#does disability? do we Need to pathologize the human condition?
Text
sometimes someone seems autistic and they're literally. just Asian. western medicine does this.
#signs#disorder#stick out#this is a critique#btw#like does neurodivergence need to necessarily be pathologized?#does disability? do we Need to pathologize the human condition?#idk maybe#we can def do smn Better tho....that facilitates more understanding and not just... separation (at best)#anyway thinking ab this lately just cause like.#so when i really figured my shit out in undergrad. i realized i want to go into health and healing#but i wanted a huamnistic perspective and not a pathologizing one#bottom-up so to speak. to appreciate the variety of humanity and alleviate suffering within that framework#so i went into communicationd with concentration in culture and disability#and in this specific instance some of autism (truly i don't think they are Symptoms bc they do not...#like. these traits are not inherent to the condition we just often display them but theyre secondary#they dont describe the core of the condition (which is just a particular neurosystem--everything else is secondary)#but is inherently smn culturally abnormal (theoretically harmful or at least disruptive)#common autistic behaviours like avoiding eye contact; low affect; high or low volume; reservedness#these are Common Traits of Asian cultures! (#obviously Most of the world is Asian so there is CONSIDERABLE variation. but the pt being that these are only abnormal from a WESTERN pov#(also I'm in the United States so i am in particular thinking about Asian Americans but this also applies to like intl interaction)#(like... idk a tiktoker from Hong Kong that ppl think is Autistic who may be allistic)#(also I'm not tryna say only westerners/usa be autistic and Asians can't LMAO)#(its a Human neurotype. just the things that depend on what is circumstantially normative)#anyway.......... hello to the 3 ppl who will see this#actually autistic#mine#critical cultural studies#coms
9 notes
·
View notes
Text
A Conversation About Demedicalization and Disorders
Let's talk about demedicalization. What is demedicalization? The Open Education Sociology Dictionary defines demedicalization as "The process by which a behavior or condition, once labeled 'sick', becomes defined as natural or normal." It is the process of normalizing a trait of the body or brain or behavior as a normal variance of human existence, rather than a pathological variance in need of treatment or correction.
Put simply, it is no longer looking at something as a sickness in need of treatment, but rather just another way of existing.
Some background info that is needed: the social and medical models of disability.
The medical model posits that the existence of disability is predicated on inherent pathological differences in the bodymind, that it is active physical limitations, some of which can be treated or "corrected", that make a person disabled.
The social model, on the other hand, states that is is a societal lack of access and accommodations that disables a person, and that a person would no longer be functionally disabled were these access barriers to be removed. Keep in mind that this does not mean they believe that people would not still have "impairments" that affect how they are able to function, but that it defines disability as the disadvantages caused by an ableist society treating impairments as needing to be "fixed" rather than accommodated. I defines being abled as being able to participate in society to the full extent an impaired individual wishes to.
I believe in a mixed social-medical model. I believe that some conditions are inherently disabling and that seeking medical treatment for them, while it should be up to disabled individuals, is helpful and good. My ADHD, for example, will still limit my participation in society to the extent I want to, without medication. You could consider medication an accommodation, but there's also the example of my chronic pain and fatigue and POTS that often keeps me housebound or bedbound. There may not be a treatment for that, and I cannot fully participate in the world around me because of that.
"Ultimately, the social model of disability proposes that a disability is only disabling when it prevents someone from doing what they want or need to do."
I am actively prevented from doing what I want or need to do by an inherent feature of my body that no amount of accommodation can allow for. However, some of my conditions would not be disabling with proper accommodation - my autism, for example, I don't generally consider disabling because the people and structures around me DO accommodate for it.
So why is demedicalization helpful or necessary, and how is is applied?
Well, three psychological examples: autism, psychosis, and schizophrenia.
Autism is currently, in the DSM, called autism spectrum disorder. However, autism is a neurotype, and many autistic people do not feel that autism inherently causes them distress or dysfunction, and is therefore not disordered. That is why many of us call ourselves autistic people or say we have autism, rather than ASD. There has been a push for years for the diagnosis itself to be changed to not contain the word "disorder", and to allow for informed self-diagnosis.
Informed self-diagnosis is also an important part of demedicalization, especially of neurodivergence. It says "someone doesn't need a doctorate to know themselves and their own experiences well enough to categorize and classify them. Good research and introspection is enough to trust a person to make the call, and labeling oneself as a specific kind of neurodivergence is harmless, even if they later find out they were wrong.
Psychosis is the next example. There is a growing movement that I've talked about before: the pro-delusion movement. Not everybody experiences distressing delusions, and even when they are distressing, this movement says that only the individual experiencing them has the right to decide whether they should be encouraged or discouraged. It states that it is a violation of autonomy to nonconsensually reality check (tell someone their delusions are not reality) someone, and that as long as a person is not harming others, they can do as they like with their delusions.
This is an example of demedicalization. Treating delusions as something not to be suppressed with medication or ignored or "treated" or "fixed", but as simply another, morally and "healthily neutral" way of existing outside homogenous neurotypical norms.
Finally plurality. Now what's key here is that demedicalization does not mean saying a thing can NEVER be disordered. In fact, that's why I made this post. I saw someone the other day say that they felt their aromantic identity was disordered. Initially, I balked, thinking they were internally arophobic, but I listened to what they had to say. Essentially, they expressed that the identity was never inherently disordered, but that it caused them distress and dysfunction and so they experienced it as such, and crucially, that wasn't a morally bad thing or something they felt they had to correct.
Because here's I think what gets left out of discussions on demedicalization: demedicalization also means no longer treating disorders as something that inherently have to be treated or fixed, that disorders can simply exist as they are if the person with a disorder so chooses; and that anything can be labeled a disorder if it causes distress and dysfunction without being inherently disordered AND without needing to be treated.
And conversely, this means that if you experience something as disordered, demedicalizing it means that you do not have to meet an arbitrary categorical set of requirements to seek treatment, but can do so based on self-reported symptoms. Treatment cannot be gatekept behind a diagnosis that only a "qualified professional" can assign you.
This means if someone wants to, they can label their autism as disordered, but it is never forced on anyone. If someone feels ANY identity - neurodivergent, disabled, queer, alterhuman, paraphilia, whatever - is disordered, they can label it as such, but they also don't have to. There are no requirements to follow through with "treating" anything you label a disorde, either. No strings attached, just the right to self-determination and the right to autonomy hand in hand,
So, back to plurality. You essentially end up with three aspects of demedicalization. You have nondisordered plurality being normalized, you have dissociative disorders that systems can choose not to pursue treatment for without judgment or coercion, and you have disordered systems that can pursue treatment for dissociative symptoms without receiving a difficult-to-access diagnosis. Based on their experiences, they can choose to label themselves as having DID, OSDD, UDD, or related disorders, or to forgo the label and simply seek treatment for whatever distress or dysfunction the disorder is causing.
"But without a specific diagnosis, what if they pursue the wrong treatment and it harms them?"
This is where the importance of recognizing self-reported symptoms as valid comes in. If an OSDD-1b system that hasn't labeled themselves or receives a diagnosis reports that they don't experience amnesia, they won't receive treatment for amnesia.
And since symptoms can mask, if a DID system reports not experiencing amnesia, they simply do not become aware of it or receive treatment for it before they are ready, which is a good thing because recognizing certain symptoms before you are ready to deal with them can be destabilizing and dangerous. More awareness of dissociative disorders will also make it easier for systems to adequately recognize those symptoms, and this isn't saying that someone else can't suggest it to the system experiencing it. It's simply saying the person experiencing a disorder takes the lead and is centered as the most important perspective.
I consider myself to have several disorders and several forms of nondisordered neurodivergence. My BPD is disordered but I am not treating it because I have healthy coping skills already. Same with my schizophrenia. My narcissism, on the other hand, is simply a neurotype. My plurality is both - the plurality itself isn't disordered, but I do have DID on top of it.
A last example, this one physical, of demedicalization: intersex variations. The intersex community has been pushing to recognize that intersex variations are natural variations in human sex, and not medical conditions that need corrected. This doesn't mean that any unpleasant symptoms related to an intersex variation can't ever be treated - in fact, it's important to the community to have that bodily autonomy to access whatever reproductive healthcare is needed - but it does mean treating our sexes as inherently normal and NOT trying to coercively "correct" them.
So in summary, demedicalization is fundamentally about autonomy. It is about considering natural human variations as such, rather than as sickness to be cured, about letting people determine for themselves whether any aspect of themselves is disordered, and the decision on whether or not to pursue treatment for anything being theirs alone. It is about trusting people to be reliable witnesses and narrators of their own subjective internal experiences, and about never forcing anyone to change any aspects of themselves, disordered or not, that aren't harming others. In short, it is about putting power back into the hands of disabled people. And that is what this blog is all about.
#unitypunk#long post#demedicalization#autonomy#social model of disability#medical model#disorders#intersex#self diagnosis
117 notes
·
View notes
Text
FrankensteinWIP - intro
Working title: „Offspring of Unhappy Days”
Genre: adult literary horror
Subgenres: dark academia, queer romance, grounded sci-fi
Themes: academic fraud and ethics, co-dependent relationships, PTSD, fear of death, loneliness, disability/neurodivergency, trans/queer experience in Eastern Europe
Comps: “Leech” by Hiron Ennes, “These Violent Delights” by Micah Nemerever, “Secret History” by Donna Tartt
Protagonist: Kristian Kalina, PhD student, late twenties; trans, queer, autistic; he/him
Short description / pitch:
When two researchers discover a horrifying truth about consciousness and death, their obsessive devotion to each other pushes them to do the unthinkable.
Setting: Kraków, Poland; a fictional institute dealing with several branches of biology situated on the outskirts of the city
Word count: 35k/100k, in drafting stage
First line (after prologue): In our labs, we are small gods, clumsy architects of nature.
Blurb and excerpt under the cut. Reply or reblog with a comment to be added to the tag list!
Blurb:
Kristian is a PhD student at the end of his rope. His scholarship is running out, his supervisor won’t let him defend, and he’s stuck at a third-rate institute with no support. As a last resort, he applies for an assistant position in a newly funded project – and ends up being the only candidate.
A connection quickly develops between him and his new boss, Leith. The two bond over their shared interests, and shared trauma. Soon, the platonic affection transforms into hungry romance. Somewhere deep down, Kristian knows that their love is more of a sick coping mechanism, but is unable to stop himself.
The tension rises when they accidentally discover a gruesome truth about brains, consciousness, and death. Any other scientist would announce this to the world and step away. Kristian and Leith conduct their experiments in secret, pushing the boundaries of ethics to advance the research. And their unquestioning devotion to each other is about to lead them into much darker places.
Excerpt (from chapter 4):
In order to fully assess the effects of a treatment (drug, pollutant, living condition, induced mutation, etc.), a scientist often needs a sample of tissue that has been washed of all unnecessary materials. A clear cut of brain, liver or intestine is best viewed when it has been infused with a fixative before being placed under a microscope. One way to achieve this is transcardial perfusion. I have performed it many times, preparing tissue samples for pathology comparisons. The protocol runs as follows: the animal is anesthetized but kept alive, after which the body is restrained, chest cavity opened, and a major blood vessel is connected to a supply of fixative. The animal’s still beating heart then does the job for you, carrying it to every point, through every capillary, until finally there is no blood left and the heart ceases to beat.
I had never gotten used to it. I am not a squeamish person and the sight of blood, urine, feces, pus, or any other biological substances does not disturb me. Many biology students deal quite well with formaldehyde preserved specimens but falter at freshly sacrificed animals. One young man had described to me the acute drop in blood pressure he felt the first time a dead rat had been placed in front of him. It wasn’t the sight (fluids, viscera, the undigested contents of the rat’s stomach) but the realization of such recent death. The tiny body still warm, motionless. Perhaps the human mind begins searching at once for the causes, and fears the proximity of whatever had killed another animal (and may be searching for its next victim). Regardless, the ability to deal with this horror is what often sorts students into specialties. Luckily, there are plenty of areas in biology that don’t require you come in contact with living vertebrates at all.
What I always wondered is whether it was possible to do transcardial perfusion on a human. Could one take a person, still living, put them under and replace their blood with some sort of protective substance? Perhaps a solution that would allow them to be frozen, preserved in a box like a packet of fish sticks, waiting for a better time. Keep them on the verge between life and death for decades to then defrost them and pump four liters of blood back into their body. Would the brain survive such a process? Would the mind? Could someone do this to me at the shortest notice and keep me asleep until S. would retire (or die) and someone else would be placed on his cases, so that I could graduate at last?
6 notes
·
View notes
Quote
Society’s interest and responsibility, when it comes to mental health, lie in providing everyone with the ability to access medical care, including psychiatric care, without undue financial hardship
Beyond fighting for this access, society has no business attempting to regulate the emotional lives of its individual members or to protect them from unhappiness and anyway has no meaningful ability to do so
Given that pain and suffering are literally and permanently unavoidable in human life, teaching others to be resilient rather than teaching them to be victims is an act of mercy, and cultivating resilience in yourself is an act of essential personal growth and adult development
Unhappy emotions, even chronic unhappy emotions, are inherent and ineradicable elements of the human condition, with boredom and disappointment something like the default state of adult life for those of us lucky enough to be financially secure in the developed world
Your pain is important and we should all want to help you heal, but everyone else is hurting too and the fact that you are hurting does not give you any special privileges
Human beings are self-deceiving creatures, and what we often need from others is to be told that we are wrong - that what we believe is wrong, that what we want is unrealistic, that the way we’ve behaved is unjustifiable
Not getting what you want is a default and healthy status, not a tragedy, though you are perfectly within your rights to be unhappy about it, and people who do not give you everything you want are not inherently “toxic,” though you’re perfectly within your rights to be unhappy with them
Self-diagnosis is inherently unhealthy, without exception
Acting as though the social and personal rules that apply to children should apply to you when you are an adult ensures that you will behave selfishly and hurt others, and the constant celebration of childish behavior in adults has profound negative consequences for all of us
Many conflicts in life involve multiple people making equally valid attempts to secure what they want in matters that are genuinely zero-sum, meaning that society actually can’t satisfy the desires of everyone, and most of the time, these conflicts are between people who are all principled and decent and who are simply trying to achieve their goals and desires the way we all do
Some people are just assholes, not narcissists, not toxic, not under the influence of the “Dark Triad,” not sociopaths or psychopaths, not BPD, not any other tendentious medicalized term you’ve used to express your distaste for them - they’re just assholes
Sometimes you're the asshole
Disagreement, expressed in language, can never be violence
When you experience trauma or grapple with your mental health, most people around you are trying their best to be kind and respectful to you, and creating long lists of behavioral or communicative standards that they will inevitably be unable to satisfy is your failure, not theirs
Sick people have as much responsibility to manage their disorders as society has to give them the tools to manage them; you cannot ask others to give you accommodation for your disability if you refuse to take accountability for it yourself
The natural place to look for love, acceptance, and affirmation when you need them is your close friends and family, the people with whom you have mutual emotional attachment, as they are the best equipped to help and the people whose opinion you care about the most; expecting strangers or society writ large to care about you the way your loved ones care about you is deluded and disordered
Some talented artists are able to turn their pain into compelling art, and some talented writers and thinkers are able to publicly explore mental illness in an interesting and generative way, but that kind of talent is rare, and trauma and mental illnesses are not only not inherently interesting, they’re usually intensely boring
You are not your pathologies, you are not your sickness, and you must be able to survive as just the person that you are, without a crutch
Once upon a time, there was strong social value in being “cool,” with the concept of cool referring to a studied indifference to the vagaries of fate; turning away from the pursuit of cool to defining ourselves according to our weaknesses and neuroses was a profound mistake, cool was a humane and correct social value, and we should return to it.
Prologue to an Anti-Therapeutic, Anti-Affirmation Movement
0 notes
Text
"You Should Never Tell a Psychopath They Are a Psychopath. It Upsets Them": Villanelle, Joe Goldberg and Feeling Sorry for Psychopaths

What do you envision when you hear the word? I’d hazard a guess it’s your prototypical psychopath with a dead-eye stare and blood-stained knife in hand. Perhaps it’s your conspiracy theorist neighbour, or that — yes, that one — ex. We’ve seen Villanelle’s theatrical murders on ‘Killing Eve’ and we’ve rooted for Joe in ‘You’ despite his murder habit. We’ve read articles with clickbait titles on how to “spot” a psychopath and immediately diagnosed our sibling, colleague or ex-best friend. It’s a term we throw around carelessly, yet it also inspires fear. A real psychopath isn’t like us and they certainly aren’t worth any kind of sympathy. We’re good people and they’re crazy, violent, controlling, unemotional and self-obsessed. Right?
Sweet but a psycho
Popular culture has given us infamous psychopaths throughout the decades and a couple of our contemporary favourites must be Oskana Astankova — the Russian assassin “Villanelle” -from hit TV show ‘Killing Eve’ and Joe Goldberg from Netflix’s ‘You’. Despite their psychopathic tendencies, fans champion their victories.

Psychologist Robert Hare devised the ‘Psychopath Checklist’ back in 1980 and it is now routinely referred to as the PCL-R. Villanelle and Joe would score highly: both characters believe they are of great importance, routinely lie, act impulsively, struggle with control, take zero to little accountability for their actions, lack empathy, and have a history of criminality and behavioural problems.
Hare’s checklist is still doing the rounds in institutions worldwide, usually prisons, but it has come under plenty of criticism for what Willem Martens (2008) deems as being an unethical psychological practice. It’s difficult to diagnose the term “psychopath” but several diagnoses may suggest a fit, from Antisocial Behaviour Disorder to psychopathy and various other personality disorders.
Already, we see how complex a diagnosis it and encounter very different views from psychologists when it comes to the question of the psychopath. Yet, as we progress as a society, so does science. Science isn’t rigid, stuck in a time of Freud and every other straight, white, wealthy, old, neurotypical male philosopher and psychologist from the 20th century. It moves with society and it adapts as our knowledge deepens. Nowadays, some psychologists and mental health practitioners are rejecting the label “psychopath” completely due to the severely negative connotations and even calling psychopathy a mental health issue or disability.
Psychology says what?
Identity is an important factor when it comes to being human. Our identities are important to us, especially as we engage and present these identities online. Psychopaths are said to be so unlike the majority they are unable to make genuine connections with others but as with anyone deemed ‘different’, it is the group that collectively rejects the ‘different’ individual, perpetuating a cycle of low interpersonal integration and marginalisation.
If given an official diagnosis with a working label of “psychopath”, combined with society’s current view of what it means to be a psychopath, a psychopath is quickly forced to the outskirts of society thus lowering their commitment to fulfilling social roles. A self-fulfilling prophecy becomes imminent: when someone is thought of and treated as if they are somehow broken, they often become it.
Noel Smith is the commissioning editor of magazine InsideTime and a former prisoner who has experienced his fair share of mental health difficulties. Writing for InsideTime, Smith says: “If people think you’re MAD, then everything you do, everything you think, will have MAD stamped across it.”
Psychologists Peterson & Seligman (2004), tired of psychology’s tendency to focus on the deviant side of humanity, proposed we all have the ability to express ‘the six common virtues’: wisdom and knowledge, courage, humanity, justice, temperance and spirituality or transcendence.
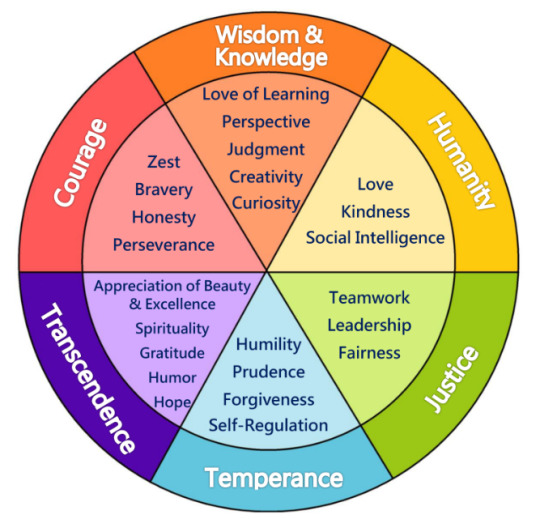
Here, Peterson & Seligman neatly demonstrated how language can create a narrative. The psychopath according to Hare’s checklist could be grandiose and controlling, but with a slightly different view, they’re confident and courageous leaders. We associate the term so often with negative traits that we ignore the possibility for positives.
Mental health matters — but not for you
“They [psychopaths] are the social snakes in the grass that slither and smile their way into your life and emotions. They feel no empathy, and only care about themselves” says Dr Xanthe Mallett, a forensic anthropologist and criminologist at Newcastle University.
Dr. Mallett’s words reinforce an age-old belief: the psychopath’s only identity is psychopath and they are incapable of being anything other than one-dimensional.
Author Nathan Filer expressed his initial dismay that once his diagnosis was televised by ‘Meet the Psychopaths’ programme on Channel 5, strangers expressed their fear and revulsion immediately. Filer states he “quickly got over” people’s negative opinions but received abuse on the streets with words such as “psycho” and “nutter” shouted at him on a regular basis, reinforcing the rejection by the collective.
Lucy Nichol, writer and mental health support activist, expressed her fears when joining a discussion panel at the Centre for Life Science’s speakeasy programme for adults in 2019. Nichol, rightfully, is anxious about the welfare of those living with psychosis and how they can be discriminated against due to fear. She worries that psychopaths can be “violent and frightening”, and any potential link between psychopaths and people living with psychosis can lead to danger for people with psychosis. Resistant to the movement of psychopathy being welcomed into the family of mental health, Nichol argues it should not be treated as a mental health concern. Her argument is that a classified psychopath lacks empathy and is unable to judge other people’s emotions and this makes the people around the psychopath vulnerable, not the psychopath.
Yet, other mental health conditions and disorders can lead to an individual not necessarily being able to empathise in the way a neurotypical person may empathise. Similarly, an individual with autism, a panic disorder or psychosis may have limited capacity to judge other people’s emotions on occasion. As a society, we tend to understand this and accommodate it.
In contrast to Nichol’s view, there are more and more calls for understanding psychopathy in broader, more compassionate terms.
Dr Luna Centifanti, Lecturer in Psychological Sciences at University of Liverpool classes psychopathy as a mental illness that means the individual experiences “disordered thinking, emotions and behaviour.” She added that psychopathy can lead to struggles with understanding emotions of others and therefore their responses to distress can be “inappropriate”.
Do better, be better
Joseph Newman is a psychologist at Wisconsin University who classifies psychopathy as a disability. Newman explains it as an ‘informational processing deficit’ where individuals have less ability to process cues immediately such as someone else’s fear or upset, inviting us to see the psychopath through a more sympathetic lens.
Campaigners, researchers, activists and those with lived experiences of mental health conditions and illnesses have made huge strides for inclusivity and understanding. As professionals such as Newman and Dr. Centifanti begin to deconstruct the pathological idea of psychopathy, it is being tentatively considered as a mental health issue.
Let’s go back to Villanelle. Her history is relatively secret, but the viewer knows she’s spent time in Russian prison and has no family, therefore little connection to others. Her violent, ‘psychopathic’ actions are a result of her occupation as an assassin as opposed to something she does simply for the joy of enacting violence.
A recent soundbite suggests the show’s writers are no longer calling Villanelle a “psychopath” after astute fans have criticised the way it reduces her to a label.
Be more psychopath
A merge of popular culture, sociology and psychology has begun to turn the connotations of ‘psychopath’ on its head somewhat. The Wisdom of Psychopaths by Kevin Dutton (2012) looks to diagnosed psychopaths to teach us how to care less about other people’s emotions and our own, be fearless in our jobs and have an unwavering belief in ourselves. Western culture is a key culprit in promoting the idea that an impressive salary equals success or showing emotion at work is unprofessional, so, maybe it’s true — we could learn a lot about success from a psychopath.
On the flip side, while these traits have the potential to lead to fantastical financial and business success in aggressively capitalist societies, that doesn’t make them inherently good. Now more than ever seems to be a time where we need to cultivate harmony, compassion and vulnerability for all people regardless of individual status, label or identity.
“It isn’t hard to convince someone you love them if you know what they want to hear”
An eyebrow raising sentence from everyone’s favourite cute psychopath, You’s Joe Goldberg. It is wonderfully inclusive to change the narrative on psychopathy but surely there’s a reason for its fierce reputation. Maybe Dr. Mallet was right in that the psychopath is always a sneaky snake, ready to pounce and sink their psychopathic poison into our blood.
Manipulation is one of the terms we regularly hear associated with psychopathy. If psychopaths are prone to manipulating others, it can be argued that simple survival instincts mean non psychopathic individuals want to protect themselves and society from such behaviour. However, by perpetuating the hype of how dangerous psychopaths are, we just come back to an earlier point made in this article that the collective ostracises the psychopath and therefore impacts their ability to comply with social norms.
Hug your local psychopath
It seems that one of the prevailing mainstream perspectives on psychopathy is that a psychopath is someone evil: they were born evil; they are evil, and they’ll die evil. Hopefully you’ll now join me in disagreeing with that sentiment and see psychopathy as a complex mental health issue where everyone experiencing it is different and deserves to have the chance to be defined beyond a label.
No one is innately criminal or violent. While yes, there are links between criminality, violence and psychopathy, it’s worth remembering that we live in a time of mass media consumption that loves to sensationalise. The need to sell and to exaggerate often win over the need to be patient, analyse and truly understand complex parts of the human experience.
Psychology’s flirtations with neuroscience have revealed fascinating results: the brain, what a non-scientist would likely assume is a fixed and unchangeable organ, does and can change. Our brains are individual and through theories of neuroplasticity we can understand the vitality of our social environment on our brain and therefore behaviour. Psychopaths cannot be excluded from this.
Psychology and sociology are working to explore links between criminality and disadvantage or oppression. If criminality is linked to psychopathy, we must ask why, and be prepared to look at an individual’s history and their social environment.
Frankly, many of the accusations thrown at psychopaths do not work for neurodiverse people. Whether it’s an anxious person unable to understand why their habits, born from their anxiety, frustrate their travel buddy or a psychopath who — as Dr. Newman believes — can’t recognise their words or behaviour has upset someone until much later, the world can be a confusing puzzle for those of us who do not fit neatly into the expected norm.
In expanding compassion and understanding to others regardless of what condition or disorder they may have, we can be instruments of change. Once we look to others and try to understand them, we deconstruct labels that lead to marginalisation and instead, we can bring people together by saying: you are not alone.
**
#xan youles#psychology#personality disorder#psychopathy#psychopath#mental health#mental health activism#anti stigma#psychologist#neuroscience#academia#academic#essay#original essay#original writing#writer#don't use terms you don't understand sweetheart#inclusive language#inclusion#inclusivity#professional#villanelle#killing eve#joe goldberg#you netflix
7 notes
·
View notes
Text
Here are somethings to think about!
Is there a significant decrease in the well-being of individuals on the experience of living in highly urbanized areas? Why?
Is living in highly urbanized area increases chances of having poor lifestyle, affects family more negatively than positively? (stress, alcohol, smoking, drug addiction, etc.)
The following are the data sets I considered to further validate the possible results of my hypothesis:
1. For the data on the experiences in living situations and environments in urban areas – I chose the data from National Longitudinal Study of Adolescent Health
2. For the comparison of data on the employment rate, income, quality of life in the urban places of different countries – I chose Gapminder data
3. For the association of epidemiological effects of drug use and other health conditions by living in urban areas - I chose the data from The U.S. National Epidemiological Survey on Alcohol and Related Conditions (NESARC)
Some findings in related literatures will also gave evidences and variables that can be contributory to the quality or kind of life some people have in urban areas.
Let’s see some researches that gives light to the reality of our questions above.
Urbanization's physical and social impacts on health and disease are known. Although causal relationships are not fully established, poor health is associated with poverty, malnutrition, poor housing, inadequate sanitation, pollution, and economic and psychological stresses, as well as with inadequate health services. Urbanization in industrialized and developing countries has brough about increased human exposure to health hazards: biological, chemical, physical, social, and psychological… but urban congestion and pollution threaten the health of people in all countries.
Statistics provided by the United Nations Center of Human Settlements show that the contribution to housing stock by the informal sector (not registered by the authorities, do not keep accounts, and employ mostly casual labour for sites and construction) is significant: for example in the Philippines 86% of the housing stock increase was produced by the informal sector, in Brazil 82%, in Venezuela 77%, in Colombia 64%, and in Chile 44% (UNCHS, 1988b).
(Urbanization, Health and well-being: A Global Perspective by G. Goldstein, 1990)
The impact of socio-economic effects on health can be complex in urban populations. High income should theoretically improve many health outcomes, but it may also support an unhealthy lifestyle, as poor early conditions increase the risk of obesity in a subsequently more socio-economically developed environment.
Increasing socio-economic status may result in an elevated risk of chronic pathologies.
Urban consumerism can be associated with a markedly elevated generation of anthropogenic pollutants, either through lifestyle choices (e.g., car usage) or industry (e.g., factories, e-waste dismantling).
Many standard air pollutants increase with degree of urbanization. These include particulate matter (PM), which has been among the highest in the world in China since economic expansion began in the 1980s, and products of combustion. Urbanization may affect water quality through an excess of contamination including endocrine disrupting chemicals, antibiotics, steroid hormones, and excess nutrients. Elevated exposures to chemicals can also arise in indoor environments (e.g., from new building materials or furnishings).
(Understanding and Harnessing the Health Effects of Rapid Urbanization in China by Yong-Guan Zhu, John P.A. Ioannidis, Hong Li, Kevin C. Jones, and Francis L. Martin, 2011)
Urban socialization leads to two characteristics, Individualistic and materialistic in their outlook. Furthermore, cities can also offer so many other negative ideologies including hedonistic cultures such as entertainment, clubbing, free sex, drugs phonographic and so on, ad search for instant gratification.
Competing for space leads to the emergence of squatter and slum areas. Concisely, urbanization trend today may be seen as nothing less than the urbanization of poverty and deprivation. This scenario is one of growing unemployment, weak social services, lack of adequate shelter and basic infrastructure as well as increasing disparities resulting in a high degree of social exclusion. These are, of course, the well-known causes of social dysfunction, crime, and violence.
Malaysian gov't is having difficulties trying to solve several social problems such as 'mat rempit', free sex and abortion that have not been heard before. Mat Rempit (illegal motorbike racing). They do not only engage in racing among themselves but also challenge other road users to race with them or they will fight with those who try to stop them. These problems are associated with dense population as well as low moral values.
Prejudice and discrimination would certainly develop in this kind of environment and social conflict will erupt at any time.
The issue of crim and violence also draws the same concern. We are aware that security and safety is paramount for human wellbeing. In the same vein, crime and violence disproportionately affect the psychology of urban residents.
Neighborhoods isolate their families because of danger. Together the populations and spaces of cities present both opportunities and challenges to well-being and healthy development. This leads to the theoretical and practical question for urban psychology i.e. the consequences of urban life for mental health, well-being, and development.
Much psychological research has documented the relationship between stress and health outcomes. Because of the nature of the urban environment (i.e., high density, diversity, environmental pollutant), many types of stress-related cases occur more frequently among its residents in comparison to rural or suburban residents.
In Malaysia, residence, or home for most of urban dwellers would means flat, condominium, apartment or terrace house with building scenario and manmade landscape which is often poorly laid out. This kind of environment would certainly affect the psychological wellbeing of the urban folks.
(Urbanism, Space and Human Psychology: Value Change and Urbanization in Malaysia by Zaid B. Ahmad, Haslinda Abdullah and Nobaya Ahmad, 2009)
Urbanization brings with it a unique set of advantages and disadvantages. This demographic transition is accompanied by economic growth and industrialization, and by profound changes in social organization and in the pattern of family life. Urbanization affects mental health through the influence of increased stressors and factors such as overcrowded and polluted environment, high levels of violence, and reduced social support.
Impact of urbanization is associated with an increase in mental disorders. The reason is that movement of people to urban area needs more facilities to be made available and infrastructure to grow. This does not happen in alignment with the increase of population Hence, lack of adequate infrastructure increases the risk of poverty and exposure to environmental adversities. Further this also decreases social support (Desjarlais et al., 1995) as the nuclear families increase in number. Poor people experience environmental and psychological adversity that increases their vulnerability to mental disorders (Patel, 2001).
A report by World Health Organization (WHO) (World Health Organization) has enumerated that mental disorders account for nearly 12% of the global burden of disease. By 2020, these will account for nearly 15% of disability-adjusted life-years (DALYs) lost to illness. Incidentally, the burden of mental disorders is maximal in young adults, which is considered to be the most productive age of the population. Developing countries are likely to see a disproportionately large increase in the burden attributable to mental disorders in the coming decades (WHO Mental Health Context 2003).
When we refer to psychiatric disorders anxiety and depression are more prevalent among urban women than men and, are believed to be more prevalent in poor than in non-poor urban neighborhoods (Naomar Almeida-Filho et al 2004). The meta analysis by Reddy and Chandrashekhar(1998) revealed higher prevalence of mental disorders in urban area i.e., 80.6%, whereas it was 48.9% in rural area. Mental disorders primarily composed of depression and neurotic disorders.
Increase of nuclear families in urban society has led to increase in cases of violence against women in general. Among them, intimate-partner violence links to alcohol abuse and women’s mental health. Analysis of community-based data from eight urban areas in the developing world indicates that mental and physical abuse of women by their partners is distressingly common with negative consequences for women’s physical and psychological well being (Lori L. Heise et al 1994). Poverty and mental health have a complex and multidimensional relationship. The urbanization leads to forming set of group as “fringe population” who earn on daily basis (Mursaleena Islam etal 2006)
Women are particularly vulnerable and they often disproportionately bear the burden of changes associated with urbanization. Domestic violence is also highly prevalent in urban areas. In both developed and developing countries, women living in urban settings are at greatest risk to be assaulted by their intimates (Kessler RC, Sonnega A, Bromet E, Hughes M, Nelson CB (1995)
(Urbanization and Mental Health by Kalpana Srivastava, 2009)
With the evidences studied all over the world about the effects of urban living to the individual wellbeing can be cautiously frightening and something that we should all be aware about specially for those who are already living in big cities.
We can find ways to use the researches and studies on urban living and make meaning to it for the improvement of life.
1 note
·
View note
Text
Gatekeeping neurodiversity is artificial, socially constructed, and subjective
In modern progressive thought, there are two co-existing ways of looking at atypical brains:
1) Mental illness
2) Neurodiversity
The orthodoxy is that mental illness is bad, while neurodiversity is good.
How do we define mental illness? Well, for starters, do we even? The WHO, for example, prefers the term “mental disorders”, defined:
Mental disorders comprise a broad range of problems, with different symptoms. However, they are generally characterized by some combination of abnormal thoughts, emotions, behaviour and relationships with others. Examples are schizophrenia, depression, intellectual disabilities and disorders due to drug abuse. Most of these disorders can be successfully treated.
The charity Mind also does not use the phrase “mental illness”, instead defaulting to “mental health problems”. For their part, they say:
In many ways, mental health is just like physical health: everybody has it and we need to take care of it.Good mental health means being generally able to think, feel and react in the ways that you need and want to live your life. But if you go through a period of poor mental health you might find the ways you're frequently thinking, feeling or reacting become difficult, or even impossible, to cope with. This can feel just as bad as a physical illness, or even worse.
So mental health issues, or mental disorders, involve:
Some combination of abnormal thoughts, emotions, behaviour and relationships with others.
The ways you frequently think, feel, or react become difficult or even impossible to cope with.
Mental health is changeable - you can go through periods of good or bad mental health.
By contrast, neurodiversity is defined by academic Nick Walker as follows:
Neurodiversity is an essential form of human diversity. The idea that there is one “normal” or “healthy” type of brain or mind or one “right” style of neurocognitive functioning, is no more valid than the idea that there is one “normal” or “right” gender, race or culture.
The classification of neurodivergence (e.g. autism, ADHD, dyslexia, bipolarity) as medical/psychiatric pathology has no valid scientific basis , and instead reflects cultural prejudice and oppresses those labeled as such.
The social dynamics around neurodiversity are similar to the dynamics that manifest around other forms of human diversity. These dynamics include unequal distribution of social power; conversely, when embraced, diversity can act as a source of creative potential.
(My formatting)
Now note that Walker’s definition doesn’t create a harsh separation between “neurodivergence” and “mental illness”. Indeed, it specifically includes a condition - bipolarity - which most people would happily class as a mental illness.
Of course, Walker isn’t the oracle of truth - he has informed opinions, but they’re just opinions, and his definition is a statement of what he considers the best definition to be, rather than a worked explanation of how he came to that definition. So, how could we separate neurodiversity from poor mental health?
First, I recently raised this question with someone who said the answer was that mental health is “not neurological”. This is not true. Depression, for example, has a big impact on your neural development, and our most effective treatments involve messing around with neurotransmitters. Your mind is entirely neurological, therefore your mental health is entirely neurological.
Second, the notion that mental illness is a thing you don’t want, while neurodiversity is a thing you do want. But some people dislike being autistic, ADHD, dyslexic, or dyspraxic, and those are supposed to be the friendly faces of neurodiversity. Meanwhile, there are plenty of people who embrace being bipolar, OCD, schizophrenic, and even depressed or anxious.
Third, the idea that neurodiversity involves talents, gifts, or valuable alternative viewpoints, while mental illness does not. Again, this quickly runs into trouble. For starters, an extreme version expects neurodivergent people to have wonderful abilities like Stephen Wiltshire. This is both untrue, and somewhat patronising. Neurodiversity is ordinary. But moreover, many conditions often deemed mental illnesses once again can come with advantages. A friend of mine with anxiety says that although she sometimes finds it unpleasant, she’s glad she has anxiety as she feels it motivates her to be nicer to other people. This is not my personal experience of anxiety, but her viewpoint is just as valid. The same clichés you hear about autistic people also apply to schizophrenics - famous schizophrenics include Jack Kerouac, Syd Barrett and John Nash, and probably Vincent Van Gogh, and in all cases their condition is routinely associated with their talent. Kanye West calls being bipolar his “superpower”.
Fourth, the idea that neurodiversity is permanent whereas mental illness is transient. Again, this doesn’t work. Many mental illnesses are not transient. As with autism, most mental illnesses have genetic components. And would we not class someone who became autistic due to a brain injury as “neurodiverse”?
Fifth, the idea that we can determine what is an “illness” and what is merely a “condition” by leaving it to psychiatrists or other professionals. Alas, we can’t - they routinely get it wrong. Diagnosis with a “mental illness”, a neurodivergence, or nothing at all is very much dependent on when and where you live. This is not meant to knock psychiatrists by any means, but we should not pretend that they are objective - they know a lot, but the founding purpose of the neurodiversity movement was to push back against common psychiatric assumptions.
I will skip over, for now, neurodegenerative conditions such as MS, ME, or dementia, but please do bear them in mind.
So, what definitions might work?
Well, try these on for size:
- Conditions are always neurodiversity. Neurodivergence is always good, but sometimes an individual will be distressed by one or more symptoms arising due to that neurodivergence and will seek treatment for those symptoms. Sometimes those symptoms could be understood as mental health difficulties.
or:
- A person can use neurodivergence and mental illness as they feel is appropriate to refer to themselves. Maybe they’re a person with chronic depression who is nonetheless glad they have a mind prone to depression. Maybe they have ADHD and want it cured. Maybe those two people are the same person. We, the neurodiversity community, should not gatekeep who gets to be part of our community.
What I’m suggesting is that, just as race, sexuality, and gender can be understood as social constructs, so too can the divide between “good neurodiversity” and “bad mental illness”.
9 notes
·
View notes
Text
Jasbir K. Puar, Bodies with New Organs: Becoming Trans, Becoming Disabled, 33 Social Text 45 (2015)
“Transgender rights are the civil rights issue of our time.” So stated Vice President Joe Biden just one week before the November 2012 election. This article critically reframes calls such as this by foregrounding a historical trajectory not celebrated by national LGBT groups or media or explicitly theorized in most queer or trans theory: the move from the 1990 Americans with Disabilities Act to the present moment of trans hailing by the US state. Such a trajectory helps map the ways that neoliberal mandates regarding productive, capacitated bodies entrain the trans body to recreate an abled body not only in terms of gender and sexuality but also in terms of economic productivity and the economic development of national economy. Rather than argue for a better form of discretion between the categories of trans and disability, this article analyzes the ontological irreducibilities of such categories, irreducibilities that dissolve them through multiplicity. In following the implications of such an argument, this article unfolds trans and disability studies' concerns within a broader analysis of the geopolitics of racial ontology.
“Transgender rights are the civil rights issue of our time.” So stated Vice President Joe Biden just one week before the November 2012 election. Months earlier President Barack Obama had publicly declared his sup- port for gay marriage, sending mainstream LGBT organizations and queer liberals into a tizzy. Though an unexpected comment for an election season, and nearly inaudibly rendered during a conversation with a concerned mother of Miss Trans New England, Biden’s remark,1 encoded in the rhetoric of recognition, seemed logical from a now well-established civil rights–era teleology:2 first the folks of color, then the homosexuals, now the trans folk.3
What happens to conventional understandings of “women’s rights” in this telos? Moreover, the “transgender question” puts into crisis the framing of women’s rights as human rights by pushing further the relationships between gender normativity and access to rights and citizenship. I could note, as many have, that failing an intersectional analysis of these movements, we are indeed left with a very partial portrait of who benefits and how from this according of rights, not to mention their tactical invocation within this period of liberalism whereby, as Beth Povinelli argues, “potentiality has been domesticated.”4 As Jin Haritaworn and C. Riley Snorton argue, “It is necessary to interrogate how the uneven institutionalization of women’s, gay, and trans politics produces a transnormative subject, whose universal trajectory of coming out/transition, visibility, recognition, protection, and self-actualization largely remain uninterrogated in its complicities and convergences with biomedical, neoliberal, racist, and imperialist projects.”5 In relation to this uneven institutionalization, Haritaworn and Snorton go on to say that trans of color positions are “barely conceivable.” The conundrum here, as elsewhere, involves measuring the political efficacy of arguing for inclusion within and for the same terms of recognition that rely on such elisions. There is a tension between the desires for trans of color positions to become conceivable and their bare inconceivability critiquing and upending that which seems conceivable.
Biden’s remarks foreshadow the steep cost for the intelligibility of transgender identity within national discourses and legal frames of recognition. Does his acknowledgment of transgender rights signal the uptake of a new variant of homonationalism—a “trans(homo)nationalism”? Or is transgender a variation of processes of citizenship and nationalism through normativization rather than a variation of homonationalism? In either instance, such hailings, I argue, generate new figures of citizenship through which the successes of rights discourses will produce new biopolitical failures—trans of color, for one instance. Susan Stryker and Aren Z. Aizura call the “production of transgender whiteness” a “process of value extraction from bodies of color” that occurs both nationally and transnationally.6 Thinking of this racial dynamic as a process of value extraction highlights the impossibility of a rights platform that incorporates the conceivability of trans of color positions, since this inconceivability is a precondition to the emergence of the rights project, not to mention central to its deployment and successful integration into national legibility. Adding biopolitical capacity to the portrait, Aizura writes that this trans citizenship entails “fading into the population . . . but also the imperative to be ‘proper’ in the eyes of the state: to reproduce, to find proper employment; to reorient one’s ‘different’ body into the ow of the nationalized aspiration for possessions, property [and] wealth.”7 This trans(homo)nationalism is therefore capacitated, even driven by, not only the abjection of bodies unable to meet these proprietary racial and gendered mandates of bodily comportment but also the concomitant marking as debilitated of those abjected bodies. The debilitating and abjecting are cosubstancing processes.
In light of this new but not entirely unsurprising assimilation of gender difference through nationalism, I want to complicate the possibilities of accomplishing such trans normativization by foregrounding a differ- ent historical trajectory: one not hailed or celebrated by national LGBT groups or the median or explicitly theorized in most queer or trans theory. This is the move from the 1990 Americans with Disabilities Act (ADA) to the present moment of trans hailing by the US state.8 Historically and contemporaneously, the nexus of disability and trans has been fraught, especially for trans bodies that may resist alliances with people with dis- abilities in no small part because of long struggles against stigmatization and pathologization that may be reinvoked through such an affiliation. But stigmatization is only part of the reason for this thwarted connection.
Neoliberal mandates regarding productive, capacitated bodies entrain the trans body to recreate an abled body not only in terms of gender and sexuality but also in terms of economic productivity and the economic development of national economy.9 Thus, trans relation to disability is not simply one of phobic avoidance of stigma; it is also about trans bodies being recruited, in tandem with many other bodies, for a more generalized transformation of capacitated bodies into viable neoliberal subjects.
Given that trans bodies are reliant on medical care, costly pharmacological and technological interventions, legal protections, and public accommodations from the very same institutions and apparatuses that functionalize gender normativities and create systemic exclusions, how do people who rely on accessing significant resources within a political economic context that makes the possessive individual the basis for rights claims (including the right to medical care) disrupt the very models on which they depend in order to make the claims that, in the case of trans people, enable them to realize themselves as trans in the first place? I explore this conundrum for trans bodies through the ambivalent and vexed relationship to disability in three aspects: (a) the legal apparatus of the ADA, which sets the scene for a contradictory status to disability and the maintenance of gender normativity as a requisite for disabled status; (b) the fields of disability studies and trans studies, which both pivot on certain exceptionalized figures; and (c) political organizing priorities and strategies that partake in transnormative forms not only of passing but also of what I call “piecing,” a recruitment into neoliberal forms of fragmentation of the body for capitalist profit. Finally, I offer a speculative differently imagined affiliation between disability and trans, “becoming trans,” which seeks to link disability, trans, racial, and interspecies discourses to make boundaries porous through the overwhelming force of ontological multiplicity, attuned to the perpetual differentiation of variation and the multiplicity of affirmative becomings. What kinds of assemblages appear that might refuse to isolate trans as one kind of specific or singular variant of disability and disability as one kind of singular variant of trans? What kind of political and scholarly alliances might potentiate when each takes up and acknowledges the inhabitations and the more generalized conditions of the other, creating genealogies that read both as implicated within the same assemblages of power? The focus here is not on epistemological correctives but on ontological irreducibilities that transform the fantasy of discreteness of categories not through their disruption but, rather, through their dissolution via multiplicity. Rather than produce conceptual interventions that map onto the political or produce a differently political rendering of its conceptual moorings, reflected in the debate regarding transnormativity and trans of color conceivability, I wish to offer a generative, speculative reimaging of what can be signaled by the political.
I. Disability Law and Trans Discrimination
The legal history that follows matters because it both re ects and enshrines a contradictory relationship of trans bodies that resist a pathological medicalized rendering and yet need to access bene ts through the medical industrial complex. The explicit linkages to the trans body as a body either rendered disabled or (perhaps and, given the teleological implications) rehabilitated from disability have been predominantly routed through debates about gender identity disorder (GID). Arriving in the DSM-III (third edition of the American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders, published in 1980, on the heels of the 1974 DSM-II depathologization of homosexuality, GID was eliminated in the DSM-5 released in May 2013, now replaced with gender dysphoria.10 These complex debates have focused largely on a series of explicit inclusions and exclusions of GID in relation to the DSM and the ADA. The inclusion of GID in 1980 and its focus on childhood behavior were largely understood as a compensatory maneuver for the deletion of homosexuality, thus instating surveillance mechanisms that would perhaps prevent homosexuality.11 In contrast, a notable passage in the ADA details the speci c exclusion of “gender identity disorders not resulting from physical impairments” as a disability—couched in an exclusionary clause that included “transvestitism, transsexualism, pedophilia, exhibitionism, voyeurism, . . . ‘other sexual disorders,’” and completely arbitrary “conditions” such as compulsive gambling, kleptomania, pyromania, and substance use disorders involving illegal drugs.12 This clause was largely understood (unlike the specific exclusion of homosexuality) as an entrenchment of the pathologization of GID. This deliberate inclusion of the terms of exclusion is a crucial piece of the story, in part because to date the ADA is “the most extensive civil rights law to address bodily norms.”13
Given the ADA’s hodgepodge of excluded conditions, many of which carry great social stigma and/or are perceived as criminal activity, most commentators concur with L. Camille Herbert’s sentiment that “while one might argue for the exclusion of certain conditions from the definition of disability as justified by not wanting to pathologize certain individuals and conditions, this does not appear to have been the motivation of Congress.”14 The process by which Congress arrived at these exclusions also appears marred by moral panic discourses about diseased and debilitated bodies, discourses that the ADA was produced in part to ameliorate. Former senator Jesse Helms (R-NC), writes R. Nick Gorton, “raised the specter that the law would provide disability protections to numerous politically unpopular groups,” concluding that most people who are HIV positive are drug addicts, homosexuals, bisexuals, pedophiles, or kleptomaniacs, among others, and that the exclusion was enacted “as a direct result of Helms’s efforts.”15 Noting that the ADA “unequivocally” endorses the use of the DSM in recognizing conditions of disablement, Kari Hong argues that “understanding why a dozen conditions were removed becomes an important task,” as the exclusion not only disqualifies certain conditions from consideration as a disability but also “isolate[s] particular conditions from medical authority.” Hong also points out that Helms’s “bifurcation of disability into ‘good’ (wheelchairs) and ‘bad’ (transvestitism) categories echoes a disturbing misuse of medicine.”16 Ultimately, Congress capitulated and sacrificed these excluded groups in exchange for holding onto the protection of another vili ed “minority” group: individuals with HIV.17 This move of course insists on problematic bifurcations, perhaps strategically so, between individuals diagnosed with GID and individuals diagnosed with HIV.
Thus, Kevin Barry argues, “the ADA is a moral code, and people with GID its moral castaways.” He adds, “GID sits at the uneasy cross- roads of pathology and difference,”18 an uneasy crossroads that continues to manifest (especially now as GID has been eliminated in the DSM-V).19 Adrienne L. Hiegel elaborates this point at length, with particular emphasis on how this exclusion recodes the labor capacities of the transsexual body. In segmenting off “sexual behavior disorders” and “gender identity disorders” from the ADA’s definition of disability, the “Act carves out a new class of untouchables. . . . By leaving open a space of permissive employer discrimination, the Act identifies the sexual ‘deviant’ as the new pariah, using the legal machinery of the state to mark as outsiders those whose noncompliant body renders them un t for full integration into a working community.”20
In essence, the ADA redefines standards of bodily capacity and debility through the reproduction of gender normativity as integral to the productive potential of the disabled body. Further, the disaggregation, and thus the potential deflation, of political and social alliances between homosexuality, transsexuality, and the individual with HIV is necessary to the solidi cation of this gender normativity that is solicited in exchange for the conversion of disability from a socially maligned and excluded status to a version of liberal acknowledgment, inclusion, and incorporation. The modern seeds of what Nicole Markotic and Robert McRuer call “crip nationalism”—the hailing of some disabilities as socially productive for national economies and ideologies to further marginalize other disabilities—are evident here, as the tolerance of the “difference” of dis- ability is negotiated through the disciplining of the body along other normative registers of sameness, in this case gender and sexuality.21 And further, what Sharon Snyder and David Mitchell term “ablenationalism”— that is, the ableist contours of national inclusion and registers of productivity—ironically underwrites the ADA even as the ADA serves as groundbreaking legislation to challenge it. Snyder and Mitchell describe ablenationalism as the “implicit assumption that minimum levels of corporeal, intellectual, and sensory capacity, in conjunction with subjective aspects of aesthetic appearance, are required of citizens seeking to access the ‘full benefits’ of citizenship.”22 In reorganizing the terms of disability, ablenationalism redirects the pathos and stigma of disability onto different registers of bodily deviance and defectiveness, in this particular instance that of gender nonnormativity. In that sense, crip nationalism goes hand in hand with ablenationalism; indeed, ablenationalism is its progenitor. While these details about the passage of the ADA are obviously not with- out implications regarding racial and class difference, the specific details of the exclusionary clause might gesture toward the multifaceted reasons that, as Snyder and Mitchell observe, “queer, transsexual, and intersexed peopled . . . exist at the margins of disability discourse.”23
It is not simply that the ADA excludes GID and, by extension, trans from recognition as potentially disabling but, rather, that transsexuality— and likely those versions of transsexuality that are deemed also improperly raced and classed—is understood as too disabled to be rehabilitated into citizenship, or not properly enough disabled to be recoded for labor productivity. Further, the ADA arbitrates the distinctions between homosexuality and transsexuality along precisely these pathologized lines. Contrary to what Hiegel claims, the sexual “deviant” is hardly the “new pariah.” Rather, there is a new sexual deviant in town, demarcated from an earlier one. Indeed, the enthusiastic embracing of the ADA by some gay and lesbian activists and policy makers for the exclusion of homo- sexuality as a “sexual behavior disorder” did not go unnoticed by trans activists who felt differently about the ADA.24 Proclivities toward queer ableism are therefore predicated in the ADA’s parsing homosexuality from other “sexual disorders,” as well as in the histories of political organizing. Zach Strassburger describes the process of homonationalism by noting that “as the gay and lesbian rights movement gained steam, the trans- gender movement grew more inclusive to cover those left behind by the gay and lesbian movement’s focus on its most mainstream members and politically promising plaintiffs.”25 Given the political history of parsing trans from queer through the maintenance of gender normativity, can disability function proactively and productively, as a conversion or translation of the stigma through which trans can demarcate its distance from aspects of LGBT organizing that are increasingly normative?26
I offer this brief historical overview to lay out the stakes for the debate between demedicalizing trans bodies (favoring the use of gender discrimination law to adjudicate equality claims) and successfully using disability law to access crucial medical care. What is evident from these discussions is that trans identity, straddling the divide between the bio- medical model and the social model of disability, challenges the postulation that disability studies is “postbinary,” especially given that vociferous debates about the utility of the medical model in trans jurisprudence persist. Strassburger, who argues for an “expanded vision of disability” based on the social model that could be applied for trans rights, notes nonetheless that the medical model of trans has often been more successful than sex and gender discrimination and sexual orientation protection, and that the transgender rights movement in its emphasis on demedicalization (despite reluctantly admitting the success of medical strategy) ignores the pragmatic aspects of litigation. Further, Strassburger notes the historical effects of stigma, writing that “demedicalization would mirror the gay rights movement’s very successful efforts to frame gayness as good rather than a disease.”27
For others, the debate between medicalization and demedicalization forestalls a broader conversation about access to proper medical care, one that has been foregrounded by feminist struggles over reproductive rights, for example.28 Proponents of the use of disability law further note that difficult access to medical care is not a complete given for all disenfranchised populations. For example, Alvin Lee argues that the “unique aspects of incarceration and prison health care justify and indeed compel the use of the medical model when advocating for trans prisoners’ right to sex reassignment surgery.”29 Lee notes that the usual bias against lower- income populations in the use of the medical model does not apply to the “right-to-care” prison context, where medical evidence is the best way to demonstrate serious and necessary rather than elective health care, given the “general principle that individual liberties should be restricted in prison.”30 Other legal practitioners such as Jeannie J. Chung and Dean Spade are curious about the success of social models of disability in transgender litigation. Spade, for example, has carefully elaborated his ambivalence about the use of disability law and the medical mode in relation to his rm social justice commitment to the demedicalization of trans, arguing for a “multi-strategy approach.”31
II. Trans Exceptionalism: Passing and Piecing
In addition to the robust debates about jurisprudence on trans and disability, transgender studies and disability studies are often thought of as coming into being in the early 1990s in the US academy, a periodization that reflects a shift in practices of recognition, economic utility, and social visibility that obscures prior scholarship. In terms of trans, for example, Stryker and Aizura note that “to assert the emergence of transgender studies as a eld only in the 1990s rests on a set of assumptions that permit a differentiation between one kind of work on ‘transgender phenomena’ and another, for there had of course been a great deal of academic, scholarly, and scientific work on various forms of gender variance long before the 1990s.” Among the various historical changes they list as significant to this emergence are “new political alliances forged during the AIDS crisis, which brought sexual and gender identity politics into a different sort of engagement with the biomedical and pharmaceutical establishments.”32
This emergence of disability and trans identity as intersectional coordinates required exceptionalizing both the trans body and the disabled body to convert the debility of a nonnormative body into a form of social and cultural capacity, whether located in state recognition, identity politics, market economies, the medical industrial complex, academic knowledge production, subject positioning, or all of these. As a result, both fields of study—trans studies and disability studies—suffer from a domination of whiteness and contend with the normativization of the acceptable and recognizable subject. The disabled subject is often a body with a physical “impairment”; the wheelchair has become the international symbol for people with disabilities. In trans identity, the more recently emergent trajectory of female-to-male (FTM) enlivened by access to hormones, surgical procedures, and bodily prostheses has centralized a white trans man subject. While the disabled subject has needed to reclaim forms of debility to exceptionalize the transgression and survivorship of that disability, the transnormative subject views the body as endlessly available for hormonal and surgical manipulation and becoming, a body producing toward ableist norms. Further, transgender does not easily signal within “conventional notions of disability” because it is not a “motor, sensory, psychiatric, or cognitive impairment” or a chronic illness.33
The disabled body can revalue its lack, but the transnormative body might desire to rehabilitate itself to a status of nondisabled. Eli Clare, a trans man with cerebral palsy, has generated perhaps the most material on the specific epistemological predicaments of the disabled trans subject or the trans disabled subject, providing much-needed intersectional analysis.34 Clare writes of the ubiquity of this sentiment: “I often hear trans people—most frequently folks who are using, or want to use medical technology to reshape their bodies—name their trans-ness a disability, a birth defect.”35 Here Clare emphasizes the trans interest in a cure for the defect, a formulation that has been politically problematized in dis- ability rights platforms, reinforces ableist norms, and alienates potential convivialities: “To claim our bodies as defective, and to pair defect with cure . . . disregards the experiences of many disabled people.”36 Disability here is not only the “narrative prosthesis”37 through which the trans body will overcome and thus resolve its debility but also the “raw material out of which other socially disempowered communities make themselves visible.”38 Seen through this mechanism of resource extraction, disability is the disavowed materiality of a trans embodiment that abstracts and thus effaces this materiality from its self-production.
Toby Beauchamp adds to the conversation about cure the notion of concealment via legal (identity documents) and medical intervention, stating: “Concealing gender deviance is about much more than simply erasing transgender status. It also necessitates altering one’s gender presentation to conform to white, middle-class, able-bodied, heterosexual understandings of normative gender.”39 The cure, then, revolves around rehabilitation to multiple social norms. Beauchamp further notes that of course the pro- cess of diagnosis and treatment inevitably reinforces this rehabilitation: “Medical surveillance focuses rst on individuals’ legibility as transgender, and then, following medical interventions, on their ability to conceal any trans status or deviance.”40 While access to adequate and sensitive health care for trans people can be a daunting if not foreclosed process, emergent conversations on “transgender health” can also function to reassert neoliberal norms of bodily capacity and debility.41 The transnormative subject might categorically reject the potential identification and alliance with disability, despite the two sharing an intensive relation to medicalization, and perhaps because of the desire for rehabilitation and an attendant indebtedness to medicalization. Clare avers that while the “disability rights movement fiercely resists the medicalization of bodies” to refuse the col- lapsing of the body “into mere medical condition,” in his estimation “we haven’t questioned the fundamental relationship between trans people and the very idea of diagnosis. Many of us are still invested in the ways we’re medicalized.”42
Even in politically progressive narrations of transgender embodiment, for example, an unwitting ableism and the specter of disability as intrinsic disenfranchisement often linger as by-products of the enchantment with the transformative capacities of bodies. For example, Eva Hayward’s take on the “Cripple” toggles a very tenuous line between the “Cripple” as a metaphor of regeneration and the crippling effects of amputation.43 Likewise, Bailey Kier, describing an instance of fishes’ ability to transsex in response to toxic endocrine-disrupting chemicals (EDCs), wonders if such transformations are a “technology beyond our grasp,” disregarding the uneven biopolitical distribution of such toxins that render his desires for a global “embracing [of] our shared transsex” violently idealistic: “EDCs are part of the food, productive and re/productive chain of nonhuman and human life and we will need to devise ways, just like sh, to adapt to their influence.”44
I would thus argue that there is a third element here that produces disability as the disavowed material co-substance of trans bodies. While there are understandable desires to avoid stigma and, as the ADA demonstrates, a demand for bodies with disabilities to integrate into a capitalist economy as productive bodies, the third factor involves aspirational forms of trans exceptionalism, one version of which is about rehabilitation, cure, and concealment. However, this exceptionalism is not only about pass- ing as gender normative; it is also about inhabiting an exceptional trans body—which is a different kind of trans exceptionalism, one that gestures toward a new transnormative citizen predicated not on passing but on “piecing,” galvanized through mobility, transformation, regeneration, flexibility, and the creative concocting of the body. Regarding “piecing” as an elemental aspect of neoliberal biomedical approaches to bodies with disabilities now globalized to all bodies, Snyder and Mitchell argue that the body has become “a multi-sectional market” in distinction to Fordist regimes that divided workers from each other:
We are now perpetual members of an audience encouraged to experience our bodies in pieces. . . . Whereas disabled people were trained to recognize their disabled parts as definitely inferior, late capitalism trains everyone to separate their good from bad—a form of alienation that feeds the market’s penchant for “treating” our parts separately. The body becomes a terrain of definable localities, each colonized by its particular pathologies dictated by the medicalized marketplace.45
While this partitioning of the body is not a recent emergence, in that there is a long history of bodily compartmentalization as a prerequisite for capitalist production,46 this piecing is not only about productive capacities but also about extending the body experientially and extracting value not just from bodies but from body parts and particles.
In this economy of alienated parts, piecing becomes a prized capacity. Jack Halberstam observes that “the transgender body has emerged as futurity itself, a kind of heroic fulfillment of post-modern promises of gender flexibility.”47 Halberstam is cautious about overinvesting in gender fluidity as transgressive capacity, noting that market economies already capitalize on “flexibility” as the hallmark of neoliberal economic productivity. But which transgender body (bodies?) is actually understood as “futurity itself”? This suturing of trans to exceptional futurity and the potential that the future offers are the new transnormative body. Again, this is not the transnormative body that passes but the transnormative body that “pieces,” the commodification not of wholeness or of rehabilitation but of plasticity, crafting parts from wholes, bodies without and with new organs. Piecing thus appears transgressive when in fact it is constitutive not only of transnormativity but also of some aspects of neoliberal or market economies.
To situate this trans body that is “futurity itself,” we might want to turn to trans organizing. Importantly, strategic interfaces between disability law and trans discrimination are also mirrored in growing political organizing and alliances between the two groups. One recent example includes a coalition of trans and persons with disabilities organized at the University of California, Santa Barbara, to jointly address issues of access, surveillance, and spatial configurations that dictate the gendered and abled expectations of public restrooms called PISSAR (People in Search of Safe and Accessible Restrooms).48 As another example, the Transgender Law Center in San Francisco has an activist handbook titled Peeing in Peace that uses disability-informed arguments for gender-neutral public toilets.49
Along with a distinction between the disability rights movement and disability justice organizing maintained by activists such as Mia Mingus, one should also retain a distinction between the transgender rights movement and trans justice organizing. TransJustice, one of the two major initiatives of the Audre Lorde Project in New York City, is a political group created by and for trans and gender-nonconforming people of color. Trans- Justice works to mobilize its communities and allies into action on the pressing political issues they face, including gaining access to jobs, housing, and education; the need for trans-sensitive health care, HIV-related services, and job training programs; and resisting police, government, and anti-immigrant violence. The members of TransJustice tend to be African-American and Latino working-class youth, and most are male-to-female (MTF). The convergence of racial identity and MTF seems significant and hardly incidental. Everything available on economic indicators, transgender health, incarceration, employment, street violence, and education amply demonstrates that trans women of color, especially black trans women, are massively disenfranchised in relation to other trans bodies and that the gulf between them and (white) FTMs is vast and growing. Data are sparse but stark: “In 2003, 14 murders of transpeople were reported in the U.S., and 38 worldwide. Most were MTF and most were people of color.”50 The major concerns of TransJustice members cluster around access to school, employment, welfare provisions, and uncontaminated and inexpensive drugs and treatments—hormones, fillers, and surgeries. Many articulate their awareness of trans identity occurring simultaneously with a realization that they were attracted to the “wrong” sex (so not only or necessarily that they were in the “wrong” body.). They desire to pass as beautiful, feminine, sexy. While a trans politics might render such forms of passing either a validation of a radical identity or a version of assimilation, misrecognition, or “selling out,” for these members it is often entwined with, albeit obliquely, avoiding police harassment, community stigmatization, and familial rejection. Their engagement with the medical industrial complex and with desires for transformative embodiment is not necessarily or only victorious, empowered by choice, or ultimately capacity building. Medicalization can be experienced as transformative, capacitating, debilitating, or all of the above, not to mention exclusionary.51 They do not embody “futurity itself”; rather, their bodies can be read as sites of intensive struggle (medical, educational, employment, legal, social) over who indeed does get to embody—and experience—futurity and who as a result will be cast off as the collateral damages of such strivings to capture the essence of the future.
Kris Hayashi, former director of the Audre Lorde Project, elaborates the emphases of trans organizing in New York City in general and Trans- Justice specifically:
In New York City, TGNC [trans-gender nonconforming] youth of color and low-income youth in the West Village neighborhood face ongoing violence and harassment at the hands of the police, as well as from residents who are primarily White and middle class to upper class. As a result, FIERCE!, an organization led and run primarily by TGNC low-income and homeless youth of color, prioritizes issues of police brutality and violence, as well as gentrification. TransJustice, a project of ALP [the Audre Lorde Project] that is led and run by TGNC people of color, has prioritized issues of unemployment and education access due to high rates of unemployment (60%–70%) facing TGNC people of color. Also in New York, a coalition of organizations and groups including TransJustice, Welfare Warriors, and the LGBT Community Center’s Gender Identity Project have prioritized efforts to end the regular harassment and discrimination faced by TGNC people seeking to gain access to public assistance. Finally, many TGNC groups led primarily by people of color and low-income communities have also prioritized ending the U.S. war on terrorism, both in the United States and abroad.52
The work of TransJustice situates the vexed relations to futurity that its trans constituency must mediate in terms of quotidian survival. In doing so, TransJustice activists put transnormativity in full relief as a function of the privilege of whiteness, foregrounding a critical approach to the racializing technologies of trans identity. Their analyses centralize the privilege of who is able to be disabled and is able to be transgender as a function of state and legal recognition that is often elusive for their bodies, demonstrating capacity—the ability to not just be but become, not to pass but to piece—rather than only debility, deviance, victimhood, ostracization, or nonnormativity at the center of these projects. The trans body that pieces, then, also passes not as gender-normative male or female but as trans. Susan Stryker and Nikki Sullivan, elaborating on this capacitation through piecing, write: “Our research . . . leads us toward a new under- standing of bodily integration, one predicated not on the organic integrity of the human organism, but rather on the body’s suitability for integration, its ability to be integrated as a biopolitical resource into a larger sociotechnical field, or into an apparatus such as the State.”53 In other words, they render a critique of the rehabilitation model as intrinsically a return to wholeness. Integration through piecing, rather than wholeness through passing, becomes a valued asset in control societies. Stryker and Sullivan continue: “The integrity of the body—that is, the ability of the body to be integrated—is thus, paradoxically, dependent on its enfleshment as always already torn, rent, incomplete, and unwhole.”54 This capacity to “integrate” oneself—not to pass but to piece—thus mediates the production as well as the lived experiences of molar categories such as race, class, and gender. What I am arguing here is that capacitation around health and attendant registers of bodily prowess, not necessarily identity as trans or disabled or abled or queer or not-trans, ultimately serves as the dividing social practice in biopolitical terms.55 The debates about the disabled self and the nondisabled other reflect wider discourses of how those selves are materially constructed through the discourses that abound on abject and successful bodies.
While the capacity to piece (in order to pass as not passing) can produce new forms of transnormativity, Stryker and Sullivan rightly point out that bodily comportments that do not strive to manifest wholeness or an investment in the self as coherent do not have to reproduce liberal norms of being: “It is this aspect of bodily being that the liberal discourse of property rights in oneself does not, and cannot, account for; it is this aspect of bodily being that we seek to highlight when suggesting that individual demands for bodily alteration are also, necessarily, demands for new social bodies—new somatechnologies that ethically refigure the relationship between individual corporealities and aggregate assemblages of bodies.”56 This formulation, then, of new somatechnologies that refuse the individualizing mandate of neoliberal paradigms of bodily capacity and debility in favor of articulating greater connectivities between “aggregate assemblages of bodies,” precisely flags the challenge of crafting convivial political praxes. And yet, it is also the case that such political praxes must never occlude the stratifications inherent in the quest to access such somatechnologies. The transnormative body of futurity that reflects neoliberal celebrations of flexibility and piecing remains an elusive reality for many. The distinctions between passing and piecing are thus fluid and shifting, given the kinds of piecing together of medical access and legal accommodations that trans of color bodies are forced to seek in any efforts to pass.
III. Becoming Trans? A Geopolitics of Racial Ontology
Molecular lines of flight trace out little modifications, they make detours, they sketch out rises and falls, but they are no less precise for all this,
they even direct irreversible processes. . . . Many things happen on this second kind of line—becomings, micro-becomings, which don’t even have the same rhythm as history. This is why family histories, registrations, commemorations, are so unpleasant, whilst our true changes take place elsewhere—another politics, another time, another individuation.
—Gilles Deleuze, Dialogues II
Thus far I have surveyed how biopolitical recognition of disability has installed a version of gender normativity, in this case specifically through the political apparatus of the ADA. I have then outlined forms of bodily exceptionalism that may produce trans ableist discourses. I turn now from the focus on subject construction—the trans subject(s) and the disabled subject(s) that are hailed and/or denied by legal legitimation, state recognition, public accommodation, and resource distribution—to offer a reconceptualization of corporeal assemblages that foreground ontological continuums in relation to epistemological bifurcations. It is also an approach that highlights how bodies are malleable not just as subjects but also as composites of parts, affects, compartmentalized capacities, and debilities, as data points and informational substrates. This continuous oscillating between the identity or rights-based claims of the trans subject and the disabled subject seeking recognition and biopolitical control that operates largely through securing the sub- and paraindividual capacities of bodies for privatized (in the United States) regimes for pay is necessary because these “poles,” as Gilles Deleuze and Félix Guattari note, are never without each other: “These two poles are inseparable; they entertain perpetual relations of transformation, conversion, jumping, falling, and rising.”57 Further, if it is understood that the battle against the extraction and exploitation of bodily capacities and habituations is not going to happen through the terrain of intersectional politics alone, and that in fact biopolitical control societies work insidiously by using disciplinary power to keep or deflect our attention around the subjection of the subject, thus allowing control to manifest unhindered, I would argue another interpretation of disciplinary apparatuses is that in part they function as foils for control mechanisms.
Enacting this oscillation moves between questions such as what dis- ability is and what trans is toward what disability does and what trans does. In disability studies, James Overboe develops the Deleuzian notion of the impersonal life—one without a self—to cut through a disability politics of identity that centralizes the self-reflexive individual. He generates this intervention in order to “affirm disabled lives that are simply expressed without cognition, intent, or agency.” Overboe writes: “The vitalism of an impersonal life is often considered noise that will be filtered out, in the name of clarity, in order to facilitate the real business of social change and so-called emancipation. This re-establishes and reinscribes the dominant language or communication style associated with being a person or individual with agency.”58 There is a refusal here of the medical impairment versus social construction impasse, in part because Deleuzian theory embraces biomateriality, foregrounding vitalism and potentiality of impairment rather than seeking its recontextualization in the social. Overboe also reminds us that the construct of the subject itself—even the disabled subject—is already discursively abled.
One could also point to efforts to articulate trans as an ontological force that impels indeterminate movement rather than an identity that demands epistemological accountability or as a movement between identities. Paisley Currah, Lisa Jean Moore, and Susan Stryker explicate the “trans-” (trans-hyphen) in the sociopolitical;59 Jami Weinstein develops the notion of transgenre.60 Deleuze and Guattari’s use of the term trans- sexuality opens to a uid spectrum of possibility: trans as a motion, not an identity, and trans as a continuum of intensity. For trans studies, Mel Chen argues that the “simultaneous limitation and promise” of a Body without Organs (BwO) is “precisely that the genitals (or nongenitals) matter, but are not necessarily constrained by normative gender and sexuality.”61 Chen is pointing to trans as a reordering of what organs signify which genders, or if any organs need to signify genders at all.62
While earlier I highlight the troubling discourse of shared transsex in relation to unmarked and uneven biopolitics of toxicity distribution, Kier’s formulation of transgender as all-encompassing category—“everyone on the planet is now encompassed within the category of transgender”— is suggestive to me not of the desire to retain the category of transgender but, rather, of its imbrication in an unfolding interspecies biopolitical vision. Kier proclaims that “we might be better off responding to this rearrangement, not through fear of the eco-catastrophic assumptions transsex invokes, but by embracing our shared interdependent transsex.”63 Weinstein also mobilizes the notion of becoming as a dismantling of the “very speciation and biopolitical identity construction” that Michel Foucault elaborates.64 In a critique of species taxonomy, Julie Livingston and I use the term biopolitical anthropomorphism or, reworded more appropriately, biopolitical anthropocentrism to “highlight the biopolitical processes that cohere the centrality of the human, and of certain humans; and, the tendency of biopolitical analyses to reinscribe this centrality by taking human species as the primary basis upon which cleavages of race and sex occur.”65 Biopolitics, as Foucault explains, is the process by which humans become a species (and in fact specimens) to join all other biological species. This becoming is also the process by which anthropomorphic frames of the human thus take force and are consolidated. Foucault explains in Security, Territory, Population that “the dimension in which the population is immersed amongst the other living beings appears and is sanctioned when, for the first time, men are no longer called ‘mankind’ (le genre humaine)” and begin to be called “the human species (l’espece humaine).”66 A paradox occurs: the animalism of humans—“the life of the body and the life of the species”67—is taken up as a project of population construction, and humans join species. The (androcentric) human is thus rearticulated as an exceptional form of animality within an anthropomorphized category: humanity. Therefore, although Foucault’s own work does not explore the implications of this in terms of interspecies relating, his theory of biopolitics understands anthropocentrism as a defining facet of modernity.
Transgender studies has taken on the question of speciation through a posthumanist or nonhumanist turn; in fact, it is leading the way toward posthumanist inquiries, a fair amount of it emboldened by Deleuzian thought. This meeting of transgender studies, animal studies, and post- humanist studies is fantastically rich, considerably complicating humanist presumptions of sex dimorphism68 and conceptualizing sex as a reaction norm in dynamic emergence with the environment and as an effect of genes and (hormonal) environments interfacing.69 Myra Hird’s work defuses the nature/culture distinction by unpacking the human exceptionalism embedded in continually evoking the trans human body as transgressive. Given its plentitude in nonhuman forms, Hird argues that trans is not a cultural artifact of technological means, or gloriously perverse in that it is unnatural, but is in fact constitutive of nature itself. Hird deploys trans not just beyond or across sex but across “traditional species classifications.” Taking a cue from the complexity of intersex and transsex and the nonapplicability of gender and sexual dimorphism to most nonhuman life, Hird argues against a nature/culture binary where the human trans body is understood as a technological invention alone. The upshot of Hird’s argument is that trans is not transgressive but, rather and in fact, natural.70 In concert with Vicky Kirby’s proposition that nature is writing and re-presenting itself, and that perhaps culture has been nature all along,71 Hird argues that technology must be understood through its interspecies dimensions: “The use of technology to distinguish between nature and culture obscures the very real and energetic invention and use of technology by nonhuman living organisms . . . as well as the extent to which so-called human technologies actually mimic technology already invented by other species.”72 Hird’s argument, which complicates if not refuses the nature/culture bifurcation, has vast implications for the debates in disability studies about the biomedical versus social model of disability. Within the context of transgender jurisprudence and activist debates regarding the use of the medical model within legislative battles for health care and attendant provisions, her analysis suggests a strategic deployment of the model that might defuse pathological conceptualizations when posited as a manipulation of the terms of technology and what constitutes the natural.
But despite challenging the foregrounding of the human and its centrality to de ning the parameters of sex, gender, and sexual reproduction, the deepening conversations between transgender studies, animal studies, and posthumanism has fastidiously avoided an engagement with disability studies, a eld always in conversation with arrangements of the human, especially as it relates to cognitive and mental disabilities. This occlusion is further notable in light of a rich, emerging dialogue between disability and animal studies.73 Further, the growing partnership between trans- gender studies and animal studies has elided discussions of racial difference crucial to debates about biopolitical anthropocentrism, foreground- ing instead the category species, as if species were not also a forum for understanding cleavages of racial difference.74 One effort to redress these elisions is Chen’s articulation of the “preflexal trans-”—a materialism of grammar—as a “way to explore that complexity of gender definition that lies between human gender systems and the gendering of animals.”75 In attending to the relationship between human animals and nonhuman animals as a racializing technology of biopolitics, Chen’s analysis articulates trans not just as “mutilating gender,”76 as the rescrambling and reorganizing of gender, but trans as mutilating or perhaps better stated as mutating race as well. In some cases, this mutating is a reterritorialization and enhanced capacitation of racial privilege and the projection of racial coherence through rearranging gender. Bobby Jean Noble, for example, describes his process of regeneration from a working-class butch woman to a trans man as one of moving from “formerly off-white [to a] now White person” in a landscape wherein “the ‘self’ is the hottest and most insidious capitalist commodity.”77 The confusing designation of “off-white” notwithstanding, Noble describes this capacitation of race—a revival of the privileges of whiteness now afforded through masculinity—as a by- product of trans body modi cation. If one queries this derivative formulation, however, the possibility that mutilating gender might not be so easily cleaved from (desires for?) racial recuperation, or from constructs of able- ism, needs to be considered. What kinds of attempted recuperation of one sort or another subtend or even preface these rearrangements of gender?
Recall that for Foucault racism is not derivative of biopower but, rather, a prerequisite for how biopolitics works; that is to say, Foucault wrenches racism out of notions of cultural tolerance by stating that the caesura in the biological spectrum that is accorded to race is necessary for licensing the four coordinates of biopolitical will: making live, making die, letting live, letting die. This formulation of racism as a “caesura in the biological domain”78 can be mobilized as a preemptive critique of a posthumanism that does not acknowledge race as a critical threshold of demarcation. Given the centrality of racial demarcatedness to biopolitics, I read Foucault’s later explanations of biopolitics, or what he calls the regime of security, later recapitulated in Deleuze’s theorization of “control societies,” as in fact a geopolitics of racial ontology.
Re-suturing the foundational function of race within biopolitics to the production of ontologically irreducible entities in control societies, the geopolitics of racial ontology marks the manifestation of different spatializing regimes of the body, and its particles, such that the biological caesura that demarcates the cut of or for racism is now not just a question of visible racial difference or of the taxonomic and eugenic science of phrenology and the scientific racism of the eighteenth through early twentieth centuries. It is, rather, the biotechnologies of genetic engineering, assisted reproduction technologies, human genome sequencing, and phenotypical variation—which may well intersect with/appear as gendered transformations—that mean the “cut” of racism is not made only through disciplinary categories of race but, more perniciously, through biopolitical control aggregates of population.79 This geopolitics of racial ontology destabilizes the relentless focus on epistemological correctives that tend to dominate political interventions. But, more trenchantly, the emphasis on geopolitics amends what might otherwise be a location-less notion of ontology, an unmarked locational investment of recent work on ontology, much of it neither accounting for the productive force of geopolitics within its scholarly purview nor acknowledging the geopolitical forces that enable theorizing.
In the oscillation between discipline and control, which is less about the end of disciplining and more about the constellation of relations between discipline and control, the question, are you trans? morphs to, how trans are you? Both discipline and control pivot on the fantasy of a body that is concretely and distinctly a real trans body—the (transnormative?) body that pieces—manifest in opposition to the body that is most certainly cisgender. Similarly, the question, are you disabled? morphs to, how abled are you? and how disabled are you? In the context of an array of medical procedures that change in terms of access, signification, cultural capital, and socialization, the moves around these questions are not signaling merely degree. The end goal—to pass? to piece?—is impossible and always shifting: there is no trans. Trans becoming masquerades as a teleological movement, as if one could actually become trans. Trans is often mistaken as the horizon of trans and, as such, is mistaken for becoming trans as linear telos, as a prognosis that becomes the body’s contemporary diagnosis and domesticates the trans body into the regulatory norms of permanence.80
Becoming trans, then, as opposed to trans becoming, must highlight this impossibility of linearity, permanence, and end points. In Deleuzian terms, becoming is the “I” cascading into the impersonal, the stripping of all registers of signification that make each body succumb to subjectification over “significance.” Becoming, as Weinstein contends, is a “wholesale deterritorialization of the human,” and a “becoming imperceptible”—a divestment of codes, of signification, of identity and a process of taking on the register of the impersonal. Becoming is not about trying to make the body more capacitated but about allowing and reading more multiplicity, multiplicities of the impersonal and of the imperceptible. Importantly, becomings have no static referent of start point, end point, or climax; they have no narrative. Becoming is awash in pure immanence, never coincident with itself, marked only by degrees of intensity and duration.81 But none of this is to obscure the fact that becoming has become a zone for pro t for contemporary capitalism, for neoliberal piecing and profiteering, a mode through which pro t is being aggressively produced. And as such, all theorizations of becoming are generated through and within the geopolitics of racial ontology that it inhabits.
As trans transition is increasingly theorized as the mobilization, modulation, and modi cation of bodily matter rather than a retroactive cutting and severing from being in the wrong body, control societies must be understood as deeply sympathetic to if not partially productive of this reframing. Control mines gradations of surface and depth, tension and attention, penetration and withdrawal, finding multiple uses for the diversification of vestments and investments. Once again, however, we can deexceptionalize trans bodies, as they are neither exceptionally susceptible to control and its forms of continuous surveillance (given the continuities between rhinoplasty and other trans surgical procedures, for example, and body modi cation in general),82 nor are they exceptionally capable of modulation, flexibility, and attunement.
Biopolitical control foregrounds the subindividual capacities, the nonhuman capacities, the prosthetic capacities, the molecular capacities, and the hormonal capacities and manipulates the telos of degree granting driven by the medical industrial complex. Beatriz Preciado develops a formulation of the “pharmaco-pornographic” to describe the proliferation of bodily modulations in control societies, forms of microcontrol he calls “soft technologies” that “enter the body to form part of it: they dissolve in the body; they become the body”: “Here the body no longer inhabits disciplinary spaces, but is inhabited by them. The bio-molecular and organic structure of the body is a last resort for these control systems.”83 The disciplinary spaces Preciado writes of—encompassing the molar categories of race, gender, sex—proliferate from bodily habitations of identity to inhabitations of the body. This inhabitation is perhaps one of the most pernicious modalities of power that control can manifest—control as discipline par excellence, in that discipline reproduces itself continuously throughout time and space. These “micro-prosthetics” of control, which Preciado claims impel “a process of miniaturization,” “take the form of the body; they control by transforming into ‘body’, until they become inseparable and indistinguishable from it.”84 Thus, the term body modi- cation becomes a redundancy: the body is (endless) modi cation. This body, however, is not only the contoured organic body with a race and a sex; it is composites of information that splay the body across registers of disciplinary space and time. The target is data, not only identity or the subject or its representation. Identitarian communities of belonging— traditionally understood through disciplinary categories of identity, spatiality, coherence—are reorganized through statistical populations, stratified through aggregates of biopolitical life chances in the nexus where state, market, scientific, and geopolitical realms meet.
While I find Preciado’s description of control economies of bodily inhabitation very persuasive, he optimistically describes the molecular as the “paradoxical condition of contemporary resistance and revolt”:
We are molecularly equipped to remain complicit with dominant repressive formations. But the contemporary pharmaco-pornographic body . . . is not docile. This body is not simply an effect of the pharmaco-pornographic systems of control; it is first and above all the materialization of . . . “power of life” that aspires to transfer to all and to every body. This is the paradoxical condition of contemporary resistance and revolt: pharmaco-pornographic subjectivity is at the same time the effect of biopolitical technologies of control and the ultimate site of resistance to them.85
We might want to pause at the formulation of the molecular and the nondocile body within which it resides as “the ultimate site of resistance,” an ontologizing of the molecular as a thriving site of resistance by virtue of its mere presence and flexible relation to biomedical control economies (indeed, part of the transnormative body that pieces, and driving the reterritorialization of whiteness). Given the geopolitics of racial ontology that condition any possibilities for becoming, for a wholesale deterritorialization of the human, and given that all the coordinates around the relation of the medical model to the social model and the access to subject recognition and the medical industrial complex revolve around not just gender and sexual alterity but also racial alterity and disenfranchisement through racial difference, I want to propose becoming trans as a capacitation of race, of racial ontologies, that informs the functioning of geo- and biopolitical control. Becoming trans is a process that courts not only the transformation of bodies in terms of gender, but also solicits the capacity of race to reinvent its terms. Race here is understood not only as a function or synonym of color but also, and perhaps more perniciously, as speciation. Becoming trans is distinct from trans being, or trans normativity that revels in the futurity of the body that pieces, because it specifically and deliberately acknowledges a political commitment to thinking through the forms of racial capacitation and reterritorialization that subtend and inform trans movements.
We could see becoming trans, then, as the dissolution of this category of signification through manifesting the intensive multiplicity of race, outpacing the forces of signification that seek to contain and compartmentalize what is raced, what is not raced. Insofar as race continues to be de ned in relation to the White Man who sets its parameters, what Amit Rai calls “race racing” proliferates racial ontologies that are irreducible and unto themselves, in relation through in nite variation rather than difference from (the White Man). The impetus for race racing stems, for Rai, from the context of antiracist organizing in Britain, where he laments the continual reiteration of the centrality and normativity of white subjects and bodies in even the most progressive antiracist political forums. On thinking race not representationally but intensively, what he calls race racing, Rai writes:
If one is to consistently think race racing as an intensive process, the multiplicity of race lacks any resemblance to itself; race racing multiplicities give form to processes, not to this or that final product (a race, a name . . . ). Indeed, the end results of processes realizing the same multiplicity may be highly dissimilar from each other, like the spherical soap bubble and the cubic salt crystal, or like Jazz music and the narrative novel, “which not only do not resemble one another, but bear no similarity to the topological point guiding their production.” The multiplicity of race racing is of an obscure yet distinct nature quite different from the clear and distinct identity of rationalistic essences.86
Race racing, as Rai elaborates, tracks the insistent becoming of race, the way race—“lack[ing] any resemblance to itself”—is always mutilating and mutating (to invoke the language from mutilating gender) its form in order to resituate and revive its capacitation within biopolitical fields. Race racing then, allows a reading of racial capacitation—deterritorialization, reterritorialization—in becoming trans. Becoming trans is of course just one potentiality of race racing. But if we are serious, to invoke Chen and others who think of trans as a movement not solely tethered to modulations and modi cations of gender and sexuality but also of species, race racing changes trans becoming insofar as it potentially changes what race is, proliferates its intensive, singular forms, reorganizes its registers of significance and signification, and reterritorializes and multiplies its capacitation, its presence, its mutability. But becoming trans also carries through and out a process of racialization as much as it also marks an intensive race racing, a moment of race becoming futurity. There is no doubt that the reterritorialization of whiteness, in particular of white masculinities, might occur through the reassembling of gender and sexuality into versions of transnormativity. But becoming trans as a practice and a politics takes on a deterritorializing force not only in relation to gender and sex but also in relation to race and speciation. The question then is not, does gender and sex nonnormativity lead to racial nonnormativity? but, rather, about creative lines of flight that mutate and distort and swerve in Lucretian fashion. Not swerve from, just swerve, creating intensive rather than qualified difference. Thinking of becoming trans as a form of race racing illuminates the relations of white trans-normative (FTM) bodies of futurity—the ones that pass by exemplifying piec- ing—to the TransJustice (MTF) bodies of color, those that struggle to piece (in order to perhaps pass), by seeing all these bodies as implicated in the redistribution of capacitations and reterritorializations of race in their intensive differences. The multiplicity, not the either/or of normativity or nonnormativity, of racial and gender difference is foregrounded. Thus, passing and piecing would be destabilized from their discrete sexual and racial referents and understood, rather, as produced through interfacing assemblages of de- and reterritorialization, of proliferating not only genders but also races and, indeed, species.
A deconstructive model of race insistently repositions the white male subject as determinant of what race is, of making sense or different sense of a representational format or forum; language dominates the political realm here. But theorists such as Arun Saldahna, Amit Rai, and myself are arguing for a political and theoretical methodology that intensifies and proliferates race rather than deconstructs it, a proliferation that, rather than hoping to dissolve binaries, makes them fade through the overwhelming force of ontological multiplicity, attuned to the perpetual differentiation of variation to variation and the multiplicity of affirmative becomings. If race is a technology of regeneration, in that race is insistently reinventing itself in manners both “obscure” and “distinct” as Rai avers, this methodology doggedly pursues the inventive movements of race itself. Writing that “race is a whole event,”87 Saldahna exhorts: “Every time phenotype makes another machinic connection, there is a stutter. Every time bodies are further entrenched in segregation, however brutal, there needs to be an affective investment of some sort. This is the ruptural moment in which to intervene. Race should not be eliminated, but proliferated, its many energies directed at multiplying racial differences so as to render them joyfully cacophonic.”88
This joyful cacophony is in part what Rai understands as “an experimentation on race itself,” one that would “continuously mutate, never resembling itself, changing the metric of its own measure through a resonance that moves beyond its terms.”89 Unlike for Preciado, for whom resistance is simply a priori installed in the molecular as the “ultimate site of resistance” and utterly unbeholden to any collective—an ontologizing and individuating politics at best, as Jord/ana Rosenberg so deftly demonstrates90— Rai calls for social and political practices of experimentation, a deeply pragmatic manipulation of the partitioning capacities of bodies. I suggest this “[move] beyond its terms” is one way of working through and also against how biopolitical control seeks to modulate sub- and para- individual capacities of the body (it seeks to modulate the impersonal, the becoming) while promoting an individual recourse to subject identification. Becoming trans, as suggested by race racing, would be a politics of manifesting beyond what control can control, a molecular line of flight, a moment of intensification in the process of becoming that is characteristic of race racing. As with all becomings, lines of flight are immanent, and their availability for reterritorialization, or capacity to newly territorialize, imminent. The revolution is not molecular; rather, movement resides in the interstitial shuttling—“the ruptural moment in which to intervene”—between intensive multiplicity and its most likely recapture.
Notes
1. Donavan Slack, “Biden Says ‘Transgender Discrimination Civil Rights Issue of Our Time,’ ” Politico, 30 October 2012, www.politico.com/politico44/2012/10/biden-says-transgender-discrimination-civil-rights-147761.html.
2. See Siobhan B. Somerville, “Queer Loving,” GLQ: A Journal of Lesbian and Gay Studies 11, no. 3 (2005): 335–70.
3. There was healthy skepticism from other quarters, including trans rights grassroots activists asking the important questions about welfare, safety, work, economics, and health care. For some examples, see S. E. Smith, “Joe Biden Calls Transgender Discrimination ‘the Civil Rights Issue of Our Time,’ ” xo Jane, 31 October 2012, www.xojane.com/issues/joe-biden-calls-transgender-discrimination-the-civil-rights-issue-of-our-time; Natasha Lennard, “What Took Biden So Long on Trans Discrimination?,” Salon, 31 October 2012, www.salon.com/2012/10/31/if_trans_discrimination_is_the_civil_rights_issue_of_our_time_why_is_biden_just_mentioning_it_now/.
4. Beth Povinelli, lecture at American University of Beirut, 14 March 2013.
5. C. Riley Snorton and Jin Haritaworn, “Trans Necropolitics: A Transnational Re ection on Violence, Death, and the Trans of Color Afterlife,” in Transgender Studies Reader 2, ed. Susan Stryker and Aren Z. Aizura (New York: Routledge, 2013), 67.
6. Susan Stryker and Aren Z. Aizura, “Introduction: Transgender Studies 2.0,” in Transgender Studies Reader 2, 10.
7. Aren Z. Aizura, “Of Borders and Homes: The Imaginary Community of (Trans)sexual Citizenship,” Inter-Asia Cultural Studies 7 (2006): 295.
8. Susan Stryker (personal communication via e-mail, 20 June 2013 and 25 August 2013) has referred to this as “transnormative citizenship.” As she wonders: “Is trans just an additive to the concept of homonationalism, or does it create (trans) gender trouble for the concept? My own sense is that homonationalism involves the capture of homonormativity by state/governmentality, and the capture of transnormative gender is another instance of the same process, but is not necessarily homo (sometimes it is, sometimes it isn’t)” (23 June 2013).
9. Dan Irving writes that “constructions of transsexuals as viable social subjects by medical experts, transsexual individuals, researchers, and allies were, and continue to be, shaped significantly by discourses of productivity emerging from and reinforcing regimes of capitalist accumulation. To move toward achieving social recognition, the transsexual body must constitute a productive working body, that is, it must be capable of participating in capitalist production processes.” Irving claims that this results in “the construction of transsexual subjectivities in ways that reinforce dominant exploitative class relations.” Perhaps it is worth affirming that while perhaps correct, this assessment can be made of many bodies solicited for neoliberal subjecthood. Irving goes on to exceptionalize the trans body by arguing that “appeals to mainstream society to accept transsexuals as legitimate subjects often emphasized their valuable contributions to society through their labor.” Dan Irving, “Normalized Transgressions: Legitimizing the Transsexual Body as Productive,” Radical History Review 100 (2008): 42.
10. Karen Nakamura, “Trans/Japan, Trans/Disability” (paper presented at “Debilitating Queerness” conference, University of Maryland, College Park, 5 April 2013).
11. See David Valentine, Imagining Transgender: An Ethnography of a Category (Durham, NC: Duke University Press, 2007); Susan Stryker, “We Who Are Sexy: Christine Jorgensen’s Transsexual Whiteness in the Postcolonial Philippines,” Social Semiotics 19, no. 1 (2009): 89; Janice M. Irvine, Disorders of Desire: Sexuality and Gender in Modern American Sexology (Philadelphia, PA: Temple University Press, 1990).
12. Section 12221 of the 1990 Americans with Disabilities Act reads as follows: (a) Homosexuality and bisexuality: For purposes of the definition of “disability” in section 12102(2) of this title, homosexuality and bisexuality are not impairments and as such are not disabilities under this chapter. (b) Certain conditions: Under this chapter, the term “disability” shall not include (1) transvestism, transsexualism, pedophilia, exhibitionism, voyeurism, gender identity disorders not resulting from physical impairments, or other sexual behavior disorders; (2) compulsive gambling, kleptomania, or pyromania; or (3) psychoactive substance use disorders resulting from current illegal use of drugs.
13. Adrienne L. Hiegel, “Sexual Exclusions: The Americans with Disabilities Act as a Moral Code,” Columbia Law Review 94, no. 4 (1994): 1451.
14. L. Camille Herbert, “Transforming Transsexual and Transgender Rights,” William and Mary Journal of Women and the Law 15, no. 3 (2009): 540–41.
15. R. Nick Gorton, “Transgender Health Bene ts: Collateral Damage in the Resolution of the National Health Care Financing Dilemma,” Sexuality Research and Social Policy Journal of NSRC 4, no. 4 (2007): 84. Gorton continues: “Therefore, although obtaining transgender services through Medicaid is difficult but possible depending on the court, obtaining federal protections through the ADA involves convincing courts not only that gender identity disorder is a legitimate illness needing treatment but also that the exclusion within the law itself is unconstitutional—a much more formidable challenge. To date, no court has struck down the ADA’s exclusion of transgender people” (84).
16. Kari Hong, “Categorical Exclusions: Exploring Legal Responses to Health Care Discrimination against Transsexuals,” Columbia Journal of Gender and Law 11 (2002): 123.
17. See Ruth Colker, “Homophobia, AIDS Hysteria, and the Americans with Disabilities Act,” Journal of Gender, Race and Justice 8, no. 1 (2004): 33.
18. Kevin M. Barry, “Disabilityqueer: Federal Disability Rights Protection for Transgender People,” Yale Human Rights and Development Journal 16, no. 1 (2013): 1–50.
19. We might ask what the shift from GID to gender dysphoria entails: Will there be a shift away from the emphasis on childhood? What new populations will be impelled and curated? While beyond the scope of this discussion, the elimination of GID from the DSM might entail that successfully litigating for ADA coverage of trans is an even more remote possibility.
20. Hiegel, “Sexual Exclusions,” 1452–53.
21. Nicole Markotic and Robert McRuer, “Leading with Your Head: On the Borders of Disability, Sexuality, and the Nation,” in Sex and Disability, ed. Robert McRuer and Anna Mollow (Durham, NC: Duke University Press, 2012), 165–82.
22. Sharon L. Snyder and David T. Mitchell, “Ablenationalism and the Geo- Politics of Disability,” Journal of Literary and Cultural Disability Studies (2010): 124.
23. Ibid., 122.
24. See “Queer Channel Media: Trans-washing the ADA,” ENDAblog, 28 July 2011, endablog.wordpress.com/2011/07/28/queer-channel-media-trans-washing-the-ada/.
25 Zach Strassburger, “Disability Law and the Disability Rights Movement for Transpeople,” Yale Journal of Law and Feminism 24, no. 2 (2012): 7.
26. If trans has become the figure of radical alterity from a now-domesticated queer, as it is increasingly claimed, then is trans the disabled Other of a queer able- ism? Is transphobia in queer organizations and communities, for example, in part a manifestation of ableism, of anxiety or phobia toward disability? This is not in any way meant to reduce transphobia to ableism, or to any otherism, but to ask what components, including race, class, and ableism, might be fueling the assemblage that is transphobia. Why is the Michigan Womyn’s Music Festival still barring trans women? Is the “inability” to completely embody originary biological femaleness responded to phobically, as if this inability were a disability? Is there value in conceptualizing transphobia as a variant of ableism?
27. Strassburger, “Disability Law,” 3–4.
28. Stryker, personal communication via e-mail, 25 August 2013.
29. Alvin Lee, “Trans Models in Prison: The Medicalization of Gender Identity and the Eighth Amendment Right to Sex Reassignment Therapy,” Harvard Journal of Law and Gender 31 (2008): 464–65.
30. Ibid., 470.
31. Jeannie J. Chung, “Identity or Condition: The Theory and Practice of Applying State Disability Laws to Transgender Individuals,” Columbia Journal of Gender and Law 21, no. 1 (2011): 1–45; Dean Spade, “Resisting Medicine, Re/Modeling Gender,” Berkeley Women’s Law Journal 18, no. 1 (2003): 37.
32. Stryker and Aizura, “Introduction,” 1.
33. Abby L. Wilkerson, “Normate Sex and Its Discontents,” in McRuer and Mollow, Sex and Disability, 184–85.
34. See Eli Clare, “Body Shame, Body Pride: Lessons from the Disability Rights Movement,” in Stryker and Aizura, Transgender Studies Reader 2, 261–65.
35. Clare, “Body Shame, Body Pride,” 262.
36. Ibid.
37. David T. Mitchell and Sharon L. Snyder, Narrative Prosthesis: Disability and the Dependencies of Discourse (Ann Arbor: University of Michigan Press, 2000).
38. David T. Mitchell and Sharon L. Snyder, “Introduction: Disability Studies and the Double Bind of Representation,” in The Body and Physical Difference: Dis- courses of Disability, ed. David Mitchell and Sharon Snyder (Ann Arbor: University of Michigan Press, 1997), 6.
39. Toby Beauchamp, “Artful Concealment and Strategic Visibility: Transgender Bodies and US State Surveillance after 9/11,” Surveillance and Society 6, no. 4 (2009): 47.
40. Ibid.
41. Jonathan M. Metzl and Anna Kirkland, eds., Against Health: How Health Became the New Morality (New York: New York University Press, 2010).
42. Clare, “Body Shame, Body Pride,” 265.
43. Eva Hayward, “Lessons from a Star sh,” in Queering the Non/Human, ed. Noreen Giffney and Myra J. Hird (Burlington, VT: Ashgate, 2008), 249–64. Hay- ward writes in a footnote: “Again, I risk reading the ‘Cripple’ as a trans-subject not to iterate the pathologization of trans-folks, but to explore the imaginings of the song. For the transsexual/transgender subject, gender assignments can feel ‘disabling’, even wounding. I’m speaking about this traumatic experience, not about transgressive exceptionalism” (254).
44. Bailey Kier, “Interdependent Ecological Transsex: Notes on Re/production,” in Stryker and Aizura, Transgender Studies Reader 2, 194, 196.
45. David T. Mitchell and Sharon L. Snyder, “Disability as Multitude: Re- working Non-productive Labor Power,” Journal of Literary and Cultural Disability Studies 4, no. 2 (2010): 190–91.
46. For an incisive critique of the ahistorical claims regarding the particlization of bodies necessary to capitalism, see Jordana Rosenberg, “The Molecularization of Sexuality: On Some Primitivisms of the Present,” Theory and Event 17, no. 2 (2014), muse.jhu.edu/journals/theory_and_event/v017/17.2.rosenberg.html.
47. Judith Halberstam, In a Queer Time and Place: Transgender Bodies, Subcultural Lives (New York: New York University Press, 2005), 18.
48. See Isaac West, “PISSAR’s Critically Queer and Disabled Politics,” Communication and Critical/Cultural Studies 7, no. 2 (2010), 156–75; also Sheila Cavanagh, “Touching Gender: Abjection and the Hygienic Imagination,” in Stryker and Aizura, Transgender Studies Reader 2, 426–42.
49. Peeing in Peace: A Resource Guide for Transgender Activists and Allies (San Francisco: Transgender Law Center, 2005), translaw.wpengine.com/wp-content/uploads/2012/05/94930982-PIP-Resource-Guide.pdf.
50. “Remembering Our Dead,” www.rememberingour-dead.org (site inactive; accessed 13 June 2013). See also Juliet Jacques, “Remembering Our Dead: Global Violence against Trans People,” openDemocracy (digital commons), 26 November 2013, www.opendemocracy.net/5050/juliet-jacques/remembering-our-dead-global-violence-against-trans-people. On the distinctions between MTF and FTM and trans women of color, see Michelle O’Brien, “Tracing This Body: Transsexuality, Pharmaceuticals, and Capitalism,” in Stryker and Aizura, Transgender Studies Reader 2, 56–65.
51. For a transnational analysis of racial difference that informs the possibility of transformative experiences of surgical procedures, see Aren Z. Aizura, “The Romance of the Amazing Scalpel,” in Stryker and Aizura, Transgender Studies Reader 2, 496–511.
52. Paisley Currah, “Stepping Back, Looking Outward: Situating Transgender Activism and Transgender Studies—Kris Hayashi, Matt Richardson, and Susan Stryker Frame the Movement,” Sexuality Research and Social Policy 5, no. 1 (2008): 100.
53. Susan Stryker and Nikki Sullivan, “King’s Member, Queen’s Body,” in Somatechnics: Queering the Technologisation of Bodies (Farnham, UK: Ashgate, 2009), 51.
54. Ibid., 61.
55. See Metzl and Kirkland, Against Health.
56. Stryker and Sullivan, “King’s Member, Queen’s Body,” 61.
57. Gilles Deleuze and Félix Guattari, A Thousand Plateaus: Capitalism and Schizophrenia, trans. Brian Massumi (Minneapolis: University of Minnesota Press, 1987), 147.
58. James Overboe, “Affirming an Impersonal Life: A Different Register for Dis- ability Studies,” Journal of Literary and Cultural Disability Studies 3, no. 3 (2009): 254. 59. Paisley Currah, Lisa Jean Moore, and Susan Stryker, “Introduction: Trans-, Trans, or Transgender?,” WSQ: Women’s Studies Quarterly 36, nos. 3–4 (2008): 11.
60. See Jami Weinstein, “Transgenres and the Plane of Gender Imperceptibility,” in Undutiful Daughters: New Directions in Feminist Thought and Practice, ed. Henriette Gunkel, Chrysanthi Nigianni, and Fanny Söderbäck (New York: Palgrave Macmillan, 2012), 155–68. Particularly, Weinstein provides an important reread- ing of Nietzsche and a corrective around Judith Butler’s use of “no doer behind the deed,” asserting that the doer and the deed are both ctions according to Nietzsche, and implores us in nonessentialist terms to “become what we are” (162–63).
61. Mel Chen, Animacies: Biopolitics, Racial Mattering, and Queer Affect (Dur- ham, NC: Duke University Press, 2012).
62. See also Lucas Cassidy Crawford, “Transgender without Organs? Mobiliz- ing a Geo-affective Theory of Gender Modi cation,” Women’s Studies Quarterly 36, no. 3/4 (2008): 127–43.
63. Kier, “Interdependent Ecological Transsex,” 189.
64. Weinstein, “Transgenres and the Plane of Gender Imperceptibility,” 156. 65. Julie Livingston and Jasbir Puar, “Introduction: Interspecies,” Social Text
106 (2011): 3–14. In the paragraphs that follow, I paraphrase several points from our cowritten introduction.
66. Michel Foucault, Security, Territory, Population: Lectures at the Collège de France, 1977–1978, trans. Graham Burchell (New York: Picador, 2009), 75.
67. Michel Foucault, The History of Sexuality, vol. 1, An Introduction, trans. Robert Hurley (New York: Vintage, 1990), 146.
68. See Joan Roughgarden, Evolution’s Rainbow: Diversity, Gender, and Sexuality in Nature and People (Berkeley: University of California Press, 2004).
69. See Eva Hayward and Malin Ah King, “Toxic Sexes: Perverting Pollution and Queering Hormone Disruption,” O-Zone: A Journal of Object Oriented Studies 1 (2013), 1–12. Hayward and King theorize toxicity as a threat and a possibility.
70. Myra Hird, “Animal Trans,” in Giffney and Hird, Queering the Non/ Human, 242.
71. Vicki Kirby, Quantum Anthropologies: Life at Large (Durham, NC: Duke University Press, 2011).
72. Lynn Margulis and Dorion Sagan, quoted in Hird, “Animal Trans,” 241.
73. Much of this dialogue seems fixated on Temple Grandin, an autistic person known for her work on livestock animal behavior. See Cary Wolfe, “Learning from Temple Grandin, or, Animal Studies, Disability Studies, and Who Comes after the Subject,” New Formations 64 (2008): 110–23; Kari Weil, Thinking Animals: Why Animal Studies Now (New York: Columbia University Press, 2012).
74. See Max Hantel’s review of Queering the Non/Human: Max Hantel, “Post- humanism, Landscapes of Memory, and the Materiality of AIDS in South Africa,” Women’s Studies Quarterly 40, no. 1 (2012): 251–56. While an excellent initial collection on the generative connections between trans studies, animal studies, and post-humanist studies, the book, edited by Noreen Giffney and Myra Hird, participates in this elision.
75. Chen, Animacies, 137.
76. Dean Spade, “Mutilating Gender,” in Transgender Studies Reader, ed. Susan Stryker and Stephen Whittle (New York: Routledge, 2006), 315–32.
77. Bobby Jean Noble, “Our Bodies Are Not Ourselves: Tranny Guys and the Racialized Class Politics of Incoherence,” in Stryker and Aizura, Transgender Studies Reader 2, 249.
78. Michel Foucault, “Society Must Be Defended”: Lectures at the Collège de France, 1975–1976, trans. David Macey (New York: Picador, 2003), 255.
79. Many other critical race theorists have made this point, including Kim Tallbear, Nadia Abu el-Haj, and Dorothy Roberts. Kim Tallbear, Native American DNA: Tribal Belonging and the False Promise of Genetic Science (Minneapolis: University of Minnesota Press, 2013); Nadia Abu el-Haj, The Genealogical Science: Genetics, the Origins of the Jews, and the Politics of Epistemology (Chicago: University of Chicago Press, 2012); Dorothy Roberts, Fatal Invention: How Science, Politics, and Big Business Re-create Race in the Twenty-First Century (New York: New Press, 2011). Denise da Silva has written on the passage from the biopolitics of race to nanopolitics: “That cancer cells do not indicate dark brown skin or at noses can be conceived of as emancipatory only if one forgets, or minimizes, the political context within which lab materials will be collected and the bene ts of biotechnological research will be distributed” (Denise Ferreira da Silva, Toward a Global Idea of Race [Minneapolis: University of Minnesota Press, 2007], 8–9).
80. On UK legislation that requires the acquiring of one’s transgender to be committed to “until death,” see Emily Grabham, “Governing Permanence: Trans Subjects, Time, and the Gender Recognition Act,” Social and Legal Studies 19, no. 1 (2010): 107–26.
81. If we follow the lines of thought that inform Deleuze and Guattari’s “becoming,” we see that becoming animal and becoming woman (two major examples that they mobilize) are aspirational trajectories not toward these intersectional coordinates but beyond them. A becoming manifests as an occupation not of these categories but of the dissolution of the binary frames that inform the coherence of the categories in the first instance. Becoming animal is not a reaching out of the human to the experiences of the animal but, rather, a dissolution of the human animal/nonanimal binary such that it no longer makes sense, no longer signifies as sensemaking, sensible. Becoming woman, for example, is Deleuze and Guattari’s version of actual transsexualism. It is the potentiality of overwhelming—not deconstructing or transcending but, rather, overwhelming through in nite multiplicity—sexual difference into incoherence. Edward Mussawir writes that “‘Becoming woman’, a figure indeed suggestive of transsexualism, links ‘minor’ politics with an ontology of movement” (Edward Mussawir, Jurisdiction in Deleuze: The Expression and Representation of Law [New York: Routledge, 2011], 53).
82. Spade, “Resisting Medicine.”
83. Beatriz Preciado, “The Pharmaco-pornographic Regime: Sex, Gender, and Subjectivity in the Age of Punk Capitalism,” in Stryker and Aizura, Transgender Studies Reader 2, 271.
84. Ibid.
85. Ibid.
86. Amit Rai, “Race Racing: Four Theses on Race and Intensity,” WSQ: Women’s Studies Quarterly 40, nos. 1–2 (2012): 67.
87. Arun Saldahna, “Reontologizing Race: The Machinic Geography of Phenotype,” Environment and Planning: Society and Space 24, no. 1 (2006): 12.
88. Ibid., 20–21.
89. Rai, “Race Racing,” 74.
90. Rosenberg, “The Molecularization of Sexuality.”
3 notes
·
View notes
Text
Weight control key in arthritis prevention, management – Expert
New Post has been published on https://depression-md.com/weight-control-key-in-arthritis-prevention-management-expert/
Weight control key in arthritis prevention, management – Expert

An Abuja-based general practitioner, Dr Dennis Otu, speaks to GODFREY GEORGE about the causes and remedies of arthritis
What is arthritis and how does it present itself in its host?
Arthritis is a disease which leads to pain and swelling of one or more joints. Some may be because of wear and tear, like the osteoarthritis, but gasteothritis leads to inflammation, so limiting the definition to only inflammation of the joint does not do justice. Traditionally the suffix “-itis” refer to inflammation. However, inflammation in this case is a sign rather than a specific disease. It can present in many ways; such as joint pain, joint swelling, restricted movement of those joints, deformity of the joints, front-line or particular tenderness, sometimes as muscle weakness and wasting, pathologic fracture. How it presents depends on the type of arthritis. However, the symptoms listed above cuts across most of them.
What are the causes of this condition?
The causes depend on the type. Some are caused by wear and tear due to age. When you have an accident, for instance, it can lead to trauma. This ‘trauma’ is a medical term which means ‘wound’. In geasteoarthris is caused by the deposition of urate crystals and other crystals in the joints. This is also what causes a condition known as ‘gout’ or ‘pseudo gout’. Psoriasis is another cause of arthritis. There are also autoimmune responses. This is when the immune system produces antibodies against one’s own body. In some cases, it causes major complications. Normally, the immune system produces antibodies which fight against diseases, but when these anti-bodies begin to fight against the host, then, that can lead to arthritis. There can be foreign body reactions and idiopathic causes.
Are there any risk factors? What are they?
The risk factors are not unconnected to the types. There are several risk factors which are usually related to the type. The ones we’d address are the ones which affect Nigerians. The risk factors for osteoarthritis include ageing, hereditary factors, gender/hormonal factors, obesity, high bone mineral density. We have some mechanical factors such as trauma (wound), the shape of one’s joint, joint alignment and usage. Someone who does contact sports such as wrestling, boxing, karate, judo, etc, are more susceptible to developing arthritis. This is because the way they exact energy on their joints and the kind of trauma (physical injury from a mechanical force) they are susceptible to makes them more at risk. We also have some musculo-skeletal disorders caused by deformities in the joint area. Others include some recreational factors. Also, previous joint injury can also be a risk factor. Someone who had had injury on the joint area before may develop the condition much later in future.
What differentiates the condition from normal swelling or tenderness of the body, maybe from stress-related activities or sprain?
The major difference between them is that, for sprains, they are just muscle injuries which do not affect the joint. In arthritis, there is progressive damage to the joint. That is the damage affects the surfaces of the joints that are making contact. This progressive joint damage can lead to a loss of articular cartilage, subchondral osteosclerosis, osteophyte formation, remodeling of joint contour, etc.
The two common types of arthritis are rheumatoid and osteoarthritis. What differentiate both of them?
Rheumatoid arthritis is caused by auto-immune reactions, where the body’s immune system fights against the body instead of against diseases. That is, one’s immune system attacks one instead of attacking a foreign body, it can lead to rheumatoid arthritis, whereas osteoarthritis is due to wear and tear.
Are they the only types there are?
We have gout, pseudogout, septic arthritis, reactive arthritis, viral arthritis, psoriatic arthritis, juvenile idiopathic arthritis, ankylosing spondylitis, neuropathic arthritis, polymyalgia rheumatica, etc. We also have viral arthritis, which are caused by viruses. This is why people living with HIV/AIDS can have arthritis because of the human immuno virus. Juvenile idiopathic arthritis occurs in children but the causes are unknown.
Is it a condition of the aged?
It is not a condition of the aged. It can happen to anybody. For the juvenile idiopathic arthritis, we can see that it can happen to children. Psoriasis and septic arthritis can also happen to both young and old people. But, when it comes to osteoarthritis, it mostly happens to the old people.
Is there reasonable research in this area of medicine?
There is ongoing research in the area of pathology. These are developmental researches also in the area. So, of course, there is reasonable research in the area. Efforts are still being made to develop new and innovative treatments every day, so we can say it is still a work-in-progress.
The main goals of arthritis treatments are to reduce symptoms and improve quality of life. Does this mean one cannot be totally free from the condition?
It depends on the type and extent of damage to the joint. How the patient was treated can also be a factor. So, if a person develops septic arthritis, and it was diagnosed early and the person undergoes adequate treatments, that person can go back to living a normal life. However, I need to point out that someone who had had arthritis and was treated still stands a chance of developing the condition in future. It is not an impossibility. The person may develop another type of arthritis even after being treated for one. So, it can be safe to say previous history of arthritis is a risk factor for future occurrence of other types of arthritis.
What is the diagnosis like for patients when they present themselves at the hospital?
Like every other medical diagnosis, a case of arthritis is diagnosed by taking a good medical history, examining the patient, and requesting appropriate laboratory and radiologic investigations. When a patient presents him/herself in the hospital and says he/she has pain, the doctor has to look at other factors like age, gender and the kind of job the person does. Is (s)he into contact sport? Is there a history of walking unaided? You take the range of motion and take some modules. You do other baseline investigations and send for an x-ray. You would then know if it is arthritis or something else.
Women are more likely than men to develop rheumatoid arthritis. How true is this assertion and what do you think women should do?
It is very true. Infact, from the statistics in the United States, among the Caucasians, the female to Male ratio is 3:1. This means, for every man who has arthritis, there are three women with the condition. Women’s joints are more lax than men’s—the bones move around more and are less stable within the joint. When joints have less stability, they are more prone to injury, and injuries can lead to arthritis.
Are there any preventive measures you’d recommend?
I would recommend weight control. Since being overweight is a risk factor, one has got to watch what one eats. It is a no brainer. There is this saying, “You are what you eat!” If you are overweight, this means you would be exerting a lot of pressure on your legs and this can lead to serious problems for you, as your legs may not be able to carry your body. People should embrace healthy food choices and lifestyle; cease smoking, moderate intake of alcohol – or none at all – aerobic exercise, stretches, use of protective gear when engaging in contact sports, control of blood sugar, (since diabetes can also be a risk factor considering the fact that it is a multi-faceted disease) routine screening and baseline investigations, avoiding a sedentary lifestyle.
Arthritis is more than just wear and tear or an old person’s disease and it is the leading cause of disability in America. Is this true for us in Africa?
There’s more to arthritis than just wear and tear and it’s a major cause of disability, not just in America, but in Africa.
What is the worst that can happen?
The worst intra-articular complications of arthritis are joint destruction, deformity and disability; pathologic fractures. There are also extra-particular complications which depend on the type of arthritis, and in some cases is life threatening.
What is the treatment plan and what is expected of these patients after that?
The first treatment is what I term as ‘patient education’. The patient needs to be aware of what is wrong with him or her and what led to the condition. (S)he also needs to be aware of how the treatment would go, what the outcome would be if followed or not followed. They actually have the right to know these things, and if you explain this thing to them, you have helped solve the problem halfway. Then, we may use exercise (aerobic conditioning and strengthening), reduction of adverse mechanical factors (pacing of activities, appropriate footwear), weight reduction if obese, analgesia, use of disease modifying therapy, local corticosteroid injections, physiotherapy (physical treatment such as heart therapy, cold therapy, physical aids and appliances), surgery (hip replacement, knee replacement). Also, the patient can be encouraged to develop coping strategies.
Are there nutritional expectations?
A well balanced diet rich in vitamins, minerals, antioxidants and other nutrients play a big role in not only arthritis but other disease conditions since it is crucial for weight management.
Is it hereditary?
Some hereditary factors are known to play a role in the development of some types of arthritis
Is there anything you think the government should do to help out since this is one of the commonest diseases in Africa?
Yes, of course. The scope of medical insurance should be expanded to cover those suffering from chronic illnesses especially the elderly since they are more commonly affected.
Copyright PUNCH.
All rights reserved. This material, and other digital content on this website, may not be reproduced, published, broadcast, rewritten or redistributed in whole or in part without prior express written permission from PUNCH.
Contact: [email protected]
Source link
0 notes
Text
A Narcissist’s Damage in A Relationship: They Poison Your Mind, Your Heart, Your Soul And Your LIFE

With narcissists, it is a hideous, demeaning, debasing, ANGRY, and abusive coexistence that we get conned and TRAPPED into.
A Narcissist clearly crosses the boundaries of defying another person’s human rights and dignity, so much so it is clearly classified as psychological/emotional abuse and domestic violence. They tear down a person’s psychological well-being in such an insidious/sadistic manner that the target becomes completely vulnerable, unprotected and fearful.
A Narcissist is completely pathological in every single aspect of how they relate to the people and the world around them. Unfortunately, their world is completely delusional, one in which they do not allow individuality because they are absolute rulers (dictators) in that world. The unfortunate fact is that a Narcissist needs people in their lives to SURVIVE but they just don’t ‘like’ or ‘relate’ to people so it is a hideous, demeaning, debasing, ANGRY, and abusive coexistence that we get conned and TRAPPED into.
Victims of Narcissistic abuse often appear uncertain of themselves, constantly seeking clarification that they haven’t made a mistake or misheard something. Their confidence becomes so low that they have trouble making simple decisions, questioning and re-questioning things.
This is a direct result of the emotional and psychological abuse used by the Narcissist to erode their self-esteem as well as instill confusion and anxiety into the victim to the point where they no longer trust their own memory, perception or judgment.
This is skillfully guided by the Narcissist and it clouds reality with leading statements like “I never said that”, “You are crazy”, or “you are imagining things.” The Narcissist will even step up the game by reinforcing what they say by backing it up with statements from friends, co-workers, or relatives that supposedly agree and ARE very concerned about the target/victim (and probably just more lies).
Gradually, the target/victim will NOT trust their own perceptions and doubt themselves completely. This more than often also induces depression and anxiety – two separate issues that will have to be dealt with as well as the ‘other’ consequences of this hideous abuse.
The target/victim is totally broken and unable to trust their own perceptions in life (the ones we take for granted as just knowing what to do in life, etc.,) so they isolate themselves because life is just too confusing and they fear it.
The victim now doubts everything about themselves, their thoughts and opinions, their ideas and ideals. Ask yourself here and now if you are experiencing this, maybe it is a feeling of hopelessness, fear, confusion, or just an abnormal sense of life, one where you feel very alone and without a real objective to change or fix this or moving forward.
Targets/victims will become co-dependent on the abuser for their reality and the Narcissist loves this because that is their goal –TOTAL CONTROL of your thoughts and actions and they are at the steering wheel driving this abuse full forward. Who does this but a highly disordered human being with a dark agenda?
Who could take, steal away or destroy any portion of another person’s life for any reason yet alone the agenda of a highly disordered Narcissist that is basically driven by their own hate AND an extortionist as well that wants everything they can take from another human being.
No relationship ever ends in such a shroud of hate and destruction as one that ends with a Narcissist. They annihilate every aspect of the relationship, the person, their life, their family, their friends AND basically everything in a manner to completely disable you/us. Every action and word that comes from a Narcissist is a bizarre attack on your personal reality.
It takes you from the goodness and normality that you have had all of your life to a dark place where you now have feelings of inadequacy and worthlessness because EVERYTHING you do is wrong and you are basically worthless. Even after separation from a Narcissist, the abuse lives on because like a poison it has entered into every cell in your body and in the case of a Narcissistic abuse the poison destroys the mind and reality of their target/victim!
OK – YOU CAN BEAT THIS! You have the ability to unlearn what the Narcissist has conditioned you into believing about yourself and purge the many negative messages out of your mind.
That old saying “A horse can be led to water but they can’t be made to drink it” – well let’s change that a little bit and say “A horse can be led to water and taste it, drink it and swallow it – BUT it can stop drinking it, walk completely away from it and not only find a better watering hole BUT greener pastures and other fully functioning horses.” You have to do this so that you aren’t stuck in a fog of lies that will only guide your life in a negative and destructive direction.
What the Narcissist has internalized in you can be EXTERNALIZED and thrown away. Move away from any level of this abuse by knowing that you and only you can change and find normality and the reality of a better life.
Say no to the Narcissist, say no to the messages in your head that say you are not worthy, SAY NO TO THE ABUSE. Those negative words and debasing actions are only a curse/spell that the Narcissist casts out on the world and it can’t stick if the Narcissist doesn’t have you under his/her spell.
Once you have the education that enables you to see the very truth about this abusive Narcissist, you can remove yourself and break the spell. You have the power to govern your own will and what you will do with your life. You have to take all of that power AWAY from the Narcissist and give it back to yourself.
Yes of course no-contact – but when you have to have minimal contact use the truth to really see the abuse that harmed you that is standing in front of you and disengage in your mind from any thought, emotions, words or actions they send your way because they are like bullets from a gun and meant to harm!
This is what starts you on your road to recovery acknowledging the truth that this was situational and administered from a personality disordered person. You are not to blame, you were conned into believing this person loved you, you trusted this person, believed in them and gave them your love in return – BUT they were NEVER that person – they were a sadistic and abusive person that caused you great distress. Know this and NEVER allow yourself to accept their abuse again.
Source:
ANA – After Narcissistic Abuse
H/t – Mystical Raven
1K notes
·
View notes
Text
If the 2ps were Doctors
Warning : Here are what would the 2ps be if they pratice Medicine and what sort of it. It’s only based on what I think fit with their personalities. It was fun to find what would fit with what character.
2p!America : Specialist of Physical and Rehabilitation Medicine (Physician who covers the care of disabled people or victims of lesions after an accident or an illness, but also in case of chronic pains.)
Even if it’s not his main passion, Allan is a great sportsman and a healthy man, so naturally he found his way towards the Physical and Rehabilitation Medicine with the aim of helping is patients to forge again their muscles after various accidents. He’s a very good coach so he really can help his patients to reach the end of their physical rehabilitation.
2p!England : Pediatrician (Pediatric specialist, medicine which study the physiological and psychomotor development of a child.)
Oliver has always loved children, they give him a lot of joy and love. He’s the nice doctor of children whom they adored because he always brings candies and kind words. Oliver feels more comfortable with children who love him rather than adults who treat him badly. For him, these sick children are a real source of happiness.
2p!France : Pulmonologist (Specialist in Respiratory Medicine, which is the discipline that studies and treats diseases of the lungs and the respiratory system.)
It’s quite odd to see a chronic smoker like François as a lung doctor, since he himself does not take good care of his. Also, he does not seem very credible in front of his patients. However, who better than a smoker knows the risks of smoking and the diseases that the lungs can have. So, he knows everything a doctor needs to know about the lungs and the best way to treat them.
2p!Canada : Veterinarian (Specialist in Animals’ Medicine and Surgery)
Matt hates people and their behavior towards animals often annoy him, but the need to save animals is stronger for him. One could say that as they have always been his closest friends, he makes it one’s duty to treating them. Since he works in close collaboration with animal associations, he does not hesitate to call them if he sees that a master is mistreating hi animal and he himself does prevention towards ignorant masters.
2p!Russia : Dental Surgeon (Medical health professional qualified to practice Odontology, therefore dentistry.)
Viktor is a bit of the cliché of the dentist with a big Russian accent and the face of a nasty movie dentist who will make his patients suffer for pleasure and tear their teeth out without anesthesia. But in truth, he’s particularly talented in the ways and means of using the drill without hurting. Despite his big hands, he’s very delicate when it comes to taking care of his patients’ teeth. However, he has some satisfaction when he pulls teeth, but always under anesthesia.
2p!China : Radiotherapist (Specialist in Radiotherapy, that is to say the treatment method based on the biological action of ionizing radiation and especially X-rays.)
Xiao has always been fascinated by the big machines of medicines and imaging methods, such as X-rays, MRIs, ultrasounds and optical methods that give an insight of the inside of the human body. He’s mostly fascinated by the dangerous products and processes he has to manipulate, such as magnetic fields, radioactivity, ultrasounds and others. He loves to touch anything that is dangerous.
2p!North Italy : Neurologist (Specialist who is dedicated to study and treatment of diseases affecting the central nervous system (brain, spinal cord) or peripheral (roots and nerves).)
His own brain’s problems, especially push him to take an interest in anything that is around this part of the body in order to try to understand himself better, even if he does not realize it. What really interests him are the neurodegenerative diseases and neuromuscular pathologies which he tries to understand the functioning for fear of having to suffer from it himself.
2p!Germany : Occupational Health Physician (The role of the occupational health Physician is purely preventive and consists in avoiding any health damage to workers while carrying out their duties. He’s responsible for monitoring occupational hygiene conditions and employee health while detecting the risk of contagions.)
Lutz could not be a doctor without working in a company; be alone in his cabinet would have made him depressed. As an occupational Physician, he is in contact with people, which he prefers, and his role is mainly to see the working conditions of companies and avoid contagion, which for him, is, therefore, a quite a simple job, but likes it a lot.
2p!Japan : Gynecologist (Specialist who is dedicated to the study of the organism of the woman and her reproductive system, from both physiological and pathological point of view.)
What more can we expect from Kuro. It must be said that this job is especially a good excuse for him to see female genitals all day. But as far as he likes to see beautiful young girls and women, he really hates to examine women he does not find pretty or old women; he finds it frankly disgusted. But this is the hazards of the job, so he takes it upon himself to remember only the best of the day.
2p!South Italy : Aesthetic, plastic and reconstructive Surgeon (Surgery Specialist grouping all the interventions consisting in improving the physical appearance of an individual.)
For Flavio, there is nothing more important than the beauty of the human body, so it is quite naturally that he helps all his patients to be as beautiful as they wish. He makes a point of honor to fulfill all the desires of his patients and to make them as beautiful as possible, but especially from his point of view. If he considers that a person is about to make them ugly by a bad choice of surgery, he makes them change their minds so that it corresponds to what he calls true beauty.
2p!Prussia : Palliative Physician (Specialist in care that aims only at the comfort of the patient, often at the end-of-life phase. The goal of palliative care is to prevent and ease physical pain, uncomfortable symptoms (nausea, constipation, anxiety…) or psychological suffering.)
Gilen wanted a medicine that would be soft to fit with his sensitive nature, but he did not realize that palliative care is by far one of the most difficult branches because of the weight and the psychological impact it has on oneself. Accompanying people before the death is far from easy. But somewhere, rather than being a burden to Gilen whose relationship with death is already pretty close, it allows him to clear his mind from his own problems by focusing on those of others.
2p!Spain : Psychiatrist (Specialist in mental health, practicing psychiatry. He diagnoses, treats and tries to prevent the psychic suffering and mental illness.)
Andres is a pretty sane man. Also, mental illnesses are a mystery for him so he tries to understand them. He has also suffered a lot from mental illnesses because people around him have always suffered from them, so he considered himself obliged to find and diagnose them so that his patients and their loved ones do not have to suffer as he had suffer in the past and still suffered today.
2p!Austria : Hematologist (Specialist in hematology (study of blood, organs where blood cells are formed and their illnesses).)
Roland is a vampire in the clinical sense of the word, that is to say that he’s a human that drinks blood (so different from vampires like in the myths). That’s the reason he went to the hematology section, in order to study it for his own interest, but also to steal it if necessary. He suffers from a mental disorder that causes him to make blood his passion, both for drinking and for using it for his satanic rituals.
2p!Finland : Cardiologist (Doctor specializes in cardiology, that is to say in the part of medicine that studies the heart and treats illnesses related to it.)
Thurston became cardiologist, especially to put into practice the methods that came from his country, including saunas and cryotherapy. So, he greatly recommends these two methods for cardiovascular diseases because he’s convinced of their benefit. He applies these methods himself on his patients, either by passing them in a sauna then confronts them with the cold, or by using cryotherapy showers in which he puts his patients for two or three minutes. Thus, he wants to show all his colleagues that these methods work.
2p!Sweden : Otorhinolaryngologist (Specialist in Otorhinolaryngology therefore the medical specialty which studies the anatomy, physiology and diseases of the ear, nose and sinus cavities, pharyngo-larynx and surrounding areas (facial and cervical).)
Let’s say that of all the medical specialties, this one was the single one that attracted the most Bernard. He would not have liked to practice a more intrusive specialty. At least with this one, he only has to look slightly deeper than on the surface and he only has to make a diagnosis. He has no operation to do, just to receive people and make assumptions. He does not like to rack his brain too much.
2p!Norway : Dermatologist (Specialist of Dermatology, that is to say who studies and treats diseases of the skin, skin appendages (hair, nails) and mucous membranes.)
Loki is a badly burnt man, much as in the hands he hides under his gloves, the body under his blouse and part of his face he cannot hide. Also, he knows a lot about skin that his studied after his burns ton understand its regeneration and its diseases. For him, the skin is a very interesting subject of study and understanding his problems have become a vocation since his own has changed.
2p!Iceland : Ophthalmologist (Specialist in Ophthalmology so the science and medical specialty that deal with the structure and function of the eyes and diseases that reach them.)
That’s pretty ironic from a boy who lost an eye to do ophthalmology, but that’s the vocation he takes up after understanding the importance of the eyes in a person’s life. His own acuity has developed around one eye with which he has learned to live, so he studies the adaptability of the eyes after an accident or illness.
2p!Denmark : Preventive Physician (Branch of medicine consisting of giving hygiene advice in a broad sense: cleanliness, but also dietetics, encouragement to a sport or physical activity, ergonomics and a way of making efforts, prevention of risk and disease screening.)
This medicine allows him not to think too much, he gives only hygiene advice and makes injections in search of screening. What he is told to do, he does. This branch allows him not to have to operate his patients, which he would not support, but it just allows him to help people, although he does not feel great joy, however, to find or stop at advance of potential disease.
5 notes
·
View notes
Text
Pain Specialist In Delhi for Chronic pain
Pain Specialist In Delhi for Chronic pain
Pain, no matter how trivial, is an unwelcome guest. It can be associated with undue suffering and disability which everyone would like to avoid. It is helpful to understand the types of pain one may experience. Pain can be categorized as acute or chronic pain.
Acute pain is the pain that is present after an injury until healing occurs. Pain in this situation is a protective response bringing our attention to the affected area and helping us protect, rest the affected tissue providing an opportunity for healing. As the tissue heals, the pain gradually abates.
Chronic or persisting pain is pain that persists even after the usual time required for healing. It is important to understand that chronic pain does not always signify on-going damage. Nerves have a memory (plasticity in medical terms) whereby they develop changes which remain even after the original inciting problem is corrected. A simple example to explain this is persisting leg pain even after amputation of the affected part. There are numerous mechanisms to explain this and your doctor can help you understand these better.
Impact of chronic pain is not limited to the involved person but also affects their loved ones and family members. The longer it persists the more chances that it will have an impact on multiple aspect of your life including your ability to work, sleeping pattern, mood, social life, relationship with family and friends etc. Hence it is important to take corrective measures to reverse or control the condition as soon as possible.
The management varies depending on the actual pathology, severity, co morbidities, patient preferences, available resources/ expertise and many other factors. At your first consultation with me you can expect a detailed assessment including history, examination and review of investigations. This is aimed at identifying the underlying reason for pain, so that an appropriate personalised management plan can be made. Some more tests may be requested as necessary. Close liaison with specialists in other fields such as neurology and surgery is maintained to formulate the best plan tailored to your condition and requirements. Some of the common pain treatment modalities include:
Medical management
I normally review your current medications and any existing medical problems prior to suggesting new medications or changes to current medications. Therefore it is a good idea to carry a detailed list of your medications and make of list of the ones you may have tried previously. Doses of medications tried previously are equally important as some medications if not used in right doses for the required duration are unlikely to be effective.
Different types of pain may need treatment with different medications, for example pain of inflammatory origin maybe be effectively managed with anti-inflammatory medication and pain due to irritation of nerve may need medication which help to desensitize the nerves. Hence the importance of identifying the likely pain generators prior to prescribing medications.
Interventional procedures
In certain situations I suggest procedures such as
Injections/ radiofrequency procedures that help to reduce the pain signals being transmitted by the nerves to your brain
Injections directly into a joint space/ around the area of problem such as a tendon or bursa which can help reduce the inflammation more effectively than medications taken orally. These procedures along with being therapeutic may also help the consultant confirm diagnosis
Regenerative medicine has opened new avenues where cells from your body are used to promote healing and reduce pain. Awareness of options such as Platelet-Rich Plasma (PRP) and stem cells is increasing and new research in this area is improving our understanding day by day.
Some interventional procedures can be done in the outpatient setting, whereas others will require a day case admission. This depends on the procedure being performed and your general health, other medical problems. We aim to reduce your pain as much as possible by offering you most appropriate interventions keeping your goals and preferences in mind and with an integrated multi speciality team approach based on biopsychosocial model of pain you have best chances of managing your pain.
Role of Physiotherapy
There are few common elements in management of most chronic pain situations like weakness accompanied by disuse of affected part for long time will require gradual mobilization and strengthening. A good chronic pain physiotherapist offers more than physiotherapy. They play an important role in
Patient education regarding their condition, do’s and don’ts specific to their condition,
Setting realistic goals-dividing exercises into smaller achievable steps
Help patients understand and implement pacing of activities
Promoting compliance, increasing confidence and making you self reliant
Challenging your unhelpful thoughts, mitigating any false believes and minimising catastrophisation
Role of Psychology
Chronic pain can generate significant distress, anxiety and depression and all these, in turn, can magnify perceived pain. This is a normal human reaction which is often more visible to friends and family. Addressing these factors can help in reducing perceived pain and in improving quality of life. Psychologists can help you by challenging maladaptive beliefs, attitudes and emotions. They can help by
Teaching coping and self-help strategies
Relaxation techniques- these can be a useful tool especially in dealing with sleep disturbances and periods of increased pain
Cognitive Behavioural Therapy (CBT)
gs >> Acute pain, Best Pain Specialist In Delhi, Chronic Pain, Pain Specialist In Delhi
0 notes
Text
Medical Insurance 101 — Know the Basics

‘Nothing in life is free.’ At Day1 Health, we agree — even basics, like bread and milk, will cost you something. We also believe that certain things, though not free, are a basic human right and should not be so unaffordable that they become inaccessible. Medical Insurance should be one of these.
Statistics indicate that Medical Aid options have priced a large proportion of the South African population out of the healthcare market. At Day1 Health, we are committed to providing access to basic primary medical insurance and hospital cover that is not beyond anyone’s financial reach.
But when it comes to healthcare options, terminology can be confusing, misdefined and easily misrepresented.
Medical Aid and Medical Insurance are not interchangeable terms.
Despite the belief that ‘an apple a day may keep the doctor away’ — when it comes to Medical Aid and Medical Insurance — we are not comparing apples with apples. They are two completely different paid-for services that have ‘medical’ in common but offer very different benefits.
If you carefully investigate Medical Insurance for its unique benefits, you are likely to come away pleasantly surprised.
What does it cost? (Pricing)
At first glance, the biggest difference is that Medical Insurance is generally priced at a considerably lower rate than Medical Aid options in South Africa. This is significant, but you need to know what you are paying for and what your money will buy you.
It is true that you get what you pay for, but it is more important to pay for what you need and can afford.
As a Medical Insurance provider, Day1 Health offers primary medical cover from as little as R265/month and hospitalisation options from R385/month — regardless of age, stage of life or economic bracket. (But please be aware that there is a price increase on your monthly premium for each additional dependant.)
Addressing the needs of those who cannot afford conventional Medical Aid cover and their rights to access affordable healthcare is the primary focus for Day1 Health. This puts you in control of your medical care.
What do I get? (Benefits)
This is where you need to look closely and understand what makes Medical Insurance tick.
Note the following unique benefits:
Pays a specified lump sum for your hospital stay which will vary depending on which plan you are on.
Focuses more on major life events and is very helpful in the case of accidental injuries, paralysis, permanent disability, or illnesses that occur after you have joined.
Includes death and funeral benefit payouts. (This is a huge advantage). Some plan options also include accidental permanent disability pay-outs.
Offers primary and basic day to day benefits, including doctor’s visits, pathology, radiology, dentists, optometry, chronic medication et al.
What don’t I get? (Exclusions)
It is always advisable to read the fine print of any Medical Insurance scheme you are considering. Make sure you are advised of exclusions and waiting periods:
All pre-existing medical conditions carry a 12 month waiting period.
There is a specific list of hospital procedures that are not covered. Medical Insurance is not, by law, compelled to cover these medical procedures.
The different plans will require specific waiting periods before certain benefits kick in. Make sure you are aware of these when you sign on.
With Medical Insurance, there is often a network of doctors and dentists, and you will only be covered if you visit those who are registered with the scheme you are on.
Day1 Health
Medical Insurance provides significantly different healthcare package to a Medical Aid. It has affordable pricing and excellent benefits that make it a good fit for the majority of South Africans. You won’t be left unprepared or uncovered when medical emergencies occur or medical treatment is required!
To find out more about Day1 Health’s different plans, please visit us to learn more so you can make an informed decision that will suit your budget, your age and your specific health needs. You can’t afford not to.
#Affordable medical aid#Gap cover#Hospital cover#Medical insurance#Day1 medical aid#Cheap medical aid#Medical aid#Medical aid pensioners#Affinity health#Discovery medical aid#National Health Insurance#NHI
0 notes
Text
Treatment modalities in chronic pain
Pain, no matter how trivial, is an unwelcome guest. It can be associated with undue suffering and disability which everyone would like to avoid. It is helpful to understand the types of pain one may experience. Pain can be categorized as acute or chronic pain.
Acute pain is the pain that is present after an injury until healing occurs. Pain in this situation is a protective response bringing our attention to the affected area and helping us protect, rest the affected tissue providing an opportunity for healing. As the tissue heals, the pain gradually abates.

Chronic or persisting pain is pain that persists even after the usual time required for healing. It is important to understand that chronic pain does not always signify on-going damage. Nerves have a memory (plasticity in medical terms) whereby they develop changes which remain even after the original inciting problem is corrected. A simple example to explain this is persisting leg pain even after amputation of the affected part. There are numerous mechanisms to explain this and your doctor can help you understand these better.
Impact of chronic pain is not limited to the involved person but also affects their loved ones and family members. The longer it persists the more chances that it will have an impact on multiple aspect of your life including your ability to work, sleeping pattern, mood, social life, relationship with family and friends etc. Hence it is important to take corrective measures to reverse or control the condition as soon as possible.
The management varies depending on the actual pathology, severity, co morbidities, patient preferences, available resources/ expertise and many other factors. At your first consultation with me you can expect a detailed assessment including history, examination and review of investigations. This is aimed at identifying the underlying reason for pain, so that an appropriate personalised management plan can be made. Some more tests may be requested as necessary. Close liaison with specialists in other fields such as neurology and surgery is maintained to formulate the best plan tailored to your condition and requirements. Some of the common pain treatment modalities include:
Medical management
I normally review your current medications and any existing medical problems prior to suggesting new medications or changes to current medications. Therefore it is a good idea to carry a detailed list of your medications and make of list of the ones you may have tried previously. Doses of medications tried previously are equally important as some medications if not used in right doses for the required duration are unlikely to be effective.
Different types of pain may need treatment with different medications, for example pain of inflammatory origin maybe be effectively managed with anti-inflammatory medication and pain due to irritation of nerve may need medication which help to desensitize the nerves. Hence the importance of identifying the likely pain generators prior to prescribing medications.
Interventional procedures
In certain situations I suggest procedures such as
Injections/ radiofrequency procedures that help to reduce the pain signals being transmitted by the nerves to your brain
Injections directly into a joint space/ around the area of problem such as a tendon or bursa which can help reduce the inflammation more effectively than medications taken orally. These procedures along with being therapeutic may also help the consultant confirm diagnosis
Regenerative medicine has opened new avenues where cells from your body are used to promote healing and reduce pain. Awareness of options such as Platelet-Rich Plasma (PRP) and stem cells is increasing and new research in this area is improving our understanding day by day.
Some interventional procedures can be done in the outpatient setting, whereas others will require a day case admission. This depends on the procedure being performed and your general health, other medical problems. We aim to reduce your pain as much as possible by offering you most appropriate interventions keeping your goals and preferences in mind and with an integrated multi speciality team approach based on biopsychosocial model of pain you have best chances of managing your pain.
Role of Physiotherapy
There are few common elements in management of most chronic pain situations like weakness accompanied by disuse of affected part for long time will require gradual mobilization and strengthening. A good chronic pain physiotherapist offers more than physiotherapy. They play an important role in
Patient education regarding their condition, do’s and don’ts specific to their condition,
Setting realistic goals-dividing exercises into smaller achievable steps
Help patients understand and implement pacing of activities
Promoting compliance, increasing confidence and making you self reliant
Challenging your unhelpful thoughts, mitigating any false believes and minimising catastrophisation
Role of Psychology
Chronic pain can generate significant distress, anxiety and depression and all these, in turn, can magnify perceived pain. This is a normal human reaction which is often more visible to friends and family. Addressing these factors can help in reducing perceived pain and in improving quality of life. Psychologists can help you by challenging maladaptive beliefs, attitudes and emotions. They can help by
Teaching coping and self-help strategies
Relaxation techniques- these can be a useful tool especially in dealing with sleep disturbances and periods of increased pain
Cognitive Behavioural Therapy (CBT)
#Pain Treatment in Delhi#Body pain treatment in Delhi#Pain Management in South Delhi#Pain management centre in Delhi#Pain specialist doctor in Delhi#Best pain specialist in Delhi
0 notes
Text
Juniper publishers-Aging In Grace and the Effects of Social Isolation on the Elderly Population

Abstract
Our conception, birth and developmental processes are as a result of human cooperation which establishes a necessity of our dependence on others for success, personal progress and well-being. Without this cooperation our full growth into adulthood will be grossly hampered. This article will discuss such cooperation and confirm the reality that we are summed by the contributions made in our lives by people we have been privileged to encounter in our journey of life.
It identifies successful aging or aging in grace within a framework of factors and conditions that encourage the potential development of the 'untapped reserves' of the elderly population. It is also aims at demonstrating how social isolation is a problem in the general wellbeing of the elderly population and "social death” as a devaluation of the humanity of others and of the human person in general. Finally, it recommends social support systems as imperative in promoting general well-being among older adults.
Introduction
In the light of our collective cynicism and stereotyping of aging and the elderly—elderly people are sick, elderly people are ugly, elderly people are obsolete, the question arises: is there any hope to age in grace or successfully, and experience some kind of tranquility and happiness in the process, and what would that entail? Aging in grace, graceful aging, successful aging, optimal aging, positive aging, productive aging, active aging, adaptive aging, or aging well, are all ideas without universally accepted definitions. A focus on aging includes concepts such as health, life satisfaction and quality of life and genetic, biomedical, behavioral and social factors.
Aging in Grace and Other Nuances
The terms aging in grace, graceful, successful, positive or optimal aging are usually used interchangeably, but, according to many gerontologists these terms focus on life-style choices that promote quality aging, and therefore minimize age-related problem. The term successful aging was made popular by Rowe and Kahn [1] in order to describe quality aging well into old age. Aging in grace is one of the ways of describing the other ways of growing old happily, successfully and normally, or the average aging development as assessed on any measure and with any age definition, and pathological aging, which incorporates acute or chronic disease that hampers a normal aging pattern and accelerates decline. Many people, view aging as 'something to be denied or concealed', but aging in grace and successful aging have to do with 'aging well' which is not the same as 'not aging at all'.
Successful aging is no longer an oxymoron but a reality. Nevertheless, a standard or uniform definition for successful aging still does not exist. Part of the problem in defining the term is a lack of consensus on what aging is, when it starts, and finding general criteria for success, since social and cultural values both play a role in the definitions [2]. Successful aging can be defined as the process of promoting gains and preventing losses through a process called 'Selection, Optimization and Compensation' (SOC). An inclusive definition of successful aging necessitates a value-based, systemic, and an ecological perspective. Both subjective and objective indicators need to be considered within a given cultural context with its particular contents and ecological demands. The solution according to Rowe and Kahn [1] is thus to use various subjective and objective criteria for successful aging, focusing on individual variability within a given culture.
Successful aging is the result of the interaction between an aging individual within his or her society over the life span, and can also be described as the process of 'adaptive competence'with regard to the challenges of later life, using both internal and external resources. Since dynamics in society influence the aging process, successful aging is not solely an inherent quality of an aging person. There is a bidirectional relationship between an aging individual's adaptive competence and the developmental tasks of society. Successful agers appear to fare well on developmental tasks. There does not seem to be clear scientific agreement on a definition of developmental tasks, but Featherman et al. [3] describe them as sequences of tasks over the life course whose satisfactory performance not only is important for the person's sense of competence and esteem in the community, but also serves as preparation for the future. Developmental tasks require using one's cognitive, emotional and behavioral skills to manage one’s life circumstances. Examples of adaptive competence include gathering social support, maintaining independence as far as possible and adjusting well to retirement. Featherman et al. [3] are of the opinion that as aging progresses, ill-structured tasks out-number well-structured tasks. Well-structured tasks are sometimes defined as problems with standard solutions or techniques, and ill-structured tasks as more ambiguous problems with relative solutions. Reflective planners tend to fare better in retirement because of their accumulated expertise in solving ill-structured problems.
I. With Rowe and Kahn, we identify three key aspects in successful aging
i. preventing disease and disability as far as possible, inter alia through good lifestyle choices,
ii. continuing with mental and physical exercise throughout the life span, and
iii. Keeping up an active life-style, by being productive and by fostering strong social relationships.
This identification was based on the 10-year MacArthur study involving a multi-disciplinary team of professionals that wanted to answer three questions:
i. the meaning of successful aging,
ii. what can be done to age successfully, and
iii. What changes are necessary in American society to facilitate successful aging.
This equally helped with a paradigm shift away from conceptualizing aging as more focused on disease and disability, to a more hopeful approach. However, research confirms that few very old people (older than 90 years) age successfully. Thus, the concept aging in grace, Ihenetu [2] suggests is more 'comprehensive' than successful aging, because aging in grace focuses on 'quality of life and a sense of well-being' despite age- related decline or ill health. Successful aging for some researches is an idealized term that is not necessarily in accordance with the present reality of aging, due to the fact that restrictive factors such as ageism, affordable housing, adequate income and quality healthcare are not taken into consideration. On the other hand, the value of successful aging lies in understanding that an individual can contribute to aging well, for example through specific activities or life-style choices. Nevertheless, few elderly people fit neatly into the categories of successful, normal or pathological aging for all capabilities and suggests that one should maximize successful aging in the capabilities one can control as early in life as possible, employing preventive measures to delay age-related decline for as long as possible.
Social Death and Social Isolation Among The Elderly Population
With the advance of science and modernity, the meaning and understanding of death has been evolving. Death can be defined on a variety of different levels but most people define death as a physical event in which there is a cessation of all bodily functions including beating of the heart. Some in the medical field will broaden this to include 'clinical' or 'biological' death. The 'social death’ phrase evolved and relates to those who die in a social sense consequent to degeneration of the brain or disease, which limits interaction with those around them.
The first available presentation of social death came from Glaser and Strauss (1966), during a discussion of 'hopelessly comatose’ patients, these authors describe their receipt of 'nonperson treatment from hospital personnel when talking freely about things that would matter to the conscious patient. They said that socially he is already dead, though his body remains biologically alive. They also describe some 'senile patients' as 'socially dead as if they were hopelessly comatose’ in the eyes of the families who consign them to institutions and thereafter fail to visit. Some individuals according to Ihenetu [4] regard certain health challenges as a result illness or old age as a social death in which the person is no more connected to society and is dying a little at a time with no hope for recovery. A person's true worth does not diminish as a result of certain health challenges, it becomes an assault for a system of society to diminish and devalue the humanity of others as socially dead or insignificant based on the condition of life.
It is important to debate the idea as to whether elderly persons who are faced with the challenges of old age can be considered socially dead because how they are perceived would directly correspond to how they are cared for and valued in society. A good place to start would be to ask the question; what it is that makes an individual into a whole person? What is it that would allow one to say that an individual has a worthwhile life or life of value? The perception of social death may have some correlation to anticipatory grief that precedes the impending death of an elderly patient. What this means is that the caregiver or family member who is in the position of contributing to the social life of the individual might have given up long before exhausting every available opportunity to communicate. Labeling someone as socially dead is a serious allegation. In essence, it is the end of an individual's social existence. It might even be considered as a self-fulfilling prophecy that could speed up actual physical death. Social death occurs when a person is treated as a corpse although he or she is still clinically and biologically alive. For instance, this is much like allowing someone who was brought into a hospital in a near death state to remain on the stretcher overnight for the fear of unnecessarily having to dirty a bed. Social death does not always lead to biological death nor is it a definite concept.
A survey by Pat Robertson (2011) which referred to Alzheimer’s patients as socially dead, 100% of the responses received from surveys sent out to caregivers show otherwise. When specifically asked if those with Alzheimer's are to be considered socially dead, here below are some of the responses received from caregivers: "Absolutely not; each time my father saw me I could see a twinkle in his sad blue eyes. He did not know my name but he called me pretty’. Another said, 'Not at all - we still can enjoy church; sing and he still goes to Sunday school but does not recall anything except the Lord 's Prayer” To the same question, a Hospice Medical Director writes 'No, because they are still relational to the family to which they belong. They interact with loved ones even until death.' Another doctor who specializes in geriatrics notes, "In those with advanced dementia though the interaction/conversation may be basic or repetitive, they can still interact and thus are not socially dead.” A palliative care doctor said, "I believe they are far from socially dead. Although they may not be able to verbalize, they do communicate in other ways - why can’t people see it?”
Self-perceived social death occurs when an individual accepts the notion that he or she is as good as dead. When a patient is given a terminal diagnosis, it can be a cause to precipitate such thought. However Kastenbaum [5] is of the view that social death must be defined situationally. In particular, it is a situation in which there is absence of those behaviors which we would expect to be directed towards a living person and the presence of behaviors we would expect when dealing with a deceased or non-existent person. Thus, although an individual may be potentially responsive and desperately seeking recognition and interaction, that individual will by this definition be socially dead if others cease to acknowledge his or her continued existence. Consequently, it is paramount to get this right. Non-cognitive or elderly persons should never be looked upon as those who cease to have continued existence [4].
On the other hand, when we look at social isolation among elderly adults, we discover that there are so many researches on the effects of isolation on children and young adults, but only a few on the effect of isolation on the elderly. However, the human need for social connection does not fade away among the elderly, which is to say, the elderly have the need for social connections. Decline of social connection is considered one of the various interrelated factors which compose well-being among the elderly. Hence, it is necessary and important to deepen the knowledge about social isolation among the elderly. According to some authors, social isolation is a subject concerned with the objective characteristics of a situation and refers to the absence of relationships with other people, that is to say, they believe that persons with a very small number of meaningful ties are socially isolated, (ibid.,35).
Meanwhile, Ihenetu [4] enumerated five attributes of social isolation as: number of contacts, feeling of belonging, fulfilling relationships, engagement and quality of network members. Consequently, even loneliness, depression symptoms and their temporal connection are not attributes of social isolation, but those concepts can be causes of being socially isolated. Therefore, lack of a sense of social belonging, lack of social contacts, lack of fulfilling and quality relationships, psychological barriers, physical barriers, low financial/resource exchange and a prohibitive environment can be possible reasons leading to social isolation.
Turning to the effects of being socially isolated, it has been associated with increased vascular resistance, elevated blood pressure, impaired sleep, altered immunity, alcoholism, progression of dementia, obesity and poorer physical health. In other words, socially isolated individuals have a higher possibility of suffering from health issues. Also, drinking, falls, depressive symptoms, cognitive decline and poor outcome after stroke, nutritional risk, increased rates of re-hospitalization, loneliness and alteration in the family process were are also specific effects of social isolation. These truly existing negative effects prove that social isolation has a far-reaching impact on elderly well-being.
Its effects on the elderly well-being are phenomenona which cannot be ignored. The socially isolated elderly persons are among the risk group for myriad other negative health consequences, such as poor nutrition, cognitive decline and heavy alcohol consumption. Therefore, social isolation has a non-ignorable influence on elderly well-being [4]. It is more prevalent in older adults due to diminished vitality and health. In other words, diminished vitality and health are direct causes for being socially isolated among the elderly. Simultaneously, vitality and health are considered a vital dimension of elderly well-being. In sum, the relevance between elderly well-being and isolation is arising from interaction.
Isolation
Working Definition
'Belonging' is a multi-dimensional social construct of relatedness to persons, places, or things, and is fundamental to personality and social well-being. If belonging is connectedness, then social isolation is the distancing of an individual, psychologically or physically, or both, from his or her network of desired or needed relationships with other persons. Therefore, social isolation is a loss of place within one’s group(s). The isolation may be voluntary or involuntary. In cognitively intact persons, social isolation can be identified as such by the isolate.
Some researches portray social isolation as typically accompanied by feelings related to loss or marginality. Apartness or aloneness, often described as solitude, may also be a part of the concept of social isolation, in that it is a distancing from one's network, but this state may be accom¬panied by more positive feelings and is often vol-untarily initiated by the isolate. Some researchers debate whether apartness should be included in, or distinguished as a separate concept from, social isolation. Social isolation as we can see has several definitions and distinc¬tions, dependent upon empirical research and the stance of the observer.
When Isolation Becomes A Problem
Social isolation ranges from the voluntary isolate who seeks disengagement from social intercourse for a variety of reasons, to those whose isolation is involuntary or imposed by others. Privacy or being alone, if actively chosen, has the potential for enhancing the human psyche. On the other hand, involuntary social isolation occurs when an individual's demand for social contacts or communications exceeds the human or situa¬tional capability of others. Involuntary isola¬tion is negatively viewed because the outcomes are the dissolution of social exchanges and the support they provide for the individual or their support system(s). Some persons, such as those with cognitive deficits, may not understand their involuntary isolation, but their parent, spouse, or significant other may indeed understand that involuntary social isolation can have a negative and profound impact on the caregiver and care recipient.
When social isolation is experienced neg¬atively by an individual or his or her significant other, it becomes a problem that requires man¬agement. In fact, according to much of the liter¬ature, only physical functional disability ranks with social isolation in its impact on the patient and the patient’s social support network (family, friends, fellow workers, and so forth). Therefore, social isolation is one of the two most important aspects of chronic illness to be managed in the plan of care.
The Nature and Distinctions of Social Isolation
Social isolation is viewed from the perspective of the number, frequency, and quality of con¬tacts; the longevity or durability of these contacts; and the negativism attributed to the isolation felt by the individual involved. Social isolation has been the subject of the humanities for hundreds of years. Who has not heard of John Donne's excla-mation, 'No man is an island', or, conversely, the philosophy of existentialism— that humans are ultimately alone? Yet the concept of social isola¬tion has been systematically researched during only the last 50 years. Unlike some existential¬ists and social scientists, healthcare professionals, with their problem-oriented, clinical approach, tend to regard social isolation as negative rather than positive,(ibid.). However, isolation can occur at four layers of the social concept. The outermost social layer is community, where one feels integrated or isolated from the larger social structure. Next is the layer of organi¬zation (work, schools, churches), followed by a layer closer to the person, that is, confidantes (friends, family, significant others). Finally, the innermost• layer is that of the person, who has the personality, the intellectual ability, or the senses with which to apprehend and interpret relationships.
In the healthcare literature, the primary focus is on the clinical dyad, so the examination of social isolation tends to be confined to the levels of con¬fidante and person, and extended only to the orga¬nization and community for single clients, one at a time. For the healthcare professional, the most likely relationships are bound to expectations of individually centered reciprocity, mutuality, car¬ing, and responsibility. On the other hand, health policy literature tends to focus on the reciprocity of community and organizations to populations of individuals, and so it deals with collective social isolation. At the level of the clinical dyad, four patterns of social isolation or interaction have been identified; although these were originally formulated with older adults in mind, they can be analogized easily to younger persons by making them age-relative:
a. Persons who have been integrated into social groups throughout their lifetime.
b. The 'early isolate’ which was isolated as an adult but is relatively active in old age
c. The 'recent isolate' who was active’ in early adulthood but is not in old age.
d. The 'lifelong isolate' whose life’ is one of isolation.
Normally there are feelings that isolation brings which are often characterized by boredom and marginality or exclusion. Boredom occurs because of the lack validation of one's work or daily routines; therefore, these tasks become only busy work. Marginality is the sense of being excluded from desired networks or groups. Other feelings ascribed to social isola-tion include loneliness, anger, despair, sadness, frustration, or, in some cases, relief.
Progressions In Social Isolation
Regardless of how social isolation occurs, the result is that basic needs for authentic intimacy remain unmet. Typically this is perceived as alien¬ating or unpleasant, and the social isolation that occurs can lead to depression, loneliness, or other social and cognitive impairments that then exacerbate the isolation. Several predisposing reasons for social isolation have been proposed: status-altering physical disabilities or illnesses; frailties associated with advanced age or developmental delays; personality or neurologic disorders; and environmental constraints, which often refer to physical surroundings but are also interpreted by some to include diminished personal or material resources.
A typical course of isolation that evolves as an ill¬ness or disability becomes more apparent is the change in social network relationships. Friends or families begin to withdraw from the isolated individual or the individual from them. This process may be slow or subtle, as with individuals with arthritis, or it may be rapid, as with the person with AIDS. Unfortunately, the process of isolation may not be based on accurate or rational information. Individuals with serious chronic illnesses come to perceive themselves as different from others and outside the mainstream of ordinary life. This perception of being different may be shared by others, who may then reject them, their disability, and their differences. Part of this sense of being different can stem from the ongoing demands of the illness. For example, social relationships are interrupted because fam¬ilies and friends cannot adjust the .erratic treatment to acceptable social activities. From such real events, or from social perceptions, social isolation can occur, either as a process or as an outcome.
Individuals with chronic illness often face their own mortality more explicitly than do others. Even if death does not frighten those with chronic illness, it frequently frightens those in their social networks, which leads to guilt, and can lead to strained silences and withdrawal. For those who lack this social support, social isolation is not merely a metaphor for death but can hasten it.
Possible Causes
The list to the possible causes of social isolation is endless. Retirement, death of a spouse or significant other, health problems and even reduced income can create situations where one becomes separated from social contacts. The key, however, is how the elderly person and caregivers choose to respond to these changes because the responses can make the difference in creating a positive or negative result.
Social isolation can develop when living at home causes a lack of communication with others. This results in the elderly person feeling lonely due to the loss of contact or companionship, as well as a deficit of close and genuine communication with others. It also can be the self-perception of being alone even when one is in the company of other people. We discuss the impact of these few:
A. Stigma: Social isolation may occur as one effect of stigma. Many persons will risk anonymity rather than expose themselves to a judgmental audience. Because chronic illnesses can be stigmatizing, the concern about the possibility of revealing a discredited or discreditable self can slow or paralyze social interaction. In a study examining chronic sorrow in HIV-positive patients, stigma created social isolation. Therefore, social roles and the robustness of network support affect social isolation. The individual with chronic illness or their families grapple with how much information about the diagnosis they should share, with whom, and when. If the illness is manageable or reasonably invisible, its presence may be hidden from all but a select few, often for years. Parents of children with chronic illnesses often manage stressful encounters and uncertainty by disguising, withholding, or limiting information to other, an action that may add to limiting their social network.
For example as siblings of children with infectious disease deal with the isolation of their brother or sister, they became vulnerable to being socially isolated themselves. Social isolation not only burdens those with chronic illness, it also extends into fam¬ily dynamics and requires the healthcare profes¬sional to consider how the family manages. Nurses must explicitly plan for the isolation in families with children who are chronically ill. Thus, with social isolation being a burden for the family, it requires the healthcare professional to consider how. The family manages the illness and the isolation. Where the stigmatized disability is quite obvious, as in the visibility of burn scars or the odor of colitis, the person who is chronically ill might venture only within small circles of under¬standing individuals. Where employment is possible, it will often be work that does not require many social interactions, such as night work or jobs within protected environments (sheltered workshops, home offices). Regardless of what serves as reminders of the disability, the disability is incorporated into the isolates sense of self; that is, it becomes part of his or her social and personal identity.
B. Social Rules: Any weakening or diminishment of relationships or social roles might produce social isolation for individuals or their significant others. Those who lose family, friends, and associated position and power are inclined to feelings of rejection, worthlessness, and loss of self-esteem. These feelings become magnified by the person's culture if that culture values community. An example of social isolation of both caregiver and care recipient occurred in a situation of a woman whose husband had Alzheimer’s disease. The cou¬ple had been confined for more than 2 year? In an apartment in a large city, from which her confused husband frequently wandered. Her comment, "I'm not like a wife and not like a single person either," reflected their dwindling social network and her loss of wifely privileges but not obligations. This ambiguity is common to many whose spouses are incapacitated. Moreover, after a spouse dies, the widow or widower often grieves as much for the loss of the role of a married person as for the loss of the spouse.
The loss of social roles can occur as a result of illness or disability, social changes throughout the life span (e.g., in school groups, with career moves, or in un accepting communities), marital dissolution (through death or divorce), or secondary to ostracism incurred by membership in a• "Wrong" group. The loss of social roles and the resultant isolation of the individual have been useful analytic devices in the examination of issues of the aged, the widowed, the physically impaired, or in psychopathology.
C. Age: Old age with its possible many losses of physical and psychological health, social roles, mobility, eco¬nomic status and physical living arrangements, can contribute to decreasing social networks and increasing isolation. This will become even more of an issue as the numbers of older adults are expected to increase arithmetically and proportionately in the next two decades. The prevalence of social isolation in older adults has been approximated now to be at 2-20% and even as high as 35% in assisted-living arrangements [4].
Social isolation has been linked with con¬fusion, particularly in older adults with chronic illness. But when the socially isolated are also immobilized, the combination of isolation and immobilization can lead to greater impairments, such as perceptual and behavioral changes (e.g., confusion, noncompliance, or time distortions). Physical barriers (such as physical plant designs) or architectural features (such as heavy doors) also contribute to social isolation or home-boundedness. All of these limits contribute to social isolation in ways that motivation alone cannot eas¬ily overcome.
Social isolation has been shown to be a serious health risk for older adults, with studies indicating a relationship between allcause mortality, coronary disease, and cognitive impairments. In a converse finding, older adults with extensive social networks were protected against dementia. And, as described earlier, although low social engagement may not be a form of social isolation per se, it is a psychological isolator and thus a risk factor in social isolation. For example, depressive symptoms in older adults were shown to be decreased by social inte-gration. Isolated older adults were shown to have increased risk for coronary heart disease, and death related to congestive heart failure was predicted by social isolation. Similarly, post-stroke outcomes, for exam¬ple, strokes, myocardial infarction, or death, were predicted by pre-stroke isolation.
The extent and nature of a, social network from local to community, and integrated to contained, as well as the positive; or negative nature of the social relationships in the social network, impact health as well as social isolation. In fact, the quality of the social relationship may have more impact than the number of ties, which suggests that a few solid relationships may be more beneficial than many ties of poor quality.
Social Isolation and Well-being
Generally discussions on well-being both the best methods for achieving it and whether or not it is an appropriate goal of human activity, have been frequent throughout history. It is known that health status and personality are the most important predictors of well-being. In consideration of the relationship between health status and age, studies show that overall dysfunction comes along with the aging process. However, it can also be influenced by the quality of life especially of social isolation and loneliness. In order to understand better wellbeing in the elderly, We shall analyze the meaning of well-being, the relationship between well-being and elderly and well-being with other predictors in order to find out if they are mutually contradictory [4].
In the contemporary policy and practice, Well-being has become a high profile issue. Rather than talking just about 'improving health' we are more likely to read about 'improving health and wellbeing', and similarly, the notion of 'welfare' is now accompanied by 'well-being': as well as 'doing well', the aim should be to 'be well.' Well-being has been associated with 'happiness', with 'quality of life’ or 'life satisfaction'. And sometimes it is talked about as 'subjective well-being’ or 'mental well-being.' So the idea of well-being involves how we feel about ourselves and our lives, rather than how our lives might be assessed by others [4].
In relation to elderly people and others who use social care services, the importance of 'activity' or 'healthy lifestyles' are highlighted as factors that contribute to quality of life, wellbeing and remaining independent. This is also based on the idea of 'choice'- which we can benefit from choosing how we live our lives and what services or supports will help us do so.
Psychologically, well-being is considered as a vital dimension of the elderly person’s quality of life. Psychological well-being is generated by two dimensions which are absence of depression and emotional loneliness; and presence of happiness, life satisfaction, feeling of security, and plans for the future. An individual will be high in psychological well-being to the degree in which positives affect or predominate over negatives. On the other hand, when negative effects are in a dominant position, the individual will be low in well-being. That is to say, to gain subjective well-being, pleasure usually predominates over pain in one's life experiences.
It not surprising therefore, that some elderly people have talked about the significance of all kinds of relationships to their well-being. These included relationships with families, friends, neighbors, service providers, and also for some at least, the nature of casual encounters with strangers at bus stops, at the checkout counter of supermarkets and elsewhere. People feel a sense of security knowing a neighbour is looking out for them, and the opportunity to have a chat and cup of tea can help if someone feels isolated. The opportunity to strike up conversations in public spaces can also help people who have limited social contact to feel connected, particularly if families are rarely seen and friends have died. Losing friends can also mean losing the chance to share memories and some people suggested that, not only is it hard to make new friends in old age, 'new friends’ do not carry the history that 'old friends’ do. So that when people join in activities in the hope that they may develop new connections, this may not always positively contribute to a sense of well-being.
Friendships are important at any age. The older people we interviewed talked about how friends contributed to well-being through offers of practical help, sustaining connections with their past, and also by enabling them to give back and contribute to the well-being of others. Family relationships can be a source of support, security, joy and pleasure. They can also enable older people to contribute to others' well-being; not only caring for partners, grandchildren or other relatives, but offering their knowledge and experience (e.g. of places they have visited, journeys they have made) for the benefit of younger people starting out on exploring the world. Two way learning and support (e.g. grandchildren helping them use the internet) helps older people feel they are involved in reciprocal relationships, helps them feel valued, stay in touch with the world and maintain their sense of identity.
Social support in isolation
Social support was initially defined by taking cognizance of the number of friends an individual has; but this definition has been extended to include the person's satisfaction with the support that is rendered. Social support could include esteem support, whereby a person's self-esteem is boosted by other people, informational support that includes information provided by other people, and social companionship, which consists of support rendered by means of activities. Finally, instrument support involves a form of physical assistance. Social support has also been defined by some authors as any input that can further the goals of the receiver. Social support can be tangible, including provision of physical resources that can be beneficial to the individual in some way, or psychological, that assists the individual in developing emotional well-being Social support can also be explained as the specific people or community resources to which an individual turns for emotional and instrumental assistance. While social support could be defined as the active participation of significant others in the caregiver's efforts to manage stress, caregivers can easily become isolated from social support as a result of their confinement and responsibilities, which places them increasingly at risk for stress-related illnesses. Both the caregiver's as well as the patient's quality of life can be adversely affected, as social support is important for coping and satisfies the need for attachment, a feeling of self-worth, stress relief, and so on. However, social support is generally defined as any action that is to the advantage of the receiver of such support.
Categories of Social Support
There are six criteria of social support that researchers have used to measure the level of overall social support available for the specific person or situation [2]. First, they would look at the amount of attachment provided from a lover or spouse. Second, measuring the level of social integration that the individuals involved with, it usually comes from a group of people or friends. Third, the assurance of worth from others such as positive reinforcement that could inspires and boosts the self-esteem. The fourth criterion is the reliable alliance support that provided from others, which means that the individual knows they can depend on receiving support from family members whenever it was needed. Fifth, the guidance of assurances of support given to the individual from a higher figure of person such as a teacher or parent, the last criterion is the opportunity for nurturance. It means the person would get some social enhancement by having children of their own and providing a nurturing experience.
Two other major categories of social support have also been identified [4], tangible support, which may include physical resources that could be beneficial to the receiver; and psychological support, which assists the receiver in developing beneficial affective or emotional states. Psychological support helps a person to feel more content (or to feel better). It is clear that social support from family and friends have an important role to play in assisting a person to translate intentions into health behaviours, while the absence of social support can have a detrimental effect on the individual’s overall health. Social support can also consist of support from individuals such as friends, family members, neighbors, co-workers, professionals and acquaintances. All types of support have been found to be beneficial in helping individuals to cope during a serious illness. There is enough evidence to suggest that in general people who receive support enjoy better health than those who do not receive such support.
Therapeutic effects of social support
Social support is one of most important factors in predicting the physical health and general well-being of everyone, ranging from children through older adults. The absence of social support shows some disadvantages among the impacted individuals. In most cases, it can predict the deterioration of physical and mental health among the victims. A regular social support is a determining factor in successfully overcoming life stress. It significantly predicts the individual's ability to cope with stress. Knowing that they are valued by others is an important psychological factor in helping them to forget the negative aspects of their lives, and thinking more positively about their environment. It not only helps improve elderly person’s wellbeing, it affects the immune system as well. Thus, it becomes a major factor in preventing negative symptoms such as depression and anxiety from developing. Social support and physical health are two very important factors that help the overall well-being of an elderly person. A general theory that has been drawn from many researches over the past few decades postulate that social support essentially predicts the outcome of physical and mental health for everyone.
Studies have equally shown that social support can effectively reduce psychological distress during stressful circumstances. In addition to providing psychosocial benefits, it appears to reduce the likelihood of illness and to speed up recovery from illness. It is clear therefore that social support helps individuals to obtain a more positive outlook on life, increases self-esteem and resistance to illnesses, and encourages people to engage in more positive, health-promoting behaviours. The form of it received can play an important role. For example, if someone needs emotional support and receives only tangible support, it can further add to the person's frustration and stress. Studies have shown that immuno-suppression may be reduced by social support, which confirms the notion that social support promotes health in general [6]. It also indicates that people with a high quantity and sometimes a high quality of social relationships have lower mortality rates. Social support appears to help people to effectively resist illnesses and minimize complications from serious medical conditions.
Its regular provision essentially predicts the outcome of elderly adults' general health condition. Inadequate social support at any time would predict that elderly adults will develop depressive symptoms over time. Elderly adults would be able to ignore the negative effects in their lives with help and reinforcement from others. This is considered a psychological effect. A lack in the availability of social support would likely make the individuals notice their daily hassles and life stressors much more clearly. This step could accelerate the deteriorating effect of their physical and mental health [7].
Conclusion
There is evidence that social experience is very essential in predicting successful aging and well-being for everyone, ranging from childhood through older adults [8]. After a few decades of studies, researchers have finally gained some understanding about the relationship between social support, successful aging and well-being. Nonetheless, some areas of research still face some problems because they sometimes focus on one population, ignoring the generalization rules for using the random samples to generalize the result to a whole population [4].
The continuity of research on the effects of social isolation and the relationship between social support and general wellbeing of elderly population will enable us to understand better the effects of good social support toward physical and mental health, along with a general well-being. Many studies have shown that if a high level of social support becomes available to the elderly population, it will benefit their overall health in a long run. The importance of social support implies to everyone in our society, ranging from young childhood through older adulthood. The providers of social support can be anyone in society who brings positive environment and reinforcement to the individuals, especially from their family members. This article is optimistic that we can have a dramatic impact on the success or failure in aging, and that there is the possibility of continued growth and development in the later years. Not only physical well-being will be improved, but also emotional and spiritual well-being, when retirement and 'aging in place' become the best stage of all instead of an indirect isolation.
To read more articles in Journal of Gerontology & Geriatric Medicine
Please Click on: https://juniperpublishers.com/oajggm/index.php
For more Open Access Journals in Juniper Publishers
Click on: https://juniperpublishers.com/journals.php
#Open Access Journal of Gerontology#Journal of Gerontology Gerontology & Geriatric Medicine#Journal of Gerontology#journal of gerontology impact factor
0 notes
Text
CBD For Fighting Cancer

Cancer and uncontrolled cell development related diseases were responsible for 600,000 deaths just in the USA in 2017. Cancer, by definition, is any cell found in the human body that has uncontrolled growth and actively invades the host with its spread. With that uncontrolled cell development comes inflammation and compression of nearby tissue and organs causing unrelenting and disabling pain. Traditional treatments for Cancer are chemotherapy and radiation therapy; both of which also can cause irritation and breakdown of solid and healthy tissue alongside the tumorous disease cells. Recent research suggests that Cannabinoids (CBD) may prevent cancer cell growth and reducing the ability of tumor cells to reproduce.
What
is CBD?
The cannabis plant contains more than 100 different
chemical compounds known as cannabinoids, which interact with the body's
endocannabinoid system. Cannabidiol or CBD is the most famous among them for
having hundreds of medical benefits.
So, Cannabidiol—CBD—is a cannabis compound that has
remarkable medical and recreational benefits, but does not make people feel
“High”. It can actually prevent the psychoactivity of THC. Cannabidiol is one
of at least 113 active cannabinoids identified in cannabis. It is a major
phytocannabinoid, accounting for up to 40% of the plants extract. The fact is
that CBD-infused cannabis strains are non-psychoactive or less psychoactive
than THC-dominant strains. It’s made CBD products a good option for patients
looking for relief from inflammation, pain, anxiety, psychosis, seizures,
spasms, and other conditions without disconcerting feelings of lethargy or
dysphoria.
What you will find in this article is reference to
numerous scientific studies that all are visible on governmental sites.
What
Is Cancer
Cancer is not one disease, but the name given to a
collection of related diseases characterized by an abnormal growth of cells.
There are more than 100 different types of cancer that are caused by both
external factors (such as smoking, viruses, or carcinogens) and genetic factors
(such as genetic mutation inherited from one’s parents). Trillions of cells
compose the human body, meaning cancer could start anywhere.
Like humans, cells grow old or become damaged and eventually
die. Other cells grow and divide to form new ones to replace these old and
damaged cells, but when cancer develops, abnormal cells including the old and
damaged ones survive even though they should die. Some of the body’s cells will
start to divide interminably and spread into surrounding tissues, creating new
cancerous cells that aren’t needed. And since these new cells won’t stop
growing and dividing, they are likely to hide in the immune system and form
abnormal growths like masses of tissue known as tumors.
Cancerous tumors can spread into and invade nearby
tissues because they’re malignant. Although they can be removed, these tumors
are likely to grow back. As tumors grow, cancer cells can break off and travel
through the blood or the lymph system to any other part of the body to form new
tumors. Often far away from the original
source. This process is known as metastasis.
Benign tumors, on the other hand, don’t spread to or
invade nearby tissue and won’t grow back after being removed. Unfortunately,
benign tumors in the brain can be life-threatening.
Cancer (and its treatments) leaves its host feeling
weak and dizzy. Symptoms may differ depending on where in the body the cancer
is located, but may include:
Blood in urine or stoolsBruisingChanges in genitaliaCoughs lasting more than a month or
accompanied by bloodDepressionDifficulty breathingDifficult bowel movementsDiscomfort after eatingFeverFatigueHeartburnLumps or swellingPersistent indigestionNight sweatsSpots and growths on the skin or changes
in size, shape, and color of an already-existing mole like yellowing,
darkening, or rednessSores that won’t healWeight lossWeight gainUnexplained bleedingUnexplained joint pain
CBD
and Breast Cancer
A standout amongst the most exciting areas of
current cannabinoid research field is the investigation of the potential use of
CBD as antitumor medications. CBD is the main nontoxic exogenous operator that
may essentially reduce Id-1 expression in metastatic breast cancer cells
prompting the down-control of tumor aggressiveness . The CBD
concentrations is powerful at restraining Id-1 expression corresponded with
those used to inhabit the proliferative and obtrusive phenotype of breast
cancer cells. Of the five cannabinoids tried: cannabidiol, cannabigerol,
cannnabichromene; cannabidiol-acid and THC-acid, it was discovered that
cannabidiol (CBD) may be the most powerful inhibitor of cancer cell development
.
CBD
and Lung Cancer
Studies demonstrate that Δ9-tetrahydrocannabinol
found in CBD has been known to decrease tumor development, number of tumors,
and the amount of lung cavity. CBD prompts ICAM-1, and thereby causing
TIMP-1 induction and subsequently may decrease cancer cell development in lungs
.
Non-small cell lung cancer (NSCLC) is the main cause
(approx. 50%) of death in lung cancer in the world. Researchers have also
proven that the treatment of NSCLC cell lines (A549 and SW-1573) with
CB1/CB2-and CB2-particular agonists Win55, 212-2 and JWH-015, respectively,
altogether may weaken the intensity of random malignancy growth in vitro
chemotaxis and chemo-invasion in these cells . Scientists also observed
critical reduction in focal adhesion complex, which plays a major role in
cancer migration. CBD may suppress tumor development and lung metastasis (to
almost ∼50%) .
CBD
and Pancreatic Cancer
Recent studies on pancreatic Cancer showed that CBD
increases the apoptosis rate of pancreatic tumor cells by means of a CB2
receptor and de novo synthesized ceramide-dependent up-regulation process of p8
and the endoplasmic reticulum stress– related genes ATF-4 and TRB3. These
discoveries added the reason for rethinking CBD as a promising option for
treating pancreatic Cancer by the National Cancer Institute .
CBD
and Prostate Cancer:
Prostate cancer cells basically expand by the high
abnormal expression of both CB1 and CB2 receptors, and CBD may result in
decreasing cancer cell sustainability, expanded apoptosis rate, and lessened
abnormal expression in these receptors expression and also may decrease
prostate-specific antigen excretion.
CBD
and Leukemia and Lymphoma
Various studies on human leukemia and lymphoma cells
show that after stimulated by CBD, CB1 and CB2 receptors serve our the immune
system quite well and work as a potential target finder for apoptosis to begin
in malignancy affected cell line. Our CB2 receptors work pretty well after
treated by cannabinoids like THC and CBD as an active anti-cancer agent but it
works best without psychotropic effects. So in this case CBD may be ideal
particularly to target and kill leukemia cells. CBD may also increase the rate
of healthy blood cell production in our bone marrow system.
CBD-treated malignancies and tumors displayed an
increased number of apoptotic cells with a decreased expression of
proangiogenic factors like VEGF a potential tumor growth factor for lymphoma.
These outcomes indicate CBD as a helpful approach for the treatment of skin
tumors .
CBD
in Cancer Treatment – Summary
Many scientific research and studies in Cancer
already proved that CBD may be highly effective in treating other rare types of
cancer like Cervical Cancer , Hepatocellular carcinoma , skin and
throat cancer. So the effectiveness of CBD as a powerful anti-cancer agent can
be summarized below.
# Activating a powerful cancer cell damage mechanism
called apoptosis.
# May prevent cancer affected cells from dividing
and spreading into healthy tissues
# May prevent new blood vessels from turning in
tumors.
# May accelerat the cell's inside 'waste disposal
mechanism' by triggering a process called autophagy. which increases the
apoptosis in cancer affected cells.
Few
Revolutionary Medical Research and Studies on CBD and Cancer
Cannabis has been the subject of various cancer
research studies over the last 20 years. Here is some honorable mentions
emphasizing CBD in cancer treatment.
Crosstalk between chemokine receptor CXCR4 and
cannabinoid receptor CB2 in modulating breast cancer growth and invasion.
Nasser MW; et al; PLoS One. 2011;6(9):e23901. doi:
10.1371/journal.pone.0023901. Epub 2011 Sep 7; http://www.ncbi.nlm.nih.gov/pubmed/21915267.
Cannabinoids: a new hope for breast cancer therapy?
Caffarel MM et al; Cancer Treat Rev.: 2012 Nov;
38(7):911-8. doi: 10.1016/j.ctrv.2012.06.005. Epub 2012 Jul 7; http://www.ncbi.nlm.nih.gov/pubmed/22776349.
“Cannabinoids Induce Apoptosis of Pancreatic Tumour
Cells via Endoplasmic Reticulum Stress–Related Genes” (Cancer Research, 2006)
“Cannabis-based medicine reduces multiple
pathological processes in A?PP/PS1 mice” (Journal of Alzheimer’s Disease, 2015)
“Inhibition of skin tumour growth and angiogenis in
vivo by action of cannabinoid receptors” (Journal of Clinical Investigation,
2003)
The role of cannabinoids in prostate cancer: Basic
science perspective and potential clinical applications;Juan A. Ramos and
Fernando J. Bianco; Indian J Urol. 2012 Jan-Mar; 28(1): 9–14;.doi:10.4103/0970-1591.94942;
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3339795/?report=classic
Delta9-tetrahydrocannabinol-induced apoptosis in
Jurkat leukemia T cells is regulated by translocation of Bad to mitochondria.
Jia W et al; Mol Cancer Res.; 2006 Aug;4(8):549-62; http://www.ncbi.nlm.nih.gov/pubmed/16908594
Cannabinoids - a new weapon against cancer? BY Pokrywka M1, Góralska J1, Solnica B1.
Closing
Thoughts
CBD can help you on the off chance that you are a cancer patient who does not say "we have done whatever we can do" to heart, but always keep the spirit and believe fighting this deadly disease. As mentioned above, numerous scientific studies and researches prove that CBD can be an ideal option for cancer patients. With safe, high quality and natural CBD products we are here to provide you a safe and standard cancer free living in. Visit us today at Whole CBD Choice.
References
Crosstalk between chemokine receptor CXCR4 and
cannabinoid receptor CB2 in modulating breast cancer growth and invasion.
Nasser MW; et al; PLoS One. 2011;6(9):e23901. doi:
10.1371/journal.pone.0023901. Epub 2011 Sep 7; http://www.ncbi.nlm.nih.gov/pubmed/21915267.
Cannabidiol as a novel inhibitor of Id-1 gene
expression in aggressive breast cancer cells; McAllister SDet al; Mol Cancer
Ther. 2007 Nov;6(11):2921-7; http://www.ncbi.nlm.nih.gov/pubmed/18025276.
Delta9-tetrahydrocannabinol inhibits cell cycle
progression in human breast cancer cells through Cdc2 regulation; Caffarel MM
et al;
Cancer Res;
2006 Jul 1;66(13):6615-21; http://www.ncbi.nlm.nih.gov/pubmed/16818634
Cannabinoids: a new hope for breast cancer
therapy?
Caffarel MM et al; Cancer Treat Rev.: 2012 Nov;
38(7):911-8. doi: 10.1016/j.ctrv.2012.06.005. Epub 2012 Jul 7; http://www.ncbi.nlm.nih.gov/pubmed/22776349
Cannabidiol inhibits lung cancer cell invasion
and metastasis via intercellular adhesion molecule-1.Ramer R et al; FASEB J.;
2012 Apr;26(4):1535-48. doi: 10.1096/fj.11-198184. Epub 2011 Dec 23; http://www.ncbi.nlm.nih.gov/pubmed/22198381?dopt=Abstract
Cannabinoid receptors, CB1 and CB2, as novel
targets for inhibition of non-small cell lung cancer growth and metastasis;
Preet A, et al; Cancer Prev Res (Phila). 2011 Jan;4(1):65-75. doi:
10.1158/1940-6207.CAPR-10-0181. Epub 2010 Nov 19; http://www.ncbi.nlm.nih.gov/pubmed/21097714?dopt=Abstract
Δ9-Tetrahydrocannabinol inhibits epithelial
growth factor-induced lung cancer cell migration in vitro as well as
its growth and metastasis in vivo; A Preetet al; Oncogene;
(2008) 27, 339–346; doi:10.1038/sj.onc.1210641; published online 9 July
2007; http://www.nature.com/onc/journal/v27/n3/abs/1210641a.html
https://www.cancer.gov/about-cancer/treatment/cam/hp/cannabis-pdq#section/all
The role of cannabinoids in prostate cancer:
Basic science perspective and potential clinical applications;Juan A. Ramos and
Fernando J. Bianco; Indian J Urol. 2012 Jan-Mar; 28(1):
9–14;.doi:10.4103/0970-1591.94942; http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3339795/?report=classic
Targeting CB2 cannabinoid receptors as a novel
therapy to treat malignant lymphoblastic disease.
McKallip RJ et al; Blood. 2002 Jul
15;100(2):627-34.; http://www.ncbi.nlm.nih.gov/pubmed/12091357
Delta9-tetrahydrocannabinol-induced apoptosis
in Jurkat leukemia T cells is regulated by translocation of Bad to
mitochondria.
Jia W et al; Mol Cancer Res.; 2006 Aug;4(8):549-62; http://www.ncbi.nlm.nih.gov/pubmed/16908594.
Inhibition of skin tumor growth and
angiogenesis in vivo by activation of cannabinoid receptors.
Casanova ML et al: J Clin Invest. 2003
Jan;111(1):43-50; http://www.ncbi.nlm.nih.gov/pubmed/12511587
Cannabidiol inhibits cancer cell invasion via
upregulation of tissue inhibitor of matrix metalloproteinases-1; Ramer Ret al;
Biochem Pharmacol; 2010 Apr 1;79(7):955-66. doi: 10.1016/j.bcp.2009.11.007.
Epub 2009 Nov 13; http://www.ncbi.nlm.nih.gov/pubmed/19914218
Anti-tumoral action of cannabinoids on
hepatocellular carcinoma: role of AMPK-dependent activation of autophagy. Vara
D et al.
Read the full article
0 notes
Last Seen Blogs

got2ghost-archive
devotion

sinntaurr
Crappy Art n' Stuff

jadadakid
Jada Da kid

sueniosfertiles
♥ Sueños Fertiles

tariqueaziz
Untitled