#reproductive services
Text
More pregnant minors forced to leave Ohio to prevent giving birth to their rapists' babies: affidavits
At least two more minors made pregnant by sexual assault were forced to leave Ohio to avoid having their rapists’ babies, according to sworn affidavits filed by abortion providers.
*****
The descriptions include those of three women who threatened suicide. They also include two women with cancer who couldn’t terminate their pregnancies and also couldn’t get cancer treatment while they were pregnant.
Another three examples were of women whose fetuses had severe abnormalities or other conditions that made a successful pregnancy impossible. Even so, they couldn’t get abortions in Ohio.
More needless pain and suffering for "pro-life" supporters to be proud of. But hey, headless fetuses have rights too!
#politics#us politics#republicans#republican hypocrisy#republican#republican family values#abortion#abortion history#abortion resources#abortion rights#rape#suicide tw#health care#reproductive freedom#reproductive justice#reproductive health#reproductive rights#reproductive choice#reproductive services#conservative christianity#pro life#conservatives#conservative#evangelical christianity#evangelical#pro chocie#pro children
16 notes
·
View notes
Text
#pro choice#prochoice#pro-choice#abortion#reproductive health#reproductive justice#reproductive organs#reproductive#reproductive care#reproductive services#reproductive rights#freedom#liberty#choice
2 notes
·
View notes
Text
How to properly take certain reproductive medications safely and covertly.
mel.on.medicine on TikTok: "Go to [Aid Access Dot Org]. ACOG supports self managed medicated ab*rti*n with proper instruction. They advocate for medications to be OTC."
#womens rights#womens health#right to choose#reproductive care#reproductive autonomy#reproductive rights#reproductive freedom#reproductive choice#reproductive cycle#reproductive organs#assisted reproductive technology#reproductive justice#reproductive medicine#female reproductive system#reproductive system#reproductive services#reproductive health#reproductive coercion#medical education#health education#bodily autonomy#bodily sovereignty#reproductive abuse
0 notes
Text
hiiii nobody ever makes posts for West Virginians, so I am going to!
Here’s some resources for abortions in West Virginia.
For people who need to travel to acquire an abortion; yes, abortion is legal in West Virginia.
It is legal up to 21 weeks and 6 days.
Here is a link for funds from charities that will help pay for the abortion itself, or lodging and more.
more resources:
#west virginia#wv#abortion#roe v wade#abortion information#abortion resources#abortion help#health#medicine#reproductive rights#reproductive services
1 note
·
View note
Link
President Joe Biden will direct the federal government on Friday to take steps to protect access to abortion and other reproductive services following the recent Supreme Court’s decision overturning Roe v. Wade.
0 notes
Text
on March 14th 2023, a Polish abortion activist Justyna Wydrzyńska was sentenced to eight months of community service for helping a woman in an abusive relationship access abortion pills
Poland has one of the strictest abortion laws in Europe.
if you can, please consider donating to ADT, the organisation that helps people in Poland access abortion!
edit: i see this post got reblogged into the terf teritory. ADT is trans friendly. please just donate and be quiet <3
#luckily they still can appeal and it's better than jail still but like.#it's so stupid that so much time is wasted on those absurd trials#i know that community service doesn't sound that bad comparing to some other things happening around the world#but still at first she was told she could face up to 3 years in jail#idk those women are heros and make me feel much more safer and less stressed living in Poland#because I know if I ever needed an abortion they would be there to help me#and also 5 dollars is almost an equivalent of a minimum hourly wage in Poland#polish currency is weaker so even 2 dollars count a lot!#and the judge was a woman! same as the leader of the constitutional tribunal that made abortion more illegal#feminism#abortion#poland#human rights#reproductive rights
2K notes
·
View notes
Text
Do people know most paper receipts are harmful to their health?
I'm going to get up on my soapbox for a minute, but do people realize how pretty much everyone is being overloaded with endocrine disruptors like BPA/BPS on a near-daily basis??
I don't think many people understand that ever since most of the world transitioned to thermal paper receipts (cheaper than ink), almost every receipt you handle from the gas station to the grocery store to the Square terminal printer at the local co-op is coated with Bisphenol-A (BPA) or its chemical cousin Bisphenol-S (BPS).
These chemicals have not only been proven to cause reproductive harm to human and animals, they've also been linked to obesity and attention disorders.
Not sure if your receipt is a thermal receipt? If you scratch it with a coin and it turns dark, it's thermal.
BPA/BPS can enter the skin to a depth such that it is no longer removable by washing hands. When taking hold of a receipt consisting of thermal printing paper for five seconds, roughly 1 μg BPA is transferred to the forefinger and the middle finger. If the skin is dry or greasy, it is about ten times more.
Think of how many receipts you handle every day. It's even worse for cashiers and tellers, who may handle hundreds in a single shift. It is also a class issue, since many people who work retail and food service are lower-income and will suffer worse health consequences over time from the near-constant exposure.
Not only that, receipts printed with thermal ink are NOT recyclable, as they pollute the rest of the paper products with the chemicals.
People don't know this and recycle them anyway, so when you buy that "green" toilet paper that says "100% recycled"? Yup, you are probably wiping your most sensitive areas with those same chemicals (for this reason, I buy bamboo or sugarcane toilet paper as a sustainable alternative to recycled paper).
This page from the Minnesota Pollution Control Agency has some good links if you want to learn more.
As consumers, we need to demand better from our businesses and from our governments. We need regulation of these chemicals yesterday.
If you are a buyer or decision-maker for a business, the link above also contains a shortlist of receipt paper manufacturers that are phenol-free.
If you work at a register, ask customers if they want a receipt. If they don't and you can end the transaction without printing one, don't print one!
As a consumer, fold receipts with the ink on the inside, since that's where the coating is. Some more good tips here.
And whatever you do, DO NOT RECYCLE THERMAL RECEIPTS
#i realized the other day that lots of ppl i talked to had no idea this was even a thing#important psa#demand more from your retailers and governments#environment#bisphenols#bpa free#bpa/bps#retail#food service#shopping#working class#capitalism#endocrine disruptors#endocrine disorders#adhd#eco lifestyle#environmental pollution#pollution#toxic chemicals#reproductive health#science#health#environmentalism#eco conscious#human health#consumer goods#consumer awareness#green living#green business#ecofriendly
161 notes
·
View notes
Text
Y’all it’s my first time getting reproductive services (gynecologist) and they let me put my name (aside from my dead name), sexuality, gender, and pronouns. They had options for trans and nonbinary people and it made me so happy. It’s so great because I live in the Bible Belt and the south. I’m definitely less nervous than I was earlier.
23 notes
·
View notes
Text
Dear English doctors - Biological males can’t get pregnant and there is no such thing as a “girl penis”. Please spend less time on worrying about language that appeases narcissistic men and more time improving care for women and babies.
England’s National Health Service (NHS) has put forward a £100,000 contract to create a “gender-inclusive” maternity care training program based on research guided by a trans-identified male who has claimed that men can give birth and that “pre-operative trans women” have “girl penises.”
On December 16, the NHS quietly released an Invitation to Quote for the “Maternity Gender Inclusion Program,” with a listed closing date for pilot submissions set for January 11th, 2023.
The contracted program is set to be rolled out to midwives in maternity departments across 40 NHS Trusts in England, and would be based on the findings of the Improving Trans Experiences of Maternity Services (ITEMS) research project, which was co-authored by a trans-identified male and is alleged to have “significant” flaws in its methodology.
With Woman, a maternity care advocacy coalition, penned an open letter highlighting the “flawed” research within the ITEMS publications, and has called for a complete pause on the contract offering entirely.
Speaking with Reduxx, a spokeswoman from With Woman raised multiple concerns, especially with the entirety of the program’s focus appearing to be on “inclusive” language and not improvements in medical care for a traditionally complex cohort.
With Woman noted that even the Invitation to Quote appears fixed, with the very short contracting and funding window raising suspicion. With Woman indicated their belief that there may be organizations already lined up to take the contract as the time frames are too brief for uninvolved organizations to adequately prepare a pilot.
The ITEMS report, which is being used as a justification for the need for the program, based its findings on the responses of just 121 people. The report determined that “birthing people” were improperly cared for because they were “misgendered,” and made unsubstantiated claims that 30% of “trans parents” secretly gave birth at home with no medical intervention.

The report was co-authored by Dr. Ruth Pearce, a trans-identified male Lecturer in Community Development at Glasgow University.
Pearce played a significant role in the direction of the ITEMS research. Pearce’s work focuses on “trans pregnancy” and “Queer, Trans and Feminist music scenes.”
In an essay posted on to his website, Pearce asserts that he is more attractive and confident than biological women.
“Quite frankly, I bet a whole load of women would love to be as confident and good looking as I am. I’ve got a pretty face, great hair, fantastic legs, and I’ve recently grown some rather shapely breasts.” He is also known for having once fronted a “queer feminist rage” music group through which he sang a song about his scrotum.
In an August 2022 video titled “Reproductive Justice for Trans People With Ruth Pearce and Francis White,” Pearce explains the focus of his work on ITEMS, policy and language surrounding “trans birth” and the need to highlight transgender people having children to counter the claims that a “trans child” may not reproduce, and to create media that contradicts Abigail Shrier’s claims that child transition can lead to “irreversible damage” of fertility.
Pearce called attention in particular to a phenomenon known as Rapid Onset Gender Dysphoria, which was coined by Lisa Littman and referenced by Jungian analyst and author Lisa Marchiano in a 2017 academic article titled “Outbreak: On Transgender Teens and Psychic Epidemics.”
In the article, Marchiano examines the role of social media in the sudden rise in teens claiming a gender identity, stating: “a young person’s coming out as transgender is often preceded by increased social media use and/or having one or more peers also come out as transgender.”

Pearce mocked the concept of children learning of transgender identities on social media, but later contradicted himself by discussing the issue in the presentation segment titled “We Are the Virus: Reproduction via Social Contagion.”
In the segment, Pearce asserted the need to help transgender-identifying people to not only sexually reproduce, but also to “socially reproduce” by means of altering medical language and policy to introduce the idea of transition to children and adults as a form of “reproductive justice,” thereby creating more transgender people.
In the video, Pearce acknowledged that social contagion is the method by which transgenderism proliferates, stating: “Alexis Davin noted that the very process that Lisa Marchiano and Abigail Shrier described as a social contagion is the means by which trans people engage in a form of social reproduction. We become visible to one another and introduce one another to a language that makes sense of our lives and our needs.”

Later in the seminar he continued, “I’ve been thinking a lot about social contagion because it’s the language of the anti-trans movement. But… the exact thing they’re describing is the exact means by which we reproduce ourselves.”
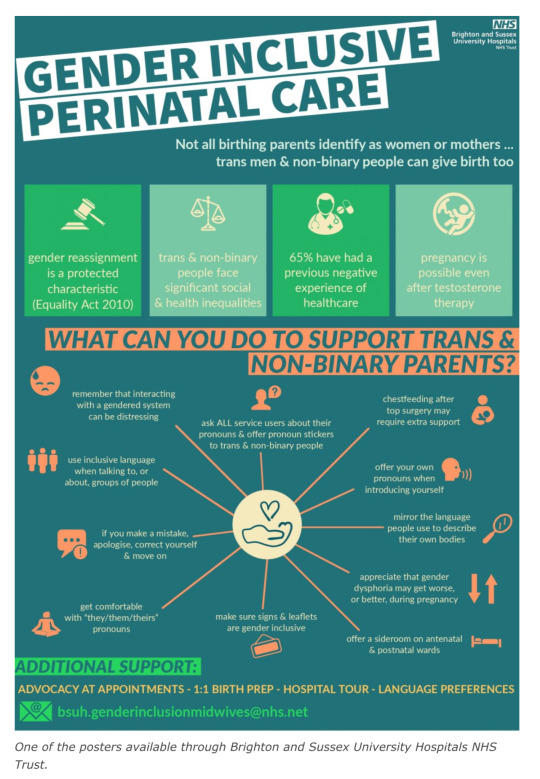
During the seminar, Pearce described the work he did with Brighton and Sussex University Hospitals (BSUH) NHS Trust, arguing for the need for “Gender Inclusive Language” to create “Language as Possibility” and posters that act as apparent recruitment advertising for the political transgender movement. Pearce elaborated by saying, “in Brighton and Sussex University Hospitals, that’s a really interesting example of queer spaces of care being created through an institution rather than through more radical networks.”
Pearce’s involvement with the ITEMS research, as well as its use to justify an NHS maternity program, comes less than one year after NHS negligence was found to have been responsible for the needless deaths of over 200 babies and 9 mothers at at Shrewsbury and Telford NHS Trust. According to internal investigations, “repeated failures in the quality of care and governance” was to blame for the deaths, which spanned over 2 decades, with an additional 1,486 families and 1,592 incidents being recorded as a result of inadequate maternity care oversight.
Reduxx has previously revealed how errors and confusion arose due to the use of inaccurate medical language which led to midwifery students at Napier University in Edinburgh being taught how to care for males giving birth through penises and prostates.
According to a course workbook, students were advised: “It is important to note that while most times the birthing person will have female genitalia, you may be caring for a pregnant or birthing person who is transitioning from male to female and may still have external male genitalia.”
#England#England’s National Health Service (NHS)#Trans Identified Male talking about maternity care#Men can’t have babies#With Woman#“Maternity Gender Inclusion Program#Improving Trans Experiences of Maternity Services (ITEMS)#Dr Ruth Pearce is a man#Dr Ruth Pearce is another TIM who thinks he is better than actual women#Reproductive Justice for Trans People With Ruth Pearce and Francis White#Gender identity and social contagion#It’s bigoted for critics to mention the link between social media and gender identity#But it’s ok for trans people to call gender identity a social contagion
102 notes
·
View notes
Text

#us politics#2022#us supreme court#scotus#dobbs v. jackson women’s health organization#roe v. wade#planned parenthood v. casey#taxes#tax returns#irs#internal revenue service#us government#abortions#abortion bans#income tax returns#fetal viability#personhood#reproductive health#reproductive rights
344 notes
·
View notes
Text
A Fake Abortion Clinic Tried to Sabotage My Pregnancy Termination
#politics#us politics#republicans#republican hypocrisy#republican family values#republican#reproductive health#reproductive choice#reproductive justice#reproductive rights#reproductive freedom#reproductive care#reproductive coercion#reproductive services#health care#conservative christianity
12 notes
·
View notes
Text
A ‘twisted’ experience: How KY’s abortion bans are depriving pregnant patients of health care
BY ALEX ACQUISTO
On the way to her 20 week ultrasound, Amy English texted her family group chat inviting guesses on her baby’s biological sex.
“Baby boy English muffin!” her father in-in-law texted.
“I thought boy at first but I’m thinking girl now,” her sister-in-law said. “My official guess is a girl :).”
It was December 28. Earlier that morning, Amy, 31, her husband David, and their 20-month-old daughter Annie had celebrated a belated Christmas at their house in Louisville with family visiting from out of state.
Amy and David had planned this pregnancy, and it was, in a way, perfectly timed. Their baby’s due date was five days after Annie’s birthday. Her children would be two years apart almost exactly to the day — a reality Amy was “ecstatic about.”
Sitting in a fluorescent-lit room inside Baptist Health Louisville, Amy looked for familiar shapes on the screen as an ultrasound tech probed her abdomen. Familiar with radiology in her career as a physical therapist, she has a baseline understanding of how to read ultrasounds: gray shapes usually indicate fluid, and bone shows up as white.
Amy remembers seeing her baby’s arms, legs and the curve of its back. But there was no recognizable outline where the skull should be.
“I couldn’t see the top of my baby’s head,” Amy said in an interview with the Herald-Leader. “I kept waiting for the tech to move the probe in a way where we could see what we should be seeing. I could tell she was searching for it, too.”
Amy had also learned in school about anencephaly, a severe fetal birth defect impacting the brain and skull. A lack of folic acid early in pregnancy increases the likelihood of this happening. This possibility flashed in her mind but she quickly batted it down; she’d been taking her prenatal vitamins, rich in folic acid, for months even before discovering she was pregnant.
The tech paused, then spoke.
“What we’re looking for here is an outline of the baby’s head, and right now I’m not really seeing that,” the woman explained before calling in Amy’s longtime OBGYN.
Over the next few minutes, Amy remembers the room blurring as she heard her doctor use the word “acrania,” which is when a fetus matures through pregnancy without ever developing parts of its skull. It can spur anencephaly, when the brain, too, is underdeveloped and partially missing. Pregnancies with either of these conditions are nonviable.
Amy’s baby, which they learned was a boy, had both. He would not survive into childhood, likely not beyond a few minutes after birth.
This, alone, was devastating news. Her dismay was compounded the next day when she learned that terminating her nonviable pregnancy, even by way of an early induction — a commonplace and provider-recommended method of treatment for such a diagnosis — couldn’t happen.
Even though Amy’s baby would never survive outside her womb, the pregnancy still had a fetal heartbeat — a technicality, considering the diagnosis. Coupled with the lack of immediate threat to her health, her doctors explained they couldn’t induce labor, much less give her an abortion. Kentucky laws forbade it, they said.
“I don’t know what was more shocking: to find out the baby had anencephaly, or that I would have to go out of state to get this care,” Amy said.
Kentucky’s abortion bans do not legally permit the standard of care treatment for a nonviable pregnancy like Amy’s. As a result, doctors must refer patients needing otherwise medically-recommended terminations out of state in droves, along with people desiring elective abortions, according to interviews with seven providers across four hospital systems. Providers who terminate pregnancies in violation of the trigger law can be charged with a felony in Kentucky.
Though this scenario is increasingly common statewide, it’s one arbiters of the state’s laws have yet to remedy, and one lawmakers are not publicly working to resolve.
Kentucky’s trigger law, enacted in late June 2022, criminalizes abortion except to prevent a “substantial risk of death,” or to “prevent the serious, permanent impairment of a life-sustaining organ of a pregnant woman.” The fetal heartbeat law also includes these exceptions but otherwise bans abortion except in a “medical emergency” once fetal cardiac activity begins, usually around six weeks.
Any time a pregnancy is terminated, each law requires a provider to document in writing why it was necessary to, in the case of the six-week ban, “prevent the death of the pregnant woman or to prevent a serious risk of the substantial and irreversible impairment of a major bodily function of the pregnant woman.”
The law permits the Cabinet for Health and Family Services to audit any licensed health care facility to make sure its abortion reporting requirements are “in compliance” with the law.
Both bans allow physicians to use their “reasonable medical judgment” when deciding whether pregnancy terminations are medically necessary. But providers interviewed for this story said that guidance is antithetical with the rest of the law’s limits, which only permit terminations in medical emergencies. There are no exceptions for fetal anomalies, or for the gamut of conditions that may make a pregnancy nonviable but don’t pose an immediate or emergent health risk to a pregnant person.
Moreover, the lack of uniform guidance from the state on what’s considered an emergency means definitions across hospitals sometimes vary, the Herald-Leader found. This has created a legal thicket for health care institutions. As a result, the final say on some critical medical decisions affecting pregnant patients is falling not to medical experts, but to hospital attorneys and administrators, who are worried about legality, liability and reputation.
The Herald-Leader asked the University of Kentucky, UofL Health and Baptist Health for insight into how their respective risk management teams and providers are navigating the laws. None responded to multiple questions about respective protocols for deciding when terminations are legally defensible, or how risk management teams, administrators and providers go about deciding.
“Clinicians have a responsibility to provide compassionate, evidence-based care and counsel to their patients, and also comply with the law,” Baptist said in a statement.
“UofL Health is committed to provide comprehensive health care to all its patients and their families,” UofL said in a statement. “In the case of a nonviable pregnancy that poses a health risk to the mother, we explain options for care while complying with all state and federal laws.”
“Although we cannot discuss when or how our legal counsel gives advice,” UK HealthCare said, “in Kentucky, state law prohibits the University’s physicians and staff from performing abortions except when the mother’s life is in danger. In the case of a nonviable pregnancy, our health care staff work with patients to determine the best course of care for the patient that is consistent with state and federal law.”
‘WE COULD NOT PROVIDE THIS SERVICE HERE’
The morning after Amy learned her baby likely had a fatal birth defect, the diagnosis was confirmed at a second ultrasound with a high-risk specialist. The buoyancy and excitement of the prior day was replaced with dread and grief. Amy remembers the quietness of the room during the second ultrasound, the hollow clicking of the keyboard keys and the intermittent clicking of the computer mouse.
Baptist Health refused to make Amy’s doctor available for an interview. But their conversation was outlined in Amy’s medical records, which were provided to the Herald-Leader.
“I discussed this finding with the patient and offered my sincerest condolences — that this was not compatible with life and that I am so sorry she and her husband are in this situation,” the doctor wrote in her notes. “She was understandably tearful.”
Amy listened as her provider explained her two options: Amy could carry her son to term and deliver him via C-section. He would immediately be taken to palliative care, where he would live a few minutes, maybe hours. Grief counselors would be on standby.
Her second option was to terminate the pregnancy early by way of an abortion or preterm induction. “Choosing not to continue the pregnancy: we discussed that this is also a loving choice for a baby that will certainly not survive,” her doctor wrote.
Pre-trigger law, termination under these circumstances would’ve happened in a hospital, and Amy’s health insurance likely would’ve covered it.
“No part of me wanted to be pregnant anymore,” Amy said. “Every flutter and kick he gave felt like a literal gut punch reminder that I would never get to take him home.”
Strangers were already approaching her at the grocery to ask to touch her stomach. Her patients at work often asked how far along she was. It seemed emotionally unthinkable to continue subjecting herself to a life where, at any moment, she would be forced to repeat that her growing body was nurturing a baby that wouldn’t live, she said.
Termination was what Amy wanted. She erupted into sobs when her doctor told her that under her current circumstances (her life wasn’t immediately threatened, and there was still a fetal heartbeat) it wasn’t an option.
“We discussed that due to our current Kentucky laws, we could not provide this service here,” her doctor wrote in her records.
“I’m sorry, I’m sorry, I’m so sorry,” Amy remembers the specialist saying.
She gave Amy a list of hospitals and clinics in surrounding states that might be able to terminate her pregnancy. Her doctor recommended calling Northwestern Memorial Hospital in Chicago, or another clinic in Illinois, where abortion is widely available.
“Am I just supposed to Google the number, call the front desk and ask, ‘How do I get an abortion at your hospital?’” Amy remembered thinking.
Over the next few days, she, her husband and sister-in-law cold-called a handful of clinics to request a dilation and evacuation abortion, common in the second trimester. But a combination of abortion restrictions in Indiana and Ohio, including gestational limits on when abortion is legal — Amy was 21 weeks along at this point — left her with few options.
Then, Amy’s sister, a nurse anesthetist at Northwestern Medicine Kishwaukee Hospital in Dekalb, west of Chicago, stepped in. Her hospital lacked the equipment for a D&E, but they agreed to induce Amy.
On January 4, after driving close to 400 miles, Amy was induced and gave birth to a son she and her husband named Solomon Matthew. He didn’t cry. His heart beat for about two minutes before it stopped.
‘NOT KNOWING WHAT TO DO’
The Republican-led General Assembly has made no moves to amend or further clarify either abortion ban since both took effect seven months ago, even though the combined impact has harmed patients, doctors have told lawmakers.
The Kentucky Supreme Court still hasn’t issued a preliminary opinion on whether either law infringes on a person’s constitutional right to bodily autonomy and self-determination. Deciding so would temporarily block one or both bans from being enforced. Convened for a regular session through March, the Republican supermajority has yet to file any bills related to reproductive health care access and likely won’t until the high court weighs in.
In the meantime, there’s disagreement about whether or not either ban infringes on providers’ ability to dole out the standard level of care to pregnant patients.
Kentucky Supreme Court Justice Michelle Keller and former Deputy Chief Justice Lisabeth Hughes raised this point during November oral arguments in the pending court case from the state’s two outpatient abortion clinics challenging the constitutionality of both laws.
The trigger law “doesn’t recognize an exception for women who are under the care of a physician who tells them that the standard of care would be to terminate the pregnancy,” Hughes told Solicitor General Matt Kuhn, arguing on behalf of the Attorney General’s office.
As a result, “What’s really happening is physicians in (hospitals) all over the commonwealth are calling the risk managers and attorneys for the hospitals not knowing what to do,” Keller added. “You’re obfuscating what this trigger statute says. There isn’t a strict life of the mother exception.”
The law’s proponents, including Republican Attorney General Daniel Cameron, have cited the provision in the law that allows for use of “reasonable medical judgment” as protecting doctors’ autonomy, and that any challenge to that fact is overblown.
“The law has an explicit health exception, (which) depends on a ‘reasonable medical judgment’ from physicians,” Kuhn told Kentucky Supreme Court Justices that day. There’s been “a lot of misinformation” suggesting the law doesn’t adequately protect a pregnant person’s health, he said, citing two advisories Cameron’s office has issued since both measures took effect. Both clarify that in vitro fertilization, and abortions as treatment of miscarriages, preeclampsia and ectopic pregnancies don’t violate the law.
As for the host of other conditions not mentioned, “we are continuing to work with Kentucky doctors giving guidance on that,” Kuhn said.
But no written evidence of that guidance appears to exist. In response to an open records request from the Herald-Leader, Cameron’s office said this week it had no written or electronic records of communication between the Attorney General’s office and licensed health care facilities or providers regarding the trigger law or six week ban.
‘AN UNNECESSARY PHYSICAL AND PSYCHOLOGICAL RISK’
It was mid June when Leah Martin, 35, discovered she was pregnant with her second child.
Pregnancy at ages 35 and above is considered geriatric. Aware that her age meant she faced a heightened risk, she opted for genetic testing early on to gauge any abnormalities.
Her first ultrasound didn’t raise any alarm. At just over nine weeks, Leah took a prenatal genetic test. The results a week later showed “low fetal fractal numbers,” she said in an interview.
That result, her OBGYN told her, could mean there hadn’t been enough material collected to show a clearer result. It could also signal an abnormality.
Leah, wanting to be judicious, got a more exact genetic test just before 12 weeks. She quickly learned her fetus had triploidy, a rare condition that causes the development of 69 chromosomes per cell instead of the regular 46. It causes not only severe physical deformities, but triploidy stunts development of crucial organs, like the lungs and heart. It means a fetus, if it even survives to birth, will likely not live beyond a few days.
What’s more, Leah was also diagnosed with a partial molar pregnancy, which causes atypical cells to grow in the uterus and, as Leah’s doctors told her, could lead to cancer.
It was mid-July, and Kentucky’s trigger law and six week ban had been in effect for barely two weeks. Leah was familiar enough with what both laws restricted and assumed that because her pregnancy could cause her cancer and was nonviable, she would lawfully qualify as an exception.
So, she weighed her options with her doctors at Baptist Health Lexington, who included Dr. Blake Bradley, her longtime OBGYN.
Similar to Amy’s diagnosis, Leah’s doctors told her that even if she opted to carry the pregnancy to term, her baby “would live a short life in palliative care, most likely never leaving the hospital. It would really be a quite painful existence,” she said.
“I have a 2-year-old at home, and I’m 35, weighing how I would like to expand my family. It seemed like the safest option for me and the compassionate choice for my unborn child was to terminate the pregnancy,” she said.
Like Amy’s, a medically-necessary abortion under these circumstances would typically take place at a hospital, doctors interviewed for this story said. Leah’s health insurance had already agreed to cover it. It was also the quickest way to help Leah to her end goal: getting pregnant again in order to birth a child that would survive.
It was July 21 and Leah was just over 12 weeks pregnant when she learned that Baptist’s legal counsel had blocked her doctors from giving her a dilation and curettage abortion.
“I was told the hospital refused to perform the procedure while the case was being litigated. I was dumbfounded,” Leah said. Hospital lawyers cited an ongoing lawsuit from Kentucky’s two outpatient abortion providers that’s pending before the Kentucky Supreme Court.
According to Leah, hospital providers, relaying the message from administration and risk management, reportedly said if her fetus died on its own, doctors would be able to terminate her pregnancy. But their hands were tied as long as it had a heartbeat.
“People minimize that pregnancy, even under its best circumstances, is associated with life-threatening risks, life-altering risks and emotional impacts,” Bradley told the Herald-Leader. “So, to compel a woman to continue a pregnancy that is by everyone’s assessment, doomed, by definition places that woman at an unreasonable and unnecessary physical and psychological risk, period.”
Baptist Health refused to make Leah’s high-risk doctor available for an interview.
The following Monday, July 25, Leah had an ultrasound at the hospital to confirm what she already knew. As an ultrasound tech probed her abdomen, a wheel of dizzying emotions spun in her head: she desperately wanted a baby, but she didn’t want to birth a child into a painful existence.
Already faced with a gutting dilemma, she felt further burdened by having such an intimate choice ripped from her. And she was furious at now being forced to remain pregnant despite there being no chance for survival, despite the risks continuing such a pregnancy posed to her own body.
She remembers staring at the ultrasound screen waiting to hear the muffled heartbeat of her fetus, racked with guilt because she hoped she wouldn’t.
“It was such a twisted experience being pregnant with a baby I desperately wanted, lying there hoping its heart had stopped,” she said shakily. “It was horrible to have to wish for that in order to receive care. It just felt so unsafe and cruel.”
Leah had already arranged to drive to Chicago to get an abortion when a Jefferson Circuit judge issued a preliminary injunction on July 22, temporarily blocking the state from enforcing both bans. She immediately called EMW Women’s Surgical Center in Louisville — one of the plaintiffs in the lawsuit against the state — and made an appointment.
On Wednesday, July 27, almost 13 weeks pregnant, Leah paid $950 out of pocket for her abortion. Her insurance wouldn’t cover it, since it was considered elective. The following Monday, the Kentucky Court of Appeals overturned the circuit court injunction, reinstating both abortion bans.
After Leah’s abortion, she sent a message to her high-risk doctor. Her doctor responded the following day. Leah shared that correspondence with the Herald-Leader.
“You’ve been on my thoughts a lot,” her doctor wrote. “Words cannot express the dismay I feel right now. I’ve spent my whole adult life learning how to care for mothers in heart wrenching or dangerous situations like yours, and the politics now make it not only impossible, but to work to take care of patients like they deserve — with compassion and science — in these horrible situations is wrong and immoral.”
“I hope your procedure yesterday was smooth, though I know it was hard,” her doctor wrote. “I’m so sorry we could not (were not allowed, rather) to take care of you here.”
#us politics#news#Kentucky Herald-Leader#2023#abortions#Abortion bans#anencephaly#acrania#nonviable pregnancies#kentucky#fetal heartbeat laws#Cabinet for Health and Family Services#dilation and evacuation abortions#Kentucky Supreme Court#Daniel Cameron#triploidy#palliative care#dilation and curettage abortions#Kentucky Court of Appeals#reproductive rights#bodily autonomy
68 notes
·
View notes
Text

📣 Exciting news from Resistbot!
They've launched a new feature called approval polls. Now you can express whether or not you would re-elect each of your federal elected officials.
This is an important step in making our voices heard and holding our elected officials accountable. Let's use this tool to let them know what they need to do to earn our votes! Try it out by texting "approval" to the bot. Your input matters!
Resistbot continues to innovate for civic engagement. I look forward to seeing more developments like this in the future. Share your thoughts and feedback in the general discussion. Let's make a difference together! 🗳️✨
📱Text APPROVAL to 50409 and earn FREE Coins!
I just tried it out and here's my feedback:
For President Biden, I might vote to reelect him because he took steps to repeal discriminatory policies like the Trans Ban (DADT 2.0). While I appreciate this progress, I hope to see a more critical approach to U.S. support and funding for Israel. Even still, Trump would be worse for Palestine. Vote Blue No Matter Who, until we get Ranked Choice Voting.
For Senator Murkowski, I approve of her reelection because I appreciate Senator Murkowski's dedication to child development and her progressive stance on LGBTQ+ rights. However, I wish she would support stronger gun regulation and prioritize green initiatives more consistently. I'm encouraged by her stance against Trump's policies.
For Senator Sullivan, I strongly oppose Senator Sullivan due to his positions against reproductive rights, transgender rights, and affordable healthcare. Additionally, his denial of climate change, support for gerrymandering, and alignment with extremist views surrounding the January 6 insurrection are deeply concerning. He is an un-American Trump Sucker and I need him out of my chair this instant.
For Rep. Peltola, I approve of her because I appreciate Senator Peltola's support for COVID-19 proposals and her progressive stance on marriage, children, LGBTQ+, and transgender rights. However, I believe there is room for improvement in her support for military service members, veterans, and moderate gun regulation.
#trans ban#DADT#palestine#Vote Blue No Matter Who#Ranked Choice Voting#early child development#President Biden#Senator Murkowski#Senator Sullivan#Mary Peltola#LGBTQ+ rights#gun regulation#green initiative#anti trump#reproductive rights#trans rights#affordable healthcare#climate change#gerrymandering#jan 6#insurrectionist#covid#marriage equality#military service members#veterans#Resistbot#Civic Engagement#Approval Polls#Election 2024#Government Accountability
4 notes
·
View notes
Text
ah yeah it's saturday and the school year's started. explains the protesters on my way to the metro station
#i passed someone holding a 'washington commits infanticide' side and i was just like. ah sidewalk prayer is back on again yeah?#*lives next to a planned parenthood#*school has a regular and well-attended 'sidewalk prayer' event on saturdays where people go and pray the rosary/protest outside it#happened during the summer too but attendance massively ticks up when students are on campus#pp posts up volunteers outside with hi vis 'escort' vests to help people Trying To Get Healthcare avoid too much harassment every week#i guess the people who just show up to pray are annoying but not disruptive. the people with angry signs and shouting suck ass though#it's annoying that they all treat pp like an abortion factory still though when that place does literally so many other things#they have a big banner out front advertising primary care services#and they'll see you for migraines. internal medicine. stuff like that. not just reproductive health although of course that's important#like honestly of i didn't already have an appointment booked across the city i'd probably move to seeing doctors there#hell of a lot more convenient. even if you have to deal with the demonstrators outside. but at least they're usually constrained to saturday#i wanna talk about me
10 notes
·
View notes
Text
me wanting to make a cybertronian reproduction appreciation zine (wow that's a mouthful) but having my own qualms with certain headcanons that would surely find their way into the project.. 🥲
i mainly want to do it because of negativity surrounding the concept of mechpreg. i want a more positive and designated space for us to enjoy it. the project could include any method of reproduction, not just mechpreg (while remaining sfw) and even any pieces with happy creators and their sparklings! it doesn't just have to be reproduction based, it can go into family dynamics!
just want something fun for my maternal ass yk. please tell me what you think! 🥺🥺
#mechpreg#i can probably get past my dislikes for the sake of positivity bc i honestly really want to do this#and donate to a good cause that works on reproductive health n services#cybertronian reproduction appreciation
87 notes
·
View notes
Text
"The Department of Health and Human Services on Monday released guidance saying that health providers who perform abortions in emergency situations are protected under federal law regardless of what bans are in place in their states.
Why it matters: The move is aimed at giving assurances to abortion providers who fear they could be prosecuted for offering potentially life-saving care.
Details: The Emergency Medical Treatment and Active Labor Act "protects providers when offering legally-mandated, life- or health-saving abortion services in emergency situations," said HHS in a guidance issued via the Centers for Medicare and Medicaid Services."
Read the full piece here: https://www.axios.com/2022/07/11/abortion-emergency-biden-providers
#abortion#abortion rights#abortion access#feminism#feminist#hhs#health and human services#reproductive freedom#reproductive rights
85 notes
·
View notes
Last Seen Blogs

rnjrsupportsquad
Supporting Team RNJR EST 2016

tues-dayy
Tuesday

endless-starlight-legacy
endless_starlight

hoke53
WEATHERING THE STORM

dicktofen
MOVED TO HERECOMESNAYA