#transfiormation
Text
30th post
Hello, y'all! Not much to report on this post, I'm still alive, I'm pretty happy still, I'm still very much enjoying spiderman 2, and for the sake of my one friend who doesn't want spoilers, I will not spoil anything in it
the only really necessary updates I guess are that I've been getting better at driving, which is pretty fucking awesome, and that some of the new transfiormer figures that are coming out within the next year look pretty fucking awesome too! and on top of that transformers news, the old transformers games coming to xbox game pass and a new game coming out within the next year are some pretty fucking great news, in my opinion!
aside from that, that's it. doing well mentally, still talking to my friends whom I care deeply about (love you guys, I know at least one of you is reading this), hanging out with in person friends as much as I can, and I try to talk to my crush friend, I guess is the best way to put it, as much as I can cause she's so awesome.
now that's it, lol. Remember to drink plenty of water, get plenty of sun, and eat well and plenty. Remember to love yourself as you love others, and I wish you love and laughter always! stay safe!
0 notes
Text
LGBT - How To Prepare For Your H.R.T. Meeting

SO YOUR SEEKING HORMONE REPLACEMENT THERAPY:
WHY?
Why do you want to seek hormone replacement therapy? What is the underlying cause to have you seek transformation? Is it because you’re sexually disadvantaged? A victim of abuse? A patient suffering from dysphoria of the body? Or have you been socially conditioned to alter your appearance? Knowing why is a must! Because 50% of those who undergo H.R.T. truly need it and 50% of those who undergo H.R.T. end up regretting it.
SEEK EDUCATION
Once you know why you want to undergo H.R.T.; you need to educate yourself about the benefits and risks of H.R.T..
If you are reading this article, then it is likely that you are in phase two and seeking education. Sadly, many (including myself) do not feel conformable bringing up this subject in public and have a difficult time doing the research online. There is so many ‘bad’ articles out there. Opinionated articles written by with pro-LGBT or anti-LGBT groups to push a narrative or agenda, using salacious data or failing to address the risks, both physiologically and psychologically to the patient.
If you can...talk to you Primary Care Physician or a center that specializes in LGBT services and ask for resources to make your own decision. Write articles, take notes, talk to your closes friends about the risks and benefits of H.R.T. and why you want to undergo this dramatic transition.
WHAT NEXT?
Prior to the clinical appointment with a physician, it is totally natural to feel nervous, anxious, excited, ambivalent, scared or all of there emotions all at once. When I was waiting, I felt all these emotions...I felt bipolar when it comes to the altering range of emotions.
One moment I am nervous (Will I be given the injection hormone? Or pills?), then anxious (time, place, money and open mindedness). Excited (I can’t believe I actually am doing this!), ambivalent (I pray this isn’t a phase...hate to ask my PCP for breast reduction!), scared (What if they deny me, or I take on too many female characteristics? Will my parents actually kill me if I beginning looking like a woman in two to six years? What will my friends think of me?).
One feeling I would add and that is: doubt
For 33 years I danced with doubt, and the last four months have been our grand ballroom dance. Even before I hear what they think, I already begun doubting myself, mostly because I realized that being on estrogen meant my transition was real, physical changes will happen and people will notice. No more hiding, no more Illuminati-like secrets...they will see and my brain will change as my testosterone levels are replaced with estrogen.
Even though I am scared, nothing will kept me from my appointment...I have been working my way to this point...it will be the greatest scientific experiment I will ever conduct...a second puberty occurring on my own body...I will document it to the tee. This might be a capstone in biological transformation that I’ve written and drawled so many times. I always placed myself in my characters shoes, but never could say what it was truly like...so now I will know!
The night after the call I kept thinking of all the things I was going to ask the doctor. Things the doctor might ask of me. HRT is like a transplant...if you are not mentally prepared, you will reject it! I ran simulation after simulation of different ways the appointment might go and my mind goes blank and the representative of me is left mumbling uh and um and yeah. I wanted to prevent this from happening, so I wrote down a few simulations. Sometimes it is better to have a list of questions prior to going into your appointment so you are collected and ready. It is also a great way to judge the doctor to see if they are the right one...remember...they are the one rebirthing you to your second birth!
PREPARING FOR DAY ONE:
Here are three areas to focus on during the first appointment...
1) To assess the providers knowledge and comfort with the different forms of treatment being oral, epidermal or endodermis.
2) To go over side effects and what to expect from starting on estrogen. This is a good way to see if the doctor knows the risks and emotional effects at which stage.
3) And to begin building a relationship with a healthcare provider that hopefully will be based on trust and openness.
It is important to be able to assess the provider’s knowledge and comfort because you want someone that can properly screen for any health issues that may be a problem in the future (I.e. heart trouble, cancer, blood clots and stroke).
Since I am Gender Neutral (closely related to Gender Fluid), it would be in my best interest to communicate with the provider that there are some things I am looking to physically change (I.e., breasts, fat distribution around the hips and butt, feminine features in the face and hair growth decrease on chest with halting male pattern baldness on head), but others that I wish to remain the same (I.e., penis, male facial features and muscular support that I have).
Lastly, having a provider that is up-to-date with the different types of dosing and methods to administer hormones is always helpful because then you are given options, options are extremely important when it comes to hormone therapy because a certain method may work well for one person, but not so well for another. (as seen in Operation B.O. H.R.T.)
SAMPLE QUESTIONS FOR PROVIDER:
So, when learning about the provider, questions that may help you assess their knowledge and comfort are as follows:
What methods do you give as options when prescribing hormones to your patients?
1a) Current options for estrogen, antiandrogens include: injectable, sublingual or oral, and transdermal.
1b) 17-beta estradiol (estradiol) is most commonly delivered to transgender women via a transdermal patch, oral or sublingual tablet, or injection of a conjugated ester (estradiol valerate or estradiol cypionate). No outcome studies have been conducted on injectable estradiol valerate or cypionate, presumably due to their uncommon modern use outside of transgender care settings; due to this limited use manufacturers have little incentive to produce this medicine, and shortages have been reported. Other delivery routes for estradiol such as transdermal gel or spray are formulated for the treatment of menopausal vasomotor symptoms and while convenient and effective in some transgender women, in others these routes may not be able to achieve blood levels in the physiologic female range. Compounded topical creams and gels also exist from specialty pharmacies; if these are to be used it is recommended that the prescriber consult with the compounding pharmacist to understand the specific details and dosing of the individual preparation. Compounded estradiol valerate or cypionate for injection also exists, and may be an alternative in times of shortage or more cost effective for those who must pay cash for their prescriptions.
Conjugated equine estrogens (Premarin®) have been used in the past but are not recommended for a number of reasons, including inability to accurately measure blood levels and some suggestion of increased thrombogenicity and cardiovascular risk. Equine estrogens are obtained from the urine of pregnant, catheterized horses; no evidence exists to suggest that these estrogens are superior to bioidentical human estradiol.
Ethinyl estradiol is a synthetic estrogen used in contraceptive preparations and is associated with an increased thrombotic risk. In the context of contraception, ethinyl estradiol has more consistent and reliable cycle control and as such is better tolerated, balancing out the potentially increased risk of VTE. In the setting of gender affirmation there is no need for cycle or bleeding regulation, and thus the use of ethinyl estradiol and its inherent risks are not warranted.
General Side effects of estrogens may include migraines, mood swings, hot flashes, and weight gain.
Spironolactone is the most commonly used androgen blocker in the U.S. Spironolactone is a potassium sparing diuretic, which in higher doses also has direct anti-androgen receptor activity as well as a suppressive effect on testosterone synthesis. Doses of 200mg daily in non-transgender women being treated for hair loss have been described as safe, though doses of up to 400mg/day have been reported without negative effect. Hyperkalemia is the most serious risk but is very uncommon when precaution is taken to avoid use in individuals with renal insufficiency, and use with caution and frequent monitoring in those on ACE inhibitor or ARB type medications. Due to its diuretic effect, patients may experience self-limited polyuria, polydipsia, or orthostasis.
5-alpha reductase inhibitors include finasteride and dutasteride. Finasteride blocks 5-alpha reductase type 2 and 3 mediated conversion of testosterone to the potent androgen dihydrotestosterone. Finasteride 1mg daily is FDA-approved for male pattern baldness, while the 5mg dose is approved for management of prostatic hypertrophy. Dutasteride 0.5mg more effectively blocks the type 1 isozyme, which is present in the pilosebaceous unit and therefore may have more dramatic feminizing effects. Since these medications block neither the production nor action of testosterone, their antiandrogen effect is less than that encountered with full blockade. 5-alpha reductase inhibitors may be a good choice for those unable to tolerate, or with contraindications to the use of spironolactone. 5-alpha reductase inhibitors may also be an option for use as a single agent in patients seeking partial feminization, or for those who continue to exhibit virilized features or hair loss after complete androgen blockade or orchiectomy.
1c)
Hormone Low Dose Medium Dose Maximum Dose
Comments
Estradiol oral/sublingual
1mg/dat 2-4mg/day 8mg/day if >2mg
Recommended divided bid dosing
Estradioltransdermal
50mcg 100mcg 100-400mcg
Max single patch dose available is 100mcg. Frequency of change is brand/product dependent. More than 2 patches at a time may be cumbersome for patient.
Estradiol valerate IMa
<20mg 2wk 20mg 2wk 40mg 2wk
May divide dose into weekly injections for cyclical symptoms.
Estradiol cypionate IM
<2mg 2wk 2mg 2wk 5mg 2wk
May divide dose into weekly injections for cyclical symptoms.
Spironolactone
25mg qd 50mg bid 200mg bid
N/A
Finasterride
1mg qd N/A 5mg qd
N/A
Dutasteride
N/A N/A 0.5mg qd
N/A
Are you familiar with the different methods and doses used? Are you open to trying different methods/doses?
2a) The answers to these questions will let you know how open your provider is, and also how knowledgeable they are regarding advances and new forms of treatment in transgender healthcare.
How many transgender clients do you currently work with?
3a) If you are the first, second, or third, you are most likely going to be learning together. If you are with a provider of over 20, 30 or 100, then they most likely are more experienced.
Do you follow the most up-to-date and current guidelines for transgender care?
4a) Although the World Professional Association of Transgender Health is not the only organization that provides Standards of Care, they are the most well-known. WPATH SOCv.7. is the old model. ICATH is the modern model.
Do they know other providers in different areas of transgender health in case you need a referral for specific care?
5a) You may have some health complications that require monitoring by a specialist. Or in the future you may require specialist care for something (it doesn’t have to be trans related) so having other provider’s names is always helpful. If your current provider has a trans-friendly referral list it may also be a sign that they are more knowledgeable and connected.
Questions to ask about hormones:
What are the side effects?
1a) If there are things they go over that causes you concern, ask for more information.
How will hormone therapy affected my fertility/reproductive options?
2a) If you are considering or would like the option of having (biological) kids in the future, then being informed of options and also risks with being on hormones therapy is something you should consider.
What is the general timeline for seeing changes?
3a) The World Professional Association for Transgender Health (WPATH) has a general timeline that can show you the expected changes as noted below:
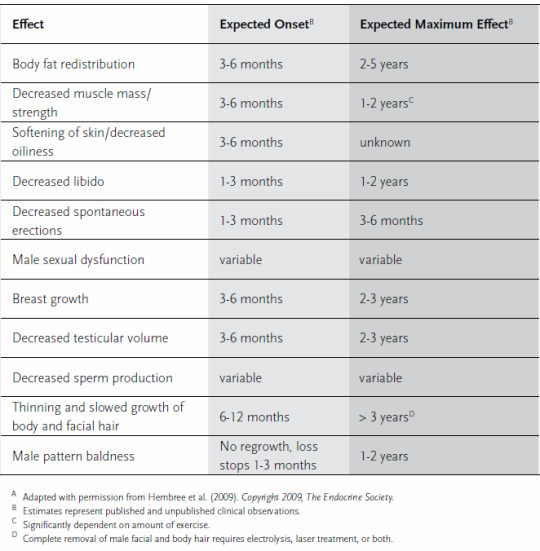
Body Fat Redistribution
3-6 months to show 2-5 years to finalize
Decreased Muscle Mass/Strength
3-6 months to show 1-2 years to finalize
Softening Of Skin/Decreased Oiliness
3-6 months to show Unknown
Decreased Libido
1-3 months to show 1-2 years to finalize
Decreased Spontaneous Erections
1-3 months to show 3-6 months to finalize
Male Sexual Dysfunction
Variable Variable
Breast Growth
3-6 months to show 2-3 years to finalize
Decreased Testicular Volume
3-6 months to show 2-3 years to finalize
Decreased Sperm Production
Variable Variable
Thinning And Slowed Growth Of Body And Facial Hair
6-12 months to show > 3 years to finalize
Male Pattern Baldness
No Regrowth, loss stops 1-3 months 1-2 years to finalize
QUESTIONS TO BUILD A RELATIONSHIP WITH THE PROVIDER:
What questions do they have for you?
1a) Question they ask may bring up more things that you wanted to ask them, but hadn’t thought of before.
Finally, if you are ready and feel good about your relationship with the provider then ask,
When can I get started!?
#gender nonconforming#transgender#gender bender#gender transformation#gender#non-conforming#nonconforming#nonbinary#transfiormation#transformation#trans#tg#lgbtq#lgbtqa#lgbtpride#lgbtq community#lgbt#body#body dysphoria#dysphoric#dystopia#estradiol#advocacy#advocate#mtf hrt#ftm hrt#hrt#ipath#wpath#cedarriverclinics
169 notes
·
View notes
Text

“The only freak without a human heart around here is you, Stuart Litt I CANT FINISH THIS POIST I HYATE MY FRINEDS STUART LITTLE IS A FREAK WITHOUT A HUMAN HEART
#⬛️⬜️ ❝HI I’M N AND WELCOME TO *STUFFING LEAVES IN HIS MOUTH*❞ ⬜️⬛️﹙SHITPOST ZONE﹚#IM LOSING MY GOD DAMN MIND#I SENT THAT LONG-ASS POST ABOUT N GOING TO HELL AT THE END OF BW#THE VERY SWERIOUS AND EMOTIONAL ONE#TO MY GC WITH MY FRIENDS AND IN THREE MINUTE S#IN THREE MOINUTES IT TRANSFIORMED INTO STUART LITTLE IS A FREAK WITHOUT A HUMAN HEART
8 notes
·
View notes
Text
Новости сайта #ENGINEERING - 工程
New Post has been published on http://engineer.city/am-helps-hand-powered-cyclists-make-history/
AM helps hand-powered cyclists make history
At the World Human Powered Speed Challenge at Battle Mountain, Nevada, USA, Paralympian Karen Darke, MBE and Ken Talbot broke world records for both male and female arm powered speed. By reaching 46.05 mph and 51.86 mph respectively, Darke and Talbot are now the first and second fastest hand cyclists in history. The records were achieved using a bike created through the ARION4 project run by the University of Liverpool Velocipede Team (ULV Team), with the support and expertise of engineering companies such as Renishaw.
As part of the ARION4 project to build the bike, Renishaw additively manufactured the central titanium support (CTS), a vital component of the bike that attaches to the headtube to hold the layshaft and front wheel in place. The component is the backbone of the ARION4 transmission system, allowing riders to put in as much power as possible without worrying about the structural integrity of the front of the bike.
"This record is the culmination of two years hard work by our engineering students”, explained Steven Bode, Senior Lecturer at the University of Liverpool’s School of Engineering and the project's Lead Academic. “Their combined passion for engineering and pushing the limits of human potential have resulted in the success of the ARION4 riders, Karen Darke, MBE and Ken Talbot. I’d also personally like to thank all of our sponsors, as without their support the Arion project would not exist.”
“We are starting to see the benefits of additive manufacturing being taken advantage of in high-speed applications, from the Bloodhound Supersonic Car to the TransFIORmers MotoGP bike,” explained Llyr Jones, Mechanical Engineer at Renishaw. “When aiming to reach high speeds, small technical enhancements can have a large impact. The design freedom of metal 3D printing ensured a crucial component of the bike was strong and light enough to meet the conditions of the race.”
Tags:
additive manufacturing solutions
Images:
Categories:
Design
Materials/Processes
Source: engineerlive.com
0 notes
Text
New Post has been published on Fetish Q&A
New Post has been published on Fetish Q&A
Anyone into transfiormation fetish??
why is it so hard to find ppl who r into TF??
#fetish #fetishism #kink
http://www.fetishqa.com/anyone-into-transfiormation-fetish/
0 notes
Text
THE DANGERS OF H.R.T. - MONITORING, TITRATION & DANGERS
-- My Transgender Journey
As with any therapy program, there is the inherent risk and dangers associated when trying to change and balance the chemistry inside the body. H.R.T. as seen in Male-to-Female transformation is poorly documented and still considered ‘not evidence based’, meaning the variables are unknown between patient to patient. Everything presented is considered as reference range. Titration of estrogen is driven by not medical evidence, but solely by the patients individual goals.
As with any drug, the elevation of dose greatly increases the probability of side effects. Personal habits (I.e. smoking and drinking or poor diet) can lead to severe medical complications. Mental stress can lead to depression and acts of suicide. Family history of ovarian, uterine and breast cancer can lead to an increase of cancer cells forming in the body. However, some with low PSA from prostate cancer can improve their condition using both estrogen and antiandrogen.
A general approach for titration would include increasing both estrogen and antiandrogen dosing until the estrogen dose is within the normal female physiologic range. Once this has been achieved, titration efforts can focus on increasing androgen blockade. There are two widely used approaches to titration of androgens:
Increase estrogen until it reaches the upper limit of the female physiologic range,
Maintain current physiologic estrogen dosing and titration upward on antiandrogens and/or addition of a progestogen.
For example:
A Transgender woman taking 4mg/day divided dose oral estradiol, 100-200mg/day divided dose of spironolactone found that all MtF patients achieved physiologic estradiol levels, though only 2 out of 3 of the MtF patients achieved female range testosterone levels.
For example:
A Gender-Nonconforming patient may prefer to maintain estradiol or testosterone levels in an intermediate range with a dose titration upward over 3-6 months. Recheck estradiol and testosterone levels at 3-6 months and titrate again.
Once hormone levels have reached the target range for a specific patient, it is reasonable to monitor hormone levels yearly, or only as needed.
Other reasons for measuring hormone levels in the maintenance phase include watching for metabolic shifts such as diabetes or thyroid disorder. Substantial weight changes, hot flashes or migraines might be a warning sign that the dose level is too high for the body chemistry.
One of the biggest issues with measuring and monitoring hormone levels is the lab.
For example:
A MtF transgender woman who is still registered as male will result in lab reference ranges reported for a biological male and not a transitioning female. Hormone levels for Gender Nonconforming/Nonbinary patients may intentionally lie in the mid-range between male and female norms.
The Monitoring Of Estradiol Levels
There is no evidence that higher estradiol levels in patients with adequate androgen suppression results in additional feminization or breast development. Maintaining estrogen levels in the physiologic range for MtF minimizes risks and side effects, and makes sense clinically. Note that the use of conjugated estrogens (Premarin®) or ethinyl estradiol (found in most combined oral contraceptives) are not accurately measured by estradiol assays and will typically result in low measured levels and should be avoided as they can increase the risk for cancer, DVT and heart disease.
In patients who have been using self-administered conjugated estrogens, or ethinyl estradiol, it is reasonable to check a total estrogens level, which may provide a more accurate estimate in these cases.
Monitoring Testosterone Levels
Testosterone levels can be very difficult to measure in MtF due to rapid fluctuations in levels, relating to pulsatile release of gonadotropins, with higher levels in the morning hours. Free testosterone represents the portion of testosterone unbound to serum proteins and depends on levels of sex hormone binding globulin (SHBG). While free testosterone can be measured, they are unreliable. Bioavailable testosterone is free testosterone plus testosterone weakly bound to albumin. SHBG is elevated in the presence of estrogen, and in particular with exogenous estrogen supplementation, more so with oral estrogen than with parenteral routes due to first pass hepatic activity.
For transgender care, The Endocrine Society recommends monitoring of the total testosterone level, with a target range of <55ng/dl. A general reference range for bioavailable testosterone is >72ng/dl (2.5nmol/L).
Monitoring Gonadotropin Levels
When indicated, measuring of gonadotropins (leutenizing hormone: LH and follicle stimulating hormone: FSH) can be done using the local lab ranges for eugonadal state as a reference.
Individualized Dosing Based On Patient Centered Goals
Some patients (like Gender Neutral) may desire limited hormone effects or a mix of masculine and feminine sex characteristics. Examples include retention of erectile function with otherwise maximum feminization, or minimal feminizing effects with the exception of body or facial hair elimination or breast growth. While manipulation of dosing regimens and choice of medication can allow patients to achieve this goal, it is important to have a clear discussion with patients regarding expectations and unknowns. Specifically, it is not possible to select in advance an exact hormone regimen that will predictably allow patients to arrive at a specified configuration of sex characteristics. Furthermore, individual genetic and physiologic variation can result in wide variations in both blood levels and response to therapy between different individuals using the same route and dose.
The best approach in these cases is to start with low doses and advance slowly, titrating to effect. At the same time, response to hormone therapy is also individualized and measures such as breast growth are variable in both degree and time course. Likely predictive factors of speed and degree of feminization include genetics, age at initiation of therapy, and body habitus. Patients should be counseled on typical time frames for changes and advised to avoid making comparisons to the experiences of others.
Anecdotal sources suggest that maximal feminization may occur within 2-5 years.
Specific considerations and conditions with H.R.T.
Loss of erectile function:
Sildenafil (Viagra) and tadalafil (Cialis) can be used for preservation of erectile function at any stage or with any feminizing hormone regimen, in consideration of the typical contraindications and precautions when using this class of medication. Individual results may vary. It is reasonable check both total and bioavailable testosterone levels, and consider reduction of androgen blockade to allow an increase in testosterone, depending on patient goals.
Low libido:
A study of sexual desire in transgender women found that 83% never or rarely experience spontaneous sexual desire, 76% never or rarely experience responsive sexual desire, and 22% meet the criteria for Hypoactive Sexual Desire Disorder (HSDD) by experiencing both of these in a way which results in personal or relational distress.
This study found no correlation between sexual desire and testosterone levels in the transgender women, though a significant correlation was found between hormones and desire in non-transgender women.
Pituitary adenoma (prolactinoma) and galactorrhea:
Prolactin elevations and growth of pituitary prolactinomas are theoretical risks associated with estrogen therapy; several cases have been reported. However, with the administration of physiologic doses of estrogen, there is no clear basis for an increased risk of prolactinomas in comparison to the population background rate in non-transgender women.
It is noted that some transgender women experience a minimal amount of galactorrhea early in their hormone therapy course. The presence of non-bloody minimal galactorrhea from more than one duct and/or bilateral is almost certainly physiologic and would not warrant further evaluation.
Venous thromboembolism:
Insufficient evidence exists to definitively guide estrogen therapy in transgender women with risk factors or with a personal history of prior VTE, either on or off estrogen. A report of 11 transgender women with a history of activated protein C resistance (the mechanism of action implicated in the hypercoaguable state associated with the Factor-V Lieden mutation) using transdermal estradiol without anticoagulation found no clotting events after a mean of 64 months of therapy.
Autoimmunity:
There is a certain but incompletely defined linkage between sex hormones and autoimmune conditions. Testosterone has been associated with overall immune suppression, and autoimmune conditions are more common in non-transgender women than men.
Patients with autoimmune conditions should be informed that their condition could potentially worsen (or improve) once feminizing therapy has begun. Hormone dosing should begin low and advance slowly, monitoring for worsening symptoms, and in collaboration with any specialists who may be managing the autoimmune condition.
Migraine:
Migraines have a clear hormonal component and may be exacerbated by estrogen therapy. Patients with a history of migraines should consider starting with a low dose and titrating upward as tolerated.
Mental health conditions:
While hormones may contribute to mood disorders (such as in premenstrual dysphoric disorder or postpartum depression), there is no clear evidence that estrogen therapy is directly associated with the onset of or worsening of mental health conditions. In fact one study found that transgender women experience improvements in social functioning and reduced anxiety and depression once estrogen therapy is begun. Mental health conditions in transgender women should be approached with a broad differential diagnosis as in any other patient. It may be advisable to avoid injected estrogen due to the potentially cyclic levels, which could bring about or worsen existing mood symptoms.
Cancer
For patients with a prior history of estrogen sensitive cancer (breast, pituitary), consultation with an oncologist is recommended. While androgen deprivation is a mainstay of treatment for advanced prostate cancer, it is unclear if estrogen therapy may confer an independent protection or increased risk of prostate cancer. mPSA should be considered unreliable in those using antiandrogen or estrogen therapy due to the high risk of false negative tests.
#gender nonconforming#transgender#gender bender#gender transformation#gender#transfiormation#transformation#trans#hormonereplacement#dysphoric#hormone replacement therapy#hormone replacement treatment#hormone#lgbtq#lgbtqa#lgbtpride#lgbtq community#lgbt#nonbinary#non-conforming#nonconforming#gender fluid#genderfluid#mtf hrt#tf#mtf#risk#disease#danger of hrt
5 notes
·
View notes
Text
MtF H.R.T. ~ To Many Unknowns
One of the hardest lesson’s I have discovered with hormone replacement therapy is to remain committed.
Before I go one; this isn’t very common for most MtF H.R.T. patients. Typically they are driven, but when you live in an area that isn’t friendly to LGBT individuals, it is hard to remain committed.
Second, my health isn’t the best as I’ve been in and out of the hospital and I have begun to wonder ‘Is This Therapy Making My Breathing Worse?’ I asked the doctor at Cedar River Clinic if he knew any case of peoples asthma getting worse, but he did not know.
With nearly a month spent in the hospital, now I need to evaluate my decision if MtF H.R.T. is really good for me. Ironically, even though I’ve been off my meds for almost a month...my measurements and remain quite level.
Like any ‘life-changing’ event, you need to evaluate the situation and then go forth and I’ve decided that I will continue as my body is already ‘in-between’ and I need to balance my body and spirit.
#genderfluid#gender bender#gender transformation#transgender#gender#Social structure#trans#transformation#transfiormation#lgbtq community#LGBTQA#lgbtq#lgbt#hormone replacement treatment#Dysphoric#body dysphoria#hormone replacement therapy#hormone#maletofemale#male to female#mtf hrt#HRT#tg#hormonereplacement#lgbtpride#replacement#Cedar River Clinics#hospital#hospitalization#asthma
2 notes
·
View notes
Text
Don’t Go To Walgreen's
If you are a trans-patient...DON’T GO TO WALGREEN’S!
I had many choices of pharmacies in my area and chose Walgreen’s Pharmacy to supply my meds. I have ran into many problems with Walgreen’s that are:
Don’t have all medicine in stock...
Unable to supply your full dose...
Unfriendly pharmacist...
Not Trans-friendly...
Question why you are taking the medicine over and over...
No public privacy...
I spoke with Cedar River physician about Walgreen’s and was informed that many patients have had a bad encounter with the staff retaliating against the patient for them being Trans.
I have switched over to Rite Aid to see how they handle my scripts and found that they have the medicine in stock, the pharmacist does not ask why you are taking these meds (but will ask if you want pharmacist to talk about your meds) and appear trans-friendly.
#gender nonconforming#transgender#gender bender#gender transformation#gender#nonconforming#gender fluid#genderfluid#transfiormation#transformation#trans#hrt#male to female#maletofemale#cedar river clinics#cedarriverclinics#walgreens#rite aid#estradiol#lgbtq#lgbtqa#lgbtpride#lgbtq community#lgbt#tg#hormone#hormone replacement treatment#hormone replacement therapy#hormonereplacement
2 notes
·
View notes
Text
LGBT - CALLING AN H.R.T. CLINIC

My Transgender Journey
February was supposed to be the month I was looking forward to:
‘Call on the first, get the earliest appointment. Come prepared and prepare to live out my dream!’
However, 26 days went by and I played a cruel game of gamble. I had time to think deep about my decisions, weigh the consequences and dwell the many possibilities. I kept telling myself:
‘H.R.T. can’t switch your gender, it is DNA! All I would be doing is putting on organic prosthetic’s.’
I wanted this to go away, I wanted to forget that I ever looked at the possibility to transform my body into half-female half-male! The story of my life! On the 24th of February, I came close to dialing, but it was Saturday and I never call on Saturday to businesses. I did whatever I had to do to run away, I wasn’t confined to dwell in my thoughts and device...hell, it was snowing and that was the biggest distraction I could ever have! By the 26th of February, fate took a cruel turn as my cystic fibrosis landed my ass in the hospital and I thought to myself:
‘Nowhere to run, nowhere to hide...call the number and let’s get this over with...’
But I made up some lame excuse and by the time I had a change of heart, it was too late! They were closed!
The 27th dawned on a crummy day to match my crummy health...I was suffering...really sick! Virus is killing me, and I wish it was John Malkovich! By 1pm, I landed in bed, miserable and depressed. I took a shower and saw my body because my body failed me and made standing nearly impossible! I looked at my AA-cup breasts...a gift from odd biology and years on prednisone. I looked at my skin and thought:
‘If I was on H.R.T. these breasts would form correctly...they look like shield volcanoes of Hawaii! I might also have to shave only once a week instead every other day! How that would be nice!’
I closed my hospital room door thinking:
‘I am terrified of my parents...I can never do this at home! This is the best and worst time to do this!’
Back in bed before I kiss the floor, I take out my tablet and cellphone and find the number to Cedar River Clinics. I take a deep breath and punch in the numbers and shake my head thinking:
‘Do this and there is no turning back. Don’t do it and regret it forever! They will know my deepest secret and desires...maybe they can help me and put me on the correct path…’
Hit send, I can’t believe I am going through with the plan. I just pray no nurse walks in on my conversation! The phone cuts immediately to a receptionist and she sounds nice and helpful.
“Thank you for calling Cedar River Clinics, my name is Destiny, how may I assist you?”
“Hi Destiny, my name is David and I am calling in regard to setting up an appointment for H.R.T.” I say as I am calm and collective...last time I called I was stumbling over my words and incoherent.
“The hormone replacement therapy?” Destiny asks as she wonders if I am calling for an honest procedure or inquiry. Her voice still friendly.
“That is correct, H.R.T...” I say as Destiny goes through her files, hearing them crackle over the phone.
“Looks like the next opening is in April...” she says as she collects her thoughts. “It will be at the Tacoma office.”
My stomach does a flip flop and the words can’t come out. I am terrified! I force myself to reply. “Which day in April?” I ask as every last word is projected on breathless lips, sounding like: Which day in Apri....?
“The 12th.” she says to my joy. I have nothing on the 12th and my mom will be at work! Secrecy upheld!
“That will work!” I say, the last word barely squeaking out.
“It is at 8:30am in Tacoma...after the first appointment, you can choose your own clinic...”
“Tacoma works well!” I reply quickly, I had hoped to go to Tacoma as it was close to home and I will get to know the doctor taking care of me.
“So you want to schedule for that appointment?” she asks softly and cheerfully. I know that the next words will place me on the path.
“Yes please!” I say, matching her attitude. I swear my voice changed and my demeanor altered to something that is not me…it was a flutter!
“Okay David...” there is a pause as if she made a cardinal sin. “I am sorry, I should have asked, do you have a female name you go by?”
I choke up...I did not think this out all the way! I was not expecting this type of personal questions. What do I say? Think quickly! I am in anguish, one does not pick their name in a flash!
A name spoke to me in my female voice saying: Tell her Mira! Tell her that your name is Mira!
I love the name Mira; the word almost slipped out. It means so much to my character...it was my secret name…
(Mira is a feminine given name with varying meanings. In the Romance languages, it is related to the Latin words for ‘wonder’ and 'wonderful.’ In South Slavic languages, it means ‘peace’ and is often used as part of a longer name, such as Miroslava (masculine form: Miroslav). In Albanian language, it means ‘goodness’ or ‘kindness’. In Sanskrit, it means ‘ocean’, ‘sea’, ‘limit’ or ‘boundary’. In Hebrew, it is a derivative of Miriam or the female equivalent of Meir, meaning ‘light’.)
Mira was all of me, a daughter of wonder and peace as my soul is at peace in her form. Also meaning goodness and kindness which is a testimony to my charity and civil service. And lastly, the one from the sea...another one of my deep ocean secrets.
I hesitate as I stop myself and I am sure now that Destiny thinks I am a fraud! “Just David at this time, I am still deciding on the name aspect.” my brutal honesty coming out. “Any other name would be dangerous in this hostile society...” as my brain says:
‘Shut up, you already made yourself sound like a fool!’
“It is totally understandable David, do you prefer going by sir?” she asks.
I can hear Admiral Gial Ackbar yelling ‘It’s a Trap!’ in my head. That is exactly what it was, a trap to assess my commitment to the therapy. “Just sir please.” my animus chimes in and I hate myself. I am neither, but I’ve never vocally told anyone that before. “For the time being…”
“Okay David,” her tone changed, not angry, just unsure of my call. Most who call either are in transition or know what they want to become, “Typically transgender individuals change their name for legal reasons like new licenses and bank records...” she rambles on as it goes over my head.
‘Oh! You screwed up big time!’ my brain mocks me. It takes in delight knowing it was right. I can’t believe Destiny is still on the line with me. I must sound really new at this and she probably wonders why now? “Okay David, I just need an address...” and I chime off my home code.
When it comes to saying my town, she laughs as the name is rather musical, like a gay French ‘la-la’. I sigh a breath of relief as I feel I am recovering from probably the easiest question to answer...your female name! “And a phone number.” she asks and I give my cell...best to have no one calling home, that would be suicide!
Coming to the end, my nerves are a wreck! “For your patient records, please provide us a pin...”
“How long?” I ask.
“As long as you want it...” she says kindly.
“Letters or numbers?” I ask.
“Anything you want...” she say, annoyed, but being polite!
“Okay, my pin is four numbers, 1…9…8…0” I say, easy to remember.
“Wonderful, now onto the appointment. We ask that you fast for 10 hours prior to your appointment” being 11:30pm on the 11th...perfect time! “And drink plenty of water! But no coffee.”
“Copy that!” I confirm.
“That will give your body time to regulate your hormone levels for the appointment...” I gulp, that means that needles will be involved! “It is important that you don’t eat for ten hours!” she emphasizes again, meaning that this rule has been broken hundreds of times before! Luckily for me, EPI would make eating before travel...messy! “I am going to transfer you over to billing, thank you for calling David and we look forward to seeing you on the 12th.”
“Thank you Destiny.” I reply as the line clicks and a minute passes and the line is answered. I gulp, this is what I truly fear...the price!
“Is this David I am talking to?” the woman asks. Her vocal tones annoy me...she paints a vivid image of Roz from Monsters Inc.!
“This is David.” I confirm, praying it isn’t over 500.00 dollars...I can’t afford that. I also don’t want my insurance in deep with them. It is odd how diagnosis’s end up in the strangest places. For example, I went to the Kitsap Mental Health clinic trying to find a way to cut my student debt by declaring myself autistic, which I am, and somehow that ended up at St. Anthony Hospital on my records!
“Hello...David.” she says, failing to give me her name. I pictures her saying: ‘Hello...boys’, so Roz It is! “The quoted cost for the appointment is 270.00 dollars, unless you have insurance.”
“I have Medicare-Medicaid...” I say as I give my Provider One number.
“How odd...” she growls in her slug tongue. “I don’t see Medicaid only Medicare and we don’t take that here!”
I won’t be deterrent, “I’ll pay the fee.” I say. My thoughts are:
270.00 for clinic and labs. A follow up appointment to read results will be an additional 170.00 and hopefully they can run my scripts through Medicare at a pharmacy of my choosing. Hell, if I can pick them up there, better! Cut out the middle man!
But if I pick up my meds at clinic, first, all TG patients can only go on Thursdays for privacy and second, I will be held accountable...no turning back...they expect me to go through a full transformation!
#gender nonconforming#transgender#gender bender#gender transformation#gender#transfiormation#transformation#trans#mtf hrt#mtf#tf#lgbtq#lgbtqa#lgbtpride#lgbtq community#lgbt#hormonereplacement#sex reassignment surgery#hormone replacement therapy#hormone replacement treatment#replacement#dysphoric#hormone#cedarriverclinics#cedar river clinics#tacoma#washington#non-conforming#nonconforming#coming out
0 notes
Text
LGBT - Needing A Social Structure
Needing A Social Structure-- My Transgender Journey
45 days have passed ever since I made the life changing call to Cedar River Clinics of Tacoma. 45 seems to be a major number for me:
45 is my life expectancy,
45 is the current President of the United States,
45 is the time of a football match period and,
45 is the atomic number of rhodium.
Between day 1 and day 45, I somehow repaired the damage between Ruth and I. I had to take the bullet and bow down to her and claim the fault as mine. It was not easy to do when you think you are in the right. Even though we did not meet face to face as I was hoping so, IMing from Facebook seemed like the best option.
I was terrified to even respond as I did not know what she would say, think or do. She might tell her mom and dad whom I respect and they will not see me for the person I am. She might tell my sister or mother about our talk and I already know their stance on the LGBTQ.
I decided that since we were no longer a couple, this might be a easy way to dealing with the stress and guilt of my actions 7 months ago. This was also a major point in my development as being Mira...the proverbial 'Coming out of the Closet' sort of speak; even though I despise the concept as I have not been in the closet!
For a few moments, I hit the keys on my tablet and sent a inquiry message with a general response to her asking if she could come over for a visit. After awhile, we began writing back-an-forward with comments, ideas, concerns and general social interaction via a computer device.
Ruth wrote an inquiry question as she asks: ‘Are you still in a nothing phase these days? I've been Snape a lot lately. Carlo and River figure prominently as well, and Agatha is back. Now that I'm off the meds that were suppressing my nightmares, I'm back to dreaming about murder like my friend the freaky bald lady.’ she writes as it harks back to out playtime as I lived out our lives in characters. Most of Ruth's characters were male and most of mine were female.
‘I have been going through some 'issues' that I've been trying to sort through personally...hard to explain as I don't know what people will think... otherwise, it's been a fog! Murder dreams...that is a nightmare!’ I respond, wanting to jump into the conversation, but too scared to do so.
‘Oh, I understand issues. You can tell me if you want, but no pressure.’ Ruth says as it hearkens to the time when she helped me through my Asperger's phase.
‘I was hoping to take your council in the issue at hand, just been scared of the repercussions...also scared to even admit a truth I've wondered about.’ I say, not really revealing much as my mind tries to debate over how much to say and reveal.
‘Yes, I'm all too familiar with that. I will treat anything you tell me as confidential. I won't even tell my family.’ she says in confidence...maybe two years ago I would have been more trusting, but I am unsure.
‘For seven months (half of the reason I have not written and been silent), I've been researching and dissecting a probability that I know my family will not accept, so I will be frank as I am still considering. As you know, we share in playing characters and even shape our lives around them (as you noted with Snape and Carlos), I too share in the activity as a way to ease a stress. But with research in my body image, mental health and lifestyles since I was a child, I think I might have a problem...many of my character names go much deeper than a name to a fictional character, most are attempts at understand the strong anima persona that I can't shake...I hope this makes sense, struggling as I totally understand it.’ I state as I take the long way around to explain my mental process so I don't seem that I am just blurting out a random phase.
‘I think I understand. Are you referring to the Roman concept of duality of Anima and Animus?’ she asks.
I shake my head, I am not talking about the Romans, I am talking about much later scholarly work, ‘I've written three articles trying to rationalize it, but the answer terrifies me. To deny it is to deny what I know is true and to hide it only makes it worse. Yes...it is my way to understand my situation, from Carl Jung's research on the male and female aspects of the human nature.’ I state, revealing my source.
‘That's right, Jung did a lot of work on that concept.’ she says.
‘Nevertheless, my conclusion is quite simple: I am out of balance. For a seven months I have been wondering how to correct it.’ even though I wanted to write:
I am out of balance, so I decided to take hormone therapy to partly feminize my body.
but even thinking like that sounds so wrong! I would be feminizing my body...I am trying to heal it!
Ruth certainly does not understand what I am saying, ‘I'm not sure I know the answer to that. Although my body is female, my soul feels as though it is simultaneously male and female, and as you know, I am attracted to both males and females. The way I see it, being female in flesh and pretending to be male characters is my way of maintaining the balance of my soul. I'm not quite sure how to help you, because I don't know what is normal for you.’ she states, wondering if my complications fall into the LGBTQ without referring to that label as the label bothers me.
‘That was near the conclusion I got to! I have learned that the soul is neither male nor female, but both at once (Animus and Anima), the Animus I can see as that is the persona of David, but the Anima is also there. I know its name and the knowledge has left me unbalanced physically. To live by the life of my Animus, I believe it contributes to most of my situations with relationship and deeper relationship since the left side of the brain is not programmed for these feelings. When I live through my Anima, it helps create bonds in relationship and creativity, but to do so is dangerous regarding my family's stance on the idea. You should know, being male was not my original ideal gender...it was Gender Neutral, it is living by this rule that has me bothered as I am compelled to correct the balance of my body. Please don't think of me wrongly, I thought I could convince myself I was either suffering a phase or guilty that I can't be romantic...sorry I am beating around the bush, I imagine this conversation with you, seeking your council, but do to my upbringing, it is harder than I thought.’ I finally say, finally revealing that I think I am Gender Neutral, LGBTQ, and that it is responsible for my inability to be comfortable with myself to be comfortable with others.
‘Oh, I completely understand. I have suspected for some time that you are asexual, and I was conducting some rather rash and insensitive experiments of my own to test the theory. For that I apologize, and you have my full support and my utmost compassion. I figured that telling me this would be difficult. I recognized the roundabout speech patterns as anxiety. You have nothing to apologize for or feel guilty about. You are who you are, and there is nothing wrong with that.’ she states as I am speechless. A mixture of disappointment, anger, frustration and joy fill my emotions as I wonder what would make her think I was asexual! However, it was the admission that she has been running experiments on me that angered me the most...but then, so have I as I tested her autism to learn about the disease. Even though she says I have nothing to feel guilty about, I am totally guilty for being this way and some could say that I am trying to atone for my sins.
‘I am glad...well with the easy part out of the way, now comes to my conclusion in Article 3...both article 1-2 looked at my possibly falling in the class of LGBT. Many of my mental imaging confirmed that being male was wrong, but also being female was wrong. The idea of hybridization between the two listed me as being Gender Nonbinary, which makes sense.’ I write, taking the long way around again. Even when I write out LGBTQ, I purposely leave out the 'Q' as it is offensive to me. I know that she has never read these article's I've written, but it helps validate my research and makes me feel 'not crazy!'
‘I would agree with that assessment. Once again, you have my full support, and I won't tell your family or mine. Hmm, maybe I should go look up what gender nonbinary is. Looks like I'm gender nonbinary, too, just at the opposite end of the spectrum!’ she states, a rather welcoming surprise to know something she does not...but also concerning to me. I have typed out a full admission to the H.R.T. program and worked out editing the text as I just still am unable to admit that I desire to mature my breasts and take on 'female' characteristics. I had to hang up as I was being discharged from the hospital and when I got home, I had to be extra careful around my family.
‘Sorry I didn't get back, just got home!’ I write, not so sound as if I blew her off.
‘Woohoo! I wondered if that might have been the case!’ she writes, sounding concerned that something might have prevented me from talking to her. Being home, I changed gears and reflected on the August 2017 trip. I wanted to tell her that she hurt me and I was upset with her behavior, but that sounded too harsh and I threaded lightly.
‘Thank you for being up front and willing to hear me out, I was concerned with our last outing which in my opinion was a nightmare that I’ve thought over and over that we would not have the same type of trust as we built over 10 years. I need to apologize for my inexcusable behavior last August, it was shameful to treat you like that.’ I state, being as diplomatic as possible.
‘Thank you. I just blamed the whole thing on the Prednisone. Yes, I was hurt by it, but I also saw that were both going through a hard time, and between my medication change and your Prednisone, it's no wonder things got tense.’ she rationalized. It was certainly true, prednisone certainly played a role in my anger...but it wasn't the chief problem!
‘It was just so much happening at once that I did not think my actions out. Sadly, been on prednisone so long, but they just took me off, trying to put me on a cancer drug called methotrexate to control my breathing.’ I say, verifying her ideas, but adding hope for an improvement.
‘Wow, that's pretty cool. I hope it works!’ she adds, apparently knowing nothing about methotrexate. It is a terrible drug!
‘Exactly, I will admit, I was very angry for a few months...but with time and reflection, it came to past. Although, I advise shorter trips next time until we can work out a plan to survive the longer ones.’ I state as I reflect on the trip...it was fun...but also a nightmare!
‘I concur. We learned to avoid each other's minefields back in college, but they have both expanded in the current political climate. The good thing is that we now know where the new minefields are.’ she states, referring to her hatred for President Trump, whereas I am quite loyal to his administration!
‘Exactly! The irony is that I broke my one rule for relationships: No politics, no religion no money! I just got overwhelmed with being attack by my friends for my political views that all I was doing was yelling at a closed door...I just don’t get people!’ I state, growing tired of this conversation.
‘As for me, I made a blunder in that I didn't realize I had pushed you to shutdown mode. If I'd known that, I would have backed off and given you the space you needed. I apologize for that. It's another cruel irony of autism that we are unable to see things from other people's perspectives, even when we try.’ she states as I just shake my head. She is half-right, on the last two days of the trip...I needed my space and I needed her to know not to push my buttons, but she was so self-centered to see her error. Even when I tried to walk away or hide in my tent...it did not help the situation as she played the 'victim card’.
‘It is okay...for years we wondered what an argument would look like and never could fathom it! I never told my folks about that event...they would have killed me for what I did! Well, knowledge is good...hopefully with this self-awareness issue coming to a maximum...might make it easy...I have not been the most compassionate and my family and friends make it clear!’ I comment as I try to wrap up this emotional conversation.
‘Once again, I understand, and I think that the awareness of ourselves and our differences is already helping. It's amazing how quickly trust can be torn down, and even more amazing how quickly it can be rebuilt.’ she wrote as I had no 'kind' response. In my family, trust takes years to build and seconds to destroy and once gone...it remains gone!
Even though we repaired our relationship and Ruth became the first person to witness my 'coming out', it is hard to see us ever being a couple again.
#transfiormation#transgender#transformation#trans#gender transformation#gender nonconforming#gender bender#gender#mtf#tf#nonconforming#non-conforming#genderfluid#gender fluid#relationship#love#family#social#social structure#social struggle#lgbtq#lgbtqa#lgbtpride#lgbtq community#lgbt#bender#tg#hrt#hormone replacement treatment#hormone
0 notes
Last Seen Blogs

ignite-theflame-dahling-blog
Amber Flame

olotypography
OLO Typography

bigramp504
Big ramp Enterprises

kunstdiary
Kunst Diary

wowright-art
Doodles and Stuff?!