#Lisa Littman
Text
38 notes
·
View notes
Text
Published: Mar 30, 2023
For over a decade, the Gender Affirmative Model has been the standard of care for gender dysphoric youth across the West. Yet, despite its widespread and long-standing use, good evidence to support it remains elusive. Maybe that’s because there isn’t any.
A new paper reports on results from a survey of 1,655 parents of children who developed gender dysphoria during adolescence or soon after. American Academy of Pediatrics guidelines recommend affirming these kids in their new gender, and supporting them along the path to social, medical (hormonal), and surgical transition.
The results of this survey provide strong support for Dr. Littman’s Rapid-Onset Gender Dysphoria (ROGD) hypothesis, which suggests that gender dysphoria in this group may resolve with time and good psychological and social support, if needed.
Key Findings
Key findings of particular concern are that these children tend to have emotional problems that predate their gender-related issues by nearly four years. Furthermore, children with mental health issues were more likely than those without to have taken steps to transition. Children who were referred to a gender specialist were also more likely to have taken steps to transition. Parents reported feeling pressured by these specialists to transition their child. And parents reported a decline in their child’s mental health and social functioning after transition.
History of Gender Dysphoria and Standards of Care
About 15 years ago, Western countries began experiencing an exponential rise in adolescents and young adults suddenly developing gender dysphoria and being referred to gender clinics for treatment. Around the same time, a new philosophy on transgenderism began to take root: Just as there is nothing wrong with being attracted to the same sex, there was nothing wrong with identifying with a gender that did not match your biological sex. In other words, being transgender is perfectly normal. It is not a mental illness. If a trans person does have any mental health issues, it can be attributed to the extreme distress of having to live in a body that does not feel right (gender dysphoria), and the stress of living in a judgmental, transphobic world.
Out of this philosophy grew the Affirmative Care Model. This model focused on reassuring (affirming) people that their gender identity was real, normal and natural, and helping them take steps to relieve their gender dysphoria through social, medical (hormonal) and surgical transition. In order to address their social distress from lack of acceptance, much effort is devoted to creating a supportive environment among friends, family, schools and society in general.
Although there was almost no evidence to support it at the time, the Affirmative Care Model quickly became the standard of care in most Western countries.
In 2016, Dr. Littman noticed an anomalous spike in teenage girls suddenly declaring themselves transgender and became concerned. She conducted a survey of their parents to learn more about this new phenomenon. Based on what she found, she proposed that a new sub-category of gender dysphoria had emerged, this one sharing more similarities with anorexia and other eating disorders than with the previously recognized types of gender dysphoria. Dr. Littman described Rapid Onset Gender Dysphoria (ROGD) in her seminal paper published in 2018.
ROGD develops suddenly, during or after puberty in a person who would not have met the criteria for childhood gender dysphoria. Most often, these kids are white, highly intelligent and come from well-educated families. ROGD affects mainly girls, and groups of friends often come out as trans together. The influence of social media is believed to play a role. They often have a prior history of mental health issues, developmental difficulties or have experienced a traumatic or stressful event before developing gender dysphoria. A prior history of self-harm and difficulty fitting in with their peers are also common. Sadly, transitioning is not likely to help these kids with their issues as it does not address the root cause. In fact, it has a good chance of making things much worse.
The ROGD hypothesis suggests that for these unhappy kids, “gender dysphoria” is a catch-all phrase for any kind of distress, and transition is the cure-all solution
Since the publication of Littman’s paper, the ROGD hypothesis has come under fire from proponents of the affirmative care model. It’s easy to see why: The affirmative care model is based on the premise that being transgender is perfectly normal. The ROGD model suggests that this particular kind of gender dysphoria – and the desire to transition – is most definitely not normal. It’s a maladaptive coping mechanism.
Unfortunately, there is little evidence to support either hypothesis.
The World Professional Association for Transgender Health’s newest Standards of Care, published in Oct. 2022 admits, “A key challenge in adolescent transgender care is the quality of evidence evaluating the effectiveness of… gender-affirming medical and surgical treatments.” “The number of studies is still low and there are few outcome studies that follow youth into adulthood.”
Testing the ROGD hypothesis presents its own challenges. In North America, gender clinics are still using the affirmative model as a standard of care, which views taking steps to transition as medically necessary and thus, would be unwilling to test the ROGD model. Further, ROGD has become such a contentious topic at universities that any academic who broaches the subject risks career suicide. Just ask Dr. Littman and Dr. James Caspian.
Survey Results
Concurring with Dr. Littman’s findings, our survey indicates children who are most likely to develop ROGD are of European descent (78.9%), with above-average intelligence. They are also more likely to be female (75%). Their gender dysphoria develops around the age of 14 for girls, and 16 for boys. This may be partly due to the fact that boys go through puberty later than girls.
Their parents are more likely to be progressive and hold positive views towards LGBTQ+ rights. Frequently, parents went out of their way to make sure the reader understood this when they told their stories. Many had family and friends in the LGBTQ+ community, and some were members themselves. They just didn’t feel it made sense in their child’s case.
A majority of these kids were dealing with mental health issues (57%) that began around the age of 10, well before they developed gender dysphoria, and 42% of them had received a formal psychological diagnosis. The most frequently-reported issues were anxiety and depression. Self-harm was also prevalent in girls. Attention deficit disorder, autism, and obsessive-compulsive disorder were reported in numbers higher than the general population.
Very often, these kids had experienced a stressful event before they developed gender dysphoria (72.6%). Some described issues that would be overwhelming even for an adult to deal with, such as the suicide of a close relative, receiving a serious medical diagnosis such as cancer, being sexually assaulted, or being present at a mass shooting. Sometimes, the stress was more mundane, like moving, breaking up with a girl- or boyfriend, or having a good friend turn on them, but the child was having a hard time dealing with it. During the lock downs due to COVID, the strain of isolation was especially hard on these kids.
Parents also reported that their kids were having a lot of trouble fitting in with their peers at an age when being accepted feels like the most important thing in the world. Only about a quarter of parents reported that their child was well liked, and only one third said their kids got along well with other kids.
Parents reported their kids spent an average of 4.5 hours per day on the internet and social media.
When asked whether their child had friends who came out at the same time, 60.9% said their daughters did, compared with only 38.7% of their sons. The average number of friends who came out were 2.4.
“My daughter used to be so lonely her only friend was her guinea pig. At 11, a girl at school befriended her as did her group of friends. All of a sudden, my daughter said she was bi, then gay, then pan, then poly, then fluid, now trans. Her mental health is deteriorating and the psychiatrists (this is her 6th) seem to push their own agenda and label me transphobic. I KNOW my daughter. When no social group will welcome you and one finally does, you’ll conform to fit in, to not lose the only ‘friends’ you have.”
~Parent of an ROGD Kid
Transition
The majority of the children had socially transitioned at the time parents completed the survey (65.3%), and girls tended to socially transition earlier (age 15) than boys (age 17). In general, parents reported that their children had not started taking puberty blockers or hormones, and surgery was especially rare.
Girls who had friends who socially transitioned were more likely to do so themselves (73.3%), compared with only 39.5% of boys who were more likely to transition if they had a friend who did so.
One very concerning finding was that children with preexisting mental health issues were also more likely to socially transition than those without. This is worrisome, because children with emotional issues may lack the judgment needed to make serious, and sometimes irreversible, decisions about their bodies.
Another troubling finding was that children who received a referral to a gender specialist were more likely to have transitioned. This is especially concerning because 51% of parents who took their kids to a gender specialist also reported that they felt pressured to transition their child.
Effects of Transition on Mental Health and Social Functioning
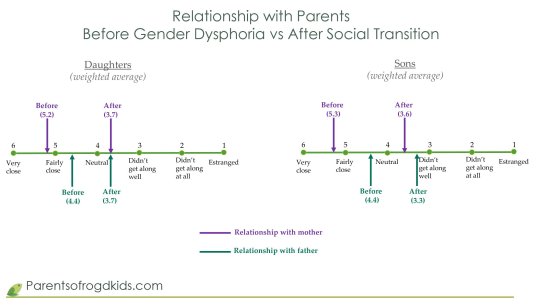
When asked about the state of their child’s mental health after social transition, they were much more likely to say it had worsened than improved.
Sadly, the change in the quality of the parental relationships also declined, as shown in the table below:
Conclusion
The results of the largest survey to date on gender dysphoric adolescents support Dr. Littman’s ROGD hypothesis. These youth are most likely using “gender dysphoria” to describe general feelings of dysphoria that they have no other name for, and do not understand. Transitioning will not help them. It can only cause irreversible harm and make things much worse.
Sweden, Norway, Finland, the UK and some States are backing away from the gender affirmative model, citing the lack of evidence and amid the growing number of detransitioners, many of whom are launching lawsuits against the gender specialists who harmed them. (See Ritchie Herron and Keira Bell, Michelle Zacchigna and Chloe Cole.)
Yet here in North America, the United States and Canadian Governments, the American Academy of Pediatrics and most other medical associations, are doubling down on the gender affirmative model.
If they truly want to “do no harm”, then they must follow Sweden’s lead and stop transitioning minors.
==
This should be good news. We have good reason to believe that distress can be resolved by treating the underlying cause, rather than through invasive and irreversible hormones, drugs and surgeries. How can this be a bad thing?
Because it's not about helping distress; if it was, they'd applaud the best treatment that causes the least harm. But it's about using anxious kids as pawns to remake society according to Queer Theory.
#Michael Sherman#Lisa Littman#Rapid Onset Gender Dysphoria#ROGD#social contagion#mental health#queer theory#gender ideology#medical transition#gender distress#gender dysphoria#mental health issues#mental health care#religion is a mental illness
94 notes
·
View notes
Text
This Transgender Day of Visibility, Gender Analysis reveals a groundbreaking timeline of the previously unknown origins of "rapid onset gender dysphoria", a hoax that misdiagnosed a generation of trans kids
#here's your tdov#visibility#rapid onset gender dysphoria#lisa marchiano#lisa littman#lisa bell#4thwavenow#transgender trend
37 notes
·
View notes
Text
Hossenfelder’s opening statement is akin to saying “On the one side are people who think vaccines are a way for Bill Gates to inject us with micro transmitters, and on the other side are people who think vaccines are safe and effective ways to reduce the spread of disease. And then there are normal people like you and I who think ‘both sides are crazy and could someone please summarize the facts in simple words,’ which is what I’m here for.”
This is known as “false balance,” or “bothsidesism,” a rhetorical trick that pretends to demonstrate an unbiased viewpoint, but in reality you’re being biased by default by comparing something backed up by reams of scientific data with something that has absolutely no basis in reality.
2 notes
·
View notes
Note
youve got a lot of really great thoughts on a transphobia and homophobia, tbh more critical thinking than most people on here, and i was wondering how much you knew about the theory of rapid onset gender dysphoria/if youd be comfortable sharing your thoughts on the ridiculous idea
It was explicitly invented by transphobes as a means of delegitimizing trans identity, and that invention was backed up by a "study" in which the person running the study never spoke to any trans people or to any professionals providing care for trans people, only spoke to the parents of trans minors, and those parents were specifically recruited from forums for anti-trans parents.
The paper which supposedly coined ROGD was taken down for a while and corrected. Further studies have found no basis for ROGD.
What's really interesting is in the cache of emails which became public earlier this year from a former detransitioner there's a paper trail which pretty clearly indicates that the term was actually created on a very heinous website called 4th/wave/now (forgive my anti-search slashes, these people are awful) well prior to the study.
Hey, you want to guess where the parents for this study were recruited from? If you guessed "the one where the term was invented," you're right!
But wait, there's more!
It appears from the journalistic work done by Mother Jones, Jude Doyle, and Julia Serano, that this term was created by an anti-trans activist who works extensively with right-wing think tanks and who went to great lengths to hide that she invented the term.
Jude Doyle:
Finding anti-trans narratives that would “sell” to the general public was a constant concern for this crowd, and Shupe says it didn’t much matter if the narratives were based in fact or not. Marchiano, for instance, eagerly watched the spread of the ROGD theory — “[transfeminist writer and researcher Julia] Serano has already written a takedown,” she exulted in one August 2018 email. Shupe suspects Marchiano’s role is larger than the public knows: “Marchiano never explicitly said she is the inventor of ROGD, but the evidence points to her, and she’s listed as a contributor to the [Lisa Littman] study on PLOS One,” she writes to me. “My ‘opinion’ is that Marchiano and the 4thWaveNow folks are behind the ROGD study, and Littman merely fronted it for them to make it appear unbiased.”
Jude Doyle again:
On July 2, Shupe sent Marchiano a link to Jones’ blog post telling her “you’ve upset Zinnia again.” (Shupe had a tendency to send Marchiano news of ROGD, and to attribute the theory to “you” — that is, to Marchiano — whether Marchiano was explicitly named or not. In the communications I’ve reviewed, Marchiano does not reject the attribution.) Marchiano responded by saying that Jones had done something to “make her nervous” — namely, she’d dug up a blog post about ROGD that Marchiano had written under her own name.
Julia Serano:
If all of this is true — that Marchiano ran YCTP and invented ROGD — then it would follow that Marchiano was also likely skepticaltherapist, the supposed parent of a trans child who invented the idea of “transgender social contagion” in the first place.
Julia Serano again:
Also on March 15, 2016, at 6:07am (so very early in the day, likely before the aforementioned YTCP piece is published), skepticaltherapist posts her final comment on 4thwavenow before mysteriously disappearing. In a reply to someone named Starrymessenger, skepticaltherapist says: 'I wanted to mention that this month’s Psychotherapy Networker is focusing on trans youth issues, and the tone of each article is uncritically celebratory — lots of mentions of “courage,” and “bravery.” You may need a subscription or at least an account to comment, but I have so far.'
At the time of this comment, "Lisa" is the *only* person to have posted a comment on this particular Psychotherapy Networker article, as the 2nd comment doesn't appear until later that evening (7:30:15 PM on March 15th; both 4thwavenow & Psychotherapy Networker appear to be based in the U.S., so the should be only a few hours apart, if at all). Therefore, "Lisa" and skepticaltherapist must be the same person.
Did you catch all of that?
This is a fraudulent "diagnosis" explicitly invented by an anti-trans psychologist who at times has used sockpuppets to manipulate online conversations, claimed at times to be the mother of a trans child, or maybe it was her friend who had the trans child, or maybe she just knew somebody who just randomly decided he was a trans boy after going on tumblr. (Boy, does Lisa Marchiano hate Tumblr, lol.)
After inventing this diagnosis and pushing it on a forum for parents who don't like that they have trans kids, Marchiano then approaches a different researcher and uses this other researcher to launder this term, launching it into the verbal stratosphere, while explicitly working with right-wing groups who used this "evidence" to manufacture anti-trans bills. This list of right-wing groups and individuals includes the Alliance Defending Freedom, the "American College of Pediatricians," -- not to be confused with the American Academy of Pediatrics, the legitimate organization, ACPeds is a fringe right-wing group.
They literally made all of this up, this idea that transmasculine people specifically are being "infected" by online sources, and then they laundered it through a shitty study and tried to hide the laundering they did, so that shit like this can happen:
The president of the American Principles Project, a member of the coalition, recently told the New York Times that his group’s goal is to eliminate all transition care, starting with children because that’s “where the consensus is.”
This isn't about protecting children or any bullshit like that, and it's not about this fallacious "disorder" because it doesn't exist -- and they know it doesn't exist. They know it doesn't exist because they were the ones who made it up.
Like... what else is there to say? It's like if I made up Purple Big Toe Disease and claimed that all people taller than 5'10" and born on a Tuesday have Purple Big Toe Disease and should not be able to buy aspirin, because it's G-d's plan that people who have Purple Big Toe Disease should not prevent themselves from feeling the pain that G-d has planned for them, and then I asked someone to write a paper about PBTD and pretend I wasn't the one who made it up so I could point at the paper and be like le gasp, PBTD is the number one problem! We need to stop everyone over 5'10" and born on a Tuesday from being able to buy aspirin! And then some dude in South Dakota starts writing up bills in consultation with a bunch of Evangelical lawyers to deny basic health care to people over 5'10" and born on Tuesdays.
If it sounds fucking ridiculous, it's because it is.
1K notes
·
View notes
Text
The Cass Review demanded clinicians perform child abuse (placebo HRT and conversion therapy) for acceptable studies on transgender children. As someone studying trans research (who was also a trans kid), I'm disgusted. We must reject all calls for abuse in gender medicine. We have 100+ years showing that HRT works!
If your review cites Lisa Littman & Kenneth Zucker as legitimate sources in 2024, you have no authority to speak about trans issues OR evidence-based medicine. Their studies have been so thoroughly debunked that they're a great example of using weak evidence to draw conclusions.
218 notes
·
View notes
Text
The idea of transgender “social contagion” was first proposed in a 2018 paper by Dr. Lisa Littman, a researcher who has pushed the theory heavily. The article, entitled “Rapid-onset gender dysphoria in adolescents and young adults: A study of parental reports,” proposed that social contagion was leading to an increase in trans identification. To support her claim, Littman solicited interviews from anti-trans websites such as Transgender Trend and 4thWaveNow. She used data from those interviews to claim that transgender youth “suddenly” develop gender dysphoria through a process known as “Rapid Onset Gender Dysphoria.”
Her paper was immediately withdrawn with an apology by the journal for correction after the data collection methods were revealed, with the republication stating that the research “does not validate the phenomenon” of transgender social contagion.
"Rapid Onset Gender Dysphoria" is derived from interviews with parents who report their children "abruptly came out as trans" without any forewarning. For numerous parents on these websites opposed to transgender rights, they claimed their children’s coming out was too sudden to be genuine. Coupled with conservative media exposure asserting that being transgender results from factors ranging from TikTok to alleged "grooming" in schools, parents frequently sought alternative explanations for their children's trans identification, instead of acknowledging the possibility that their children were authentically transgender.
A pivotal study published in The Journal of Pediatrics in 2021 entirely debunked this concept. Professionals who work closely with transgender populations frequently observe that individuals harbor dysphoria for an extended period before revealing their feelings to loved ones. Upon coming out, these individuals often swiftly embrace their transgender identity, motivated by the liberation that comes with acknowledging one's true self. To determine whether transgender identification is genuinely "rapid," researchers sought to pose a direct question to transgender teenagers: How long have you known you were transgender?
The results were stunning. Transgender teens knew they were trans for an average of 4 years before coming out as trans and getting their first clinical visit.
The study did not stop there, however. It also analyzed the few transgender teens who indicated their gender dysphoria realization was more recent. It found no linkages among those groups with depression, online support, having transgender friends, or any other proposed mechanisms for “rapid-onset gender dysphoria.” To put it simply: transgender people often know they are trans for a long time before coming out, and having transgender friends does not influence you to “become transgender.”
514 notes
·
View notes
Text
What are Radblr's thoughts about this? I'm on my way to take a test when this article popped up on my screen, and I wanted to post this before I leave, especially given that this is published by Scientific America. However, Im personally skeptically that "social contagion" doesn't play a factor at all; I wouldn't doubt it plays into this even a little bit. I'm sure everyone knows about articles posted in favor of this fad from, like, two years ago from even big names like Mermaids, who have either been proved wrong or backtracked.
I have pasted the article below. There are links in the original article.
----------------
Health Care
Evidence Undermines ‘Rapid Onset Gender Dysphoria’ Claims
Fears of “social contagion,” used to support anti-transgender legislation, are not supported by science
By Timmy Broderick on August 24, 2023
A recent study claiming to describe more than 1,600 possible cases of a “socially contagious syndrome” was retracted in June for failing to obtain ethics approval from an institutional review board. The survey examined “rapid-onset gender dysphoria,” a proposed condition that attributes adolescent gender distress to exposure to transgender people through friends or social media. The existence of such a syndrome has been the subject of intense debate for the past several years and has fueled arguments against transgender rights reforms, despite being widely criticized by medical experts.
The American Psychological Association and 61 other health care providers’ organizations signed a letter in 2021 denouncing the validity of rapid-onset gender dysphoria (ROGD) as a clinical diagnosis. And a steadily growing body of scientific evidence demonstrates that it does not reflect transgender adolescents’ experiences and that “social contagion” is not causing more young people to seek gender-affirming care. Still, the concept continues to be used to justify anti-trans legislation across the U.S.
“To even say it’s a hypothesis at this point, based on the paucity of research on this, I think is a real stretch,” says Eli Coleman, former president of the World Professional Association for Transgender Health. Coleman helped create the organization’s most recent standards of care for trans people, which endorse and explain the evidence for forms of gender-affirming care.
Many transgender people experience gender dysphoria, meaning that the gender that was assigned to them at birth and their gender identity don’t align, causing distress. ROGD was proposed as a gender dysphoria subtype in a 2018 paper by physician and researcher Lisa Littman, then at Brown University.* Littman’s survey asked parents of transgender adolescents—recruited predominantly from anti-transgender websites and forums—to describe their child’s “sudden or rapid onset of gender dysphoria” and to state if it coincided with increased social media usage or the child’s friends coming out as transgender.
Littman later issued a correction that updated the methodology, including a brief description of the websites and forums, and noted that ROGD is not a formal diagnosis. But the concept had already been taken upin books and podcasts—and by politicians—to promulgate the idea that peer pressure and social media are making kids transgender or that being transgender is a form of mental illness. As legislation targeting trans people has reached an all-time high in the U.S., ROGD’s alleged social contagion has been invoked by lawmakers in states such as Missouri, Utah and Arkansas to justify banning or restricting gender-affirming care for young people.
“This is just a fear-based concept that is not supported by studies,” says Marci Bowers, president of the World Professional Association for Transgender Health. The term ROGD is being used to “scare people or to scare legislators into voting for some of these restrictive policies that take away options for young people. It’s cruel, cruel legislation.”
Like the 2018 study that coined the term rapid-onset gender dysphoria, the recently retracted paper, which was published this March in Archives of Sexual Behavior, surveyed parents of transgender children about their children’s experiences. The study was co-authored by Michael Bailey, a psychologist at Northwestern University, and Suzanna Diaz, a pseudonym used by a mother of a child with gender dysphoria. Diaz is not affiliated with an institution and had already collected the survey data before collaborating with Bailey on the paper. The study was retracted because Diaz and Bailey did not get consent from the survey’s respondents to have their responses published, although Bailey disputes this. (Bailey declined to answer questions about the retraction from Scientific American.)
The participants in both the 2018 and the retracted 2023 studies were recruited from online communities that were explicitly critical about many aspects of gender-affirming care for transgender kids. Littman’s research was inspired in part by parents’ posts on these skeptical websites.
In response to criticisms that recruiting parents from anti-transgender websites may have biased the results, Littman says, “I reject the premise that parents who believe transition will harm their children are more likely to discredit their kids’ experiences than parents who believe that transition will help their children.”
Most experts cite the survey of parents rather than transgender children themselves as another major flaw in the methodology of both studies.
Diane Ehrensaft, director of mental health at the University of California, San Francisco, Child and Adolescent Gender Center, concurs. “To talk about what children are thinking, feeling and doing, particularly as they get old enough to have their own minds and narratives, you need to interview them,” she says.
Parents can often be the last to know about their child’s gender identity, Ehrensaft says. Coming out can be terrifying for many transgender kids. Family members often respond with violence or distrust or may even kick the child out of the house. Almost 40 percent of transgender youth experience homelessness or housing instability, according to a 2022 report from the Trevor Project, a nonprofit that provides crisis support for young LGBTQ+ people. Many kids who wait to discuss their gender identity with their parents before appearing to “suddenly” come out are simply keeping themselves safe, Ehrensaft says.
“It is not rapid-onset gender dysphoria,” she says. “It’s rapid-onset parental discovery.”
Many experts have also questioned what length of time qualifies as a “sudden” experience of gender dysphoria. Both the 2018 and 2023 studies left the definition up for parental interpretation. Complicating this, there isn’t one pathway or time line for being transgender, says Tey Meadow, a Columbia University sociologist who studies sexuality and gender. “For some people, it can evolve slowly. For others, it can evolve quickly,” she says.
For most transgender youth seeking gender-affirming care, considerable time elapses between when they realize they may be transgender and when they receive such care. A recent analysis of 10 Canadian medical centers in the Journal of Pediatrics found that 98.3 percent of young people seeking gender-affirming care had realized more than a year prior that they may have been transgender. “If ROGD were a real thing, we would expect to see two discernible streams of patients coming in [to receive care],” says Greta Bauer, a co-author of the study and director of the Eli Coleman Institute for Sexual and Gender Health at the University of Minnesota Medical School. There would be a distinct group of adolescents with more recent knowledge about their gender identity going to clinics and another group that had had such knowledge for years. “But we didn’t see that,” she says.
Thomas Steensma, a psychologist at Amsterdam University Medical Centers who provides gender-affirming therapy, says he has not seen evidence of the “social contagion” component of ROGD, and he cautions against even using these terms. “Rapid means out of control, and contagion signals a warning, and that warning induces fear,” he says. “There’s no evidence that certain developmental pathways are more problematic or less beneficial or helpful than others” for a child’s gender identity.
Steensma reports that he sees two “peaks” of referrals in his clinic: young adolescents and 15-year-olds. In a 2020 study Steensma and his colleagues looked at adolescent referrals from 2000 to 2016 and found no measurable difference in the psychological functioning or the intensity of the gender dysphoria between more recent referrals and those who came to the clinic starting in 2000. If adolescents are presenting with a different form of gender dysphoria, Steensma has not seen it.
The researchers did observe a change in their referral population in recent years, however. More kids assigned female at birth have been transitioning in recent years than those assigned male at birth. Many studies have captured this difference—including the 2018 survey proposing ROGD—but experts are unsure of its cause. Littman suggests that female-assigned kids are more susceptible to the “social contagion” of gender dysphoria because they feel social pressure more acutely than male-assigned kids. But Ehrensaft says nothing in the clinical literature corroborates this assertion. Instead she attributes this discrepancy to shifting cultural factors that influence how children express themselves and explore their identity. In our culture, Ehrensaft says, “there’s a lot more gender stress for the boy in the tutu than the girl in the football uniform.”
Other forms of gender incongruence, such as identifying as nonbinary or gender nonconforming, further challenge the idea that children should be forced to abide by traditional gender categories. And the best way to understand what kids are experiencing is to ask them questions and listen to their answers, Ehrensaft says.
“In some ways, [kids] are far more advanced than I am, as somebody in my 70s, about how they live and understand gender,” Ehrensaft adds. “So if we want to really understand gender, turn to the experts—and that would be the youth themselves.”
*Editor’s Note (8/24/23): This sentence was edited after posting to correct Lisa Littman’s occupation and her affiliation at the time of her 2018 paper.
#terfsafe#terfblr#radblr#radfems please touch#radfems interact#terfs please touch#terfs interact#radfem safe#radfemsafe
54 notes
·
View notes
Text
A new look at “Rapid Onset Gender Dysphoria" (ROGD), a transphobic pseudo-science

"While the ROGD theories claim that these people are 'becoming' trans, the truth is that we were always here."
Two papers pretending to prove that trans youth becomes trans because of social contagion have been redacted.
The first one, by Lisa Littman, asked parents visiting transphobic sites about the gender variance of kids, while the second, mentioned by Faefyx Collington in Into, was redacted this year due to lack consent from the participants.
Collington explains why ROGD is a pseudo-science:
The basic idea is that there are now more people being diagnosed with gender dysphoria and identifying as transgender and nonbinary because it is “cool” to do so...
While there has certainly been a significant rise in people coming out as trans, nonbinary, gender-non-conforming, etc., there is also a much simpler explanation...
The increase in our recognized population is centered around greater knowledge of trans identities and increased social acceptance, not some sort of “social contagion.”
Ultimately, this comes down to the same sort of survivorship bias that we see with things such as autism. Something that was once misunderstood or shunned by society is now more likely to be accepted and understood, and thus seems to be more common.
We also see this with the seeming increase in the number of lefthanded people from around 1910 to 1950. People weren’t suddenly becoming lefthanded; the idea of being lefthanded was simply no longer as likely to be demonized and people were less likely to try and beat or train it out of children.
Read the whole article here: Your favorite anti-trans pseudoscience is back but now it’s just sad
Photo: itchySan
#transgender#trans#lgbt#queer#nonbinary#genderqueer#rapid onset gender dysphoria#rogd#transphobia#science
23 notes
·
View notes
Text
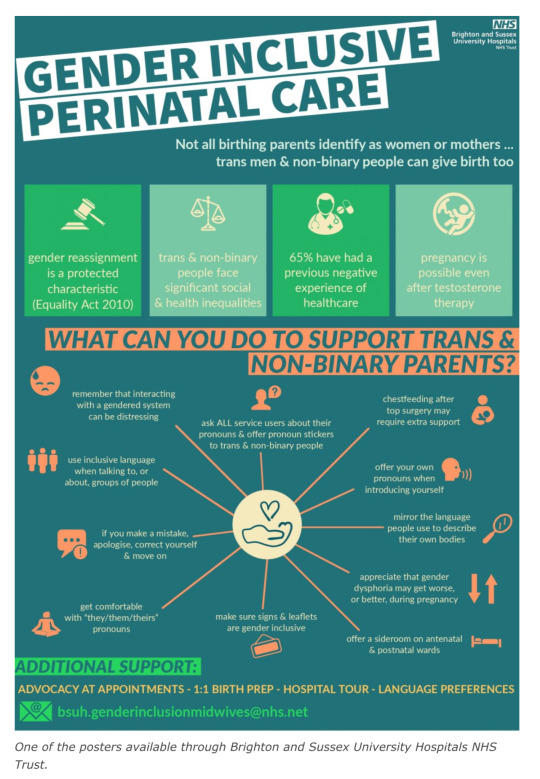
Dear English doctors - Biological males can’t get pregnant and there is no such thing as a “girl penis”. Please spend less time on worrying about language that appeases narcissistic men and more time improving care for women and babies.
England’s National Health Service (NHS) has put forward a £100,000 contract to create a “gender-inclusive” maternity care training program based on research guided by a trans-identified male who has claimed that men can give birth and that “pre-operative trans women” have “girl penises.”
On December 16, the NHS quietly released an Invitation to Quote for the “Maternity Gender Inclusion Program,” with a listed closing date for pilot submissions set for January 11th, 2023.
The contracted program is set to be rolled out to midwives in maternity departments across 40 NHS Trusts in England, and would be based on the findings of the Improving Trans Experiences of Maternity Services (ITEMS) research project, which was co-authored by a trans-identified male and is alleged to have “significant” flaws in its methodology.
With Woman, a maternity care advocacy coalition, penned an open letter highlighting the “flawed” research within the ITEMS publications, and has called for a complete pause on the contract offering entirely.
Speaking with Reduxx, a spokeswoman from With Woman raised multiple concerns, especially with the entirety of the program’s focus appearing to be on “inclusive” language and not improvements in medical care for a traditionally complex cohort.
With Woman noted that even the Invitation to Quote appears fixed, with the very short contracting and funding window raising suspicion. With Woman indicated their belief that there may be organizations already lined up to take the contract as the time frames are too brief for uninvolved organizations to adequately prepare a pilot.
The ITEMS report, which is being used as a justification for the need for the program, based its findings on the responses of just 121 people. The report determined that “birthing people” were improperly cared for because they were “misgendered,” and made unsubstantiated claims that 30% of “trans parents” secretly gave birth at home with no medical intervention.

The report was co-authored by Dr. Ruth Pearce, a trans-identified male Lecturer in Community Development at Glasgow University.
Pearce played a significant role in the direction of the ITEMS research. Pearce’s work focuses on “trans pregnancy” and “Queer, Trans and Feminist music scenes.”
In an essay posted on to his website, Pearce asserts that he is more attractive and confident than biological women.
“Quite frankly, I bet a whole load of women would love to be as confident and good looking as I am. I’ve got a pretty face, great hair, fantastic legs, and I’ve recently grown some rather shapely breasts.” He is also known for having once fronted a “queer feminist rage” music group through which he sang a song about his scrotum.
In an August 2022 video titled “Reproductive Justice for Trans People With Ruth Pearce and Francis White,” Pearce explains the focus of his work on ITEMS, policy and language surrounding “trans birth” and the need to highlight transgender people having children to counter the claims that a “trans child” may not reproduce, and to create media that contradicts Abigail Shrier’s claims that child transition can lead to “irreversible damage” of fertility.
Pearce called attention in particular to a phenomenon known as Rapid Onset Gender Dysphoria, which was coined by Lisa Littman and referenced by Jungian analyst and author Lisa Marchiano in a 2017 academic article titled “Outbreak: On Transgender Teens and Psychic Epidemics.”
In the article, Marchiano examines the role of social media in the sudden rise in teens claiming a gender identity, stating: “a young person’s coming out as transgender is often preceded by increased social media use and/or having one or more peers also come out as transgender.”

Pearce mocked the concept of children learning of transgender identities on social media, but later contradicted himself by discussing the issue in the presentation segment titled “We Are the Virus: Reproduction via Social Contagion.”
In the segment, Pearce asserted the need to help transgender-identifying people to not only sexually reproduce, but also to “socially reproduce” by means of altering medical language and policy to introduce the idea of transition to children and adults as a form of “reproductive justice,” thereby creating more transgender people.
In the video, Pearce acknowledged that social contagion is the method by which transgenderism proliferates, stating: “Alexis Davin noted that the very process that Lisa Marchiano and Abigail Shrier described as a social contagion is the means by which trans people engage in a form of social reproduction. We become visible to one another and introduce one another to a language that makes sense of our lives and our needs.”

Later in the seminar he continued, “I’ve been thinking a lot about social contagion because it’s the language of the anti-trans movement. But… the exact thing they’re describing is the exact means by which we reproduce ourselves.”
During the seminar, Pearce described the work he did with Brighton and Sussex University Hospitals (BSUH) NHS Trust, arguing for the need for “Gender Inclusive Language” to create “Language as Possibility” and posters that act as apparent recruitment advertising for the political transgender movement. Pearce elaborated by saying, “in Brighton and Sussex University Hospitals, that’s a really interesting example of queer spaces of care being created through an institution rather than through more radical networks.”
Pearce’s involvement with the ITEMS research, as well as its use to justify an NHS maternity program, comes less than one year after NHS negligence was found to have been responsible for the needless deaths of over 200 babies and 9 mothers at at Shrewsbury and Telford NHS Trust. According to internal investigations, “repeated failures in the quality of care and governance” was to blame for the deaths, which spanned over 2 decades, with an additional 1,486 families and 1,592 incidents being recorded as a result of inadequate maternity care oversight.
Reduxx has previously revealed how errors and confusion arose due to the use of inaccurate medical language which led to midwifery students at Napier University in Edinburgh being taught how to care for males giving birth through penises and prostates.
According to a course workbook, students were advised: “It is important to note that while most times the birthing person will have female genitalia, you may be caring for a pregnant or birthing person who is transitioning from male to female and may still have external male genitalia.”
#England#England’s National Health Service (NHS)#Trans Identified Male talking about maternity care#Men can’t have babies#With Woman#“Maternity Gender Inclusion Program#Improving Trans Experiences of Maternity Services (ITEMS)#Dr Ruth Pearce is a man#Dr Ruth Pearce is another TIM who thinks he is better than actual women#Reproductive Justice for Trans People With Ruth Pearce and Francis White#Gender identity and social contagion#It’s bigoted for critics to mention the link between social media and gender identity#But it’s ok for trans people to call gender identity a social contagion
102 notes
·
View notes
Text
Some of my views on trans topics
Some increased number of youth have been diagnosed with gender dysphoria due to the reduction of false negatives in recent years. This is good. (Cf. discourse on autism, as well as increase in recognition of left-handedness, and similar topics). Also some youth have come to identify as trans *without* gender dysphoria. I claim this is good OR neutral.
If gender dysphoria has increased, which has *maybe* happened (or maybe not), this would probably be *somewhat* bad (w/ caveats)-- insofar as dysphoria (i.e. a kind of feeling bad) is bad. (I think feeling bad is bad!!!) However, this has not been *shown* to have happened. Evidence for this claim is highly indirect at most.
Relatedly, all the (few) "Rapid Onset Gender Dysphoria" studies seem to be garbage or of highly suspect quality (e.g. Lisa Littman & a few follow-ups by her and others).
I cannot rule out the possibility that a very few people may have something like ROGD. Similarly for "autogynephilia" and "homosexual transsexuality" (Blanchard-Bailey-Lawrence). Also, I make no judgment against anyone who may have such conditions, if there are any. Which maybe there are. (But for some criticism, see Julia Serano's several essays and posts against Blanchardianism.) I think the whole AGP/HSTS theory is likely bunk-- but *if* some properly nuanced version of it is legit, I think that's basically okay.
For instance, I think Tailcalled (Survey-Anon) is a really decent and reasonable Blanchardian.
I know for a fact there are a lot of people who consider themselves AGP, and I suspect there are some people who consider themselves to be HSTS or ROGD (which I've heard secondhand, but not firsthand). However, unlike perhaps some people, I don't consider someone's (gender-related or otherwise) self-identification to be a sufficient reason that the rest of us ought to agree uncritically with their own theory (although I think a certain degree of respect is called for-- and this goes for trans [and cis] people whose self-conceptions I see no reason to disagree with, and for trans [and cis] people whose self-conceptions I see some reason to disagree with).
(Similarly, I think it's fine for pretty much anyone to disagree with some religious people's self-identification, and with some Dissociative Identify Disorder patients' or multiples' self-identification, among others. For that matter, I think it's okay to disagree with the self-identification of some people who consider themselves to be persons, if e.g. you have a Parfitian theory or error theory regarding personhood, or if you believe there is merely matter in motion, etc.)
One big reason to be open to disagreeing with some trans people's self-identification is that there are some trans women who say "I'm actually a man (or male)" or similar assertions. This is an interesting puzzle for some versions of self-ID theory. You can easily find these posts on gender-critical feminist blogs, who reblog these sorts of posts frequently (for obvious reasons). Also some trans people are traditionally religious (e.g. some of them think they have male or female or other gendered souls) or have weird gender theories (which are, in some sense or other, a commonplace in all philosophical literatures, gender-related and otherwise, including secular)-- and I think it's fine to believe they are mistaken. I think this is of some interest, despite the dubious place that many gender-critical feminists are coming from.
To be honest, I think the gender-critical feminist movement is broadly fascist or at least fascist-adjacent, even though some of them are reasonable and decent people on an individual level (much like anti-abortionists, some of whom are reasonable and decent individually, even though their movement is insane, misogynist, and often fascist). This does NOT mean every gender-critical feminist is fascist on a personal level. However, if you are trans or a trans-ally, I also think (on e.g. freedom-of-association grounds, despite my not being a capitalist libertarian) that you do not *have* to associate with people who very much do *not* validate the legitimacy of trans people's identities.
I honestly do not think I am very biased on this topic, contrary to common allegations that all skeptics are biased. (Zack Davis, among others, seems to make this assertion.) This is for many direct and indirect reasons. Unlike some people, I would not care much if ROGD or Blanchardianism (AGP/HSTS) were true, but I think there are many reasons to consider these views most likely untrue-- both in general, and for a sizeable majority of trans people.
It is hard to emphasize enough how unbiased I think I am on this topic, both for personal and intellectual reasons.
I understand there is a lot of actual and perceived bias on this topic, in regard to wokeness or political correctness or suchlike, so I don't know how to prove this. But IF I believed that (say) trans women were in fact men, then I believe I would say so openly. I'd make some serious effort toward saying this respectfully, but I *would* say it, and I'd say it directly. I do not say so, because I do not believe so.
I think a lot of people think there is widespread dishonesty on this topic. Quite possibly there is. Many people would be yelled at if they said openly that they believed trans women were men, so this is some reason to think many people wouldn't say so even if they believed so. But I swear I'm not being dishonest on this topic.
All that said, the ROGD studies appear to suck, so likely ROGD isn't common, and allegations otherwise are bunk and most likely very biased. (I also suspect AGP and HSTS are bunk, although I admit my allegation on this matter is more complex and less blatantly correct.)
I think gender dysphoria (in itself) is bad-- insofar as dysphoria (i.e. a type of feeling bad) is bad. I disagree with some number of trans advocates who think curing gender dysphoria (i.e. successful conversion therapy) would be bad in itself. Also it seems plausible to me that gender-critical feminists such as Holly Lawfort-Smith are correct in saying that the failure of trans-conversion therapy has been exaggerated. However, I also think wanting to transition is basically okay (at whatever age, including under 18 and under 13), and I disagree with the view that transition per se is bad (apart from the inconvenience and cost, which I grant is somewhat bad in itself).
Also, I reject transmedicalism and the notion that one needs to have gender dysphoria to be trans. I also (approximately) affirm self-ID as sufficient without dysphoria. So if & insofar as some increased number of young people have come to self-ID as trans (trans men, women, nonbinary), even if they don't have gender dysphoria, I think this is totally fine.
If some increased number of young people self-identify as trans due to a "trend" or "social contagion," or even a "paraphilia" (with various caveats), then I think that's cool, this is fine.
Cry about it.
15 notes
·
View notes
Text

Abstract
The study’s purpose was to describe a population of individuals who experienced gender dysphoria, chose to undergo medical and/or surgical transition and then detransitioned by discontinuing medications, having surgery to reverse the effects of transition, or both. Recruitment information with a link to an anonymous survey was shared on social media, professional listservs, and via snowball sampling. Sixty-nine percent of the 100 participants were natal female and 31.0% were natal male. Reasons for detransitioning were varied and included: experiencing discrimination (23.0%); becoming more comfortable identifying as their natal sex (60.0%); having concerns about potential medical complications from transitioning (49.0%); and coming to the view that their gender dysphoria was caused by something specific such as trauma, abuse, or a mental health condition (38.0%). Homophobia or difficulty accepting themselves as lesbian, gay, or bisexual was expressed by 23.0% as a reason for transition and subsequent detransition. The majority (55.0%) felt that they did not receive an adequate evaluation from a doctor or mental health professional before starting transition and only 24.0% of respondents informed their clinicians that they had detransitioned. There are many different reasons and experiences leading to detransition. More research is needed to understand this population, determine the prevalence of detransition as an outcome of transition, meet the medical and psychological needs of this population, and better inform the process of evaluation and counseling prior to transition.
Sir,
Bustos et al1 aimed to measure the prevalence of regret following gender-affirmation surgery. Given the significant rise in young people seeking medical intervention for gender dysphoria, which can include surgery, outcome studies that accurately assess regret are of increasing importance. In this letter, we argue that the conclusions of their systematic review and meta-analysis are questionable due to limitations in their methods and shortcomings of the studies selected.
Starting with methods, the authors overlooked numerous relevant studies, including one of the best-known,2 raising questions about the adequacy of their search strategy. One study3 was inappropriately included as it only investigated regret regarding choice of surgical procedure, not of surgery itself. In addition, there are significant data extraction errors, leading to erroneous conclusions. For instance, the sample for surgical regret in their largest included study4 was inflated from 2627 to 4863, likely due to a miscalculation from a table reporting the treatment patterns of that paper’s total study population.
Besides these methodological inaccuracies, data in this field are often of low quality because of “lack of controlled studies, incomplete follow-up, and lack of valid assessment measures,”5 as well as the long amount of time regret can take to manifest (the average and median are estimated at 8–8.5 years2,4). Many of the included studies had participants with follow-up periods of only 1 or 2 years postsurgical transition. None appear to have a long enough follow-up period to reliably identify regret. The study contributing almost half of the participants4 explicitly noted their inclusion of participants with short follow-up time, relative to time to regret, and their large 36% loss to follow-up as limitations. These shorter studies only provide an estimated lower limit, as the large numbers of patients lost to follow-up add correspondingly large uncertainties to any quoted number.
Bustos et al1 acknowledge “moderate-to-high risk of bias in some studies.” Actually, this affects 23 of the 27 studies. The majority of included studies ranged between “poor” and “fair” quality: only five studies—representing just 3% (174) of total participants—received higher quality ratings. However, even these had loss to follow-up rates ranging from 28% to more than 40%, including loss through death from complications or suicide, negative outcomes potentially associated with regret.
A last and major concern involves sample selection. The cohort presenting with gender dysphoria today is substantially different from the cohort presenting during the research periods of the included studies. Further, there has been a significant liberalization over time of the criteria assessing readiness for surgery. Thus, the outcomes reported may be of limited relevance for estimating current surgery outcomes. Additionally, the generalization to “TGNB” populations seems unreliable, as it is based on an explicit sample size of only one “non-binary” patient. The authors do not address these issues.
In light of these numerous issues affecting study quality and data analysis, their conclusion that “our study has shown a very low percentage of regret in TGNB population after GAS” is, in our opinion, unsupported and potentially inaccurate.
Abstract
Two Dutch studies formed the foundation and the best available evidence for the practice of youth medical gender transition. We demonstrate that this work is methodologically flawed and should have never been used in medical settings as justification to scale this “innovative clinical practice.” Three methodological biases undermine the research: (1) subject selection assured that only the most successful cases were included in the results; (2) the finding that “resolution of gender dysphoria” was due to the reversal of the questionnaire employed; (3) concomitant psychotherapy made it impossible to separate the effects of this intervention from those of hormones and surgery. We discuss the significant risk of harm that the Dutch research exposed, as well as the lack of applicability of the Dutch protocol to the currently escalating incidence of adolescent-onset, non-binary, psychiatrically challenged youth, who are preponderantly natal females. "Spin" problems—the tendency to present weak or negative results as certain and positive—continue to plague reports that originate from clinics that are actively administering hormonal and surgical interventions to youth. It is time for gender medicine to pay attention to the published objective systematic reviews and to the outcome uncertainties and definable potential harms to these vulnerable youth.

Abstract
Introduction
Concerns about future regret and treatment discontinuation have led to restricted access to gender-affirming medical treatment for transgender and gender-diverse (TGD) minors in some jurisdictions. However, these concerns are merely speculative because few studies have examined gender-affirming hormone continuation rates among TGD individuals.
Methods
We performed a secondary analysis of 2009 to 2018 medical and pharmacy records from the US Military Healthcare System. We identified TGD patients who were children and spouses of active-duty, retired, or deceased military members using International Classification of Diseases-9/10 codes. We assessed initiation and continuation of gender-affirming hormones using pharmacy records. Kaplan-Meier and Cox proportional hazard analyses estimated continuation rates.
Results
The study sample included 627 transmasculine and 325 transfeminine individuals with an average age of 19.2 ± 5.3 years. The 4-year gender-affirming hormone continuation rate was 70.2% (95% CI, 63.9-76.5). Transfeminine individuals had a higher continuation rate than transmasculine individuals 81.0% (72.0%-90.0%) vs 64.4% (56.0%-72.8%). People who started hormones as minors had higher continuation rate than people who started as adults 74.4% (66.0%-82.8%) vs 64.4% (56.0%-72.8%). Continuation was not associated with household income or family member type. In Cox regression, both transmasculine gender identity (hazard ratio, 2.40; 95% CI, 1.50-3.86) and starting hormones as an adult (hazard ratio, 1.69; 95% CI, 1.14-2.52) were independently associated with increased discontinuation rates.
Discussion
Our results suggest that >70% of TGD individuals who start gender-affirming hormones will continue use beyond 4 years, with higher continuation rates in transfeminine individuals. Patients who start hormones, with their parents’ assistance, before age 18 years have higher continuation rates than adults.
#Christina Buttons#Leor Sapir#Dr. Phil#Lisa Littman#detrans#detransition#transition regret#medical scandal#medical malpractice#medical corruption#evidence based medicine#gender affirming care#gender affirming healthcare#gender affirmation#religion is a mental illness
3 notes
·
View notes
Quote
Many of the College’s most radical views target transgender people, and in particular, transgender youth. The leak, which had been indexed by Google, includes volumes of literature crafted specifically to influence relationships between practicing pediatricians, parents, and their children. It includes reams of marketing material the College aims to distribute widely among public school officials. This includes pushing schools to adopt junk science painting transgender youth as carriers of a pathological disorder, one that’s capable of spontaneously causing others–à la the dancing plague–to adopt similar thoughts and behaviors.
This is one of the group’s most dubious claims. While unsupported by medical science, it is routinely and incuriously propagated through literature targeted at schools and medical offices around the US. The primary source for this claim is a research paper drafted in 2017 by Lisa Littman, a Brown University scholar who, while a medical doctor, was not specialized in mental health. The goal of the paper was to introduce, conceptually, “rapid onset gender dysphoria”—a hypothetical disorder, as was later clarified by the journal that published it. Littman would also clarify personally that her research “does not validate the phenomenon” she’d hypothesized, since no clinicians, nor individuals identifying as trans, had participated in the study.
The paper explains that its subjects were instead all parents who had been recruited from a handful of websites known for opposing gender-affirmative care and “telling parents not to believe their child is transgender.” A review of one of the sites from the period shows parents congregating to foster paranoia about whether there’s a “conspiracy of silence” around “anime culture” brainwashing boys into behaving like girls; insights plucked in some cases straight from another, more insidious forum (widely known for reveling in the suicides of the people it has bullied).
American College of Pediatricians Leak Exposes 10,000 Confidential Files | WIRED
19 notes
·
View notes
Text
This is a copy of the letter I mailed to the surgeon who performed my double mastectomy or “top surgery” when I was 20 years old. This letter, addressed as a “Notification of Detransition” was mailed to the cosmetic surgeon. I wrote this letter to inform the doctor and his staff that a former patient of his 100% regrets the operation performed on her, and has detransitioned and is now living as a biological female with no functioning breasts.
I kept the letter short and emotionally detached and, despite my traumatic feelings around this loss of self and body parts in my private life, knew it was crucial to maintain a rational composure in stating the facts of my situation. I described how my gender dysphoria was not cured by surgery or medical transition, but instead was fully resolved within 2 years through cognitive behavioral therapy, because the “gender dysphoria” was in reality, complex post-traumatic stress disorder. I described how I realized, only 2 years later at age 22, that the surgery had been a mistake, and that I didn’t receive proper mental health treatment when I was obtaining the surgery, the supposedly necessary gatekeeping he required to perform the operation.
This was important to include because, although I doubt as a cosmetic surgeon who has made his career entirely dedicated to performing double mastectomies on young women and girls as young as 16, that he cares about the mental wellbeing of his cliental, he advertises his practice as being a legitimate medical service by insisting that he follows the “WPATH Standards of Care”, the leading organization of trans medicine which requires at least 2 letters of referral from mental health providers for a patient to receive medical transition. The Standards of Care advocate for thorough screening for mental wellness, and selecting only appropriate patients who would truly benefit from transition.
It was crucial to inform the doctor that, in my case, the Standards were not met, as the mental health care I was receiving, and the subsequent referral letters, were negligent in providing assessment of my mental health situation, and therefore, his practice was not actually following the WPATH Standards of Care. Furthermore, what I did not include in the letter due to a desire to preserve my anonymity, was the fact that I openly discussed being suicidal with the doctor during our consultation, and feeling suicidal on the day of the actual surgery. Regardless of the recommendation letters, I presented to my doctor as not of sound mind to make a major elective surgical decision, but he performed the operation anyway.
After relaying my personal beliefs that this treatment was unethical in my case, I made it known to my doctor that I am far from the only former FTM patient who regrets medical transition, and cited Dr. Lisa Littman’s study of detransitioners showing how high the comorbidity rates are of various mental disorders in the FTM population, and how this issue is not just a personal error, but a growingly widespread phenomenon. I closed the letter with a call to action for the doctor to reconsider what his practice views as ‘medical treatment’ to treat mental disorders. I plainly asked him to confront the reality that he removes young women’s and even minor children’s breasts to treat problems inside their minds, and if he truly believes that is following the medical oath to “Do No Harm.”
My story is similar to many detransitioners who share why they felt they needed to transition. I grew up on the autism spectrum, experienced verbal, emotional, and psychosocial abuse from family resulting in PTSD, depression, and anxiety, had severe depression from attachment issues and hormonal dysregulation from PCOS, felt chronically othered and different as a girl, young woman, and person, suffered with relationship difficulties with romance, sex, and friendship due to undiagnosed trauma, and latched onto “gender dysphoria” as the cause of most of my difficulties.
I sought treatment for my gender related distress and learned online that the only solution was to accept being transgender and transition to live as a gay man. I followed the usual coaching of the process to “healing”, first, to socially transition and come out as nonbinary and transgender, second, to receive hormones from an informed-consent clinic, with no mental health evaluation or gatekeeping, and finally to have top surgery, the greatest rite of passage for the FTM cult. Throughout this process I saw multiple doctors, a psychiatrist, and therapists, none of whom questioned my identity, traumas, or provided help for my complex mental health issues. I had just turned 20 and was fresh out of an inpatient psychiatric ward for suicidal ideation when I desperately made my appointment to try and heal my depression through altering my body with surgery.
There is no need for further explanation. I was 20, developmentally immature, mentally ill, suicidal, had PTSD, and not in a rational state of consciousness, yet the mental health system failed to provide its due service, and my doctor and other cosmetic surgeons hungrily leapt at the opportunity for fresh meat to profit from operating on, in this unchecked, wild west market for “gender medicine.”
I share this letter with you to showcase real-life consequences of trans medical propaganda, and the repercussions our young people and children are facing. The last I checked; my doctor operates on girls as young as 16. I’ve done my soul-searching, grieving, extensive therapy, and self-punishment for the mistakes of my childhood self, but am healed enough to have progressed into self-forgiveness, acceptance, and upholding unrelenting boundaries around my peace, sanity, and healing process. I did not provide a return address on the letter I mailed, as I did not want to endure excuses or shaming correspondences.
The letter remains a rallying cry from the young women of the detrans movement to advocate for better medical treatment, no placation or bullshit apologies desired. I don’t claim to speak on behalf of anyone else, but unfortunately appreciate that my story is identical to countless other girls, and I hope that sharing this will somehow help them heal, or better yet, prevent the need for their healing in the first place.
—
Dear Dr. XXXX and Top Surgery Clinicians,
I am a former patient who you performed a double incision mastectomy on in 2017 while I was 20 years old. I am writing to inform you and your office that I have detransitioned and no longer identify as male/transgender and have returned to living fully as my biological female sex. I want to inform you that I fully regret having the surgery to have my breasts removed. My symptoms of gender dysphoria were the result of CPTSD from childhood abuse and my transgender identity was a maladaptive coping mechanism to deal with the reality of the trauma.
I have fully resolved my feelings of gender dysphoria through cognitive behavioral therapy and view the surgery and transition as a placebo that gave me only false hope of feeling better about myself. I 100% regret the surgical outcome of my body and miss having my healthy breasts. I was 20 when I had my identity crisis and detransitioned 2 years later at 22. I believe I did not receive proper mental health screening by my psychiatrists who wrote my surgery recommendation letters because they said I was mentally stable while I was actually suicidal and exhibiting symptoms of undiagnosed PTSD.
I have found healing and community within the online population of other detransitioned women with similar experiences of trauma, and I want to inform you that I do not believe removing the breasts of young women, especially minors, is medically ethical given the severe rates of comorbid mental health issues in the FTM population. I do not believe I was stable or mature at 20 to transition and I don’t think a minor child under 18 in any circumstance is stable or mature to consent to having her breasts removed.
There is a rising number of detransition cases just like mine as evidenced by the rapid increase of detrans stories on Youtube, and the Subreddit r/detrans. There has also been a recent study by Lisa Littman at littmanresearch.com on detransition which shows that 60% of the detrans study participants transitioned due to underlying mental health and trauma reasons, and 25% due to being lesbian or gay.
I ask you to consider my story and the stories of others as your ethical duty as a clinician to first do no harm, and rethink if removing healthy breasts of women and children so they can pretend to be men is physically or mentally doing no harm.
Your patient, Laura
52 notes
·
View notes
Text
Una delle scuole più prestigiose d'America, la Brown University, ha visto un'impennata degli orientamenti sessuali LGBTQ negli ultimi dieci anni, con quasi quattro studenti su dieci che ora si identificano come qualcosa di diverso dall'eterosessuale.
Un sondaggio del mese scorso del quotidiano dell'università della Ivy League, il Brown Daily Herald, ha rilevato che il 38% degli studenti ora si identifica come LGBTQ. Ciò si confronta con il 14% nel 2010, il primo anno da cui erano disponibili i dati.
La maggior parte dell'impennata è avvenuta negli ultimi tre anni. In effetti, quasi l'80% degli studenti si identificava ancora come eterosessuale nel 2019. Un rapporto del Washington Examiner di domenica ha suggerito che il balzo di Brown nell'identificazione LGBTQ riflette un "contagio sociale" - piuttosto che un drammatico cambiamento negli orientamenti sessuali del corpo studentesco o un improvviso aumento della fiducia nell'esprimere apertamente le identità LGBTQ.
Lisa Littman, una ricercatrice sulla disforia di genere che in precedenza era assistente professore alla Brown, ha sostenuto che alcuni giovani si identificano come transgender a causa della pressione dei pari. Uno studio dello scorso anno del Centro statunitense per lo studio della partigianeria e dell'ideologia ha rilevato che i tassi di identificazione LGBTQ vanno dal 51% al 70% in tre delle scuole private di arti liberali più elitarie d'America: i college Oberlin, Wellesley e Smith. (Fonte: RT - Tramite Laura Ruggeri)
🔴 Per ricevere tutti gli aggiornamenti segui Giorgio Bianchi Photojournalist
Emulazione...
2 notes
·
View notes
Text
TW: Transphobia
If you see a news article claiming that a “new study is proving that transgenderism is socially contagious among teen girls.” I’ll save you the vitriol filled article. It’s not new, it’s not even a valid study. It’s just the 2018 Rapid Onset Gender Dysphoria “study.”
For those unfamiliar the ROGD paper was written by Dr. Lisa Littman and suggested that there was a modern phenomenon of teens becoming transgender due to social pressure.
Littman did not include a single transgender person or even teen in her “study.” Her entire sample was of parents of transgender children that she gathered from openly anti trans websites.
No accredited medical institution recognizes ROGD as a valid medical diagnosis or phenomenon. It has been widely renounced as “fake science.” Not only has no study that includes transgender individuals supported the claims Littman made, countless have directly contradicted them.
If you have to make up science to justify oppression, then oppression isn’t justified.
I love you all, stay safe. My DMs are open if you need a break from the transphobia.
Here’s some reading:
Littman’s Paper
#trans#queer#rogd#transphobia#transisbeautiful#trans rights#transfem#transmasc#nonbinary#TERFs dni#transgender#transgirl#trans boy#gender#gender queer#genderqueer#genderfluid#stay safe#and do some goddamn research ffs
6 notes
·
View notes
Last Seen Blogs

gbdreamers
G.B.Dreamers
life-around-me-yura15cbx
Life around me

laydownmyhead
Tired
zrclk
zero o'clock

eizerartz
EIZER