#cancer patients
Text
THEY ORDERED TO DISCONTINUE THE CARE OF CHILDREN WITH CANCER!??????? I CANNOT MAKE THIS UP
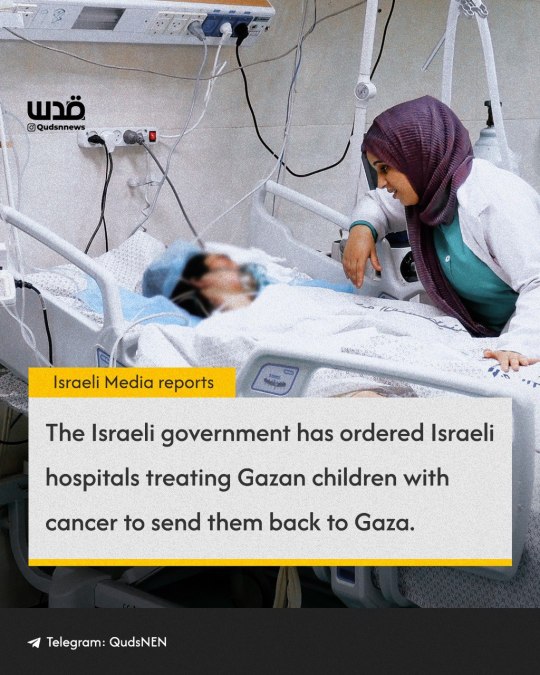
Media Coverage | According to Israeli media reports, the Israeli government has ordered Israeli hospitals hosting pediatric oncology patients from Gaza to discontinue their care so they can be sent back to Gaza.
Source: Quds News Network. As of 22nd March 2024.
#palestine#Gaza#cancer patients#Children#Israel#israel is committing genocide#israel is evil#israel is an apartheid state#free palestine
35 notes
·
View notes
Text
Fighting for Cancer
All Stickers and emoji sales will be used for Uncle Dindo’s medical debts and balances for his wake and burial, Auntie Sam’s and my ongoing Hormonal and chemo treatment. We also set a targeted amount through our goal for donations. We thank you all, thank you so much for everything.
We deeply appreciate all donations and purchases that will be made.
To all who have helped me in the past. I am eternally grateful.
Please help me share this post, reblog. It will help me a lot.
❤️🩹❤️🩷🧡💛
Hello Dear friends,
I hope you are all doing well. It’s been a long time since I have made an update about my health and everything that is happening to my life. Life has been so busy.
As you read the title for this campaign. Yes, Fighting for cancer, as some of you know I fought with the same battle several years ago, to my friends who helped me financially and all. My never ending gratitude to all of you.
I became okay and I chose to deal with financial struggles myself, because I know that I am already giving too much burden to my friends over the course of more than a year. I went back to do regular jobs despite lower grade pays in order to survive, and pay the remaining debt for my medication.
Where I live, we are paid daily, not hourly and daily wages are between $12-$15/day. And work 8-12 hours a day.
Unfortunately, life does not always end like a fairytale.
I am doing this campaign again. Not just for myself but for the other two people that are important to my life. I guess this battle runs into the family. I lost so many family members battling this. I lost my Dad to Stage 4 lung cancer last 2015. And last night(March 25,2024) I lost my Uncle Dindo in the same battle, after several months of intensive treatment. It left us drowning with hospital bills, and debts and it cost us nearly $130,000 and is still running. Uncle Dindo left her wife and two daughters, one who is deaf and mute.
Not only that, my Aunt Sam, is also dealing with her Stage 3 Breast Cancer, and it costs us almost $2,000 - $3,000 a week. Her right breast has already been removed. But she is also under close observation. And she was forced to have her unpaid leave at her job, as she needed rest. This also adds up with the financial struggles that we are dealing with too. We have bad healthcare here in PH. And if you are not rich you will die easily.
As for me. After I survived my battle in the Lungs. Tumors have popped up in other parts of my body, most of them are benign(but closely monitored for changes), if there will be malignant tumors again that will also pop out too. If you will see my previous posts, last year there had been a concern about my breast and a surgery was needed, but I decided not to proceed and I went through herbal medication, as it is the most affordable way. They helped me, but some backfired. And I am so afraid to lose a body part.
Unfortunately, I got bad pneumonia on-off, and the pain in my right breast is unbearable, after several tests. I am diagnosed with Stage 1. Doctors have already warned me in the past about this. And I also asked for a second opinion, because last year it was just only a close call. I will currently take hormone medication, and another chemo. I do not want another surgery at the moment, if it can be avoided. I have high hopes that I will survive this. I can still do jobs to pay for home and other bills. And be with you all.
I decided not just to do this campaign alone, but I also made a Ko-Fi Shop to sell digital stickers. With a collaboration and help from a friend, we currently made 11 printable stickers that you can print on the comfort of your home or print shops with a size of 2x2 inches. You can also use the emoji stickers through your streaming channel, please message me through my Twitter, so I can follow your stream. And for those who printed the physical stickers, it would make us happy if you can tag a photo of them through my twitter. You can put them through notebooks, tumblrs….etc.
Here is the link for our Ko-Fi Store.
Please follow me on twitter or here on Ko-Fi for updates. As we are still working on more Sticker designs.
We Can-CerVIVE.
I appreciate all the help that we could get. And thank you so much for understanding.
Please take good care of yourselves. Never take your health for granted. Health is wealth. And prevention is better than cure.
Love,
Jasky(Your Eternal Sprout)
P.S. To my friends in-game don’t worry you will still see me <3 I love you all! Stay happy and smiling.
These are the digital stickers that we are currently selling.

To all my friends, I badly need your help. Please. Thank you. Sorry for tagging you. Reblog and if you can tag your friends too. Thank you for understanding.
@measurelessdreamer @c1a1r3r3df1e1d @samblerambles @nearlybitches @sunhatllama @leonshinkai @shotce @crazyworldhuh @sparkie96 @silvertonguelover @fossil-finder @vietnoodle @irishspringyum @kevinbuiyin @angelspin @thecloudstan @neji-vuldarak @takuyasaeki1001 @valhethella @artofshiroginko @yuko27 @junie-junette @chris-is-not-evil @wuekka @nelyth-v @ya2do @rebrandedbard @tielmamon @signalboostr @mcqraw @risingoflights @travelling-hydaelyn @thedemonofcat @leonisdumbasallhell @litoperezito @priscilla-a-moreno @waywards-thing @chreonweek @heliosani @residentevilx4 @lemonadeswift @prozdvoices @doomednarrative @neil-gaiman @aussiepineapple1st @matchalilly @highball66 @purpledusty @diviedrawn @residenceevil
33 notes
·
View notes
Text
This is cross posted from Reddit. You can find the original here vvv
If you don’t know me, hey there I'm B.
December of 2022 u/mrtechnodad gave me the challenge of finding something good in every day, no matter how small. Since then I’ve been sharing monthly updates with a few of my good things from that month.
Anyone who's followed my updates has probably noticed that the title is different and I missed part of my usual intro.
That's because today's list only has one thing:
- I'm officially cancer free
After 708 days, countless hours of chemo, and 4 major surgeries, I have beat almost impossible odds.
Along my journey I've lost too many people who were important to me. Each of them gave me a new reason to keep going. My first roommate taught me how to be strong, how to push through the darkness. My second roommate taught me the power of compassion, how to use my voice to help others. A friend taught me how to laugh, how to see the fun in even the worst situations. And Techno, Technoblade taught me how to fight, how to win any war.
It's no secret I've struggled with survivor's guilt for almost as long as I was sick. I've asked the question, "Why them and not me?" so many times it's become a mantra. I've realized it isn’t about me or them. I think it's about finding what my purpose is. Their lives had purpose, they were full of love and joy. For so long I didn't think I had those things, that there wasn't a reason for me to still be here. I still have a purpose here. I think I know it. At least part of it.
I'm here to share my story. I'm here to share the good I see in every day. I'm here to live.
I'm alive to live.
And so are you.
Be alive. Wake up to wake up. Laugh, cry, sing, dance. Feel everything, sadness, joy, grief, shame, love. Watch the sunrise and live to see it set again. Then do it all again. And again.
Be alive to live.
Today I sat on a beach and watched the sunrise with the love of my life. For the first time in almost two years it wasn't tainted by the possibility of being my last. Instead the sun rose on the first day of my future. It's the first one of a lifetime of new days. Sunrises are no longer a symbol of bitter relief. Now they represent the promise of tomorrow.
I am beyond grateful to be alive. Since my diagnosis I was so sure I wouldn't make it. I had so little hope. Now my voice can shift from the cries of a fighter to the laughter of a survivor.
I am a survivor. Those are words I never dreamed of speaking.
Thank you to everyone who followed my journey. Thank you for your love, your support, and your endless compassion. Without this community my story would be very different.
Remember, "no matter how ridiculous the odds may seem, within us resides the power to overcome these challenges and achieve something beautiful. That one day, we'll look back at where we started and be amazed by how far we've come."
Until next time.
Your friend, B
#BRUHHHH#The fact that I can make this post#is insane#I'm a survivor baby!#cancer#cancer survivor#cancer patient#cancer awareness#cancer patients#heythereimb#technoblr#technoblade#dsmp techno#techno#dream smp#techno support#technodad
39 notes
·
View notes
Text
instagram





#cancer patients#cancer#human rights#human health#palestine#free gaza#i stand with palestine 🇵🇸#gaza#free palestine 🇵🇸#gaza strip#free palestine#gazaunderattack#palestine resources#endisraelsgenocide#israeli terrorism#israel is a terrorist state#israel is committing genocide#Instagram
21 notes
·
View notes
Text
"I wanted you to know that my friend Chris Tucker is reacting great to his treatments !"
Thank you sweet Jesus for your Mercies and Grace, the healing that comes from above, and the love you give us for our daily journey. Please dear Lord, continue with healing of Chris as well as so many cancer patients. Give them the fearless strength not only to battle through this part of their life but to also look beyond the physical needs, to seek your loving embrace spiritually for healing. Let them be filled with the glorious realization of Your Love. Heal them Lord as witness' to Your Glory; Your will of what is to be. We humbly ask this in the Precious Name of Jesus -- amen.
Our Lady of Lourdes, please intercede on our behalf.
St Bernadette, please pray for us.
In the name of the Father and the Son and the Holy Spirit. amen
I hope that other people will join us in prayer for Chris. Please also add prayer for Chris' family and friends @meegan420 and @krist-420
#prayer report#giving praise#cancer patients#healing#our lady of lourdes please intercede#st bernadette pray for us
7 notes
·
View notes
Text
My best friend's mom was recently diagnosed with Metaplastic Breast Cancer
If you can, please consider donating to help ease Michelle and her family's financial burden while she battles breast cancer. It's ok if you can't donate; even a share and reblog would be very appreciated
Thank you for taking the time to read through this post and the link, and keep Michelle and her family in your thoughts
#fundrasier#fundraising#please consider donating#donations#breast cancer#cancer patients#cancer diagnosis
8 notes
·
View notes
Text
"Cancer survivors are blessed with two lives. There is your life before cancer, and you life after. I am here to tell you your second life is going to be so much better than the first."
Hoda Koth - American Journalist and TV Personality
#quoteoftheday#quotes#quotesoftheday#quotes of tumblr#breast cancer awareness month#hoda koth#tv personality#cancer survivors#cancer awareness#breast cancer awareness#cancer patients#support for cancer patients
3 notes
·
View notes
Text
Here's some cancer sketches I did yesterday at the hospital b4 they doped me up for spinal chemo. Everything could've gone worse but I still feel like shit :/ original bone marrow results are negative (massive sigh of relief) but the leukemia is still showing up positive in my spinal fluids. It really do be hiding in my central nervous system, and my oncologist said the scary "Car T Cell Therapy" yesterday. Hopefully if I do anymore treatments it just monoclonal antibodies bc I will cry if I lose my hair again :(( but at the same time I don't want to DIE so ig I'll do what I gotta do :^)
I was gonna make more zukka fanart but I have to focus on my health and school

#artists on tumblr#sketch#cancer#cancer patients#gay art#leukemia#brain surgery#iwantmorefriendsbclifesucksandidontwanttodiealone:(
7 notes
·
View notes
Text


If I had a nickel for everytime Technodad talked about me on TommtInnit's stream, I'd have two nickels. Which isn't a lot but it's weird that it's happened twice
#literally still freaking out#Technodad my beloved#I cant believe this#tommyinnit#dsmp tommy#tommy innit#technodad#techno support#technoblade#technoblr#cancer#cancer survivor#cancer patient#cancer awareness#heythereimb#dsmp techno#techno#dream smp#cancer patients
46 notes
·
View notes
Text
instagram

#in need of medical care#in need of medical care abroad#endisraelsgenocide#israeli terrorism#israeli terrorists#israeli war crimes#israel war criminal#palestine#gaza#basic human rights#human rights violations#cancer patients#cancer#medical crisis#i stand with palestine 🇵🇸#free palestine 🇵🇸#free gaza#gaza strip#free palestine#palestine resources#gazaunderattack#israel is a genocidal state#israel is a terrorist state#israel is a war criminal#israel is an apartheid state#israel is an illegal occupier#israel is committing genocide#Instagram
13 notes
·
View notes
Text
I feel the wool of dread in my throat
like the thought of my future
is an allergic reaction;
I stay away from thinking too far ahead
in a desperate act of self-preservation.
Inevitably, I will begin to live again,
through the droplets of water on a tomato leaf -
an unusually soft sun on my shoulders,
but the dread will return in 3 month intervals
and yank my chain back to the present.
On the days I am forced face-to-face
with my own fate
I think of what could lie ahead,
and my throat closes to protect me from
swallowing the fear.
You hold a match to my sliver of survival -
and rip me out of a future
I have finally learned to welcome.
#cancer#poem#poet#poetry#cancer patient#cancer patients#tw death#mortality#don’t mind me just having an existential crisis#chronic illness#diagnosis#chronically ill
3 notes
·
View notes
Text




3 notes
·
View notes
Text
Use of acupressure to reduce nausea and vomiting in cancer patients receiving chemotherapy (literature study) by Maher Battat in Journal of Clinical Case Reports Medical Images and Health Sciences

ABSTRACT
Nausea and vomiting are distressing and serious problems for cancer patients receiving chemotherapy despite the fact that they are receiving antiemetics according to the standard guidelines which this problem is a huge challenge to nurses involved in cancer care.
Purpose: To explore and assess the effectiveness of using acupressure as a non-pharmacological intervention in addition to pharmacological interventions in reducing nausea and vomiting in cancer patients receiving chemotherapy.
Method: A literature review was conducted of 8 articles published between 2006 and 2014. These included one study of a randomized, double-blind, placebo controlled trial; one quasi-experimental model with a control group; four articles reporting on randomized control trials (RCTs); one systematic review study; and one review study. Key Findings: Seven of the articles we read supported the effect of an acupressure P6 Wristband in reducing chemotherapy induced nausea and vomiting in cancer patients and other databases also supported that finding. The one article with neutral results showed that there was no difference between a combination of acupuncture and acupressure treatment at P6 and at the sham point for the nausea score, but the level of nausea was very low in both groups.
Conclusion: We conclude that the acupressure P6 wrist band when applied to acupuncture point P6 is effective, safe, convenient, cost effective, and provides an easy, self-administrated, non-pharmacological intervention that can be used to reduce chemotherapy induced nausea and vomiting.
Keywords: Acupressure, Chemotherapy, Nausea and Vomiting, Cancer patients, Chemotherapy-induced nausea and vomiting.
INTRODUCTION
Nausea and vomiting are serious and troublesome side effects of cancer therapy. We chose this research topic in order to become familiar with the topic of the nausea and vomiting facing cancer patients during their chemotherapy treatment, which we have observed during our experience in the Oncology departments.
As nurses, we normally use updated and standard guidelines for managing clinical challenges. We reviewed the literature to explore whether there are alternative approaches to pharmacological management that might reduce or eliminate this problem. We found there are many interventions, such as music, acupuncture, acupressure, and yoga. We decided to assess the effectiveness of using acupressure to reduce the nausea and vomiting in cancer patients receiving chemotherapy. Acupressure is a type of complementary and alternative medicine which the National Cancer Institute (NCI Dictionary of Cancer Terms) defines as follows: “Acupressure is the application of pressure or localized massage to specific sites on the body to control symptoms such as pain or nausea".
THE RESEARCH QUESTION
Can acupressure reduce nausea and vomiting in cancer patients receiving chemotherapy?
We have chosen to use the definitions of the NCI Dictionary of Cancer Terms:
“Nausea is an unpleasant wavelike feeling in the back of the throat and/or stomach that may lead to vomiting", and “Vomiting is throwing up the contents of the stomach through the mouth”.
Nausea and vomiting affect the patient’s whole life. These side effects lead to metabolic imbalance, fatigue, distress, and lowered quality of life. We would like to fine a simple, effective and cost effective way to manage these problems so we can put it to use in our hospital.
METHOD
A literature study is, “A critical presentation of knowledge from various academic written sources, and a discussion of the sources in view of a particular research question" (Synnes 2014). There are many challenges when doing a literature study. There are many databases and much literature and our search process had to find the correct, scientific and relevant databases. It required a lot of time and effort to find the full text of all relevant articles. Fortunately, we received excellent help from the librarian at the Betanien University High school.
We started the search process by making a PICO outline to narrow down the search and to find the correct key words and mesh terms.
P: (Population or participants) Cancer patients experiencing chemotherapy-induced nausea and vomiting.
I: (Intervention or indicator) Acupressure.
C: (Comparator or control) No comparison or placebo.
O: (Outcome) Reduce nausea and vomiting.
We used PUBMED, Google scholar, scholar.najah.edu and other search engines. When we used Acupressure as a search word we found more than 800 studies. When we added chemotherapy, cancer patients, and nausea and vomiting, we brought this down to 14 articles. We read these and decided to use 8 articles only, one of which was a systematic review. We also used an unpublished Master’s thesis from An Najah National University. This thesis was cited in one of the articles that we decided to review. The key words used were: Acupressure, Chemotherapy, Nausea and Vomiting, Cancer patients, Chemotherapy-induced nausea and vomiting, with Acupressure as a mesh term.
We then critically appraised all the articles according to our checklist. We included only those articles that followed the IMRAD style (i.e. those including an introduction, method, results and discussion section). We excluded all articles that were more than ten years old (i.e. published before 2004), except for two articles: one was about the mechanism of acupressure, which seemed to be directly relevant to our research topic, while the second article was used in the discussion section to discuss certain factors related to the topic. We also excluded one of the review articles because its method appeared to be weak. One of the Cochran reviews was also dropped because it had not been updated.
Despite applying these strict criteria, we were still concerned lest we had left out some important articles or included an inappropriate one. However, we were reassured by the fact that the librarian at Betanien had guided us in our search.
THEORETICAL PART
Nursing Need Theory and basic human needs
The Nursing Need Theory was developed by Virginia A. Henderson to define the unique focus of nursing practice. The theory focuses on the importance of increasing the patients’ independence to hasten their progress in the hospital. Henderson’s theory emphasizes the basic human needs and how nurses can assist in meeting those needs.
The 14 components of Need Theory present a holistic approach to nursing that covers the patient’s physiological, psychological, spiritual and social needs.
Physiological components
Breathe normally.
Eat and drink adequately.
Eliminate body wastes.
Move and maintain desirable postures.
Sleep and rest.
Select suitable clothes – dress and undress.
Maintain body temperature within normal range by adjusting clothing and modifying the environment.
Keep the body clean and well groomed and protect the integument.
Avoid dangers in the environment and avoid injuring others.
Psychological aspects of communicating and learning
Communicate with others in expressing emotions, needs, fears, or opinions. Spiritual and moral
Worship according to one’s faith. Sociologically oriented to occupation and recreation
Work in such a way that there is sense of accomplishment.
Play or participate in various forms of recreation.
Learn, discover, or satisfy the curiosity that leads to normal development and health, and use the available health facilities.
There is much similarity between Henderson’s 14 components and Abraham Maslow’s Hierarchy of Needs. Henderson’s Components 1 to 9 are comparable to Maslow’s physiological needs, with the 9th component also being a safety need. Henderson’s 10th and 11th components are similar to Maslow’s love and belonging needs, while her 12th, 13th and 14th components match Maslow’s self-esteem needs (Vera 2014).
The second of Henderson’s physiological needs is the need to “Eat and drink adequately”. Only the need to breathe is given a higher priority than the need for adequate nutrition. For cancer patients receiving chemotherapy and suffering from chemotherapy-induced nausea and vomiting, this need is the most critical.
Cancer prevalence and treatment
Cancer is a group of diseases characterized by uncontrolled growth and the spread of abnormal cells. It may be caused by internal factors, such as an inherited mutation, or a hormonal or immune condition, or it may result from a mutation from metabolism, or from external sources, such as tobacco use, radiation, chemicals and infectious organisms. Cancer is prevalent all over the world, in both developed and developing nations; it affects both sexes at all ages (Said 2009). The American Cancer Society (2010) estimated that 1,529,560 new cases of cancer were diagnosed in 2010 and that 80 % would be treated with chemotherapy; this means more than 1 million patients will be undergoing chemotherapy in any given year (Lee et al. 2010).
Cancer treatment may be based on chemotherapy, radiotherapy and surgical interventions. Chemotherapy is an important treatment in cancer care but it is associated with several side effects, such as bone marrow suppression, increased susceptibility to infection, diarrhea, hair loss, appetite changes, nausea and vomiting, among others (NCI Chemotherapy Side Effects Series, 2014).
Chemotherapy-induced nausea and vomiting (CINV) is the most prevalent and one of the hardest side effects to manage (Suh 2012).
Nausea and vomiting
Nausea and vomiting (N&V) can be acute or delayed. The incidence of acute and delayed N&V was investigated in highly and moderately emetogenic chemotherapy treatment regimens. Patients were recruited from 14 oncology practices in six countries. Overall, more than 35% of patients experienced acute nausea, and 13% experienced acute emesis. In patients receiving highly emetogenic chemotherapy, 60% experienced delayed nausea and 50% experienced delayed emesis. In patients receiving moderately emetogenic chemotherapy, 52% experienced delayed nausea and 28% experienced delayed emesis. CINV was a substantial problem for patients receiving moderately emetogenic chemotherapy in ten community oncology clinics. Thirty-six percent of patients developed acute CINV, and 59% developed delayed CINV (NCI, Nausea and Vomiting, 2015).
Chemotherapy is the most common treatment-related cause of N&V. The incidence and severity of acute emesis in persons receiving chemotherapy varies according to many factors, including the particular drug, dose, schedule of administration, route, and individual patient variables.
Risk factors for acute emesis include:
Poor control with prior chemotherapy
Female gender
Younger age
Emetic classification:
The American Society of Clinical Oncology has developed a rating system for chemotherapeutic agents with their respective risk for acute and delayed emesis.
High risk: Emesis has been documented to occur in more than 90% of patients on the following chemotherapeutic agents:
Cisplatin (Platinol).
Mechlorethamine (Mustargen).
Streptozotocin (Zanosar).
Cyclophosphamide (Cytoxan), 1,500 mg/m2 or more.
Carmustine (BiCNU).
Dacarbazine (DTIC-Dome).
Moderate risk: Emesis has been documented to occur in 30% to 90% of patients on the following chemotherapeutic agents:
Carboplatin (Paraplatin).
Cyclophosphamide (Cytoxan), less than 1,500 mg/m2.
Daunorubicin (DaunoXome).
Doxorubicin (Adriamycin).
Epirubicin (Pharmorubicin).
Idarubicin (Idamycin).
Oxaliplatin (Eloxatin).
Cytarabine (Cytosar), more than 1 g/m2.
Ifosfamide (Ifex).
Irinotecan (Camptosar).
Low risk: Emesis that has been documented to occur in 10% to 30% of patients on the following chemotherapeutic agents:
Mitoxantrone (Novantrone).
Paclitaxel (Taxol).
Docetaxel (Taxotere).
Mitomycin (Mutamycin).
Topotecan (Hycamtin).
Gemcitabine (Gemzar).
Etoposide (Vepesid).
Pemetrexed (Alimta).
Methotrexate (Rheumatrex).
Cytarabine (Cytosar), less than 1,000 mg/m2.
Fluorouracil (Efudex).
Bortezomib (Velcade).
Cetuximab (Erbitux).
Trastuzumab (Herceptin).
Minimal risk: Emesis that has been documented to occur in fewer than 10% of patients on the following chemotherapeutic agents:
Vinorelbine (Navelbine).
Bevacizumab (Avastin).
Rituximab (Rituxan).
Bleomycin (Blenoxane).
Vinblastine (Velban).
Vincristine (Oncovin).
Busulphan (Myleran).
Fludarabine (Fludara).
2-Chlorodeoxyadenosine (Leustatin).
In addition to the emetogenic potential of the agent, the dose and schedule used are also extremely important factors. For example, prescribing a drug with a low emetogenic potential to be given in high doses may cause a dramatic increase in its potential to induce N&V. For example, standard doses of cytarabine rarely produce N&V, but these often occur with high doses of this drug. Another factor to consider is the use of drug combinations. Because most patients receive combination chemotherapy, the emetogenic potential of all of the drugs combined needs to be considered, and not only that of individual drug doses.
Delayed (or late) N&V is that which occurs more than 24 hours after chemotherapy administration. Delayed N&V is associated with cisplatin and cyclophosphamide, and with other drugs (e.g., doxorubicin and ifosfamide) when given at high doses, or if given on 2 or more consecutive days.
Delayed emesis: Patients who experience acute emesis with chemotherapy are significantly more likely to have delayed emesis as well.
Risk factors: All the predicative characteristics for acute emesis are also considered risk factors for delayed emesis (NCI, Nausea and Vomiting, 2015).
The nausea and vomiting that are often associated with chemotherapy are a serious problem for cancer patients. Despite recent improvements in pharmaceutical technology, about 60% of cancer patients who receive antiemetic medications with their chemotherapy still suffer from nausea and vomiting, and as many as 20% of patients refuse to continue chemotherapy due to the severity of the nausea and vomiting (Shin et al. 2004). Early studies reported that patients cited nausea and vomiting as the most distressing symptoms when receiving chemotherapy. The distressing effect of severe nausea and vomiting can lead to nutritional deficiencies, dehydration, electrolyte imbalance, fatigue, depression and anxiety; they can also disrupt the activities of daily living and cause a lot of work time to be lost (Said 2009).
Uncontrolled nausea and vomiting can interfere with adherence to treatment regimens, and may cause the oncologists to reduce chemotherapy doses. Chemotherapy-induced nausea and vomiting is classified as being either “acute” if it happens within 24 hours post chemotherapy, or “delayed” if it occurs on days 2–5 of the chemotherapy cycle. The latter is particularly troublesome because there is no reliable pharmacological treatment for this problem. The American Society of Clinical Oncology’s (ASCO) recommendations include giving 5-HT3 (5-hydroxytryptamine, or serotonin) receptor antagonists plus corticosteroids before chemotherapy to patients who are at high risk for emesis. Nevertheless, many patients still experience nausea and vomiting related to chemotherapy, and approximately one-third of patients have nausea of at least moderate intensity, resulting in a significant reduced quality of life (QOL). Therefore, the experts emphasize the need for an evaluation of additional ways to reduce these symptoms (Said 2009).
Pharmacological interventions for the management of nausea and vomiting
Historically, antiemetic treatment has steadily improved since the introduction, in 1981, of high-dose metoclopramide which reduced the amount of emesis. This was followed by the development of serotonin (5-HT3) antagonist in the early 1990s, and the 5-HT3 antagonists proved to be more effective than the prior medications in preventing CINV. The concomitant use of corticosteroids was found to further improve the control of emesis. Despite these improvements, nausea and vomiting still remain a problem for many patients. Recently, a new drug, the neurokinin NK (1) receptor antagonist has been shown to be more effective at preventing both acute and delayed CINV for patients treated with highly emetogenic chemotherapy (Said 2009).
Non-pharmacological intervention for management of nausea and vomiting
Traditional Chinese medicine offers a possible intervention for the non-pharmacological treatment of nausea and vomiting in cancer patients. Traditional Chinese medicine (TCM) is a system of medical care that was developed in China over thousands of years. It looks at the interaction between mind, body and environment, and aims to both prevent and cure illness and disease.
TCM is based on Chinese views and beliefs about the universe and the natural world. It is a very complex system. In this essay we can only give a brief overview of what TCM involves. It is very different from Western medicine; Chinese medicine practitioners believe there is no separation between the mind and body and that illness of every kind can be treated through the body. They use a combination of various practices that may include:
Herbal remedies (traditional Chinese medicines).
Acupuncture or acupressure.
Moxibustion (burning moxa – a cone or stick of dried herb).
Massage therapy.
Feng shui.
Breathing and movement exercises called qi gong (pronounced chee goong).
Movement exercises called tai chi (pronounced tie chee).
TCM practitioners say that TCM can help to:
Prevent and heal illness.
Enhance the immune system.
Improve creativity.
Improve the ability to enjoy life and work in general.
Beliefs behind TCM
According to traditional Chinese belief, humans are interconnected with nature and affected by its forces. The human body is seen as an organic whole in which the organs, tissues, and other parts have distinct functions but are all interdependent. In this view, health and disease relate to the balance or imbalance between the various functions. TCM treatments aim to cure problems by restoring the balance of energies.
There are important components that underlie the basis of TCM:
Yin-yang theory is the concept of two opposing but complementary forces that shape the world and all life. A balance of yin and yang maintains harmony in the body, the mind and the universe.
Qi (pronounced chee) energy or vital life force flows through the body along pathways known as meridians, and it is affected by the balance of yin and yang. It regulates spiritual, emotional, mental, and physical health. If there is a blockage or an imbalance in the energy flow, the individual becomes ill. TCM aims to restore the balance of qi energy.
The five elements – fire, earth, metal, water, and wood – is a concept that explains how the body works, with the elements corresponding to particular organs and tissues in the body.
The TCM approach uses 8 principles to analyse symptoms and puts particular conditions into groups: cold and heat, inside and outside, too much and not enough, and yin and yang (Cancer Research, UK, 2015).
In summary, chemotherapy related nausea is not well controlled by pharmacological agents and identifying methods to prevent and alleviate treatment-related nausea remains a major clinical challenge. Non-pharmacological interventions such as music, progressive muscle relaxation (Said 2009), and ginger herbal therapy (Montazeri A et al. 2013) have all been shown to reduce CINV. Among the non-pharmacological interventions that reduce CINV are acupuncture and acupressure, based on the assumption that the individual’s welfare depends on a balance of energy in the body and their overall energy level (Said 2009). Yarbro et al. (2011, p. 645) also indicate in Cancer nursing: principles and practice book that acupuncture and acupuncture-related interventions (electroacupoint stimulation, acupressure, acustimulation wrist bands, and electroacupuncture) can be used to control nausea and vomiting in cancer patients.
Molassiotis et al. (2007) claim that the need for additional relief has led to the interest in non-pharmacological adjuncts to drugs, such as acupuncture or acupressure, since combining anti-emetics with other non-pharmacological treatments may prove to be more effective, safe and convenient in decreasing nausea than antiemetics alone.
From the National Cancer Institute website we found that acupressure is recognised as one of the non-pharmacologic strategies used to manage nausea and vomiting (Nausea and Vomiting, 3 September 2014). We used this website to get up to date, relevant information.
Acupressure
Acupressure involves putting pressure with the fingers, or with bands, on the body’s acupoints and is easy to perform, painless, inexpensive, and is effective. The P6 (Pericardium 6) point (Nei-Guan) refers to a point located on the anterior surface of the forearm, 3-finger widths up from the first wrist crease and between the tendons of flexor carpiradialis and Palmaris longus (figure1). P6 can be stimulated by various methods. The most well-known technique is manual stimulation by the insertion and manual rotation of a very fine needle (manual acupuncture). An electrical current can be passed through the inserted needle (electroacupuncture). Electrical stimulation can also be applied via electrodes on the skin surface or by a ReliefBand, a wristwatch-like device providing non-invasive electrostimulation. Pressure can be applied either by pressing the acupoint with the fingers or by wearing an elastic wristband with an embedded stud (acupressure).
Figure 1: Done by M.Battat & I.Amro 2015 The Acupressure P6 point determined in the picture And showing the SEA BAND acupressure
Acupressure is based on the ancient Eastern concept that Chi energy travels through pathways known as meridians. Along the meridians are acu-points, which are controlling points for the Chi energy flow. If the energy flow in meridians is slowed, blocked, or hyper-stimulated, it can be rebalanced or re-stimulated either by applying pressure (acupressure) or by inserting a needle (acupuncture) into one or more of these acupoints. Two points are known for relieving nausea and vomiting: the Nei-Guan point (P6) and the Joksamly point (ST36, located at 4-finger breadths below the knee depression lateral to the tibia).
Patients tend to prefer the P6 point over the ST36 point, Because of its ease of access and the freedom from restriction. When these points are correctly located and pressure applied, either through acupressure or acupuncture, the Chi energy flow is rebalanced, resulting in relief from nausea and vomiting.
The practice of acupressure requires some training and experience, but the technique is widely accessible to any healthcare professionals, particularly to clinical nurses. This acupressure technique is an approach that should be tried not only by healthcare professionals but also by family members or the patients themselves (Shin et al. 2004).
According to the teaching of traditional Chinese medicine, illness results from an imbalance in the flow of energy through the body. This energy or Qi (chee) is restored through the use of acupuncture and acupressure at certain points on the body that have been identified through critical observation and testing over 4000 years. In scientific terms, the neurochemicals that are released after needling or pressure at a specific point may be responsible for this effect. The most commonly used point for nausea and vomiting is Pericardium 6 (Neiguan or P6), located above the wrist (Molassiotis et al. 2007).
The literature review on acupressure
Acupressure for chemotherapy-induced nausea and vomiting in breast cancer patients: a multicentre, randomised, double-blind, placebo-controlled clinical trial. (Said 2009)
For a master degree in public health from An-najah National University, Said (2009) described a randomized, double-blind, placebo controlled trial that was done in Palestine with 126 women on chemotherapy for breast cancer. In this study the researcher divided the patients into 3 groups: the first group (n=42) received acupressure with bilateral stimulation of P6, the second group (n=42) received bilateral placebo stimulation, and the third group (n=42), which served as a control group, received no acupressure wrist band, but all groups received pharmacological management of their nausea and vomiting. Acupressure was applied using a Sea-Band (Sea-Band UK Ltd, Leicestershire, England) that patients had to wear for five days following the administration of chemotherapy. Assessment of acute and delayed nausea and emesis, quality of life, patients’ satisfaction, recommendation of treatment and requests for a rescue antiemetic were obtained. Said (2009) concluded that the acupressure showed benefits for delayed nausea and the mean number of delayed emetic episodes. Acupressure may therefore offer an inexpensive, convenient, and self-administered intervention for patients on chemotherapy to reduce nausea and vomiting at home during days 2-5 after chemotherapy. In addition, the percentage of patients who were satisfied with the treatment (≥ 3 on a 0-6 scale) was 81% (35/42) in the P6-acupressure group, and 64% (27/42) in the placebo group (p= 0.0471). The percentage of patients who would recommend acupressure treatment was 79% (34/42) in the P6-acupressure group, and 62% (26/42) in the placebo group (p= 0.0533). We used this study because it had a lot of essential information, it used the IMRAD system and was also mentioned in the literature (Genç and Tan 2014). This study demonstrated that the mean scores for the acupressure group were lower for both acute and delayed nausea.
Review of Acupressure Studies for Chemotherapy-Induced Nausea and Vomiting Control. (Lee et al. 2008)
In the Journal of Pain and Symptom Management Jiyeon Lee et al. (2008) reviewed ten controlled studies on acupressure in order to evaluate the effects of a non-invasive intervention, acupressure, when combined with antiemetics for the control of CINV. The review evaluated one quasi-experimental and nine randomized clinical trials, which included two specific acupressure modalities, namely, an acupressure band and finger acupressure. The effects of the acupressure modalities were compared study by study. Four of the seven acupressure band trials supported the positive effects of acupressure, whereas three acupressure band trials did not support the effects of acupressure. However, all the studies with negative results had methodological issues. In contrast, the one quasi-experimental and two of the randomized finger acupressure trials all supported the positive effects of acupressure on CINV control. The reported effects of the two acupressure modalities produced variable results at each stage of CINV. Acupressure bands were most effective in controlling acute nausea, whereas finger acupressure controlled delayed nausea and vomiting. The overall effect of acupressure was strongly indicative but not conclusive. We used this article because it is relevant, a review study, and is from a known journal.
The effects of P6 acupressure in the prophylaxis of chemotherapy-related nausea and vomiting in breast cancer patients. (Molassiotis et al. 2007)
As reported in the journal Complementary Therapies in Medicine, acupressure was applied using wristbands (Sea-Band™) in a randomized controlled trial conducted in two centres in the UK. Patients in the experimental group had to wear these bands for the five days following their chemotherapy administration. Assessments of nausea, retching and vomiting were obtained from all patients, daily, for five days. Molassiotis et al. (2007) evaluated the effectiveness of using acupressure on the Pericardium 6 (Neiguan) acupoint in managing CINV. Thirty-six patients took part in the study, with 19 patients allocated to the control group and 17 to the experimental group. The results showed that nausea with retching, nausea, and vomiting with retching, and the accompanying distress were all significantly lower in the experimental group as compared to the control group (p < 0.05). The only exception was the vomiting, where the difference was close to significance (p = 0.06). We used this article because it had a strong study design and also used an IMRAD system.
Acupuncture and acupressure for the prevention of chemotherapy-induced nausea- a randomized cross-over pilot study. (Melchart et al. 2006)
In a randomized, cross-over trial, Melchart et al. (2006) studied 28 patients receiving moderately or highly emetogenic chemotherapy and a conventional standard antiemetic for one chemotherapy cycle, followed by a combination of acupuncture and acupressure at point P6 for one cycle, and for another cycle a combination of acupuncture and acupressure at a close sham point. The results showed that there was no difference in the nausea score between the combined acupuncture treatment at P6 and at the sham point, but the level of nausea was very low in both cases. We used this study because the article had neutral results and because we trusted the source of article, coming as it did from a cancer support care journal.
The efficacy of acupoint stimulation for the management of therapy adverse events in patients with breast cancer: a systematic review. (Chao et al. 2009)
This is a systematic review of 26 articles published between 1999 to 2008 examining the efficacy of acupressure, acupuncture or acupoint stimulation (APS) for the management of adverse events due to the treatment of breast cancer. Published online on 17 September 2009 in the Breast Cancer Research and Treatment journal, 23 trials reported revealed that APS on P6 was beneficial in treating CINV. Chao et al. (2009) also presented the findings from three high quality studies comparing APS groups with control groups, which indicated that APS is beneficial in the management of CINV and especially in the acute phase, even with the non-invasive intervention. Health care professionals should consider using APS, and in particular acupressure on the P6 acupoint, as an option for the management of CINV. Furthermore, as a cost effective intervention, it warrants further investigation. We used this article because it used the IMRAD structure.
'Until the trial is complete you can’t really say whether it helped you or not, can you?’: exploring cancer patients’ perceptions of taking part in a trial of acupressure wristbands. (Hughes et al. 2013)
In Complementary and Alternative Medicine, Hughes et al. report on qualitative research undertaken with patients receiving chemotherapy in the UK. A convenience sample of 26 patients volunteered to participate in the clinical trial and to explore their experiences of using acupressure wristbands. Participants were recruited from three geographical sites: nine were recruited from Manchester, nine from Liverpool, and eight from Plymouth and the surrounding regions. Ten of the participating patients received true acupressure during the trial, 9 received sham acupressure, and 7 received no acupressure. Hughes et al. (2013) concluded that the research provided insights into cancer patients’ motivations and experience of taking part in a clinical trial for a complementary alternative medicine intervention, in which the participants perceived acupressure wristbands to reduce the level of nausea and vomiting experienced during their chemotherapy treatment. This article is important because it includes the benefits experienced by the patients taking part in the trial. This is also the first qualitative study to explore patients’ experiences of using acupressure wristbands and their perceptions of the effects. In the study, the patients perceived the wristbands as reducing their level of nausea and vomiting experienced due to their chemotherapy treatment. The study was an RCT.
The effect of acupressure application on chemotherapy-induced nausea, vomiting, and anxiety in patients with breast cancer. (Genç and Tan 2014)
Genç and Tan (2014) reported on a quasi-experimental study in Turkey with 64 patients with stages 1–3 breast cancer who received two or more cycles of advanced chemotherapy. Thirty two patients were in the experimental group, and thirty two in the control group. To determine the effect of acupressure P6 on CINV and anxiety in these patients, the P6 acupressure wristband was applied to the experimental group. Genç and Tan (2014) concluded that the total mean scores for patients in the experimental group, for nausea, vomiting and retching, were lower than those of the patients in the control group over the five days of application. We used this article because it is a recent and quasi-experimental study and used the IMRAD system.
The effects of P6 acupressure and nurse-provided counselling on chemotherapy-induced nausea and vomiting in patients with breast cancer. (Suh 2012)
Suh (2012) reported in the Oncology Nursing Forum on a RCT in South Korea with 120 women who were receiving chemotherapy for breast cancer. These patients had all had more than mild levels of nausea and vomiting during their first cycle of chemotherapy. The participants were assigned randomly to one of four groups: a control group (a placebo on a specific location on the hand); a counselling only group; a P6 acupressure only group; and a P6 acupressure plus nurse-provided counselling group. The purpose of the study was to evaluate the effects of pericardium 6 (P6) acupressure and nurse-provided counselling on CINV in patients with breast cancer. Suh (2012) concluded that nurse-provided counselling and P6 acupressure were together the most effective in reducing CINV in patients with breast cancer. We used this article because it is the first RCT evaluating the isolated and combined effects of P6 acupressure and counselling in reducing CINV among non-Western patients. The findings of the study support the use of P6 acupressure together with counselling that is focused on cognitive awareness, affective readiness, symptom acceptance, and the use of available resources as an adjunct to antiemetic medicine for the control of CINV. The article used the IMRAD system.
DISCUSSION
Can acupressure reduce nausea and vomiting in cancer patients receiving chemotherapy?
In our experience, we have usually used metoclopramide (pramin) plus serotonin (5-HT3) antagonist (as Ondansetron and Granisetron), plus Dexamethasone plus neurokinin NK (1) (as Emend - aprepitant) for moderate to high ematogenic chemotherapy, yet some of the patients have still suffered from nausea and vomiting. After reviewing the literature we would like to use the acupressure P6 wrist band to solve this problem as the findings of our literature review confirm that the acupressure P6 wrist band reduces CINV in cancer patients receiving chemotherapy. This result is corroborated by 7 of the articles reviewed.
The National Cancer Institute website supports the finding that acupressure is one of the non-pharmacologic strategies that may be used to manage nausea and vomiting (NCI Dictionary of Cancer Terms). Said (2009) adds that acupressure may offer an inexpensive, convenient, and self-administered intervention for patients on chemotherapy, helping to reduce nausea and vomiting at home on days 2-5 of chemotherapy. Genç and Tan (2014) conclude that the total mean scores for CINV in patients in the experimental group to whom they applied the P6 acupressure wristband were lower compared to patients in the control group over the five days of application. Lee et al. (2008) found that the two acupressure modalities produced variable results in each phase of CINV: acupressure bands were effective in controlling acute nausea, whereas acupressure controlled delayed nausea and vomiting. Molassiotis et al. (2007) showed that the experience of nausea and vomiting was significantly lower in the experimental group than in the control group. Chao et al. (2009) found that P6 acupoint stimulation was an option for the management of CINV. In the study reported by Hughes et al. (2013) the participants perceived that acupressure wristbands reduced the levels of nausea and vomiting experienced during chemotherapy treatment. Suh (2012) concluded that the synergistic effects of P6 acupressure together with nurse-provided counselling appeared to be effective in reducing CINV in patients with breast cancer.
Five of the seven articles investigating breast cancer patients, namely Said (2009), Chao et al.( 2009), Molassiotis et al. (2007), Suh (2012) and Genç and Tan (2014), involved breast cancer patients receiving highly ematogenic chemotherapy (e.g. Cisplatin and cyclophosphamide), and moderate risk ematogenic chemotherapy (like doxorubicin).
It is necessary to mention other therapeutic regimens that can also be used in cancer treatment that contain other types of chemotherapy that cause nausea and vomiting, for example, doxorubicin-containing regimens like ABVD (Adriamycin, Bleomycin, Vinblastine, Dacarbazine), CHOP (Cyclophosphamide, Adriamycin, Vincristine, Prednisone) and FAC (5-Fluorouracil, Adriamycin, Cyclophosphamide), and ACT (Adriamycin, Cyclophosphamide, Taxol) (Said 2009) and from our experience cisplatin-containing regimens which that classified as highly ematogenic chemotherapy we noticed the patients still experienced nausea and vomiting after they received the antiemitecs. We think it is necessary to use additional intervention like acupressure to be included in the nausea and vomiting management.
Based on the reviewed findings we plan to use acupressure for cancer patients receiving chemotherapy, because the acupressure in the studies conducted in breast cancer patients reported was used with highly ematogenic chemotherapy in addition to the standard antiemetic treatment, so it is reasonable to conclude that it will work equally well with other less ematogenic types of chemotherapy.
We prefer the use of the acupressure wrist band at P6 acupoint because it is an inexpensive, convenient, and self-administered intervention involving pressure instead of needles at the same point as that used in acupuncture. Furthermore it is safer than acupuncture and patients can easily learn to put pressure on their own wrists, whereas the acupuncture involves using needles that are about the diameter of a hair and can cause temporary discomfort during insertion (Said 2009; Molassiotis et al. 2007). Acupressure seems to be a good way to complement antiemetic pharmacotherapy as it is safe and convenient, with minimal (with bands) or no (finger acupressure) costs involved. It is thus an easy to use, cost-effective, non-invasive intervention (Lee et al. 2008; Melchart et al. 2006).
There was no study result that showed any negative effect from the acupressure wrist band at P6 point, except the review by Lee et al. (2008), which mentioned that three of the ten reported acupressure band trials did not support the possible positive effects of acupressure, but these studies all had methodological issues, such as a small sample size, no true control group, and a concern about the sham acupressure band having a possible antiemetic effect. Melchart et al. (2006) said that no difference was detected in the nausea score between the acupuncture treatment at P6 acupoint, and that at the sham point. Said (2009) mentioned that the acupressure showed no benefit in relation to the incidence of delayed vomiting, early vomiting, or acute nausea, but Melchart and Said’s studies were done with breast cancer patients and it could be that the acupressure benefits were not evident due to the breast cancer patients having had axillary lymph node resection that may have affected the meridian pathway or caused damage to the median nerve as mentioned by Roscoe et al. (2003). Consequently, we think that the evidence suggesting that there is no benefit from the acupressure method for reducing CINV is weak.
Regarding the placebo effect in the articles reviewed here, Melchart et al. (2006) indicated that there was no difference in the nausea score for the combined acupuncture treatment at p6 or that at the sham point, although the level of nausea was very low in both cases. Molassiotis et al. (2007), Said (2009) and Roscoe et al. (2003) all suggested that the placebo effect may be the result of psychological factors.
Application of acupressure in clinical practice
It is important to put this theory into practice, and health care professionals could consider using APS, in particular acupressure on the P6 acupoint, as an option in the management of CINV (Chao et al. 2009). Melchart et al. (2006) said acupressure bands can easily be used in busy oncological wards, while Suh (2012) supported the use of P6 acupressure with counselling focused on cognitive awareness, affective readiness, symptom acceptance, and the use of available resources as an adjunct to antiemetic medications for the control of CINV. Hughes et al. (2013) concluded that the research provides an insight into cancer patients’ motivations for and experiences of taking part in a clinical trial for a complementary alternative medical intervention in which the participants perceived the acupressure wristbands as reducing their level of CINV. Said (2009) suggests that oncology nurses should include acupressure in their list of options for the management of CINV, and especially delayed nausea and vomiting. Special recommendations by oncology nurses are not only useful but are also much appreciated by patients as shown in a study in which the patients were satisfied with the antiemetic treatment given by both P6-acupressure, and placebo-acupressure. The percentage of patients who were satisfied (≥ 3 on 0-6 scale) with their treatment was 81% (35/42) in the P6-acupressure group, which was in agreement with Roscoe et al. (2003), and 64% (27/42) in the placebo group (p= 0.0471). The percentage of the patients who would recommend acupressure treatment was 79% (34/42) in the P6-acupressure group, which again was in agreement with the results of Roscoe et al. (2003) and Hughes et al. (2013), compared to 62% (26/42) in the placebo group (p= 0.0533). This study presented the patients’ compliance with the use of acupressure. Acupressure is easily learnt and taught and patients should be informed about its potential role and taught how to apply it. Leaflets about acupressure for the management of nausea and vomiting could be available in chemotherapy units so that patients who are interested to use such a technique would be encouraged to come forward and learn more from nurses or other health professionals. This could add to the patients’ options for antiemetic approaches and empower them to be involved in the management of these distressing side effects. Acupressure offers a no-cost, convenient, self-administered intervention for chemotherapy patients to reduce acute nausea. Acupressure devices (i.e. Wrist Bands, travel bands, and acupressure bands) have been developed to provide passive acupressure on P6. Acupressure can be administered by healthcare providers, family members, or patients themselves, and does not involve puncture of the skin.
We therefore found that the acupressure wristband is a good way to reduce nausea and vomiting for cancer patients receiving chemotherapy by applying it in the correct position with the stud over the pericardium 6 acupoint located on the anterior surface of the forearm, 3-finger widths up from the first wrist crease, and between the tendons of flexor carpiradialis and Palmaris longus.
Lee et al. (2008) encourage the application of acupressure bilaterally, rather than unilaterally, in CINV control. They recommend three minutes of finger acupressure once daily, with additional acupressure as needed, as the optimal intervention, because both three and five minute trials have succeeded in achieving positive effects. On the other hand, Molassiotis et al. (2007) claimed that there is no correlation between the frequency of pressing the studs and the level of nausea and vomiting. Lee et al. (2008) and Molassiotis et al. (2007) therefore claim opposite results in the relationship between CINV and the frequency of pressing the stud of an acupressure P6 wrist band. But when applying the acupressure P6 wrist band bilaterally, Lee et al. (2008), Said (2009), Molassiotis et al. (2007), Suh (2012), and Genç and Tan (2014) all reported a positive effect with P6 stimulation in reducing CINV.
We would like to discuss some factors related to CINV in relation to nausea and vomiting: expectancy and gender: Roscoe et al. (2003) argued that patients who received the acustimulation bands and expected them to be effective did report having a higher quality of life and less nausea, and in relation to gender, that women are more likely to experience nausea when receiving chemotherapy. Lee et al. (2008) say this may be caused by classical conditioning and also that breast cancer patients may have had a damaged median nerve due to axillary lymph node removal, but Lee et al. (2008) also mention that P6 acupressure in younger women had a significantly greater positive effect on delayed nausea than those on a placebo or those in the no-intervention control group. On the other hand, Molassiotis et al. (2007) mentioned that younger age is associated with greater nausea. We think that men may have tolerated greater stimulation of the acupressure points, and therefore experienced greater symptom relief, so it may be that the acupressure is more effective for men than for women, but these questions of gender, age and the frequency of pressing the studs would need further investigation.
Based on the reported studies, we support the belief that acupressure on P6 is applicable in clinical practice for CINV for cancer patients provided the required education, training and counselling is given to maintain the acupressure benefits.
Acupressure side effects
The study by Molassiotis et al. (2007) found that there were no side effects from the use of the wristbands, but one patient reported that she had to take the bands off because they were too tight and left her with marks for a few days. Chao et al. (2009) also mentioned that very few minor adverse events were observed.
Melchart et al. (2006) did report adverse effects from the treatment in five cases. One suffered a hematoma when wearing the acupressure band at P6. In the sham group, one hematoma was reported after acupuncture, and another three adverse effects from the acupressure band were reported (one hematoma, one skin irritation, one eczema). Hughes et al. (2013) also reported that participants had not experienced any restrictions from wearing the wristbands in terms of everyday activities, other than when washing and bathing. As one female participant commented, for most participants the wristbands were found to be comfortable to wear. However, a few participants reported that they had experienced minor irritation, such as the wristbands feeling tight or painful, or their wrists becoming itchy. Reported adverse side effects were generally deemed minor and acceptable. In the study by Said (2009), no side effect or discomfort was noticed from wearing the acupressure wristband. Said told the patients that if the bands caused discomfort, they could be removed for 30 minutes every two hours. In this way, by taking it off for regular periods, we can prevent the side effects of acupressure, even its minor and rare effects.
Acupressure reduces CINV in cancer patients, in addition it reduces anxiety (Genç and Tan 2014) and that affects overall quality of life (Said 2009). Quality of life is defined by the NCI Dictionary of Cancer Terms as “The overall enjoyment of life and the individual’s sense of well-being and ability to carry out various activities”. Based on the physiological components of the Virginia Henderson’s theory of basic human needs and Abraham Maslow’s Hierarchy of Needs, the patient needs to eat and drink adequately, and sleep and rest (Vera, 2014). This means that when we are providing the required management for distressing symptoms, such as nausea and vomiting, by including the acupressure wrist band in addition to standard antiemetics, the patient’s appetite will improve, leading the patient to eat and drink adequately and improve their sleeping pattern. These may then also improve other aspects of the cancer patient’s life. According to the Henderson Nursing Need Theory, when we meet a patient’s needs, it results in an improved quality of life for the cancer patient receiving chemotherapy. Another way of expressing this is that it restores the balance of Yin and Yang energy that leads to reduced nausea and vomiting and improves the patient’s ability to enjoy life and work in general through a maintaining of the harmony of body and mind, as described in traditional Chinese medicine (Cancer Research UK, 2015).
We believe that it is essential for cancer patients undergoing chemotherapy treatment to have adequate nutrition to maintain their strength to fight the cancer. Different nursing actions are necessary to maintain adequate nutrition including the relieving of CINV. From this we extrapolate that using the acupressure P6 wrist band to reduce CINV improves the patient’s quality of life.
CONCLUSION
Chemotherapy-induced nausea and vomiting may be life threatening and is therefore a huge challenge to nurses involved in cancer care. Even with the best pharmacological management of CINV, patients continue to experience nausea and vomiting.
From a review of eight articles with strong methodology, seven supported the positive effect of an acupressure P6 wristband in reducing CINV for cancer patients. This was also supported by other databases. The one article with neutral results showed that there was no difference between a combined acupuncture and acupressure treatment at P6 and at a sham point in relation to the nausea score, but the level of nausea was very low in both groups. We conclude that the acupressure wrist band applied to acupuncture point P6 is effective, safe, convenient, cost effective, an easy and self-administrated non-pharmacological intervention from traditional Chinese medicine that reduces CINV. Solving the problem of CINV is a fundamental nursing task that can lead to improved quality of life and nutritional status, reduced anxiety and increases patient compliance. In the light of these results, and due to the effectiveness and inexpensiveness of acupressure, together with its ease of use, we suggest that it should be used in conjunction with pharmacological agents for CINV prophylaxis. To maintain the effectiveness of the acupressure, special education and training is needed to reassure the patient that the acupressure is at the correct point (P6) and counselling by the nurse is required.
We recommend the use of acupressure P6 in oncology departments and that future research should be conducted to include cancer patients receiving radiotherapy, and to investigate more about the relationship between the frequency of pressing the stud on the wrist band for acupressure P6 and CINV, and the relationship between gender and CINV, and whether it is better to apply it unilaterally or bilaterally.
For more information: https://jmedcasereportsimages.org/about-us/
For more submission : https://jmedcasereportsimages.org/
#Acupressure#Chemotherapy#Nausea and Vomiting#Cancer patients#Chemotherapy-induced nausea and vomiting#NCI#PICO#CINV#Mustargen#Zanosar#Platinol#Cytoxan#BiCNU#DTIC-Dome#Maher Battat#jcrmhs
4 notes
·
View notes
Text
Tw: gore, cancer, sickness, body horror
I feel the cancer today, but i do not see it. It crushed my chest so I cannot breathe or speak. Carving the scares back open, my soul in agony, but it is a show for one.
It traces the devastation in invisible ink and jams the black light into my eye so I am blinded by blood only I can see. Everyone is ecstatic about its vanishing act but I’m left with the solution that ruins its grandeur.
Behind the curtain it is slowly ripping my hair out by the handful. It is breaking my teeth, cracking my lips, drinking from the iv pole that saved my life by killing me. I am bald. Weak. Dying. I am suffering by its needle fingers as I watch screaming for help and all I hear are the whispers of those who tried to play it’s game and lost
“I can’t watch..” “are you sure you want to continue treatment?” “God I could never do chemo.” “Please I know you’re tired just do this for me please…”
It’s already twisted face forms over and over again to the ones who left. Lovers. Family. Friends. My youth, my fucking life.
And I am left in a pile of congratulations and confetti. I am left with people sobbing in relief and smiles. And I am left with the ghost of cancer haunting the party I never should’ve had to have in the first place.
5 notes
·
View notes
Text
sorry i havent been on. im so tired lately cuz chemo's almost every day now, but its workin again, so thats good! doctors predict i'll be able to go home for christmas! good progress for someone who's supposed to be dead, huh? December 2022. holy cow. never thought i'd make it this far, but here i am, on my way to 2023. i love you guys, keep fighting, its so worth it.
#age regression#agere#sfw agere#little space#agerespace#agere positivity#sfw age regression#age regressor#agere blog#cancer tw#cancer under 50#cancer patients#cancer latest updates
4 notes
·
View notes
Last Seen Blogs

joy-the-poet
joy-the-poet

commissaire-maigret
Le commissaire Maigret

imarvelatthestars
on hiatus

jauhri
Jauhri

soberboyandthepuritans
here lies