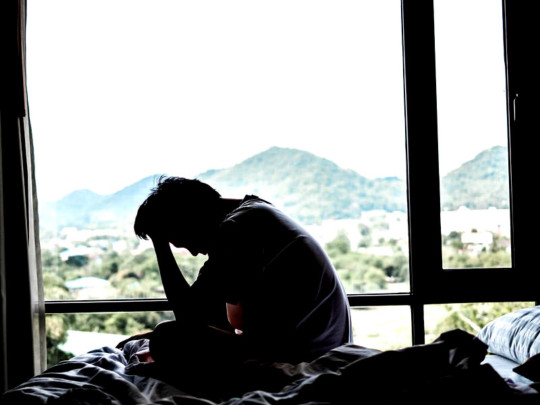
#managing chronic illness and disability while socially isolated is like that
Text
Realizing that I respond in text conversations with friends like an AI chatbot would in a customer service window is. Something.
#in my defense its because i DEAL with so many customer service robots#managing chronic illness and disability while socially isolated is like that#but i also felt like it made things simple. esp with my psychosis.#just being able to go 'okay! (follow up question that has two options for elaboration)' is easy#cant wait for the next psychotic delusion to tell me I'm actually customer service robot kin. /s
2 notes
·
View notes
Text
James Donaldson on Mental Health - Social Isolation and Loneliness
Social connection is important for our physical and mental well-being. It helps prevent feelings of isolation, which may cause things like anxiety, depression, cognitive decline and unhealthy lifestyle habits.
When we think about staying healthy, making sure you have social support may easily get lost on our list of to-do’s. But while taking care of your health includes the things you might think about — like eating a balanced diet and exercising regularly — and also it also includes taking time to be with friends and family.
Who is most affected by social isolation?
While loneliness may impact anyone at some point in their life, certain groups of people may be at greater risk of spending too much of their time solo. That means they may not get much social interaction for one reason or another. It’s important to recognize people commonly affected by loneliness so you can identify them in your own life. Then maybe consider extending an invite to your next social gathering. Here’s who may benefit:1
Older adults: Older adults and seniors have an increased risk of loneliness because they may experience more things that keep them home. That includes things like mourning the loss of a loved one, managing a chronic illness or living with hearing loss that keeps them out of conversations. Plus, they are more likely to live alone.
People new to an area: Anyone new to any area may not have strong social ties to their neighborhood or local community.
People in specific groups (such as immigrants, people who are Lesbian, Gay, Bisexual, Transgender, Queer or Questioning, Intersexed (LGBTQ+); people with disabilities): When people are in specific groups, they may feel like they don’t fit in with their peers, which could keep them home by themselves. For immigrants, it may be harder to meet new people and form friend groups, especially if there’s a language barrier.
What are the health risks of loneliness?
There are also very real physical and mental health side effects that may come with too much alone time. Here are a few:2
- Increased stress
- Hindered sleep
- Decreased sense of purpose
- Depression and anxiety
- Increased inflammation
- Poor immune system (less immunity)
- For adults 50 and older, recent studies found that social isolation was associated with a 50% increased risk of dementia, and an overall increase in depression, anxiety and suicide.3
#James Donaldson notes:Welcome to the “next chapter” of my life… being a voice and an advocate for #mentalhealthawarenessandsuicideprevention, especially pertaining to our younger generation of students and student-athletes.Getting men to speak up and reach out for help and assistance is one of my passions. Us men need to not suffer in silence or drown our sorrows in alcohol, hang out at bars and strip joints, or get involved with drug use.Having gone through a recent bout of #depression and #suicidalthoughts myself, I realize now, that I can make a huge difference in the lives of so many by sharing my story, and by sharing various resources I come across as I work in this space. #http://bit.ly/JamesMentalHealthArticleFind out more about the work I do on my 501c3 non-profit foundationwebsite www.yourgiftoflife.org Order your copy of James Donaldson's latest book,#CelebratingYourGiftofLife: From The Verge of Suicide to a Life of Purpose and Joy
Link for 40 Habits Signupbit.ly/40HabitsofMentalHealth
www.celebratingyourgiftoflife.com
What are tips to help with loneliness?
Make and nurture social connections
Consider an animal companion
Find time for mindfulness
Practice self-care
Where can I find more resources on social isolation and loneliness?
This educational resource has more information on social isolation and loneliness and tips for staying connected. If you are feeling isolated or lonely a lot of the time, you may want to visit your primary care provider and share your concerns. Talking with a doctor about how you feel physically, emotionally and mentally may help them make recommendations that could be helpful to you.
Read the full article
0 notes
Text
What Are Health Conditions And How Can They Affect You?
Health conditions are physical, mental or social issues that affect an individual's ability to function. Often, they are caused by genetics, environmental or lifestyle factors and can be treated with medication or other methods of treatment.
Anxiety is a common condition that affects over 40 million Americans. Fortunately, there are treatments available to help you manage and overcome your anxiety.
Depression is another common mental health condition that can lead to severe symptoms like sleep problems, loss of appetite, low energy and more. If you're struggling with this condition, it's important to seek help as soon as possible to get your life back on track.
Infectious disease is a broad term used to describe any disease that is caused by microorganisms, including bacteria, viruses, fungi, parasites or protozoa. It may be contagious, meaning that it can be transmitted from one person to another by contact, or non-infectious, which means that it can be prevented or treated with antibiotics and other preventative measures.
Chronic health conditions are long-lasting diseases or medical disorders that need to be managed on a regular basis in order to keep a person healthy and functional. They are the leading cause of death and disability in the United States, and they drive up the cost of health care.
Disease is an encompassing term that refers to any medical condition that causes pain, dysfunction or distress. It also includes injuries, disabilities, illnesses, disorders, syndromes, infections, isolated symptoms, deviant behaviors and atypical variations in structure or function that are not necessarily contagious.
Some diseases, such as asthma, diabetes mellitus and cancer, are idiopathic. Idiopathic diseases are those with no known cause or whose cause is not well understood.
Idiopathic diseases can be cured, but many are not. Some have a genetic component, so they can be passed from one generation to the next.
A primary disease is one that has its root cause in a particular system or organ, as opposed to secondary disease, which is a disease that is a result of the root cause. For example, a cold or bacterial infection is a primary disease, while rhinitis is a secondary disease.
Body-skin health-tips
A skin condition is a problem with the texture or appearance of the surface of the skin, which can be due to a number of reasons. For example, if you have psoriasis, your skin will look red and scaly. If you have eczema, your skin will have itchy, dry patches.
The skin is an important part of the human body, affecting how you feel and look. When your skin is unhealthy, you can have more problems with your overall health.
Pregnancy is a time of tremendous change for women and their babies. There are many health risks for pregnant women, including infection and blood clots.
It's important to learn the warning signs for these health conditions, and to make sure you have a safe and healthy pregnancy and delivery. You can reduce your risk of pregnancy-related health problems by eating a balanced diet, exercising regularly and getting enough sleep. A good healthcare provider will provide you with a prenatal care plan to ensure your health and safety during your pregnancy and after.
1 note
·
View note
Text
How Physical Therapy is Essential for a Person in Mental Trauma?
Dealing with mental trauma? In this ever-changing world, we all deal with some of the other things. Stress and mental illness have become a part of our lives. But just like every problem has a solution, mental trauma has physical therapy billing services.
So a wise decision would be to opt for a physical therapist as they work to improve a person's quality of life preventing further disability. If you're still wondering if physical therapy is essential for a person's mental trauma, then here are the benefits you should know about it.
1. It instils Hope
During a pain treatment programme, patients may be assisted in a series of activities to improve overall physical performance. For instance, exercise helps the body create hormones called endorphins, which help in inhibiting pain and discomfort sensations. It improves overall mobility along with preventing problems from getting worse overtime.
2. It strengthens the Immune System
Regular exercise increases flexibility and strengthens the immune system, making a person less vulnerable to illness and discomfort in the future.
Also, inpatient psychiatric billing services are concerned with long-term management rather than short-term relief. So instead of taking pills for temporary relief, you can opt for physical therapy as it helps us avoid recurrence of injury.
3. It Inspires Us to Keep Going
Inpatient psychiatric billing services offer positive encouragement from excellent physical therapists who help in motivating a person to keep exercising and improving. And when the term encouragement is used and implied in the right way in a person's life it can really make a huge difference.
A physical therapist not only gives you exercises to help you function better, but they also provide emotional support.
4. Improves Mood
Be it chronic discomfort or an injury, the best way to enhance your range of motion is by seeking physical therapy. Besides improving functional mobility, it also allows people to reengage in activities they enjoy.
As a result, it has a favourable impact on the body's biochemistry as a whole. It improves sleeping patterns which automatically regulates mood and lessens the chances of brain damage.
5. Diminishes Negative Self-Perceptions
Not only do physical therapy patients deal physically but also suffer from the isolation which as a result increases anxiety, insomnia, post-traumatic stress disorder, etc. This is where physical therapists come in as they act both as mentors as well as external support.
By offering social opportunities and implementing different techniques they overall improve the quality of life.
Professional Treatment can Help you Develop the Right Personality
No doubt, there are many physical therapy billing services available these days, but as physical billing therapy is complex not everyone is able to provide you with the best services. Moreover, physical therapy help depends on different individuals' cases and their severity.
So if you want to become more compliant while maximizing your reimbursement, then make sure you do some research and choose a company that has years of experience in the field and offers comprehensive services.
0 notes
Note
Hey! My character is made into an experiment by the government due to him having a supernatural ability. The one who handed him over was his partner, who has been a part of that organization all along. He is usually a very confident person, powerful and extroverted. I'm not sure how his mental state is supposed to change? I don't feel like the whole loosing their will to live and becoming incredibly depressed thing would fit him as a person. How could I still show that the torture effects him?
There isn’t a sure fire answer to how any one person will change when they’re tortured. We know the possible symptoms, but most people won’t experience every possible symptom and we don’t have a way to predict who gets what.
There’s a post that talks about the possible symptoms over here.
Here’s the thing though: there is a lot of variety in survivors, in the symptoms they get and the way they personally express those symptoms. Some people do become suicidal. Some people do become depressed. And some people do lose their faith in humanity.
But there is not one universal survivor experience.
This means that there’s a big range in realistic responses. It also means that as a writer you actually have a lot of options. You should be picking 3-5 symptoms from the list of possible options, but the list has 14 things on it and some of those things can manifest in multiple ways.
I think that, since we can’t predict symptoms, the best thing you can do as a writer is pick symptoms based on what you feel fits your character and story best.
Depression and suicidal thoughts don’t do that, so let’s have a look at some of the others.
Memory problems are incredibly common in real survivors and are almost never portrayed accurately in fiction. You can read about the four basic types here.
I’d really encourage you to use one of these if you feel it fits your story. They create a lot of interesting narrative challenges for the character and they can make for really good emotional/introspective moments. If for instance you want to explore self-doubt giving the character memories he later finds out are inaccurate could feed into that, leading to him questioning whether he ‘really’ was betrayed.
General forgetfulness (ie low level difficulty forming memories) can give the character a lasting disadvantage in everyday life, creating a much more traditional injury-recovery arc as he tries to find adaptions to this new normal.
Intrusive memories, when handled well, can help create a deeper connection between the reader and the character. Because it lets you create situations where the character’s mood flips in an instant, the other characters don’t understand why but the readers do.
Memory loss can be trickier, mostly because it’s rarely handled well in fiction. It doesn’t effect older memories, such as childhood memories, the person’s name etc. It almost never effects memories of torture itself. But it does effect other aspects of the time they’re held, the period prior to capture and sometimes a few weeks after release. It’s a distressing and disorientating experience and it’s a good pick if there’s any sort of investigation or prosecution.
Because memory problems (especially memory loss and inaccurate memories) are a big part of why torture trials are really hard to conduct. Having the character find that he doesn’t actually remember the crucial details and watching the process of people trying and failing to help him, that can be a really powerful addition. It’s also a good way to form a rift between him and his friends without depression or having him lose faith in others. It gives a reason for any distance between them, even if it’s an emotional rather then logical reason.
Read through the masterpost and really think about whether any of these memory problems could fit your story.
Narratively speaking memory problems don’t link the character’s personality but they do have a strong impact on plots and sub-plots. Memory loss, inaccurate memories and intrusive memories will all effect the character’s emotional arc and sense of self. They can also throw up barriers for the character.
He might be missing a couple of crucial details about his life before he was snatched. He might have some key details about how and where he was snatched wrong. Think about how those sorts of problems could feed into your plot, because they can add interesting conflicts and challenges.
Chronic pain is also incredibly common in torture survivors and it often doesn’t have a single cause. Back, muscular and joint pain are particularly common.
It can lead to a character seeming angry, unapproachable, anti-social or like they have a hair-trigger temper. It can also make it seem as though they have really bad mood swings or a short temper.
This can lead to interesting character moments as non-survivors struggle to empathise with an ‘asshole’ while the survivor is struggling to express the fact they’re in physical pain. It can also lead in to discussions of disability and the way we treat invisible disabilities in society.
It can also often be improved by, again, life style adjustments and sometime medication.
If you wanted to use addiction as a symptom then chronic pain is a common reason behind addiction in survivors. Essentially they start taking more and more powerful pain medications in order to try and feel ‘normal’.
Chronic pain doesn’t always lead to addiction though. Making good, consistent life style adjustments (using a mobility aid, being able to sit instead of having to stand for long periods and so on) can help keep pain at manageable levels allowing a healthy relationship with pain medication.
Insomnia is another really common symptom in survivors. This basically means the character is always at least slightly sleep deprived. Which has knock on effects on absolutely every part of a person’s life.
You can read about the effects of sleep deprivation here.
I’d suggest thinking carefully about what you need the character to do before using this one. It might sound counter intuitive but a character with disabling chronic pain is probably more capable of the occasional bout of superheroics then a chronically sleep deprived character is.
Insomnia caused by mental illness is also notoriously difficult to treat. Medication for the mental health problems survivors tend to have makes it harder to sleep and reduces the quality of sleep. Medication to ‘make’ people sleep often decreases the quality of sleep, when it works. It does not work for everyone.
Essentially don’t treat insomnia as an ‘easy’ option with less impact on the character. It impacts every part of a person’s life, making them more likely to get sick, slower to react, more emotionally volatile and less able to learn/remember everything.
There are so many things that insomnia effects that- well I find it easiest to think of it as a permanent lowering of ability across all categories. This does not mean that a character automatically becomes incapable of things; it means they are worse at them then they were before.
If they were already really good at something then other people might not notice the difference. But the character himself will. Which can have a knock on effect on self esteem.
Any of the things I’ve mentioned can result in social isolation. Because survivors can come across as aggressive, volatile and inconsiderate which can lead to people… avoiding them. Especially when other characters don’t have a good understanding of mental illness or experience dealing with trauma survivors. (Having said that, remember that a pretty significant proportion of the population experiences mental health problems at some point in their life. Think about how likely experience vs ignorance is, rather then assuming one or the other.)
Isolation exacerbates pre-existing mental health problems.
And any combination of the above symptoms make up the frame work of any long term personality change. For instance you describe this character as confident and capable: if he gets multiple forms of memory problems does that impact his confidence in certain areas? And if it does how does he cope with that? It could be by expressing his self-doubt but it could also be by taking a more passive role within a group, letting others take the lead instead of stepping in.
I have an old ask over here that goes through how I pick symptoms for a character and how I vary them depending on the sort of plot I have in mind.
Wrapping up, I think that we make these symptoms individual when we consider how the symptoms interact and what that means for the character.
Depression does not have to mean someone looks overtly miserable. It can look like nausea, like struggling to eat and sleep, like being quieter in social situations. It can feel like going through life disconnected from the world, not so much the presence of misery as the absence of joy.
You’ve listed these characteristics; confidence, power, extroverted and survivors can hold on to all those things. As always the central point is nuance. Because that confidence probably won’t be completely unshaken anymore, that extroversion might not be effortless anymore, his relationship with that power could change.
The character might have developed a lot of self doubt and, though it’s a struggle, continue to make firm ‘confident’ decisions because he feels that’s important either to himself or to everyone else. It could be a way of him showing that he’s still ‘strong’, that he survived, that he can still support the other characters.
The character could still be extroverted and depending on the symptoms you pick socialising might be harder, it could take up more energy. He might be hiding the cost from his friends. Or, another common way it plays out, is that he could just come across as… a lot more inappropriate: making dark ‘jokes’ that non-survivors don’t find funny, having obvious mood swings that make others uncomfortable. You get the idea.
Torture does change people. But those changes are unpredictable and they often don’t look like we expect.
Our fiction often tries to use depression and suicidal ideation as an excuse to turn survivors into passive objects. They are not.
One of the things that stood out to me the more I looked at prominent survivors was anger. Because yes, despair is possible, common even. But so is spite and vitriol and rage. So is determination.
There is more then one way to be powerful. Confidence does not need to be unshakable to be real.
In essence: you are aiming for an understandable change in what is already there, not an excision of the characteristics you’ve already established.
As a final note you might want to take a look at the masterposts I have on medical experiments (which you can find here and also here.) It’s worth deciding whether you want to show unethical but genuine experiments, or torture. You can have a look through the tags on unethical experimentation and pseudo-scientific torture for more information.
I hope that helps. :)
Available on Wordpress.
Disclaimer
#writing advice#tw torture#tw medical abuse#writing survivors#writing recovery#tw suicide#effects of torture#torture and memory#chronic pain#insomnia#choosing symptoms#writing symptoms#unethical experimentation#pseudo scientific torture#fantasy ask
75 notes
·
View notes
Text
Q&A Master Post
The Total List As Of September 22, 2019
Question Categories:
Ableism
Accessibility
Bathrooms
Design And Engineering
Disability And Identity
Disability And Representation
Disability Policing
Friendship, Social Situations, And Etiquette
Gear
Health And Safety
How To
Insurance And Healthcare
LGBTQIA+
Mobility Aids
Parents And Parenting
Sex, Sexuality, And Relationships
Writing About Disability
Ableism
Am I Being Ableist for Wanting to Use a Wheelchair Instead of Crutches?
Are My Parent’s Religious Beliefs Ableist?
How Do I Avoid Accidentally Saying Something Ableist?
How Do I Deal With People Being Ableist?
Is it Ableist to be Glad I’ve Made Something More Accessible?
Accessibility
Do Speed Bumps Create Accessibility Issues?
How Do I Make My Home More Accessible?
How Do I Make an Aquarium Touch Tank More Accessible?
How Do I Make My Walking Event More Accessible?
How Do I Talk to My School About Improving Accessibility?
How Do I Make a Staircase More Accessible?
Bathrooms
If the Accessible Stall is the Only One Available, Should I Use It?
Is it Acceptable to Use the Accessible Restroom Due to Too Much Noise?
Is it Okay For Able‐bodied LGBTQIA+ to Use Accessible Restrooms?
Design And Engineering
How Can I Create or Improve an Assistive Device?
How Do You Think Advancements in Robotics Will Improve Wheelchairs?
Disability And Identity
Am I Being Selfish For Using Accessible Spaces Due to Occasional Pain?
Are Mental Illnesses a Disability?
How Do I Deal With the Idea of Being Chronically Ill?
How Do I Stop Feeling Like I’m not Disabled Enough?
How Do You Deal With Comparing Yourself to Other Disabled People?
Disability And Representation
Are My Disabled Characters With Magical Enhancements Problematic?
Are Newly‐Disabled Peoples’ Lives Ruined?
Can an Able‐bodied Person Cosplay a Disabled Character?
How Can Disability Representation in Media be Improved?
How Do Advancements in Mobility Aids Cause Disability Erasure?
What Traits Do You Want to See In Disabled Super Heroes?
Why Aren’t There Any Servers in Wheelchairs?
Disability Policing
Am I Being Selfish For Using Accessible Spaces Due to Occasional Pain?
Have You Ever Seen Someone Misuse an Electric Store Cart?
Friendship, Social Situations, And Etiquette
Can a Disabled Person Take an Able‐bodied Person’s Seat?
How Can I Get Over My Fear Of Going Out By Myself?
How Do I Make More Able‐bodied Friends?
How Do I Avoid Accidentally Saying Something Ableist?
How Do I Deal With Friends Inviting Me To Inaccessible Places?
How Do I Explain My Medical Related Absence to My Friends?
How Do I Politely Ask a Disabled Person If They Need Help?
How Do I Respond to Family Members’ Questions About My Cane?
How Do I Stop People From Pushing My Wheelchair Without Permission?
How Do I Stop Security From Following Me When I’m In My Wheelchair?
How Do I Teach My Friends Proper Wheelchair Etiquette?
How Do I Tell My Friend I Have a Chronic Illness?
Is it Okay to Compliment Someone’s Mobility Aid?
Is it Rude to Kneel Down Next to a Wheelchair User?
Is it Wrong to Want More Disabled Friends?
Should I Start a Campus Group for Disabled Students?
Gear
What Do You Know About Frog Legs?
What Kind of Bag Do You Recommend For Cane Users?
What Kind of Lightweight Power Chair Do You Recommend?
What Kind of Shoes Do You Recommend?
What Kind of Spill‐proof Dishes Do You Recommend?
What Kind of Under‐Chair Storage Do You Recommend?
What Kinds of Accessories Do You Recommend for Manual Wheelchairs?
What Safety Gear Do You Recommend for a Manual Wheelchair?
What’s the Best Way to Wear a Backpack While Using a Wheelchair?
Where Can I Buy Armrest Covers for My Wheelchair?
Health And Safety
How can I Prevent Blisters When Pushing My Wheelchair?
How Do I Cope With Feelings Of Isolation?
How Do I Stay Safe During a Fire-drill in My Dorm?
How Do I Keep My Wheelchair Clean and Hygienic?
What Exercises Can I Do to Help Me Push My Chair Better?
What Safety Gear Do You Recommend for a Manual Wheelchair?
What’s the Best Way to Push My Chair to Avoid Damaging My Thumbs?
Will a Wheelchair Help with my Epileptic Seizures?
Would Using Wheelchair Help Keep Me Safe During an Autistic Meltdown?
How To
How Do You Find A Job as a Wheelchair User?
How Do I Apply for SSI/SSDI?
How Do I Keep My Job Secure While Managing a Chronic Illness?
How Do I Navigate the Hills in My Town in My Wheelchair?
How Do I Navigate Tight Spaces in My Wheelchair?
How Do I Push My Wheelchair Up Inclines and Slants More Easily?
How Do I Reduce Pain and Exhaustion When Using My Wheelchair?
How Do I Stay Comfortable on a Long Flight?
How Do I Stop People From Pushing My Wheelchair Without Permission?
How do I Walk a Dog While Using a Wheelchair?
How Do I improve the Suspension on My Mobility Scooter?
How Do You Cut Your Toenails With Cerebral Palsy?
How Do You Keep a Suit Jacket Clean While Pushing a Wheelchair?
How Do You Navigate a Water Park in a Wheelchair?
How Do You Push a Wheelchair in the Rain?
Insurance And Healthcare
How Do I Convince My Doctor I Need a Wheelchair?
How Do I Get a Cheap Wheelchair Without Going Through Insurance?
How Do I talk to my Doctor About Getting Referred to a Specialist?
Will My Doctor Help Me Get a New Wheelchair?
LGBTQIA+
Is it Okay For Able‐bodied LGBTQIA+ to Use Accessible Restrooms?
Is My Disability Defining My Sexuality?
Mobility Aids
Am I Being Selfish For Using Accessible Spaces Due to Occasional Pain?
Can Wheelchair Users Easily Wear Rings?
Do You Have Any Tips for Using a Wheelchair in the Snow?
Have You Ever Seen Someone Misuse an Electric Store Cart?
How Do Advancements in Mobility Aids Cause Disability Erasure?
Is it Okay to Compliment Someone’s Mobility Aid?
Is There an In‐between Chair?
What Brands of Wheelchair Do You Recommend?
What Mobility Aid Should I Use for Temporary Paralysis?
What’s the Best Way to Wear a Backpack While Using a Wheelchair?
When is the Right Time to Get a Wheelchair?
Will My Doctor Help Me Get a New Wheelchair?
Parents And Parenting
Are My Parent’s Religious Beliefs Ableist?
How Do I Convince My Parents to Let Me Use My Wheelchair?
How Do I Talk to My Parents About My Chronic Pain?
Sex, Sexuality, And Relationships
Am I Devotee For Wanting to Date an Intellectually Disabled Person?
Am I a Terrible Person For Identifying as a Devotee?
Am I Ableist for Not Wanting to Date Another Disabled Person?
Am I Ableist for Only Wanting to Date Disabled People?
How Can I Play a More Active Role During Sex?
Is My Disability Defining My Sexuality?
Writing About Disability
Are My Disabled Characters With Magical Enhancements Problematic?
How Can Disability Representation in Media be Improved?
How Do I Find a Sensitivity Editor For My Story?
How Do I Realistically Write a Character Who Can Only Use One Arm?
How Do I Write a Stealthy Disabled Character That Uses a Wheelchair?
How Should I Introduce My Physically Disabled Character?
Is it Realistic to Write a Quadriplegic Character That Studies Art?
Is Suffers From Ever Appropriate When Talking About Disability?
Should I Write a Story About Technology Completely Healing a Disability?
What Traits Do You Want to See In Disabled Super Heroes?
Wanna see your question on this list? Submit an Ask or use the Ask form on my site:
343 notes
·
View notes
Text
SSAFA, the Armed Forces charity supports the entire Armed Forces family. It is a UK non-profit charity that provides long life support to individuals who are currently serving or have served within the British Armed Forces and their families. This impressive organization has been operating since 1885 and was founded by Major James Gildea. Today SSAFA boasts of 5,000 volunteers to help upwards of people every year and is the UK's oldest national tri-service Armed Forces charity.

Why is Collectable Corner choosing to support SSAFA?
The problem people tend to have when it comes to charitable donations and fundraising is not knowing how much of the donors funds are reaching the desired goal of helping someone in need. While we can't speak for the charities themselves, we (myself and my family) can talk about our experience with SSAFA and why we're confident that the money gets exactly to where it is needed the most.
Brian Cook, a loving husband, father, great grandfather and (my) grandad served in the Royal Air Force (RAF) and was a part of the Christmas Island nuclear bomb tests in the 1950's which exposed the soldiers to radiation due to being closer to the bombs than any human should ever be. Today only a handful of the Suicide Squad Veterans are still alive. Almost (if not all) of the soldiers involved died through multiple various cancers and ill health such as chronic arthritis and heart, lung, liver diseases. There is evidence to support the fact that these health conditions can be directly related to what the soldiers were made to do. But not only has it affected the veterans themselves but their families genetics has also caused numerous health problems generation after generation. This will carry on for generations to come also and the UK is one of the only countries involved to not accept these findings and therefore the support for these individuals and families has been lacking. Unfortunately Brian (grandad) was no different, neither is his family.
In January 2018, Brian fell ill and was taken to hospital where within three days of admittance was diagnosed with late stage liver and lung cancer, all that could be done was to make him as comfortable as possible. Over the course of the following four days we prepared for his return home. We gave a sofa away from our living room to make room for the hospital bed due to Brian losing the use of his legs, and we turned a downstairs room into a bathroom. Monday came round and Brian had been in hospital for 7 days, Monday to Monday. He arrived home via hospital transport and we got him settled in as best we could. Grandad always wanted to die at home my grandmother tells me. At 3am tuesday morning, after being home for around 10 hours Brian, my grandmother's husband, my mother's father, and my very special grandad passed away. It was, as anyone who has lost a loved one will know, devastating. It all happened so fast.
During the period between Brian's death and his funeral service SSAFA actually offered us money towards the cost, which we refused based on the fact we would rather it had gone to someone more in need than ourselves, but it stuck with us in our hearts and minds. What we learned is that SSAFA, the Armed Forces charity, gets the money and help to the people who really need it. We didn't expect nor ask for it either. At this period in Collectable Corner didn't exist, what existed was another hobby project that never worked out but a vow was made by myself to use the public platform to raise donations for SSAFA in loving memory of RAF Veteran Brian Cook. Now after a couple of years of hard work, dedication and grind, Collectable Corner, i am elated to tell you is working out and in a position to honour that vow and may he rest in peace.
Who does SSAFA help? And how does it help?
SSAFA, the Armed Forces charity helps people in a variety of ways.
For currently serving personnel and their families provides:
Support in service communities
SSAFA has a network of volunteers on Army, RAF, and Naval bases in the UK and around the world who give local support.
Housing
Housing for wounded, injured, and sick serving personnel and their famiies SSAFA Norton House, Stanford Hall provide home-from-home accommodation for families visiting wounded, injured, sick service or ex-service personnel and outpatients. SSAFA also provides day-to-day management of Fisher House UK at the Queen Elizabeth Hospital, Birmingham (QEHB).
Mentoring for service leavers
SSAFA's mentoring scheme was set up in 2011 and supports those transitioning out of the Forces. SSAFA's volunteer mentors provide support to wounded, injured, and sick leavers through a long-term 'one-to-one' relationship that underpins the transition from the military. SSAFA Mentoring is nationally accredited by the Mentoring and Befriending Foundation.
Adoption for military families
SSAFA is a registered adoption agency dedicated to helping military families through the adoption process.
Additional need and disabilities support
SSAFA provide specialised support to military families with additional needs including their Forces Additional Needs and Disability Forum (FANDF).
Short breaks for children and young people with additional needs from Forces families
SSAFA coordinates holidays and events that focus on offering new experiences and activities for children and young people from services families.
Stepping Stone Homes for women and their children with a service connection
Stepping Stone Homes provides short-term supported accommodation, help, and advice during difficult times. Female spouses and partners of serving or ex-service personnal, along with their dependent children are all eligible to stay there.
Professional health care
SSAFA's professional health care staff provide patient-focussed care to military families worldwide.
Personal support and social work for the RAF
Working alongside the RAF, but outside the Chain of Command, SSAFA staff provide support for RAF personnel and their families worldwide.
Independent Service Custody Visiting
SSAFA provides independent oversight of Army Service Custody facilities.
Support available to veterans and their families:
Housing advice
SSAFA offers practical housing advice and support to Armed Forces veterans and their dependents including guidance around housing benefits and accessing social housing.
Debt advice
SSAFA can help veterans to get advice on dealing with debt when they have fallen behind on their bills or repayments to credit cards and are struggling to get by or at risk of losing their home.
Mobility assistance
SSAFA volunteers seek financial assistance for veterans to help maintain mobility and independence at home. Trained volunteers can help veterans get mobility equipment such as Electronically Powered Vehicles (EPV) or mobility scooters, stair lifts, riser and recliner chairs.
Providing household goods
SSAFA can provide veterans with essential household items, including white and brown goods.
Support for homeless veterans
SSAFA has a range of specialist services to support veterans who are homeless or facing homelessness.
Joining Forces
SSAFA's partnership with Age UK to improve the lives of veterans born before 1950.
Gurkha services
Providing tailored support for Gurkhas and their families who live in the UK.
Glasgow's Helping Heroes
Glasgow's Helping Heroes' is an award-winning service provided by SSAFA in partnership with Glasgow City Council for current and former members of the Armed Forces and their dependants or carers who live, work, or wish to relocate there. It's dedicated team work with national and local governments and third sector providers to resolve clients employment, housing, health, financial and/or social isolation issues.
Forces helpline
SSAFA also offers Forcesline, which is a free and confidential telephone helpline, web chat, and email service that provides support for both current and ex-service men and women from the Armed Forces and their families.
As you can see, SSAFA goes above and beyond to help as many serving and veteran pesonnel and their families as possible who have sacrificed for our country and ensures the aid gets to exactly the places it is needed most. To do this requires a lot of time and money, as you can imagine.
Covid-19 and the SSAFA Emergency Response Fund
Covid-19 has had an impact on everyone regardless of if you are ill. It looks like it will remain a part of our lives for a long time to come, heck, it may be a permanent part of modern life. At SSAFA, calls and requests for help from the vulnerable people, such as the elderly, low income households, and those with serious underlying health conditions. In response to this SSAFA has an Emergency Response Fund. The strain on the organization is obviously high as more people need help with mental health, housing, and financial issues. SSAFA provides this support for the British Armed Forces, serving and veteran personnel, and their families but to do this SSAFA needs to ensure it's staff and volunteers are kept as safe as possible with PPE. Combine the huge rise in help requests and the need to protect SSAFA staff, volunteers and those they help results in a large increase in costs which is why donations are so important and critical to its operations to continue the vital work SSAFA does.
What is Collectable Corner doing to help?
We have purchased over a thousand Royal Air Force (RAF) Dog Tags, Ball Chain Necklaces, Rubber Silencers and Packaging, which we are asking for a donation of £10 per set plus £2.29 for postage of which 100% of the £10 is being donated to SSAFA. Collectable Corner is paying any processing fees and extra postage fees that may incur. Essentially, the Dog Tags are a token of gratitude from us to you for making your donation and helping us to support and help as many people as we can together. In total we have 504 sets of Dog Tags available so that equates to £5,040 in funds to generate. We also have the ability to purchase more should we require them.
How are the donations being made and how often?
We will deposit the donations directly to SSAFA at the end of each month via bank transfer to an account SAFFA has provided to us*.
How will donors know that donations were made?
We understand how important it is to be absolutely transparent with charity work to ensure that everyone knows when and how much is being donated and it is just as important to us at Collectable Corner as to donors and customers. Collectable Corner will of course be publishing monthly updates on our blog and in our newsletter which we urge you to sign up for, along with publishing the donation receipts and sales records minus people's private data such as names and addresses etc. We also have a backend application running on our website which allows visitors to CollectableCorner.shop to view in real time exactly how many sets of dog tags have been claimed.
Share your experiences of SSAFA
Collectable Corner is welcoming you to share your stories with visitors to our website. On each product page is a review section where anyone can make use of by letting others know your story. Maybe it is about how SSAFA has helped you or someone close to you, or maybe you have fundraised and donated in the past. Maybe you are someone who works or have worked with and volunteered for SSAFA who wants to share with us all, or maybe you simply want to say hello.
Thank you...
We, at Collectable Corner, want to thank SSAFA for the amazing work the staff and volunteers have, will and do do. The impact this charity has had on so many lives truly is something to be marvelled at.
Thank you to anyone who helps us to make some real world differences by ordering a set of RAF dog tags with the knowledge that you are donating to a truly awesome cause.
Thank you to all of the past, present and future British Armed Forces personnel who have sacrificed, and do sacrifice everything for our great nation. You make us proud each and every day.
Finally, thank you Brian Cook, my Grandmother's Husband, my Mothers Father, a Great Grandfather, and my Grandad for being such an inspiration, thank you for being the best and only Father i ever had. May you sleep easy and Rest in Peace.
*Please note that the information in this article has been vetted by and in part supplied by SSAFA prior to being released to the public and is accurate at the time of this publication. Collectable Corner has the permission of SSAFA of the logo to be used and they are the copyright owner. SSAFA is a non-profit charity registered in England and Wales (210760), Scotland (SCO38056) and the Republic of Ireland (20202001). Collectable Corner is not in a partnership with nor affiliated by SSAFA, however we are in contact. Anyone who wishes to confirm that SSAFA is aware of Collectable Corner's campaign to raise donations and the methods being used can do so by emailing [email protected] or [email protected]


1 note
·
View note
Text
Mental Health and Covid-19
Introduction:
The current pandemic due to the novel Coronavirus (SARS-COV-2), COVID-19, has resulted in considerable stress to the health systems throughout the world. COVID-19 pandemic has left in its wake an unprecedented challenge for mental health services across the world. With almost all affected, mental health service delivery to address the psychological consequences at the individual level has become near impossible. Pandemics, like other natural disasters, negatively affect the mental health of the community in general and those with pre-existing mental illness in particular. While natural disasters also result in significant stress and strain to the health systems, the relative non-involvement of other regions allows one to divert the health resources from other regions.
As the focus during a disaster is on stress and anxiety-related disorders, there needs to be literature on the specific needs of people with severe mental illness during pandemics. Considering that a considerable proportion of patients with severe mental illness require continued management even during a pandemic, strategies to continue the care need to be developed. Otherwise, disruption to or absence of access to care can have serious negative consequences in patients with severe mental illness.
Different aspects:
The existing health services are at its breakpoint to control the spread and reduce the mortality of COVID-19. Policymakers though aware of the mental health consequences are prioritizing the capacity building of the health services and attempting to reduce the socio-economic hardships of communities following COVID-19.
Mental health issues noted in (biological) disaster zones including COVID-19 can be classified into an acute phase during the outbreak (approximately 2-6 months) and long-term phase after the control of the outbreak (>6 months).
a) Acute Phase (during the outbreak) – Issues to be dealt with include immediate mental health impacts such as fear, denial, anxiety, insomnia, dissociative symptoms, depressive symptoms, suicidal ideas/attempts, substance withdrawal, and relapse of pre-existing mental health problems. Besides, stress-related issues of the health care providers and frontline personnel need to be addressed.
b) Long-term phase (after the control of the outbreak) – Issues commonly presenting include grief, survivors’ guilt, depression, substance use, relapses of pre-existing mental illness, PTSD, and somatization disorders. The major stressor during this period will be the direct and indirect socio-economic impact of COVID-19. Along with the diagnosable mental health issues, the affected community also harbors a large number of the worried well. Mental health professionals should be aware of this phenomenon and restrain themselves from labeling this population with mental disorder and treating them aggressively with medications.
In addition, all health care and frontline personnel should be aware that mental health issues post-COVID-19 (or any disaster), represent the emotional reactions of normal people in abnormal situations and for a majority these symptoms are self-limiting.
Case Finding:
There are possibly three streams for case-detection/identification of mental health issues that need to be focused in the acute phase of COVID-19.
1. Case Identification by front-line medical and non-medical personnel (including police officers, Members of Local Self Government, Community/health workers)
- Points of entry into the country/state –Airport/Railway Station/State borders etc.
- Home quarantine visits
- Other Medical Emergencies
2. Case Identification by health care professionals (non-psychiatric)
- Hospital quarantine/isolation
- Routine out-patient assessment for other illness
3. Self-referral/Walk-ins to mental health professionals
4. Identification of frontline medical and non-medical personnel in need of help/support for stress management or burnout
5. Screening of the high-risk (vulnerable) population once Community Transmission is established
Who are the most Vulnerable?
· Children
· Senior citizens
· Pregnant women
· Persons with disability
· Homeless individuals, Poor social support & lower economic status
· Marginalized communities
· Life-threatening chronic medical conditions like cancer, chronic renal failure, liver diseases, asthma/COPD, immunocompromised patients
· History of severe mental illness and wandering mentally ill
Mental Health Issues:
1. Mental Health Issues of Home Quarantine:
Quarantine is defined as the separation of people who have been exposed to a contagious disease to ascertain whether they become sick, thereby reducing the risk of them infecting others. Presently governments across the world and in India are using a combination of measures to stop the spread of the COVID-19 pandemic. While considered essential under the present circumstances, quarantine can be a taxing and distressing experience for many. Based on studies from previous epidemics/ pandemics we shall identify some of the mental health concerns which people in quarantine face and propose solutions/remedial measures for the same. It must be acknowledged at the outset that we could not find any intervention studies which have examined the effectiveness of the various remedial measures. Rather, these measures are proposed based on the problems people in quarantine had faced in previous epidemics.
2. Mental Health Issues in Hospital Quarantine/Isolation:
Quarantine is done for the larger interest of the community by curtailing the right of the individual. The quarantine can lead to physical, psychological, emotional, and financial stress due to fear of contracting the illness, boredom, loneliness, loss of personal freedom, a new set of daily routine, and lack of social togetherness.
The mental health issues following the hospital quarantine period can be
a. New-onset mental health problems
b. Exacerbation of pre-existing mental health problems.
3. Mental Health Issues in Children and Adolescents Children:
All of us, children included, are trying to make sense of the overwhelming uncertainty in front of us due to the global pandemic caused by the Coronavirus (COVID-19). Children and adolescents have already been at home – with schools being shut early – for over three months in several parts of India. Their regular schedules have been disrupted, with no clear idea of when they will be restored. Children may experience a range of psychological issues such as anxiety, fear, worry, depression, difficulty sleeping, and loss of appetite.Quarantine and isolation may also lead to an acute stress disorder, PTSD, and grief in many children. Children with various physical and mental disabilities – and especially mental health disorders – are more vulnerable during this trying time.
Social isolation may worsen the living situation of children in abusive environments as well as children with special needs. Children may even go through loss and grief at this time.
4. Addressing Mental Health Issues among Pregnant and Postpartum Women during COVID-19:
Positive mental health is particularly important during pregnancy and postpartum. Currently, available literature has consistently shown an association between depression, anxiety during pregnancy, and small for gestational age, low birth weight, and preterm delivery. During the postpartum period around 10-15% of women experience depression and anxiety.
It has also been observed that postpartum depression is one of the reasons for poor bonding with their babies. In the current period of COVID-19 pandemic, even routine visits to health care facilities for antenatal care and infant immunization are likely to create a great sense of anxiety in mothers about their health and that of their unborn or newborn baby. It is thus a matter of priority to address these concerns to ensure positive mental health and early interventions for perinatal mental health issues.
Ø Symptoms of anxiety and psychological distress during the perinatal period related to COVID-19:
· Excessive worry about getting the infection even when all precautions are being taken and even after reassurance
· Lack of sleep because of anxiety
· Focusing excessively on social media messages about COVID-19
· Getting anxious about infection control procedures in family members
· Excessive worrying about missing work
· Feeling sad and angry because of isolation and not being able to meet family and friends
· Feeling nervous, anxious, or on edge
· Not being able to stop or control worrying
· Trouble relaxing
· Being so restless that it's hard to sit still
· Becoming easily annoyed or irritable
· Feeling afraid as if something awful might happen
5. Suicidality in the context of COVID-19 Pandemic:
The ongoing COVID-19 pandemic worldwide has been increasingly associated with suicides. Instances of suicide in the context of the pandemic have been reported among individuals who have tested positive for COVID-19 infection, those who have suffered severe financial setbacks. The COVID-19 pandemic has led to significantly increased levels of stress at the community, family, and individual levels with a consequently increased vulnerability to suicide.
6. Counseling for home quarantined using telephone helplines and telepsychiatry:
For subject’s in-home quarantine, supportive counseling can be provided by telephone helplines and telepsychiatry platforms. These have an important advantage over the face to face counseling, as they provide specialist services, which can be accessed from the convenience of peoples' homes without endangering the health personnel and the larger community.
Telepsychiatry Video Consultations (VC)
In the background of the COVID-19 pandemic, advancements in digital communication (telepsychiatry) has meant that there are means to overcome this to a great extent. During the ongoing COVID-19 pandemic, it may be a safer alternative to provide infection-proof consultations from both the user (patients and their family) and the provider (psychiatrists).
What is telepsychiatry?
It means that patient care is provided by the psychiatrist to the service users employing digital technology.
Conclusion:
In conclusion, considering the possible higher risk of contracting the infection, patients with severe mental illness requires special attention. Continuation of community-based treatment is essential to prevent relapse or worsening of the severe mental illness which can add additional burden to the stressed health infrastructure. Technology platforms need to be widely used for teleconsultations to achieve the same.
Quarantine, isolation, and social distancing in the times of a raging pandemic can be psychologically distressing for many people. However, there are simple and effective actions that you can take as a health care provider. Psychological issues following the pandemic are likely to be common. Most affected will require only brief assessments and immediate support. Given the lack of knowledge base, a clinical decision needs to be made and treatment for COVID-19 needs to be individualized in patients with severe mental illness.
2 notes
·
View notes
Text
My ask box continues to fill up, and I have no answers for any of this. I’ve gotten comments that @dreamworksanimation is good about things like fair representation in other shows when it comes to disability, queer relationships, racial diversity, and just plain solid storytelling. Why was @voltron the exception?
Or you can just have the questions from my asks:
I really, really wanted [Dreamworks execs] to address the situation, to tell us why VLD took that enormous shitty turn and to apologize and do us better. But I'm guessing we already know the answer (arrogant inexperienced EPs) and I think they won't do anything about it, just try to fade Voltron to the background as it's ending and focus on She-ra, if they ever decide to apologize, they're just gonna focus on the LGBT rep as if its the worst problem of their story.
You know what, I hope someone makes an extensive list of all the morally questionable messages Voltron has sent with all its characters (Shiro & Kuron everything, and Lotor as abuse victim in particular), all in detail and shove them in their faces saying, but to you it's 2 guys in love and in a healthy relationship that is wrong, instead of ableism, racism, homophobia, etc. When I think of what the kids will take from Voltron I feel sick. But queer love is the problem here, right. I’m disgusted.
Us: can we get a happy ending too like the het people and couples in the show?
VLD: no, not a happy or even semi-happy ending, you'll get a miserable ending but get this, we're going to write the last survivor of the 4 queer characters we killed off to be totally on board with this. We'll write him and animate him as if he's happy and got resolution, growth, and catharsis and not as if he got demoted, sidelined, isolated, discarded by his family, worst of all by Keith. We'll say a monster like him can’t be a paladin.
Let’s also go back to talking about how they not only made Lotor, a victim of child abuse not to mention biracial character who grew up with everything against him: suddenly evil, be the same as his abusive "father" and "mother" (who even after remembering who he is pulled the same crap as before), took every happiness away from him and had the nerve to mock his abuse in S7?! As a child abuse survivor I'M HORRIFIED.
The messages in the Shiro/Adam scene is disgusting, this is such a difficult subject, even for adults show with plenty time to explore and be fair to both characters while being explicit about it all. I was worried: in a kids’ show? how can they write this in a way they'll get it? With barely time for it? but look what they wrote, Adam gave an ultimatum instead of support and died, then they blamed the disabled guy for everything. Message: you’re gay so your relationship and your life are worthless, you'll be miserable and alone.
For a team that is all about working together, voltron members after 7 seasons still don't feel like a family and more like colleagues from work. ¯\_(ツ)_/¯
It feels odd knowing that they weren't actually battling homophobic higher ups. It feels more tactical and greedy for social justice points than out of genuine desire to showcase diversity. Is it coincidence that the character they dislike the most is the one selected for this honor? As a lesbian fan i'm skeptical and angry and refuse to watch anything else by these two.
People keep trying to excuse this stuff with "Voltron is a kids' show", but you know what? There are gay kids out there. There are disabled kids out there. Much as we may wish it otherwise, there are kids out there experiencing trauma. Do we REALLY want to teach those little kids that they are broken and tainted forever and nothing good is waiting for them in the world from here on out? People need to know how damaging it is to have ZERO stories in media showing realistic healing of trauma.
The lady who betrayed them got a proper send off scene even tho she send Adam & the others like pigs to slaughter & betrayed them & caused them all to almost lose and die. Got screentime & some characterization. But sure why respect Adam that way too. I will never forget the dread I had for him when I saw he was with the fighters who were sent to die, then watched them one by one lose their lives until he too, was killed. I still feel sick thinking about it. We never even learned his last name.
I know it's been a while but I'm not over how they treated Lotor in s6. I'm from a broken and dysfunctional home and this show I watch for escapism told me I'm doomed to repeat the same mistakes of my parents, end up just like them. ... Are they even aware of the messages they send to their audience? Not all of us had good childhood like Allura.
From a chronically ill perspective, I felt downright insulted by the choice they made to give Shiro a degenerative illness. The idea of a chronically ill hero is cool but they pull the cure narrative, they don't give him a real illness, and it's just used for cheap irrelevant drama. Plus the whole "Has to choose between loved ones and goals" thing was pretty insensitive, we're already expected to sacrifice so much as ill people so the reinforcement of that was unpleasant to watch and read meta on.
Even if everyone was white cishet abled guy the messages sent to kids were awful: One who fought to carve his own path was forced to become someone else, one who suffered and fought till the end was told he’s a monster that can’t be a paladin, the insecure one will never be worthy as himself and he'll always be someone else’s replacement, one who survived genocide and suffered loss upon loss until reduced to nothing, one who suffered by his parents’ hand became like them, the whole Kuron thing. You cant brush off all THAT.
going into the new semester with the horrible messages of s7 on my mind...i’m lethargic. i have been since the “retired paladin” interview. it was bad for me to balance my mental health on the state of a fictional character, but it was really effective. Until that awful message that disabled people are helpless in controlling their own lives. I’m trying to disconnect and thrive anyway, out of spite against ableism if nothing else.
I had this horrible realization: you know how Shiro is a victim of abuse and him getting the Black Lion was him regaining the control the lack of he suffered in his capture? I think they gave him the illness and handwaved it with the clone, so as to argue for his removal from the Black Lion. They claim that the reason he wanted control was the illness and not the victimization in the Galra hands. They're essentially erasing his trauma.
Writers: so we'll write endearing multidimensional characters with many layers, we'll have them subvert stereotypes, especially those that characters like them usually are written with, ie. Keith isn't a loner nor is he angry just 'cause, but a lonely abandoned kid with trust issues due to his mom leaving him, thus has poor emotional control and anger management, struggles to connect and open up, he is the one whose arc embodies the found family theme more than anyone.
EPs: nah we want stereotypes loool
We talk about Shiro and all the ableism in his story but we don't talk nearly enough about how horrifying the message is that Keith is the one to take it all from him and kick him aside. Keith chose to discard Shiro because he's broken and useless, so he can take his place. I've been through things they both have and I find all that horrifying. S7 sent terrible messages to kids watching.
They had the chance to let Shiro overcome and be a hero. To defeat his own abuser (Sendak) except Keith takes over everything and fixes everything for him while he lies helpless on the ground without a new arm yet. They had the budget. The animation. They could have empowered Shiro. They saw how many people saw themselves in Shiro's struggle. They must have seen the concerns. And they actively chose to go against that.
The Bury Your Gays trope is even worse this season when you consider the heavy lesbian subtext with Lotor's former generals who get blown up on screen. And naturally, it's the one with a crush on Keith who turns good and survives.
Was there a minority that hasn't been screwed over? Bury Your gays was merely the last shocking straw, because the whole season was chockful of terrible messages and proved they would never treat their characters right and address stuff from before. Homophobia, racism, ableism, sexism, mocking of abuse, excusing abandonment & so on.
I’m adding my voice because I'm so, so tired. None of the characters i see on screen are the characters we got to know in s1/2. The character i most related to was beaten down out of spite for 4 seasons and now may as well be a cardboard cutout. DW and the EPs don't seem to give a single shit about how badly this season has affected people. i don't know whether to jump ship or spit fire over everything. i'm just... exhausted.
I want a transparent statement & apology from DreamWorks. I want to know THEIR stance & role in this, ALL the events that ended up with us getting a show that is not only homophobic but also ableist, racist, mocks child abuse and so much more. I want them to acknowledge & explain why they allowed the marketing team to bait fans with ship content in their videos, thumbnails and even that EP interview about shipping. I want to know who and why allowed the show to to take a worse direction in recent seasons.
I have no answers for any of this, @dreamworksanimation. If there are any explanations, any reassurances that you’ll work hard to prevent any repeat, you need to say so. The longer you’re silent, the more it looks like you’re fine with the story and all its horrific messages. Are you?
130 notes
·
View notes
Text
New Zealand's most shameful secret: 'We have normalised child poverty'
One-third of the country’s children, or 300,000, now live below the poverty line – 45,000 more than a year ago
For 14 days and 14 nights Elijah Saitu, 15, has lived in a damp motel room, bordered by KFC to the left and a Denny’s 24-hour takeaway to the right.
He spends his days watching music videos on television and eating white bread, tinned sardines, fizzy drinks and packets of chips.
“He’s suffocating,” says Elijah’s mother, Emily Fiame Saitu, who has been begging the government to help her family.
“It’s cut-throat in New Zealand. If you’re struggling you get left behind.”
The Saitu family are a tragic portrait of New Zealand’s most shameful national secret: an epidemic of child poverty that belies the image of a Pacific haven offering equality of opportunity and a prosperous, clean, healthy life of plenty for all.
The family of six have been living in two motel rooms in South Auckland for a fortnight.
The motel bill is paid for by Housing New Zealand, a government agency, while the family wait for a state house that is warm and dry enough not to make the Saitu kids sick (they have all suffered serious respiratory illnesses from cold, damp homes).
Elijah, who is autistic, spends all day staring at the pink wall next to his single bed, stroking the flaking paint. His three siblings aged 17, 14 and 12 – also spend their days inside, watching music videos. Their parents are wary of letting them wander around the cut-price motel, which largely caters to solo travelling truck drivers.
None of the Saitu children attend school, and haven’t for months. Without a permanent address – or any idea when or where one will come – in the local catchment area, enrolling in any of the local schools has been a battle.
Two of the Saitu children are severely disabled and need to attend special education schools, where government places are competitive and difficult to secure. Apart from a few picture books and a couple of dolls their play and intellectual stimulation is nil.
“I feel like I am screaming for help,” says Emily Saitu, adding: “When I say we are desperate, people avoid my eye, they don’t listen to me. They don’t want to know that I am going crazy trying to make a life for my children.”
The Saitu children are not alone in their desperation. A third of New Zealand children, or 300,000, now live below the poverty line – 45,000 more than a year ago.
Unicef’s definition of child poverty in New Zealand is children living in households who earn less than 60% of the median national income – NZ$28,000 a year, or NZ$550 a week.
The fact that twice as many children now live below the poverty line than did in 1984 has become New Zealand’s most shameful statistic.
“We have normalised child poverty as a society – that a certain level of need in a certain part of the population is somehow OK,” says Vivien Maidaborn, executive director of Unicef New Zealand.
“The empathy Kiwis are famous for has hardened. Over the last 20 years we have increasingly blamed the people needing help for the problem.
“If you can’t afford your children to have breakfast, you’re a bad budgeter. If you aren’t working you’re lazy. But our subconscious beliefs about some people ‘deserving’ poverty because of poor life choices no longer apply in today’s environment. We have to ask ourselves as a society, are we really prepared to let our children grow up this way?”
We have to ask ourselves as a society, are we really prepared to let our children grow up this way?
For a third of New Zealand children the Kiwi dream of home ownership, stable employment and education is just that – a dream.
For poor children in the developed South Pacific nation of 4.5 million illnesses associated with chronic poverty are common, including developing world rates of rheumatic fever (virtually unknown by doctors in comparable countries such as Canada and the UK), and respiratory illnesses.
Meals are irregular and nutritionally poor, consisting of meat pies, hot chips and 99c white bread. School attendance may be patchy or skipped entirely, and protective clothing and footwear for the harsh New Zealand climate is a luxury.
While poor children don’t die of starvation in New Zealand, they increasingly live a strained existence.
“Poor children in New Zealand don’t fully participate in life, they miss out on so many things that make life rich and meaningful,” says Linda Murphy, a social worker with the Auckland City Mission. “Like music, like sport, like a full education, like the expectation that they will grow up and find a job.
“The momentum in these young lives becomes about survival, nothing else.”
The mission is located in busy central Auckland but the most deprived regions of this increasingly chaotic mega-city are in South Auckland, in the ghettoised suburbs of Otara, Papatoetoe and East Tamaki.
This is where Hirini Kaa, an academic on the management committee for Child Poverty Action Group, and an Anglican pastor, has lived for most of his life.
“It is interesting the world believes New Zealand to be an ideal country,” Kaa says. “But it’s more interesting that we also believe that myth about ourselves.”
Catch a bus or two from Britomart in central Auckland, and after an hour and a half and you will arrive in the urban slum of South Auckland.
Here, houses are wooden, damp and mouldy and often hold in excess of 10 people. Young children walk the streets in mid-winter with no shoes and gummy eyes. Looming over polluted streams and rubbish-strewn parks is the vast Double Brown Beer Brewery.
“Child poverty has always been here – especially among Māori and Pacific populations – but it wasn’t until homeless people started interrupting middle-class voters having coffee in central Auckland that the government decided to ‘tackle’ it,” Kaa says.
“If it’s segregated in South Auckland, fine. If it’s interrupting my latte asking me for money, we have a problem.”
Before the 2014 election the prime minister, John Key, said tackling child poverty would be a priority for his government.
The government’s child poverty strategy is built on getting Kiwis off benefits and into jobs.
But the problem is that any of New Zealand’s poorest children are now living in families with one or more parents in employment who still can’t get by or make ends meet.
“The consistent message from the government is that work is the route out of poverty, even though around 37% of children in poverty have two parents with two incomes,” says associate professor Michael Anthony O’Brien from the school of social work at Auckland University, who is also a member of the Child Poverty Action Group.
“The government is doing as little as they can get away with … the most significant action they’ve taken is increasing the benefit by about $25 a week for beneficiaries with kids. That’s it – that’s the biggest thing they’ve done.”
Darrin Hodgetts, a professor of societal psychology at Massey University and an expert on poverty in New Zealand, says the government’s stance that jobs would lead poor families out of poverty was nothing more than propaganda. “We have to stop blaming the poor for being poor,” he says.
“The myth that these families are somehow inherently dysfunctional and they can’t look after their kids. That is not true. That children are failing because their families are bad. It is not true. The state is abusive, the welfare system is abusive, and after decades of this many people can’t cope.”
Although child poverty is most visible in the major cities, Kaa says he has relatives in the isolated regions of the East Cape and Northland who are going without many basics – including electricity.
“The level of intergenerational, ingrained child poverty has reached a point that it is challenging the idea New Zealand has of itself as an egalitarian nation; the myth that we are god’s own country,” he says.
It’s Sunday night at the Rayland Motel and Emily Saitu is preparing for another week of holding out the begging bowl.
In her youth she worked for the ministry of justice as a secretary. She thrived on the order and routine of the job, and the regular pay cheques that allowed her to eat pancakes and cappuccinos at Denny’s with her brother.
But that was nearly 20 years ago – before she had four children, before her husband lost his job in a meat processing factory, before life in New Zealand became hard.
“When I meet my counterparts around the world they are deeply shocked to learn of such ingrained, desperate poverty in New Zealand,” says Maidaborn of Unicef. “We have been very good at selling a brand New Zealand. And increasingly that brand is being exposed as a marketing ploy, not a deep systemic reality.”
As Saitu pores over files of documentation – applications for benefits, applications for disability assistance, applications for help – her two daughters draw pictures in the misted glass of the motel room. Looking in from outside the whole door is covered in their finger paintings – squiggly patterns, rain drops and a frowning sun.
“New Zealand is ashamed of us, they want to forget about us,” says Saitu, aggressively wiping tears from her eyes. “New Zealand doesn’t want my children.”
Reference: New Zealand's most shameful secret: 'We have normalised child poverty' by Eleanor Ainge Roy Tue 16 Aug 2016 01:42BST. Retrieved from: https://www.theguardian.com/world/2016/aug/16/new-zealands-most-shameful-secret-we-have-normalised-child-poverty
2 notes
·
View notes
Link
#Anxiety#CelebratingYourGiftofLife#Depression#Isolation#JamesDonaldson#JamesDonaldsonnotes:Welcometothe“nextchapter”ofmylife…beingavoiceandanadvocateformentalhealthawarenessandsuicideprevention#JamesDonaldsonMentalHealth#JamesDonaldsononMentalHealth#Loneliness#MentalChallenges#MentalHealth#MentalHealthProfessionals#MentalHealthStigma#MentalIllness#MentalIssues#SocialIsolation#YourGiftofLife#YourGiftofLife.org#YourGiftofLifeFoundation
0 notes
Photo

(via Cannabis Refugee, Esq. One Year Later. (Meta Discussion))
Cannabis Refugee, Esq.
Advertising / Media / Cultural Conversation
,
Alternative Treatment
,
Capitalistic Patriarchal Medicine
,
Crohn's Disease
,
Crohn's Disease Stories
,
Euthanasia / Suicide
,
Family / Friends
,
Financial
,
Fundraising / Patreon / Please Support this Project
,
Law / Legal / Benefits
,
Marijuana / Cannabis
,
Natural Law
,
Other Autoimmune Diseases
,
Radical Feminism
,
Storytime
March 7, 2019
As my readers may’ve seen or sensed from the recent comments and content on this blog, I have become disillusioned with the CRE writing project and may decide not to continue writing about my experience as a Crohn’s patient trying to survive outside the Western medical system that was not helping me and was only making me worse. As far as I can tell, this project has not inspired any additional writing or critical thinking on this subject, my posts have not been widely shared or inspired much interesting feedback, and this work has not opened up any additional opportunities for me in the way of writing or activism. Of course, those were not the reasons I started this blog in the first place but they are to be considered when looking into the future of this project and whether it is in my or anyone’s best interest that it continue.
My original intent in starting this project nearly one year ago was to document my experiences as a seriously ill woman for whom conventional medical treatments were not working including the social, financial and health-related fallout of this system that seems designed to control and punish sick people while we carry the blame and shame for Western medicine’s failures and even its lies. At times my health and financial situation have been so precarious that I actually believed (and still do believe) that I am going to die here, alone and in the middle nowhere, and I wanted the truth about what happened to me to be known or at least knowable by those who would wonder what the hell could’ve possibly happened that led to that sad and lonely end.
Through this project I have documented how, as strong and intelligent as I was, and regardless of how much I prioritized and activated toward my own health and wellbeing, one woman is simply no match for this hideous system of Western capitalism and patriarchy and how and why that is. I documented every step of this horrible journey including Western medicine’s early failures to treat my pain and symptoms, how prohibition and regulation of medical cannabis drove my search for relief 1000 miles away from my partner, my family and my profession, and how corporate propaganda serving both Western medical and cannabis interests misled me (and others) to believe that I could cure myself of an incurable, progressive disease.
Ultimately, all of this has led me to where I am now: still sick and extremely vulnerable, having spent my entire life’s accumulations in pursuit of effective treatment and where my friends and family now believe that my life is falling apart because of my obstinate noncompliance with Big Medicine and “reefer madness” and not because Crohn’s disease is a dangerous, debilitating, incurable and progressive disease that predictably and consistently robs people of their money, their independence, their dignity and their very lives regardless of how and even whether they attempt to treat it. Over the past 6 years treating first with Western medicine and then with medical cannabis and reflecting on my experiences, and after a year spent writing about it, I now believe that Crohn’s disease is a terminal illness where I have to medicate constantly in order to eat.
This collection of articles comprising the CRE blog documents the reality of all of this and stands in opposition to the propaganda about Western medicine and medical cannabis generally and of Crohn’s disease specifically where seriously ill people are given false hope and ultimately blamed when our incurable illness predictably is not cured and where our progressive pain, symptoms and disability predictably get worse, and not better, over time. And I, as an individual woman, have been unable to change these fundamental truths about my illness and about my existence as a female-bodied person under capitalism and patriarchy. Thanks to feminist gaslighting though, I foolishly believed otherwise and that somehow I would be able to wrest back control over my health and my life against all the odds and against all evidence. This has been a rude awakening for me and has left me broken and terrified with little to no hope for my future.
So that is where I am now and I do not know where I will go from here. I had hoped this whole time that somehow, maybe through the care and concern of others (and maybe not) I would manage to get myself into a sustainable living situation. For me, that means that I will continue to manage my pain and retain my dignity indefinitely as a seriously ill person who is not likely to get better. The reality is that there is probably no way I will be able to do that, and that reality has caused me endless terror and grief. However, what even is “sustainable” under the current system and how many of us live sustainably whether we are sick or well? How many women are safe and secure financially and materially under any circumstance?
Despite my best efforts, I wasn’t ever able to reliably control my outcomes when I was (relatively) well so there is even less chance I will be able to do that now that I am seriously chronically ill. Just because I stubbornly believed otherwise, and had to believe otherwise to retain my alleged “sanity” doesn’t mean it was ever true and it very obviously was never true was it? For now, I am starting to recognize and process the apparent fact that everything I am experiencing, including progressive pain and symptoms; aggregating side effects from medications; abuse and neglect by Western and alternative medical systems; rejection by and unconcern of family and friends; hopeless poverty, social isolation and crippling despair; suicidal ideation and/or attempts and completed suicide; even early and current Autism Spectrum Disorder (ASD) symptoms — all of it — is part of the Crohn’s experience. And as a sick person and especially as a sick female there will be little or nothing I can do to mitigate this experience for myself or for anyone.
Any support including donations I can muster now are probably not going to get me into a sustainable situation since that really does not exist. Donations including from my Patrons will simply buy me time until the inevitable arrives, or until I get the miracle I have atheist-prayed for since I’ve been so seriously ill. So thank you, Patrons, for buying me some time, which I am spending with my beautiful cats in a gorgeous geographical area, treating my pain and symptoms with medical cannabis, and (for now) thinking and writing about what this all means. I do think this has been a worthwhile project and I have been pleased with the content if not the outcome which seems to have been, basically, for naught. We really appreciate your support.
Please feel free to contact me through my Patreon page or consider becoming a Patron if you have used or enjoyed my work. Thank you for reading.
3 notes
·
View notes
Note
☂ - favorite season?, ✘ - hates?, ♛ - favorite hair color?
☂ - favorite season?
spring !!
♛ - favorite hair color?
i love when people dye their hair fun colors, my favorite are like soft pastel colors or bright reds and blues. i also like that really platinum blond and i like silvers!
PUTTING THIS UNDER READ MORE BECAUSE I WENT ON A MESSY RANT
✘ - hates?
let me get serious for a second because i think this is a bigger issue than i was aware of. there’s a subreddit called ‘illnessfakers’ and they “”””call out”””” youtubers or social media influencers i guess you would say and claim that they’re faking their illnesses for money and such. and it’s disgusting to see honestly, like even the reasons they come up with for them “faking” it are so dumb they don’t even know what it’s like to be chronically ill and can’t even grasp the concept of every second of your life being in pain or what it’s like to have your life controlled by something you have no control over.
or maybe they do have some sort of illness and that’s what makes them feel so entitled but honestly??? if you’re someone who’s dealt with/dealing with a chronic condtion of any kind and see someone struggling but still getting money and decide that they’re faking it? you are truly a person that needs to take time to educate yourself and learn some empathy.
and what i want to say is what my mom tells people with me: you don’t live with her, you don’t see her every day, so you don’t know what she’s feeling
i hate the fact that these people have taken it upon themselves to put themselves on this high pedestal to “call out” people who have these conditions and most likely have been told things like ‘you’re faking it’ or ‘it can’t be that bad’ for a long time to begin with
i also hate the fact that one of my favorite youtubers who gave me a lot of hope for the future and gave a positive but honest look at chronic illnesses has been the subject of these cretins and unfortunately and devastatingly she passed away recently. and now i’ve seen people saying that ‘ she did it to herself because she got treatment she shouldn’t have ‘ and it makes me so upset i cry because i can’t imagine her having to see all these dillweeds saying she was faking it while she was in the hospital and while she was dying.
on that point this youtuber, chronically jaquie, was amazing and made me think differently about being disabled and gave me a lot of hope and smiles and i’ll be forever grateful to her for that
BASICALLY IF YOU AREN’T A DOCTOR AND HAVE NEVER EVEN MET SOMEONE IRL IT’S NOT YOUR BUSINESS AND YOU DON’T HAVE ANY RIGHT TO FEEL JUSTIFIED IN STARTING RUMORS ABOUT ANYONE
yes there are people who”fake it” but that should be up to their DOCTORS to diagnose and help them try and learn to cope and deal with that mental illness because, if you take time to research factitious disorders, munchausens in particular seems to be their interest, that they don’t know the exact cause of this but it’s common belief that the people that suffer with it are victims of abuse and/or neglect as children and what they need is a doctor who cares and doesn’t write them off and wants to get them the help they deserve. they don’t deserve to be torn a part by the internet, that’s not going to help them. even if people who “fake it” make the community as a whole look worse we need to understand and recognize that these people are truly suffering from a serious mental condition.
all i know is when i first got sick i was very scared and very isolated from my family and peers. i lost all my friends AND THAT’S NOT THEIR FAULT IT’S MINE AS WELL and i have a lot of family members and family friends that don’t like me simply because my mom puts me first (even if i would appreciate if she would stop using me as an excuse now that i’m older).
what happened was that everyone except my mom made me think that i was purposefully making myself pass out somehow and purposefully throwing up no matter what i ate. i was at the point i started praying for something to be seriously wrong with me, not to prove them wrong entirely, but so that it would kill me and i wouldn’t have to deal with the pain anymore.
and maybe i do exaggerate some things but i know dang well that every day i do my best to be smiley and happy no matter how i’m feeling because i got sick and tired of being miserable all the time.
also there’s no shame in taking pain pills or any other medication. i don’t take them because i don’t notice a difference and the stronger ones i didn’t like how they made me feel--but i don’t think any less of people who do their best to do what they can to make their life more manageable for them.
and again, something common i’ve seen amongst people who have chronic illness is this: fake it till you make it. so what you see of people online might be the best of the worst or the best of the best.
and another thing PEOPLE SHOULDNT HAVE TO PROVE THEY’RE SICK BY BEING THE STEREOTYPE OF WHAT WE SEE IN THE MEDIA. chronic illness can happen to anyone. anyone.
and life is hard enough for them so please get off your high horse and learn some empathy and respect.
// distract me please
#answered#SORRY I RANTED I WAS MAD ABOUT THIS EARLIER MAN#also hello i hope you're doing okay <3333#theyooniverse-93
1 note
·
View note
Text
MY JOURNEY: The Beginning
To whom it may concern,
I have decided to begin a blog that tells the story of my trials and tribulations with Mental Health and Chronic Fatigue Syndrome. There are a number of reasons why I have chosen to embark on this task, from spreading awareness of these monstrous illnesses, to simply venting when I am struggling. I hope you will find this useful to yourself, as I am hoping that by sharing my experiences with you, you will feel less alone and isolated when battling with your own demons.
To begin this journey I will start by telling you a bit about myself, so if you're sitting comfortably, lets begin…
My “journey” began when I was in Year 8 at Secondary School (aged 13) as I was facing a lot of difficult challenges at home and at school. After a while this started to impact on my mental health and I was referred to Child and Adolescent Mental Health Services (CAMHS), a service for children up to the age of 18, and this is where everything began to take a turn for the worse. For the next 6 years I began battling with my Mental Health and even with the help of a team of psychologists, psychiatrists and social workers, I was deteriorating rapidly. I was firstly placed on a programme of counselling in my local centre for CAMHS, which soon turned into a course of Cognitive Behavioural Therapy (CBT). However despite me attending weekly sessions, my health did not improve and so it was deemed necessary to start me on a course of medications - a combination of anti-depressants, anti-psychotics and sleeping tables. Since then, I have rotated around a number of different combinations of medications at a number of different dosages.
In February 2017 I was admitted to my first CAMHS inpatient unit under Section 3 of the Mental Health Act of 1983. Little did I know that this was going to be the start of a string of hospital admissions, A&E trips and further Sections. This admission was in the middle of my first year of A - Levels and so I struggled with keeping up my studies as well as trying to mend my body and my mind. After 7 months inpatient, I was discharged just in time for my 18th birthday, however living in the community didn't last for very long and I soon ended up back in hospital.
This time however it was different, as I had turned 18, I was now placed on an adult ward. Of all my units that I have had the misfortune of being on, this one was the worst, I was constantly on 1:1 support - where a member of staff is at arms length from you at all times (this is particularly demeaning when you need to use the bathroom), I began to struggling with what rapidly turned into my Anorexia Nervosa and as well as this, my sleeping became more disjointed and despite having slept for 15 + hours I was still exhausted. Having been admitted for severe self harm with suicidal ideology, along with a whole host of other symptoms, I received my worst diagnosis to date, Borderline Personality Disorder (BPD) also known as Emotionally Unstable Personality Disorder (EUPD). When I was discharged from this unit 4 months later, I was labelled with this horrible illness that since has taken what normal life I had left away from me.
During this ‘free’ time, I lived in a shared house for people with mental illnesses and learning disabilities, where I made friends and began to become re-accustomed to what can only be described as ‘civilian life’. However once again, after being discharged, I barely managed Christmas and New Year before being re-admitted to my local psychiatric unit. This was preceded by a number of trips to A&E and being placed on numerous 136 Sections by Police. Once again I was placed on a Section 3 and I ended up back in the system that I whole heartedly detest. By this crisis point, my mental health became worse that ever with my symptoms increasing as one of my symptoms is to cease taking medications as I detest thinking that I need them. I was back on 1:1 with a bedroom with only a mattress and pillow and spent weeks in rip-proof clothing for my own safety. However, after a month it was deemed that the ward I was on was not suitable for my needs and that I would soon be moved to an Open Rehabilitation Centre. This placement would be one that is considerably longer than any i had pre This was one of the scariest moments for me as I was informed that the unit I would be moving to is a 4 hour drive from my hometown and subsequently wouldn't be seeing my friends or family that often.
Despite having a very tricky move, from being handcuffed by police, to travelling in the back of an ambulance with restraints on, I arrived at my new unit in March 2018. However as I was so ill, my brain has erased a number of memories from my first few months here. I went from a shy, timid schoolgirl to what can only be described as a ‘vocal, distressed, patient’. I was being injected on an almost daily basis with sedatives and I was being threatened with a move to another PICU (Psychiatric Intensive Care Unit). However after regaining some strength and getting my eating disorder to a decent stage of physical health, I began what really I can call my journey to recovery. This journey would be by no means easy or short and I would have to face a number of problems such as Depression and Anxiety, BPD, PTSD and atypical Anorexia Nervosa. Since then, I have had a number of relapses and stages that I thought that I would never recover from but I now know I'm at least in the right place for treatment.
However, even though I am now on the path to good health I have also had to fight my corner to be heard sometimes with regards to my illnesses. Since the age of 16, i have struggled with unexplained aches and pains, as well as extreme fatigue that doesn't improve with rest. This when coupled with other symptoms such as migraines is known as “Chronic Fatigue Syndrome’. I had known that I have CFS for a number of months before I received a diagnosis of it as my current consultant just blamed medication and its side effects, so after a long battle I managed to get my voice heard and explain my side of the story.
Chronic Fatigue Syndrome effects me in a lot of different ways, but the main problem i face is extreme fatigue that is worsened by any sort of exercise and does not improve with any amount of sleep. I can rest all day and sleep more than 12 hours a night and still wake up with my body feeling like lead. My joints ache for no apparent reason and once again are worsened by exercise.
In late September, i had my Section 3 renewed for another 6 months which now means I will spend Christmas here in hospital but I will visit my family on Boxing Day hopefully. It is now November and I have been in rehab for nearly 9 months but I must say they've been the most productive 9 months of my life. I really feel like I am finally improving, yes I may be taking numerous medications and having psychology on a nearly daily basis along with occupational therapy but I feel like I am improving and also becoming more independent. Hopefully I will continue to look positively at my journey and keep you up to date in the meantime…
4 notes
·
View notes
Text
Back to School with Diabetes Amidst the COVID-19 Variants – Diabetes Daily
New Post has been published on https://depression-md.com/back-to-school-with-diabetes-amidst-the-covid-19-variants-diabetes-daily/
Back to School with Diabetes Amidst the COVID-19 Variants – Diabetes Daily

This content originally appeared on Beyond Type 1. Republished with permission.
By Lala Jackson
This article was published on August 13, 2021. As of Monday, August 23, the FDA has granted the Pfizer and BioNTech COVID-19 vaccine full approval for ages 16 and up, with the Emergency Use Authorization (EUA) still in effect for ages 12-15 and for booster doses for immunocompromised individuals. Full approval for other COVID-19 vaccines currently under EUA is expected soon.
While hopes were high that we could head back to school for the 2021 school year as though we were closer to “normal,” the development of COVID-19 variants amidst low vaccination rates has thrown a wrench in plans. But when kids need to get back to in-person schooling for quality of life, quality of learning, and socialization, how can we best keep them safe?
To help answer this and other questions about going back to school safely, JDRF—in collaboration with American Diabetes Association and Sansum Diabetes Research Institute—hosted a conversation with doctors and experts from the CDC, ADA, and the Fairfax County Health Department (Virginia).
Moderator Dr. Kristin Castorino, senior research physician at Sansum Diabetes Research Institute, kicked off the event with the most pressing question—is it even safe for students and their teachers who have diabetes to return to in person schooling, particularly for those under 12 who cannot be vaccinated yet?
“I’d change the question from ‘is it safe?’ to ‘is it appropriate?’ and I think it is,” answered Dr. Fran Kaufman, pediatric endocrinologist and chief medical officer at Senseonics. “There aren’t known answers as things change… but we need to get our kids back to school, not only for learning but for socialization.”
Dr. Kaufman stressed that the best way to make school safe is for everyone who can get vaccinated to do so. Dr. Christa-Marie Singleton, MD, MPH, senior medical advisor at the CDC later elaborated, “Vaccines protect folks against serious symptoms, hospitalization, and death. The best way to protect ourselves, our families, and our youngest people is for the adults and kids over the age of 12 around them to get vaccinated.”
“We also know about the importance of masking,” continued Dr. Kaufman. “It’s important to follow the CDC’s recommendation that all children and adults should be masked in the indoor school environment.”
What About the Legal Rights of Kids With Diabetes?
Particularly as some states ban school districts from being able to require masks in indoor learning environments, what legal protections do kids with diabetes have to stay safe in school? Crystal Woodward, MPS, director of the ADA’s Safe at School campaign, stressed “the rights of students with diabetes do not go away during a pandemic. They have legal protections under federal and state laws. Those accommodations may look a little different, but they do not go away.”
Similarly to how the Americans with Disabilities Act protects people with diabetes in the workplace, section 504 of The Rehabilitation Act protects the education of children with disabilities like diabetes. This law allows children with diabetes and their families to create what are known as 504 plans, which clearly outline agreed upon accommodations for students with disabilities at school.
While parents cannot dictate the actions of other students, they can include directives for their own children to stay safer from COVID-19 in 504 Plans, like instructions that their student must always wear a mask or will need extra physical distance in a classroom setting.
“It’s imperative that [children with diabetes] have a section 504 plan,” Crystal explained. “Everyone needs to be clear on what accommodations will be provided and by whom, like the student having the ability to take an exam at an alternate time if blood glucose levels are out of range during the scheduled test time.” Ensuring the student also knows what is in their own 504 plan can help them feel more empowered and comfortable asking for what they need.
For distance learning, 504 plans can dictate that children with diabetes can take snack or meal breaks at times best for the student, or have an agreed upon communication method with the teacher if the student needs to take a break to attend to a low or high blood sugar.
“Bottom line: the rights of students do not go away,” Crystal reiterated. “Students with diabetes and their families should work with schools and everyone needs to understand their role and responsibilities, and the plan should be updated as needed. It’s always better to get it in writing. Put the 504 plan in place while everything is going well—you never know if a principal or a nurse or a teacher is going to be there throughout the year.” Panel members stressed that families who don’t speak English, particularly in public schools, have a legal right to translators who can help establish 504 plans.
Jacqueline McManemin, RN, BSN, certified diabetes education and care specialist (CDECS) and assistant nurse manager for the health services division of Fairfax County Health Department in Virginia, spoke about what they’re continuing to do in their school district (one of the 15 largest in the nation) to keep students safe. “Parents should expect to see much of the same precautions this year that were in place last year. Particularly when students are inside, they should be masked.”
School administrators across the country can work to make schools more safe for all children, particularly those with chronic illnesses like asthma and diabetes, by putting in protective measures like establishing two different health clinics—one for people exhibiting symptoms of COVID-19 or other communicable illnesses and a separate clinic for routine care and injury treatment. Meals can be eaten outside as weather permits and student interaction in hallways can be minimized by teachers rotating between classrooms rather than groups of students switching classrooms every period. Protocol also needs to be clearly communicated with all staff and parents about what to do if a student starts showing symptoms of COVID-19 while at school.
Getting Kids Mentally Ready for in-Person School
Back to school doesn’t just mean a change of location, it’s a change in schedules, types of interaction and stimulation, and levels of distraction that can also impact diabetes care. Psychologist Cynthia E. Muñoz, PhD, MPH, assistant professor of clinical pediatrics at the University of Southern California’s Keck School of Medicine and president of healthcare and education for the American Diabetes Association, reminded the community that the impact of the pandemic on each individual has been unique and therefore approaches to regain a sense of normalcy must be unique too.
“For parents and guardians, be aware of how you’ve been impacted. Seek support, through family, through primary care, through a therapist. Find ways to talk about your fears or concerns,” encouraged Dr. Muñoz. She went on to suggest ways to get kids mentally and physically ready for school again.
“Now that schools are starting to open, it’s time to start looking at sleep schedules, screen time, and start shifting routines and schedules to get children ready for the new routine,” she noted. “Many people watch a lot of content on social media or television—not just kids, everyone—but it’s a passive interaction with others. Shifting to a more active form of communication with others can be another way to help people ease into the change of a lot more interaction than people have had in the last year or so.”
Helping Kids Who Feel Singled Out
Kids with diabetes often deal with feelings of being the odd kid out, having to visit the school nurse, having to deal with special routines. When COVID-19 is added, kids with diabetes may feel like they’re the only ones taking special precautions, which can be additionally isolating. How can parents help children dealing with these feelings?
“I like to approach this question around the concept of support, building layers of support around the student,” Dr. Muñoz explained. “One level should be ensuring that someone at the school should know that the child has diabetes and knows what kind of support they need. Another category is who could know [the student has diabetes], but doesn’t necessarily have to, like friends. For the student with diabetes, getting support from a friend or classmate they trust could go a long way. If the student feels like they’re going to be the only one wearing a mask, they can ask a friend to wear it with them.”
“I think it’s important for adults to be sensitive to this,” Dr. Muñoz continued. “Saying “everyone has something different” might minimize how a student feels. Acknowledging their feelings and taking the time to ask them what will help goes a long way.”
To get advice from other parents and guardians or to help your student with diabetes find other kids who understand, be sure to join the Beyond Type 1 community.
Learn more about the JDRF – Beyond Type 1 Alliance here.
You Can Watch the Entire Conversation Here:
youtube
Post Views:
4
Read more about American Diabetes Association (ADA), COVID-19, diabetes at school, Diabetes Research Institute (DRI), eversense, Intensive management, JDRF, kids with diabetes, pfizer, school.
window.fbAsyncInit = function () //Initialize the Facebook JavaScript SDK FB.init( appId: '8485090309', //App ID from the app dashboard channelUrl: 'http://www.diabetesdaily.com/channel.php', //Channel file for x-domain communication status: true, //Check Facebook Login status xfbml: true //Look for social plugins on the page );
//Logged In Users FB.getLoginStatus(function (response) if (response.status !== "unknown") ga('set', 'dimension1', 'Logged In'); );
//Facebook Likes FB.Event.subscribe('edge.create', function (href, widget) var currentPage = jQuery(document).attr('title'); ga('send', 'hitType': 'social', 'socialNetwork': 'Facebook', 'socialAction': 'Like', 'socialTarget': href, 'page': currentPage ); );
//Facebook Unlikes FB.Event.subscribe('edge.remove', function (href, widget) var currentPage = jQuery(document).attr('title'); ga('send', 'hitType': 'social', 'socialNetwork': 'Facebook', 'socialAction': 'Unlike', 'socialTarget': href, 'page': currentPage,
); );
//Facebook Send/Share FB.Event.subscribe('message.send', function (href, widget) var currentPage = jQuery(document).attr('title'); ga('send', 'hitType': 'social', 'socialNetwork': 'Facebook', 'socialAction': 'Send', 'socialTarget': href, 'page': currentPage ); );
//Facebook Comments FB.Event.subscribe('comment.create', function (href, widget) var currentPage = jQuery(document).attr('title'); ga('send', 'hitType': 'social', 'socialNetwork': 'Facebook', 'socialAction': 'Comment', 'socialTarget': href, 'page': currentPage ); ); ;
//Load the SDK asynchronously (function (d, s, id) var js, fjs = d.getElementsByTagName(s)[0]; if (d.getElementById(id)) return; js = d.createElement(s); js.id = id; js.src = "https://connect.facebook.net/en_GB/all.js"; fjs.parentNode.insertBefore(js, fjs); (document, 'script', 'facebook-jssdk'));
Source link
0 notes
Text
Mental Health Is Equally Important As Physical Health

Mental health involves your emotional, social and psychological wellbeing. It impacts how you feel, think and act in your regular lives. Your capacity to manage stress, emotions, the way of socialising with people, and also making decisions are highly determined by your psychological or mental health. If you have any mental disorder, you must have its best treatment under expert care. Dr Anil Yadav is the best neuropsychiatrist in Gurgaon and the top psychiatrist in Delhi. His rehabilitation centre in Gurgaon and Delhi provides high-quality treatment for various mental health issues that may harm physical wellbeing too. Read below about the different ways how improper mental state can affect your physical health.
Mental health can impact your physical wellbeing
You must realise how your body and mind are connected. Like physical pain can weaken your mental state, leading to depression, anxiety, stress, etc., the opposite also happens. Mental health issues can deteriorate your physical state. For instance, with chronic depression and anxiety, you might find it difficult to sleep, risking your physical health.
Mental health impacts one’s financial stability
You might not understand how mental fitness is linked to financial stability as the impact is not as obvious as for physical health. Those who suffer from untreated mental weakness, earn much less than those who’re mentally fit. Mental health issues like depression destroy one’s productivity. This then affects sufficient income. Besides, if you have mental disabilities, you will more possibly take medical leaves more often. Even while working, you may fail to focus fully on your work. Thus, all such problems can destabilise your financial state.
Your mental state can impact your family
If you have mental illnesses, your kids will tend to experience a higher risk for neglect, abuse and also several behavioural and emotional problems. These children usually find no one to turn to, thereby isolating themselves from others. These effects can eventually follow into adulthood and they may grow up as adults suffering from mental health problems of their own. If you undergo mental weakness, your family will share the consequences of your stress, job loss, financial strain and more. For this, recovery for the whole family is sometimes recommended so that all can heal to move on.
Untreated, extreme mental disorder or instability may become dangerous
Untreated mental disorders and their relation to violent crimes are matters of debate nowadays. Alcohol or drug abuse becomes a risk factor for those possessing mental diseases already to suffer further. However, a more significant concern involves how victims of mental health issues are generally prone to violent crime as well. While research is still being performed to ascertain the connection between untreated, chronic mental disorders and violence, patients of such issues unluckily become the victims of maltreatment or abuse.
Sound mental health can lead to a happier and longer life
You must learn that your mental state can impact your overall life expectancy. So take care of your mental health by exercising regularly, practising yoga and meditation, avoiding alcohol, cigarettes and drugs and, finding more reasons for smiling and being happy every day. Besides, whenever you find any symptoms of a mental health issue bothering you, seek the best treatment as soon as possible to prevent it from affecting your life.
#TopPsychiatristInDelhi#Best psychiatrist in Delhi#BestNeuropsychiatristindelhi#Bestpsychiatristindelhi#best Psychiatrist in Gurgaon
0 notes
Last Seen Blogs

enzo-bi-tbdl
Enzo-bi-TBDL
sperandiopeggy
Untitled

nicolequeenlover
Queen & NostalgiaCore

snow-angel-16
all.i.do.is.cry
cinephile-inc
the theater is my home away from home