#erin reed
Link
Rep. Zooey Zephyr, the first transgender woman elected to Montana's legislature, attended a Montana House of Representatives session to oppose an anti-transgender bill that would remove references to transgender individuals from more than 40 sections of state code. The bill, which would define sex in a way that excludes trans people, was one of over a dozen heard this year. The previous day, her strong speech against the gender affirming care ban the state had passed led to the Montana Freedom Caucus calling for her censure while intentionally and repeatedly misgendering her. When she punched in, they refused to recognize her to speak, and instead moved forward to pass the bill.
Tensions flared on the House Floor when the entire Democratic Caucus rose to demand that she be permitted to speak. In a strikingly undemocratic move, Republican House Speaker Regier declined to allow it, asserting that he could refuse to allow anyone to speak at his discretion. When Minority Leader Abbott objected, they moved to a packed rules committee meeting, which upheld the ruling. Following that, the Speaker stated it was his intent to no longer allow Representative Zephyr to speak moving forward.
#US Politics#Erin Reed#our current besiegement by theocratic fascists#transphobia#government-sanctioned hate#in support of an informed and engaged electorate
11K notes
·
View notes
Text
1K notes
·
View notes
Text
Critics are saying a new bill introduced into the Texas Legislature this year will only encourage a bounty-hunting trend that targets drag queens and transgender people. Texas state GOP Rep. Steve Toth filed House Bill 4378 on Thursday, March 9 that will allow anyone in Texas to sue people who perform in drag or host a drag performance where children are present.
The bill targets events like family-friendly brunch shows at restaurants or drag queen story time events at libraries or other family-oriented drag queen events. The bill says that people who sue a person or venue can be awarded $5,000 in damages.
Erin Reed, a transgender rights activist and independent reporter, tweeted about HB 4378 on Saturday, March 11, saying that the piece of legislation could easily be used to target transgender people who perform.
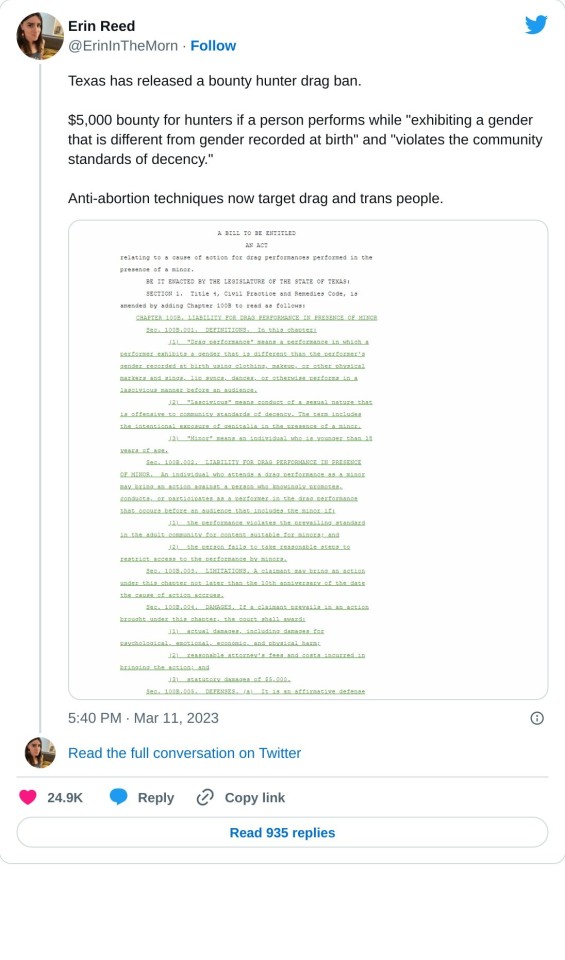
The bill defines drag as "a performance in which a performer exhibits a gender that is different than the performer’s gender recorded at birth." It goes on to say this performance can involve using makeup and clothing to dance, lip sync, or perform "in a lascivious manner."

The bill joins 17 other proposed pieces of Texas legislation that targets transgender people, drag queens, and the LGBTQ+ community. The Advocate reported in November 2022 that Texas legislators have proposed anti-LGBTQ+ bills for the upcoming legislative session. This now includes HB 4378 and the recent heterosexual tax cut bill from state Rep. Bryan Slaton.
That proposed bill would provide massive tax cuts, up to 100%, for straight families that stay married and have children. Slaton also pushed a bill that would have outlawed minors at drag shows.
#us politics#news#my san antonio#texas#2023#Texas Legislature#transphobia#trans rights#transgender pride#transgender#lgbtqia+ rights#lgbtqia+#House Bill 4378#Steve Toth#drag queen show#drag queen story hour#drag queens#drag#erin reed#@erininthemorn#tweet#twitter#republicans#conservatives#gop#gop policy#The Advocate#heterosexual tax cut#Bryan Slaton
4K notes
·
View notes
Text

Erin Reed
Gender: Transgender woman
Sexuality: Queer
DOB: Born 1988
Ethnicity: White - American
Occupation: Journalist, activist
#Erin Reed#queerness#trans femme#trans rights#lgbt rights#transgender#trans woman#queer#1988#white#journalist#activist#popular#popular post
182 notes
·
View notes
Text

Following publication of the final report there have been a number of questions and points for clarification about the findings and recommendations. We have collated those questions, along with our answers, on this page.
-
Did the Review set a higher bar for evidence than would normally be expected?
No, the approach to the assessment of study quality was the same as would be applied to other areas of clinical practice – the bar was not set higher for this Review.
Clarification:
The same level of rigour should be expected when looking at the best treatment approaches for this population as for any other population so as not to perpetuate the disadvantaged position this group have been placed in when looking for information on treatment options.
The systematic reviews undertaken by the University of York as part of the Review’s independent research programme are the largest and most comprehensive to date. They looked at 237 papers from 18 countries, providing information on a total of 113,269 children and adolescents.
All of the University of York’s systematic review research papers were subject to peer review, a cornerstone of academic rigour and integrity to ensure that the methods, findings, and interpretation of the findings met the highest standards of quality, validity and impartiality.
-
Did the Review reject studies that were not double blind randomised control trials in its systematic review of evidence for puberty blockers and masculinising / feminising hormones?
No. There were no randomised control studies identified in the systematic reviews, but other types of studies were included if they were well designed and conducted.
Clarification:
The Review commissioned the University of York to undertake an independent research programme to ensure the work of the Review and its recommendations were informed by the most robust existing evidence. This included a series of systematic reviews which brought together, analysed and evaluated existing evidence on a range of issues relating to the care of gender-questioning children and young people, including epidemiology, treatment approaches and international models of current practice.
Randomised control trials are considered the gold standard in relation to research, but there are many other study designs that can give valuable information. Explanatory Box 1 (pages 49-51 of the final report) discusses in more detail the different kinds of studies that can be used, and how to decide if a study is poorly designed or biased.
Blinding is a separate issue. It means that either the patient or the researcher does not know if the patient is getting an active treatment or a ‘control’ (which might be another treatment or a placebo). Patients cannot be blinded as to whether or not they are receiving puberty blockers or masculinising / feminising hormones, because the effects would rapidly become obvious. Good RCTs can be conducted without blinding.
The University of York’s systematic review search did not identify any RCTs, blinded or otherwise, but many other studies were included. Most of the studies included were called ‘cohort studies’. Well-designed and executed high quality cohort studies are used in other areas of medicine, and the bar was not set higher for this review; even so the quality of the studies was mostly only assessed as moderate.
-
Did the Review reject 98% of papers demonstrating the benefits of affirmative care?
No. Studies were identified for inclusion in the synthesis (conclusions) of the systematic reviews on puberty blockers and masculinising/feminising hormones on the basis of their quality. This was assessed using a standard quality assessment tool appropriate to the types of study identified. All high quality and moderate quality reviews were included in the synthesis of results. This totalled 58% of the 103 papers.
Clarification:
The Newcastle-Ottawa scale (a standard appraisal tool) was used to compare the studies. This scores items such as participant selection, comparability of groups (how alike they are), the outcomes of the studies and how these were assessed (data provided and whether it is representative of those studied). High quality studies (scoring >75%) would score well on most of these items; moderate quality studies (scoring >50% – 75%) would miss some elements (which could affect outcomes); and low-quality studies would score 50% or less on the items the scale looked at. A major weakness of the studies was that they did not have adequate follow-up – in many cases they did not follow young people for long enough for the long-term outcomes to be understood.
Because the ranking was based on how the studies were undertaken (their quality and execution), low quality research was removed before the results were analysed as the findings could not be completely trusted. Had an RCT been available it would also have been excluded from the systematic review if it was deemed to be of poor quality.
The puberty blocker systematic review included 50 studies. One was high quality, 25 were moderate quality and 24 were low quality. The systematic review of masculinising/feminising hormones included 53 studies. One was high quality, 33 were moderate quality and 19 were low quality.
All high quality and moderate quality reviews were included, however as only two of the studies across these two systematic reviews were identified as being of high quality, this has been misinterpreted by some to mean that only two studies were considered and the rest were discarded. In reality, conclusions were based on the high quality and moderate quality studies (i.e. 58% of the total studies based on the quality assessment). More information about this process in included in Box 2 (pages 54-56 of the final report)
-
Has the Review recommended that no one should transition before the age of 25 and that Gillick competence should be overturned.
No. The Review has not commented on the use of masculinising/feminising hormones on people over the age of 18. This is outside of the scope of the Review. The Review has not stated that Gillick competence should be overturned.
The Review has recommended that:
“NHS England should ensure that each Regional Centre has a follow through service for 17-25-year-olds; either by extending the range of the regional children and young people’s service or through linked services, to ensure continuity of care and support at a potentially vulnerable stage in their journey. This will also allow clinical, and research follow-up data to be collected.”
This recommendation only relates to people referred into the children and young people’s service before the age of 17 to enable their care to be continued within the follow-through service up to the age of 25.
Clarification:
Currently, young people are discharged from the young people’s service at the age of 17, often to an adult gender clinic. Some of these young people have been receiving direct care from the NHS gender service (GIDS as was) and others have not yet reached the top of the waiting list and have “aged out” of the young people’s service before being seen.
The Review understands that this is a particularly vulnerable time for young people. A follow-through service continuing up to age 25, would remove the need for transition (that is, transfer) to adult services and support continuity of care and continued access to a broader multi-disciplinary team. This would be consistent with other service areas supporting young people that are selectively moving to a ‘0-25 years’ service to improve continuity of care.
The follow-through service would also benefit those seeking support from adult gender services, as these young people would not be added to the waiting list for adult services and, in the longer-term, as more gender services are established, capacity of adult provision across the country would be increased.
People aged 18 and over, who had not been referred to the NHS children and young people’s gender service, would still be referred directly to adult clinics.
-
Is the Review recommending that puberty blockers should be banned?
No. Puberty blocker medications are used to address a number of different conditions. The Review has considered the evidence in relation to safety and efficacy (clinical benefit) of the medications for use in young people with gender incongruence/gender dysphoria.
The Review found that not enough is known about the longer-term impacts of puberty blockers for children and young people with gender incongruence to know whether they are safe or not, nor which children might benefit from their use.
Ahead of publication of the final report NHS England took the decision to stop the routine use of puberty blockers for gender incongruence / gender dysphoria in children. NHS England and National Institute for Health and Care Research (NIHR) are establishing a clinical trial to ensure the effects of puberty blockers can be safely monitored. Within this trial, puberty blockers will be available for children with gender incongruence/ dysphoria where there is clinical agreement that the individual may benefit from taking them.
Clarification:
Puberty blockers have been used to suppress puberty in children and young people who start puberty much too early (precocious puberty). They have undergone extensive testing for use in precocious puberty (a very different indication from use in gender dysphoria) and have met strict safety requirements to be approved for this condition. This is because the puberty blockers are suppressing hormone levels that are abnormally high for the age of the child.
This is different to stopping the normal surge of hormones that occur in puberty. Pubertal hormones are needed for psychological, psychosexual and brain development, and there is not yet enough information on the risks of stopping the influence of pubertal hormones at this critical life stage.
When deciding if certain treatments should be routinely available through the NHS it is not enough to demonstrate that a medication doesn’t cause harm, it needs to be demonstrated that it will deliver clinical benefit in a defined group of patients.
Over the past few years, the most common age that young people have been receiving puberty blockers in England has been 15 when most young people are already well advanced in their puberty. The new services will be looking at the best approaches to support young people through this period when they are still making decisions about longer-term options.
-
Has the Review recommended that social transition should only be undertaken under medical guidance?
The Review has advised that a more cautious approach around social transition needs to be taken for pre-pubertal children than for adolescents and has recommended that:
“When families/carers are making decisions about social transition of pre-pubertal children, services should ensure that they can be seen as early as possible by a clinical professional with relevant experience.”
Parents are encouraged to seek clinical help and advice in deciding how to support a child with gender incongruence and should be prioritised on the waiting list for early consultation on this issue. This should include discussion of the risks and benefits and the voice of the child should be heard. It will be important that flexibility is maintained, and options remain open.
Clarification:
Although the University of York’s systematic review found that there is no clear evidence that social transition in childhood has positive or negative mental health outcomes, there are studies demonstrating that for a majority of young children presenting with gender incongruence, this resolves through puberty. There is also evidence from studies of young people with differences of sex development (DSD) that sex of rearing seems to have some influence on eventual gender outcome, and it is possible that social transition in childhood may change the trajectory of gender identity development for children with early gender incongruence. Living in stealth from early childhood may also lead to stress, particularly as puberty approaches.
There is relatively weak evidence for any effect of social transition in adolescence. The Review recognises that for adolescents, exploration is a normal process, and rigid binary gender stereotypes can be unhelpful. Many adolescents will go through a period of gender non-conformity in terms of outward expressions (e.g. hairstyle, make-up, clothing and behaviours). They also have greater agency in how they present themselves and in their decision-making.
Young people and young adults have spoken positively about how social transition helped to reduce their gender dysphoria and feel more comfortable in themselves. They identified that space to talk about socially transitioning and how to handle conversations with parents/carers and others would be helpful. The Review has therefore advised that it is important to try and ensure that those already actively involved in the young person’s welfare provide support in decision making and that plans are in place to ensure that the young person is protected from bullying and has a trusted source of support.
Further detail can be found in Chapter 12 of the Final Report.
-
Did the Review speak to any gender-questioning and trans people when developing its recommendations?
Yes, the Review has been underpinned by an extensive programme of proactive engagement, which is described in Chapter 1 of the report. The Review has met with over 1000 individuals and organisations across the breadth of opinion on this subject but prioritised two categories of stakeholders:
People with relevant lived experience (direct or as a parent/carer) and organisations working with LGBTQ+ children and young people generally.
Clinicians and other relevant professionals with experience of and/ or responsibility for providing care and support to children and young people within specialist gender services and beyond.
A mixed-methods approach was taken, which included weekly listening sessions with people with lived experience, 6-weekly meetings with support and advocacy groups throughout the course of the Review, and focus groups with young people and young adults.
Reports from the focus groups with young people with lived experience are published on the Review’s website and the learning from these sessions and the listening sessions are represented in the final report.
The Review also commissioned qualitative research from the University of York, who conducted interviews with young people, young adults, parents and clinicians. A summary of the findings from this research is included as appendix 3 of the final report.
-
What is the Review’s position on conversion therapy?
Whilst the Review’s terms of reference do not include consideration of the proposed legislation to ban conversion practices, it believes that no LGBTQ+ group should be subjected to conversion practice. It also maintains the position that children and young people with gender dysphoria may have a range of complex psychosocial challenges and/or mental health problems impacting on their gender-related distress. Exploration of these issues is essential to provide diagnosis, clinical support and appropriate intervention.
The intent of psychological intervention is not to change the person’s perception of who they are but to work with them to explore their concerns and experiences and help alleviate their distress, regardless of whether they pursue a medical pathway or not. It is harmful to equate this approach to conversion therapy as it may prevent young people from getting the emotional support they deserve and make clinicians fearful of providing this group of children and young people the same care as is afforded to other children and young people.
No formal science-based training in psychotherapy, psychology or psychiatry teaches or advocates conversion therapy. If an individual were to carry out such practices they would be acting outside of professional guidance, and this would be a matter for the relevant regulator.
==
Like any religious fanatics, pathological liars like "Erin" Reed and "Alejandra" Carballo still won't stop lying, since it's all they have. But their disciples should really be noticing how they've been directly refuted.
#Cass review#Cass report#Hilary Cass#Dr. Hilary Cass#disinformation#misinformation#pathological liars#Erin Reed#Alejandra Carabello#Michael Hobbes#medical scandal#medical corruption#medical malpractice#gender affirming care#gender affirming healthcare#gender affirmation#compulsive liars#gender fanatics#gender cult#gender ideology#gender identity ideology#queer theory#intersectional feminism#puberty blockers#cross sex hormones#wrong sex hormones#religion is a mental illness
55 notes
·
View notes
Text
Fact Check: Fact Check: 216 Instances Of Factual Errors Found In Right-Wing "WPATH Files" Document

In response to the WPATH files being dropped, transgender activist Erin Reed made a response, fact checking the claims made in the editorial of the original document, written by Mia Hughes. Reed claims that there are 216 “instances of factual inaccuracies, erroneous citations, misinterpretations of what is “leaked,” and purposeful omissions contradicting the authors central editorialized claims.”
The introduction is spent discrediting the organizations involved as “right wing” and “anti trans.” Reed alleges that the quick rate at which the files were spread was a “coordinated and organized embargo campaign, leaving those in support of care with scant time to review the voluminous documents and respond.”
The first claim that Reed alleges to be false is the claim that the Beyond WPATH declaration was signed by many people who were not doctors, pointing out signatures with occupations such as “DJ” and “yoga instructor” as well as comments like “concerned parent.” The original document does not claim that all signatures were from doctors, with the exact quote stating that it was “now signed by over 2,000 concerned individuals, many of whom are clinicians working with gender diverse young people.” (bold text mine). Nowhere does it imply that only doctors were able to sign it, it simply acknowledges that many people who signed the petition were doctors. One important thing to note is that the creator of the petition, Dr. Joseph Burgo, alleges that the petition was hijacked by trans activists adding fake signatures. (timestamp: 16 min)
Here is a screenshot of the top signers of the petition. Highlighted are all medical professionals.

Note that one of the signers, Stephen B. Levine, was a former president of WPATH who left due to the organization becoming less evidence based and more focused on activists.
Next, Reed criticizes the quality of the citations, stating, "When addressing supposedly "scientific" citations, the report's performance is equally lacking." One example given is an article from The Guardian from 2004, and another being “a conservative site called "The New Atlantis, " Upon visiting the link to the New Atlantis’s “about” page, they explicitly state they are a nonpartisan organization. That being said, other sources do allege this particular publication is right wing. However, this attempt to frame any opposing source as "right wing" or "conservative" is a significant part of Reed's argument on why the information is unreliable.
Reed accuses many of the studies cited to be misrepresented. One study cited in the WPATH files is a Swedish study which is quoted as finding, “rates of completed suicide post-surgical transition to be greatly elevated over the general population.”
Reed links to an article from a site called Trans Advocate, which contains an interview with the author of the Swedish study on how her work has been misinterpreted. In this article, the study is quoted as saying, “no inferences can be drawn as to the effectiveness of sex reassignment as a treatment for transsexualism. In other words, the results should not be interpreted such as sex reassignment per se increases morbidity and mortality.” The study does not conclude that sex reassignment surgery works, but there is also no reason to suggest it causes people to be more suicidal than they were pre-transition. Hughes does imply that suicide risk can increase after transition in cases where certain mental health conditions such as BPD are left untreated, and the patient comes to regret transition later, but this is not cited as scientific fact (42).
On the page before the Swedish study is referenced (42), Hughes discusses the mental health issues commonly found in trans-identified youth and how those issues may account for the higher rate of suicidality. Reed fails to acknowledge the Amsterdam study that concluded “the suicide risk in transgender people is higher than in the general population and seems to occur at every stage of transitioning.” While some parts of the Swedish study may have been misinterpreted, there are other studies with similar findings. The point is not that suicidality increases after transition, but rather that there is little evidence to suggest that transition has a long-term benefit on a person's other mental health issues.
Reed links to three studies disputing both the 2009 study and the Swedish study, implying that all of this “much newer research from peer-reviewed articles,” completely invalidates the findings of the other studies. The first study that Reed gives as a rebuttal does not actually come to the conclusion that there is a “substantial improvement in the quality of life for transgender individuals.” This 2017 study concludes that, “Our results show that transgender women generally have a lower QoL compared to the general population. GRS leads to an improvement in general well-being as a trend but over the long-term, QoL decreases slightly in line with that of the comparison group.” Basically, it claims that quality of life increases shortly after surgery, but later declines after about 5 years. They acknowledge that this is the case in the general population as well, and they state that there is still little consensus on trans identified people’s quality of life.
The second study Reed cites looks at the quality of life of patients who have received phalloplasties. Only 32 patients were part of this study, and they found that “88% of our patients were very satisfied with the aesthetic result, 75% have had sex after surgery, and 72% were very satisfied with sexual function after GAS. Eighty-one percent had a strong improvement of QOL, and 91% would undergo the same treatment again.” However, there is more evidence that phalloplasty is a dangerous procedure, and Reed fails to acknowledge any of those studies, such as this study of 1731 phalloplasty patients, finding that the "Overall complication rate was high at 76.5%"
The third study was a survey of 27,715 trans identified adults from 2015. The introduction of the study admits that “Mental health effects of gender-affirming surgery thus remain controversial.” In this survey, only 25% of participants had undergone surgery. This study was only a secondary analysis of these survey responses, comparing results of those who did not undergo surgery with those who had.
Reed implies that the 2% fatality rate of the vaginoplasty performed on males who had previously been on puberty blockers is irrelevant because the death “occurred from a wound infection, a potential complication for any surgery.” Hughes acknowledges that the patient died of necrotizing fasciitis, (19) and the case report that Reed links states that the patient, “developed septic shock and multiple organ failure on the basis of an extended-spectrum β-lactamase-producing Escherichia coli. A severe progression of the necrotizing fasciitis was lethal, despite repeated surgical debridement, intravenous antibiotic use, and supportive care at the intensive care unit.” The study that Reed then links to prove this treatment is successful contains extremely graphic images detailing the surgery without any warning. This does not discredit the study, but for that reason I cannot really look at it.
Reed attempts to debunk the accusation that those who took puberty blockers cannot orgasm, by alluding to there being two studies disproving this. However, it appears that Reed linked the same study twice within this quote, "To ensure factual accuracy, studies have shown that those who took puberty blockers are capable of orgasm" Only the abstract is available to me for this study. Because this study is behind a paywall, it is difficult for me to verify Reed’s claims about their results. The study is a survey of group of 31 primary total laparoscopic intestinal vaginoplasty patients, and is a survey about general quality of life one year after the surgery. It states that the group was “relatively young,” and states that the, “median age at time of surgery = 19.1 years, range = 18.3–45.0.” However, it gives no indication of when the patients began transition. It does imply that patients were on "Puberty-suppressing hormonal treatment”, but does not make any mention of when the patients started puberty blockers. Marci Bowers, head of WPATH, has explicitly stated that “I’m unaware of an individual claiming ability to orgasm when they were blocked at Tanner Stage 2.” Tanner Stage 2 is around the age of 11. It is possible these patients began blockers later on, but that evidence is not available to me either way. Another important thing to note is that the conclusion of the second study states, “This group of relatively young transgender women reported satisfactory functional and esthetic results of the neovagina and a good quality of life, despite low Female Sexual Function Index scores.” (bold text mine) “The mean Female Sexual Function Index total score of sexually active transgender women was 26.0 ± 6.8.”
This study is a survey relying on patients to self report their satisfaction, and Hughes does acknowledge the flaws of self reported studies on page 33, stating that measurable studies showed less positive results than surveys. Many of the studies Reed cites as rebuttals rely on self report.
Finally, Reed criticizes the idea that gender dysphoric youth would eventually desist post-puberty. One of the links provided as evidence against this claim leads to another article of Reed's. The criticism of Kenneth Zucker's research from the 90s appears to be that it classifies children with "gender identity disorder" as those who are simply gender non-conforming. The article uses this graphic to illustrate the difference between gender identity disorder and the current DSM-5 diagnosis of gender dysphoria, implying that the latter has stricter requirements.

Reed dismisses any correlation between social transition and desistance rates and accuses Hughes of implying that, “social transition prevents this “natural” desistance, a hypothesis that has not been validated.” While there may have been some flaws in Zunker's original study, this massive difference between then and now certainly raises questions on how the impact of social transition affects a child.
In the next section, Reed claims that the “leaked material” is frequently misrepresented, yet only provides three examples of this occurring. It does appear that Hughes left out the part about the orgasm in the first example, which would have been important context to include (28). In the second example, Reed accuses Hughes of leaving out the fact that it was a detransitioner who used the phrase “gender journey” and not a clinician. In reality, Hughes does not specify who said this, simply stating “There is talk about detransition being just another step in a patient’s “gender journey.” (31) However, we only have the clinicians word to go off to prove that the patient used that phrase, and there is evidence of another clinician pushing patients to identify with their language. This doctor decided to label a patient as “eunuch identified,” despite him not claiming that label himself (51). The third example of a misrepresentation consists of a patient developing a hepatic adenoma (liver mass) after taking testosterone. Reed is correct that hepatic adenomas are benign and that they are linked to both contraceptives and hormones. However, Reed accuses the document of leaving out the fact that the patient was on both oral contraceptives and testosterone. Hughes does in fact state that the patient was on norethindrone acetate, which is a contraceptive. In the WPATH document, the doctor specifically suspects that the hormones are the cause of the liver masses as opposed to the contraceptive.
Reed alleges that Stella O’Malley and Genspect “teased a young trans girl testifying in front of a school board.” The linked tweet reads: “US-UTAH: 11 yr old “Alison” came out as trans at 8 after having a vision of wearing a long white dress in a field. Dad says his “daughter” must be “validated in who she is” & allowed to use girls spaces bc many trans-identified people consider suicide.”
Overall, Reed’s fact checking only provides a few examples, nowhere near the 216 claimed. Many of the studies linked as rebuttals do not come to the same conclusions as Reed implies. In my opinion, it appears that Reed did not expect the audience of this article to go and read the WPATH files for themselves, or for that matter, even check the links thoroughly. The few good points that are made here do not discredit the entirety of the report, and Reed fails to address the main claims in the report; such as WPATH members admitting that children do not have the capacity to consent, their disregard of proper scientific protocol, the experimental approach to healthcare, disregard of patients' other mental health issues, and lack of ethics.
If anyone wants to add things to this or expand on anything, please feel free to do so. There were a couple sections where my understanding was a bit limited, such as the limitations of the trans youth desistance study, and the puberty blockers/vaginoplasty study.
Edit: Moving this disclaimer down here because a TRA quit reading immediately after they saw this. I would like to acknowledge that I am not a doctor or any type of medical professional (neither is Reed) and some scientific studies may be difficult for me to interpret.
Edit 2: Removed the part about the New Atlantis because I have seen mixed info on it's political leanings.
#wpath#wpath files#transgender#trans#gender critical#erin reed#terfblr#radfem#radical feminism#radical feminists do interact#trans activism
68 notes
·
View notes
Text

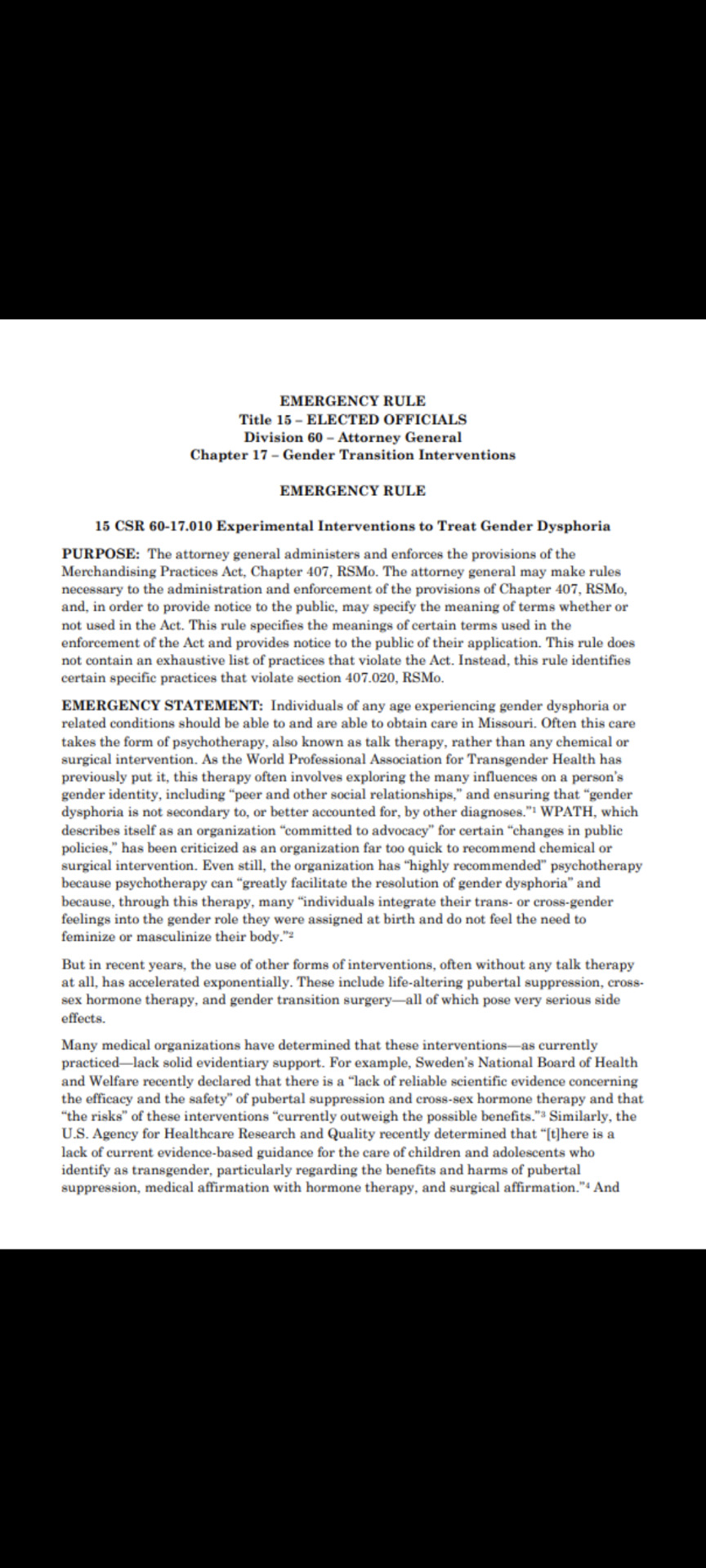





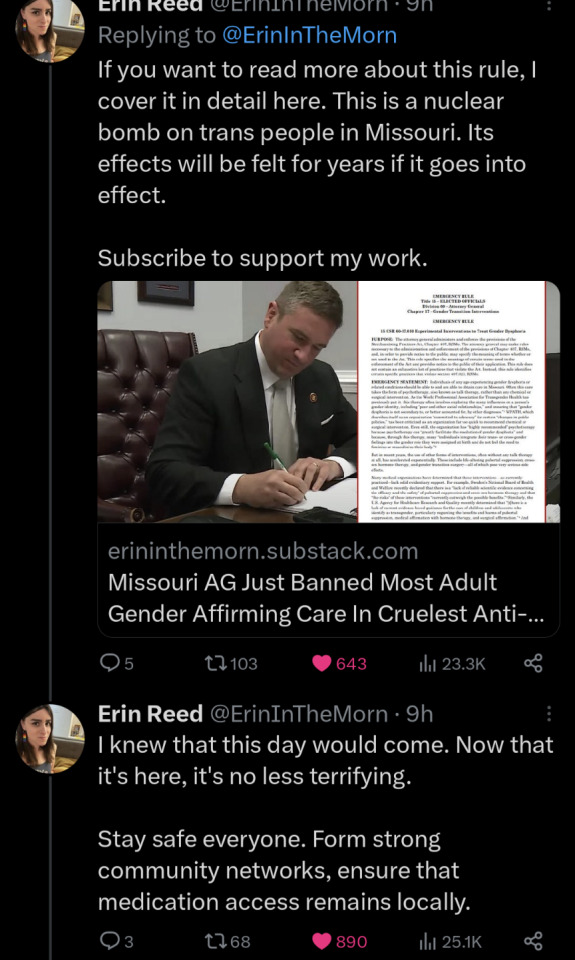
The vile transphobic cult told us it was STRICTLY about not wanting kids being trans. No. It never was. Republicans, conservatives, TERF's, and Neo-Nazis all want to genocide trans people through legislation aka mass transgender violence. This was never about the kids. Stay safe, get armed, and be prepared to have trans refugees.
source | Erin in the Morning Substack | Bill
#trans rights#transgender#Missouri#erin reed#erin in the morning#lgbtq#lgbtq rights#trans rights are human rights#protect trans lives#protect trans kids#trans lives matter#fuck transphobes#fuck transphobia#fuck terfs#terfs are fascists#terfs are rightwing#terfs are white supremacists#trans women are valid#trans men are valid#anti trans bills#legislation#fuck fascism#antifascist action#republicans are evil#fuck republicans#trans adults#trans youth#human rights#trans genocide#genocide
211 notes
·
View notes
Text
#us politics#anti trans bills#twitter#representative government my ass#erin reed#erin in the morning#4th of july
86 notes
·
View notes
Text


When I saw Zooey Zephyr proposed to her girlfriend Erin Reed...well, my week got a bit better.
Congrats to the couple 👭
131 notes
·
View notes
Text
At midnight on Saturday, more than 20 anti-LGBTQ+ bills died in West Virginia after the legislature adjourned sine die. Bills that did not pass included the misleadingly named "Women’s Bill of Rights," which would have ended legal recognition for transgender people in the state, as well as a bill that would have prohibited gender-affirming care for all transgender youth. West Virginia is the second state in a week hinting that anti-transgender legislative attacks are encountering resistance. Last week, Florida's legislature also adjourned, effectively killing dozens of anti-transgender bills.
One bill that failed to pass as the West Virginia legislature adjourned was House Bill 5243, also known as the misleadingly-named "Women’s Bill of Rights" by its proponents. The bill primarily aimed to exclude transgender individuals from all legal gender protections in the state. Riley Gaines, who heavily promoted the bill, joined Governor Jim Justice at a press conference where it was announced as a major policy priority. The proposed legislation would have led to bathroom restrictions, prohibitions on driver's license and ID changes, and the elimination of legal recognition for transgender people's gender identities. Despite frantic, last-minute efforts by some Republicans to pass it, Democratic lawmakers countered by proposing dozens of amendments for debate. As a result, Republicans placed it at the bottom of the calendar.
“HB 5243 offered no real tangible protections for cisgender women, all while punching down on another marginalized community, and sought to erase protections for transgender West Virginians,” says Ash Orr, a trans organizer in West Virginia, “Essentially, it amounted to yet another culture war bill designed to divert attention from genuine issues affecting all residents of West Virginia.”
Another bill that did not pass in West Virginia was House Bill 5297, which sought to entirely prohibit gender-affirming care for all transgender youth. The state had previously enacted a ban on gender-affirming care, but it included an exception for transgender youth experiencing "severe dysphoria." HB 5297 aimed to eliminate that exception. More than 400 health care providers signed a letter opposing the bill, describing gender-affirming care as lifesaving and urging the legislature to reject it. The bill failed to pass before the legislature adjourned, meaning that at least some transgender youth in the state will continue to be able to receive care, making it one of the few red states where this is still the case.
The state is the latest in a series of developments suggesting that the anti-transgender panic gripping the GOP may be diminishing in the lead-up to the 2024 elections. Florida also recently adjourned without passing numerous anti-transgender and anti-LGBTQ+ bills. Recent elections have raised questions about the effectiveness of anti-transgender policies in driving voter turnout. In 2023, more than 70% of Moms for Liberty candidates were defeated. The Virginia legislature shifted to Democratic control, despite Governor Youngkin's efforts to campaign for Republicans by emphasizing anti-transgender politics as a policy priority. Governor Andy Beshear was reelected in Kentucky despite substantial ad expenditures attacking him for vetoing anti-transgender legislation.
When asked about the failure of these to pass, Orr stated, “The truth is, transgender people of all ages are living happy, complete, and beautiful lives - this contradicts the false narrative created around our community by anti-transgender politicians.”
The only bill that did pass in the state was a bill that would stop non-binary gender markers on birth certificates, though it is unclear what effect the legislation would have given that the state did not have a history of issuing such birth certificates.
Although these bills are failing to pass in states that have historically targeted transgender individuals, it remains unclear whether their failure signifies a genuine shift away from targeting LGBTQ+ people or merely a pause in anticipation of the 2024 election outcomes. The threat remains significant in many areas, with a few extreme bills being enacted this year, including a gender-affirming care ban in Wyoming and an adult bathroom ban in Utah. Additionally, some new states have witnessed the successful advancement of anti-trans legislation, such as a "Parents Rights in Education" bill in Washington, which could lead to forced outings, and a bill in New Hampshire that permits sports and bathroom bans. The national budget debate also includes anti-trans provisions that are still under negotiation.
Nevertheless, activists in states that have experienced the most severe attacks see reasons for celebration and hope. The failure of dozens of bills targeting the LGBTQ+ community means that residents in these states will have another year to prepare and strategize. If the 2024 elections yield unfavorable results for Republicans who have advocated anti-transgender legislation, similar to the outcomes in 2022 and 2023, it could further argue against the political viability of making these bills a policy priority. Most importantly, transgender individuals in these states are granted the valuable gift of time to catch their breath following the relentless barrage of legislative efforts that have dominated political discourse over the past five years.
#us politics#West Virginia#protect trans lives#Erin Reed#in support of an informed and engaged electorate#your vote matters SO MUCH
87 notes
·
View notes
Text
Erin Reed (January 16, 2024). "Erin's Anti-Trans Risk Map: Early Legislative Session Edition." Erin in the Morning. https://www.erininthemorning.com/p/erins-anti-trans-risk-map-early-legislative
This post on Erin Reed's blog tells all about the current status of anti-transgender bills and laws throughout the United States.
#rated G#US politics#USpol#transgender#transphobia#sexism#ErinInTheMorning#Erin In The Morning#Erin Reed#law#bill#anti-transgender bills#transgender youth#geography#links#news
17 notes
·
View notes

Text

By: Sammy Gecsoyler
Published: Apr 21, 2024
The doctor behind a landmark review of the NHS’s gender identity services for children and young people has said fears had been raised about her personal safety amid online abuse after the report’s release.
Dr Hilary Cass told the Times she wished to address the “disinformation” circulating about the findings and recommendations handed down by the Cass review when it was published on 10 April.
She said she had received online abuse in the wake of the report and had been advised to stop using public transport.
The report said the evidence base for gender medicine in young people had been thin and children had been let down by a “toxic” public discourse around gender.
Cass told the Times: “I have been really frustrated by the criticisms, because it is straight disinformation. It is completely inaccurate.
“It started the day before the report came out when an influencer posted a picture of a list of papers that were apparently rejected because they were not randomised control trials.
“That list has absolutely nothing to do with either our report or any of the papers.”
Referring to the online abuse she had received, she said: “There are some pretty vile emails coming in at the moment, most of which my team is protecting me from, so I’m not getting to see them.”
She added: “I’m not going on public transport at the moment, following security advice, which is inconvenient.”
The report said the now shuttered Gender Identity Development Service (Gids) at the Tavistock and Portman NHS Foundation Trust, the only NHS gender identity development service for children in England and Wales, used puberty blockers and cross-sex hormones despite “remarkably weak evidence” that they improved the wellbeing of young people and concern they may harm health.
The report recommended that young people struggling with their gender identity should be screened to detect neurodevelopmental conditions and there should be an assessment of their mental health, because some who seek help with their gender identity may also have anxiety or depression, for example.
When the report was released, Cass stressed that her findings were not intended to undermine the validity of trans identities or challenge people’s right to transition, but rather to improve the care of the fast-growing number of children and young people with gender-related distress.
NHS England has since announced a second Cass review-style appraisal of adult gender clinics. Cass confirmed to the Times that she would not take part in the adult report after the abuse she suffered in recent weeks.
She said: “You heard it right here: I am not going to do the adult gender clinic review.”
--


==
"If someone doesn't value evidence, what evidence are you going to provide to prove that they should value it? If someone doesn’t value logic, what logical argument could you provide to show the importance of logic?"
-- Sam Harris
These gender ideologues are cultists. There's no science, no evidence, no reasoning that would convince them of reality, because they don't believe based on science, evidence or reality. They believe entirely on ideology and faith. Nothing will convince them that, wait, perhaps we got this wrong? Is there something we missed? Could this have gotten out of hand? Is there information we don't know about?
They don't care.
They do not care.
They don't care about truth. They don't care about people. They don't care about kids; they just use them as a shield from criticism. They don't care about anyone. They only care about their ideology of gender revolution and "queering" the world, no matter the cost, no matter who gets hurt along the way.
Never ever forget and never ever forgive. Make sure these lunatics are as notorious in history as Mengele and Lysenko.
#Leor Sapir#Dr. Hilary Cass#Hilary Cass#Cass Review#Cass Report#gender cult#disinformation#medical corruption#medical scandal#medical mutilation#gender affirming care#gender affirming healthcare#gender affirmation#queer theory#gender identity ideology#gender ideology#intersectional feminism#religion is a mental illness#Alejandra Caraballo#Erin Reed#Michael Hobbes#Evan Urquhart#pathological liars#known liars#gender fanatics#gender reckoning
14 notes
·
View notes
Text
I feel like the Nex Benedict ruling should make Oklahoma the next "Do Not Travel" state on the Trans Risk Map, at least for trans youth
8 notes
·
View notes
Text
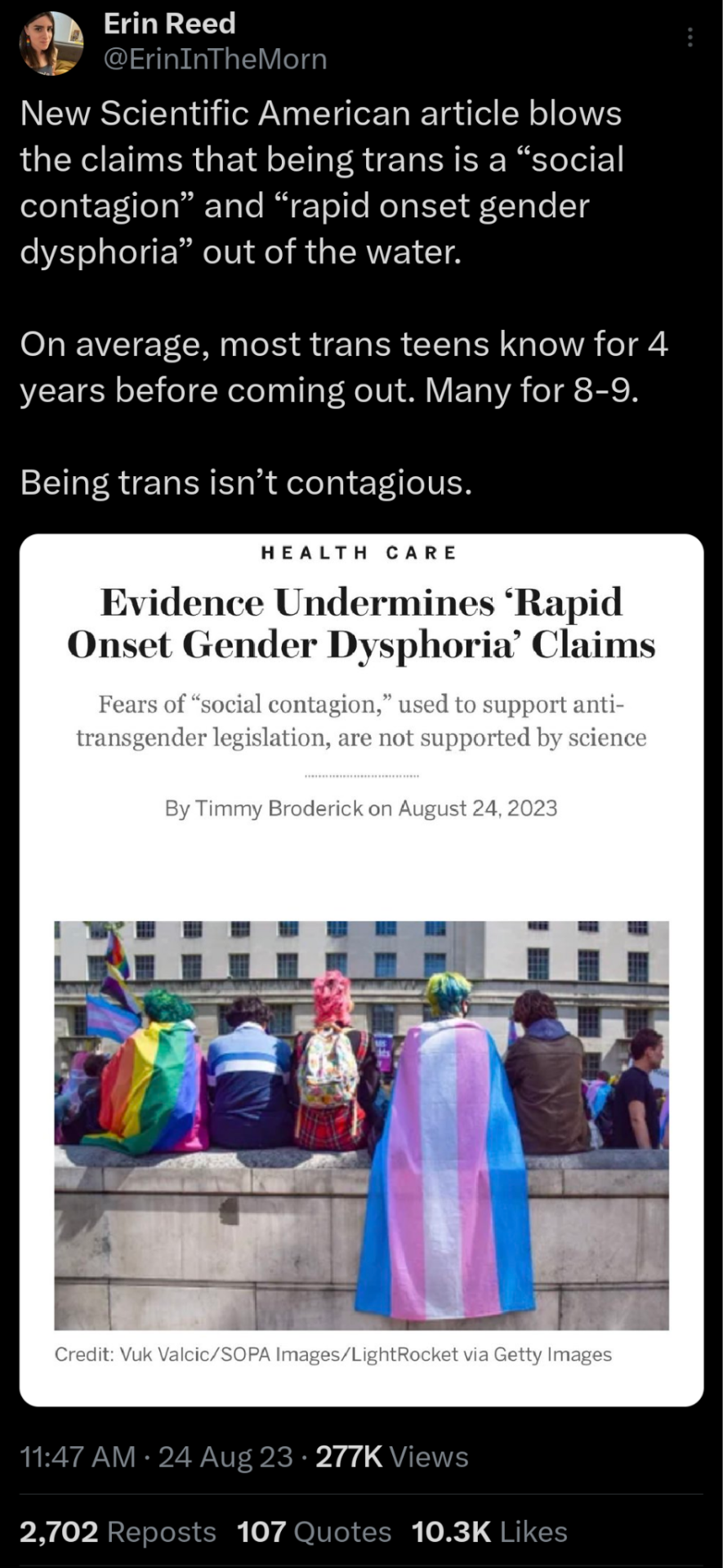
This will no doubt piss off the fascist gender criticals and then claim science has gone woke.
#fuck transphobes#translivesmatter#trans rights#trans rights are human rights#fuck TERF's#fuckterfs#terfs are fascists#terfs are white supremacists#fuck terfs#LGBTQ#erin reed#erin in the morning#twitter#x#gender dysphoria#onset gender dysphoria#transphobia#gender isnt real#gender is a social construct#trans healthcare#gender affirming care#protect trans kids#trans liberation#queer liberation
85 notes
·
View notes
Text
Ferret filibuster. Ferret. Filibuster. FERRET FREAKING FILIBUSTER
Maybe this planet isn’t entirely doomed.
#ferret filibuster#support trans people#yeet transphobes into the sun#uk politics#the mps are alright#congresscritters take note#this is how we do it people#erin in the morning#erin reed#trans rights
11 notes
·
View notes
Last Seen Blogs

weepingtragedytheorist-blog
RE-construction

bolajudi1
Liga188

0104-vikita
Vikypoopsiekins

rouletteislam744-blog
rouletteislam

momoaoil
momomo