#state of disorder EP
Text
TERENCE FIXMER // ENTROPY
[STATE OF DISORDER EP, JUN 2023]
#RELEASE RADAR#audio#terence fixmer#EBM#industrial#electro#state of disorder EP#techno#electronic#music
15 notes
·
View notes
Text
love love love yellowjackets but sometimes they're on thinner ice than javi with their mental health representation
#yellowjackets tag#postcard for next ep uses a straitjacket.......#and i kinda....#am constantly getting rubbed the wrong way by how tai's fugue state is handled#i know tawny said in an interview recently it's not supposed to be DID#and i've heard there's an REM disorder it could be instead#it's not... explicitly badly done!#some of it just feels like if they take one half step in the wrong direction it's gonna be really bad looking back#same with lottie's probable schizophrenia#from the wording on some things it just feels a bit like they're trying to avoid having to do the work to#make the possible mental health implications be done carefully bc 'oh well we dont intend for it to be x!1!1!' or#they dont explicitly mention it in canon etc#and i could be very wrong#like i said there's nothing too concretely bad yet#it's just. future stuff could make current stuff look awful in retrospect lol so im constantly very wary#also i do know it's a dark show so u cannot expect Super Positive Representation UwU#i'm not rly talking about positive rep i'm talking about accurate rep which is important if they want#to stay grounded in the conversation of 'is it supernatural or is it their warped perceptions/trauma/mental illness/etc'#but i also dont personally have anything tai or lottie probably have so who knows!#the straitjacket thing just rly brought the possible sensationalism issues to the forefront of my brain today#and therefore the possibilities (key word being possibilities) of them ditching accuracy in favor of telling an exciting story#again i love the show and bc i love it i do not want them to do this badly im just haha a bit scared bc of the#seeming lack of education on these matters#and that's where this stems from - not 'i expect perfection in my teevee shows and so i'm going to get mad about#every little thing that's literally just up for interpretation actually but i'm accusing them of being ableist etc'#it's 'i really love this show and i really want to have more faith in them to handle these things but they're very close#to letting me down very bad'
5 notes
·
View notes
Text
The Basics of DID/OSDD
DID, or Dissociative Identity Disorder, is a trauma-caused disorder that forms in early childhood, anywhere before the age of 9 (cutoff age is debated but the typical range is before age 6-9, but some people extend it to 10 because that's the typical age where your identity starts forming independant of your primary caregivers)
Most of the established and spread facts about DID come from the Theory of Structural Dissociation (TOSD)
Here's a good resource explaining The TOSD:
To sum things up, there are levels of dissociation that can occur, and disorders that fall into each level. The lowest end of this spectrum is PTSD, and the highest is DID. Here's a graphic of those levels, and I'll go into each disorder briefly:
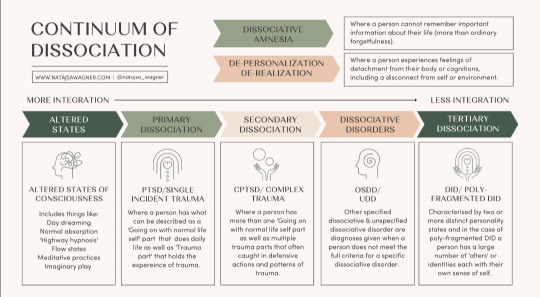
Altered States
Altered states are normal, and likely to occur in everyone at some point. No trauma is required to cause these states. Altered states include normal daydreaming (not including MaDD which is disordered)
Primary Dissociation
Primary Dissociation occurs in people with PTSD. This presents as having one ANP (Apparantly Normal Part, aka you) and one EP (Emotional Part, which occurs when having PTSD flashbacks)
This level is specifically for single-event PTSD, as C-PTSD falls under the next level:
Secondary Dissociation
Complex-PTSD falls under this level because of the occurance of multiple EPs, but still one ANP. These EPs are for a myriad of traumas a person with C-PTSD has experienced.
Dissociative Disorders
This is where we start touching on systems. This level includes OSDD and UDD.
OSDD (Otherwise Specified Dissociative Disorder) is a bit of an umbrella disorder, and it encapsulates multiple different types of OSDD. The one you've most likely heard of is OSDD1b, but I'll go into all of them.
OSDD1a is a disorder in which a person has multiple identity states but they lack distinction. They have intense enough amnesia to qualify for DID, but their identity states aren't differentiated enough to fully qualify for DID. This can sometimes (not always, of course) present as multiple identity states that are all one person, just at different ages when trauma happened.
OSDD1b is a disorder in which a person has multiple identity states that qualify for DID, but have no amnesia. A common misconception is that to be diagnosed with DID, you have to have blackout amnesia (will explain amnesia types later in the post), but any type of amnesia can qualify. OSDD1b is for systems who have absolutely no amnesia.
OSDD2 is a disorder in which there are identity disturbances and dissociation caused by brainwashing, torture, cults, and things of that sort. From what I understand, OSDD2 occurs after the cutoff age of DID or OSDD1, hence why this disorder does not cause a system.
OSDD3 seems to be a temporary diagnosis for symptoms of dissociation, derealization, depersonalization, amnesia, sudden loss of motor skills, ect for less than one month, occuring directly after a traumatic event. If the symptoms persist after this one month period, another diagnosis may be looked at.
OSDD-4 is a disorder in which people experience dissociative trances that do not have any known cause. People slip in and out of these trance states, often unaware of their environment while in them, and may "come to" confused and with amnesia from their time in the trance state.
And lastly, UDD. UDD, or Unspecified Dissociative Disorder, is exactly as it sounds. It's a catchall diagnosis for when a dissociative disorder is present, but it's unknown exactly which one. This can include systems, or it can include other dissociative disorders.
Tertiary Dissociation
Teritary Dissociation is what includes DID, C-DID, and HC-DID.
DID is the disorder we are all reading this post for. It is a disorder that causes multiple identity states that are distinctly different, called alters (or other terms depending on the system's comfort, such as headmates or sysmates), and amnesia between these identity states.
C-DID is a community term which stands for Complex DID. It is synonymous with Polyfragmented DID; they both mean the same thing. C-DID is characterized by a more complex system structure and the presence of many fragments, occuring because of more complex and longterm trauma that starts before the age of 5 (so earlier than the DID cutoff), and typically continues long after the system forms. There are many signs of polyfragmentation in a system, but the most siginifigant are the earlier onset of trauma, presence of many fragments, and more complex internal structure.
HC-DID is another community term which stands for Highly Complex DID. This term is synonymous with programmed systems/RAMCOA systems. These systems formed because of childhood trauma involving Mind Control (the MC of RAMCOA), aka programming. I won't go too in-depth on HC-DID systems, because I'm not confident in my knowledge at this time. However a great blog I can recommend for anyone wanting to learn more is @cultishhellvent
Misc.
You might have noticed at the top of the graphic I included earlier a little blurb about DPDR, or Depersonalization Derealization Disorder. This is a dissociative disorder characterized by, well, persistant depersonalization and derealization. This disorder cannot co-occur alongside DID, but DID can cause depersonalization and derealization. The DPDR diagnosis is for those who don't have another dissociative disorder like DID, but do experience those specific symptoms of depersonalization and derealization.
P-DID, or Partial DID, is a version of DID in which one alter is almost always fronting. Other alters are present, and may front in specific situations, but typically the one alter will stay at front and other alters will come and go from co-con or co-front.
Things To Know About Systems
So here is a bunch of catagories of info about systems that I feel are necessary to know if you're looking to know the basics.
Amnesia Types
Blackout Amnesia is amnesia that is full and total. Periods of blackout amnesia will be fully gone from the person's memory. However, contrary to popular belief, blackout amnesia does not entail literally 'blacking out' and 'waking up' at a later time. It simply means the memories from a time period are totally and utterly gone and inaccessable to you.
Greyout Amnesia has two typical definitions. The first is amnesia that slowly occurs as time goes on, like slowly forgetting the days as you pass them, at a faster rate than would be considered typical for those without a dissociative disorder. The second definition is similar to blackout amnesia, except some memories can be retained. So you may not fully remember an event you went to last week, but you might be able to recall a few blips of major things that took place. Most detail is usually lost.
Emotional Amnesia is when you remember the actual event or time frame, but none of the emotions attached to it. This usually presents as being able to remember a traumatic event, but feeling numb or disconnected to it, or like it happened to someone else.
And something important to keep in mind is that these amnesia types are not hard rules, and amnesia is often somewhere between these three labels.
Innerworlds
Innerworlds, or headspaces, are internal worlds in which alters can go when they aren't fronting (fronting meaning to be in control of the body)
Not all systems have innerworlds, and many systems with Aphantasia (when you can't visualize) simply don't have the ability to create them.
Innerworlds are often created unintentionally as the system grows up, but they can be intentionally created and that can be a beneficial process to the system.
Alter Roles
Alter roles are labels systems can assign to their alters to describe what role they play in the system's life. Some common ones include Host (primary fronter), Protector (self-explanitory), Persecutor (causes the system harm for whatever reason), Traumaholder (alters who hold trauma), and Littles (child alters)
These roles are not hard set, they are simply labels to help explain and put words to what certain alters' jobs in the system may be. And, not all alters have a discernable role.
Introjects
Introjects are alters who form based on an existing identity. This is common in fragments, since they aren't as fully formed, but can of course also happen in fully formed alters.
There are two main catagories of introjects, however many people like to get specific with the terms they use.
Fictives are introjects of fictional characters. This can be from visual media, books, OCs, ect.
Factives are introjects of real people. This can be from friends, abusers, family, celebrities, ect.
Introjects are NOT the same as the thing they are sourced in. They are their own separate people, and should be treated as such.
One of the specific terms I mentioned could be songtives (introjects from songs). I wanted to briefly mention that as an example of the specific terms systems may use.
Co-Con/Co-Front
Co-con, or co-conciousness, is when two or more alters are present at the front. This is usually used to describe one alter fronting, with one or more other alters hanging out nearby and talking occasionally.
Co-front, or co-fronting, is when two or more alters are sharing the front together fully. Think of two people trying to drive the same car at once.
I think I've covered everything I wanted to cover. If I missed anything, said anything incorrect, or you'd like something added please feel free to send an ask or comment/reblog.
#did#osdd#udd#pdid#anti endo#anti tulpa#polyfrag system#c-did#hc-did#ramcoa#actually traumagenic#endos dni#did community#traumagenic did#system#osdd system#actually osdd
583 notes
·
View notes
Text
I've heard one of my posts is causing waves
Here's some more things that are normal in DID/OSDD systems, and some weird myths, in no particular order
- Not realizing you're a system until later is normal (average age of system discovery is 18-21)
- It's rare for children to display distinct alters (not impossible, just a rare occurrence in a rare disorder (based on numbers, it's considered rare, yes), alters tend to form in mid-teens)
- Feeling as though you "created" an alter is normal (related to unconscious feelings of control over an uncontrollable situation, and/or tricking yourself into an explanation, also, if you have a need to be filled, the brain WILL provide)
- "mixed origin systems" are totally normal for DID/OSDD. I have a couple alters that could be considered "endogenic", but I'm really just... DID, with normal alters forming in normal ways
- Alters forming at any age/time is normal (you can form a brand new alter at fifty, after having undergone complete fusion, once the ability is there, it's always possible to split)
- Alters don't always appear immediately after a traumatic event (alters can take YEARS to come to front after forming, making it impossible to tie them to specific events unless THEY'RE aware of the connection)
- Alters can form from stress, not just trauma (and the brain is notoriously good at hiding how stressed you are from yourself)
- Comfort splits ARE normal in DID/OSDD
- The amnesia criteria in DID doesn't mean you need to experience amnesia day-to-day, you still have DID if you can't remember childhood events but have good communication now
- The dysfunction criteria is redundant and circular, where the symptoms themselves fulfill the criteria, and as per the DSM, doesn't imply any inherent need for treatment or distress-- so being happy, loving your system, feeling like your system helps you more than it hinders you, all normal (and good!) but still DID/OSDD
- OSDD 1a does not involve alters as they're known, but states or modes that influence you, and amnesia occurs during these periods of influence; OSDD 1b involves "emotional amnesia" only (which is just a stupid, fancy word for dissociation (an emotional disconnect from a memory) that doesn't actually exist in the medical world)
- You can have as many EPs and ANPs as you'd like. The majority of systems with OSDD feel as though the one ANP theory doesn't fit them, and there have recently been updates to theories to acknowledge this
- Integration is the lowering of dissociative barriers to allow for better communication between system members, and is absolutely necessary for functional multiplicity (fusion is the joining of two or more alters). These definitions come from the ISSTD, and it IS recognized by the ISSTD that integration and functional multiplicity are viable and attainable treatment goals. Keep this in mind when conversations about these topics come up-- if you can communicate clearly with alters, you're already well integrated. It's not scary, it's not bad, and no one can or will make you fuse.
- CPTSD, the basis of dissociative disorders and DID, presents very differently from PTSD -- mostly presenting as a negative view of the self and vigilance rather than the flashbacks and nightmares you'd see in PTSD (it's quite similar to BPD, but the view of the self is negative rather than unstable). If you resonate with some aspects of BPD and have a system, and you don't experience the "typical" presentation of PTSD, that's normal. That's CPTSD (complex PTSD, not chronic PTSD), maybe read up on it.
- You don't need to know your trauma to acknowledge that you have DID/OSDD, and no one should be pushing that you search for trauma. Who cares, move at your own pace, maybe you'll never figure it out, and that's perfectly fine. People who push others about their trauma will face my wrath.
- Trauma isn't an action, but a REACTION to an event. What traumatizes one person, may not have any effect on another person, and vice versa. This isn't about what might have happened to you, but how you felt about it. There is no Trauma Olympics, and people who play that way are ridiculous. Trauma reactions are personal and unique, and come from anything-- bullying, isolation and loneliness, abuse. And yes, other disorders can make you more susceptible to trauma reactions. Having autism or ADHD or BPD, EDs, psychosis, schizophrenia-- all of these create more opportunities for trauma reactions, and make someone more susceptible. That doesn't mean you're not trauma based. It doesn't mean those things caused your system. It means those things made it harder for you to navigate life and left you more susceptible to trauma. That's it.
- MADD is typically trauma based
There's so, so many more. Other DID/OSDD systems, feel free to add on, endogenic systems, ask if something is normal.
#syscourse#actuallyplural#actuallymultiple#actuallytraumagenic#actuallyosdd#actuallydid#osdd#did#endogenic#totally normal things
1K notes
·
View notes
Text
Job Roulette.. or Not: A Post about Alter Roles
Roles like Hosts? Protectors?.. maybe a Cleaner? an Academic?.. why is there an alter who comes out only for driving?! What about these other alters who don't really do much--they got to have one right??
--Are probably what you might be thinking when this topic comes up. But, there's something more into it,, it's not all about what job or how the role is assigned to an alter only.
Well, for this post, lets talk EVERYTHING about how roles work, what kinds exist, why it's there?? And especially, why are some more task specific, multi-role, or even... none? Bowl straight to the point, let's roll out. Haha punny
Ok J, spill. What are they?
Hold on. Im pulling out this dictionary definition of it--ah!
"defined positions that are associated with given responsibilities and are usually allocated according to the position or ability of each person."
To put it in system terms, it's how different parts can do something that others couldn't, or, feel a sense of responsibility in one particular aspect. That's making sense right? But oh.. you still want to know why they're there at the first place. Fine, follow me!
Yeah, show me why!
As aforementioned, this disorder boxes up our different parts of selves with amnesia and weaker bonds of connection which really sets us back on easing our 'modes' for different situations.. not only that, a part's moods and state/personality can greatly affect what kinds of jobs they get, it's not so random as you'd thought.
So, thing is, because some alters have a distinguished ability capable in doing something, depending what fragment or pre-existing knowledge/experience it holds, that can become it's very own job task.
They can be hereditary (upon split or formed), gained (fuse or passed traits), or even learnt (by its own commitment, without any prior skills). Roles come from many origins, and none of them are so different.
But, some are more complex..
I get it, some can have more than one, have ultra specific ones, or literally just don't have any. Now it makes you think--if it was from predisposed strengths each alters naturally have, then why are some more niche? or like, anything else? I know why:
Our brains are complex alright. We both can think maybe we can do (even if we don't like it) and not do something, and these are all compartmentalized in each alters, so basically its part feelings, part acceptance of such trait, and part commitment as the formula. Even confidence or the call to action affects this outcome!
This can apply to who can handle more than one jobs, or for those who are more specific or lesser known roles. In fact, roles do not have any limits, they are specifically tailored for your functionality so don't fret if you have an alter who's job is only to sleep, or anything else 'silly' !
What about the ones without.. roles?
Do you think it feels wrong to not have roles? While it is true that roles are needed, they're not actually a required standard for everyone to have a job task. Mainly, ANP's are the one who usually have roles, but EP's can too.
If they do not have a role, they might be disinterested or think they don't have any potential, or sometimes they're only there to hold memories / don't have the qualified skill sets, and thats okay! You can take proactive action in anyhow you'd like, just remember, every parts aren't forced to contribute, you know? It doesn't make them useless, maybe more on passive support/back ups.
I've also seen some systems who don't really have roles because the alters are all well-rounded, as in pick up other's tasks and that they're not assigned/compelled to do a particular job at all times, like being flexible. everyone's different!
Make sense, anything else?
Well, that we are not bound to roles, they do not define us, and that we can lose, or change roles according to our growth. Have anyone ever mentioned that?
Im aware that we tend to put too much emphasis on having jobs and being contributive, but the most important thing to keep in mind is that we all in this together, and to help each other, in a way or another.
Never forget that you're more than your job! Maybe try to enjoy other parts of life, yeah?
--
Thats the end of the post. What will you do if you find a new alter with no impressions of having a role? How do you see roles in your own pov? What's the first thing you'd do if you were to be free from your job task, if any? Feel free to let me know, i hope this has been informative, im willing to add anything if something's missing!
- j
#did#actually did#did community#did osdd#did system#dissociative identity disorder#sysblr#plural#system stuff#jeducates
79 notes
·
View notes
Note
Plural culture is being pissed off because you’re a firm believer of “you can have a symptom/trait without having the entire disorder/disability/etc” (for example we have narc traits but not enough to be classified for a NPD diagnosis bc it comes from our BPD, or people who may experience hyperactivity without it necessarily being ADHD, things along those lines) but “Endogenics” keep twisting this to basically say to you that you can’t believe that and then not believe in the existence of Endogenics systems because “we simply have a trait and not the whole disorder <3”, and getting angry because they can’t have a system without the disorder because the whole reason a system forms is due to the trauma that stops ANP and EP ego states from fusing in childhood and as the brain continues to develop a personality, these separated ego states will still develop meaning instead of one personality, there’s multiple. There’s no other reason for the system to develop apart from sectioning horrific trauma off to literally survive.
Does this make sense we’re blurry and pissed off /lh
.
#endos dni#osdd#pdid#did#did system#pdid system#osddid#actually did#traumagenic#actually dissociative#plural culture is#syscourse
42 notes
·
View notes
Text

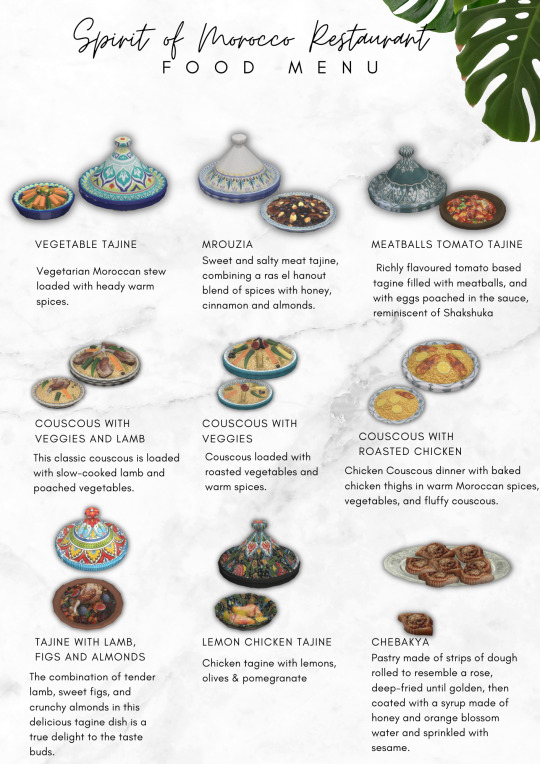
Spirit of Morocco
Hi guys! The following post has been made by Mirai on her Patreon page, who asked me if I can share it from her name on Tumblr to gather more views, since she is having troubles with Tumblr recently:
Hello guys! I hope you are doing well! I know I have been a little quiet lately because I had to be hospitalized routinely again at the end of last month because of my autoimmune disorders, but everything is fine. However, I did hear about the earthquake in Marocco at the beginning of the month and I am heartbroken. I had the privilege to visit this magical country at the beginning of this year, and I fell in love immediately with their rich culture, fantastic food, beautiful sights, and friendly people. And that's why I wanted to do something.
I've been working really hard with no break since the day I heard about the event to make sure I can create as many items as possible. So I present to you 'Spirit of Marocco' a food kit filled with some of the most emblematic dishes from Moroccan cuisine. In total contains 13 different dishes and 5 canned goods.
All typical for Moroccan cuisine. - Three types of couscous dishes, four types of tajine dishes, Pastilla, Seffa, Mrouzia, Harira, Chebakya.
All canned goods require Cottage Living EP*
All dishes require the latest version of my food enabler
Until the 30th of October, you can purchase this custom food set 'Spirit of Morocco' on the Ko-Fi platform, and all collected money there will be donated to Morocco Earthquake Relief Fund by GlobalGiving:
Of course, the set will also be uploaded on my Patreon, to honor all the people who support me monthly, but if you want your money to go towards the charity, make sure to download the set from my Ko-Fi shop.
Ko-Fi Shop
Mirai's Patreon
How to help Morocco:
Thank you and happy Simming!
Mirai M ~
THE FOOD IN GAME**





@maxismatchccworld @sssvitlanz @scarlets-realm @luthsthings
#ts4 custom content#s4 download#ts4 download#s4 custom content#ts4 maxis match#ts4 maxis mix#s4 maxis match#sims 4 download#s4 mm cc#ts4 mm cc#ts4 custom food#ts4 custom drink#ts4 custom objects#ts4 custom recipe#ts4 custom recipes#s4 custom food#s4 custom drink#s4 custom object#s4 custom drinks#sims 4 custom food#sims 4 custom content#sims 4 custom recipes#ts4 maxis cc#ts4 alpha mix#ts4 alpha
91 notes
·
View notes
Text
Stop Posting Hate and Disinformation in Endogenic Tags!

Does it? Are you sure? Because that's a really bold way to start off a post in a community with a lot of people who have PTSD!
But even bolder is this claim:
I would ask for the source for this, but I already know it.
youtube
Now, to be fair, there is a lot of wiggle room where some can argue semantics of what an "alter" is.
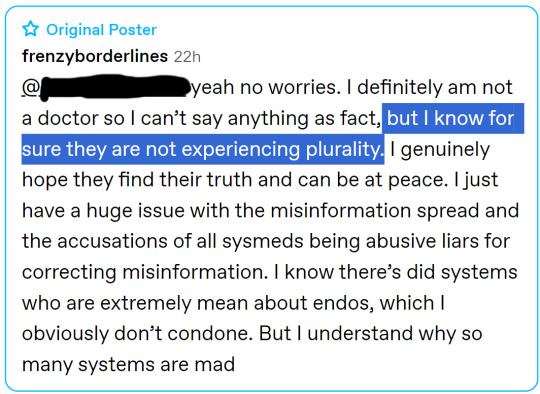
Luckily, today we aren't arguing semantics, as they made it clear in a comment that they don't believe endogenic systems are experiencing any sort of plurality! Yay!
Now, back to their claims... it's true that most evidence of any forms of consciousness in psychology is based on believing people's personal experiences.
Psychology is distinct from neuroscience in this way. Hopefully, we can get neurological evidence too. Stanford University was conducting an fMRI study into tulpamancers. But that study isn't complete yet.
But it is worth noting that practically every researcher who has looked into endogenic and non-disordered plurality do believe it's a real phenomena.
As mentioned above, Stanford University has invested anywhere from tens of thousands of dollars to hundreds of thousands of dollars into a neurological study of tulpamancers.
The ICD-11 by the World Health Organization states that you can have multiple "distinct personality states" without a disorder.
The creators of the theory of structural dissociation have said that hypnosis and spiritual mediumship may create "self-conscious dissociated parts of the personality."
Transgender Mental Health by Eric Yarbrough has an entire chapter discussing plurality, including acknowledging non-disordered and endogenic plurality. Eric Yarbrough is a Distinguished Fellow of the American Psychiatric Association, and this book was published by APA Publishing.
And these are but a few.
Psychiatrists and psychologists overwhelming support the existence of endogenic plurality.

Is there any reason for the human brain to just randomly decide to be a singlet?
Why do the 80-billion neurons in the human brain just decide to be one person? Why is a singlet treated as inherently the default for humanity?

Total side tangent, but not all alters fit neatly into the ANP/EP dichotomy. The thing that defines an ANP is not simply being dissociated from the trauma, but trying to continue on with normal life and avoid it. Hence, being "apparently normal."
Many alters though, just don't fit into that as described. I would argue that a non-traumagenic alter who never fronts isn't really an ANP according to the Theory of Structural Dissociation.

Yup. That's why I'm responding to this. Your post is nothing but misinformation.
Most words have etymology in other cultures. Hurricane, for example, comes from an indigenous religion that referred to storm gods. This is a natural process as cultures interact.
For the record, "tulpamancy" IS created headmates. The term "tulpamancy" is purely Western, with the -mancy suffix originating in Latin. And whether you like it or not, the ongoing studies into tulpamancy will be into this Western practice, not the Tibetan sprul pa from which it draws its etymology.

Maybe you should take your own advice.
Although if you have a single credible source proving that endogenic plurality can't exist, you're welcome to show me.
You: "Stay out of DID/OSDD spaces"
Also You: *Tags post as "#endogenic" and "#endogenic systems"*
Anyway, as always, anti-endos coming into endogenic tags means the response goes to anti-endo tags. If anti-endos do not like me posting in their tags, please take a moment to explain to @frenzyborderlines why crosstagging into our spaces is bad (and incredibly hypocritical from someone telling endogenic systems to stay out of CDD spaces) so I won't need to do this again.
#syscourse#pro endo#pro endogenic#anti endo#anti endogenic#endogenic#endos are real#endos aren't real#multiplicity#endogenic system#psychology#psychiatry#science#actually plural#actually a system#Youtube
68 notes
·
View notes
Text
Shadow the series: hopefully an enabling post
I want as many people as are interested to be able to watch this series so as promised: Here's a non-spoilery summary of potential triggers and squicks in Shadow the Series eps 1-7.
The really brief version: this show is really good, lots of intense things happening with family trauma, family violence, mental health, and abuse, but the actual supernatural stuff is pretty mild and the gore and violence is very minimal. There are also light comedy moments, and pining, and friendship, and the mystery is fun to watch unravel, so I didn't find it too spooky (but I have a high spooky tolerance so you may want to take breaks or otherwise do what you need to).
Ep1
Vomiting
Some creepy music
Slight jump scares
Depictions of drowning
Homophobic slurs
Bullying (including punches)
Scars (potentially self-harm but it's not clear)
Mention of ghosts, non-graphic ghost, creepy amorphous smoke
Ep2
References to hypnosis, potential gaslighting or hallucinations, uncertainty of reality
Institutional homophobia
Bullying (non-graphic)
Homophobia
Mention of possible teacher/student relationship (potentially unrequited)
Ep3
Bullying, homophobia
Mention of dead bodies
Mention of ghosts
Mention of family violence
Depictions of drowning
Flickering lights
Mild corporal punishment
Non-graphic ghost
Mentions of cancer
Creepy grinning (lmao idk how else to list this)
Ep4
Mentions of cancer and treatment including deteriorating physical state
Depictions of deteriorating mental state
Depiction of end-of-life medical care in hospital
Depictions of family violence (yelling, grabbing, threats, slapping, kicking, beating, threats with a gun) of both a mother and child
Hospitalization for mental illness, psychosis
Mention of antidepressants
Threatening someone's freedom with hospitalization
Accusations of infidelity
Depiction of suicide by hanging (not the actual death, just the body in partial shot)
Description of what sounds like childhood sexual assault from the perspective of a child (non-graphic, vague)
Depictions of alcoholism
Child neglect (feeding a child food they are allergic to)
Allergic reaction in a child
Beating (not too graphic but there is blood on knuckles and blood on face shown)
Funeral, death of a parent (mother and father)
Floating body
Ep 5
Floating body
Systemic inertia (probably not triggering but seriously infuriating)
Mentions of narcotic use
Mentions of bipolar disorder
Creepy mask
Casual mentions of father's death
Implied one-sided teacher/student crush (student hugging teacher from behind)
Non-graphic ghost
Homophobia, bullying
Teacher/student relationship (kissing, implied sexual relationship between older woman and younger male)
Negative self-talk around mental illness and medicating mental illness
Descriptions of hallucinations
Ep6
Smoking (supposed to be marijuana but looks like manufactured cigarettes)
Wet dream resulting from an erotic-coded moment with amorphous smoke (idk how to properly warn for this lol)
Scratches on body (ambiguous source)
Mentions of pregnancy
Implied infidelity (by a married couple)
Slap
Bite, punches
Non-graphic ghost, mild jump scare
Creepy "fun house" with decorations including a lot of bloody handprints/blood-sprayed walls, creepy clown, distorting mirrors, screaming, flashing light, red lighting
Ep7
Creepy "fun house" with decorations including a lot of bloody handprints/blood-sprayed walls, creepy clown, distorting mirrors, screaming, flashing light, red lighting
Multiple people punched in the head, bruised faces from being punched in the mouth (mostly student-on-student but one parent punching their child)
Mild jump-scare with a loud sound
Vision of multiple bodies on the ground, with pools of blood (brief, no visible wounds, gore is mild)
Clothed heavy makeout between married female teacher and male student
Flash of someone blindfolded and someone with a gun
Implied sexual dream with amorphous smoke
Mention of loss of a limb, dripping of blood (no wound visible)
Mentions of drug use (spoon over a flame shown, implying heroin)
Depictions of someone dying by firing squad as a death sentence (death not shown)
Non-graphic ghost
Someone being choked
The preview for the second half has a bunch more stuff, but nothing that hasn't been warned for in the first half (choking, punching, hanging, creepy mask, amorphous smoke, etc.)
96 notes
·
View notes
Text
What Happened to Trin? aka Paying Attention to My Favorite Straight Boy
Friends. Romans. Country men.
I have a confession.
Yesterday I reblogged a Shadow gifset of Josh cuddling Nai in the middle of the night after returning from his evening of smoking in the woods with Dan. In that reblog, I wrote the tag “Josh is my favorite straight boy in the show”. I showered praise upon him for being secure enough in his own sexuality to cuddle with the Known Queer. But I am concerned I may have been mistaken.
I was chatting with @khathastrophe about some Shadow theories and she sent me a screen shot of a conversation she had had with @brazilian-whalien52 about her theories around Josh.

Now, I personally do not think that Trin had a crush on Josh, unless they are intentionally obfuscating the context around the two conversations that Trin had with Joe where he did pretty much everything but explicitly state his feelings for Joe. And I hadn’t been thinking about Josh in relation to drugs, because yeah, he smoked weed, but if you couldn’t tell already, I have been hyperfocused on trying to unravel the One Armed Man thread and he is the only one I could remember having explicit ties to narcotics.
BUT! I had already been working my way through a re-watch of Episodes 1-7 to see if there was any new information I could glean from the show now that I had better knowledge of all the characters and their relationships to one another. And tonight, I was already planning on watching Episodes 5-7, so I said “you know what? I have been 0% suspicious of Josh the entire way through, but this show is steeped in mystery and it would be irresponsible of me no to pay attention to the character that I write off…after all, in a mystery it’s always the inconspicuous ones,”

And thus began my Josh!focused Rewatch of Episodes 5-7 (shout out to @so-much-yet-to-learn for bullying me about this, thank you for keeping me humble friend <3).
Some things I noticed in Episode 5:
Anan was running against Trin for student body president
When Trin is speaking in to the megaphone about wanting to change the bathrooms, Josh is in the crowd of students listening, but he does not participate in the chants everyone else is saying. And the second the Head Master appears, he is running off before he can really be registered as in attendance of this gathering.
Josh was out of the room when Joe saw Trin’s ghost, he returns after Trin’s ghost disappears, and Josh has left the auditorium when Trin’s ghost reappears and Nai sees him following after Joe.
Trin’s medical records state that he has bipolar disorder which can cause him to have hallucinations, he was off his medication, and he was using narcotics to treat his symptoms
It is later revealed that Trin got a medical check up after his arm injury, where it was discovered that he had consumed marijuana.
All in all there isn’t much to go off of here, expect that Josh seems rather non-committal to Trin’s policy changes, and he does not want to be seen in the company of unruly students.
Episode 6, however, is where it starts getting interesting for me, because Episode 6 is where Josh invites Dan out for a little smoke sesh.
Now, I will admit, at the time of my initial watch, most of the conversation between Dan and Josh whizzed right on past me, obviously the only reason he had called Dan out there was to ask if he liked Cha-aim and to showboat a little bit. But on this watch through, thinking about Trin and Josh and drugs, the conversation hit much different, and it warranted a theory.
The Build Up


Dan asks Josh where he got the weed from, and Josh tells him he got it from a man named Bancha, an alumnus of the school who is a witch doctor. (now that I think about it, that is probably who this person is from the promos for Ep 8-14 (to your question @slayerkitty):

ANYWAY, Josh tells Dan that Bancha is a hermit who lives near the woods, and is a witch doctor that can treat mental illnesses. He asks Dan if he’s been having trouble sleeping and upon hearing Dan confirm his sleeping issues, tells Dan that Bancha could totally help him get rid of his sleeping problems.
So why did this start ringing alarm bells for me this time through? Because a) I was watching Josh with more scrutiny these episodes, b) I’ve been paying a probably unhealthy amount of attention to arms in Shadow over the last few weeks and c) I remembered more details about Trin.
The Puzzle Pieces
When Trin’s parents come storming in to Brother Anurak’s office pissed the fuck off because their sons medical records got leaked to the press, Brother Anurak mentions to them that Trin about a year ago (which is around the time Trin disappeared), Trin was treated in a hospital for an injury to his arm.
We open Episode 1 of Shadow with Trin running through the forest, with his left arm bandaged up.

Brother Anurak also tells Trin’s parents that he had weed in his system when he got that treatment. (When I heard this at first I brushed it off because it felt like between the mention of bipolar, hallucinations, and narcotics use, adding the weed on top was just a few too many things to try to discredit any potential intel Trin might have had and to distance the school more from his disappearance).
Josh is the only person we have seen with weed (so far).
Trin was diagnosed with bipolar disorder, and did not like the medication he was on. He wanted to feel “normal” and to get off his medication, which we are told through a flashback conversation between Trin and Master Joe in the theater. We also learn that Trin is going somewhere, he wants to give Master Joe a pen of his to hold on to while he is away and tells Joe, “when I come back and I’m rid of this disease, I will give you your answer” [side note: Joe does not take Trin’s pen, yet he has it in his desk in 1999, so he had to get it back from Trin somehow]
In short, Trin wants to be cured of his bipolar disorder and this Banchan guy that Josh mentioned is a witch doctor that can treat mental illness.
The Theory
So with these things in mind, that Josh was in a lot of the flashback scenes with Trin, that Trin had smoked weed at some point before his disappearance, wanted to be rid of his mental illness, had an injured arm, and was running through the woods when we first are introduced to him, I came up with a theory.
Josh played an active role in Trin’s disappearance.

gif from @pharawee
With the crumbs they have presented to us so far, my theory is that at the beginning of Episode 1 we are seeing Trin escaping the witch doctor that Josh has convinced Trin to go see. Trin had an injured arm at the beginning of Episode 1, and Brother Anurak mentions an arm injury, so I’d have to imagine they are the same injury. Which means that Trin had probably smoked weed with Josh like Dan had smoked weed with Josh. I can imagine that Trin asked the same question about where Josh got his drugs from, and that Josh gave the same answer. I can imagine Josh potentially knowing about Trin’s medical diagnoses, or at least observing in part Trin’s own experience with hallucinations and relying on that to help convince Trin to go see the witch doctor.
I can see Josh getting closer to Trin, close enough to get Trin comfortable with him, close enough to get Trin to trust him. I can see Josh and Trin sneaking out to the edge of the woods to smoke, and how that might make it easier to get Trin alone, away from prying eyes, and more comfortable with being in the forest at night. I can see Josh either walking Trin straight to the witch doctor’s door, or telling Trin how to get there. I can imagine the witch doctor trying to do something to “cure” Trin, whether that be an exorcism, a poisoning, an attempted murder, or something else entirely, and Trin managing to escape. Which would explain why we see him running through the woods, because as Josh said, Bancha lives right near the woods.
I see some things repeating themselves in the promo for the second half of the season, namely Dan having his left arm bandaged the same way that Trin’s was at the beginning of the show and running through the woods looking behind him scared the same was Trin was at the beginning of the show.

Do I think Josh is alone in all of this? No. If he is involved in this at all, I literally have no gauge or understanding of how complicit and aware of what he is doing Josh is. If Josh did play a role in Trin’s disappearance, is he sticking so close to Nai because he feels guilty? Or if my theory does hold true and Josh is pulling Dan aside for conversations and smoke sessions, is he intentionally setting something up?

Josh seems really comfortable and at ease with being physically affectionate and flirty with Nai, despite the potential to be subjected to homophobia, yet he also thinks theater is gay and tells Dan not to join because people will think he is a fag (which, I believe is the closest translation of “toot” to English, fruitcake is certainly not it).
When Trin was getting beaten up by Anan, Josh just puts his Walkman radio on and ignores the entire fight. Anan and Josh both say Trin is dead (and to be fair, if it were me and a student at my high school went missing a full year before, I would probably also assume they had died).
Oh! And another thing, one of the drawings in Dan's vision of the One Armed Man was a camera, you know who is associated with cameras?

Josh, our resident Photographer and General Assistant
I think @brazilian-whalien52 made a great point in the conversation I had with her: “Shadow seems like the type of drama everybody had a little hand in. Not an individual blame, but a look through society and the roles we play that affect others,”
All of which is to say, I unfortunately, will be withholding granting Josh “favorite straight boy” status in Shadow until the narrative proves my theory wrong.
#shadow#shadow the series#shadow the series meta#shadow the series analysis#shadow the series theory#clown checkpoint#seriously i need the back half of this show so it can prove all my theories wrong and i can move on with my life#please forgive the lack of photos of Trin related details. Gaga is on the fritz so I couldn’t take screenshots
59 notes
·
View notes
Text
넘버스 - Numbers - Whump List - 🇰🇷

Whumpees: (GIF) 장호우 (Jang Ho Woo) played by 김명수 (Kim Myeong Soo) and 한승조 (Han Seung Jo) played by 최진혁 (Choi Jin Hyeok)
Synopsis: Seung Jo is the ace accountant of the firm who's quite the opposite of Ho Woo in terms of motives, status and personality. These two work together with numbers to achieve their own goals. Their goals are different, but they are headed towards the same target. Will they be able to serve justice in this accounting firm and allow Ho Woo the closure he so desperately desires? (MDL)
Genre/Tags: Office, Romance, Tragic Backstory, Found Family, Orphan ML
Watch On: Viki, DramaCool, KissAsian
⚠️CAUTION: Ep 1 has a s**cide 15 minutes in —- Ep 5 has mentions attempted s**cide 22 minutes in⚠️
WARNING: POSSIBLE SPOILERS BELOW
장호우 (Jang Ho Woo)
1.01 : tragic backstory reveal ::: fought ::: picked up at the police station, hit on the back of the head (semi comical), cut on his face ::: fought, strangled, manhandled, beaten, cut lip, angry, thrown ::: concerned for someone, in shock, grieving, sobbing ::: (flashbacks: grieving, sobbing), angry ::: stressed
1.02 : none
1.03 : traumatic flashbacks, upset ::: in a car wreck, cut on his cheek ::: traumatic flashbacks, emotional
1.04 : cuts still on his face, emotional ::: (in someone’s flashbacks: in shock, hands covered in blood) ::: nosebleed, refusing help, angry ::: emotional ::: pushed up against a wall, manhandled, someone tries (and fails) to intimidate him ::: emotional ::: in shock
1.05 : in shock ::: emotional ::: drunk, in a depressed state ::: emotional ::: (nightmare: traumatic memories, beaten), woke up sweating, heavy breathing
1.06 : cold ::: coughing, concern for him ::: looked after ::: emotional ::: thrown against a wall, collar grabbed
1.07 : in shock ::: using himself as a shield (very minor), in shock
1.08 : in shock ::: emotional ::: running until he’s exhausted ::: fought, ran into a burning building to save someone, nearly in an explosion, concerned for someone
1.09 : fought, ran into a burning building to save someone, nearly in an explosion, concerned for someone, in shock, stumbling ::: emotional ::: in a depressed state in bed ::: in shock ::: emotional ::: angry
1.10 : out of it, fought, angry, restrained (manhandled), struggling ::: friends come get him from the police station, black eye, busted lip ::: in bed in a depressed state, concern for him, refusing to speak, curling in on himself ::: emotional, concern for him ::: running a fever, concern for him, shaky breathing ::: scolded (sorta), wound reveal, emotional
1.11 : none
1.12 : panicked ::: emotional ::: grieving, traumatic flashbacks ::: looked after

한승조 (Han Seung Jo)
1.01 : someone attempts to fight him
1.02 : none
1.03 : in a car wreck
1.04 : (traumatic flashbacks: crying), intense chest pain (panic attack), collapsed, writhing ::: looked after, asleep, woke up, groaning, reveal that he has/had a panic disorder ::: emotional, angry, punched ::: emotional ::: in shock
1.05 : in shock ::: emotional
1.06-1.07 : none
1.08 : fought, nearly in an explosion, concerned for someone
1.09 : fought, nearly in an explosion, concerned for someone, emotional ::: fought, grabbed a knife with his hand to protect someone, concern for him ::: emotional
1.10 : emotional, crying
1.11-1.12 : none
———+———
MORE WHUMP LISTS >>> {x}
105 notes
·
View notes
Text
COME AROUND
TERENCE FIXMER
[STATE OF DISORDER EP, JUN 2023]
#RELEASE RADAR#audio#terence fixmer#EBM#electro#industrial#state of disorder EP#techno#electronic#music
7 notes
·
View notes
Note
We really loved your post about CDDs... However you overlooked C-PTSD which forms one ANP and multiple EPs... This can be considered plural (not a system!!!!!!!) and is still disabling, like other CDDs you mentioned <3
/nm , info
i have quite a lot to say about this ask. i've let it fester in my inbox for a while now, but i am ready to debunk all of the misinformation it contains.
first, & my most obvious point: C-PTSD is not a complex dissociative disorder.
C-PTSD, as you can tell by the name, is a post-traumatic stress disorder. just because a disorder (sometimes) presents with dissociative symptoms, does not make it a dissociative disorder. C-PTSD is a post-traumatic stress disorder, not a dissociative disorder. the word "complex" is describing the "post-traumatic stress" aspect, not the dissociative aspect, because dissociation is not the key feature of C-PTSD.
next, i believe you are misunderstanding the theory of structural dissociation.
the ANP & EPs theorised to be found in C-PTSD (aka, intrusive & avoidant) are not the same as the ANPs & EPs found in complex dissociative disorders. they do not have separate identities, but are instead aspects to one identity. this is because C-PTSD is not high enough on the dissociative spectrum to be able to create the individualised self-states seen in DID & related disorders. as you can read below, C-PTSD would fall under primary or possibly secondary structural dissociation. this verifies again that, no, C-PTSD is not a complex dissociative disorder, even if you do take into account the TOSD.
lastly, a few final points:
of course C-PTSD is disabling. nearly any mental disorder/condition can be disabling. this does not change what category it fits into!
C-PTSD's ANPs & EPs are not full identities so, no, it cannot be considered "plural". however, "plural" is not a medical term, so i will mostly be letting this comment slide.
please provide a source if you're going to claim something as misinformed as "complex PTSD is a complex dissociative disorder". that is an absolutely HUGE thing to claim without any scientific backup.
that's all from me. i remind you to check the definition of what a CDD *is* in the post you're referencing. (found here)
#the tone tags crack me up though :sob: like why would you be mad#you're wrong#it's okay to be wrong just please take a look at these sources & learn from it please#blurry❔.txt#;#📬
23 notes
·
View notes
Text

Actors role playing DID can be identified from differences in brain activation patterns, compared to people with DID - and brain activation patterns depend on whether an trauma holder alter / EP is in charge or a Apparently Normal Part / host - supporting the Theory of Structural Dissociation of the Personality (TSDP).
Multiple brain scan studies support structural dissociation, brain activation differences between alters, brain activation differences between people with DID and healthy controls or trained actors pretending to have DID.
Regions of the brain activated are those known to be associated with self-referencing and sensorimotor actions, but not the regions linked to imagination
Schlumpf YR, Reinders AATS, Nijenhuis ERS, Luechinger R, van Osch MJP, Jäncke L (2014) Dissociative Part-Dependent Resting-State Activity in Dissociative Identity Disorder: A Controlled fMRI Perfusion Study. PLoS ONE 9(6): e98795.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3791283/
#neuroscience#medical research#dissociative Identity Disorder#actually dissociative#dissociativeidentitydisorder#did research#A lot is known about DID#structural dissociation#theory of structural dissociation#theory of structural dissociation of the personality#DID evidence#Schlumpf2014#TSDP#actually traumagenic
59 notes
·
View notes
Text
Re: my tags on the plurality post I just reblogged. I realize this may not be well known information so. Here is the You're Wrong About ep about "multiple personality disorder"
There is a very good transcript available on that page if you are not able to listen to the podcast.
The tl;dr is that the entire phenomenon of "MPD" as we conceptualize it popularly is extraordinarily closely linked to both the phenomena of "repressed childhood abuse memories" and, necessarily, the satanic panic. There is this idea of like, certain types of abuse which somehow cause the "self" to "shatter" in some objective way that can itself be used as concrete evidence OF that abuse... and that's pretty much from 1 book in the 70s that became a huge cultural phenomenon. There's a citation in the podcast transcript here for a book which picks that apart called Sybil Exposed by Debbie Nathan where you can learn more about that specific case. It's also worth mentioning that the "MPD as a result of childhood abuse/repressed memories of childhood abuse" thing actually became a significant issue in legal matters where psychologists were coercing people into inventing repressed abuse memories in order to provide "evidence" to incarcerate people. It was a whole thing.
Here is an excerpt from the transcript that I like:
Sarah: Yeah. And immediately, it becomes just a cultural phenomenon. The author gets bushels of letters, almost all of them from American women and girls. And a lot of them write about feeling like they don't have multiple personality disorder, but they feel like they have all these different selves and different people they are at different times. And it's like, yeah, because being a woman in 1973 means that you in a very obvious way, sociologically are being torn between all of these positions in society. It's like, you want to be a good daughter, but you want to have sex and you want to maybe have a job or stay home and iron a little, I don't know.
Mike: And probably a lot of unaddressed traumas too. I mean, probably a lot of the people had seen terrible things and we're still dealing with the trauma of it. And this gave them somewhat of a voice to their trauma or a lens through which to view their trauma that, you know, something happened to you that day and I'm still dealing with it because it's not like in 1973, society was great at being like, let's listen to people who say that they have trauma.
So like, none of this is to say that DID "isn't real" or that any way of framing having a lot of conflicting parts of oneself or different internal selves or whatever is bad or not useful. It is self evidently very useful for many people.
However. Our cultural understanding of what it means to have "other personalities" specifically AS A RESULT OF TRAUMA, as like, this objective THING that takes place inside your brain when something is DONE to you... is like a VERY culturally specific concept.
And obviously DID/plural/system stuff is often quite distinct from "MPD" style framing of multiple selves. Specifically the psychologist obsession with MPD often revolves around the "solving" or integration of selves, whereas plural/system people I know tend to decry that. Theres many other differences also. HOWEVER I think that learning about the history of how this has been framed and who invented a lot of the commonly accepted "facts" about it is like... really important. In terms of being able to control your own experience of conceptualizing your internal state. Regardless of what framing and models you find to be useful or true. Like... as people whose brains are constantly being pathologized and moralized we should ABSOLUTELY know about & be concerned about patterns of psychological abuse which may play into concepts we have of how our brains work. You know?
And because people are not good at taking posts like this in good faith: I know that people describing having multiple selves has been a thing in many places over many time periods, I think the experience of having more than one 'self' is real (I mean what is a self anyway, per my last reblog, right) and I have friends who are plural/systems/etc. I myself absolutely feel that I have many facets to my "self" which I do often find it helpful to conceptualize as discrete entities when I'm working through stuff. I don't personally find the framing of plurality or systemhood useful *for my self* but you know if you read this blog that means nothing in terms of whether I think it's useful or real for other people.
I just.
As a psych abuse survivor I really want us to be intentional and precise about these things and make sure we have all the information we need to make sure we aren't reinforcing some really narsty shit that's been used to hurt a lot of people.
And also to be like, whose word am I taking for this? What rules do I think this phenomenon follows and why do I think that has to be true? Like it is one thing to put words to an experience or a framework, right, and it is another to go "well the system blog I read says that one self has to be fronting at a given time so now I have to figure out which of my selves is doing that" or whatever like... with ALL frameworks for internal experiences ("diagnoses" lol) I think it's important to be like, am I taxonomizing this by describing how it is for me, or am I trying to sort my experiences into these boxes as described by someone else? And like, the latter is not good for people in general I don't think. And of course in any group or community you will get people who are prescriptive about who belongs in what categories and how your experience has to look in order to belong there or use whatever terminology. And that's not true. You can use whatever frameworks you want and if they don't fit later you can modify or discard them!
Wow I hope this is coherent. Anyway going to go ahead and make this puppy unrebloggable because lmao but I am happy to talk about it with people so please feel free to leave replies or asks as long as no one is yelling at me and accusing me of like, denying experiences. Because I am extremely not doing that. Ty
131 notes
·
View notes
Text
My final comments on CDDs
Anything after this will be deleted or ignored for my own MH
People fully admit they're not taking anything anyone says in good faith and refusing to allow anyone the chance to elaborate, and I'm not down for that
So
Complex: I've stated repeatedly that calling one thing complex is not saying another thing isn't. This isn't a complexity competition. I'm not comparing the complexity of anything, but instead discussing what falls under the HEADER of CDD and why. Whether it's under the HEADER or not means nothing (see quote below).
Parts/alters: fully autonomous with their own continuous sense of self (ANP or ANP-like, based on Nijenhuis' updated ToSD definitions)
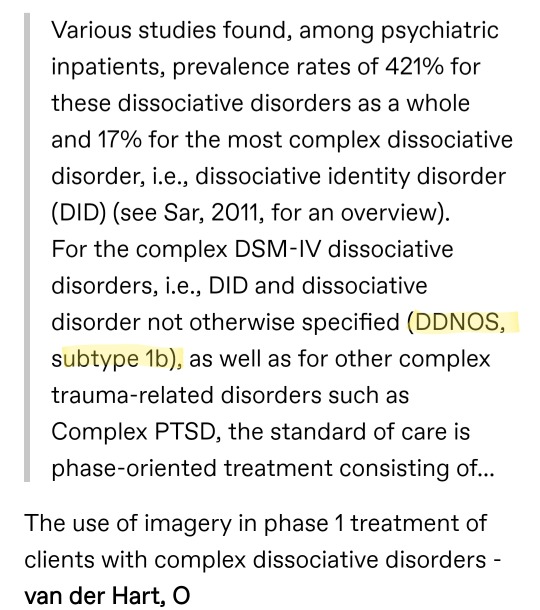
Distinction between OSDD 1a and b as CDDs: I said that OSDD 1 falls into secondary SD (it does, generally, see below), though 1a falls firmly in the middle and 1b falls closer, or into, tertiary. This isn't just my own words, but coming from the authors of the ToSD.
Neither is more complex than the other. In fact, it's suggested that the opposite is true.
-(there's another quote I want to include here, just need to find it)-
In principle, the number of parts of the personality in a given individual has little bearing on whether dissociation is at the secondary or tertiary level. A patient with secondary structural dissociation may have many EPs, while a patient with tertiary structural dissociation may only have two ANPs and two EPs.
The Haunted Self
The theory predicts that overcoming tertiary dissociation in DID is less demanding than overcoming secondary dissociation.
Trauma-Related Structural Dissociation of the Personality, van der Hart, Nijenhuis, Steele
CDD as a term simply encompasses multiple ANPs and multiple EPs. That's it.

In my initial post about OSDD 2, I specifically chose the word "parts" instead of alters because I didn't want to leave out OSDD 1a. I should have used a different word or elaborated more on what definition I was using, and how OSDD 2 did not share that feature.
OSDD 2: is about identity confusion, not alteration. That's coming from the DSM. I said, if you experienced those things and have "parts" or a system or alters, OSDD 1 or DID would override the OSDD 2 diagnosis.

I'm not sure why that's controversial. This doesn't say anything about the complexity of the disorder or the causes behind it. It just doesn't have alters or distinct parts. Why is everyone so angry?
OSDD 1a doesn't have alters: see this post with backup info. This does not mean that I believe OSDD 1a isn't systemhood or that they don't belong in this community. Again, just just a fact about the presentation of the disorder.
BPD and OSDD 1a: I provided sources where I was getting my comparison from. The difference here seems to be levels of amnesia and the... Strength? Of EPs. Does that make sense? In fact, I'd argue trauma-based, dissociative BPD belongs in our communities too for support.
According to the Haunted Self:
However, patients with BPD have lower scores for dissociative amnesia on the DIS-Q than patients with DID and lesser degrees of identity confusion and alteration. These differences distinguish BPD from DID... Some patients with BPD have severe dissociative symptoms, and may actually border on DDNOS or DID. Our clinical observations suggest that dissociative parts in BPD patients have less emancipation and elaboration, and a less distinct sense of self than in DDNOS or DID.
I think that's everything, but if you send an ask with a point you'd like further clarification on, I'll likely add it here, but I won't be directly engaging any further.
Additional edit:
I'm not sure if it's because I live in America's hat, or just my own education, but DDNOS was always described as "not yet" and "not quite". People were diagnosed with DDNOS when they either failed to switch during diagnostic interviewing, or they showed no signs of amnesia, and the vast majority would go on to eventually display both and later be diagnosed as DID.
For example, during initial interviews, we would go into "states" where we believed we were still in active danger. We would cry and panic and completely shut down. If this was an alter, it was little more than a fragment that would manage to completely overpower the rest of us with the sheer... Size of its fear. Recognizing where our life was currently was just... Beyond our grasp in this state, and even if it could be convinced we were safe and calmed to hold a conversation, any progress was undone by the next time it appeared.
I came out of these sessions with only minimal awareness/memory. I knew I'd made a fool of myself, but not much else, though the way I tried to play it off as nothing major implied I had more awareness than I did.
This was the EP, I was told.
Its function was extremely limited and it was driven by emotional distress. Talking to it in any coherent fashion wasn't possible. It couldn't recognize our life as it was currently and was terrified that our abuser was standing outside the office door, waiting for us to finish. All that could be done was to reassure it until the episode passed. It believed it was me, but thought that I was someone else. That sounds confusing, but it was very much a part of me/us, and related to this body, this life, and the trauma we experienced, but somehow thought that we were a little boy, at the same time.
I am not a little boy, and I was little girl at the time that abuse occurred.
Again, confusing, nothing ever makes sense, it's wonderful.
Amnesia wasn't clear enough at this point, not for switching and not for past abuse.
I have never managed to fully switch in therapy, though at home my system is extremely comfortable with my partner. Several years later, long after I had chickened out of further testing, I was in therapy again and my doctor was aware of my previous history with OSDD. I still couldn't let us switch in front of her, but my husband was brought in to talk about some of my other alters.
Some appeared, by description, to be fully fledged ANPs. Aware of our life as it was, vaguely aware of our history, but relatively unbothered and disconnected from the... Fallout of that history. They had likes and dislikes and could hold conversations about current, relative topics, and held their own opinions and ideas about those topics.
For example, all except for one of my ANPs thinks COVID was bad. One of us thinks the world needed a culling to bring to population down before we completely kill the planet. That's fucked up, but he's got opinions and he's damn well going to share them, whether any of us like it or not.
This alter was a mix of an ANP and EP. He was still largely driven by paranoia and anger, and he occasionally found himself confused about days and times or where he was (sometimes even what species he was). He was mostly capable of holding conversations about current topics, though very selfish in that it would always turn back to him and his problems.
The EPs have no idea what COVID is (though if I split one because of COVID, that would be a different story), and have no interest in hearing about it.
I have never once said that OSDD 1a are not systems. They very much are. They still switch and have just as many (if not more) problems as I do. They still have parts.
However, in the context of CDDs, they don't fall into tertiary SD. That all I said.
EPs are not "alters" as they're known in DID because they have little to no awareness of positive life changes and instead remain stuck in trauma. I've lost hope of my little EP ever taking on ANP traits, and instead now focus on internal care for him.
Because he fucking deserves it.
I needed to stop hoping and expecting, because it was putting more strain and stress on him, and I needed to accept the little emotional bundle that he was. He likes mug cakes and watching Marble Olympics after he's been calmed. It helps him relax so we can scoop him back up in a hug and put him to bed, because naps after crying are the best.
In my opinion, all this makes DDNOS/OSDD 1 a pretty useless diagnosis, and I think it should all be part of one single diagnosis. I think OSDD should be in tertiary, regardless of EP/ANP configuration because of the relative emancipation and awareness of EPs in 1a. They may not be as distinct and autonomous as ANPs or alters, but this is clearly part of the same disorder and it goes above and beyond that of the other disorders considered secondary SD.
There have been dozens of recommendations for how this should happen, all with their own problems and positives.
I don't really have any thoughts myself on how to do this.
But I never meant to downplay anyone's experiences. I only meant to discuss the literature on SDs.
#syscourse#actuallydid#actuallytraumagenic#actuallyosdd#did#osdd#ptsd#ToSD#structural dissociation#cdd
60 notes
·
View notes
Last Seen Blogs

clitoris-maximus
Bard of Hearts

takepoyosuper-blog
ドラゴンボールZドッカンバトル

flossmoss
MOSS!

hiya825
恋の王道。

embracing-the-ineffable
Embracing the ineffable mystery