#trans suicide
Text
CW discussion of a high publicity trans suicide from 8 years ago, I'll be tagging this obv but want to say off the bat that this may be a tough read - I'm not exactly sure what I want to say.
I've been thinking a lot about Leelah Alcorn lately. She would've been 24 this year - only a year older than myself - and it's been almost 8 years since her suicide. I won't ever forget her, I don't know how anyone who was around at the time could.
If you weren't on tumblr/the internet in general at the time, it's probably hard to conceptualise how... big it was. How many people were talking about this one trans girl's suicide. Reading her note, published on her blog via the queue function. Seeing all the pain, and outrage, art and activism happening all at once. Being a young trans kid who was only beginning to unpack their own gender, and wondering if it was worth it. Feeling hurt and outraged in ways you couldn't quite articulate. That was my experience, anyway.
To be honest, it was scary. After the initial flood of conversation, discourse, tributes, I kind of... locked it away, for a while. Tried not to think about it. It was morbid and terrifying and I didn't have anyone I could actually talk to about it. It's not like my parents knew what was happening in the 2014 tumblr trans community. It's not like I could've explained it, or how it was making me feel.
But at the same time as terrifying me, it incensed me. How dare her parents let this happen, and refuse to respect her even after her death? And so many people felt the same. This was a community boiling over with rage and hurt, in a way I had certainly never seen before. People came to Leelah's defence, told the bastards we will say her name, we will remember her, we will honour her. And she has been honoured. Her name has been spoken, so many times, by so many people. People were screaming, we love you, we love you, we love you, and we're sorry. And fuck, that was powerful. At such a formative time in my personal political growth, trans unity like this was powerful.
I've been thinking a lot about Leelah Alcorn lately. I never knew her, and I don't even know if I would have liked her. I wish I had the chance to find out. But I remember her. Her name is etched into a corner of my soul.
I'm not sure if I have a point, or how to end this. But just... remember her, if you can.
128 notes
·
View notes
Text

Goodbye everyone. To my family and friends, I'm sorry, but this is the only way.
4 notes
·
View notes
Text
“You just looked so much better as a girl!”
well Susan I wanted to kill myself every time I looked in the mirror and this is the first time I’ve ever felt comfortable in my own body so I think my opinion matters a little more in this situation
#tw suicide mention#Suicide mention#trans suicide#trans#Transgender#trans ftm#trans man#trans masc#trans masc non binary#Afab
8 notes
·
View notes
Link
By: Scott Newgent
Published: Oct 6, 2020
At a recent gathering, a daughter’s friend told us, “I’m probably trans because I don’t like female puberty.” This instantly got my attention, because I have known this child for years, and I never saw any indication of her being trans. I innocently asked her why she would say that. Was it a joke, perhaps? She replied, “I don’t like my boobs growing, and Reddit says I’m probably trans.”
That night, I tracked down these Reddit exchanges, and my jaw dropped when I saw how many people and organizations were heavily pushing the possibility of her being trans. But perhaps I shouldn’t have been surprised, given the way such attitudes have gone mainstream. This includes the pediatrician mom whose recent opinion piece for the New York Times was titled What I Learned as the Parent of a Transgender Child. For kids Googling this subject, the overall effect is the equivalent of one big glitter bomb going off on their screen.
I write all this as a 47-year-old transgender man who transitioned five years ago. I’m also a parent to three teenagers. Though I admire the good intentions of parents who seek to support their children, I have serious concerns about reckless acquiescence to a child’s Internet-mediated self-diagnosis. Many older transgender folks share these concerns, too. In many cases, we are people who have been quietly going about our lives in society for years, anonymously sharing shops, offices, elevators, and sidewalks with everyone else, without making a big deal of our identity or proselytizing to others. We like it that way. But given the current climate, we now need to speak out.
That one comment by my daughter’s friend caused me to investigate the organizations that purport to advocate on behalf of the trans community. I found that they typically push an approach based on quickly and enthusiastically affirming any indication of gender dysphoria. As someone who is trans myself, I know that this is the wrong approach. Yes, some children who say they are trans really will need to transition one day, because they have a lifelong condition. But parents who automatically assume that this is the case with their child aren’t necessarily following the child’s best interests.
Transgenderism isn’t a vague feeling, or a distaste for stereotypical roles. It’s a serious internal condition that causes you to want to become the opposite sex. Medical transition, such as the kind I went through, can enhance an illusion that helps some gender dysphoric individuals navigate the world with more comfort. It did for me, and it was the right path for me to choose.
I wasn’t “born in the wrong body.” I was born female. But I didn’t like it. So I changed my appearance, at significant monetary, psychological, and physical cost, with plastic surgery and hormones. My sex never changed, though. Only my appearance changed.
Anyone going through this is in store for a brutal process. Yet we now have thousands of naïve parents walking their children into gender-treatment centers, often based on Internet-peddled narratives that present the transition experience through a gauzy rainbow lens. Many transition therapies are still in an experimental phase—as you will learn if you become sick during or after these treatments.
During my own transition, I had seven surgeries. I also had a massive pulmonary embolism, a helicopter life-flight ride, an emergency ambulance ride, a stress-induced heart attack, sepsis, a 17-month recurring infection due to using the wrong skin during a (failed) phalloplasty, 16 rounds of antibiotics, three weeks of daily IV antibiotics, the loss of all my hair, (only partially successful) arm reconstructive surgery, permanent lung and heart damage, a cut bladder, insomnia-induced hallucinations—oh and frequent loss of consciousness due to pain from the hair on the inside of my urethra. All this led to a form of PTSD that made me a prisoner in my apartment for a year. Between me and my insurance company, medical expenses exceeded $900,000.
During these 17 months of agony, I couldn’t get a urologist to help me. They didn’t feel comfortable taking me on as a patient—since the phalloplasty, like much of the transition process, is experimental. “Could you go back to the original surgeon?” they suggested.
Whenever you question the maximalist activist line on trans affirmation, you are directed to The World Professional Association for Transgender Health (or WPATH) as a reference. But much of what you find there consists of vague phrases such as “up to doctor’s discretion.” Several lawyers suggested I had a slam-dunk medical-malpractice case—until they realized that trans health doesn’t really have a justiciable baseline. As a result, treatment often is subpar, as I have experienced first-hand.
Lupron, the hormone blocker some doctors seem intent on giving to kids like Tylenol, isn’t even FDA-approved to treat children with gender dysphoria. (In 2001, the manufacturer pled guilty to fraudulent sales practices with regard to its marketing as a prostate-cancer drug.) We don’t yet know its long-term effects off-label, despite the fact parents have been assured that its effects are safe and even reversible.
Here is what we do know: The long-term use of synthetic hormone therapy shortens lives. Specifically, these medications are associated with an increased risk of heart attacks, pulmonary embolisms, bone damage, liver and kidney failure, mental-health complications, and more. Almost a quarter of hormone-therapy patients on high-dose anabolic steroids (such as the testosterone taken by female-to-male transitioners) exhibit major mood-syndrome symptoms. Between three and 12 percent go on to develop symptoms of psychosis.
Children who claim to be trans typically are receiving such drugs at a pivotal time in the development of brains and bones. They’ve become a generation of guinea pigs, to answer such questions as: What will happen to a biological boy who takes sex hormones associated with the opposite sex (or vice versa), and grows up without the benefit of natural puberty? What happens to a male body on estrogen over the long term? No one knows.
In regard to the emotional effects of transition, many activists will refer you to a 2018 Pediatrics journal article entitled “Transgender Adolescent Suicide Behavior.” But the study reported therein was based on just three years of data—collected between 2012 and 2015. What matters is the long term. And in this regard, the gold standard is a study of 324 medically transitioned adults, based on 30-year longitudinal data. The authors found that completing sex-reassignment surgery was associated with “considerably higher risks for mortality, suicidal behaviour, and psychiatric morbidity” as compared to the general population. Kids who are suicidal before their transition will likely continue to be suicidal, and the most intense ideation often comes years after transitioning. (Transgender folks themselves sometimes speak anecdotally of a seven-to-10-year trans suicide “itch” observed within the community.)
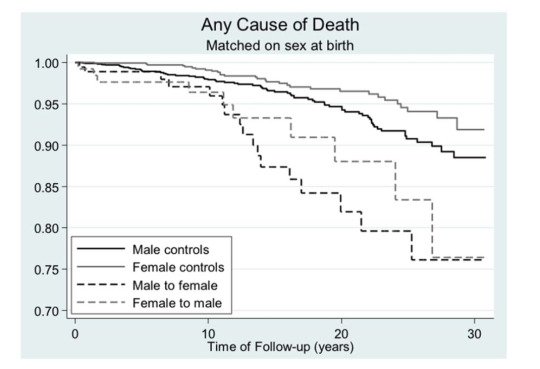
[ Death from any cause as a function of time after sex reassignment among 324 transsexual persons in Sweden. Source: NCBI. ]
None of this is information that radicalized trans activists seek to publicize. In 2019, they trumpeted an article entitled Reduction in Mental Health Treatment Utilization Among Transgender Individuals After Gender-Affirming Surgeries, published in the American Journal of Psychiatry, which purported to show the benefits of transition. When the same authors came back in August 2020 to admit that their data actually didn’t show any significant benefit from transition, few bothered to report the correction.
I have observed that when any argument is raised against a policy of no-questions-asked affirmation, activists seek to pre-empt discussion of the actual data by instead summoning up the specter of suicide—some version of “I would rather have a live daughter than a dead son.” Terrified parents are made to feel as if any expression of concern or skepticism is a gateway to the grave. It’s a passive aggressive form of emotional terrorism.
From my own experience, and from countless conversations with my transgender friends, I can report that most of us regret at least some—though maybe not all—parts of our transition. Even for those who transition successfully, finding peace has stages and takes time. At first, everything is new and exciting. Then, as the years go on, reality sets in, and you have to face up to the reality of biological sex, not to mention the health issues. This is not a life of glitter bombs.
The UK seems to be further ahead than North America in coming to understand that treatment decisions are happening too fast. The National Health Service (NHS) recently changed its stance on medically transitioning children, from presumed approval to a more cautious approach, even warning parents (accurately) that it is “not known whether hormone blockers affect the development of the teenage brain or children’s bones.” The NHS also notes that “most treatments offered at this stage are psychological rather than medical. This is because in many cases gender variant behaviour or feelings disappear as children reach puberty.” Perhaps the law suits are causing people to wake up. “I should have been challenged on the proposals or the claims that I was making for myself,” reports one British plaintiff. “And I think that would have made a big difference as well. If I was just challenged.”
As someone who has experienced medical transition first-hand, I am convinced that it’s better to err on the side on discretion, and leave life-altering decisions to adults who have the benefit of a fully developed brain. The next time my daughter’s friend, or any child, comes to me for advice on their gender dysphoria, here’s what I’d tell them: “There are people who need to medically transition to walk peacefully through their lives, and you, kiddo, might be that person. But, right now, you are a child, and your body is developing everything you need to be a healthy, happy, strong adult. When you grow up, you get to decide about your life.”
For parents, I would say this: It is simply not your right or duty to decide to medically transition your child. Remove that burden from your mind. Medical transition is for adults. The negatives associated with medical transition are vast, and you won’t be the one who lives with the consequences. It will be your child. If your child tells you they will kill themselves if you do not allow them to medically transition (perhaps following a script he or she is provided on Reddit or Tumblr), take them to the hospital so they can be treated for suicidal ideation. Suicidal ideation and seeking transition are separate issues, so separate them.
We talk a lot about oppression and marginalization. Well, I’m one of the people who’s been oppressed and marginalized—more so now that I have outed myself so that I can try to help others. The least you can do is pay attention to my message.
#Scott Newgent#gender ideology#queer theory#gender transition#medical transition#gender pseudoscience#gender dysphoria#social contagion#mass psychogenic illness#biological sex#medical malpractice#biological dimorphism#dimorphism#trans suicide#wokeness as religion#cult of woke#woke activism#wokeism#woke#religion is a mental illness
68 notes
·
View notes
Text
[tw su*c*de mention]
My evil trans agenda is making sure my trans little brother doesn't kill himself
#trans#im a trans man and so is my brother#he actually came out before i did#anti trans bills#kansas#im so afraid#tw suicice#su*c*de#trans suicide
9 notes
·
View notes
Text
I'm really sad today. I have a lot of trans people in my life (best friend, brother, cousin, some other friends and people ive known casually, i dont have a problem with trans people obviously). So a while ago there was this news about my dad's half sibling transitioning from male to female. I never saw that person again and kind of wondered why. Well I found out today it's because my trans aunt did not want to go to a therapist first and went out of state and got bottom surgery and then shortly after killed herself. Trans medicalization is transphobic and can be extremely damaging to the mental and physical health of trans people. If you really love trans people you should want better for them. They deserve more than this. Obviously gender affirming surgery is beneficial for some trans people who HAVE NO OTHER ALTERNATIVE TO DEAL WITH IT, but I think we also need to normalize trans people who don't want to medically transition or get surgeries. If we really want to destroy the gender binary then we need to detach ourselves from this idea of gender equalling sex. It's harmful and actually contributes more to trans people's dysphoria in some cases. Treating trans people like they have to medically transition to be valid as trans is transphobic and sexist in my opinion.
Maybe this will make some people mad, but I ask you why it makes you angry to want trans people to be happy and alive and to care more about them and their issues. I would ask you why it makes you mad when I say a trans person shouldn't have to change their body to be affirmed as a certain gender.
#personal#tw death#trans death#death of a trans person#trans suicide#trigger warning#tw#death#suicide#trans
1 note
·
View note
Text
When I was a very suicidal trans activist in Texas, Benjamin Sisko saying “sure, you would [die for your people]. Dying gets you off the hook. The question is: are you willing to live for your people?” changed and possibly saved my life. It’s up there with “if we are going to be damned, let us be damned for who we really are” from Picard. Star Trek not only shows us a better world, it teaches us how to make it there
14K notes
·
View notes
Text


All the links to the above charities here.
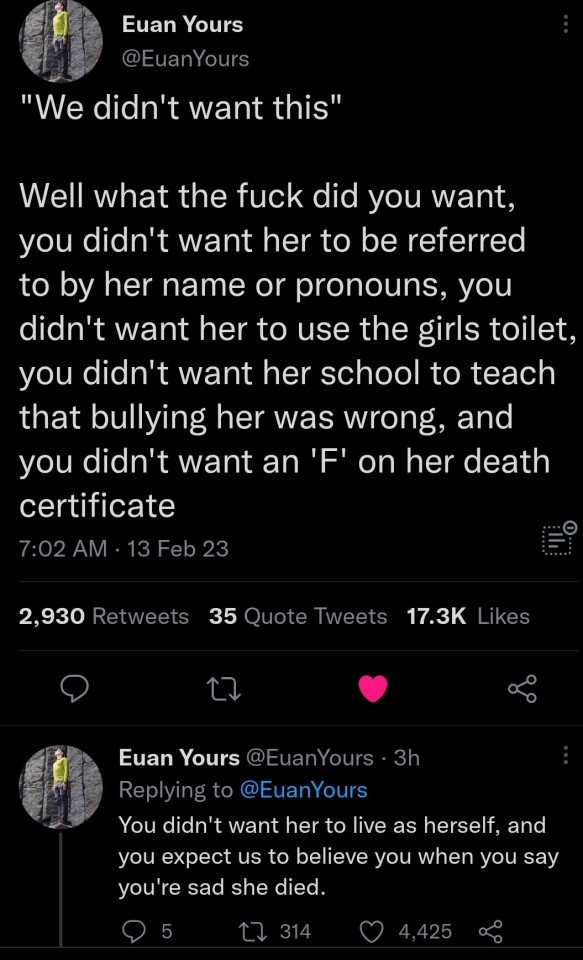
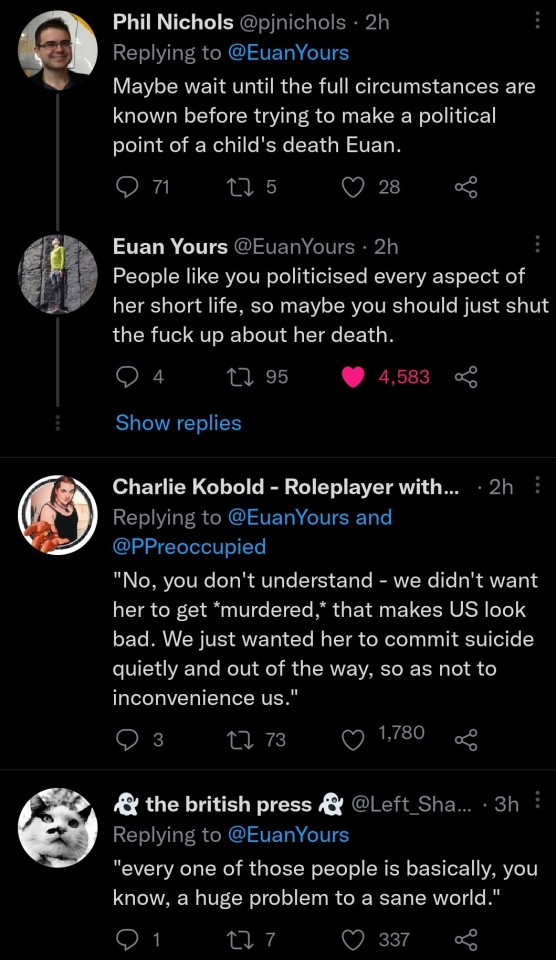
Brianna Ghey's family:
STA:
Gallop:
Mermaids:
GI:
#twitter#trans rights#lgbt#tw suicide#brianna ghey#transgender#fuck the gender critical movement#pieces of shit
13K notes
·
View notes
Text
A closeted person, forcibly outed as having a trans online persona by a "conservative news site," died by suicide after being publicly ridiculed after the outing.
Then, the head of that "news site" sent condolences to Bubba's "victims and family."
There aren't any victims, of course, because the clothing you wear in private and the fiction you write isn't anybody's business, but it's important to understand that these people really do think that trans people have "victims" bc we are somehow hurting people just by existing.
Do not add any kind of transphobic or anti-closet rhetoric to this post.
Turns out there were plenty of good reasons for him to stay closeted, nu? Show his memory the same grace and gentleness you'd want shown to someone you love.
3K notes
·
View notes
Text
What'd'y'all think should I join the 40%?
1 note
·
View note
Text
If I can take a moment to share my experience as a trans woman on the internet
My experience is by no means unique, it's just one experience in the plethora of trans feminine experiences and not unique to only tumblr. Though, I'll mostly talk about what I've experienced here. In the light of recent events, the reaction of "the ceo," and the comments he contributed regarding dog pile harassment; I simply wish to share my experiences that I have had to juxtapose the dynamic of his statements against a lived experience.
This account started as a way to document my social transition and eventually my journey with HRT. Tumblr had always had a large lgbtqia+ community. The queer people here inspired me and gave me hope. What I didn't know, but soon learned, is that there were people here who hated me for being trans. Being early in my transition I was a prime target. TERF groups would plan raids on my account. What this entailed was: rebloging my selfies into circles that would say the most vile things about me, threaten to kill, tell me I was ugly, tell me that everyone I knew thought I was a joke, I was a monster, my family hated me, that I should kill myself, they'd download and edit my photos into caricatures or depictions of violence. They would fill my ask box with hundreds of asks detailing how they'd kill me, call me slurs, describe the ways that I should kill myself, and pretty much everything else I mentioned above with the reblogs. Their words were carefully curated to try and break me, break my spirit, break my will to live. I tried reporting it. But it was impossible to keep up with, and like many others I saw no real response. Eventually I learned that I had to block all of them. 100's of blogs, eventually 1000's of blogs. My block list these days is incredibly extensive. I had to wade through their blogs, traverse sickening hate speech and imagery to eliminate entire circles of people harassing me. I became jaded to the hate speech, hardened to it. But mind you, I shouldn't have had to expose myself to all of this just to be at peace here amongst my community. I received no help, I was left to my own devices to protect myself. The people who hurt me never saw consequences. It was painful, it was unfair, and no one else should have to put the hours upon hours of effort and exposure to hate in to protect themselves like I did. But again my experience is not unique.
I have had to repeat this process of preemptive blocking periodically once a new circle discovers me. Blocking them all before they can start the process of hate all over again. A process of hate that seems to be hitting my community with rapidly increasing fervor as of late.
I've seen others experience far worse than me. The TERF circles will hunt down their personal information and doxx them. Expose their home address, telephone numbers, names of their family members. I can't begin to imagine the terror my queer siblings must feel when someone tells then that they want to murder them all while showing them that they know where you live. This is not a new thing, not a rare tactic, it happens. And we've all seen the news stories of trans people being murdered by people who planned it and were vocal about it.
I know this is depressing. And it doesn't reflect all of my experiences. I've had wonderful experiences here, met amazing people, made close friends, found inspiration, found hope. I found a community.
And it's my community, and I never want to let it go.
I do have fear that making this statement will get me banned. But, I wanted to say it. I wanted it to exist in the world so that everyone who doesn't know our experiences has a chance to understand and with luck empathize.
I'll part on these words and hope for the best both for myself and for every member of the community.
#transgender#transisbeautiful#trans#trans is beautiful#this is what trans looks like#okay to rebagel#trigger warning: transphobia#potentially triggering#trigger warning#trigger warning: description of harassment#trigger warning: description of violent harassment#trigger warning: description of suicide bating harassment#stay hopeful#stay strong#trans community#queer community#lgbtq community#spread love in the community and build each other up
420 notes
·
View notes
Text
About to fall asleep ramble time, this has been kicking around in my brain for a bit and I need to get some form of this thought out
I was diagnosed with ADHD and gender dysphoria one day after the other back in August. Extremely stereotypically zillenial of me, I know. Handling both of these has dramatically improved my quality of life. yes yes insert discourse about how much you need to have dysphoria as a diagnosis, it's just a tool for the medical system that's ultimately meaningless, that's not what this is about.
There's one thing that was really, really weird about the experience of getting care for both of these.
Most treatment and public talk of transition and motivations to transition are about misery. How much despair your birth sex gives you and how gender affirming care is the only stopgap against suicide (oftentimes, used as a barrier to entry that it should only be given when it's at the suicidal point). How crushing dysphoria is.
In contrast, most of the public perception of ADHD is this cutesy, "omg look I'm so quirky" kind of thing. People talk of ADHD "superpowers" and how neat it is to have hyperfixations (I'm low key starting to dislike that word, even though it's an accurate description of many things- it's very overused).
My actual experience has been almost exactly the opposite.
I absolutely had gender dysphoria, and still do, and misery associated with being AMAB. But is that what defines my trans experience? No, and in fact, it feels like a more incidental blip in it. My trans experience has mostly been defined by joy, by feeling my mind and body slowly make me more and more content with my default existence day after day. And the exploration of it all! The social roles, the romantic dynamics, the friendship dynamics, even small aesthetics like clothes and makeup, and again, the body and mood changes. It's incredible and it brings me joy so much of the time. That, more than anything, has defined my trans experience.
In contrast.... ADHD has objectively made nearly every aspect of my life more miserable. Working with my therapist and my pysch, as well as feeling what it's like to be properly medicated, have shown me extremely well how much the constant feelings of misery I always seemed to have were caused by ADHD. ADHD means being unable to receive a baseline level of dopamine to function under normal circumstances, so your brain starts looking for any way it can get new sources. And wouldn't ya know it, novel stimuli are a perfect way to do that. Keep in mind that dopamine isn't just "the pleasure molecule" it's a neurotransmitter with a broad range of functions. If you don't have ADHD, or even if you do, I want you to think about how miserable of an existence that is. Your default state is depression and inability to do things. It has been for me for most of my life. Additionally, anxieties creep into your head and distract you far more easily. You're less functional. You can't do simple things most of the time. You're distracted and have anxiety spikes easily. Continuous tasks are hard. And day in, day out... You are miserable. Almost constantly.
Oh also, you're easily addicted to extreme novel stimuli. For me, it was self harm. And when that stopped working... Well, I was in a state of mostly background depression that was only punctuated by spikes of massive, overwhelming anxiety that my brain hooked itself on. At a certain point, I just wanted it to end, by any means necessary.
It's been almost ten years since that day, and at this point I can genuinely say that I'm glad I'm still here.
But it wasn't dysphoria that did that (it contributed a bit, but still wasn't the biggest factor). Or a depressive disorder. Or bipolar. Or whatever the big, more "scary" mental illnesses or neurodivergencies are. They tried to treat me for some of them, and it ended horribly. My symptoms fit mixed presentation ADHD perfectly, including my physiological response to stimulants. They don't fit anything else. I likely don't have any strong comorbidities, unless you count the symptom-level anxiety and depression. ADHD did all of that to me. The "cute and quirky" one.
By the time I got around to a diagnosis, my pysch was astounded that I made it as far as I did with symptoms as severe as mine. Tackling ADHD has removed so much misery from my life, it's indescribable. Adderall has been the only thing that has ever actually gotten rid of my constant anxiety.
It's not fucking cute. Keeping with this being the flip side to my dysphoria, I do try to keep it light most of the time, and I join in on all of the classic "whoopsie doopsie my ADHD" trains and jokes. You don't have to stop making those, hell, they're fun. There are cute and funny parts to having ADHD, and ways it's made my personality what it is. But don't forget that this is also something that makes people genuinely suffer well beyond the "oopsie I'm such a procrastinator!!!" Type thing.
Idk where this thought is going. It's just kind of an observation that's been kicking around in my head for a bit. So uh. Hope it at least generates discussion? Feel free to add your experiences if you think it'll help you. But fuck I need to sleep lol
342 notes
·
View notes
Text
youtube
Watch the American Climate Leadership Awards 2024 now: https://youtu.be/bWiW4Rp8vF0?feature=shared
The American Climate Leadership Awards 2024 broadcast recording is now available on ecoAmerica's YouTube channel for viewers to be inspired by active climate leaders. Watch to find out which finalist received the $50,000 grand prize! Hosted by Vanessa Hauc and featuring Bill McKibben and Katharine Hayhoe!
#ACLA24#ACLA24Leaders#youtube#youtube video#climate leaders#climate solutions#climate action#climate and environment#climate#climate change#climate and health#climate blog#climate justice#climate news#weather and climate#environmental news#environment#environmental awareness#environment and health#environmental#environmental issues#environmental justice#environment protection#environmental health#Youtube
6K notes
·
View notes
Link
By: Leor Sapir
Published: Jul 20, 2022
In a recent exchange between Senator Josh Hawley (R-MO) and Berkeley Law professor Khiara Bridges on the ramifications of the Supreme Court’s decision to overturn Roe v. Wade, Hawley wanted to know whether the Court’s decision affected women as a class. After initially informing Hawley that not all “cis women” have the “capacity for pregnancy” while some “trans men” and “non-binary” people do, Bridges appeared caught between her loyalties to gender identity ideology and to the long-held idea that abortion is a women’s issue. And so rather than clarify her position, Bridges berated Hawley for his “transphobic” line of questioning, insisting that he and those like him are the reason why “one in five” transgender people attempt suicide.
The affirm-or-suicide mantra has become the central strategy of contemporary transgender activism, and at times it would seem that activists have little else in their rhetorical arsenal. Federal courts have used it to impose new policies on schools under Title IX. When Florida passed the Parental Rights in Education Act—a law that limits classroom discussion of gender identity and sexual orientation to “age appropriate” circumstances and that requires schools to notify parents when their children are being “socially transitioned” to the opposite gender—Secretary of Transportation Pete Buttigieg agreed with his husband Chasten that it would “kill kids.” Florida’s law was in response to, among other things, books like Gender Queer: A Memoir, which contains graphic depictions of oral sex, appearing on school library shelves. The book’s “non-binary” author, Maia Kobabe, countered that her book’s presence in libraries was “life-saving.”
A few weeks later, transgender Assistant Secretary for Health and Human Services Rachel Levine used the same word to justify the federal government’s support for “gender affirming” interventions. Neither Levine nor President Biden, who has given his own imprimatur to the controversial practice, seemed to care much that Europe’s most progressive welfare states have been moving in the opposite direction, placing strict limitations on the use of puberty blockers to treat adolescents in distress presumably because of their “gender.” Scandinavians are not indifferent to teen suicide. Rather, they have examined the evidence behind the affirm-or-suicide claim and have found it wanting.
Despite the unwaveringly confident manner in which these claims are often asserted, there is no good evidence that failing to “affirm” minors in their “gender identity” will increase the likelihood of them committing suicide. As I discuss below, that claim is based on a small handful of deeply flawed studies that, at most, find loose correlations between “affirming” interventions and improved mental health. Some find no reduction of suicide at all, and a new study claims to find that puberty blockers actually increase the risk of suicide.
Not only is the empirical basis for the affirm-or-suicide mantra shoddy at best, but its dissemination is also profoundly irresponsible. Such extreme rhetoric limits our ability to better understand and respond to mental health problems in vulnerable youth, and may itself contribute to the real and documented phenomenon of “suicide contagion.”
* * *
Part of the problem is the vagueness of the term “suicidality.” There is a difference between thinking about suicide, attempting it, and actually doing it. And even within the first two categories, shades of grey prevail. A “suicidal attempt,” for instance, can mean climbing to a roof of a building without actually stepping onto the ledge, but it can also mean surviving a self-inflicted gunshot wound to the head. Women are far more likely to think about and attempt suicide, but men are more likely to die by suicide. Actual suicide is obviously more serious than suicidal attempts, and attempts more than ideation. Human beings may go through periods of depression in which they contemplate suicide, even seriously, but this does not mean that they are at permanent risk for suicide. It’s a messy, dark, and multifaceted topic ill-served by the moral panic-mongering of activists.
Gender activists commonly argue that roughly four in ten transgender-identified youth (TIY) attempt suicide when not socially and medically “affirmed.” Does the research bear this out? The simple answer is: no.
Firstly, surveys of TIY suicidality rely on self-report and do very little to vet respondents when they say they “attempted” suicide. Secondly, studies purporting to show that TIY are at elevated risk of suicide tend to compare suicide rates in TIY with rates in non-TIY—a deeply misleading comparison. This is because TIY, especially among the new clinical cohort of “rapid onset gender dysphoria” (ROGD) teenagers, exhibit extraordinarily high rates of mental health problems (psychological co-morbidities) quite apart from their gender-related distress.
To the extent proponents of the “gender affirming” approach recognize these co-morbidities, they regard them as the product of social hostility and lack of acceptance (though, oddly, they also claim that rapidly rising rates of transgender identification are the result of a society increasingly accepting of transgender identity). Yet no evidence supports this hypothesis and mounting evidence vitiates it. ROGD teens are known to have very high rates of anxiety, depression, history of sexual trauma, anorexia, and eating disorders, all of which typically precede their gender-related distress. And as we’ve learned from detransitioners, many continue to experience these problems long after they have gone under the knife. According to a review of the U.K.’s Gender Identity Development Service, roughly one out of three girls seeking gender transition has autism—a significant finding, considering that “being in the wrong body” might provide these teenagers with a convenient explanation for their social isolation. Regardless, each of these mental health conditions is a known predictor of suicidal behavior.
Thus, while it is true that suicidal behavior is much more likely among TIY, rates of actual suicide are extremely low within the population and there is no basis for believing that “affirming” them with puberty blockers, cross-sex hormones and surgeries will reduce those rates even further. Importantly, when researchers compared TIY with non-TIY with similar mental health profiles, the disparities in suicidal behavior reduced considerably, suggesting that it is not the lack of gender affirmation that seems to be driving suicidal behavior.
The dubious claims about mental health benefits from “gender affirming” medicine, alongside the obvious risks, is why Sweden and Finland have recently moved to restrict the practice, with the U.K. likely to follow suit. It is also why medical authorities in France, Australia and New Zealand have issued strong statements highlighting the uncertainties and experimental nature of “affirming” interventions.
The gold standard for finding a causal relationship between “affirming” medicine and suicide would be the randomized controlled trial (RCT). To date, no RCT has ever been conducted to study the effects of puberty blockers on mental health (including suicidality) of gender-distressed youth. For this reason, the FDA has never approved the use of Lupron or other puberty suppressants for gender dysphoria. Claims about the reversibility of puberty blockers, which are essential to “gender affirming” advocates’ ethical case for allowing children to use them, rely entirely on referencing the drug’s original purpose, which is treating precocious puberty.
As for their safety, the risks of puberty blockers are not fully known but are thought to include cognitive impairment and bone malformation. It is becoming increasingly clear, however, that another major risk is iatrogenesis, meaning that the use of puberty blockers to “treat” gender dysphoria virtually guarantees the persistence of the condition and continuation of the patient to more extreme and risky types of intervention.
At nearly $40,000 per implant, which lasts for one year, these drugs are extraordinarily expensive and a potentially lucrative source of revenue for drug manufacturers. So why not expand the market by getting FDA approval for a new type of use? Considering how ROGD could be a goldmine for drug companies, why not conduct RCTs? One reason is that activists and professional medical organizations already insist puberty blockers are safe and medically necessary interventions. If this is true, then withholding such interventions from minors with gender dysphoria (something required in a controlled experiment) would be unethical and even life-endangering. Another reason is the common (but misguided) belief about reversibility of puberty blockers: once the “pause” button is lifted, the thinking goes, adolescent development can seamlessly pick right back up as if nothing happened.
Authorizing RCTs for puberty blockers would require that activists allow their basic assumptions to be put to the test, but the intrusion of identity politics into medicine makes that unlikely. “Gender affirming” care is premised on the conviction that medical professionals should never steer a patient toward a non-transgender over a transgender outcome, as doing so assumes that transgender identity is abnormal or, at any rate, less preferable than “cisgender” identity. In the United States, identity politics has been framed as “civil rights,” so it is in the name of this venerable tradition and its robust judicial supervisory mechanisms that activists have waged holy war against alternatives to “gender affirming” care such as “watchful waiting” or therapy-only.
In countries without a strong civil rights state, medical rationales for “affirming” interventions can be more easily interrogated and, if necessary, challenged. Sweden, Finland, France and the U.K. have either recognized or are on the verge of recognizing the experimental nature and inherent risks of puberty blockers. Medical authorities in these countries have come under pressure from activists, but due in part to the absence of potent analogies to Jim Crow they have been able to weigh the pros and cons and consider the trade-offs of “affirming” interventions—precisely the kind of considerations that American “rights talk” is designed to make verboten. These countries have “pressed pause,” but on the use of puberty blockers rather than puberty itself.
A 2011 Swedish study found that, even after medical transition, “transsexual” patients were nineteen times more likely to die by suicide than non-transexuals, but the study’s lack of adequate controls makes it difficult to draw any definitive conclusions. It does, however, cast serious doubt on the belief that “gender affirming” interventions are medically necessary measures for preventing suicide. Meanwhile, suicide remains an extremely rare event for TIY, even among the ROGD cohort. Between 2010 and 2020, the U.K.’s Tavistock Clinic recorded four deaths by suicide out of a total of 15,000 patients—and this notwithstanding the two-year waiting period for the clinic’s services.
* * *
At present, the studies purporting to find that puberty suppression in minors leads to reduced suicidality come nowhere near the level of causal determination normally required before approving new drugs or old drugs for new uses. I recommend anyone who hasn’t already done so to read Jesse Singal’s long Substack post on the flaws in these studies and how media tend to overlook them.
Among the serious deficiencies of studies such as those published by psychiatrist and “gender affirming” advocate Jack Turban are reliance on biased samples (the subjects in Turban’s studies were recruited through transgender advocacy and support groups) and non-random assignments of treatment. The latter is especially important: Turban and colleagues compared subjects who wanted hormonal interventions but didn’t receive them to those who wanted and received them. One of the reasons the former but not the latter received these interventions, however, might be because they were already more psychologically stable to begin with. The subjects of Turban’s studies would have been exposed to treatment protocols implemented before the surge in “affirming” therapy, meaning under the more rigorous “Dutch protocol,” which emphasized prescreening for mental health co-morbidities as a precondition for receiving hormones. In short, nothing in Turban’s studies can refute the possibility that improved mental health was the result of something other than medical suppression of puberty.
Here we must note a perennial problem for science in a democratic society, which is that science can neither explain itself to the non-scientific public, nor can it present a self-explanatory plan of political action. Science requires mediators to interpret its findings and make them relevant to contemporary concerns, which are invariably value-laden and often political. Despite acknowledging—if not as forcefully as he should have—within his own study the limitations of his findings, Turban sold his work to an eager media environment as having found strong evidence that puberty blockers are life-saving and medically necessary. And they gobbled it up uncritically.
What makes an RCT reliable as a source of knowledge about causality is the “R.” Before the FDA can approve a new drug, it must have confidence that the reason why some subjects got the drug and benefitted from it while others did not is not some factor related to the positive outcome itself. For example, if an experimental drug for schizophrenia is given only to subjects who are hospitalized and the recipients experience improved mental health, researchers may falsely conclude that it was the drug that caused the improvement when in fact it was the hospital setting where patients were exposed to other therapeutic supports. Ideally, chance (i.e. randomness) alone should determine who gets the drug and who doesn’t.
In the absence of RCTs, and to avoid the pitfalls of studies like those of Turban and colleagues, researchers might try to approximate causality by introducing unrelated criteria for assigning treatments to some subjects but not others. Random chance is the ideal unrelated criterion because, almost by definition, it is the most unrelated to any measurable outcome. Short of that, researchers can seize on second-best proxies for randomness.
That is what Jay Greene, a former university professor who recently joined the Heritage Foundation, did in a new study investigating the causal relationship between puberty blockers and suicide. Greene’s “natural experiment” uses state minor consent rules—that is, laws that permit minors to consent to medical treatment without parental approval—adopted well before and for reasons unrelated to gender dysphoria. For that reason, they are exogenous to the outcome. “Whether adolescents live in a state that imposes fewer or no restrictions on accessing puberty blockers and cross-sex hormones,” Greene explains, “is effectively random and should have nothing to do with later outcomes other than through the mechanism of receiving those interventions or not.” The fact that a blue state like Connecticut lacks a minor access provision and is thus coded as more restrictive for puberty blockers, while red states like Texas and Missouri have such provisions and are coded as more permissive, is not a problem for Greene’s research design, but an advantage. It suggests that Greene has not introduced a confounding criterion for treatment assignment.
Using this admittedly counterintuitive—but in the social sciences, well recognized—research design, Greene finds that puberty blockers actually increase the risk of suicide by 14 percent. It must be emphasized, however, that the causal link here is weak. It comes nowhere close to proving conclusively that puberty blockers increase suicide. Greene’s study is simply less bad than competing studies, including those by Turban and colleagues, which purport to find that blockers reduce suicide.
Now, there is a danger, as the saying goes, in making the perfect the enemy of the good. A political scientist by training, Greene knows that policymakers must often make choices on the basis of imperfect information; policymaking is rarely a choice between good and bad options, but more frequently between bad and worse ones. Faced with weak evidence for the dangers of blockers and even weaker evidence for their therapeutic benefits, a reasonable policymaker would prefer to halt their use pending further research.
When I posted a shortened version of this comparison of Turban and Greene on Twitter, Turban responded that his work, unlike Greene’s, was peer-reviewed and published in a “high-impact” journal (Pediatrics). As Turban surely knows, peer-review may increase the likelihood of a claim being true, but hardly guarantees it. And peer-review is only as good as one’s peers and the degree to which a field hasn’t been captured by fashionable political ideologies. While peer-review remains the most reliable mechanism for sorting science from pseudoscience, it has taken several serious and deserved blows to its reputation over the past few decades.
I’m not even referring to the hoaxing of the so-called “Grievance Studies,” where peer review is often little more than gatekeeping by postmodernist identitarians who cannot distinguish their own research from pure gibberish, or even to the low standards of the law reviews, where reviewers are law school students with little expertise in law (let alone in more substantive areas of scientific inquiry). A recent survey found a spike in the number of peer-reviewed article retractions, most of them “highly cited articles published in high-impact journals.” And of course, the academy has spent the past decades purifying itself of heretics (such as Colin Wright and myself) who might otherwise challenge approved research narratives. In short, even under these ideological conditions peer-review is nothing to scoff at, but to invoke it as proof of concept is either naïve or disingenuous.
Take Pediatrics, the journal of the American Academy of Pediatrics (AAP) that published Turban’s 2020 paper on puberty blockers and suicide. In 2018, Pediatrics published a paper entitled “Ensuring Comprehensive Care and Support for Transgender and Gender-Diverse Children and Adolescents,” by Dr. Jason Rafferty and others. The article contains a shocking number of errors, omissions, and blatant mischaracterizations of the available research on pediatric gender transition, some of them so fundamental and egregious as to suggest bad faith in the authors. The article’s central conclusion—that “gender affirming” medicine is the only ethical and scientifically-grounded approach to treating gender-related distress in youth—is negated by its very own citations, to say nothing of its flawed logic. I recommend Dr. James Cantor’s fact-checking of the AAP paper; it is one of the most thorough and devastating refutations of an academic “study” I have ever read.
Unfortunately, policymakers—including, most recently, a Trump-appointed federal judge—regularly cite the AAP statement and other unsubstantiated statements by American medical organizations as conclusive evidence that the gender-affirming approach is “settled science” and that it saves lives. A faulty peer-review process, it would seem, can be more dangerous than no peer-review process when it bestows false confidence or complacency.
The problem is worse than the mere mistaking of correlation for causation. The obsessive emphasis on “gender” as being both the source of and solution to suffering ultimately distracts parents, clinicians, teachers, and patients themselves from pursuing more effective strategies of mental health improvement. A teenage girl with a history of sexual abuse or eating disorders is ill-served by medical professionals who mistake the symptom of her distress (gender distress) for its underlying cause. A common complaint from a rising number of detransitioners is that no one was there to help them explore the true sources of their suffering. They have a point.
A known complaint among American medical providers is that systemic pressures discourage them from conducting careful and drawn-out diagnoses. Two friends of mine, both doctors, have raised this complaint to me several times in the past year alone; both wish they could spend more time with their patients in order to better understand their problems. One recently started his own practice in order to give his patients the quality of care they need and deserve.
One aspect of the gender affirming approach that makes it so attractive to therapists is its simplicity: it provides a single, easy, indeed all-too-convenient explanation for what is wrong with a teenager in distress. And it has the additional advantage of deferring to that teenager’s self-diagnosis, leaving her temporarily satisfied that she is finally being listened to. The affirm-or-suicide mantra lubricates this process by injecting it with a sense of urgency. Is this “gender ideology”? Perhaps, but it is no less the combination of a misguided belief about suicide, the pressures of a healthcare system that incentivizes swift diagnoses and expensive treatments, and an unchecked ethos of medical consumerism.
Another perverse outcome of the affirm-or-suicide narrative is that it may itself contribute to suicide. Social scientists and health officials have warned of a “contagion” effect following public discussions of suicide. A 2020 study found that teen suicide “increased significantly” in the month following the release of the Netflix series “13 Reasons Why,” which deals with—and some critics argue glamorizes—that subject. As one group of experts recently emphasized, “any conversations about suicide should be handled with great care, due to its socially contagious nature.”
Many countries, including the United States, have media guidelines on how to report on suicide so as not to inadvertently encourage people to engage in the behavior. Among the things that the CDC has warned not to do is “[p]resenting simplistic explanations for suicide.” As the agency explains, “Suicide is never the result of a single factor or event, but rather results from a complex interaction of many factors and usually involves a history of psychosocial problems.” It's difficult to imagine a more “simplistic explanation” than “kids will kill themselves if their gender identity is not affirmed.”
If there is scant evidence for the affirm-or-suicide narrative, and if using that narrative as a strategy for “transgender rights” might have negative repercussions for the very people activists and policymakers claim to want to protect, why do they continue to tout it? Some, perhaps, might simply not have given the matter much thought. Or perhaps they are uniquely vulnerable to emotional extortion due to some pathological excess of empathy or unexamined ideological assumptions. But I suspect that there are at least three additional motives at work, whether conscious or not.
First, as Colin Wright, myself, and other commentators on the trans phenomenon have argued, the trans movement is mired in confusion and self-contradiction. Activists tell us that the body has no relevance for being male or female, but also people with a male (or female) “gender identity” need a male (or female) body in order to live “authentic” lives; that women deserve their own category of sports but that access to that category should have nothing to do with physical sex distinctions; and that gender identity is an innate, immutable, even biologically derived, and socially valuable property of persons, but also that it is a system of social subordination to be resisted through “non-binary” and “queer” performances. When skeptics want to get beyond the contradictory statements to the truth of the matter, they are told that “getting at the truth is deeply transphobic.” The suicide panic enables activists to change the subject, diverting attention away from their contradictions.
Unlike other critics of gender ideology, I tend to think that what we have seen unfold in Western societies is equal parts “gender ideology” and a therapeutic attitude underwritten by half-baked relativism (or is it relativism underwritten by a therapeutic attitude?).
Second, from a more practical point of view, hyperbole surrounding the suicide threat is designed to get us to overlook the fundamentally experimental nature of pediatric gender medicine, suspend everything we know about adolescent psychology, and create an exception in our normal application of principles regarding patient autonomy and consent. The famed trans activist and child therapist Diane Ehrensaft argues, for instance, that just as we would allow a child to sever a limb to save his life, so too we must allow children to sacrifice their future reproductive and health prospects on the grounds that “gender affirming” care is life-saving. Any medical treatment, but especially one targeted at minors, requires a careful weighing of pros and cons, benefits and risks. The point of suicide alarmism, it seems to me, is to get us to not do this careful balancing act.
Third, transgender interest groups, which are now for the most part ideologically captured gay rights interest groups, face strong incentives to exaggerate threats and present themselves as standing in between transgender youth and impending doom. Obviously, alarmism is not unique to the world of LGBT advocacy organizations; pretty much all “public interest” groups who face collective action problems rely on what the late political scientist James Q. Wilson called “purposive incentives.” For an entity like the Trevor Project, an organization founded over two decades ago for the purpose of preventing suicide by (mainly gay) youth, public belief in a suicide epidemic is vital for soliciting donations, securing grants, recruiting talent, and exercising influence over the policy process. Especially under Democratic administrations, bureaucrats in federal and state education departments will cite Trevor Project statistics on LGBT suicide as justifications for more aggressive regulation of schools. None of this is to suggest that the people who work at Trevor are being dishonest, but only that they face strong institutional incentives to exaggerate the suicide threat.
Teen suicide is one of the most horrific and tragic events that can befall any parents. To exploit this primordial fear for political gains is cynical. If activists wanted to get serious about addressing the supposed “epidemic” of suicide among transgender youth, they would do three things. First, they would read the studies on suicide more carefully. Second, and as a result, they would take the therapeutic focus off of gender and, without completely excluding gender from the picture, place it on the more plausible causes of teen distress. And third, they would resist the temptation for suicide fearmongering and lay off the simplistic narrative that suicide results from not being “affirmed” in one’s “gender identity.”
We should not hold out hope that activists will do any of this, however, given how invaluable the suicide threat has been toward achieving their goals in the political arena.
==
The rhetoric, emotional manipulation and outright gaslighting we’re being fed is comparable to when we’re scolded not to criticize Islam otherwise it will put Muslims in danger. Just, cranked up to a thousand.
They can call it “transphobic” if they like, but all that means is they have only an ad hominem. And like accusations of “Islamophobia,” they’ve overplayed that card to try to prevent people from looking behind the curtain that it’s rather meaningless at this point.
They don’t care about kid’s health or wellbeing or they’d say yes, more health care, more thorough exploration, no matter what the outcome is, hey, you’re not trans, that’s great, maybe you are, okay, we can work on the actual problems because the health and wellbeing of the person supersedes ideological motivation. They should care about getting the best mental and physical healthcare, no matter what.
But they don’t. It’s the opposite. Do not question it. Do not suggest exploring alternatives. Do not point out the inconsistencies. Do not point out the data showing a social contagion. Do not point out the comorbid conditions. Do not point out the desisters or the detransitioners. Do not notice that it’s based on stereotypes and goes after gay kids at an inordinate rate. Do not look closely at the false rhetoric around suicide. Do not use the scientific method, use only presuppositional, unfalsifiable faith. They care only about their authoritarian ideology. Shockingly like Islam, by the way.
#Leor Sapir#affirm or suicide#trans or suicide#gender ideology#emotional manipulation#queer theory#suicide#trans suicide#ideologically motivated#ideological corruption#ideological fanaticism#ideological capture#moral panic#false statistics#statistics#fear mongering#medical malpractice#wokeness as religion#woke activism#wokeism#cult of woke#woke#religion is a mental illness
14 notes
·
View notes
Text
Today I’m think about how harmful and deliberate the invisibity of trans men and mascs is. In pretending we don’t exist and have never existed we are denied a community and a history. Young trans boys grow up thinking they’re completely alone contributing to the insanely high rates of suicide we have. (A study by the American Academy of Pediatrics showed that more then half of trans male teenagers have attempted suicide. Link)
Older trans men are denied healthcare especially “woman’s healthcare.” that they need and even though we have higher rates of assault then cis men and woman we are denied recourses for safety and recovery. Link
It’s so harmful and exhausting to watch this invisibility even happen in our own communities.
452 notes
·
View notes
Text
A new landmark study has found that access to gender-affirming healthcare significantly reduces rates of depression, gender dysphoria, and suicidality among transgender people.
While it’s no secret that providing gender-affirming care to transgender individuals who ask for it can greatly benefit their well-being, an increase in transphobic rhetoric and bans on gender-affirming healthcare has prompted thorough medical studies into the impact of such care.
Now, brand new research conducted in Melbourne, Australia, has found that allowing transgender people to access the care they’re after can reduce suicidality by a stunning 55%.
As part of the first-ever randomized controlled trial (RCT) on gender-affirming care, researchers took 64 transgender and gender-diverse adults who had been looking to start testosterone therapy and randomly split them into a treatment group and a control group.
While the treatment group was allowed to begin hormone therapy that week, the control group waited three months for their treatment to begin.
Before the study began, both groups were evaluated on depression, gender dysphoria, and suicidality. Three months later, the two groups were evaluated again.
RCTs for medical care can often be hard to conduct due to practical and ethical concerns. However, researchers of this study found a way to hold an RCT for this study by incorporating a shorter follow-up period. Rather than giving the control group a placebo drug, or no treatment at all, they were simply given a longer wait time.
The results showed a notable decrease in gender dysphoria, depression, and – most significantly – suicidality.
The group that received gender-affirming care right away saw a 55% reduction in suicidality compared to a 5% drop within the control group.
Depression scores in the treatment group decreased by half, while gender dysphoria rates also significantly decreased.
Breaking down their findings, researchers Brendan J. Nolan MBBS, Sav Zwickl, PhD, and Peter Locke wrote: “There was a statistically significant decrease in gender dysphoria in individuals with immediate [access to gender-affirming care] compared with delayed initiation of testosterone therapy.”
“A clinically significant decrease in depression and a decrease in suicidality also occurred with immediate testosterone therapy.”
“The findings of this trial suggest that testosterone therapy significantly decreases gender dysphoria, depression, and suicidality in transgender and gender-diverse individuals desiring testosterone therapy.”

Of course, this isn’t the first time that research has shown significant drops in depression and suicide rates among transgender individuals who receive gender-affirming care.
A 2022 medical study showed that young transgender people who have access to puberty blockers are 73% less at risk of suicide and report improved well-being.
But, as anti-trans activists advocate for further bans on gender-affirming care, one of the key arguments is that the evidence in support of the care isn’t up to scratch with GRADE (Grades of Recommendation, Assessment, Development, and Evaluation) standards.
So research like this landmark RCT is so significant to the transgender community and its allies as the fight for their healthcare rights rumbles on.
#us politics#news#pinknews#2023#gender affirming care#gender affirming healthcare#transgender healthcare#transgender#trans rights#trans healthcare#suicidality#depression#gender dysphoria#Australia#randomized controlled trial#trust the science#Brendan J. Nolan#Sav Zwickl#Peter Locke#testosterone therapy#Grades of Recommendation Assessment Development and Evaluation#lgbtqia+#lgbtqia+ rights
449 notes
·
View notes
Last Seen Blogs


byeiris
In The iddle of midnight

whiteboi-inferiority
I see you.

hannahsread
Hannahs Read

thatsmolmusicnerd
Rio~