
mcatmemoranda
MCAT Memoranda
Originally, this blog was for things to be remembered for the MCAT. Then I included EMT training and then medical school; and now residency. Basically, this is where I keep some of the things I am studying or learning so that I can easily look them up when I need to. Search the tags to find stuff!
11162 posts
Don't wanna be here? Send us removal request.
Last Seen Blogs
hoperock
hoperock

kondo-hijikata
just miburo things

whosthereee
Untitled

billubackchod-blog
Bakchod Billu

loverglow13
melanie (taylor’s version)

Text
VEOZAH™ (fezolinetant) for Vasomotor Symptoms due to Menopause
Just saw a commercial about this med for hot flashes.
1 note
·
View note
Text
BRIXADI is bupreborphine injection. Apparently it’s less likely than Sublocade to cause injection site issues. Have a pt on it who complains of pain/a lump at the injection site even days after injection.
3 notes
·
View notes
Text
I didn't get COVID until end of 2022. Then I got it again in January this year. I'm going to get a COVID vaccine tomorrow. I had tried to schedule an appointment to get it at CVS earlier this year, but they didn't have any vaccines available. Now they do. It wasn't that bad. Just annoying. I wonder if they'll start making a yearly combined COVID and flu vaccine. That would be convenient.
0 notes
Text
Have a 22 y/o pt who complained of heart palpitations. Went to ED and had subclinical hypothyroidism and some PACs and ectopic beats in bigemininy and trigeminy. Sent him to cardiology, who recommened: beta blocker, antiarrhythmics, or APC ablation. He decided to start metoprolol XL 25 mg qd and will be getting an echo to rule out structural heart disease.
1 note
·
View note
Text
Fecal calprotectin just tests for inflammation. Can differentiate between IBD and IBS.
1 note
·
View note
Text
I have a pt who has history of hep C that was treated. I checked him for hep C RNA PCR viral load and it came back undetected, which means his treatment worked. This is called "SVR," sustained viral response. So when you do the hep C antibody screen, it still comes up positive, but the viral load (RNA PCR) is undetected, so no further treatment is needed.
1 note
·
View note
Text
Off label tx for plantar warts: Tagamet 800 mg QID x3 weeks
1 note
·
View note
Text

Strokes will spare the forehead, unlike Bell's palsy.
8 notes
·
View notes
Text
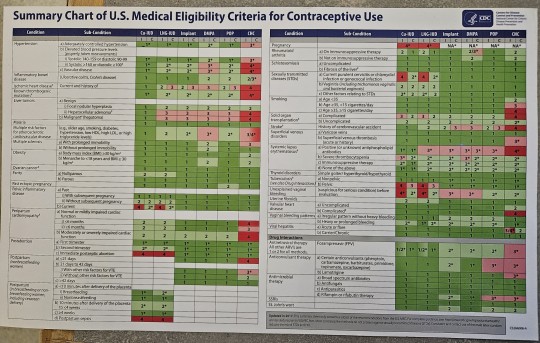

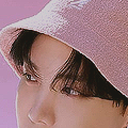
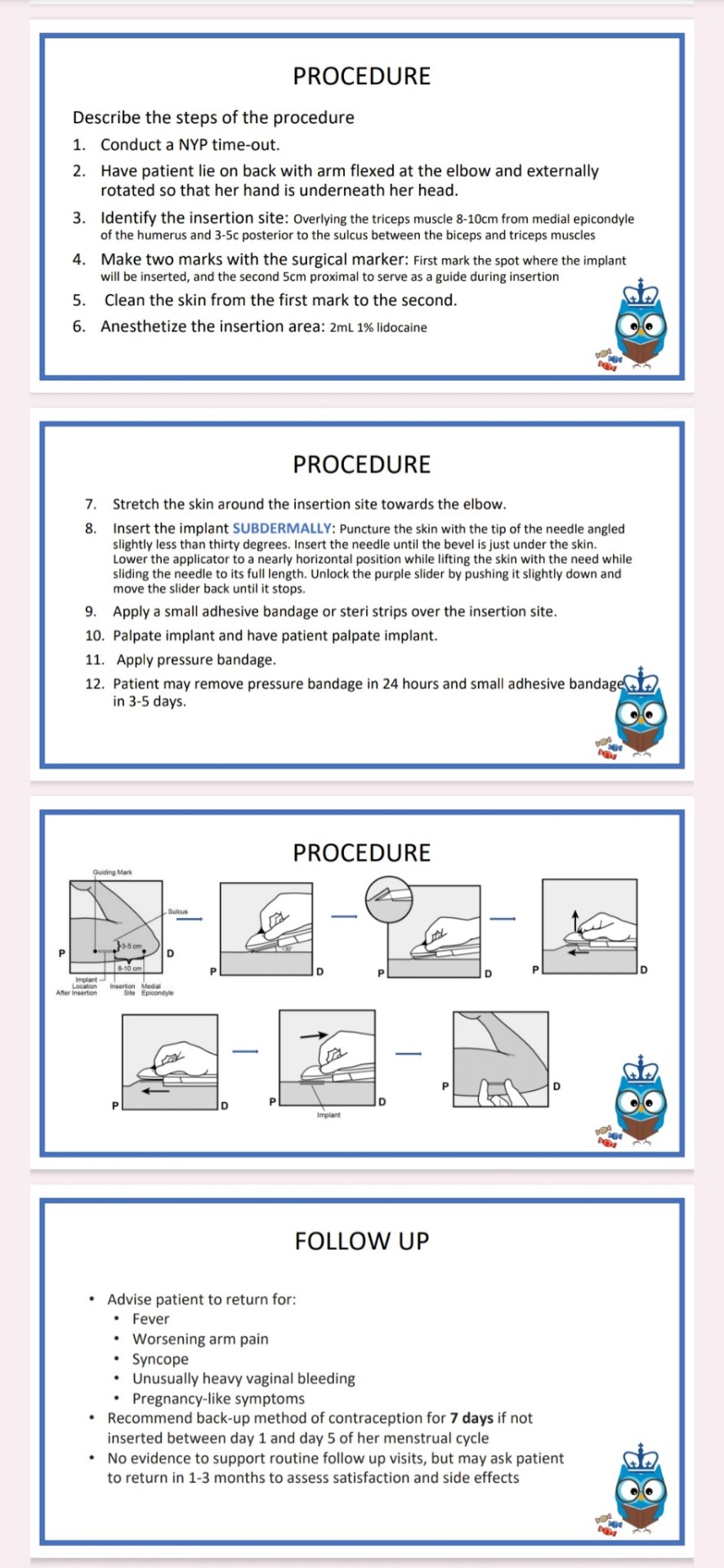
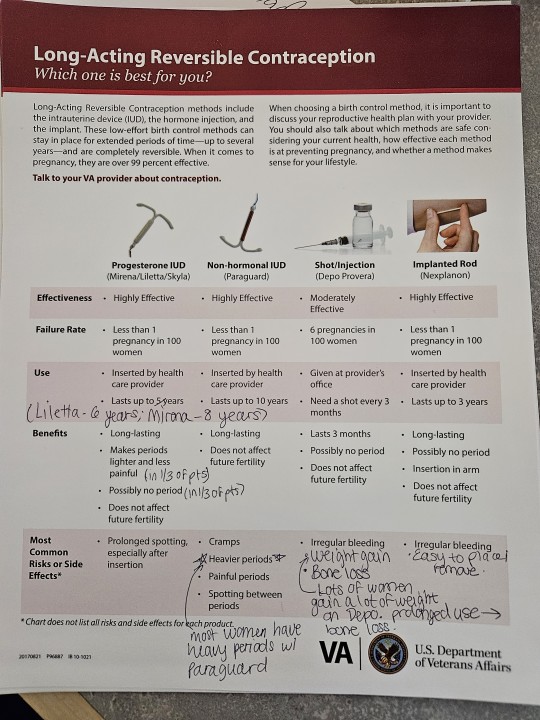
Will have to zoom in close to see this!
2 notes
·
View notes
Text
Liraglutide (Saxenda) dosing: Start 0.6 mg daily for 1 week. If tolerated, increase to 1.2 mg daily for 1 week. Increase by 0.6 mg a day per week (i.e., 1.8 mg per day on week 3, then 2.4 mg a day on week 4, then 3 mg a day on week 5). Maximum dosing is 3 mg daily. Discontinue if weight loss less than 4% after 16 weeks or if 3 mg daily is not tolerated.
1 note
·
View note
Text
Semaglutide can be used to treat alcohol use disorder.
4 notes
·
View notes
Text
The Rotterdam 2003 criteria are the most widely used diagnostic criteria for PCOS, endorsed by multiple national and international professional societies. These criteria require the presence of two out of the following three features: oligomenorrhea, hyperandrogenism, and the presence of polycystic ovaries on ultrasonography. When the first two of these criteria are clearly met, ultrasonography to establish the presence of polycystic ovaries is not required.
1 note
·
View note
Text
Hormone therapy is not required for all transgender patients, but those who receive treatment generally report improved quality of life, higher self-esteem, and decreased anxiety. Feminizing and masculinizing hormone therapies, including the use of estrogen and/or androgen therapies such as testosterone, are partially irreversible. Thus, it is important to make a reasonable, educated decision and use informed consent prior to treatment. Patients who receive masculinizing therapy are at increased risk for erythrocytosis and those who receive feminizing hormone therapy often experience reduced muscle mass and fat redistribution
2 notes
·
View notes
Text
I have a pt in clinic who I diagnosed with C. diff. According to UpToDate, the treatment for an initial infection is fidaxomicin (200 mg bid x10 days).
Regimen selection – For patients with an initial episode of nonsevere CDI, appropriate treatment regimens include either oral fidaxomicin or oral vancomycin; we favor fidaxomicin over vancomycin given a small benefit with respect to recurrence rates, in accordance with 2021 Infectious Diseases Society of America (IDSA) guidelines
2 notes
·
View notes