe Refuge#Transgender Sanctuary State#Abortion Sanctuary State#Abortion#Gender Affirming Healthcare#LGBTQ+#Transgender Health#Transgender#WPATH
27 notes
·
View notes
Text
I'd rather be called a TERF than be someone who is ok with TQ+ organizations dedicated to minors without the commonsense approach of vetting the adults in the organizations or someone who pushes TQ+ studies without caring that the author is a pedo.
By Genevieve Gluck April 16, 2024
A gay couple who co-founded a Swiss LGBTQIA+ youth organization are being investigated by the public prosecutor after sexually exploiting two teenagers who were in their care. The men had created locations for their youth group, Sozialwerk.LGBT+, for children aged 13 and up in the city of Chur and in the municipality of Buchs, Switzerland.
While their identities were concealed by the press in Switzerland, Reduxx is naming the men involved as Holger Niggemann and his husband, Björn.
Holger, 42, is alleged to have had sexual contact with two 17-year-olds who had sought help for bullying with the organization. Holger was a board member of the group at the time, while his husband Björn was the business manager. The two men are said to have had a three-way sexual relationship with one of the teens, a 17-year old boy, according to a report by Tages-Anzeiger.
Numerous documents substantiate what happened in the group, including text messages, emails and voice messages, reports Tages-Anzeiger. Founded in 2020, Sozialwerk.LGBT has received public funding to set up facilities for at-risk youth as young as 13 who believe they are LGBT+.
During an investigation into the allegations, local media spoke to fifteen people close to the group to check the veracity of the allegations. The majority of those who came forward decided to remain anonymous.
One exception is Daniel Huber, a former board member of the association, who, with one other board member, reported the couple to public prosecutor Annina Grob, co-director of Avenir Social, the professional association for social work in Switzerland.
“For us, the behavior of the two is a total abuse of power, and the young people also felt that way. I brought it up again and again,” said Huber, who attended the meetings as a teenager before joining the board in a leadership role. “It is important not to look away from such behavior.”
According to statements from anonymous sources, the Niggemanns also took the 17 year-old boy on vacation to Germany with them.
See rest of article
By Genevieve Gluck April 13, 2024
Reduxx can reveal that a Dutch-American academic with a history of advocating for the normalization of adult-child sexual relationships has had a working relationship with the World Professional Association for Transgender Health (WPATH). Theodore Sandfort’s research has been presented at the organization’s symposium as recently as 2016.
Sandfort, a Columbia-affiliated academic and LGBT activist, previously worked with self-declared pedophiles in the Netherlands, documenting adult men’s sexual abuse of boys as evidence to support his theory that adult-child relationships are “predominantly positive.”
Prior to relocating to Columbia University, Sandfort received a PhD in Clinical Psychology from Utrecht University in the Netherlands. He was also the Chairman of the Interfaculty Department of Lesbian and Gay Studies at Utrecht University and Director of the Research Program “Diversity, Lifestyles and Health” at the Netherlands Institute of Social Sexological Research.
A faculty member at Columbia’s Mailman School of Public Health, Sandfort has also been employed as a Professor of Clinical Sociomedical Sciences, and worked at the university’s HIV Center alongside former WPATH president and Director of the institution’s Gender Identity Program, Walter Bockting. Like Sandfort, Bockting relocated to Columbia University from the Netherlands, having completed his doctoral degree in psychology from the Vrije Universiteit, Amsterdam.
Bockting and Sandfort also worked together in a professional capacity while acting as members of the editorial board for the academic journal Psychology and Sexuality in 2015.
The following year, in 2016, research co-authored by Sandfort was presented at a WPATH symposium in Amsterdam.
The paper, titled “Gender nonconformity and peer victimization: Sexual attraction and gender differences by age,” focused on the experiences of Dutch same-sex attracted adolescents aged 11 to 18. The study concluded that gender non-conforming youth were bullied by their peers, leading Sandfort and his colleagues to recommend that “key educational messages that address sexual and gender diversity should be delivered during childhood before early adolescence.”
However, Sandfort’s prior work dealt with sympathetic portrayals of pedophilic relationships between adult men and adolescent boys. In recent years, he has also had access to vulnerable youth in New York City’s foster care system, and, in 2020, he was dismissed from this position when his troubling research history dealing with the sexuality of children came to light.
In 1983, Sandfort authored an article for Youth and Society (Jeugd en Samenleving) titled “Erotic moments in working with children,” a small-scale study of sexual desires among five adult group leaders for the children in their care.
The men described deriving sexual pleasure from working with children, specifically when exercising together, bathing the children, or holding them on their laps. One man, identified as “Lex,” spoke of being aroused while “tickling” children aged “2 or 3,” wearing only his underwear, and proceeding to touch the toddlers’ genitals.
See rest of article
#Switzerland#Sozialwerk.LGBT+#Keep men away from minors#Publicly funded TQ+ organizations for minors#Netherlands#World Professional Association for Transgender Health (WPATH)#Theodore Sandfort#Netherlands Institute of Social Sexological Research
8 notes
·
View notes
Text
What are Radblr's thoughts about this? I'm on my way to take a test when this article popped up on my screen, and I wanted to post this before I leave, especially given that this is published by Scientific America. However, Im personally skeptically that "social contagion" doesn't play a factor at all; I wouldn't doubt it plays into this even a little bit. I'm sure everyone knows about articles posted in favor of this fad from, like, two years ago from even big names like Mermaids, who have either been proved wrong or backtracked.
I have pasted the article below. There are links in the original article.
----------------
Health Care
Evidence Undermines ‘Rapid Onset Gender Dysphoria’ Claims
Fears of “social contagion,” used to support anti-transgender legislation, are not supported by science
By Timmy Broderick on August 24, 2023
A recent study claiming to describe more than 1,600 possible cases of a “socially contagious syndrome” was retracted in June for failing to obtain ethics approval from an institutional review board. The survey examined “rapid-onset gender dysphoria,” a proposed condition that attributes adolescent gender distress to exposure to transgender people through friends or social media. The existence of such a syndrome has been the subject of intense debate for the past several years and has fueled arguments against transgender rights reforms, despite being widely criticized by medical experts.
The American Psychological Association and 61 other health care providers’ organizations signed a letter in 2021 denouncing the validity of rapid-onset gender dysphoria (ROGD) as a clinical diagnosis. And a steadily growing body of scientific evidence demonstrates that it does not reflect transgender adolescents’ experiences and that “social contagion” is not causing more young people to seek gender-affirming care. Still, the concept continues to be used to justify anti-trans legislation across the U.S.
“To even say it’s a hypothesis at this point, based on the paucity of research on this, I think is a real stretch,” says Eli Coleman, former president of the World Professional Association for Transgender Health. Coleman helped create the organization’s most recent standards of care for trans people, which endorse and explain the evidence for forms of gender-affirming care.
Many transgender people experience gender dysphoria, meaning that the gender that was assigned to them at birth and their gender identity don’t align, causing distress. ROGD was proposed as a gender dysphoria subtype in a 2018 paper by physician and researcher Lisa Littman, then at Brown University.* Littman’s survey asked parents of transgender adolescents—recruited predominantly from anti-transgender websites and forums—to describe their child’s “sudden or rapid onset of gender dysphoria” and to state if it coincided with increased social media usage or the child’s friends coming out as transgender.
Littman later issued a correction that updated the methodology, including a brief description of the websites and forums, and noted that ROGD is not a formal diagnosis. But the concept had already been taken upin books and podcasts—and by politicians—to promulgate the idea that peer pressure and social media are making kids transgender or that being transgender is a form of mental illness. As legislation targeting trans people has reached an all-time high in the U.S., ROGD’s alleged social contagion has been invoked by lawmakers in states such as Missouri, Utah and Arkansas to justify banning or restricting gender-affirming care for young people.
“This is just a fear-based concept that is not supported by studies,” says Marci Bowers, president of the World Professional Association for Transgender Health. The term ROGD is being used to “scare people or to scare legislators into voting for some of these restrictive policies that take away options for young people. It’s cruel, cruel legislation.”
Like the 2018 study that coined the term rapid-onset gender dysphoria, the recently retracted paper, which was published this March in Archives of Sexual Behavior, surveyed parents of transgender children about their children’s experiences. The study was co-authored by Michael Bailey, a psychologist at Northwestern University, and Suzanna Diaz, a pseudonym used by a mother of a child with gender dysphoria. Diaz is not affiliated with an institution and had already collected the survey data before collaborating with Bailey on the paper. The study was retracted because Diaz and Bailey did not get consent from the survey’s respondents to have their responses published, although Bailey disputes this. (Bailey declined to answer questions about the retraction from Scientific American.)
The participants in both the 2018 and the retracted 2023 studies were recruited from online communities that were explicitly critical about many aspects of gender-affirming care for transgender kids. Littman’s research was inspired in part by parents’ posts on these skeptical websites.
In response to criticisms that recruiting parents from anti-transgender websites may have biased the results, Littman says, “I reject the premise that parents who believe transition will harm their children are more likely to discredit their kids’ experiences than parents who believe that transition will help their children.”
Most experts cite the survey of parents rather than transgender children themselves as another major flaw in the methodology of both studies.
Diane Ehrensaft, director of mental health at the University of California, San Francisco, Child and Adolescent Gender Center, concurs. “To talk about what children are thinking, feeling and doing, particularly as they get old enough to have their own minds and narratives, you need to interview them,” she says.
Parents can often be the last to know about their child’s gender identity, Ehrensaft says. Coming out can be terrifying for many transgender kids. Family members often respond with violence or distrust or may even kick the child out of the house. Almost 40 percent of transgender youth experience homelessness or housing instability, according to a 2022 report from the Trevor Project, a nonprofit that provides crisis support for young LGBTQ+ people. Many kids who wait to discuss their gender identity with their parents before appearing to “suddenly” come out are simply keeping themselves safe, Ehrensaft says.
“It is not rapid-onset gender dysphoria,” she says. “It’s rapid-onset parental discovery.”
Many experts have also questioned what length of time qualifies as a “sudden” experience of gender dysphoria. Both the 2018 and 2023 studies left the definition up for parental interpretation. Complicating this, there isn’t one pathway or time line for being transgender, says Tey Meadow, a Columbia University sociologist who studies sexuality and gender. “For some people, it can evolve slowly. For others, it can evolve quickly,” she says.
For most transgender youth seeking gender-affirming care, considerable time elapses between when they realize they may be transgender and when they receive such care. A recent analysis of 10 Canadian medical centers in the Journal of Pediatrics found that 98.3 percent of young people seeking gender-affirming care had realized more than a year prior that they may have been transgender. “If ROGD were a real thing, we would expect to see two discernible streams of patients coming in [to receive care],” says Greta Bauer, a co-author of the study and director of the Eli Coleman Institute for Sexual and Gender Health at the University of Minnesota Medical School. There would be a distinct group of adolescents with more recent knowledge about their gender identity going to clinics and another group that had had such knowledge for years. “But we didn’t see that,” she says.
Thomas Steensma, a psychologist at Amsterdam University Medical Centers who provides gender-affirming therapy, says he has not seen evidence of the “social contagion” component of ROGD, and he cautions against even using these terms. “Rapid means out of control, and contagion signals a warning, and that warning induces fear,” he says. “There’s no evidence that certain developmental pathways are more problematic or less beneficial or helpful than others” for a child’s gender identity.
Steensma reports that he sees two “peaks” of referrals in his clinic: young adolescents and 15-year-olds. In a 2020 study Steensma and his colleagues looked at adolescent referrals from 2000 to 2016 and found no measurable difference in the psychological functioning or the intensity of the gender dysphoria between more recent referrals and those who came to the clinic starting in 2000. If adolescents are presenting with a different form of gender dysphoria, Steensma has not seen it.
The researchers did observe a change in their referral population in recent years, however. More kids assigned female at birth have been transitioning in recent years than those assigned male at birth. Many studies have captured this difference—including the 2018 survey proposing ROGD—but experts are unsure of its cause. Littman suggests that female-assigned kids are more susceptible to the “social contagion” of gender dysphoria because they feel social pressure more acutely than male-assigned kids. But Ehrensaft says nothing in the clinical literature corroborates this assertion. Instead she attributes this discrepancy to shifting cultural factors that influence how children express themselves and explore their identity. In our culture, Ehrensaft says, “there’s a lot more gender stress for the boy in the tutu than the girl in the football uniform.”
Other forms of gender incongruence, such as identifying as nonbinary or gender nonconforming, further challenge the idea that children should be forced to abide by traditional gender categories. And the best way to understand what kids are experiencing is to ask them questions and listen to their answers, Ehrensaft says.
“In some ways, [kids] are far more advanced than I am, as somebody in my 70s, about how they live and understand gender,” Ehrensaft adds. “So if we want to really understand gender, turn to the experts—and that would be the youth themselves.”
*Editor’s Note (8/24/23): This sentence was edited after posting to correct Lisa Littman’s occupation and her affiliation at the time of her 2018 paper.
#terfsafe#terfblr#radblr#radfems please touch#radfems interact#terfs please touch#terfs interact#radfem safe#radfemsafe
54 notes
·
View notes
Note
Hello 🌼 I was thanking about facial hair. I'm AFAB. I don't plan on going on T (and I heard it can make you grow facial hair naturally?) but I still would want to grow a beard, or a mustache perhaps, in the future. Would hair transplant help me with that or would my hight estrogen/ lower testosterone make it not work out?
Lee says:
For folks who are unfamiliar, a facial hair transplant involves taking hair from a donor site on your body (usually the back of the head) and transplanting it to your facial region.
It's a common procedure for individuals who cannot grow facial hair naturally or who have patchy beards, and a beard transplant is a viable option for people who do not want testosterone, or were not happy with the amount of facial hair they grew on testosterone.
Transplanted hair behaves like natural hair. Once it's transplanted, it will fall out initially and then start to grow back over the next few months, eventually growing like regular facial hair, even if you're not on testosterone.
AnotherPascal has posted about his beard transplant on Instagram and TransLife&Wife has posted about his on YouTube.
There's an article about beard transplants for trans folks called Facial Hair Transplantation for Transgender Patients: A Literature Review and Guidelines for Practice that was published in the Aesthetic Surgery Journal in 2021. I believe it's open access and I would highly encourage you to read the whole thing!
Like natural facial hair, transplanted hair may require regular trimming or shaving, depending on your desired look.
Testosterone & facial hair:
However, as you've heard, testosterone can indeed stimulate facial hair growth, which is why individuals who take testosterone (T) may experience increased facial hair over time.
You mentioned you do not plan on taking T, which is perfectly valid, but if you think there's a chance that you may change your mind in the future then I would consider waiting for the facial hair transplant until you're at least a couple of years on T because it can take time for your facial hair to fill in.
If you choose to not take T and just go straight for the transplant, having higher levels of estrogen won't necessarily negate the effects of a hair transplant. The transplanted hair is genetically programmed to grow in its new location.
In theory, the lack of testosterone might mean that the hair grows less densely or slowly than it might for someone with higher testosterone levels, but I don't think that's necessarily the case here because the follicles being transplanted are from the head so they'd behave more like head hair than beard hair.
Finding a Trans-Friendly Provider (for a facial hair transplant):
If you're considering a facial hair transplant, the first step is to consult a doctor specializing in hair restoration. They can assess your hair quality, discuss your expectations, and determine whether you're a good candidate for the procedure.
Referrals: Consider asking for referrals from local LGBTQ+ groups, transgender support groups, or healthcare providers known to be trans-friendly.
Consultations: Schedule consultations with potential surgeons. Use this opportunity to ask about their experience with transgender patients and facial hair transplants specifically.
Online Research: Look for reviews or testimonials online. Some websites are dedicated to reviewing medical professionals, and others are focused on the LGBTQ+ community.
Professional Organizations: Check if the surgeon is a member of professional organizations like the World Professional Association for Transgender Health (WPATH), which could indicate they're up-to-date on best practices for transgender healthcare.
Keep in mind that any surgical procedure comes with risks and costs. Ensure you're aware of these, and don't hesitate to seek a second opinion if you're unsure.
It might also be helpful to connect with others who have undergone similar procedures or are exploring similar options. Online communities, support groups, or LGBTQ+ centers can be great resources, but it isn't a very common procedure so you may have more look looking to cisgender men who have done similar things.
Facial hair transplants are often considered cosmetic procedures, which many insurance plans do not cover. However, coverage varies widely, so it's important to check with your insurance provider. It may be possible to appeal a denial for coverage by saying testosterone isn't indicated for you so this is a necessary treatment to resolve gender dysphoria etc.
If a procedure can be deemed medically necessary (for example, as part of gender-affirming treatment), insurance might cover it. A therapist might be able to help you make this case to your insurance company by writing a WPATH-style letter of support saying that you need it for Gender Dysphoria Reasons tm. It's also helpful if the office of the doctor doing the hair transplant writes a letter of medical necessity too.
Look for a surgeon who is board-certified in plastic surgery or dermatological surgery. This indicates they've met specific educational, training, and professional standards. It's also beneficial if the surgeon has experience with transgender patients, as they may be more attuned to your specific needs and goals, and may know how to get insurance to cover it.
It may seem obvious, but you have to make sure they have extensive experience with hair transplants, particularly facial hair transplants. Unfortunately some doctors are in it for the money and don't put patients first and/or think they're more capable than they are. To make sure they're up to the task, ask to see before and after photos of previous facial hair transplants they've performed, especially for patients with similar goals to yours.
And again, look for patient reviews or testimonials about their experiences with the surgeon. Pay particular attention to the experiences of trans individuals. I can't emphasize how important we are as a community-- we need to look out for each other and make sure that people don't see predatory providers!
Finally, it's crucial that you feel at least somewhat comfortable with the surgeon. They should treat you with respect, listen to your concerns, and provide thorough, honest answers to your questions. You don't need to be best buddies and they don't need a stellar personality either, but you need to feel like they're competent and that you are comfortable asking them questions about your care and could speak to them if you had complications.
While you wait for your consult, there is one alternative that you can try.
Minoxidil (Rogaine):
You can try minoxidil to increase your hair growth. A lot of people use minoxidil (rogaine) on their faces, and a few use it for body hair. It’s considered an “off-label” use- it’s officially approved for head hair and not other locations. Lots of medicines are used off-label, even prescriptions can be given off-label safely. Topical minoxidil is generally safe, as long as you use the dose recommended by the doctor/the bottle.
There's anecdotal evidence that minoxidil can stimulate new facial hair growth and may help thicken existing hairs. However, its effectiveness can vary, and there's limited scientific research on its use for facial hair specifically.
You can get it over-the-counter (aka without a prescription) online through Amazon or other sites, or at a pharmacy like CVS or Walgreens (it’s usually in the isle with men’s hair products like beard dye, and razors).
Minoxidil is generally safe but can cause side effects like dry skin, itching, and irritation. It's also a long-term commitment; you'll need to continue using it to maintain any new hair growth.
You shouldn’t use more than the recommended dose per day, no matter what body part it goes on (i.e. you shouldn’t cover your legs in it, unless you can stretch the normal dose that far). This is because minoxidil is a vasodilator, which lowers blood pressure. You also shouldn’t use oral minoxidil for hair growth because oral minoxidil is used primarily to lower blood pressure.
Will minoxidil (i.e., Rogaine) enhance my facial hair growth?
Using Minox for facial hair
Minox is deadly to some pets like cats and may cause hair growth in unusual places
A high concentration of minoxidil (like 12.5%) can cause low blood pressure
My Personal Experience with Minoxidil Pre-T
If you have some peach fuzz from Minox, dying your existing hair darker with facial hair dye might make it more obvious. This is also true for your body hair.
Will facial hair dye make my facial hair appear thicker/denser?
Remember, there's no one "right" way to be you. Whether through medical procedures, hormone therapy, or personal expression, what matters most is that you feel comfortable and authentic in your own skin. If you're sure that you don't want T, then maybe a facial hair transplant might be the right option for you!
Followers, anything to add?
#Lee says#facial hair transplant#testosterone#facial hair transplant without testosterone#beard transplant#hair transplant#surgery m
42 notes
·
View notes
Text
Medical professionals were aware of at least one case of cancer thought to be linked to a hormonal medication taken to aid gender transitioning, leaked documents from a worldwide transgender nonprofit organization suggest.
In a report released on Monday, the think tank Environmental Progress published hundreds of messages it said were from an internal forum of members of the World Professional Association for Transgender Health (WPATH), in which they discussed gender-affirming treatment and the complications that had arisen from particular cases.
The report comes amid a national debate on gender-affirming health care, as states across the U.S. have introduced legislation to limit treatment for young people who identify as transgender.
Among the messages is one, dated February 24, 2022, in which a person—identified by the report as a doctor—said a colleague developed hepatocarcinomas, or liver tumors, after eight to 10 years of taking testosterone.
"To the best of my knowledge, it was linked to his hormonal treatment," the message said. "Unfortunately I don't have much more details since it was so advanced that he opted for palliative care and died a couple months after."
Newsweek could not independently verify the authenticity of the messages, which appear in the report as screenshots and printouts, and many have names redacted.
When approached for comment, a WPATH spokesperson did not confirm the veracity of the messages, but said it "stand[s] opposed to individuals who misrepresent and de-legitimize the diverse identities and complex needs of this population through scare tactics."
A potential link between testosterone—which regulates pubic development, and which biological males produce naturally more than females—and liver cancer has been noted before.
A 2020 paper published in The Lancet detailed one case in which a 17-year-old transgender man developed liver tumors after taking testosterone. The patient was advised to stop taking testosterone, and the study said the relationship between the hormone and the tumor growth was unknown.
Another study, published in October, found cases in which transgender individuals receiving hormone therapies developed liver tumors, but it said the results were "not sufficient to conclude that there is an association" between the two.
Gender-affirming hormone therapies have also been linked to other forms of cancer—though research has so far been inconclusive.
A 2019 study of transgender adults in Amsterdam found there was an "increased risk of breast cancer in trans women" who had received hormone therapy compared to biological men.
However, last year, another study in the U.S. found that while there were signs of cellular changes with some hormone treatments, testosterone "does not appear to increase risk for breast cancer" and "additional studies are needed to investigate the mechanism responsible for these changes at a cellular level and its role in cancer development."
The message referring to a case of liver cancer was seemingly in response to an earlier one, posted in December 2021, detailing an instance of a 16-year-old patient who had developed hepatic adenomas, benign liver lesions, after being on testosterone for a little over a year and a synthetic form of progesterone.
Hepatic adenomas are rare, but they are associated with oral contraceptive pills and are seen in patients treated with anabolic steroids, according to the National Library of Medicine.
In the messages, the WPATH members discussed academic papers, asked for advice on issues surrounding gender-affirming care and shared their professional experiences. Environmental Progress said the leaks showed members appeared to be improvising treatments and, in some cases, spoke out against safeguarding requirements.
Michael Shellenberger, the president and founder of Environmental Progress, said in a statement that the leaks show that WPATH members "know that the so-called 'gender-affirming care' they provide can result in life-long complications and sterility and that their patients do not understand the implications."
While proponents of gender-affirming care say that such treatments help overcome gender dysphoria—and that barriers to treatment can worsen the mental health of those who feel they are trapped in the wrong body—opponents say that a rise in young people exhibiting gender dysphoria may be in part a product of wider mental health issues that should be identified and addressed before changing a person's body.
Dr. Marci Bowers, president of WPATH, told Newsweek in a statement that it "is and has always been a science- and evidence-based organization whose recommendations are widely endorsed by major medical organizations around the world.
"We are the professionals who best know the medical needs of trans and gender diverse individuals—and stand opposed to individuals who misrepresent and de-legitimize the diverse identities and complex needs of this population through scare tactics."
Bowers added: "Gender, like genitalia, is represented by diversity. The small percentage of the population that is trans or gender diverse deserves healthcare and will never be a threat to the global gender binary."
Update 3/6/24, 4:10 a.m. ET: This article was updated to include comment from Marci Bowers of WPATH.
14 notes
·
View notes
Text

In 2017 I interviewed Bernadette Wren, then head of psychology at the Tavistock Gids clinic, and asked what effect puberty blocking drugs have on the adolescent brain. Looking highly uncomfortable, she replied that the evidence so far was only anecdotal but that the clinic would study its patients “well into their adult lives so that we can see”.
Even back then, before whistleblowers had exposed the rush to medically transition children, it was alarming to hear that heavy-duty GnRH agonists such as triptorelin — used to treat advanced prostate cancer and “chemically castrate” sex offenders — were being prescribed to arrest puberty in hundreds of children as young as 11.
Moreover, they were being used “off-label” before any clinical trials. And the long-term study Wren promised never materialised: Gids (the Gender Identity Development Service) routinely lost touch with patients, and the 44 it did follow reported little long-term mental health improvement.
This shocking chapter in medical history, where the ideological objectives of trans rights campaigners trumped the welfare of disturbed children, is coming to an end worldwide. The decision by NHS England effectively to ban the prescription of puberty blockers comes after the Cass review noted these drugs could “permanently disrupt” brain development, reduce bone density and lock children into a regime of cross-sex hormones requiring life-long patienthood.
NHS England unites with other national health services including those in Finland, France, Sweden and, most notably, the Netherlands — where the “Dutch protocol”, a regime of early blockers then hormones, was devised in 1998 — in pulling back from prescribing them.
Even in the United States, where a toxic combination of extreme activism and medical capitalism has pushed child gender medicine to grotesque extremes, with double mastectomies performed on 14-year-old girls, there is some retrenchment.
Leaks from the World Professional Association for Transgender Health, the body which formulates guidance on “trans healthcare”, reveal doctors perplexed at how they should explain to an 11-year-old child that drugs will render them infertile. Crucially, liberal media such as The New York Times are now reporting grave medical misgivings about child transition, once dismissed as a culture-war issue for the Republican right.
Yet the question remains: how was this ever allowed to happen? For years, puberty blockers were cheerily billed as a mere “pause button”. In 2014, Dr Polly Carmichael, the last head of Gids before the Cass review ordered its closure, went on CBBC in a show called I Am Leo, saying of blockers: “The good thing is, if you stop the injections, it’s like pressing ‘start’ and the body carries on developing as it would if you hadn’t started.”
The BBC permitted her to make this unevidenced claim to an impressionable audience of six to 12-year-olds. Imagine hearing this as a developing girl, freaked out by your new breasts and periods. No wonder Gids referrals subsequently rocketed.
Carmichael failed to mention that she did not know if pressing “restart” on puberty is always medically possible — it is not — and in fact, almost every child Gids put on blockers went on to irreversible cross-sex hormones.
After years in a Peter Pan state while their peers developed, they understandably felt there was no way back and forged on with treatment. Yet if allowed to experience natural puberty, almost 85 per cent of gender dysphoria cases resolve themselves.
Nor did Carmichael tell CBBC kids that the blockers-hormones combination, if taken early enough, not only results in sterility but kills the libido so that a young person will never experience an orgasm.
At the 2020 judicial review brought by a former Tavistock clinician and Keira Bell, the brave young detransitioner rushed onto hormones by Gids, judges expressed astonishment at Gids’s lack of an evidence base.
Reporting on this issue for seven years, I too have been struck by a complete clinical incuriosity. Not only was data not collected, but those who queried treatments or pressed for evidence faced angry condemnation. Perhaps activists knew what research might find because one long-term Finnish study, recently reported in the BMJ, destroyed the myth used to justify blockers: that a child will commit suicide if denied them.
The Finns found that “gender-affirming care” does not make a dysphoric child less suicidal. Rather, such children had the same suicide risk as others with severe psychiatric issues. In other words, changing bodies does not fix troubled minds.
Yet even after NHS England’s announcement, activists refuse to heed the now-overwhelming evidence. In its response, Stonewall persists with the myth that puberty blockers “give a young person extra time to evaluate their next steps”.
Many questions remain unanswered: will private clinics still be permitted to prescribe puberty blockers; and is Scotland’s Sandyford child gender clinic still determined to close its ears to all evidence? Plus, we have few details on how the NHS’s new “holistic” treatment for gender-questioning children will operate when it opens next month.
This repellent experiment — in which girls who like trucks or little boys who dress as princesses, and who invariably grow up to be gay, are corralled inexorably down a road towards life-changing treatments — belongs in the book of medical disgraces. As do the cheerleaders who raised money for Mermaids and those who persecuted whistleblowers or damned journalists asking questions as transphobic.
In 50 years, chemically freezing the puberty of healthy children with troubled minds will be regarded with the same horrified fascination as lobotomies — which, never forget, won the Portuguese neurologist Antonio Egas Moniz the 1949 Nobel prize.
--------------------
{Article source (behind paywall)}
16 notes
·
View notes
Last Seen Blogs

mas-sin-menos
About someone

fuzzypalaceroadstudent
مِزنَه☁️
uninspired-choatic-angel
Uninspired Artist


viglantecandy18
Madam Red