#this month is just assessments and exams and next month is just clinical posting
Text
IM FREEEEEEEEE
(she is, in fact, not free because she has assignments to do during the weekend.)
#but im back baby#my next exam is on the 20th so long way to go#have a few assessments to do though so yeah 😔😔#this month is just assessments and exams and next month is just clinical posting#but yeah at least a hell ish week is over#fucked up my exam yesterday but after some reasoning its just 30% and i have finals to make it up to not fail#and today's quiz is actually 35% but it wasn't bad fortunately#so yeah so far yesterday's exam is the only thing that spoiled my streak of doing well in exams but nothing's perfect anyway#but yup yup im free for now <333333#personal.txt
2 notes
·
View notes
Text
JULY!!!!!
hello everyone, lads and lasses, i hope you are all well and happy! buckle up because this post is going to be long for i want to put down as many details as i can - i'll just go straight to the point that i'm uncharacteristically on time for this July post because i just can't wait to relay the news!
here we go, the main highlight of this month is that i can finally confide in you guys for what is the true nature of my project because it went super duper well! and if you follow me on instagram or twitter, yes: i got accepted to Dentistry UI's Orthodontic Residency program ✨
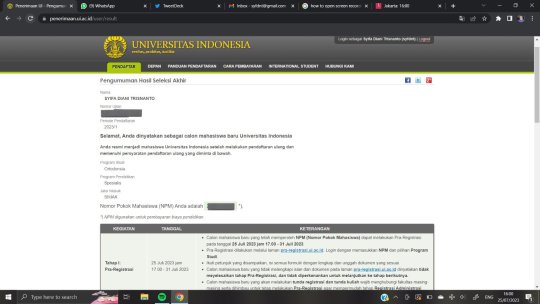
look at that. i still can't believe it says i got in. still feels like a fever dream, but it's real 🥺
so July has been such a tremendous emotional rollercoaster for me... well honestly the past year has been one. i prepared for the SIMAK UI exam since October 2022 because there were just so many things to take care of, not to mention actually studying for the exam(s). yep, there were different exam steps and each has a challenge of its own. before i explain them and the timeline, i just want to put a disclaimer that orthodontic residency is one of the hardest to get into and i went in with complete surrender of how the result will turn out. there were 19 candidates and only 11 are accepted.
there were eight different exams: TPA (some sort of academic potential test), GMAT English test, MMPI (and i quote from Google: "The Minnesota Multiphasic Personality Inventory is the most common psychometric test devised to assess personality traits and psychopathology."), orthodontic theory computer based test, orthodontic theory essay, English essay, orthodontic wire bending practical exam, and the last being an interview with the professors of the department.
if the amount of tests already made you cower, then the dates and intervals of when the exams were held will tip you over the edge: all eight exams are done in just the span of four days! i remember checking out the schedule and got a headache immediately because i was so worried of the time constraint. and the way that there's an exam day where i had four exams done... i literally ate next to nothing and got a bit sick afterwards (sorry, a force of habit with so much stress lol)
so many went in as an effort to put my best out there, and it wasn't easy. to get into residency programs it's a well known public secret that you need to have an insider or a recommendation letter from higher-ups, and really... i have none. i remember my mum saying that all i have is Allah's help. as anyone who know me may guess, i did everything i could (obviously) 😂
for the orthodontic theory exams i had to read two thick textbooks that took me two months to finish, because it was just too much of new information i need considerable amount of time to understand the theories. there was no guideline on what to expect or what kind of question will appear on the exams, so i just blindly read everything and try to make a sense out of it. i think 6 months before the exam week every day was just me reading anything orthodontics related, revising them, working on sample exam questions i have from my previous clinical years, and practicing wire bending (it got me bruised fingers for weeks) i think for this time i can say i'm very proud of myself for being able to push through despite many hindrances, for getting in on my first shot because as i stated earlier many ortho residents had to try twice or even thrice until they're accepted.
the exam week went from July 2nd to July 6th, i think i was a zombie during this time because i couldn't eat well at all and my brain just programmed my body to react as best as i could to everything that transpired in those five days 😭 the announcement was on July 25th and i was on a clinic shift where i had a patient one hour before announcement time and it felt like i was downright insane counting down to the moment i refresh the website... i remember jumping up and down as i see congratulations written 🥺 on July 26th there was a meeting for all residents and i finally got to meet my 10 'classmates'! to be frank i'm so nervous of what's to come but as always, i'll meet it when it does. class will start around late August/early September, so wish me luck for the next three years of residency!
second highlight is my East Sumba trip!!! as usual it was my dad's office trip again for the nth time and i thoroughly enjoyed it as it was five days after i was done with SIMAK UI's exam week! the trip lasted for six days (2 days of journey to and from included) and let me tell you: Sumba. is. so. beautiful. i ran out of objectives, all i could do while exploring just a small portion of Sumba is praise Allah's name because what else would i do? nothing manmade will ever replicate or even come close to the omnipotent presence of nature. i went to Wairinding Hills (it's a hit tourist spot that showcases Sumba's unique terrain, the sunset view is one of a kind), Tanggedu Waterfall (super blue, cold waters here i could spent hours just submerging my feet in it, the view is also great), Walakiri Beach (the special part about beaches in East Sumba is that it has mangrove trees as a way of land protection and during sunset, it gave the impression of the sea mirroring the tree and the people, so yeah top notch photo spot) and of course seafood culinary trip! being near the sea in every direction it gives access to fresh water creatures and the cuisines are heavenly. i thoroughly enjoyed my time here 🥺
from this East Sumba trip i finally decided i'd rather go exploring Indonesia's hidden gem islands rather than going abroad, and i'm not saying this to make a jab to other countries really, it's just i can't believe there are still so many undiscovered untouched ethereal parts of nature in my own country and it's so close to home! i feel like it's a top priority in my bucket list to see them at least once in my life. the only disheartening thing is how the government seems to not care even an ounce about these places. i wish they would notice and make sure the locals can actually benefit from these full of potential tourist spots. also really sad to see most of the tourists here are foreigners because of how expensive domestic flight tickets are to these secluded islands. i sincerely hope for a better plan for these issues...
i know i'm jumping a bit on the timeline here but back again to July 29th i got to see a longtime friend, Nurul! our fathers work at Bank Indonesia and we met while we were in junior high school on a BI event. and i love the fact that even a small inconsequential occurrence turned out into a friendship that stays strong through the years 🥺 we had lunch and watched Oppenheimer together!
then at last July 30th i went to an orphanage that my parents are patrons of, and held a lil celebration of me becoming an orthodontic resident and my sister graduating. it was fun seeing all the kids i've first met back in 2018 as i was starting my clinical years to be a dentist and they are a major part of my journey from becoming a dentist to now a resident. we had lunch and i gave mini dental health education and free dental health checkup - it was hilarious how the boys were more embarrassed than the girls about doing the latter!
that's it for July. oh how time flies :) it's always a mind acrobat looking back and, though it hasn't settled fully yet, knowing how far i've come... i've said this 348573495 times but really, it's an amazing feeling to see things i didn't understand back then are now starting to come back to me in full circle. especially how now i understand never giving up and conceding decisively go hand in hand. life will reveal its secrets and why things go the way they are, all in good time.
dear friends, be patient, do good and be good 😉 good things come to those who wait - they're coming our way. see you in next post!
#alhamdulillah#masyaAllah tabarakallah#i'm officially back to school#yet again#bismillahirrahmanirrahim#excited for this new journey!!!#LET'S GO
4 notes
·
View notes
Text
Nervous Breakdown // Jay Halstead x Reader

Photo by @karihighman
Description: Jay is there when you start to break down.
Words: 1539
Warnings: None
Pairing: Jay x Reader
A/N: So, this I wrote for me. The schedule Reader talks about is my actual schedule. The sign offs are the things I actually need. This was me last night, except I didn’t have someone like Jay to talk me down from my nervous break down, I just had it and then had to be at my clinical this morning (which I’m still at btw lol). But yeah. Hope you enjoy. And if my posting is sporadic in the next month or so, this is why.
“Come to bed,” Jay told you softly, leaning on the doorframe of your bedroom with his arms crossed over his chest as he looked at you with papers spread across the floor, couch, and coffee table.
Your movements were frantic as you tried to organize them all, trying to figure out the best system to keep everything together. Every section was chronologically ordered for the online documentation, paper clips holding each stack together. Then, there were the colored sheets that had even more important signatures on them. You had to make sure everything was in order as class was drawing to an end.
“I’ll sleep when I’m done, Jay,” you snapped at him before closing your eyes and taking a deep breath. “I’m sorry, I just-”
“I know.” He walked over, stepping around the stacks before sitting directly behind you in the only place clear of paper. “Come here.”
You couldn’t stop yourself from leaning back into his chest, his arms wrapping around you. Grounding you as your mind went a mile a minute. You also couldn’t stop yourself from grabbing your calendar, flipping it open to this month.
“What’s the schedule look like?” His chin rested on your shoulder as he looked at the planner.
“I have to help with the EMT class Saturday from seven to three. Then I start my shift at work at eight tomorrow night. Then, work Sunday night. So I’m going to try and catch up on some sleep on Sunday. I have my exam in Med Emergencies on Monday. Then, I have an ambulance clinical AM shift at seven. Same on Wednesday. A quiz in Med Emergencies on Thursday. Then, I work Thursday night. Off at eight on Friday morning, but I picked up a shift from two to ten Friday day. Then, ambulance clinical on Saturday AM shift.
Same with that next Sunday. A quiz in Med Emergencies on the seventeenth. Then work that night. Work the night of the eighteenth, but I’m off at four in the morning instead of my usual eight. Mainly because I have an OR clinical on the nineteenth from seven to three. But then I work that night, off at five on the twentieth because I have an exam in Med Emergencies that day. Ambulance clinical AM shift on the twenty-first. Twenty-second, I have an ER shift from seven to three, then I work that night. Work Sunday night, so I’m going to try to catch up on sleep that day.
Twenty-fourth I have another exam in Med Emergencies. Ambulance AM shift on the twenty-fifth and sixth. Then, we review for our Final in Med Emergencies, but I work that night. I’ll get off at six to get to my ambulance clinical on the twenty-eight at seven. I work that night, but off at five to get to my Maternal-Fetal Truck shift by eight.
On the thirtieth, I have an ER shift from three to eleven. The thirty-first, I have my final in Med Emergencies, and then work that night. Off the day of the first, but I work that night. Then, an ER shift at three on the second. Then, I work that night, but I’m going to try to switch shifts just because my ER shift won’t finish until eleven. The third, we have our student evals. The fourth, I’m helping the junior class with their Ops day, and then I have an ambulance clinical that night. Off the fifth, but work that night. Off the sixth, but work that night. Seventh is labor day, so completely free. ER shift on the eighth at three. Then, on the ninth, OR shift at seven.
“After that, I don’t know because we haven’t signed up for our capstone. Which all of this,” you said, motioning to the mess of papers, “is me getting everything in order to make sure I have everything done and what I still need. Because we can’t start capstone until all of our skills check offs are done, and we’ve hit all of our demographics.”
“What do you have left to do for your skills?” That question got you to sigh, putting the planner down and grabbing a notebook. You had to push your glasses back up on your face as you looked down at your messy handwriting.
“Five peer reviews for pediatric intubations. Two peer reviews for needle cricothyrotomy. Three peer and two instructor reviews for trauma assessment. Five peer reviews for trauma intubations. Two instructor reviews for joint splinting -- which I’m already an EMT, why the Hell do I have to sign off on the BLS stuff again? Same with long-bone. I need one peer review and two instructor for traction splint. Again, BLS bullshit. Seven peer reviews for medical and cardiac scenarios. Eleven peer reviews for IV starts, and one instructor. One instructor for IV piggyback. Five peer reviews for IO. Oh, and another instructor. Three peer for IM injection. Three peer for synchronized cardioversion. One peer for defibrillation. Three peer transcutaneous pacing. Four peer reviews and one instructor for adult team lead scenarios. Five peer reviews and one instructor for pediatric team lead scenarios. Eleven peer reviews for being a team member. Three peer reviews for being a team leader for geriatric scenarios. Six peer and one instructor reviews for adult physical assessments. And finally. Six peer and one instructor review for pediatric assessment,” you read off, letting the paper fall to the ground.
He held you a little tighter. You felt bad. With all the stress you’d been under for the past month, and with how crazy his job was, the two of you hadn’t gotten to spend a lot of time together. And the next month was going to be even crazier.
“When are you supposed to start your capstone?” He pressed a kiss to your neck, your eyes fluttering closed in response.
“They want us to start September Ninth, but I’m going to be the last one who gets to sign up because I’m so far behind! Everyone is going to pick the cool preceptors, and I’m going to get stuck with the ones nobody else wants,” you vented before huffing in frustration.
It was indeed very frustrating, stressful, and downright annoying that you were so far behind compared to everyone else. That’s what happens when you have to be off for six weeks because you tore your knee. Now, it was a constant game of catch-up.
“Just breathe when I breathe,” Jay instructed in that calming voice, following his breathing pattern. It got your heart rate down as tears came to your eyes, despite your internal protests. You were on the verge of a nervous breakdown, and it wasn’t going to be pretty.
“Maybe you should email your instructor?” he suggested when you had your breathing under control on your own.
“And have her take me off all my clinicals and reschedule everything? No. No fucking way. I can’t just email her and schedule my nervous breakdown, Jay. She was very clear in first semester that if we took on too much and couldn’t handle it, she’d take us off our clinicals and completely reschedule everything. I can’t do that, Jay. I can’t because then I’ll be even further behind.” You were talking a mile a minute, Jay taking a deep breath behind you. You took the hint and matched your breathing again.
“Okay, then don’t email her. But, I want you to come to bed right now. It’s two in the morning. You have an ambulance clinical in five hours. You need your sleep. All of this will be waiting for you when you come home tonight,” he insisted. You didn’t want to, but you knew he was right.
The two of you stood up, walking into the bedroom. You couldn’t help it as you collapsed on the bed with a groan, much more comfortable than the hard floor in the living room. He wasted no time in joining you, pulling you close again. This time, you were able to see his face at least, tracing his features gently with soft fingertips. You missed him.
“How about we do something Labor Day? Just you and me to destress a bit?” you asked, Jay nodding in agreement before lips met gently. “I miss you.”
“I miss you too,” he said with a soft chuckle, kissing you again. “But you’re almost done. This is the worst of it. After your final, you’re pretty much done with lecture. Capstone is your last hoorah. Then, your tests and you’ll finally be a paramedic after over a year. Doing this through a pandemic. Through all your family crap. I’m proud of you.”
“You really know how to sweet talk a lady,” you joked, resting your head on his chest.
It was the exact thing you needed to hear. Jay always knew what to say. You were so close to being done. Then, you’d be in your dream career. All the hard work was going to be worth it. The thousands of hours in clinicals, the hundreds of hours in class. The countless sleepless nights and caffeine filled days. Yes. It would be all worth it. Just a couple more months to go. And Jay was by your side.
194 notes
·
View notes
Text
Laser Teeth Whitening - At Home Bleaching.
Content
In Surgical Treatment Whitening.
Teeth Whitening At The Practice
Teeth Whitening Blog Site.
Specialist Teeth Whitening In Dorchester.
Laser Teeth Whitening Solutions In Manchester.
Furthermore, some teeth whitening products may experience some discomfort while using them. Bleaching agent can also cause teeth sensitivity or irritation. Some users may experience a stinging sensation while using the product. If this happens to you, it is best not to use the product until the problem is resolved. Consult your dentist if this is experienced to avoid any further complications.
In Surgery Whitening.
Is it worth getting your teeth whitened at the dentist?
Professional teeth whiteners are safe, effective, and done under the supervision of a dental professional. In most cases, it is worth the extra cost to visit the dentist to get long-lasting, safe results. Yes, teeth whitening is very safe when done correctly.
Teeth Whitening At The Method
Most teeth whitening procedures are done with the use of a bleaching agent, usually hydrogen peroxide or carbamide peroxide. A bleaching gel is applied to the teeth and left on for a set amount of time depending on how sensitive the teeth are to whitening agents. It can take several applications for a noticeable difference in the tooth's color to become apparent. Hydrogen peroxide has been the most effective at whitening as well as being the safest, but some people are allergic to it, which limits its use to teeth whitening.
"See to it you see your dentist and hygienist for six monthly exams and also cleansing. Some individuals go every three months if they consume a lot of merlot for example. We're grinning from ear to ear at all the nice things individuals have stated about us. Keep reading and also you'll see why we are just one of one of the most popular dentists in Cardiff. At celebteethwhitening’s free best teeth whitening high-wycombe , we likewise supply Mobile Laser Teeth Whitening solution around the Manchester as well as West Yorkshire location.
One of the major side effects of teeth whitening includes gum tenderness and mouth sores. You may experience pain in your gums if you were not careful enough when using the teeth whitening procedure. Most people do experience minor mouth soreness but there are some who experience severe pain after undergoing the procedure. Hence, it is important that you discuss this matter with your cosmetic dentistry professional.
Teeth Whitening Blog.
Teeth whitening or teeth bleaching is usually the cosmetic procedure of whitening the yellowish or brownish color of teeth. teeth whitening warwick is a cosmetic treatment to improve the smiles of people who don't feel their smiles are all that appealing. Whitening is most often desired when teeth become stained over time and is also done by affecting the color or appearance of the tooth's surface. Some people choose to whiten their teeth when they need a quick fix to their situation, like a job interview where they need to have a whiter and brighter smile to get the attention of the hiring person or to simply brighten up their day.
youtube
Teeth sensitivity is another problem that is associated with the bleaching process. It is also considered to be a normal result of the teeth whitening process. The reason for this is because the sensitivity stems from the chemical used during the dental procedure. If you have sensitive teeth, it may not be possible for you to tolerate the intensity of light when you are undergoing the dental procedure. Hence, it is important that you consult your dentist if this problem persists after you have completed the entire teeth whitening process.
Prices differ as well as laser whitening is extra costly than professional whitening.
We'll also give you some top-up trays to use in your home to assist maintain your whiter smile.
After that, utilizing your mouthguard in the house, you routinely apply the gel for a specified period of time over 2 to 4 weeks.
Adhering to a preliminary assessment † with your dentist, when you have your Philips Zoom!
treatment, it takes an hour, as component of a two-hour consultation, so you'll just sit back and kick back while your dentist deals with whatever.
Some whitening gels can be left on for as much as 8 hrs at once, which reduces the therapy period to 1 week.
Otherwise, teeth whitening by a dentist or various other dental specialist can only be done privately since it's taken into consideration to be a cosmetic therapy.
Another issue that is considered safe when it comes to teeth whitening is the procedure used by the dentist. There have been cases observed where patients experienced discomfort after whitening their teeth at the dentists. However, there are several procedures available to deal with such problems and you may consult your dentist before using any of them. However, your dentist would be able to recommend the most suitable procedure to you.

The bleaching agent that one will use should be approved by the Food and Drug Administration in order to avoid serious side effects. Moreover, teeth whitening methods can only work effectively with the support of bleaching agent that contains a good concentration of hydrogen peroxide and carbamide peroxide. These ingredients have the capability to penetrate deep into the surface of teeth to reach the stain.
There are two types of teeth whitening products that can help you get rid of your discolored teeth. One is the tray system and the other is the bleaching pen. However, both have their own advantages and disadvantages. Toner tray system involves applying the bleaching gel directly onto the teeth. However, this method is not very effective as it only brightens the shade of teeth that are discolored and not eliminate the discoloration completely. On the other hand, using the bleaching pen is less effective as compared to the trays as the gel gets accumulated in between the teeth unlike the trays, which remain on the teeth for an extended period of time.
youtube
Our reasonable profession rates plan guarantees you get a top quality solution at a very budget-friendly rate without leaving the convenience of your office or home. We work around you to fit your routine any time of the day, 7 Days a week. Our skilled personnel will place a retractor right into your mouth, this will certainly allow the mouth to stay open throughout the procedure.
How to Brush Your Dog's Teeth Without All the Fuss - Yahoo Lifestyle
How to Brush Your Dog's Teeth Without All the Fuss.
Posted: Wed, 30 Dec 2020 22:59:00 GMT [source]
Specialist Teeth Whitening In Dorchester.
Tooth whitening or teeth bleaching is the procedure of shining the shade of teeth at lightening or whitening the color. Teeth whitening can be done by either using bleaches or teeth whitening products, which are available at the nearest drugstore or supermarket. There are many kinds of teeth whitening products that one can use to whiten the shade of teeth. However, these products have some limitations that one should consider before using it on their teeth.
Nestled amongst the busy upmarket style boutique as well as cafés of the Lisburn Road you will certainly locate The White residence. Our Teeth Whitening Belfast City clinic opened its doors in 2011 and also we lie in a very easy to gain access to location on the Lisburn road BT9 next door to Tesco. Do not hesitate to drop into our Teeth Whitening Belfast clinic as well as greet to our friendly staff as well as grab a leaflet. When you see any kind of website, it might save or recover details with you internet browser, typically in the kind of cookies. Considering that we value your right to personal privacy, you can select not to allow information collection from specific kinds of solutions. Nevertheless, not enabling these solutions may influence your experience as well as what we are able to supply you.
Locate Your Local Bupa Dental Treatment Method Offering Teeth Whitening
The toothpaste that you use plays an important role in bleaching your teeth. The toothpaste that you use should contain fluoride to prevent the formation of plaque on your teeth. It is also recommended that you should brush your teeth with fluoride toothpaste regularly to minimize the formation of plaque. It is important to note that although your dentist has advised you to whiten teeth using the at home method, you may still have certain whitening methods to follow. You may discuss this issue with your dentist.
Best teeth whitening strips and toothpaste - CNET
Best teeth whitening strips and toothpaste.
Posted: Tue, 29 Sep 2020 07:00:00 GMT [source]
After positioning it right into your mouth and also placing a set of protective safety glasses on. Because of the non-invasiveness, people that are generally frightened by a journey to the dental practitioner no longer need to be. Due to the fact that there is no discomfort, there is no need for any person to be anesthetized for this procedure. Best quality cosmetic work that will certainly fit your individual needs.
Why won't my teeth whiten?
As people age, their enamel can become thinner, a result of decades of wear and tear. The thinner the enamel, the more likely the yellowish dentin shows through. That's why older people often have yellowed teeth. Bleaching products won't help in this situation because they don't affect the dentin.
We use cookies from 3rd component services to supply you a far better customer experience. We use Microabrasion to remove superficial white spots a technique of brightening the superficial enamel with acid as well as pumice can be used. This gives a conservative, immediate renovation in the appearance of the teeth. When obtaining Laser Whitening, patients must additionally obtain a residence set-- such as Shop or Enlighten. Your smile is among the initial things individuals notice about you, as well as it has a big impact on your self-confidence. We advise a top up at around 4 weeks after your very first therapy and once every 6 months there on after for optimum enduring outcomes. A sterile mouth guard is after that eliminated from a secured foil packet and the non peroxide gel is after that used on it.
#teeth whitening#laser teeth whitening#best teeth whitening#teeth whitening UK#teeth whitening England#teeth whitening United Kingdom
1 note
·
View note
Text
Prostatectomy Surgical Treatment: What Are The Difficulties?
2 In 1 Hifu Facial Facelift Hifu Genital Tightening Maker Skin Lift Device
Content
Treatment For Lines & Wrinkles At Orchard Home:.
What Can Profhilo Treatment Help With?
What Are Botox Side Effects?

The therapy works by boosting the degrees of dopamine in the substantia nigra. Numerous phase III medical tests have actually revealed istradefylline, when taken orally, to be safe and also efficient in the treatment of PD throughout OFF durations. If accredited, istradefylline will give a new restorative option to taking care of people with Parkinson's as the first non-dopaminergic add-on treatment. Tideglusib is being advancement for the therapy of genetic myotonic dystrophy kind 1. CMD1 is a type of myotonic dystrophy type 1, a rare, genetically figured out neuromuscular disorder. CMD1 begins at or around the time of birth and also is characterised by serious muscle weak point, cognitive impairment as well as various other developmental abnormalities. The condition typically happens when the mommy currently has DM1 and then it is handed down to her child in a much more severe kind.
Which is better for wrinkles retinol or hyaluronic acid?
Is one better for your skin than the other? While hyaluronic acid works its repairing and hydrating magic on the upper layers of the skin, retinol is able to have multiple effects deeper within the skin.
CMD1 is commonly associated with substantial clinical morbidity and sudden death. No details therapy is currently on offer, although encouraging care to manage symptoms is offered. Treatment intends to boost feature as well as wellness and includes antispastic dental medications, physical rehabilitation, and also off-label use of botulinum contaminant type A. Botulinum toxin type A is presently in stage III scientific tests contrasting its impact on lower-limb spasticity as well as scientific international impact. Dermal Filler is a clinical visual product derived from Hyaluronic Acid a naturally taking place compound in the body.
Treatment For Lines & Creases At Orchard Home:.
In our hide clinic we utilize various brand names of Botulinum Contaminant depending on our individuals wishes. The most usual brand name we are requested for is Azzalure ® however essentially all brand names are the same contaminant produced by different firms. Botox is the most generally used name to explain the toxin and also Botox Therapy. We offer a wonderful variety of treatments for all your Visual requirements. RBF-- People are getting fillers and also botox to free themselves of a stern relaxing expression. Radio frequency is a procedure for non-invasive firm of loose or sagging skin. The mild method to rejuvenate the skin, using Real ® Dermaroller.
Chippenham hifu non surgical facelift =embed">
Restylane ®, Juvederm Ultra ®, Teosyal ®, Perlane ® as well as Belotero ® are all brand names for Hyaluronic acid based facial fillers. there are a number of Botulinum Toxin therapies readily available under various trademark name. Each is a prescription medicine in the UK and also this ought to be you primary problem when looking for anti wrinkle injectables. Our clinically trained as well as knowledgeable Visual Registered nurse Prescribers have a wealth of experience to guarantee your therapy works and also most significantly delivered securely. Botox can be utilized to treat migraines really successfuly when administered by a physician. Our degree 7 qualified nurse prescribers can discuss your signs and symptoms during a consultation and also may suggest Botox therapy for migraines.
What Can Profhilo Treatment Help With?
It promotes your skin by improving collagen production and also makes it fix itself. It is clinically verified to deal with acne marks, to company and tighten up the skin to lower sun damage and eliminate visible stretch marks. Right here at The Quay Dental Method in Bideford we offer a wide range of the most up to date specialist face and body treatments. Side -impacts such as bruising, swelling and inflammation at the shot site prevail as well as self-limiting and also ought to diminish within the next couple of hours of therapy.
SonaCare Medical Announces Chinese Regulatory Approval - PR Web
SonaCare Medical Announces Chinese Regulatory Approval.
Posted: Tue, 21 Jul 2020 07:00:00 GMT [source]
Arnica tablets/gel or Vitamin K oxide cream can be made use of if wounding is substantial and long term and can use up to 10-days to resolve. If you get on specific medications such as blood thinning drug such as aspirin, warfarin or steroids or Roaccutane then is ideal to seek medical recommendations from your physician before planning such therapies.
What Are Botox Adverse Effects?
If you are a physician as well as wish to discover how to provide these therapies, please see our offered programs right here. When it comes to aesthetic injectable treatments, whether they are for visual or restorative factors, it is critical that you make educated choices. Make certain that you choose a trustworthy practitioner that has a clinical history to ensure that you are in the safest hands to reduce any kind of potential threats. Botulinum toxic substance can aid eliminate frustrations that are triggered by teeth grinding, which is an amazing alleviation for those suffering from TMJ disorder. This therapy can likewise help those that do grind or squeeze their teeth prevent pricey oral job brought on by these activities. The relief after this therapy permits the person to ultimately execute daily tasks that many consider approved such as speaking, chewing and swallowing, without pain.

Just how much does Botox price at The Light Touch Visual Appeals Facility in Bury? We have a basic prices framework and offer extremely great worth for money when contrasted to any kind of various other centers. You will be tough pressed to find a less expensive therapy supplied by Degree 7 skilled registered nurses. Botox when administered properly is not painful due to the dimension of the really great needle utilized to carry out the item. It typically lasts in between months nevertheless this can be much shorter or longer. Typically results start to reveal in between 2 -3 days post therapy with the fuller effect revealing between weeks.
Hifu Body Contouring And Therapy.
We typically discuss this in our complementary consultation where we experience the various therapy options available to you and also the threats as well as benefits of each treatment. Contact us to organize an assessment and we can talk through your expectations of treatment with you. Quick, pain-free and also very easy-- Botox therapy takes around half an hour to carry out as well as is likewise pain-free. It is advised not to touch the treated areas for a minimum of 4 hours. At the initial browse through the conversation and also exam can take around half a hr. Anti-ageing and anti wrinkle shots in Essex are executed by clinically educated medical professionals. Our therapies are therefore tailored to you instead of being a "one size fits all".
What collagen does Jennifer Aniston use?
Original Collagen Peptides
Here's what Aniston had to say about this fan-favorite supplement: “My go-to collagen routine is adding Vital Proteins Collagen Peptides in my morning cup of coffee or smoothie — so easy to use.” This unflavored powder also contains other skin saviors like vitamin C and hyaluronic acid!
The ASA likewise ruled that the claim was a medicinal one and also had been made without the essential MHRA authorisation. Online marketers who use injected therapies which aren't POMs in addition to supplying Botox might promote utilizing the term "aesthetic fillers" or "infused fillers". They should, nonetheless, guarantee they do not describe Botox directly or explain therapies at all that may indicate Botox is being offered.
What Will Occur If I Stop Having Therapies?
Online marketers have to take care to stay clear of an indirect promotion of the product. https://wootton-bassett.spireaesthetics.co.uk/hifu/ has gotten lots of attention with many stars rumoured to have undergone this therapy. The aging process happens to all of us at some point whether we wish to confess or not! One of the ways in which this can show up is with a slight decreasing in the brows. Istradefylline is a discerning adenosine A2A receptor inhibitor; these receptors are found approximately the mind that suffers deterioration in PD.
youtube
#hifu review#hifu reviews#hifu Benefits#hifu Advantages#hifu before and after#hifu treatment cost#hifu reviews 2021#hifu treatment pros and cons#hifu reviews UK#hifu facelift reviews#hifu facelift cost uk#hifu treatment cost uk#hifu facelift near me#hifu treatment near me
1 note
·
View note
Text
Puppy Love
Main Characters: Bucky Barnes x Reader
Summary: A continuation in the What He Wants universe where Bucky and you spend the weekend snowed in with your new puppy.
Warnings/ Content: definitely a warning (spoiler?) the puppy breaks his leg in the snow. It’s not graphic or very descriptive of the injury but it’s a topic and he’s gonna be just fine after the vet trip. But it’s still a little heart breaking because... puppy.
Word Count: 2518
Author’s Note: First off, a HUGE thanks to @lancsnerd who gave me the deets on how to post a fic with the “keep reading” option on an iPad. This fic would not have been posted anytime soon without her help. Also, @lancsnerd is a BRILLIANT fanfic writer so if you haven’t read anything of her’s yet you are missing out and should do so ASAP. Now about Puppy Love... I seriously meant to write just a sweet little fic about Bucky and the reader adjusting to puppy parenthood but.... I’ve been angsty lately. Sorry not sorry. When I was a little kid my dog broke his leg in the same way Poe does and got a little purple cast too. So that’s where that came from. If you haven’t read the rest of the What He Wants series it isn’t super necessary but I’m kinda in love with it so you can find the master list HERE if you want to check it out first.
Okay, I’ve rambled enough for now. Love you all & thanks for reading!! XOXO - Ash
Puppy Love
There was a distinct learning curve for all three of you when Poe arrived. You had visions of early morning snuggles, warm, and cozy in bed with your man and puppy. The reality was something very different.
“Oh no! Not again!” you scold as Poe tries in vain to wiggle his little butt under your blankets. It’s your first weekend morning with him and you just want to sleep in a little. Bucky had taken him out for his morning potty trip and now he was ice cold and far too wiggly.
“Come on, he just needs mama snuggles.” Bucky protests on Poe’s behalf, giving you equally sad puppy dog eyes.
You grumble but make room, allowing both man and beast to slide into the warm bed next to you. It’s barely a minute before Poe and Bucky are both restless and resort to playing peek-a-boo with the comforter. Cold air hits your bare skin and you squeal, displeased with the commotion in your bed. Giving up on your dreams of warm, snuggly weekend mornings you get up to find clothes and start the coffee.
“My boys.” you call out affectionately from the doorway when you return. Bucky is sprawled out on his back with Poe flopped on top his chest, having apparently worn each other out with their play. You set the coffee mugs down on your dresser and pull your phone off of it’s charging station so you can snap a few pictures of the saccharine sweet domestic scene. Bucky grins up at you from the bed and extends his right hand, beckoning you to join them.
Bucky straightens up so you can hand him his mug and Poe reluctantly shifts down onto his lap. He hasn’t bothered to put his prosthetic on yet but he did carefully pin up the empty sleeve on his left; there will be no risking leaving it down in bed and having Poe think it’s a toy again. “I think the snow’s almost here. The wind was picking up a bit while we were out earlier.” Bucky tells you.
“I hate March snow storms, just when you think we’re done… Nope! And I’m sorry it ruined your party, love.” You kiss his shoulder gently to punctuate your apology. You had spent an hour on the phone with Pepper canceling and rearranging everyone’s plans the night before when the severity of the pending storm was confirmed.
“It’s not a big deal, we can go up in two weeks and it’ll be just as fun. ‘Sides, I’d rather spend the weekend curled up with you two anyway.”
Shooting him an indulgent smile you lean your head to rest on his shoulder lightly. As much fun as it would have been to see everyone again, a quiet weekend at home to get adjusted with Poe is a much more appealing option. Bucky is, as you suspected, a completely over the top puppy-dad. He had spent the better part of his nights the past two days finding “the best” dog care items out there from a feeding bowl with a time release function to a cozy dog bed that looked like an actual human bed. Toys were coming in endless supply as well as books on training and Bucky had already started talking about moving Poe onto a “filler free” puppy chow as soon as possible. It was all a bit over the top but Bucky cared so much, you didn’t have the heart to dissuade him.
By noon the storm was in full swing and so were Bucky’s efforts to train Poe. The books all agreed that formal training should wait until he was a little older but Bucky was determined to teach him the basics. So far you had been lucky with no accidents and he wasn’t big on barking so that left what Bucky deemed the “fun” bits of training like responding to small commands to sit, stay, follow, speak, roll over, and shake. You watch quietly over the top of your book as Bucky sits cross legged on the floor with Poe trying to teach him “speak”, mimicking a yipping sound to encourage him. It’s tempting to get a quick video of the ridiculousness for the Avengers group chat but you resist the urge long enough that they moved on to “shake” before you can.
Eventually Bucky hops back up announcing it’s time for another potty break, scooping Poe up in his arms. Bucky dresses him carefully in the little red and black flannel dog coat he had purchased for him, insisting it’s too cold for a tiny dog outside. Bucky had been amazed by next day shipping and the plethora for dog items on Amazon. Not that you had any room to talk, you had found a Bucky-sized coat that matched Poe’s exactly and it was due to arrive later that afternoon. It was too good of an opportunity to pass up and their twinning is guaranteed to bring you endless amounts of amusement each winter.
They are only outside for a minute when you hear a sharp, high pitched yelp followed by Bucky screaming Poe’s name. You bolt up from the sofa, forgetting the blizzard outside and racing into the storm. The ice and snow bite at your sock clad feet and the wind hitting your face stings like needles. You yell for both of them frantically, fearing the worst, until finally Bucky comes into view holding a crying Poe in his arms. Bucky is a mess, eyes large and watering from more than just the storm, his expression panicked. “He got a little far out so I called him back and he was being a good boy and listened but he when he jumped back up on the patio he slipped on the damn ice and fell off. He couldn’t get back up and he’s not letting me touch his back leg now. I think he’s hurt bad. What do we do?” Bucky rambles breathlessly, clinging to the tiny, whining puppy in his arms.
“Okay.” you steel yourself against your own growing concern. They both need you to be strong right now. “Okay, we need to get everyone back inside so we can see what we’re dealing with and go from there.”
Bucky nods and follows you back up to your apartment where you can better assess Poe’s condition. It’s obvious something is seriously wrong by the way Poe keeps his leg curled up close to his body and actually growls when you get within an inch of it. It’s his back right leg and Bucky has been careful not to hold him there. “Let’s set him down and see if he can put any weight on it.” you suggest and Bucky shoots you a look but places him carefully on the floor between you. Poe’s leg stays curled close to his body and he limps three leggedly towards his bowl. “I’ll call the vet now.” you say and Bucky hurries over to pick him up. You watch as Bucky carries Poe over to his food bowl and sits down with him on the floor to hand feed him so he can stay comfortable in Bucky’s arms.
The vet agrees he needs to be seen immediately and they have a 24 hour emergency clinic that can take them. Thankfully Poe and Bucky are already bundled up so as soon as you have your coat and shoes on you are out the door and slowly navigating the roads to the vet’s office. Bucky sits ramrod straight the entire ride, a haunted look in his eyes as he watches Poe, whispering a never ending stream of comforting words to him. His fear and worry are palpable and it’s heartbreaking that things have gone so terribly wrong just a few days into having him.
The emergency vet clinic is empty when you arrive and they take Poe back right away. Bucky glares down the nurse who requests she take him back for xrays and you step in. “Sweetheart, she has to do this. If his leg is broken we need to know.” you tell him softly, rubbing his back in a soothing motion. Bucky nods stiffly and hands over Poe to the patiently waiting nurse. “I know you’re worried, I am too.” you assure him.
“He’s just so tiny. And it’s my fault. I was calling him back and he was hurrying because he’s just such a good boy and then he fell...” Bucky’s voice cracks and he trails off, not trusting his voice to continue.
You wrap your arms around him, pulling him close. “I know, love, I know.” You tuck your head below his chin, snuggling against his still cold coat and letting the contact comfort you both.
It is an agonizing ten minutes until the nurse reappears with Poe. They gave him something for the pain but encourage Bucky to not touch his hurt leg when he takes Poe back into his arms. She tells you the vet will be in to go over the results in a few minutes and thankfully the waiting time is brief.
“Hi folks.” a tall, grey haired woman announces as she joins you in the small exam room. “I’m Doctor Kate, it’s good to meet you, though it could have been under better circumstances.”
You shake her hand and give her a quick smile. She is the vet you were supposed to have Poe’s well check with next month. “I’m Y/N and this is my fiance, Bucky.”
“And this little guy must be Poe.” she reaches out to scritch Poe behind the ears affectionately. “So, we have bad news and good news.”
“Just give it to us straight, doc.” Bucky requests, his voice thick with concern.
“My kind of people.” Dr. Kate gives him a kind smile before continuing, “So your little guy did break his leg when he fell. He’s going to need a cast while that heals but the good news is that puppies heal amazingly fast. About half the time of an adult dog. So we’ll get you all back for another set of x-rays in about four weeks and hopefully the cast will be able to come off then too. Do you have any questions?”
“Do you have any care instructions for while he’s healing?” Bucky asks.
Dr. Kate nods, “Yep, I have a whole bunch of papers printed out for you to go home with. You can start reading over them if you want while we get Poe’s cast on him.”
Bucky thanks the doctor and trades her Poe for the stack of papers. You curl up under his arm to start reading along with him while the doctor takes Poe off to get his cast put on. “He’s gonna be okay.” You remind Bucky.
“I know, but… it’s still hard.” He sighs heavily, scrubbing a hand across his face.
“But we get through it. When have our lives ever been easy?”
Bucky huffs a wry laugh, “Yeah. Pretty much never.”
You tilt your head up to kiss him, needing the grounding connection of your lips against his. A sigh slips from your throat and you nestle in against him when you finally break the connection.
Dr. Kate returns a few minutes later with Poe who is sporting a small purple cast on his broken leg. “Do you have any more questions?” She asks handing the puppy back to Bucky’s eager arms.
You shake your head, “No, I think we’re good for now. Thank you so much for helping him.”
“That’s what I’m here for. You folks have a safe trip home.”
You shake her hand and gather your things to leave.
The ride home is more difficult in the storm than the ride there but the mood inside the car is significantly less tense. Bucky is talking softly to Poe who is looking a little more alert than he had been.
“You know,” Bucky tells him, “I fell and got hurt too, a really long time ago. It was scary but I’m okay now and you’re gonna be okay too. And you, lucky pup, get to keep your leg.”
You take a shuddering breath, trying not to become overwhelmed with emotion while driving. You know exactly what fall he’s talking about and it makes your entire body ache to think about what he had gone through at the hands of HYDRA because of it. How he can so calmly talk about it now is extraordinary but shows he really has been working hard to move on from all the trauma in his past, and god knows there was a lot of it.
Safely back in your apartment, Bucky sets Poe down in his new doggie bed and tucks him in with a tiny fleece blanket which is as necessary as it is cute. He joins you on the sofa where you're curled up to watch Netflix, burrowing in so that his head rests on your chest. You move your arms to hold him, his adrenaline rush from earlier is crashing now that everyone is home safe. Bucky helps pick out a show and you wiggle your way out with a promise to be quick so you can get two tumblers of whiskey. After an afternoon like that, a little whiskey is absolutely called for. With the serum degrading, he’s been able to feel the effects of alcohol again, a new and amusing discover for you both.
You cuddle up once again, letting him use you as a pillow, and hand him his glass. He’s picked out a documentary on the solar system and it doesn’t surprise you in the least. Bucky is fascinated by space and loves learning more about the world outside of your own. He sips his drink slowly and you can smell the sharp sweetness on his breath when he cants his head up for a leisurely kiss.
“He really is gonna be okay.” Bucky says with a long sigh.
You smile down at your poor worried soldier, “Of course he is. A few more weeks and it’ll be like it never happened.”
“Watching him fall into the snow… it was awful. Brought back some memories I wish I didn’t have.”
“I can’t even imagine. But you held it together. You helped our boy and got him to the doctor so he could get patched up. You did everything you possibly could have.”
“I know.” He says slowly, letting his mind catch up to everything he’s feeling, “I know I did. I think I just need a little time to process everything that came up today. It was a lot.”
“Oh, sweetheart, of course. We don’t have to do anything else this weekend except lay together watching space shows and drinking whiskey. If you want to talk I’m here, and if you want to just sit quietly we can do that too. Whatever you need, love.”
“Just need you.” Bucky says into your chest, nuzzling in comfortably.
You card your fingers through his silky hair, watching as your engagement ring catches in the low light. “You got me. Always.”
Tag list lovelies: @my-current-fandom-is @blacklightguidesnic @amazonianbeauty @abswritesfandoms @rupestria @dark-night-sky-99 @ladyemofhousestark ***IF ANYONE WANTS ADDED / REMOVED JUST LMK :)
#Bucky Barnes#bucky fanfic#bucky barnes x reader#bucky barnes fanfic#Protective Bucky#what he wants#marvel#Marvel Avengers#marvel fanfic#Marvel fangirl#MARVEL FANDOM
37 notes
·
View notes
Text
California BBS Requirements Towards Obtaining a Professional Clinical Counseling License
In this post I’m going to talk about everything I had to fulfill to get my Associate Professional Clinical Counselor (APCC) registration number and what requirements I have left to move onto the next step, Licensed Professional Clinical Counselor (LPCC). This will include all paperwork, fees, additional courses, etc. At the end of the post, I will include the approximate total of how much everything has/will cost me.
✔ = What I’ve completed so far
My comments are in bold.
Information about the California Board of Behavioral Sciences’ (CA BBS) requirements per https://bbs.ca.gov/pdf/forms/lpc/lpc_app_oos_01012016.pdf
---
Application Fee for Associate Professional Clinical Counselor Registration was $100
Fee for LiveScan Fingerprinting $32. I think I paid $150 for something fingerprint related?! It’s been a year and I can’ even remember...I’ll find out eventually.
How much it cost me to get fingerprints done at my local county jail- $20
Physical transcripts mailed to the CA BBS 3x (I had to send it multiple times because the CA BBS told me they did not receive it) $36
EDUCATIONAL REQUIREMENTS
✔ Master’s degree or higher that is counseling or psychotherapy- I earned my degree outside of CA, so my university’s Program Chair and I had to submit a Out-of-State Degree Program Certification form (in addition to some course syllabi).
For me, the cost of my degree was about $21,000 in student loans with ~5-6% interest per loan. The $21,000 was for graduate in-state tuition alone and this total was after factoring in approximately $10,000-worth in scholarships/stipends. I’m not calculating rent and living costs. Although, it was fairly cheap since I lived in Emporia, Kansas- a town with a whole lotta nothing (except for some kind, helpful mentors and peers).
✔ Courses to take in addition to having a Master’s:
Initially, I thought I would have to spend hundreds of dollars on courses offered at accredited colleges or universities. However, I found a cheap, online continuing education website called AspiraCE through the California Association for Licensed Professional Clinical Counselors (CALPCC) website. I bought a one-year subscription for $129.99. So over the course of a couple months I would plough through these additional courses during my work breaks and weekends. I haven’t found a cheaper option for these courses yet, but if I do I’ll post it in this blog.
✔ a) Suicide Risk Assessment and Intervention 6 hours of coursework or applied experience All applicants submitting an application on or after January 1, 2021 (otherwise will be required upon license renewal). See BPC section 4999.66
✔ b) Human Sexuality 10 hours Instruction must include the study of the physiological, psychological, and social cultural variables associated with sexual behavior, gender identity, and the assessment and treatment of psychosexual dysfunction. See BPC sections 25 and 4999.62 and Title 16, California Code of Regulations section 1807
✔ c) Spousal/Partner Abuse Assessment, Detection and Intervention 15 hours Instruction must cover spousal and partner abuse assessment, detection, intervention strategies, and same-gender abuse dynamics. See BPC section 4999.62 37A-642A (New 01/2020) 4 5. ADDITIONAL COURSEWORK LPCC OUT-OF-STATE APPLICANTS (continued) Course Length Content Required
✔ d) Child Abuse Assessment and 7 hours Instruction must include detailed knowledge of the Reporting in California California Child Abuse Neglect and Reporting Act (CANRA). It must also include assessment and methods of reporting of sexual assault, neglect, severe neglect, general neglect, willful cruelty or unjustifiable punishment, corporal punishment or injury, and abuse in out-of-home care. The training shall also include physical and behavioral indicators of abuse, crisis counseling techniques, community resources, rights and responsibilities of reporting, consequences of failure to report, caring for a child’s needs after a report is made, sensitivity to previously abused children and adults, and implications and methods of treatment for children and adults. See BPC sections 28 and 4999.62 and Title 16, California Code of Regulations section 1807.2
✔ e) Aging, Long Term Care and 10 hours Instruction must cover aging and long-term care, Elder/Dependent Adult Abuse including biological, social, cognitive and psychological aspects of aging, and instruction on the assessment and reporting of, as well as treatment related to, elder and dependent adult abuse and neglect. See BPC section 4999.62
✔ f) Mental Health Recovery Oriented Care and Methods of Service Delivery 45 hours or 3 semester units Instruction must cover principles of mental health recovery-oriented care and methods of service delivery in recovery-oriented practice environments, including structured meetings with various consumers and family members of consumers of mental health services to enhance understanding of their experience of mental illness, treatment and recovery. See BPC section 4999.62
✔ g) California Cultures and the Social 15 hours or Instruction must include an understanding of various and Psychological Implications of 1 semester California cultures and the social and psychological Socioeconomic Position unit implications of socioeconomic position. See BPC section 4999.62
✔ California Law and Ethics course (included in AspiraCE) - Counselors from other states must take the 18-hour course in California
APCC REGISTRATION ANNUAL RENEWAL COST- $100
EXPERIENTIAL REQUIREMENTS
3,000 hours of post-master’s supervised counseling experience. 1,750 have to be Direct Client Contact hours. I’ve completed 6% of my post-master’s hours as of last week. I would have been much further in my experiential hours, but it took almost a year to receive my APCC registration number. After going back and forth with the CA BBS, my hours officially began on March 9, 2020. I was working with patients at least 6 months prior to that, but unfortunately, I had to discount those hours.
I found a supervisor that would see me for $50 and another that would see me for free. While I was looking for a supervisor, I talked to people who were going to charge me $150 per hour of supervision. In my opinion, that is outrageous. I understand that as a qualified, accomplished supervisor, you’d want to charge for the quality of supervision. HOWEVER, if I was a supervisor, I’d do it as cheap as possible. Getting a license is super expensive and it’s rare to meet a trainee who doesn’t have student loans. Anyway, I’ve probably spent about $2,000 this past year on supervision. I know that seems like a bummer since much of it couldn’t count towards my clinical counseling hours, but my supervisor is also an art therapist so I just counted everything towards my art therapy certification. And YES! Hours can simultaneously count towards clinical counseling and art therapy (this is for another blog post).
EXAM REQUIRED
NCMHCE – taken after experiential requirements have been fulfilled. It costs $275 to register for the NCMHCE.
AND
California Law and Ethics/Jurisprudence Examination– taken while acquiring supervision. I am trying to register for this, but #COVID. Also, the initial exam fee cost $100. It must me taken every year for APCC registration renewal and I believe it costs $100 to re-take it.
---
So, let’s talk about my overall cost. In-state tuition was approximately $31,000 (my total cost in student loans and scholarships/stipends). It cost me $467.99 to register as an APCC with the CA BBS. My first year of supervision costs $2,000. From graduate school to obtaining an LPCC, it would cost me about $39,042.99. For people who just want to know how much it may cost me to get licensed post-graduate school, it’ll be about $8,042.99. That’s on the cheaper end too because I’m pretty frugal.
After listing the requirements and costs, I’m thinking, is it all worth it? For me, I’ll say, “Sometimes no, but overall, yes!” I will answer my own question in the next blog post. Frankly, I’m exhausted from running these numbers.
1 note
·
View note
Text
End of Active Treatment
Month 14, Day 21
I went in to see Radiation Oncologist. She not only cleared me for “a few months,” she’s set me to six months. Hooray.

Which means I’m no longer in “active treatment,” Which also means, for those of you who only follow me here, I’m going to https://medium.com/@patrickkmc10
I may or may not update this blog, but it’ll look more like my updates prior to 2017 - infrequent and occasionally garbled. I now have to figure out what to do, post-cancer, even though GBM is, in the most technical sense, forever. I have another neurocognitive exam tomorrow, then it’s into the great wide open. Maybe We’ll see.
So, I began this weird, freakish, writing project 82 years ago in undergrad as an e-mail to all my old high school friends and family (yeah, if you signed, “keep in touch” in my yearbook, I did keep in touch), occasionally during my time as an EMT, and intermittently in grad school. Then I got into medical school, and I somehow lost the time and/or will to write, and only intermittently did this blog during the recovery from tumor #2. That was a mistake.
If there is one take-away moment I’ve had in the past year, it’s that I should - even if it’s only as a hobby - be writing. Every day. You should, too; if you’re not living a life where you come home with a new story or joke you want to share, you’re not maximizing your potential. Based on the people who tracked me down - from roommates I haven’t thought of in a decade, to people I’ve known for over 20 years, to the radiation tech who called me after-hours to thank me for writing them a thank-you note, it’s that my best opportunity to leave something like a legacy behind is to leave a paper trail of notes. I’ve been informally studying intelligence for most of my life, and the two things that seem absolutely unique to our species are opposable thumbs, and the written word. Other species do rudimentary math, chimpanzees have entered the Stone Age (according to anthropologists), ours is the only one that seems to have the idea of leaving a written record of events.
When I was very young, I wanted to be a writer. Then life happened, in the form of my first brain tumor at age 17, and I wanted to be a doctor, because that was the only way I could see forward to helping others in my position. I think I got blinded by that for far too long, and then, six years ago, I really wound up in deep shit thanks to Tumor #2, an astrocytoma (which inevitably develops into glioblastoma). I probably passed up far too many opportunities over the last six years under the belief that my time had already come. I think I gave up.
Then, on Nov. 10, 2017; I got the news I’d been dreading for over a decade: I had a terminal diagnosis. And, throughout this whole, horrific process, there was one thing that kept me going: finding out there were a few people - not enough, but a few - who had made it through the deepest, darkest trenches of the abyss and made it out the other side. I’m not there yet - I’m still in the recovery phase, and I still have a disease the World Health Organization has described using phrases like “abysmal” and “inevitable.” But, in the last year - I know, because I’ve literally spent some days just hitting the “refresh” button on the FDA’s clinical trials website - science has made huge strides in developing immunology-based treatments that should last.
The lasting lesson of the past year is that I should’ve spent a lot more of those six years networking and making contacts, because I’m apparently really good at that, and that’s a far better route to success than gnawing away at something I’m not great at. So, if some of you get a phone call in the near future from me asking for a favor, I do hope you’ll help me out.
The final lesson - apart from the importance of self-care (which is like shoveling snow - it’s not taking a relaxing bath, it’s doing the important-but-boring stuff like eating properly, getting to the gym every day, and showing up for your blood-draws).
Speaking of showing up for the blood samples, Radiation Oncologist told me that I was one of the few patients who’d consistently shown up for the neurocognitive study/assessment. This struck me as very odd; I also saw on the Barrow Neurological Institute’s page that no patient - no one - has ever refused to have their tumor tissue banked. That makes a little more sense. When you really do believe your end is imminent, you stop worrying about yourself, and start worrying about the next folks in line. I suppose that’s the defining trait of our species; we actively help others when our own end is in sight. And, as the year went on, I started to feel - to believe - that my life wasn’t over, it was just - in a weird way - beginning. I think that’s what I lost six years ago, and I’m starting to recover. And, that, I think, is the handle on the whole, weird, “brain cancer” thing that you, reader, can take with you to your own life - every moment should feel like you’re beginning something grander than your own self.
3 notes
·
View notes
Text
Title: Seams
Series: My Hero Academia / 僕のヒーローアカデミア
Pairing: Yaoyorozu Momo/Todoroki Shouto (TodoMomo)
Summary: Experience will always be the best teacher. (T+, Gen)
Note: I lost a bet. But I don’t know how to write smut. Very, very slight spoilers for manga chapters 96-114. (for @peonydee ) Also simultaneously posted in AO3 [LINK]
Yaoyorozu sighed, then coaxed his hold to relax on the needle forceps.
One bright eye stared at her pinched expression, before he glanced away, succumbing to the inevitable lecture.
He might be terrifyingly instinctual to battle tactics and villain confrontations, but advanced emergency treatments and protocols weren’t his forte. The recent failure of his mid-assessment exam during his hero licensure remedials were proof of that.
He wasn’t really cut out for rescue missions.
“I guess, this isn’t really helpful.” She mused as a finger poked on the rubber mannequin “It doesn’t really compare to the real thing, right?”
“I’ve done stitches before.” He refused to elaborate on the details when her brows creased - in trepidation, or worry? It didn’t matter. What mattered was that they both agree with the results: his sutures were unsatisfactory, despite how concise his technique was.
Shouto needed to know what he lacked.
“Judging from your approach, Todoroki-san. I guess your bedside manners are lacking.”
“I’m not an EMT.”
“Yet, as a hero, you’re always going to be a first responder. Empathy is always the key, Todoroki-san. And your stitches! First of all,” She gestures to the uneven spaces between his threads. “They should be as small as possible, to prevent colloidal formations."
“I can use ice for improvised anesthetic. They won’t feel a thing.”
“And if time is of the essence, or possible hypovolemia, you’ll opt for cauterization.” She moves the mannequin out of the examination bed. “But we can’t just knock out severely wounded civilians especially during a crisis, or wait for paramedics. That’ll effectively unfetter you from having to deal with their acute stress reaction, but hardly helpful for their later recovery from the mental trauma of the entire experience. Frankly put, you have completely failed to establish rapport with the victim during this exercise.”
A clinical gaze swept over their makeshift infirmary in the dorms, her dark eyes flitting over the remaining aseptic materials on the table.
Shoto didn’t like the expression on her face.
It reminded him of Midoriya before he braced himself to break his bones.
"Yaoyorozu?"
"You need experience." Her words are firm, even if her hands were trembling. "But we can't create realistic life-threatening simulations."
Unless we wait for the next villain attack or any devastating catastrophe, which will be a bit unnerving. Or too late.
To his bewilderment, she piled her unruly ponytail into a tight bun at the crown of her head. Next, she went to the sink and started to soap her elbows with a strong smelling solution.
"Yao-"
"Honestly, I think it'll be more practical to use pork meat. Or even purchase a cadaver." Momo wrinkled her nose in distaste, as she now scrubbed her arms with a brush. "But in your case, a live subject would be better."
"No."
"Relax, Todoroki-san. Some field medical trainees do this. Especially when they have to take their licensure exams. It's not new. And you have my consent."
If this was true, he hasn't heard of it.
"We can also test if how effective your ice quirk will be on wounds. It'll be beneficial if we can also train you to sterilize equipment. Think of the possibilities. Midoriya-san might even chip in if I raise this subject-"
"No. Don't." He cut her off, took a shuddering breath, and reiterated, "There's no need."
It was absolutely eerie how calm Yaoyorozu was, as she contemplated where to make a clean laceration on her arm. He knows that he should decline.
That was the right thing to do.
"Yaoyorozu, you don't have to do this."
To his surprise, she smiled as she twirled a scalpel in between the gaps of her gloved fingers like she did with her pen at times when bored. "See? Todoroki-san, that's a start. But this won't even hurt."
A thin line bloomed red on her forearm. Her eyes fluttered, her breath quickened, but she didn't cry in pain. The scalpel dragged a bit deeper, till she deemed it satisfactory.
Before she even discarded her blade, cold air soothed the sting.
"Three inches. About ten stitches should cover it."
He knew that she noticed the way his trembling right hand, the constant way his gaze darted to her face, to her bleeding wound and her suppressed flinches. Her self-inflicted cut was a pale comparison to the several gashes that Iida had on his own arm a few months ago, but it was enough to bring back that same throb of fear in his chest, making sure that he’ll be more careful this time around.
"Yaoyorozu." He hoped that her name was enough to convey his admonishment, as his left hand was already gloved and holding the forceps.
"According to your performances during practicals, you do better under pressure." Her lips curled in pride as the curved needle sank to her flesh for the first stitch. "Don't worry, I don’t feel-"
"Your fingers are twitching.”
"It only stings a little, Todoroki-san. I’ve felt worse."
But when he pulled the string, her breathing became shallow and he stopped.
“What’s wrong, Todoroki-san?”
“Yaoyorozu.” He smoothed his face into concern. “Are you okay?.”
“Yes, I’m fine.” She even looked apologetic. “Is the skin too taut? I’ll try relaxing my arm then.”
By the fifth stitch, he was ready to stop this exercise, for her eyes brimmed with tears. Yet the grim line of her mouth and the way she didn’t even flinch from meeting his stare made him hesitate to voice his protests.
Somehow, it hit him how much Yaoyorozu trusted him.
It’s different to know that from the very start that he can trust Yaoyorozu. And how much he trusted Yaoyorozu - An intelligent, powerful young woman who knows that she can carve her own path. She could have settled for being an heiress and living in luxury, yet she knew that with her quirk, she could make a difference - be a hero.
He respected Yaoyorozu. She’was the first one he ever saw as an equal when his world started to expand from the walled confines built by his father. She could have even been his first friend if she hadn’t been hindered by her own insecurities and awkwardness. If he hadn’t been too preoccupied with how much she had reminded him of his own flaws as well.
And yet, even if she was oblivious to his personal distress, she still trusted him.
The warmth that filled his chest, unlike the usual flames he wielded, was foreign.
But not unwelcome.
“I’m having trouble with situational triage identification problems in the exams; can you identify which one to prioritize?”
“Of course, Todoroki-san.” She lit up, her thumb twitching slightly when he started the eighth stitch. “Can you explain what the question was about?”
The topic was successful enough to distract her from the careful way he pulled the sutures on her wound that she didn’t even notice that he was already dabbing the topical antibiotic on her wound.
“-just place them in one safe place and mark the wall with a red shirt to tag them. The yellow ones should be-” Her explanation stutters when she finally noticed that he had already wrapped her arm with a gauze. “Todoroki-san?”
His fingers threaded through her still shaking fingers. Her mouth was open, cheeks flushed with surprise, heat spreading across the bridge of her nose to her ears. It was a familiar, comforting sight.
“Does that cover empathy?”
“Ye-Yes.”
“Good.”
And he drops a soft kiss on her wound.
“Todoroki-san!”
“What?” To his confusion, it made Yaoyorozu more flustered, and it wasn’t in his best interest for her to suffer hyperventilation. “My mother used to do this to my wounds.”
“Not to strangers, Todoroki-san.”
“Duly noted.” He nods in understanding. “Should this only be limited to acquaintances, then?”
“Only to those you’re comfortable with, Todoroki-san.”
87 notes
·
View notes
Text
Wednesday to Wednesday
A Week Update
Okay, so, I thought that I’d make one big life update post since a lot happened this week and I thought it would be better to make one big post.
So last Wednesday (Feb. 21) I had my second psychiatrist appointment. He asked to see my kindergarten to grade six report cards, so I did that. I had at least one term’s report card from each year. On some of the envelopes my parents had written comments as well (they were supposed to about how they thought school was going) and he said that those comments were really helpful. Those combined with the comments from my teachers indicated to him that I had been displaying symptoms of ADHD since childhood, which matched my self assessment. This combined with what we had talked about before made him comfortable to make the diagnosis of ADHD.
In terms of my treatment, he wants to treat the depression first, so he prescribed me an antidepressant. He prescribed me 20mg of fluoxetine which is prozac. I have been taking it, and he might raise the dose next month when I see him. Next month he also wants to start me on ADHD meds.
That day in the afternoon I also had a hematologist appointment. The doctor was really nice. She took a history, looked at some of my old blood work, did a quick physical exam, and got me to do some more blood work which I was able to do on the same day. I have another appointment with her this coming week (March 7), so I guess I learn more then. I don’t really know anything else other than I have very little iron, and the rest of my blood seems pretty good.
Thursday and Friday I had two really good clinical days which I have already posted about. After clinical I studied patho. I volunteered doing first aid at an event on Saturday. We put one band aid on a dude lol. It was a good chill day. Afterwards I studied patho as well. Allllll day sunday I studied patho for my midterm which was on Monday. I think it went okay, but it was generally pretty meh.
THIS Wednesday (yesterday) I had an appointment with my councillor at school. We talked about a bunch of things. I had told my parents about everything that had been going on and the meds and everything so that’s cool. I have another appointment booked with him after my next psychiatrist appointment, which is on March 21.
Yesterday I found out my mark on my terrible midterm which I talk about in this post. I got 73.7% which I’m really happy about. Now I just need my paper mark back...
Tonight I need to pack for the weekend, because I’m going camping this weekend! I’m pretty excited. Erik and Alex are going to be there too.
#semester 4#personal#mine#alex#camping#mental illness#mental health care#psychiatrist#physical health#hematology#life update#actually adhd#medication#medicated and mighty#clinical placement#patho#pathophysiology#midterms#midterm exams#erik#nurse#nursing#nurblr#nursing student#student nurse#nursing school#nursing studyblr#studyblr#medblr
1 note
·
View note
Note
I'm in my last year of undergrad and I feel like everything has gone to shit. The past year and a half have been awful, i have depression, anxiety and im almost positive i have ADHD too. I feel like such a piece of shit because I keep asking for the extensions on projects and exams, and I'm afraid I'm gonna be this way forever. Sorry this is a lot but do you have any advice on how to take the first step in digging myself out of this hole ive created?
Okay, so it seems like you came in via this post. That’s pretty much my philosophy here. I don’t know if you’re gonna “be this way forever” or not--I know I will probably be the way I am (depressed, anxious, with ADHD) forever, but that isn’t necessarily the same as being a trash disaster on academic probation forever.
I’ll be honest, I kind of feel like after a year and a half, you’re kind of an expert on what you can do with two hands and a shovel. You’ve been digging yourself out as fast as you can, and it’s been a real struggle. I think it’s time for you to get actual help, as in, other people. Reaching out to me was a good first step. I can help you decide where to go from here.
Keep it simple and take it slow. If you don’t know where to find any of this stuff, feel free to private message me your school’s website; I have a minor knack for reading organizational structures.
For the next week, pick ONE OR TWO of the following options. Even if they’re all good ideas, keep your goals manageable. And then, of those one or two, pick one or two SMALL ACTIONS you can do to pursue them, like looking up a number in your student handbook or making an appointment. If you do more, that’s great, but the siren song of our people is, “I’m gonna accomplish so much!”
Without further ado: Some Options For Help
Your school’s Disability Services/Accessibility Office/Office of Inclusion/whatever they call it
You’re looking for the office that helps Deaf/Blind/mobility-impaired students succeed in school. Mental health falls under the same category. It’s their job to make sure your school is providing you with as much chance at an education as it would provide to someone who’s totally neurotypical. Tell them what you told me.
Stuff they can do:
Tell you what your school’s requirement is for documenting a disability
Give you information on local assessment and treatment options--what psych professionals locally are good? Is there a fund somewhere that will cover your testing? Does the student health centre have a psychiatrist?
Provide you with a letter that tells your instructors that giving extensions, having flexible schedules, or dropping penalties for non-attendance is a legal requirement to accommodate you. This is not necessarily a free pass--a professor may decide that some things are mandatory or non-negotiable--but it is an easy way to bring these problems up early, before they become an issue.
Help find your or fund you a tutor (more on this later)
Help you find other resources and services on your campus
Your school’s Counselling Centre/Wellness Services/Social Work Office/wherever they hide the shrinks
This is the place where they offer free counselling. If there’s walk-in, go to walk-in; if they can book an appointment in a week, go in a week; if there’s a three-month waitlist, get your name on the waitlist.
Funny story--I had graduated undergrad before I realized that students got free counselling on-campus. I’d been in therapy since I was 16, but five years of undergrad? Yeah, no clue. I was looking for therapists on Psychology Today and shelling out hundreds of dollars out of pocket, and there were hot and cold running therapists under my very nose.
In fact, there might be more than just therapists. The school I worked at had regular counsellors, and also a Learning Specialist, whose job included teaching people with executive function disorders like depression and ADHD how to study effectively! It’s worth asking about.
When you see one of these people, it’s very tempting to think they are An Adult Who Is The Boss Of You. They will look at you, understand you with their expert knowledge, tell you what your deal is, and give you instructions on what to do now!
In reality, therapists are not Sherlock Holmes, or profilers on TV. We can’t just look at you and go, “I see by the way you button your coat that you’re a middle child and ambiguity makes you uncomfortable.” We rely a lot on “client report”--on what you say is true. Psychological assessment is a process involving interaction, not a detached observation of stable qualities. If a therapist says something about you that seems inaccurate, it is beneficial and good to say, “No, actually, I think you’re mistaken. To me, it looks more like...”
You’re recruiting an experienced co-traveller to go on a trip with you. They know a lot about rocks and trails and climbing harness, but they don’t know the territory you’ll be travelling together. So first and foremost, you want to find someone you want to go on a trip with: a therapist who is a good fit for you.
If you don’t like your assigned therapist, ask for a new one. We have an ethical responsibility to provide referrals when we can’t provide someone with the treatment they need, and since a good client-therapist relationship predicts therapy outcome like 70% of the time, simply not liking or trusting your therapist is a good enough reason to try somebody new. If you want you can just email them after the session and say, “I don’t think you and I quite clicked. With what you know now of my personality and issues, is there someone else in your office you can refer me to?”
Medication. Different medication.
Not gonna lie, going on antidepressants was like... getting the inside of my brain whitewashed. There was so much space. So much room. I could think and feel without being constantly smothered in negativity! And going on ADHD meds on top of that was like.. the thoughts that had always been slippery, unable to grasp or manipulate, suddenly became solid in my hands. I could grip them, slow them down, tell them to go somewhere else.
Both times, it took five to ten adjustments to get to the right cocktail and dosage. For example, I was on an antidepressant that stopped me from crying and freaking out all the time but killed my creative drive, so we added a drug that gave me more energy so I could write again. Then money got tight, we tried me on a generic, found that didn’t work, and found a way to pay for the first version. Each time, it meant seeing the doctor, trying a dose for two weeks or a month, and then going back to report progress and try adjusting it again.
Again: It’s a process, an interaction. It’s something you get a say in. And if you’re currently on meds--well, let me just say: If you sent me an ask like that, your meds aren’t doing their job. They’re not the right ones for you. So it’s time for an adjustment.
If you can get to or afford a psychiatrist, great! A general practitioner who’s known you for a while will often do. And if you need to, well, I’ve gotten my meds adjusted by a different doctor every time at a walk-in family practice clinic. You do what you can. Information on who and what is available is often why Disability Services is a great resource--who knows, maybe there’s a psychiatrist on campus you can see for free who sees the depression/anxiety/ADHD trifecta all the time!
(General life tip: When they give you an assessment for depression, anxiety, or ADHD, don’t downplay your symptoms. Answer the way you would on a bad day or when you’re struggling. Of course you know how to cope with these challenges, but the unfair part is that you have to cope with them at all)
A tutor or academic coach
This never occurred to me for a long long time, because I was always a “smart kid”, and I always thought tutors were for people who didn’t intellectually grasp the material. Meanwhile: Surprise! I have a developmental disability that significantly impacts my learning! My grad school put me on academic probation and effectively foisted a person of this job description on me, and it was the BEST THING EVER.
If you’ve ever felt like you would work so much better if only you had someone sitting there all the time making you work? Or a sympathetic friend who could help you break it down and be less overwhelming? If the only time you get your work done is when someone else asks you about it? This is the person for you.
Most schools provide these services to students for free, or subsidize disabled students’ tutoring. If all else fails, you can find a tutor on your own and say, “I get this stuff intellectually, but I really need someone who makes me spend time with it, because left to myself I’d get anxious and ignore it all until the night before the deadline.”
If you have good friends who can do this for you, that’s great too--but the biggest objection to the post that brought you here is, “I’m depressed and socially anxious--I don’t HAVE anybody to help!” So this post is aimed at linking you up to people whose explicit job it is to help you--people you, your insurance, or your tuition dollars directly pay for.
47 notes
·
View notes
Text
Leveraging Time by Doing Less in Each Chronic Care Visit

By HANS DUVEFELT, MD
So many primary care patients have several multifaceted problems these days, and the more or less unspoken expectation is that we must touch on everything in every visit. I often do the opposite.
It’s not that I don’t pack a lot into each visit. I do, but I tend to go deep on one topic, instead of just a few minutes or maybe even moments each on weight, blood sugar, blood pressure, lipids, symptoms and health maintenance.
When patients are doing well, that broad overview is perhaps all that needs to be done, but when the overview reveals several problem areas, I don’t try to cover them all. I “chunk it down”, and I work with my patient to set priorities.
What non-clinicians don’t seem to think of is that primary health care is a relationship based care delivery that takes place over a continuum that may span many years, or if we are fortunate enough, decades.
Whether you are treating patients, coaching athletes, raising children or housebreaking puppies, the most effective way to bring about change is just about always incremental. We need to keep that in mind in our daily clinic work. Small steps, small successes create positive feedback loops, cement relationships and pave the way for bigger subsequent accomplishments.
Sometimes I avoid the biggest “problem” and work with patients to identify and improve a smaller, more manageable one just to create some positive momentum. That may seem like an inefficient use of time, but it can be a way of creating leverage for greater change in the next visit.
I actually think the healthcare culture has become counterintuitive and counterproductive in many ways; it helps me when I focus intensely on the patient in front of me, forgetting my list of “shoulds” (target values, health maintenance reminders and all of that) and first laying the foundation for greater accomplishments with less effort in the long run.
Six months ago I wrote this about how I try to start each patient visit. And in my Christmas reflection seven years ago I wrote about the moment when a physician prepares to enter an exam room:
I have three fellow human beings to interact with and offer some sort of healing to in three very brief visits. Three times I pause at the doorway before entering my exam room, the space temporarily occupied by someone who has come for my assessment or advice. Three times I summarize to myself what I know before clearing my mind and opening myself up to what I may not know or understand with my intellect alone. Three times I quietly invoke the source of my calling.
It’s all about the patient, the flesh and blood one in front if you in that very moment and what he or she needs most from us today. In physics I learned that you get better leverage when your force is applied a greater distance from the fulcrum. In human relationships and in medicine it is the opposite; the closer you are, the greater leverage you achieve.
Hans Duvefelt is a Swedish-born rural Family Physician in Maine. This post originally appeared on his blog, A Country Doctor Writes, here.
Leveraging Time by Doing Less in Each Chronic Care Visit published first on https://wittooth.tumblr.com/
0 notes
Text
Leveraging Time by Doing Less in Each Chronic Care Visit

By HANS DUVEFELT, MD
So many primary care patients have several multifaceted problems these days, and the more or less unspoken expectation is that we must touch on everything in every visit. I often do the opposite.
It’s not that I don’t pack a lot into each visit. I do, but I tend to go deep on one topic, instead of just a few minutes or maybe even moments each on weight, blood sugar, blood pressure, lipids, symptoms and health maintenance.
When patients are doing well, that broad overview is perhaps all that needs to be done, but when the overview reveals several problem areas, I don’t try to cover them all. I “chunk it down”, and I work with my patient to set priorities.
What non-clinicians don’t seem to think of is that primary health care is a relationship based care delivery that takes place over a continuum that may span many years, or if we are fortunate enough, decades.
Whether you are treating patients, coaching athletes, raising children or housebreaking puppies, the most effective way to bring about change is just about always incremental. We need to keep that in mind in our daily clinic work. Small steps, small successes create positive feedback loops, cement relationships and pave the way for bigger subsequent accomplishments.
Sometimes I avoid the biggest “problem” and work with patients to identify and improve a smaller, more manageable one just to create some positive momentum. That may seem like an inefficient use of time, but it can be a way of creating leverage for greater change in the next visit.
I actually think the healthcare culture has become counterintuitive and counterproductive in many ways; it helps me when I focus intensely on the patient in front of me, forgetting my list of “shoulds” (target values, health maintenance reminders and all of that) and first laying the foundation for greater accomplishments with less effort in the long run.
Six months ago I wrote this about how I try to start each patient visit. And in my Christmas reflection seven years ago I wrote about the moment when a physician prepares to enter an exam room:
I have three fellow human beings to interact with and offer some sort of healing to in three very brief visits. Three times I pause at the doorway before entering my exam room, the space temporarily occupied by someone who has come for my assessment or advice. Three times I summarize to myself what I know before clearing my mind and opening myself up to what I may not know or understand with my intellect alone. Three times I quietly invoke the source of my calling.
It’s all about the patient, the flesh and blood one in front if you in that very moment and what he or she needs most from us today. In physics I learned that you get better leverage when your force is applied a greater distance from the fulcrum. In human relationships and in medicine it is the opposite; the closer you are, the greater leverage you achieve.
Hans Duvefelt is a Swedish-born rural Family Physician in Maine. This post originally appeared on his blog, A Country Doctor Writes, here.
Leveraging Time by Doing Less in Each Chronic Care Visit published first on https://venabeahan.tumblr.com
0 notes
Text
My PHP journey. By guest blogger, Ola Abdelhadi
“I am quitting paediatrics.” I said to myself. I could no longer cope with my ongoing health struggles on top of a busy neonatal rota and keep up with my paediatric training requirements. I had just finished ST1 and now spending my first day of induction in ST2 in a new hospital. I had spent the weekend in bed crippled with abdominal pain and I was struggling to listen to induction due to a mixture of physical symptoms and uncertainty about my future.
I have struggled with physical symptoms for the past 3 years Abdominal pain, diarrhoea, bloating and vomiting became my new ‘normal’ and I was finally diagnosed after numerous investigations with a malabsorption requiring enzyme replacement every time I ate. I used to get abdominal pain nearly on a daily basis with a visit to the Emergency department every 2 months when my symptoms were at their worst. I was even wheeled down in a wheel chair to A&E on a busy night shift after having a severe exacerbation of my symptoms. My symptoms were unpredictable and sometimes I would avoid eating on a long shift so that I would not have to deal with the pain. This fuelled my anxiety around eating and around my condition.
I have always been a perfectionist and describe myself as having type 1 personality (as most paediatricians probably do). I have always felt stressed however; I feel that I perform better under pressure. However, I was beginning to crack. The stress of a busy paediatric rota, dealing and managing sick babies and children as well as coming to terms with the lifelong nature of my health condition as well as the physical aspects was becoming overwhelming and I could feel myself drowning.
I was worried about what my colleagues would think of me. I worried about the number of sick days I had taken off and if that would affect my training or the way people thought of my dependability. I was worried about the babies on the postnatal ward, had I missed something on the baby check. I worried every morning if I would have severe abdominal pain that day. I was worried that my physical symptoms were affecting my mental well being. I was worried what my medical family would think if I decided to quit.
I managed to attend the first day of induction but by lunch time I was dreading the thought of a another training year. I had used all my physical and mental strength to finish ST1 in one piece. One of the speakers at induction was Dr Simon Broughton, the one of many doctors that I will forever be grateful to for helping me. He mentioned that he was the Paediatric TPD and that if we had any concerns we could go to our educational supervisors or speak directly to him. I decided it was time to say something and at lunch I approached him. He kindly took me to his office where I told him about my past year and my health struggles. He was extremely empathetic advised I take some time to recover from my physical symptoms and arranged a support meeting with the London Deanery and advised I refer myself to PHP.
I met with Dr Camila Kingdon, the Head of the School of Paediatrics, and another doctor at the support meeting not long after. They supported me to take some time out of my training to get better and supported my decision to get help from PHP. PHP stands for the Physician Health Programme/GP health service which is a confidential self-referral NHS service for doctors and dentists struggling with their mental wellbeing. Doctors or Dentists living in London or training in London can self-refer themselves and those outside of London can be referred by their GP.

Referring myself to PHP was the best decision that I have made in my life so far (second to marrying my husband). It was an easy process to refer myself with an online form followed by a telephone consultation for a further assessment. I met Dr Eleanor Cole, a Consultant Psychiatrist, a few weeks later and my journey to recover began. I had an initial consultation and she thought that I might benefit with CBT for my anxiety. I commenced CBT with Simon Lyne and had 6 sessions of CBT in total with some follow ups with Dr Cole to check my progress. I went back to work the next rotation and continued my CBT and follow ups with PHP. I also had regular emails with Dr Kingdon checking on my progress and another support meeting when I returned to work.

CBT has helped me process the challenges that my life has thrown at me and to change the way I worry about things. I was also given tasks to do in between CBT sessions and was advised to some mindfulness on the ‘Calm’ app to help as well. I was able to go back to training in a much better mind frame, complete my membership exams and successfully apply for an academic clinical genetics post. I am forever indebted to all the people that have encouraged me to get help and take time off. I would like to thank Dr Broughton, Dr Kingdon, Dr Cole and Simon Lyne for the time that they have given me to help me as well as my husband, my family and friends and the Paediatric teams at King’s College and St George’s Hospital who supported my return to work. My one regret during this whole process was not going to PHP prior to my final burn out and I hope this long account of my story will help another trainee seek advice or help sooner. You have to be well to your treat patients, so treat yourself first.
https://php.nhs.uk/
0 notes
Note
So I've heard you talk about working in a hospital a lot -- as a fellow Blindspot-slash-biomedical-science enthusiast, would you mind talking a little about the kind of work you do? Sorry if I'm bothering you, have a lovely day!
Hi there! No, you’re not bothering me at all, I’m always happy to answer questions– though I’ll admit I don’t usually get ones about myself, so this is kinda different haha.
So anyhow, you probably already know from some of my posts that I work as a doctor (I used to not really advertise that, but lately it’s come up a couple of times in my recaps because apparently I simply can’t refrain from commenting on terrible ‘TV medicine’ despite myself lol). So basically I’ve been working as a doctor in a large regional hospital for a couple of years now, rotating through all different specialties before I settle down and pick one. Overall I’ve done terms in surgery, general medicine, anaesthetics, psychiatry, orthopaedics, ICU, emergency medicine, obstetrics & gynaecology, general practice, and even forensic medicine. Forensics (both the clinical and pathology aspects) is definitely a special interest of mine– for example, I’m trained as a sexual assault examiner– but it will be unlikely to be the main focus of my career. For the rest of this year I will mostly be in the emergency department (we call it ‘ED’ here rather than ‘ER’), and while I do love ED, I’ve pretty much decided 100% to do GP (which I also love). I’ll sit the GP exam in a couple of months and will hopefully start the training program for it next year.
So to give you a basic idea: on most of the above rotations, my day would generally consist of ward rounds in the morning, then spending the rest of the day chasing up tests and reviewing unwell patients and sending people home and basically signing a lot of stuff; unless of course I was in the ED, in which case it’s just ten hours of assessing and managing patients with anything from a stubbed toe to a heart attack. And that’s honestly about it, really; I don’t really know what else to say about my job that will be of interest to you. I do get a lot of people asking if it’s like Grey’s Anatomy, which used to make me snort and say ‘no’… but after being in the hospital for a while and seeing just how many people are hooking up, and all the ~personal drama~ that happens, I have to say there are some things it really does get right. Not the medicine part, though. Not even close haha. (And actually, one of the first things we learned at medical school was that Scrubs is the closest medical show to reality. Scrubs. Bet you didn’t see that coming).
But seriously though, I do really love my job, and while it can actually often be waaaay more unexciting than you might expect (so much paperwork oh my god) I have also had some pretty insane highs and lows; have had my heart break and soar by turns. I’ve also worked with many amazing people, whether those are nurses or doctors or patients (mostly nurses tho bc lbr nurses are THE BEST), and had many amazing experiences. So basically I am just so, so thankful for all the factors that worked together to get my past-self through medical school– because while there were definitely times when I desperately wanted to say ‘fuck it’ and quit, being out on the other side has shown me that I am now exactly where I have always wanted to be.
But anyhow, Anon, as ever I have seemed to ramble my way into a ridiculously long answer lol, though I hope that it has been at least moderately interesting for you. And if you have any further questions, I’m happy to answer them as well (just know that this copious word-vomit is what you’re getting yourself in for haha)
10 notes
·
View notes
Text
Therapy Update: Implanted Neurostimulators for Sleep Apnea
Therapy Update: Implanted Neurostimulators for Sleep Apnea Read more on: www.ellymackay.com
Inspire Medical, Respicardia, LivaNova, and Nyxoah share the latest data on their devices.
By Sree Roy
FDA APPROVED
Inspire Medical Systems Inc Inspire Upper Airway Stimulation
Information source: Howard Green, vice president of marketing
FDA status: FDA approved in April 2014.
Size: 15 cc
Implant location: Inserted just under the skin of the neck and chest through 3 incisions.
Lead location: The sensing lead is placed in the intercostal muscle area; the stimulation lead is wrapped around the hypoglossal nerve (which controls the muscles and movements of the tongue).
How it works: As a patient sleeps, Inspire senses when they breathe in and delivers mild stimulation nudging the tongue forward, opening the airway. The patient uses a sleep remote to turn Inspire on when they go to sleep and off when they wake up.
Treats: Moderate-to-severe obstructive sleep apnea. AHI between 15 and 65.
Titration: Inspire is turned on about a month after it’s implanted. The patient is given a sleep remote and initial settings are established. The patient uses Inspire at home for 2-3 months and adjusts the amplitude using the remote to find a level that gives them comfortable, restful sleep. After this, the patient has an overnight sleep study where stimulation levels can be adjusted to optimize patient outcomes.
Future titrations: The vast majority of patients find stable settings after one lab titration. Inspire is customizable so any adjustments can be made simply in the physician’s office.
Overall efficacy: A recent peer-reviewed publication on the ADHERE Registry concluded that: median patient AHI was reduced from 34.0 to 7.0 events/hour; quality of life: ESS was reduced from 12 to 7; after 12 months, patients used Inspire 5.7 hours per night; 94% of physicians rated improvement in patients after Inspire implant. Patient-reported response to therapy experience: 94% stating they would undergo Inspire implant again; 96% of patients reported they would recommend Inspire to family and friends; 94% of patients reported they were overall satisfied with Inspire therapy.
Efficacy by demographic: Men and women within the FDA-approved AHI range (15-65) benefit equally from Inspire therapy. The ADHERE registry concluded: Inspire is an effective option for OSA patients age 65 or older, with significant outcomes and fewer complications than traditional sleep surgery.
Compliance monitoring: The Inspire system collects adherence data which can be viewed on Inspire Cloud, similar to how CPAP compliance is monitored.
Long-term outcomes: The STAR Clinical Trial data were published in the January 9, 2014 edition of the New England Journal of Medicine. The significant improvements and reductions measured after 1 year were sustained over a 5-year follow-up period. The outcomes include: 79% reduction in AHI events; significant improvements in FOSQ score; significant reductions in daytime sleepiness as measured by the ESS; 90% of bed partners reported soft or no snoring for their partner using Inspire, as compared to only 17% of bed partners at baseline.
Third-party payer status: Inspire is covered with most Blue Cross Blue Shield franchises, Aetna, Medical Mutual, and many other payers. In total, there are positive coverage policies from commercial US insurers covering over 80 million lives.
To find physicians qualified to do the implant surgery: www.inspiresleep.com/doctor-search
Surgeon appointment(s): A patient schedules a consult with an ENT to determine candidacy for Inspire. This includes an exam of the patient’s airway anatomy. If the patient is approved for Inspire, the surgery is scheduled.
Extraction information: Similar to pacemakers, Inspire is expected to be replaced when the battery depletes (~11 years). In rare circumstances, infection or other complications require a device to be removed in a routine outpatient procedure.
Expected developments in the next 12 months: Inspire is launching the Inspire Cloud patient management system, providing sleep physicians with easy access to insights into patients’ therapy usage, outcomes, and adherence.
More information: Strollo PJ, et al. Upper-airway stimulation for obstructive sleep apnea. N Engl J Med. 2014;370:139-49. Heiser C, et al. Post-approval upper airway stimulation predictors of treatment efficacy in the Adhere Registry. European Respiratory Journal. 2019 Jan.
FDA APPROVED
Respicardia remedē System
Information source: Robin Germany, MD, chief medical officer
Size: 39 cc (similar size to implantable cardiac defibrillators)
Implant location: The pulse generator is placed under the skin in either the right or left side of the upper chest. In most cases, physicians select the right side as cardiac devices are typically placed in the left side of the upper chest.
Lead location: The stimulation lead is placed transvenously in either the left pericardiophrenic vein or right brachiocephalic vein (in close proximity to the phrenic nerve for unilateral stimulation of the diaphragm). In some cases, physicians also place a sensing lead to monitor respiration.
How it works: During sleep, the remedē System delivers low amplitude electrical stimulation pulses to the phrenic nerve, contracting the diaphragm and restoring a normal breathing pattern and volume. The device turns on automatically each night.
Treats: Moderate to severe central sleep apnea in adult patients. This is usually defined as an AHI ≥ 15 events/hr with predominantly central events. In the pivotal trial, the mean AHI was 46 events/hr and the mean central apnea index was 28 events/hr.
Titration: The system is typically activated one month after implant. During this month, the device gathers data about the patient’s sleep habits (sleeping patterns, positional data, and nighttime respiration). Then the patient returns for activation, during which the device is individually programmed using the data. The device then auto-titrates over the next 4–6 weeks. This gives the patient time to acclimate to the therapy. A sleep study may be administered after titration to assess efficacy and/or direct the physician toward additional device programming to optimize results.
Future titrations: Physicians typically perform device checks 2 to 4 times per year. Diagnostic information (such as nighttime respiration, sleeping patterns, and the number of hours of delivered therapy) along with patient feedback can be used during an office visit to adjust device settings or program the device’s auto-titration, which allows for therapy adjustments for changing patient needs over time.
Overall efficacy: The remedē System pivotal trial met its primary endpoint, percentage of subjects demonstrating a ≥50% reduction in AHI, and all 7 secondary endpoints, comprehensively demonstrating improvements in sleep metrics, sleep quality, and quality of life. The remedē System is the only CSA treatment to demonstrate significant improvements in arousals, percent of REM sleep, or quality of life in a randomized trial (Costanzo MR, et al. Lancet. 2016;388:974-82. Costanzo MR, et al. Am J Cardiol. 2018;121:1400-18). 88% of patients demonstrated decreased apnea and hypopnea events, with a mean reduction of 81% in the central apnea index from baseline; 79% of patients reported a quality of life improvement; 95% of patients reported they would “elect to have the medical procedure again”; 91% freedom from serious adverse events; and 97% implant success rate.
Efficacy by demographic: Various subgroups were analyzed following the pivotal trial demonstrating treatment effects were consistent across subgroups. There are less women than men with CSA, but efficacy was the same in both men and women. Similar efficacy was seen when separated by age, including those over age 65. There was no difference in efficacy in patients with an AHI in either the moderate or severe range or in patients with atrial fibrillation. In light of the limited treatment options for patients with heart failure and CSA, Costanzo et al. showed in a post hoc analysis that the heart failure subgroup responded similarly to the non-heart failure cohort with regard to safety and efficacy (Constanzo MR, et al, European Journal of Heart Failure. 2018; doi:10.1002/ejhf.131).
Compliance monitoring: The system activates automatically each night, alleviating most compliance concerns. It retains approximately 30 days of data on nighttime respiration, sleeping patterns (positional, activity, etc), and hours of delivered therapy.
Long-term outcomes: Outcomes data has been published showing 6-, 12-, and 18-month results, and we expect our 24- and 36-month data to be published in mid-2019. Observed safety and efficacy have been consistent over time. We are following patients from the remedē System pivotal trial out to 5 years.
Third-party payer status: Aetna was the first private payer to cover the remedē System in early 2018. Also in 2018, CMS granted the remedē System a Transitional Pass-through Payment. The remedē System is also included on the Federal Supply Schedule for the VA. Until broad coverage is established, the remedē System is being reviewed by payers on a case-by-case basis.
To find physicians qualified to do the implant surgery: www.respicardia.com (list of current implant sites)
Surgeon appointment(s): This can vary, but the minimum visits include a follow-up visit approximately one month after the procedure to activate and begin auto-titration of the therapy. In most cases, at least one additional appointment would be needed in the next 3 months to assess the device diagnostics and optimize programming. These follow-up visits can be done in either the sleep clinic or with the implanting cardiologist.
Extraction information: Like a cardiac pacemaker, when the battery of the device nears expiration an electrophysiologist would replace the implanted pulse generator, requiring the previously implanted device to be extracted—a common, routine procedure. Occasionally, one or more of the leads also need to be replaced. While the experience and implant duration here is limited, we have thus far seen almost all extracted leads come out safely with simple traction. A small number required extraction techniques and instrumentation similar to cardiac pacemaker leads. Patients typically go home the morning after the extraction procedure.
Expected developments in the next 12 months: The focus will be working with 30-40 new centers to build out their sleep and cardiology suite of services to include the remedē System. There will also be some exciting advances in clinical and product development. New clinical data is expected to be published including 3-year follow-up from the pivotal trial and a meta-analysis combining the pilot and pivotal patient populations. Additionally, a multi-center, prospective, post-market trial is beginning enrollment now, seeking approximately 500 subjects in both the United States and Europe to collect additional safety and effectiveness data. Finally, the next generation of the system is underway, but we have not released a projected availability date.
Additional information: The remedē system activates the diaphragm to generate negative pressure, similar to how people breathe naturally. This is in contrast to the positive pressure generated from mask-based therapies. Users are highly compliant, as the device activates automatically each night when three conditions are met: 1) it is within the patient’s designated sleeping hours, 2) the patient is in a reclined position, and 3) the patient is not moving. The patient’s body is the controller—the patient can roll over or sit up to suspend therapy; the device will reactivate once the patient is still again.
A doctor will need to evaluate the patient’s condition to determine if the remedē System is appropriate. Patients will not be able to have an MRI or diathermy (special heat therapies) if the remedē System is implanted. The remedē System may be used with another stimulation device such as a heart pacemaker or defibrillator; special testing will be needed to ensure the devices are not interacting. As with any surgically implanted device, there are risks related to the surgical procedure itself which may include, but are not limited to, pain, swelling, and infection. Once the therapy is turned on, some patients may experience discomfort from stimulation and/or from the presence of the device. The majority of these events are resolved either on their own or by adjusting the therapy settings. The remedē System may not work for everyone. There are additional risks associated with removing the system. If it is decided to remove the system, another surgery will be required. Be sure to understand all of the risks and benefits associated with the implantation of the remedē System.
The remedē System is contraindicated for use in patients with an active infection or patients known to require magnetic resonance imaging (MRI). See the Instructions for Use for complete information regarding the procedure, indications for use, contraindications, warnings, precautions, and potential adverse events.
More information: Costanzo MR, et al. Transvenous neurostimulation for central sleep apnoea: a randomised controlled trial. Lancet. 2016;388:974–82.
INVESTIGATIONAL
LivaNova Aura 6000 (LivaNova acquired ImThera in 2018)
Information source: John Webb, vice president, sleep apnea
FDA status: In clinical trials
Size: 11 cc volume; 0.8 cm thickness; 16 g weight
Implant location: ~4 cm below the clavicle
Lead location: A lead with cuff is placed proximally around the hypoglossal nerve before the nerve branches.
How it is designed to work: The Aura6000, a fully implantable device, helps treat OSA by delivering mild stimulation to the tongue during sleep, hence significantly reducing or eliminating sleep apnea events.
Hopes to treat: Obstructive sleep apnea. AHI ranges in clinical trials are 20 to 65.
Anticipated titration: Settings are optimized at a titration visit following implantation.
Anticipated future titrations: Settings can be optimized, as needed, over the course of the implantation.
No response to other questions asked due to the device being in clinical trials.
INVESTIGATIONAL
Nyxoah Genio system
Information source: Rémi Renard, vice president, therapy development and education
FDA status: Working toward FDA approval. The Genio system received EU CE Mark approval in early 2019.
Implant location: The Genio is implanted in the chin area through a minimally invasive surgery. It sits like “a saddle on a horse” on the genioglossus muscle; its stimulation electrodes face both branches of the target hypoglossal nerve.
Lead location: The Genio is leadless. The tiny neurostimulator is powered by an external source of energy. Every night, when the user goes to bed, he/she positions the activation chip under his/her chin through an adhesive disposable patch. In the morning, the patient needs to remove and discard the patch and put the activation chip on the charging unit.
How it is designed to work: By stimulating bilaterally the hypoglossal nerve in a cyclical manner, the Genio system helps maintain the upper airway open and prevent apnea and hypopnea events.
Hopes to treat: Moderate to severe OSA. AHI range between 15 and 65 events/hour.
Anticipated titration: Similar to other hypoglossal nerve stimulation systems, the Genio system is titrated during the first months after implantation. A wide range of parameters will be adjusted during polysomnography nights to deliver optimal therapeutic outcomes.
Anticipated future titrations: The stimulation parameters can be adjusted any time.
Overall efficacy: The BLAST OSA study is pending publication in a medical journal, so detailed data can currently not be shared. Patients from the BLAST OSA study show a major improvement in their sleep apnea symptoms (AHI and ODI) and their quality of life.
Expected compliance monitoring: The activation chip integrates features allowing for monitoring of nightly compliance.
Expected developments in the next 12 months: Nyxoah is focusing on gathering additional clinical evidence on the Genio system, initiating European market development activities, and continuously working on technology development to improve the therapy efficiency and patient quality of life.
Sree Roy is editor of Sleep Review.
Information in this update submitted by neurostimulator marketers. Sleep Review strives for accuracy but cannot be held responsible for claims made by marketers. Marketers were not charged to have their device update published. All neurostimulators may not be included. E-mail sroy[at]medqor.com if your device was not included in this update but should be considered for future updates.
from Sleep Review http://www.sleepreviewmag.com/2019/05/neurostimulators-sleep-apnea/
from Elly Mackay - Feed https://www.ellymackay.com/2019/05/29/therapy-update-implanted-neurostimulators-for-sleep-apnea/
0 notes
Last Seen Blogs

thepublicworld
The Public World

nesrinsk
İsimsiz

underratedcharactersimagines
Underrated Characters Imagine


duronaabm
Sem título