#Critical Illness Polyneuropathy
Text
Low Carb vs Insulin Sensitivity
Hello my lovelies I am having an autoimmune flare presently and this has triggered the symptoms of Reactive Hypoglycemia (RH for short) as well. So it took several days before I could continue this blog post today. The flare I think was on its way a few days ago as I started waking up more than usual. My blood glucose which was fairly stable, started waking me up with autoimmune symptoms and…

View On WordPress
#alternative#Alternatives#anxiety#autoimmune#autoimmune disease#autoimmune health#autoimmune reactions#autoimmunity#belly health#Biology#Blog#blogger#blood#blood disorders#blood glucose#blood sugar#blood sugar levels#bowel health#Brain health#breathing#breathing problems#Carbohydrates#carbs#children&039;s health#chilli pepper#Chronic Illnesses#Cooking#Critical Illness Polyneuropathy#Diabetes#Diabetes management
0 notes
Text
»
The poisoned donor blood of those vaccinated
The medical catastrophe caused by Covid vaccinations is becoming more and more unprecedented. Now it comes out: blood from vaccinated people contains the dangerous spike proteins .
It has been clear to a critical minority of doctors, which also includes the group of colleagues writing at Achgut , since the summer of 2020 that the so-called “vaccines” against SARS-CoV-2 are actually gene therapeutics that have no effect against the pathogen but are toxic . The suspicion soon arose that the blood of “vaccinated” blood donors could poison the recipients. This question is now addressed in a scientific review from Japan by Ueda et al. after.
…
1. Blood clotting disorders such as platelet deficiency (thrombocytopenia), deep cerebral venous thrombosis or pulmonary embolism, all of which are fatal or often cause severe chronic damage.
2. Deformation of erythrocytes (red blood cells), contamination of the blood with residues from vaccine production as well as inflammation and autoimmune diseases caused by the lipid nanoparticles (BioNTech and Moderna).
3. Damage to all organs due to the production of the spike protein in the blood vessel endothelia and the parenchymatous (function-bearing) cells of the organs. The best-known examples are myocarditis and glomuerulonephritis (destruction of the kidney). This also includes the damage to the fetus caused by vaccinating pregnant women, which may have led to the largest decline in the birth rate ever recorded in 2022.
4. Vaccine-induced autoimmune diseases. These will continue to make people sick in the next few years who were last “vaccinated” in 2021, because it can take years before the resulting organ damage becomes clinically visible. Many organs tolerate partial cell failure and only functionally fail when half or more of the parenchyma is destroyed.
5. VAEH and VAIDS, which are immune deficiency caused by vaccination and increased likelihood of contracting COVID. This can also lead to an increased likelihood of other infectious diseases, as well as a greatly increased risk of developing cancer and having a worse course of the disease than unvaccinated people (so-called turbo cancer). An important mechanism of these syndromes is overproduction of IgG4.
6. Central neurotoxicity due to direct organ damage to the brain through spike-induced formation of amyloid, which can lead to cognitive deficits and even dementia.
7. Damage to the peripheral nervous system with severe syndromes such as Guillain-Barré (a polyneuropathy with muscle weakness) or causalgia (diffuse burning pain throughout the body).
First, the highly toxic spike protein is found in the blood of those vaccinated, especially if they donated shortly after vaccination. They can harm the recipient.
Second, the blood products may contain lipid nanoparticles that can transfect the recipients, giving them an undesirable vaccination effect like a vaccinee. The particles themselves promote inflammation and can also trigger a so-called adjuvant-induced autoimmune disease in the transfusion recipient, regardless of the effect of the spike protein.
Third, the donor blood may contain thrombi (blood clots) that harm the recipient, for example through microinfarcts in the brain.
Fourth, due to their immunodeficiency, donors may be acutely or chronically infected with pathogens that are in the blood. These can be transmitted to the recipients and also make them permanently ill, because infection through the bloodstream is much more dangerous than through natural routes (such as breathing or eating).
Fifth, amyloids and amyloid microtubule aggregates form in the bodies of the vaccinees. These are tiny protein clumps that consist of aberrant spike-induced proteins, such as those found in Alzheimer's, and the remains of the cytoskeleton of cells destroyed by vaccination. These amyloids and aggregates are toxic and can cause organ and brain damage.
Sixth, the donor blood contains IgG4-positive plasma cells (a special type of immune cell), which can trigger chronic inflammation in the recipient.
«
[source]
Apparently we not only need a dating platform for unvaccinated people, but also something like a separate blood donation for purebloods.
People think it's over, but the poison is in them, especially the boosted ones. The birth rate is falling significantly with many more miscarriages, and sudden deaths.
Those who survive this madness in the next 20 years will face a completely other world.
4 notes
·
View notes
Text
I have a pt who had an emergent splenectomy and evacuation of hemoperitoneum at an outside hospital who was then transferred to my hospital for ICU care, had status epilepticus likely 2/2 EtOH/benzo withdrawal, was intubated in ICU, and is now weak and aphasic. She has PMH of autoimmune hepatitis, EtOH use d/o and takes clonazepam. So they think she seized 2/2 withdrawal from EtOH or clonazepam. We did stroke w/u and MRI brain and CTA head/neck were negative for ischemia or mass or any findings to explain her weakness and aphasia. So she apparently didn't have a stroke. A case manager asked for a diagnosis so pt can be transferred to rehab. My senior suggested critical illness polyneuropathy. It doesn't explain her aphasia though. Will read up on critical illness polyneuropathy.
4 notes
·
View notes
Link
Neuromuscular evaluations proved useful in most of these patients with long COVID. However some symptoms, exam changes and test results may have been false-negative, given that assessments were not often optimally timed (e.g., #6) and many patients reported care delays. This reported case of multifocal motor neuropathy (Figure 1) increases the spectrum of COVID-associated dysimmune neuropathies. Critical illness neuropathy—reported in approximately 10% of intubated patients with COVID—is attributed to various prolonged insults including intense inflammation and nerve compressions.6 Inherent study limitations include bias toward referrals for sensory neuropathy and underpowering. The initial evaluations reported occurred at varying times during the illness and treatment, whereas longitudinal assessments at standardized intervals are ideal for diagnostic and treatment decisions. Timing also complicates analysis of blood testing for immune markers (not shown). We screened patients with newly diagnosed neuropathy for all common established causes of distal sensory neuropathy, including routinely measuring ANA, ESR, IgG anti–SS-A/SS-B antibodies, and complement components C3 and C4, the most productive markers of dysimmunity in initially idiopathic SFN.7 We did not detect evidence of Sjögren syndrome, and other inflammatory markers were only occasionally elevated. Interpretation is complex as early elevations could be nonspecifically associated with acute COVID, and many months later, inflammation and markers might have subsided leaving residual axonopathy as the proximate cause of current symptoms. Regeneration can take up to 2 years or be incomplete. These results identify small-fiber neuropathy as most prevalent in this small group of patients with long COVID, also known as post-acute sequelae of SARS CoV-2 infection.2 In SFN, the small-diameter unmyelinated and/or thinly myelinated sensory and autonomic fibers are predominantly affected, although most patients with severe or advanced polyneuropathy, e.g., case 9, develop large- and small-fiber damage. The small fibers are disproportionately vulnerable, with their lack of myelin exposing them to environmental stressors including immunity, while inability to use saltatory conduction increases metabolic demand, and cytoplasmic paucity limits axonal regeneration. However, small-fiber axons grow throughout life to reinnervate continuously dividing tissues such as the skin and to help repair injuries. If toxic conditions improve, axon elongation and sprouting accelerate to increase the probability of reinnervating enough target cells to resolve symptoms. Here, most patients treated with sustained IVIg, the primary treatment for inflammatory neuropathy, with preliminary evidence of effectiveness for dysimmune SFN,8 perceived improvement (e.g., Figure 1, eFigure 1, links.lww.com/NXI/A697). Some treated only with corticosteroids did as well; participant 3 reported that prednisone helped her toward 90% improvement and was discontinued only because of adverse effects. Others improved substantially without immunotherapy (e.g., case 17), documenting spontaneous recovery and need to individualize treatment decisions. The hypothesis that some long COVID symptoms reflect underlying small-fiber pathology is supported by research observation of small-fiber loss applying in vivo corneal confocal microscopy to patients with long COVID.9 As with other post-COVID neurologic illnesses, susceptibility to inflammatory mediators appears essential. Autopsy study of post-COVID patients identified neuritis with perivascular macrophage infiltrates but no viral antigens, implicating inflammatory immune responses rather than direct infection. In addition, 1/4th of human DRG neurons express mRNA for SARS-CoV-2–associated receptors and deploy ACE2 protein. Thus, virus or spike protein fragments may attach to them, promoting formation of antibodies that can also target adjacent neural epitopes. Here, the slightly delayed onsets, prolonged postinfectious courses, and apparent responses to continued immunotherapy suggested dysimmune mechanisms. This report strengthens evidence linking several idiopathic multisymptom conditions—including SFN and fibromyalgia—with dysimmunity, sometimes incident to infections or vaccinations.2 As with COVID-incident Guillain-Barré syndrome and all referral-based case series, the current cases neither confirm causality nor the clinical significance or magnitude of any association. However, identifying small-fiber neuropathy and multifocal motor neuropathy in 1 small sample of patients with WHO-defined long COVID provides rationale and preliminary data for larger investigations and may influence interim medical evaluations of similar patients.
0 notes
Photo

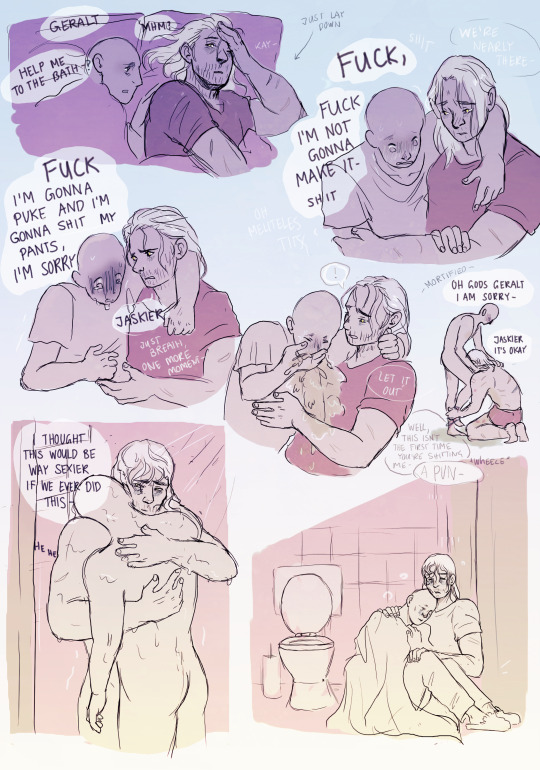

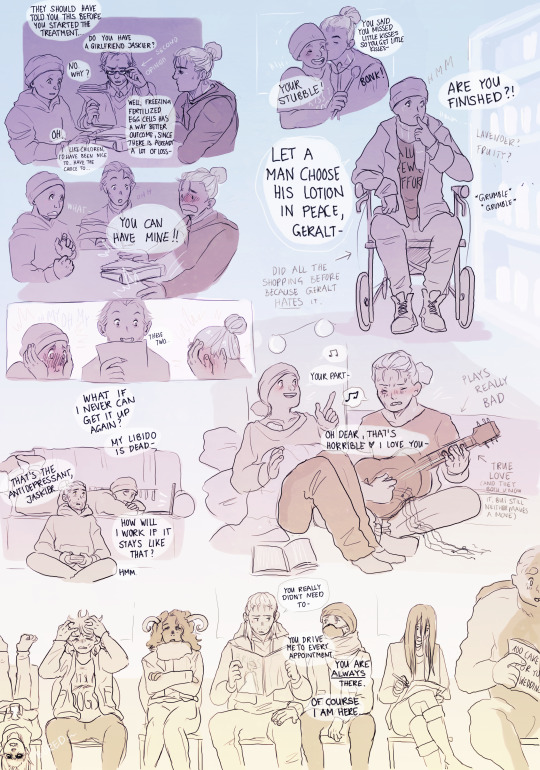

Things are hard, but they have many happy moments too.
[Masterpost]
Jaskier started out with a thyroid tumor here (which was more or less my modern take on the djinn) but things got complicated after that. There are also (here and there) little hints of what it means to be a witcher in that universe, but we will see if I get to draw more of that!
(the rest of the wolves are gonna be so pissed once they find out.)
This is still pre-relationship, since this is a flashback, but it’s also not an completely unknown quantity between them that they love each other. This somehow ended up being the slowest slowburn that ever burned, but with them (while not knowing for sure) also kinda recognizing what simmers there and in which direction they are moving.
#onlyfans!jaskier#trans!geralt#geraskier#modern!geraskier#jaskier#cancer tw#critical illness tw#vomit tw#vomit cw#tw emeto#illness tw#cancer cw#medical procedure cw#this isn't medically correct but it's at least semi realistic#with the diet changed the polyneuropathy the pain the antidepressants#vomiting and (honestly) sometimes shitting your pants#everytime Jaskier is wearing a hoodie here it's one of Geralts - for comfort and because he's cold#also muscle cramps#the thing under his collarbone is his port#wearing heavy boots and tying them tightly can increase stability if your feet are numb#all that stuff
2K notes
·
View notes
Photo
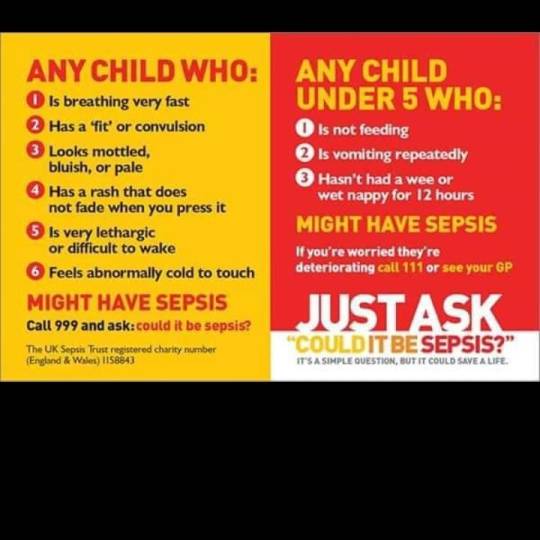
Hello lovelies looking through my camera roll I thought I'd share these.. While covid is a virus we need to be mindful of, especially when you're vulnerable to illness and unable to have the vaccine. Sepsis is another immune system response to be aware of also. The cause of Sepsis (for me) was a result of double Pneumonia I came in with bacterial Pneumonia & caught viral Pneumonia the 2nd time while still in hospital. This is where I can see the resemblance between sepsis and severe covid (leading to more covid deaths as there's plenty of info on covid Pneumonia & Sepsis)of those who passed of Covid as a result of having Sepsis. I'm not downplaying or minimising any experiences especially of a loved ones passing of covid. But I can see the very familiar pattern in my own experience. I wouldn't be at all surprised to hear from any covid warrior who survived sepsis (experiencing very similar issues to me) to say, they'd experienced PTSD too) I had Severe Sepsis shock twice. Complications from this included clots on the lungs (due to the trauma) pluresy, 2 blood transfusions, NORAD treatment for my blood pressure. Kidney dysfunction respiratory failure twice drains in my lungs & heart on life support twice including being intubated for a month. I wore cpap oxygen hood the first time round. I was in a coma twice & last rites were given as I weren't expected to survive. In the end they had to hope the coma would help my immune system to start fighting again as my kidneys stopped working as well as my lungs.. My final point all these complications are avoidable if you catch Sepsis early and a full recovery can be made. Post Sepsis I have chronic pain and PTSD and anxiety attached to this. I have Critical Illness Polyneuropathy (CIP) Costochrondritis severely damaged and scarred lungs & heart, Post Sepsis Syndrome, a progressive lung condition aswell as living with GORD/GERD (Acid Reflux) Hypothyroid Reactive Hypoglycemia and Prediabetes aswell as my sight is damaged. I have missed other conditions out to avoid this being longer. Sepsis is a individual journey. I didn't have mottled skin. You don't need to have EVERY symptom to diagnose #Sepsis. #sepsiskills https://www.instagram.com/nellythevegan/p/CY8h487FGRQ/?utm_medium=tumblr
0 notes
Note
Sorry, when you say 'CIP' do you mean "Congenital insensitivity to Pain", or do you mean "Critical illness polyneuropathy"? I assumed the first, but there are a lot of "CIP" abbreviations.
The former
1 note
·
View note
Text
10 Things Most People Don't Know About anxiety massage points
Luckily, a therapy known as it may relieve some of the numbness in your feet. It works to reestablish the body's wellbeing.
Foot spa in diabetes isn't always suitable. The reflexology for diabetes has been shown to be really powerful. Acupuncture is an alternate treatment for diabetic neuropathy that numerous people today are unaware of.
A adequate amount of pressure should be implemented when massaging with the stones. Obviously, individuals are usually relaxed and sometimes a tiny disoriented after getting a massage. On the reverse side, you have got lifestyle changes that will need to go made.
Because diabetes affects nerve endings and may put the wellness of your feet, there are particular questions regarding diet, exercise, and massage which are frequently requested. Cholesterol reflexology massage for people who have hyperlipidemia can make it even more successful by performing it in conjunction with cholesterol guidelines (lifestyle changes). There are many advantages of massage treatment for people who have diabetes.
There are numerous known approaches to control or check diabetes. For people who have diabetes, you have probably already tried several practices and alternative procedures to relieve the signs. Fortunately, study after study demonstrates that there's a all-natural treatment for.
Your body is able to use this fuel immediately, or it might keep it on your body cells, like your liver, and muscles. Besides controlling or preventing incurable issue, these reflexology glands can enhance the general being of your wellness. Massage enhances the blood flow in the human body and decreases the ill effects generated due to diabetes like hardening of blood vessels.
The energy necessary for physical activity should have a supply, which is going to trigger the uptake of simple sugars like glucose from your bloodstream on your muscle cells and tissues, thereby doing the exact same task as insulin, even as you shed weight and improve your wellbeing at the very same instant! This sort of nerve damage is referred to as diabetic polyneuropathy. There are tons of factors that add to the growth of ulcerations.
Massaging the reflex points of those organs can be beneficial to prevent any complication because of long-term diabetes. It's also valuable for treating hyperthyroidism. Pancreas gland is situated underneath the adrenal gland in the center of your foot.
DAN could be detected in nearly all patients with diabetes. Development in various kinds of neuropathy is connected with the expression of diabetes and glycemic control. So were a number of the anemia.

There are a number of house treatments for diabetes that assist with controlling the fluctuations of sugars. The two most typical causes of diabetic conditions are obesity and sedentary way of life, as stated by the American Diabetes Association.
In addition, there are drugs out there for individuals experiencing pain, including eye pressure points lots of this antidepressant. This disorder occurs more frequently among women and specifically young ladies. For further info, see www.naturestonesinc.com.
Because the body is designed to react to stress with a fight-or-flight response, stress tends to raise blood glucose levels. The impacts of massage may endure for longer duration hence the diabetic patient should check their blood glucose levels at fixed intervals. Other people experience what is called hypoglycemic unawareness, in which they are unaware of a critical drop in blood glucose.
0 notes
Text
Human Immunoglobulin (pH4) for Intravenous injection (COVID-19) Market
Global Human Immunoglobulin (pH4) for Intravenous Injection (COVID-19) Market Size, Share, Growth, Industry Trends and Forecast 2020-2030
The Global Human Immunoglobulin (Ph4) For Intravenous Injection (COVID-19) Market held USD 43205.8 million in 2020 and is to grow with a CAGR of 12.5% from 2020-2030. The glycoprotein molecules in white blood cells are immunoglobulins. Human immunoglobulin (pH4) is a colorless / clear, or light-yellow solution for intravenous injection. It that show opalescence but with no turbidity. Immunoglobulin treatment applies to a combination of immunoglobulins being used to manage different health problems. Such disorders involve form of infections where there is no more precise immunoglobulin available, such as certain HIV / AIDS and measles outbreaks, polyneuropathy, and more. These formulations are delivered straight into the patient's vein. Human blood plasma is used in the production of human immunoglobulin, and these contain antibodies to combat many viruses.
Download Sample Copy of the Report to understand the structure of the complete report (Including Full TOC, Table & Figures) @ https://www.decisionforesight.com/request-sample/DFS020393
Market Dynamics and Factors :
Key human immunoglobulin for intravenous injection market trends on emerging developments include outbreaks of infectious illness, elevated incidence of chronic lymphocytic leukemia and increasing appetite for immune globulin items. According to the American Cancer Society, in 2020 about 60,530 new cases of leukemia will be detected in the US, out of which 21,040 new cases of chronic leukemia (CLL) will be identified. Similarly, about 3,500 new cases of chronic lymphocytic leukemia (CLL) have been diagnosed in the UK in 2017, according to Cancer Study UK. Additionally, growing cases of coronavirus globally will further enhance the growth of global human immunoglobulin (ph4) for intravenous injection (covid-19) market growth.
Market Segmentation :
Global Human Immunoglobulin (Ph4) For Intravenous Injection (COVID-19) Market – By Type
IgG
IgA
IgM
Global Human Immunoglobulin (Ph4) For Intravenous Injection (COVID-19) Market – By Disease
Kawasaki disease
Immune-mediated thrombocytopenia
Primary immunodeficiency disease
Covid-19
B chronic lymphocytic leukemia(b-cll))
Global Human Immunoglobulin (Ph4) For Intravenous Injection (COVID-19) Market – By Distribution Channel
Hospital
Retail
Online
Global Human Immunoglobulin (Ph4) For Intravenous Injection (COVID-19) Market – By Geography
North America
U.S.
Canada
Mexico
Europe
U.K.
France
Germany
Italy
Rest of Europe
Asia-Pacific
Japan
China
India
Australia
Rest of Asia Pacific
ROW
Latin America
Middle East
Africa
New Business Strategies, Challenges & Policies are mentioned in Table of Content, Request TOC at @ https://www.decisionforesight.com/toc-request/DFS020393
Geographic Analysis :
The global human immunoglobulin (pH4) for intravenous injection (COVID-19) market demand is expected to witness significant growth potential in forecast period owing to spurt in disease outbreaks such as coronavirus and the growing prevalence of chronic lymphocytic leukemia. In addition, the immune globulin (IG) drugs is projected to fuel market growth in human immunoglobulin (ph4) for intravenous injection (COVID-19). For starters, the U.S. on 12 August 2019 The Food and Drug Administration (FDA) reported that demand for immune globulin products has risen in recent years, and that there is a lack of Immune Globulin (Subcutaneous) (IGSC) and Immune Globulin (IGIV) products throughout the United States. The U.S. Food and Drug Administration works closely with manufacturers of various (intravenous) immune globulin (IGIV) products to help mitigate the supply situation.
Competitive Scenario :
Global human immunoglobulin (ph4) for intravenous injection (covid-19) demand is highly competitive, consists of a few major players. In terms of human immunoglobulin (ph4) for intravenous injection (covid-19) market share, few of the major players currently dominate the market. Key players enhancing the global human immunoglobulin (ph4) for intravenous injection (covid-19) market size include ADMA Biologics, Inc., Hualan Biological Engineering Inc., Baxter International Inc., CSL Behring, Sichuan Yuanda Shuyang Pharmaceutical Co., Ltd., Bayer AG, Grifols, S.A., Octapharma AG, China Biologic Products, Inc., Takeda Pharmaceutical Company Limited, Boya Bio-Pharmaceutical Group Co., Ltd., and Sinopharm Group Co., Ltd.
Connect to Analyst @ https://www.decisionforesight.com/speak-analyst/DFS020393
How will this Market Intelligence Report Benefit You?
The report offers statistical data in terms of value (US$) as well as Volume (units) till 2030.
Exclusive insight into the key trends affecting the Global Human Immunoglobulin (pH4) for Intravenous Injection (COVID-19) industry, although key threats, opportunities and disruptive technologies that could shape the Global Human Immunoglobulin (pH4) for Intravenous Injection (COVID-19) Market supply and demand.
The report tracks the leading market players that will shape and impact the Global Human Immunoglobulin (pH4) for Intravenous Injection (COVID-19) Market most.
The data analysis present in the Global Human Immunoglobulin (pH4) for Intravenous Injection (COVID-19) Market report is based on the combination of both primary and secondary resources.
The report helps you to understand the real effects of key market drivers or retainers on Global Human Immunoglobulin (pH4) for Intravenous Injection (COVID-19) Market business.
The 2021 Annual Global Human Immunoglobulin (pH4) for Intravenous Injection (COVID-19) Market offers:
100+ charts exploring and analysing the Global Human Immunoglobulin (pH4) for Intravenous Injection (COVID-19) Market from critical angles including retail forecasts, consumer demand, production and more
15+ profiles of top producing states, with highlights of market conditions and retail trends
Regulatory outlook, best practices, and future considerations for manufacturers and industry players seeking to meet consumer demand
Benchmark wholesale prices, market position, plus prices for raw materials involved in Global Human Immunoglobulin (pH4) for Intravenous Injection (COVID-19) Market type
Buy This Premium Research Report@ https://www.decisionforesight.com/checkout/DFS020393
About Us:
Decision Foresight is a market research organization known for its reliable and genuine content, market estimation and the best analysis which is designed to deliver state-of-the-art quality syndicate reports to our customers. Apart from syndicate reports, you will find the best market insights, strategies that will help in taking better business decisions on subjects that may require you to develop and grow your business-like health, science, technology and many more. At Decision Foresight, we truly believe in disseminating the right piece of knowledge to a large section of the audience and cover the in-depth insights of market leaders across various verticals and horizontals.
Contact:
Email: [email protected]
For Latest Update Follow Us:
https://www.facebook.com/Decision-Foresight-110793387201935
https://twitter.com/DecisionForesi1
https://www.linkedin.com/company/decision-foresight/
0 notes
Text
Life & Other Things
Hello my lovelies I’ve started with this photo. I’ve placed the photo here first, so you can see the situation I’m living with. Whether I have Reactive Hypoglycemia events or not, I’m affected by another condition called Hypothyroidism. It is sometimes known as an underactive thyroid meaning it is not working normally…
Thyroxine tablets I take one daily. It has to be taken on an empty…

View On WordPress
#Anecdotal#autoimmune#autoimmune disease#autoimmune health#autoimmunity#bereavement#Blog#blogger#blood glucose#Brain health#Chronic health#Chronic Illnesses#CIP#Critical Illness Polyneuropathy#dairy free#day in the life#death#death in the family#Diabetes types#Diet#diet management#Disabilities#disability life#Disabled life#Educational#endocrinology#father#food intolerances#food is a medicine#Food Science
1 note
·
View note
Text
A case report of polyneuromyopathy with severe demyelinating myelitis 2 weeks after receiving the influenza vaccination.
PMID: J Child Neurol. 2009 Jun ;24(6):758-62. Epub 2009 Mar 4. PMID: 19264734 Abstract Title: Critical illness polyneuromyopathy in a child with severe demyelinating myelitis. Abstract: We report a child presenting with severe demyelinating myelitis complicated with critical illness polyneuropathy. This previously healthy 8-month-old boy presented with acute superior limb weakness, absent tendon reflexes, and respiratory failure. Spinal magnetic resonance imaging showed an extensive cervical demyelinating lesion. Spinal cord trauma was suspected and high doses of dexamethasone were administered. Electromyography and nerve conduction studies showed absence of compound muscle action potentials and sural nerve sensory action potential, which was suggestive of a severe Guillain-Barré syndrome. However, intravenous immunoglobulins did not induce any improvement. Afterward, sural nerve biopsy showed a mild neuropathy, but muscle biopsy revealed abnormalities compatible with severe critical illness myopathy. After 5 months of evolution without improvement, the patient died following withdrawal of life support therapy. This case highlights the possible occurrence of critical illness polyneuromyopathy when treatment with corticosteroids are used in patients with acute demyelinating myelitis.
read more
0 notes
Text
The Conversion from Continuous Sufentanil Infusion to Oral Retarded Opioid Medication: Beware of the Equi-Analgesic Opioid Ratios - A Case Series-Juniper Publishers
Abstract
Background: Sufentanil has an outstanding place in clinical practice and one cannot think of surgery or intensive care therapy without it. However, the routine use of continuous sufentanil infusion may cause severe problems if stabilized patients are discharged from the ICU after surgical treatment and need to be converted to oral opioids.
Aim & method: Here we report our experiences with a series of six patients that we have converted from intravenous sufentanil to oral morphine.
Cases: In 6 cases, we report intensive care (ICU) patients after surgical or medical therapy, who received sufentanil infusion for analgosedation. The patients were between 45 and 68 years old. It can be demonstrated that the optimal dose of sufentanil can be converted to minor doses of oral medication than expected from the calculated equi-analgesic ratios. Despite of lower oral opioid medication pain levels did not increase after conversion.
Conclusion: We recommend to begin opioid conversion with 10% of the calculated equivalent dose of intravenous sufentanil when converting to oral long-acting morphine and afterwards to further adapt the dosage.
Introduction
Since its development in the late 70s, sufentanil has an outstanding importance in clinical practice and one cannot think of surgery or intensive care routines without this treatment. The substance delivers a much higher potency than its parent drug fentanyl with an expanded therapeutic range [1,2]. From the beginning of its clinical use, sufentanil was the intravenous opioid of choice for hemodynamically instable patients [3]. Due to its outstanding hemodynamic stability resulting from a minor impact on cardiac index, left ventricular ejection fraction and heart rate [4], sufentanil is broadly used for critically ill patients in cardiac and non-cardiac surgery. In comparison with fentanyl, it has a shorter context-sensitive half time that results in better controllability [5] and predisposes the use of sufentanil in extended cases and for continuous infusion in intensive care.
The decoupling of analgesia and respiratory depression [6] is another reason for preferring sufentanil during weaning of mechanically ventilated patients or in those with spontaneous breathing. However, the routine use of continuous sufentanil analgosedation in the ICU may result in the problem that stabilized patients are still not free of pain or suffer from chronic pain and thus need to be converted to oral opioid medication, if discharged from the ICU after surgical or medical therapy. For example, common dosage of 20μg of sufentanil per hour has to be substituted by oral opioids as the patient should be transferred to the floor. The calculated equivalent dose for oral substitution would be 1440mg morphine per day, which is, of course, not practicable.
The following cases should demonstrate that sufficient pain therapy can be achieved also with significantly lower morphine doses. We report here six cases in which the hospital pain service was consulted to assist non-anesthetic intensive care units in the conversion from intravenous sufentanil to oral medication.
Case Presentation
Case 1: Patient J.S., male, 44 years old, weight 170kg, height 175cm; septic shock with multi-organ failure
The patient who suffered from arterial hypertension, atrial fibrillation, type-II-diabetes mellitus and morbid adipositas was admitted due to severe and rapid deterioration of his general condition. He developed a septic shock with subsequent multiorgan failure including renal insufficiency requiring dialysis, and liver failure. Furthermore, he developed a cardiogenic shock with a left ventricular ejection fraction of about 10%, and required cardio-pulmonary resuscitation (CPR) as ventricular fibrillation occurred.
After improvement and when the patient was able to be transferred to the floor, he received sufentanil infusion with 25μg per hour. The patient reported pain scores between NAS four and eight with burning quality. Pain therapy was converted orally to long-acting morphine (MST®, Mundipharma Ltd., Limburg an der Lahn, Germany) 3x100mg and 30mg mirtazapine (REMERGILSolTab®, MSD Sharp & Dohme GmbH, Haar, Germany) in the evening and short-acting morphine(Sevredol®, Mundipharma Ltd., Limburg an der Lahn, Germany), 20mg up to six times daily on demand. After a stepwise reduction of the morphine dose down to 3x30mg long-acting morphine per day and 30mg of mirtazapine, the pain service could sign off after seven days.
Case 2: Patient P.M., male, 63 years old, weight 97kg, height 180cm; serial rib fractures with pleural empyema
*This patient received additionally transdermal fentanyl (Durogesic SMAT 75pg/h)
The patient suffered from a traumatic left-sided rib series fracture and developed pneumonia and a pleural empyema while under conservative therapy. Secondary diagnoses comprised arterial hypertension, COPD, type-II-diabetes mellitus and chronic renal insufficiency. After surgical intervention and intensive care therapy with prolonged weaning, the patient was presented to the pain service for conversion to oral opioids. The current pain therapy was 20μg/h of i.v. sufentanil (Table 1). The patient was switched to 3x60mg long-acting morphine sulphate (MST®, Mundipharma Ltd., Limburg an der Lahn, Germany) and 15mg mirtazapine (REMERGIL SolTab®, MSD Sharp & Dohme, Haar, Germany) in the evenings; additionally Sevredol® 20mg up to eight times daily was prescribed, if VAS exceeded 5. After a stepwise reduction of the morphine dose down to 3x30mg with an evening dose of 15mg mirtazapine, pain service consultation ended after four days, the patient being satisfied at VAS <4.
Case 3: Patient S.L., female, 53 years old, weight 146kg, height 170cm; sepsis with multiple arterial emboli
The patient was primarily treated for a sepsis with unknown focus and suffered from morbid adipositas, a history of hypertension and type-II-diabetes mellitus in the intensive care unit. During the clinical course, both legs had to be partially amputated due to multiple arterial emboli; the right leg below the knee, the left leg above.
Under sufentanil infusion of 40μg/h, the patient was presented for conversion to oral therapy. The initial regime comprised 3x100mg of long-acting morphine with pregabaline (Lyrica®, Pfizer®, Berlin, Germany), 2x150mg, and Sevredol®, 20mg up to 6 times daily, if VAS exceeded 5. The consultation ended after five days, with morphine dosage reduced to 3x30mg of long-acting morphine and pregabaline 2x150mg. The patient was satisfied at VAS <3.
Case 4: Patient K.K., male, 58 years old, weight 104kg, height 180cm; osteomyelitis and acute renal failure after coronary arterial bypass grafting (CABG) surgery
The patient was treated for sternal osteomyelitis and acute renal failure after coronary arterial bypass grafting. In addition, the patient suffered from arterial hypertension, peripheral arterial vascular disease, hyperlipoproteinemia, COPD (GOLD III) and had been treated previously for laryngeal cancer with laryngectomy and bilateral neck dissection. At presentation to the pain service for conversion to oral medication, the patient received 20μg/h sufentanil with additional transdermal fentanyl (Durogesic SMAT 75μg/h, JANSSEN-CILAG, Neuss, Germany), which the patient had already before surgery. Pain scores of VAS=6 with peaks at VAS=8 were reported. The patient was converted to long-acting morphine 3x100mg/day and additionally with 3x100mg carbamazepine (Carbamazepin HEXAL®, Salutas Pharma, Barleben, Germany) with opportunity of receiving supplementary 20mg Sevredol®, up to 8* per day. After reducing long-acting morphine to 2*50mg with carbamazepine 3*300mg, pain service consultation ended after six days, the patient being satisfied at VAS=3-4.
Case 5: Patient R.S., male, 66 years old, weight 80kg, height 178cm; Multiple Myeloma and ARDS
The patient needed mechanical ventilation support for acute respiratory insufficiency under pre-existing multiple myeloma. During the clinical course, the patient developed acute renal failure requiring dialysis, aspiration pneumonia and critical illness polyneuropathy. After prolonged weaning, an apparently pain stricken patient was presented to the pain service receiving 20μg/h sufentanil, for conversion to oral analgesics.
At pain levels of VAS=5 and peaks of VAS=9, initially long- acting morphine 3*100mg/day with 150mg pregabaline (Lyrica®, Pfizer, Berlin, Germany) in the evenings was prescribed, with the possibility of additionally receiving 8*20mg Sevredol® per day. After stepwise reduction of morphine dose to 2*20mg/d of long-acting morphine and 150mg pregabaline in the evenings, the patient was discharged from the ICU with VAS=3 and the patient was discharged with 2*10mg/d long- acting morphine and with 150mg pregabaline.
Case 6: Patient K.B., male, 62 years old, weight 60kg, height 160cm; hemorrhagic shock after bypass surgery of the femoral artery
Following bypass surgery of the femoral artery with secondary hemorrhage and hype volemic shock, the patient developed an urosepsis. Preexisting diagnoses were peripheral vascular disease, arterial hypertension, type-2-diabetes mellitus and stage-III-renal insufficiency. After stabilizing the patient and planning for discharge to the ward, pain service was consulted for conversion of i.v. Sufentanil, 20μg/h, to oral medication.
The patient described pain as having piercing/stabbing qualities at VAS=3, peaking at VAS=9. After a stepwise reduction of initially 3*100mg/day long-acting morphine with mirtazapine 15mg for the night, the patient was discharged from the ICU with 3*60 mg/d long-acting morphine with afore mentioned mirtazapine at VAS=1.
Discussion
In clinical practice, sufentanil is indispensable for anesthesia and intensive care therapy. However, a conversion from continuous sufentanil infusion to oral opioid medication is essential for discharge from the ICU; however, current literature offers no usable conversion algorithms.
The pain levels of a series of six patients presented here indicate that opioid conversion to lower oral doses does not result in an increase of pain scores. Additionally administered psychotropic drugs may also have an effect on alleviating pain, yet two aspects have to be taken into account: (1) pain aggravation by under-dosing of opioids cannot be compensated by psychotropic medication, and (2) if the opioid dose is titrated to an optimum, psychotropic drugs cannot further reduce this dose. They can only be used to avoid severe side effects of opioid therapy [7]. In the present cases, psychotropic medication was used to treat effects of opioid over-dosing after conventional conversion, and was needed to treat the neuropathic aspects of the respective pain qualities [8].
It is important to note that the conversion to oral opioids is not an "opioid rotation", although one has to calculate an equi- analgetic dose. The concept of opioid rotation addresses the problem of excessive side effects [9] of a single opioid or the insufficient effect on pain [9,10]. This was not the case in the presented patients. In those, we intended to switch an i.v. opioid to an orally applied one, much in the way a morphine drip is switched to oral retarded morphine.
Sufentanil is available as a non-i.v. preparation for sublingual, buccal and nasal administration but not in a long- acting formulation. As the application route switch is usually for a single compound and the long-acting formulation is commercially unavailable, change to long-acting morphine was necessary, but not in the sense of an opioid rotation.
In current references, only the general recommendation to begin oral substitution with approximately 50% of the equivalent dose can be found [10,11]. These recommendations are based on the thought that on one hand the patients have not benefitted from the current opioid and on the other they offer concomitant clinical limitations (i.e. advanced age, renal damage, cardiopulmonary insufficiency, etc.) that makes a 1:1 switch to a new opioid inappropriate.
The patients in the presented cases had an i.v. sufentanil medication near the optimum dose. The available conversion tables and factors suggested a 900% higher dosing than that we eventually applied. Even with a reduction of 50% from the given i.v. dose, the orally administered amount would still have been in excess of 350% of the dose that is finally necessary. This is striking, as inadequately high doses of opioids can lead to severe side effects such as attention deficits, optical hallucinations and ultimately respiratory depression [12,13].
From the present data, we provide evidence that, when converting i.v. sufentanil to oral morphine, a much steeper reduction of the equivalent dose is urgently warranted.
We would like to recommend starting with 10-20% of the calculated equivalent dose of sufentanil infusion when converting to oral long-acting morphine and afterwards adapting the morphine dosage further. Possible co-medication with neuroleptics and benzodiazepines should not be ignored in order to further minimize opioid doses and to decrease severe side effects.
In the possible case that the conversion to a long-acting opioid proves insufficient, a similar approach as usually followed in opioid conversion should be used: In addition to the estimated dose, rescue medication needs to be provided. This can be claimed every hour by the patient and, in the case of using morphine sulfate, doses of 10mg and 20mg with an onset of 15 to 20 minutes should be available. It seems important that none of our patients claimed rescue medication.
Conclusion
Owing to safety considerations, we propose to approach the final opioid dose from a lower dose. By doing this, severe side effects and a possible readmission to the intensive care unit can be avoided. Moreover, since the increased pain perception precedes withdrawal symptoms, correcting the opioid dose in an hourly interval would not have led to withdrawal indicators [14-18].
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.com
For more articles in Journal of Anesthesia & Intensive Care Medicine please click on:
https://juniperpublishers.com/jaicm/index.php
For more Open Access Journals please click on: https://juniperpublishers.com
#Juniper publishersPublons#Juniper Publishers Review#Online Publishers#Juniper Publishers#Open access Journals
0 notes
Text
The Case of Martha Rendell
Welcome to our first episode of our Western Australia season! Fair warning, this episode discusses the death of children. Remember when we said we weren’t gonna cover child murder cases? We’re massive liars.
Life’s tough out there for a kid in 1907. You have to write on a literal rock at school, the only thing you have to play with is a hoop and a stick, there are no video games yet, and you’re dodging the Grim Reaper at every turn. If the ol’ infant mortality rate doesn’t get you, or the common cold, maybe your own stepmother will.
This episode, we discuss the Wicked Stepmother of East Perth, Martha Rendell, and we question whether or not this lady really did poison three of her stepchildren with hydrochloric acid, or if she actually committed a far more serious crime for the early 20th century – being an unattractive, unmarried woman who was living in sin.
EPISODE NOTES:
Annie, Olive and Arthur Morris died from what was believed at the time to be illnesses arising from complications with an earlier bout of diphtheria. But all the children had curious symptoms that were unable to be diagnosed by some of the best doctors in Australia at the time. They suffered from seizures, typhoid fever, and burning pains in the stomach that didn’t seem to have a clear cause. The children were buried, and the Morris family was considered to be terribly unlucky, until one day George Morris accused Martha Rendell, the family’s housekeeper and his father’s mistress, of poisoning his siblings with spirit of salts – the old-timey name for hydrochloric acid.
Martha was put on trial, and the press had a field day when it was uncovered that she was not really the children’s mother, as she presented herself, but really just Thomas Morris’ mistress, a homewrecker who had been having an affair with Thomas for over ten years. The salacious supposed murder of the three children painted Martha as a wicked and uncaring stepmother who delighted in children’s suffering.
She was sentenced to hanging in 1909, but in recent years there has been much discussion about whether Martha was really responsible for the deaths, or if she herself was a victim of the society in which she lived.
I myself suffered from some kind of paresis of the brain nerves and thought it would be “fun” to reference this week’s sources in Harvard style, because I used a lot of journal articles and I’m a uni student and was like, this will be a fun gag, then halfway through I was like, what is wrong with me. Anyway, if you want to learn more about Martha Rendell and the social circumstances acting on her, please look here:
Haebich, A 1998 'Murdering stepmothers: the trial and execution of Martha Rendell',Journal of Australian Studies vol. 22, no. 59, 66-81, accessed 31 August 2019, available <https://doi.org/10.1080/14443059809387425>
Haebach, A 2010 'Revisiting the Trial of Matha Rendell', The New Critic, accessed August 31 2019, available <http://www.ias.uwa.edu.au/new-critic/thirteen/?a=1314992 >
For all the fun medical information, go here:
Koschny, R et al 2013, 'Fatal Course of a Suicidal Intoxication with Hydrochloric Acid', Case Reports in Gastroenterology vol 7 no 1, 89-96, accessed 31 August 2019, available <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3618096/>
Paget, G E 1883, 'Case of Coexistence of Diphtheria and Typhoid Fever', The British Medical Journal vol 2, no 1176, 67-68, accessed 31 August 2019, available <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2372714/?page=1_>
Piradov, M. A et al 2001, Diphtheritic Polyneuropathy: Clinical Analysis of Severe Forms,Archives of Neurology vol 58 no 9 1438-1442https://jamanetwork.com/journals/jamaneurology/fullarticle/780257
I used so. many. newspaper articles. for this episode. They’re all available from the National Library of Australia (trove.nla.gov.au, search ‘Martha Rendell’), but here are some bangers to get you started:
Closing Chapter of The Remarkable Morris Myster: Martha Rendell Handed to the Hangman. On the Threshould of Eternity she Protested Her Innocence, and Declared Her Life had been Sworn Away. Review of the case – the Execution – Scene at the Graveside – the Man Morris – and Jack Ketch https://trove.nla.gov.au/newspaper/article/207402944
A City Sensation – The Deaths of the Three Morris Children – The Inquest Opened – How the Little Ones Died – The Brothers' Story https://trove.nla.gov.au/newspaper/article/26234843?searchTerm=martha%20rendell&searchLimits=
The Murder Trial – Death of Arthur J. Morris – Judge McMillan's Summing Up – Mrs Rendell Sentenced to Death. Thomas Morris Acquitted https://trove.nla.gov.au/newspaper/article/26237508?searchTerm=martha%20rendell&searchLimits=exactPhrase|||anyWords|||notWords|||requestHandler|||dateFrom=1909-09-01|||dateTo=1909-09-30|||sortby=dateDesc
If you like what we do please consider supporting us on PATREON
Subscribe to the podcast on ITUNES, STITCHER, SPOTIFY or your podcatcher of choice.
Find us on FACEBOOK, TWITTER, INSTAGRAM or EMAIL us on [email protected]
www.thatsnotcanonproductions.com
#true crime#crime#investigation#police#australia#justice#podcast#brisbane#forensic#evidence#murder#criminal#tasmania#victoria#new south wales
0 notes
Photo
Hi my lovelies in between autoimmune flares I do simple physio exercises to strengthen my legs and especially left side. I also do adapted yoga moves aswell as stretching for mobility strengthen and flexibility all over. I have neuropathy aswell as Osteoarthritis in my spine and coccyx. I have 3 inoperable prolapsed discs so I can't do any impact exercises like my former loves and faves 😍 running, yoga, and going to the gym using freeweights and machines aswell as exercise balls and treadmill etc. I'm naturally hyper and the gym suited me as I'd get bored easily I've swam in the past and enjoyed it. But there's only so many laps you can do. Of my 51 years since leaving school, I've always did some kind of exercise. So when I was told bluntly by my specialist (who was the director of his department and top consultant in orthopedic and a surgeon, so he knew his stuff) I had to stop all high impact exercise and to cancel my gym membership. I'd been going to the gym for almost 20 years going 6 days every week...Anyway I have l doing gentle no and low impact exercise for the last 6 months and I have had no additional problems because of the arthritis. However since 2013 and having been in ICU for almost 2 months on life support. I was unable to move let alone rollover or get out of the bed. I was also left with new health problems and was diagnosed with Fibrosis Bronchietatis and Costochrondritis and CIP (Critical Illness Polyneuropathy) this made me physically weaker (I suppose I have to factor in the lung damage and the Pulmonary Embolisms I had)my legs were weaker. I am also in constant pain because of this. I still need help to get up if I fall over so I have found these and something I can work up to build strength without impacting negative consequences. Weight bearing exercises will help everyone over 50. But I have reach the limit where I need to start lifting some weight. I don't need to lose any weight but improve on my current 14.5%bodyfat 🙏🏽😁looking forward to seeing how this goes. #healthjourney #exercisehelps #vegansofig #fitnessover50 #womenfitness #wellbeing #thyroidhealth #weightliftinggirls #vegansoffacebook #fibrosis #romanigypsyfitnessgoals (at At Home..
#healthjourney#exercisehelps#vegansofig#fitnessover50#womenfitness#wellbeing#thyroidhealth#weightliftinggirls#vegansoffacebook#fibrosis#romanigypsyfitnessgoals
0 notes
Text
Significant Impact of COVID-19 on Electromyography Devices in Healthcare Industry

COVID-19 Impact on Electromyography Devices in Healthcare Industry
OVERVIEW AFTERMATH OF COVID-19 AND GOVERNMENT ROLE
A recent SARS-CoV-2 virus has caused a general pandemic of respiratory disease, called COVID-19. The infection initially showed up in Wuhan, a city in China, in December 2019. The patients experiencing COVID-19 were dealt with cautiously with all the safety measures since this disease spreads aggressively through actual contact.
There are now numerous vaccines in use. The first mass vaccination program commenced in early December 2020, and as of 15th February 2021, 175.3 million vaccine doses have been administered. World Health Organization (WHO) issued an Emergency Use Listing (EULs) for the Pfizer COVID-19 vaccine (BNT162b2) on 31st December 2020, issued another two EULs for two versions of the AstraZeneca/Oxford COVID-19 vaccine, manufactured by the Serum Institute of India and SKBio on 15th February 2021. On 12th March 2021, WHO issued a EUL for the COVID-19 vaccine Ad26.COV2.S, developed by Janssen (Johnson & Johnson).
As per the WHO report, globally, as of 5th June 2021, there have been 179,513,309 confirmed cases of COVID-19, including 3,895,661 deaths, reported to WHO. As of 23rd June 2021, a total of 2,624,733,776 vaccine doses have been administered. In India, from 3rd January 2020 to 10:21 am CEST, 25th June 2021, there have been 33,257,768 confirmed cases of COVID-19 with 597,727 deaths, as reported to WHO. As of 17th June 2021, a total of 317,983,185 vaccine doses have been administered.
Even though immunization is found for COVID-19, safeguards incorporate incessant hand-wash, wearing a face mask, and keeping up social separating.
NCS and EMG findings indicate a direct action of COVID-19 on nerves and muscles. SARS−COV-2 demyelinating polyneuropathy and elements of myopathy could be new pathological entities to be considered in the COVID-19 management. More studies would be required to confirm these electrophysiological findings.
The goal of electromyography is the pre-symptomatic detection of the aberrant electrical activity of the skeletal muscles so that treatment may be commenced at the earliest to prevent, or improve, the long-term consequences of neuromuscular diseases.
In light of the fiery impacts of the infection, there are hypothetical dangers that the viral contamination could delay the early testing and detection through electromyography as there have been limited visits to the hospitals and testing centers due to the lockdown imposed by the government in different countries.
IMPACT ON PRICE
Because of COVID-19, the market is upset to a major level. The few foundations have been stay shut while others had downsized the activities or put a pause to the extension plans as they attempted to endure the uncommon emergency.
The current COVID-19 episode has influenced essentially every industry on earth, and the electromyography devices market is no exemption. There has been a tremendous and sudden lessening in the volume of elective joint substitutions worldwide as wellbeing situation legitimately organize their COVID-19 reaction.
States must develop and implement policies that allow for interstate licensure and practice of medicine (entailing the use of telemedicine) to enable consultation and communication to remote areas and ensure the swift flow of information across state lines.
Now, as the demand for telehealth innovation is turning out to be very demanding by human beings, this will make the market more competitive due to new and more innovative equipment that will be launched by the makers, by decreasing the overall cost of the new and innovative new product launches.
IMPACT ON DEMAND
Since the pandemic, due to the lockdown situation, the economic growth of a country is declining day by day. And the manufacturing units for various items shut down due to the non-availability of manpower.
Coronavirus disease (COVID-19) causes acute respiratory illness ranges from mild to severe pneumonia with respiratory failure. Moreover, neurological involvement is more common in severely affected patients with COVID-19 than in those with less severe illness. Electromyography devices are required to treat severe coronavirus disease (COVID-19) patients,
Moreover, the growing number of COVID-19 patient pools in developed, as well as developing countries illustrates the huge future demand for electromyography devices across the globe.
For instance,
· According to the World Health Organization (WHO), till 25th February 2021, there have been 112,209,815 confirmed cases of COVID-19, including 2,490,776 deaths
Thus, the growing cases of coronavirus disease (COVID-19) indicate a huge demand for electromyography devices across the globe. Henceforth, it is estimated that the global electromyography devices market is anticipated to boom up in the forecasted period.
IMPACT ON SUPPLY
Because of the pertinacious COVID-19 lockdown, sanctions have been forced by administrations of different nations. These limitations and boundaries across the nation’s borders prompted a diminishing stockpile because of restricted materials and labour force and the halting of the assembly line.
The COVID-19 pandemic has transformed many organizations’ business environments. Supply availability has been hampered by a number of issues, including export and travel restrictions by some producing countries, and the lockdown has forced suppliers to (temporarily) shut down. To minimize supply chain crises, healthcare organizations have been firmly monitoring the supply chain with the assumption that the COVID-19 outbreak may adversely impact the supply chain of electromyography devices, including shortages of electromyography devices or potential disruptions in its supply chains.
To manage such critical situations, many organizations are looking forward to improving and diversifying the supply chain model in all aspects. A diversified supply chain model is anticipated to enhance the availability of electromyography devices in the market as well as increase end-to-end visibility. The resulting COVID-19 pandemic has shown the various ways for supply chain management, which may be effective within a remote working environment.
The supply chain units are taking stringent measures and risk mitigation protocols to provide the devices to the manufacturers to the customer. The presence of key market players for the development and launch of the electromyography devices will increase the net sales and may show a surplus growth in the market.
Additionally, the manufacturers are also taking crucial steps to ensure the availability of raw materials by and also they have to look into the quality of products. But since the demand is increasing day by day, so as to meet the demand, the major manufacturers and suppliers are collaborating with each other’s to ensure the supply of raw materials.
STRATEGIC DECISIONS OF GOVERNMENT AND MANUFACTURERS
The key players engaged in global wound healing manufacturing are making improvements to keep the speed during COVID-19. They are taking every single choice cautiously so the development can be expanded on a consistent schedule for the market. The manufacturers are likewise giving a great deal of consideration in the improvement of inventive items that can be utilized for the attractive impacts. Organizations working in the electromyography devices market are embracing a few systems, including joint effort, arrangements, association, and market development to improve their business. These essential choices by the organizations are required to give huge occasions to the market players working in the electromyography devices market.
A large pool of the population is affected by the COVID-19 virus, and its spread is expanding across the world in the last few months. To deal with the COVID-19 outbreak challenges, many electromyography devices market players are creating new strategies. To tackle the pandemic situation and to increase the company revenue and growth, companies are now opting for digital media such as telecommunication, mobile applications, webinars, and other digital media to support patient requirements. Moreover, to accomplish the market demand, small as well as major market players utilizing the strategy such as partnerships, agreements, and organizing conferences. It is predicted that these strategies are anticipated to escalate up the company revenue and its growth in the forecasted period.
For instance,
· In April 2020, Neurosoft S.A. organized NYC Neuromodulation 2020 Conference. This conference has anticipated enhancing the company’s presence in the global market.
Furthermore, for the economic recovery after the pandemic of COVID-19, the manufacturers of electromyography devices have to adopt several types of strategic initiatives in terms of increasing R and D activities, conduct numerous types of market surveys to know the current situation and mind-set of consumers towards their need. The increasing R and D activities will help the manufacturers to launch the advanced devices by knowing the advanced technology or need of the end-user.
For instance,
· In August 2020, NIHON KOHDEN CORPORATION launched Version 12 of the Polysmith software used in Polysomnography Devices. This new version of software launched by the company includes more than 40 market-driven features, which aids in good analysis and outcomes. Thus, this product launch by the company leading to enhance the sales growth of the company.
CONCLUSION
It is estimated that the COVID 19 pandemic outbreak is having a positive impact on the growth of the global electromyography devices market owing to the elevation in demand for electromyography devices. Moreover, many governments and organizations are exclusively focusing on the rapid recovery of COVID-19 patients, and this priority, as well as the essential requirement, is illustrating the further growth of the electromyography devices market. Many government bodies and major electromyography devices market players are closely associated with patients as well as healthcare professionals for better patient health as well as experience.
It can be concluded that the COVID 19 pandemic situation has a significant impact on the global electromyography devices market, including the price and demand of electromyography devices.
For instance,
· December 2017, Eone-Diagnomics Genome Center (EDGC), a Korean genetic analysis company, announced its decision to apply machine learning-based artificial intelligence (AI) technology to its non-invasive prenatal test (NIPT) NICE0. In 2019, AI specialist FDNA and PerkinElmer Genomics partnered to launch Face2Gene Labs for newborn testing. This decision enabled the company to flourish further in the market and helps in revenue generation.
#Electromyography Devices Market#Electromyography Devices Market Analysis#Electromyography Devices Market Size
0 notes
Text
Long-term outcome of critical illness polyneuropathy
http://dlvr.it/NJ0fr9
0 notes
Last Seen Blogs

timemachinesims
Time-Machine Sims

gihcaa
gihcaa

beharahospital
Behara Hospital

reylo-y
Untitled

344245
Untitled