#pterygopalatine
Text
Comendo a nega gostosa
Borrachas
Vanessa Cage Decides To Show Off Her Wilder Side
PORNSTARPLATINUM MILF Alura Jenson Creampied In The Kitchen
TS Alexa big dick cumming online
Horny stepsis sucks cock
NWORSHIP Young Black Girl Tiny Star with Wet Creamy Pussy
Ebony Squirting During Anal
Blonde With Extremely Beautiful puffy nipples on iffycams
Sexy nurse Skin Diamond dances and teases
#unhumane#helianthin#key#blip#mariposas#iterance#pterygopalatine#dimpliest#prevoid#ritualistically#tenant#vinify#thermogenic#Everson#uncontiguous#wine-soaked#nonreceptivity#antrophore#biotins#periodontic
0 notes
Text
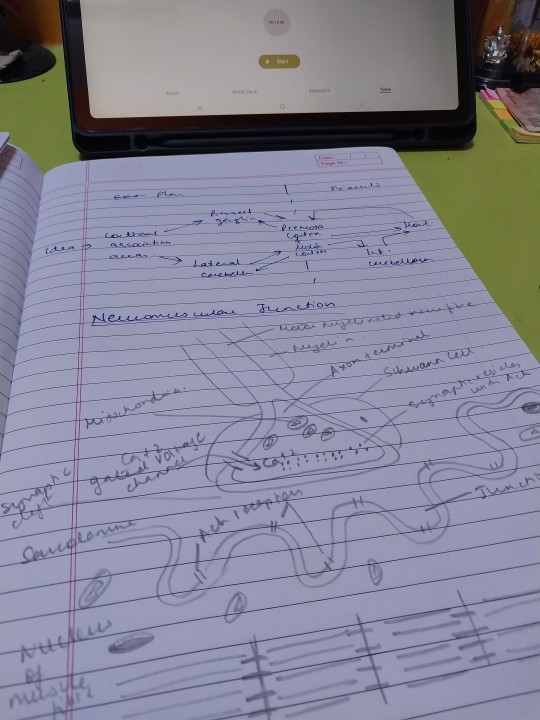
7 November 2023 // 20 days to finals
Today has been productive !
Studied :
Physiology:
REM sleep
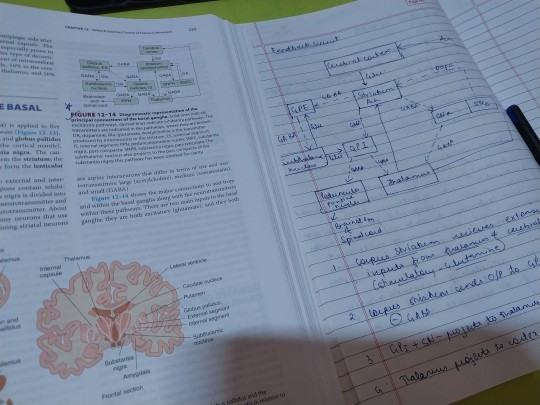
Basal Ganglia ( components, connections , functions)
Neuromuscular Junction
Myasthenia Gravis
Properties of skeletal muscles
Anatomy :
Joints ( this was a loooot , I'm so happy I completed this )
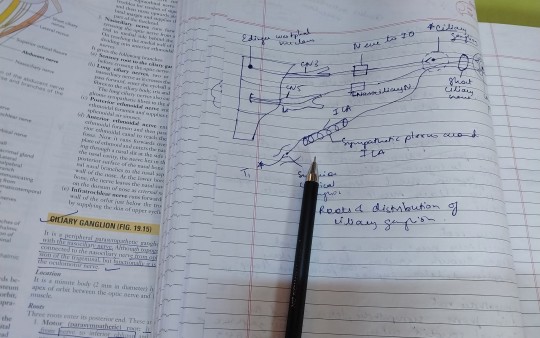
Ciliary Ganglion
Pterygopalatine ganglion
Imma be sleeping now 😴
Tata
#studyblr#productivity#study motivation#study blog#study hard#med school#stdyblr#aesthetic#studtblr#study inspiration#medical student#medical school#medicine#med student#med studyblr#medblr#medical studyblr#college studyblr#desi studyblr#studyspo#study inspo#chaotic academia#study aesthetic#exam study#studying for finals#final exams#firstyearmbbs#study study study#study community#work hard
17 notes
·
View notes
Text

Note: Turkish,English,German and Arabic description
🇹🇷🦋Yanak inceltme yada popüler adıyla ‘Hollywood yanağı’da denilen ameliyat kısa süreli,kalıcı, etkin ve sonuçları çok başarılıdır.
🦋Buccal Fat Pad (BFP)Removal ,Partial buccal lipectomy, Hollywood yanağı, yanak yağı aldırma,yanak inceltme gibi isimlendirilir.
🦋Temel amaç yuvarlak, kare yada geniş yanaklı, elmacık kemiği(zigoma/malar bölge) çıkıntılı olmayan yüzü ince görünmeyen kişilere yapılabilir.
🦋En sık kadınlara yapılsada son yıllarda erkekler de tercih etmektedir.
🦋Yanakta bulunan bu yap yastığını ilk olarak 1732’de Heister tanımlamıştır.
🦋1802’de M.F.X.Bichat anatomik yapısını ayrıntılı açıklamıştır.
🦋Dr.Bichat adıyla anılan ‘Bichat yağ yastığı’ 4 uzantıya ve 3 ayrı loba ayrılır.
🦋Posterior(arka) lob; temporal, ptergoid, ptergopalatin be bukkal kısımlardan oluşur.
🦋Ameliyat tekniği: lokal anestezi genelde yeterli olup iki taraflı üst çene(maksilla) lateral(dış) mukozasından 5-10 mm’lik insizyon yapılarak ‘fatpad’in %40-50’i çıkartılır.
🦋Ortalama volüm 6mm kayıptır( kadınlarda 7.2-10.8 mm ve erkeklerde 7.8-11.3 mm).
🦋Bu miktardan fazla çıkartmalarda yanakta çökme ve/ veya asimetri oluşabilir.
🦋Bu ameliyatı bazı otorler 25 yaş sonrası için önerirler.
🦋Ameliyat süresi 20-40 dakikadır.
🦋Ameliyattan hemen sonra belirgin görüntü oluşsa da 2-3 hafta ödem/şişlik görülmesi doğaldır.
🦋7-10 gün korse kullanımı, antibiyotik, ağrı kesici, gargara ve ağız hijyeni önerilir.
🦋Genelde dikiş alınmasına gerek yoktur 1 haftada eriyecektir.
🦋İdeal görünüm 2-4 ayda ortaya çıkar.
🦋Deneyimli cerrahlarda komplikasyon minimaldir.
🦋Bazı araştırmalarda komplikasyon %8.45 bildirilmiştir.
🦋Bu komplikasyonlar; ödem, kanama(internal maksiller arter), enfeksiyon, asimetri, trismus, fasial sinir bukkal dal yaralanması, paratis bezi stenson kanal yaralanması sayılabilir.
Kaynak;
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6051676/
https://www.ncbi.nlm.nih.gov/books/NBK576413/
Note: Turkish,English,German and Arabic description
🇻🇬🦋Cheek thinning, or popularly known as 'Hollywood cheek' surgery, is short-term, permanent, effective and its results are very successful.
🦋Buccal Fat Pad (BFP) Removal, Partial buccal lipectomy, Hollywood cheek, cheek fat removal, cheek thinning.
🦋The main purpose is that it can be performed on people with round, square or wide cheeks, without protruding cheekbones (zygoma/malar area), and whose face does not look thin.
🦋Although it is most commonly performed on women, men have also preferred it in recent years.
🦋Heister first described this cheek pad in 1732.
🦋In 1802, M.F.X.Bichat explained its anatomical structure in detail.
🦋The 'Bichat fat pad', also known as Dr. Bichat, is divided into 4 extensions and 3 separate lobes.
🦋Posterior lobe; It consists of temporal, pterygoid, pterygopalatine and buccal parts.
🦋Surgery technique: local anesthesia is generally sufficient and 40-50% of the 'fatpad' is removed by making a 5-10 mm incision in the lateral (external) mucosa of the bilateral upper jaw (maxilla).
🦋The average volume loss is 6 mm (7.2-10.8 mm in women and 7.8-11.3 mm in men).
🦋Decals exceeding this amount may cause sagging and/or asymmetry on the cheek.
🦋Some authorities recommend this surgery for people after the age of 25.
🦋Surgery time is 20-40 minutes.
🦋Although a clear appearance occurs immediately after the surgery, it is natural to see edema/swelling for 2-3 weeks.
🦋 7-10 days of corset use, antibiotics, painkillers, mouthwash and oral hygiene are recommended.
🦋 Generally, there is no need to remove stitches, it will dissolve in 1 week.
🦋The ideal appearance appears in 2-4 months.
🦋Complications are minimal in experienced surgeons.
🦋In some studies, complications were reported as 8.45%.
🦋These complications; edema, bleeding (internal maxillary artery), infection, asymmetry, trismus, facial nerve buccal branch injury, paratis gland Stenson canal injury.
Source;
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6051676/
https://www.ncbi.nlm.nih.gov/books/NBK576413/
Hinweis: Türkische, englische, deutsche und arabische Beschreibung
🇩🇪🦋Eine Wangenverdünnung, im Volksmund auch „Hollywood-Wangenoperation“ genannt, ist kurzfristig, dauerhaft, effektiv und die Ergebnisse sind sehr erfolgreich.
🦋Entfernung des bukkalen Fettpolsters (BFP), partielle bukkale Lipektomie, Hollywood-Wange, Wangenfettentfernung, Wangenverdünnung.
🦋Der Hauptzweck besteht darin, dass es bei Menschen mit runden, eckigen oder breiten Wangen durchgeführt werden kann, ohne hervorstehende Wangenknochen (Jochbein-/Malarbereich) und deren Gesicht nicht dünn aussieht.
🦋Obwohl es am häufigsten bei Frauen durchgeführt wird, bevorzugen es in den letzten Jahren auch Männer.
🦋Heister beschrieb dieses Wangenpolster erstmals im Jahr 1732.
🦋Im Jahr 1802 erklärte M.F.X.Bichat seine anatomische Struktur im Detail.
🦋Das „Bichat-Fettpolster“, auch Dr. Bichat genannt, ist in 4 Fortsätze und 3 separate Lappen unterteilt.
🦋Hinterlappen; Es besteht aus temporalen, pterygoidealen, pterygopalatinalen und bukkalen Teilen.
🦋Operationstechnik: Lokalanästhesie ist im Allgemeinen ausreichend und 40–50 % des „Fettpolsters“ werden durch einen 5–10 mm langen Schnitt in der seitlichen (äußeren) Schleimhaut des beidseitigen Oberkiefers (Oberkiefer) entfernt.
🦋Der durchschnittliche Volumenverlust beträgt 6 mm (7,2–10,8 mm bei Frauen und 7,8–11,3 mm bei Männern).
🦋Abziehbilder, die diese Menge überschreiten, können zu Durchhängen und/oder Asymmetrien auf der Wange führen.
🦋Einige Behörden empfehlen diese Operation für Personen nach dem 25. Lebensjahr.
🦋Die Operationszeit beträgt 20-40 Minuten.
🦋Obwohl unmittelbar nach der Operation ein klares Erscheinungsbild auftritt, ist es natürlich, dass für 2-3 Wochen Ödeme/Schwellungen auftreten.
🦋 7-10 Tage Korsetttragen, Antibiotika, Schmerzmittel, Mundwasser und Mundhygiene werden empfohlen.
🦋 Im Allgemeinen ist es nicht nötig, die Fäden zu entfernen, sie lösen sich innerhalb einer Woche auf.
🦋Das ideale Aussehen stellt sich in 2-4 Monaten ein.
🦋Komplikationen sind bei erfahrenen Chirurgen minimal.
🦋In einigen Studien wurden Komplikationen mit 8,45 % angegeben.
🦋Diese Komplikationen; Ödeme, Blutungen (Arteria maxillaris interna), Infektionen, Asymmetrie, Trismus, Verletzung des Wangenasts des Gesichtsnervs, Verletzung des Stenson-Kanals der Paratisdrüse.
Quelle;
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6051676/
https://www.ncbi.nlm.nih.gov/books/NBK576413/
ملحوظة: الوصف باللغات التركية والإنجليزية والألمانية والعربية
🇮🇶🦋تنحيف الخد أو المعروفة شعبياً باسم "جراحة خد هوليوود" هي عملية قصيرة الأمد ودائمة وفعالة ونتائجها ناجحة جداً.
🦋إزالة وسادة دهون الخد (BFP)، استئصال شحم الشدق الجزئي، خد هوليود، إزالة دهون الخد، تنحيف الخد.
🦋الغرض الرئيسي هو أنه يمكن إجراؤها على الأشخاص ذوي الخدود المستديرة أو المربعة أو العريضة، دون عظام الخد البارزة (منطقة الوجنة / الوجنات)، والذين لا يبدو وجههم نحيفًا.
🦋على الرغم من أنه يتم إجراؤه بشكل شائع على النساء، إلا أن الرجال يفضلونه أيضًا في السنوات الأخيرة.
🦋وصف هيستر وسادة الخد هذه لأول مرة في عام 1732.
🦋في عام 1802، شرح M.F.X.Bichat بنيته التشريحية بالتفصيل.
🦋تنقسم "وسادة الدهون بيشات"، المعروفة أيضًا باسم دكتور بيشات، إلى 4 ملحقات و3 فصوص منفصلة.
🦋الفص الخلفي. وهو يتألف من الأجزاء الصدغية والجناحية والجناحية الحنكية والشدق.
🦋تقنية الجراحة: التخدير الموضعي كافٍ بشكل عام ويتم إزالة 40-50% من "السادة الدهنية" عن طريق إجراء شق 5-10 ملم في الغشاء المخاطي الجانبي (الخارجي) للفك العلوي الثنائي (الفك العلوي).
🦋متوسط فقدان الحجم هو 6 ملم (7.2-10.8 ملم عند النساء و7.8-11.3 ملم عند الرجال).
🦋الملصقات التي تتجاوز هذه الكمية قد تسبب ترهل و/أو عدم تناسق في الخد.
🦋توصي بعض السلطات بإجراء هذه الجراحة للأشخاص بعد سن 25 عامًا.
🦋مدة الجراحة 20-40 دقيقة.
🦋على الرغم من ظهور مظهر واضح بعد الجراحة مباشرة، إلا أنه من الطبيعي رؤية الوذمة/التورم لمدة 2-3 أسابيع.
🦋 يوصى باستخدام المشد لمدة 7-10 أيام، ويوصى بالمضادات الحيوية ومسكنات الألم وغسول الفم ونظافة الفم.
🦋 بشكل عام ليس هناك حاجة لإزالة الغرز فهي ستذوب خلال أسبوع واحد.
🦋يظهر المظهر المثالي خلال 2-4 أشهر.
🦋المضاعفات ضئيلة عند الجراحين ذوي الخبرة.
🦋في بعض الدراسات، بلغت نسبة المضاعفات 8.45%.
🦋هذه المضاعفات؛ وذمة، نزيف (الشريان الفكي الداخلي)، عدوى، عدم تناسق، ضزز، إصابة فرع الشدق في العصب الوجهي، إصابة قناة ستنسون في الغدة النظيرية.
مصدر؛
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6051676/
https://www.ncbi.nlm.nih.gov/books/NBK576413/
#opdrazimetozdemir#aesthetic#surgery#bestplasticsurgeon#turkey 🇹🇷#plastic#Bişektomi#bichectomy buccalfatpadremoval istanbul Istanbul Estetik plastikcerrahi#yanakinceltme#Bichat#estetikcerrahi#istanbulestetikcerrahi#buccal fat removal#yanakyagıalma#Hollowoodyanağı
2 notes
·
View notes
Note
OKAY DONT JUDGE ME THOUGH LMAO
- Shigaraki likes to go to payphones just to call you up and leave moans and breathy messages about how he's going to defile you. It's his hobby.
- Sir Nighteye is into tickling but tickling until you wet yourself and can't stop crying. Probably into feet too. Keeps a whole freaky basement of bdsm furniture
- Overhaul is into fisting. I can just see it so well... Maybe it's the gloves.
- Rlly weird: I think Hawks is into watching you give birth to eggs. More than oviposition, he likes seeing them go in and come out while you're in pain. He likes to comfort you while you do it too. I don't know, I just think he's a fucked up little bird man.
Anon I would never ever ever ever judge you!! I used to be a freelance fetish artist and I think about piss every day, I am the last person to judge anyone on here 😭 You can truly tell me everything ♡
tw. ovi, stalking, piss, fisting -- everything anon mentioned, really
"It's his hobby" - hfdjhfj idk but that killed me. Totally. Our little stalker ♡ Mmmh the messages would be so juicy - and he works really hard on them, thinks about them all day! You better appreciate his efforts and cry for him the next time he calls you. He's basically giving you free phone sex, who doesn't want that? Don't be so fucking ungrateful.
You know what? I can live with Sir and feet 😂 (tmi tmi tmi but feet are erogenous zones that is all I'm saying saghjds) And the tickling until you piss yourself thing? I think someone mentioned that a day or two ago - but I have to reiterate - that'd be so cruel and mean. It'd hurt so bad and it would be sooo humiliating. Probably tells you not to piss yourself, no matter what happens (but of course aims for that) and then acts all digusted and disappointed in you. Verbally belittles you until you're nothing but a bundle of snot and tears (and piss).
Overhaul and fisting?! That fucker wants to crawl into every crevice you have, nostrils and pterygopalatine fossa included. He'll prepare you well beforehand and then he straps you down so tight you can't even think of getting away. Talks throughout the whole procedure to belittle and degrade you as he slips in. Maybe a ruined holes type of guy? Kai wants to see how far he can go - he can always just overhaul you, after all. Also the king of degrading dirty talk ♡And hmmm ovi with Hawks ♡ The pain is the appeal for me - it's almost sweet how he talks you through it, kisses the top of your head and keeps you close 🥺 you're going through all of this pain for him and you're taking it so well - you're so strong, even with a face full of tears and sweat. In fact, you've never looked better! I love this 🤭
72 notes
·
View notes
Text
not a to do list, bc there’s No Time™ for that, i’m just gonna keep track of the topics i covered today:
✅the orbit, infratemporal & temporal fossae
✅the pterygopalatine fossa, synchondroses & sutures of the skull
✅the joints: atlanto occipital, atlantoaxial, and temporomandibular
✅the muscles of mastication
✅Thieme flashcards
#sabrina attempts productivity#🤡 hours#<- blacklist if you don't want to see my exam season posts :)
29 notes
·
View notes
Photo

anterior view of sphenoid bone
The sphenoid bone is a singular and key bone in the skull having many foramina and fissures and articulations with several other bones. In this anterior view, the lesser wings are separated from the greater wings by the superior orbital fissure. Centrally, the body of the sphenoid contains the sphenoid sinus. Projecting inferiorly are the paired pterygoid processes consisting of lateral and medial pterygoid processes separated by the pterygoid fissure. In this view, one can see the openings of the foramen rotundum and Vidian canal at the posterior wall of the pterygopalatine fossa for transmission of the maxillary nerve and Vidian nerve, respectively. The medial wall of the infratemporal fossa is bounded by the lateral surface of the lateral pterygoid plate. The roof of the infratemporal fossa is formed by the infratemporal surface and crest of the greater wing. At the roof are the foramen ovale and foramen spinosum (not visible in this view). The inner surface of the greater wing in this perspective serves as part of the lateral wall of the orbit while the external surface bounds part of the temporal fossa. (Image courtesy of AL Rhoton, Jr.)
17 notes
·
View notes
Text

Grant’s Atlas
Pterygopalatine ganglion = sphenopalatine ganglion
It can be used to increase parasympathetic tone and decrease goblet cell activity so that secretions will be more watery. Can be used to treat upper respir infections.
6 notes
·
View notes
Photo

Johan P Reyneke’s Techniques, Tips, Tricks & Traps Vol 4:: Pterygopalatine Ganglion Block (azw3+ePub+Original PDF) #Anesthesiology #PainMedicine
0 notes
Photo

This is an excellent Review of the Maxillary Artery SWIPE & READ notes below @rev.med 🗣 Tag your friends in the comments below & test each other! Maxillary Artery and it’s Branches 🩸 ✅ Overview External carotid artery terminates into the superficial temporal artery & the 'Maxillary Artery'. It is found behind the neck of the mandible and it courses through the parotid gland, anterior to the ramus of the mandible and then runs superficial & deep to the lateral pterygoid muscle. Its blood supply is for the deep structures of the face. The lateral pterygoid muscle is what we use to divide the maxillary artery. @rev.med ✅ 1st Part: Mandibular (5 branches) Goes around deep around the neck of the mandible 1. Deep auricular artery (external acoustic meatus) 2. Anterior tympanic artery (enters squamotympanic fissure) 3. Middle meningeal artery (enters foramen spinosum) 4. Accessory meningeal artery (enters foramen ovale) 5. Inferior alveolar artery (enters mandibular foramen) giving off the artery to mylohyoid. @rev.med ✅ 2nd Part: Pterygoid (5 branches) Within the 2 heads of lateral pterygoid muscle 6. Deep temporal branches 7. Lateral pterygoid artery 8. Medial pterygoid artery 9. Masseteric artery 10. Buccal artery @rev.med ✅ 3rd Part: Pterygopalatine (6 branches) Anterior to lateral pterygoid muscle entering pterygopalatine fossa 11. Artery of pterygoid canal 12. Pharyngeal artery (enters palatovaginal canal) 13. Greater (descending) palatine artery (enters greater palatine foramen) 14. Posterior superior alveolar artery 15. Sphenopalatine artery (enters sphenopalatine foramen) 16. Infraorbital artery (enters inferior orbital fissure) ‼️ MORE in the Comments (Mnemonics)‼️ @rev.med @rev.med #maxillaryartery #REVMED #REVupyourbrain #REVmedicine https://www.instagram.com/p/CRHMSquhO3u/?utm_medium=tumblr
0 notes
Text
Sphenopalatine Ganglion Block: An Underutilized Tool in Pain Management_Crimson Publishers
Sphenopalatine Ganglion Block: An Underutilized Tool in Pain Management
by Barry J Kraynack in Developments in Anaesthetics & Pain Management_Crimson Publishers: Journal of Anaesthetics

Abstract
The sphenopalatine ganglion (SPG) block has been utilized to treat a wide variety of pain disorders. Postganglionic parasympathetic, sympathetic neurons, and the somatic sensory afferents can all be blocked by an SPG block. We examine the SPG anatomy, the techniques of blockade and the vast spectrum of conditions and indications for SPG block for pain relief. SPG block is an easy, safe and cost-effective method of management of acute, chronic and breakthrough pain which provides immediate relief and minimal side effects. It can be performed in a hospital or surgery center, clinic, office, ER department or at home. It is presently an underutilized and overlooked tool in pain therapy that should be more widely used.
Introduction
Anatomy
Because the sphenopalatine ganglion (SPG) has diffuse and extensive anatomical connections within the trigemino-autonomic (parasympathetic) reflex, it is of great interest to clinicians who treat pain conditions [1]. The SPG is a large extra cranial parasympathetic ganglion with multiple neural roots, including autonomic, sensory, and motor [2,3]. The SPG is a five-mm triangular shaped parasympathetic ganglion, located superficially and anterior to the pterygoid canal in the pterygopalatine fossa at the level of the middle nasal turbinate bilaterally. It is also known as the pterygopalatine, nasal or Meckel's ganglion [4]. It is enclosed in mucous membrane and a thin layer (1 to 1.5mm) of connective tissue. It is denoted as parasympathetic because preganglionic parasympathetic fibers synapse within the SPG. It is the largest peripheral parasympathetic ganglion with manifold connections to general sensory fibers and the internal carotid plexus [5-7].
For more open access journals in Crimson Publishers please click on link: https://crimsonpublishersresearch.com/
For more articles in Journal of Anaesthetics please click on below https://crimsonpublishers.com/dapm/index.php
Follow On Linkedin : https://linkedin.com/in/chyler-henley-ba9623175 Follow On Medium : https://medium.com/crimson-publishers/crimson-publishers-journals-f29e22da8f5c
#Crimson Publishers#Crimson Publishers LLC#Anesthesia Management#Pain Management#Geriatric Anesthesia
0 notes
Text
VII Cranial Nerve - Facial Nerve
VII Cranial Nerve – Facial Nerve
Functional components
Facial nerve has the following functional components
• Special visceral efferent (SVE) fibres arise from motor nucleus and supplies the muscles derived from the mesoderm of 2nd pharyngeal arch, viz. muscles of facial expression, etc.
• General visceral efferent (GVE) fibres are preganglionic parasympathetic fibres to the pterygopalatine and submandibular ganglia for…

View On WordPress
0 notes
Photo

at least now when i’m crying while studying for the final i’ll know it’s the work of the pterygopalatine ganglion 🙃
39 notes
·
View notes
Text
Use of Sphenopalatine Ganglion Blockade in Chronic Migraine Management
Authored by Michelle Androulakis

Case Report
Chronic migraine (CM) is a debilitating neurological disorder which affects more than 4 million individuals in the United State and 2% of the global population [1] in 2015, the Health Care utilization was estimated at $5.4 billion and the total cost associated with management of comorbidities exceeded over $40 billion in united states [2,3]. Different acute and preventive therapies, which are available for chronic migraineurs, are generally sub-optimally effective and are accompanied by side effects that are difficult to tolerate. Currently, Botulinum toxin therapy (Botox) is the only FDA approved CM preventative therapy, however, it is expensive and up to 9% of patients experience side effects such as neck pain after the injections. Recently, SPG neuromodulation has gained interest among headache specialist in management of CM. A series of SPG blockade using intranasal bupivacaine was efficacious for acute pain reduction in CM. However, further investigation into the long term preventative benefit of SPG block is warranted as this study sample size was too small to reach its statistical significance [4,5].
Sphenopalatine ganglion (SPG) has been a very important target for headache management since the beginning of the 20th century. SPG is the largest extra cranially ganglion of the head and is likely to play an important role in migraine pathogenesis through the activation of trigemino-autonomic reflex [6]. Up to 70% of migraine patients have cranial autonomic symptoms such as eyelid edema, nasal congestion, lacrimation, conjunctival injection, rhinorrhea, and facial swelling [7]. SPG modulation via electrical stimulation, microvascular decompression, surgical or radiofrequency ablation, and radiosurgical lesion have been performed for head pain in operating room settings, however, adverse effects of these interventions can be extensive. The SPG is located just posterior/superior to the tail of the middle turbinate on the lateral nasal wall and superior to the pterygopalatine fossa.
Manipulation of this region was often very challenging, as there is no direct access to the SPG and it is covered by a thin layer of nasal mucosa (1-1.5mm). New methods to modulate the SPG with a topical, intranasal approach have proven to be among the safest, least invasive, and least costly of all SPG interventions in headache management.
Recently, several new devices have been developed which facilitate a more accurate and effective delivery of the local anesthetics into the SPG. The risks of this procedure are typically minimal and may include minor discomfort during and after the procedure, a numbing or burning sensation, bitter taste from the anesthesia, bleeding from the nose (rarely), and lightheadedness. These side effects typically resolve within minutes to a few hours. There is also a very small risk of allergic reactions.
Use of SPG block has been recommended by American Headache Society (AHS) as part of comprehensive headache management plan. Indeed, repetitive SPG blockade twice a week for 6 weeks provides an alternative migraine prophylaxis for those with chronic migraine but could not tolerate (i.e. needle phobia) or unresponsive to Botox therapy. SPG block generally provides a better outcome for treatment of CM with head pain in frontal and/orbital regions, and may also help CM patients with coexisting medication overuse headaches to wean off excessive use of pain medications.
Nausea, which has been suggested as one of the main contributing factors for migraine chronification, is also another possible symptom that can be relieved with a series of SPG block. The area postrema area, located at the infer posterior part of IV ventricle, is responsible for nausea and vomiting through its connection to the nucleus of the solitary tract. The superior salivatory nucleus (SSN) provides preganglionic parasympathetic innervation to SPG, but also receives inputs from multiple areas, such as nucleus of solitary tract, limbic, and cortical regions. Repetitive intranasal SPG blockade with bupivacaine may reduce nausea and vomiting via inhibition of superior salivatory nucleus given its direct connection with the nucleus of solitary tract.
The exact mechanism of SPG neuro modulation remains to be elucidated. It has been postulated that inhibition of the parasympathetic outflow from the SPG would inhibit pain and autonomic symptoms that accompanying recurrent migraine attacks. This inhibition of parasympathetic outflow would decrease activation of perivascular nociceptors in the cranial and meningeal vasculature, especially in the frontal regions of the brain [8-10]. Additionally, modulation of the SPG may in turn modulate brain networks activity involved in pain processing. In a recent resting state functional MRI connectivity study, our group demonstrated that a series of SPG block treatment in chronic migraine significantly improved two intrinsic resting state functional connectivity networks (manuscript in preparation). This increase in functional connectivity coherence may represent that after effective treatment, reorganization of resting state brain networks to normalized states may occur.
Additionally, reduced parasympathetic outflow due to repetitive SPG inhibition may help to restore baseline homeostasis of brain networks involved in pain processing, via improved mesocorticolimbic modulation [11-13]. A large double blinded, randomized, placebo controlled clinical trial is warranted to evaluate the efficacy of repetitive SPG block in CM (Figure 1 & 2).
For more open access journals in juniper publishers please click https://juniperpublishers.com/
For more articles on Open Access Journal of Neurology & Neurosurgery Please click on https://juniperpublishers.com/oajnn/
Open Access Journal of Neurology & Neurosurgery in Full text in Juniper Publishers
0 notes
Text
Rare tumour removed from patient's skull
Pterygopalatine fossa schwannomas arise from the maxillary division of the trigeminal nerve, pterygopalatine ganglion, the inferior orbital nerve, and ...
from Google Alert - nerve surgery https://ift.tt/2U6P6MN
0 notes
Text
Harry Potter and the pterygopalatine recess of the superior nasal meatus
Harry Potter and the pterygopalatine recess of the superior nasal meatus
— Potter Papers (@PotterPapers) December 21, 2017
#Harry Potter#Potter Paper#Potter Papers#academia#Twitter#Harry Potter and the pterygopalatine reces
0 notes
Text
Endoscopic transorbital and endonasal approach for trigeminal schwannomas
Endoscopic transorbital and endonasal approach for trigeminal schwannomas
J Neurosurg 133:467–476, 2020
Trigeminal schwannomas are rare neoplasms with an incidence of less than 1% that require a comprehensive surgical strategy. These tumors can occur anywhere along the path of the trigeminal nerve, capable of extending intradurally into the middle and posterior fossae, and extracranially into the orbital, pterygopalatine, and infratemporal fossa. Recent advancements…
View On WordPress
#endoscopic endonasal approach#endoscopic transorbital approach#Surgical technique#Trigeminal schwannoma
0 notes
Last Seen Blogs

brunastyles
BrunaStyles_Art

zhria-rodqz-blog
Anitah Rodqz

thiccy-uwu
Mama Mia :•O

happythoughtsrecordings
Nathan De Leon

randhsinghlaw
R & H Singh Law PLLC