#endothelium
Text
Staunch Supporters
Bacterial toxins can compromise blood vessels' leakiness affecting blood pressure. This study reveals that blood vessel lining cells' membranes, under the control of proteins called caveolin-1 and cavin1, stiffen to regulate the leakiness via tunnels called transendothelial cell macroapertures
Read the published the research article here
Video from work by Camille Morel and colleagues
Institut Pasteur, Université Paris Cité, CNRS UMR6047, Inserm U1306, Unité des Toxines Bactériennes, Département de Microbiologie, Paris, France
Video originally published with a Creative Commons Attribution 4.0 International (CC BY 4.0)
Published in eLife, March 2024
You can also follow BPoD on Instagram, Twitter and Facebook
23 notes
·
View notes
Photo

endothelium
8 notes
·
View notes
Text
Ladyboy seduced by future boss big cock fucking and cumshot
NOVINHA BRINCANDO COM AS TETINHAS ESCONDIDA
Ebony Goddess Sarai Minx Interracial Breeding
Slave gay sex stories free xxx Jamie Gets Brutally Barebacked
Sex stories camp young gay boy Levi is hungry for dick, the gifted
Skinny polish teen Lina sex
Sexy Latina Fucked In an Orgy
Bubble butt Julianna Vega takes money to make love
Desi boy Cum in car with gf
Girl stands in doggie and feels schlong fucking her from behind
#dermatomyces#call-over#lotase#Lamprey#intimado#amphibious#duckish#amrev#undefilable#green-boled#caffa#orthoplastic#rough-tongued#top-piece#lawyer's#Suwannee#Ayurvedic#endothelium#mnemonic's#Knickerbocker
0 notes
Note
You're 25 have some shame
i am 25 so at least my pre-frontal cortex is fully developed unlike yours :)
anyway i'm learning about anti-platelet and anti-coagulant drugs in school right now. and i'm gonna use your anon to brain dump everything i know so that some actual use can come from the three seconds of my life i wasted reading this. okay so from my understanding when there is an injury that causes bleeding the injured endothelial cells release endothelium which promotes vasoconstriction of the smooth muscle cells to prevent blood loss. they also secrete von willebrand factors which bind to the collagen that the endothelial cells reveal underneath them. the platelets are just zooming by in our blood but they stop and bind to the von willebrand factors via their gpIb receptor, this binding also leads to a localized effect. this causes platelet activation and degranulation of thrombin, serotonin, thromboxane A2, and ADP. the thrombin binds to the PAR-1 receptor on the surface of the cell and further promotes platelet activation. TXA2 promotes vasoconstriction and helps promote the activation of the GP2B3A receptor. ADP can bind to either the P2Y1 or P2Y12 receptors, when it binds to P2Y1 it causes an increases in intracellular calcium. when it binds to P2Y12 it leads to a breakdown of cAMP via phosphodiesterase which eventually can lead to the activation of the GP2B3A receptor on the surface of the cell. the fibrinogen is able to bind to the GP2B3A receptor and then be converted into fibrin in order to start the linkage and meshwork surrounding the platelets. and then you have the whole coagulation cascade going on that i don't feel like explaining right now. you have COX-1 inhibitors like aspirin which irreversibly inhibit, via acetylation, the COX-1 enzyme that produces TXA2 so those levels will decrease leading to less vasoconstriction and less activation of the GP2B3A receptor. aspirin has adverse SE like GI issues like ulcers because in inhibiting COX-1 it's preventing COX-1 from producing PGE2 which helps protecting the stomach lining from the stomach acid. aspirin "allergies" work similarly, you can have bronchospams because PGE2 promotes bronchodilation. another class of anti-platelets would be P2Y12 inhibitors. your first-line would be clopidogrel, however, there is some genetic variability in how patient's react to it because it is a pro-drug. other pro-drugs that are irreversible inhibitors are prasugrel and ticlopidine, the latter is specifically not a first-line because it has an adverse effect of causing neutropenia. a P2Y12 ihibitor that is not a pro-drug and is reversible is ticagrelor. all four of these drugs have a rare SE of TTP. You also have PDE inhibitors that prevent phosphodiesterase from breaking down cAMP which would prevent the expression of the GP2B3A receptor. those are cilostazol and dipyridamole, the latter of which is on the beer's list and should not be prescribed to the elderly because there is an increase fall risk associated with it due to it cause orthostatic hypotension. there's also GP2B3A inhibitors that are only administered IV in hospitals because they have short-term effects so that means they are reversible; they are also used when patients are allergic to P2Y12 inhibitors. lastly, you have par-1 inhibitors like vorapaxor that prevent thrombin from binding to the par-1 inhibitor which will decrease platelet activation. and that's all i got because i don't feel like talking about anti-coagulation drugs right now.
#my brain feels full#i have so much studying to do#like whats the point of this anon hate#you gave me zero context lmaooooo#anyway i hope you learned something!!#rip i had a typo it's endothelium and endothelial cells!!!!
9 notes
·
View notes
Text
fam im STUDYING this isn’t fun
#ooc : give me a second I need to get my story straight#((tunica intima tunica media tunica adventitia))#((vascular endothelium + internal elastic membrane -> non-striated myocytes + elastic lamellae + external elastic membrane-> d.i. connective#((it's the summer and i am memorizing tubes))
3 notes
·
View notes
Text
10 Surprising Health Benefits of Eating Dark Chocolate
Introduction:
Dark chocolate is not only a tasty treat, but it also has a variety of health benefits that may surprise you. From improving heart health to boosting brain function, there are many reasons to indulge in a bit of dark chocolate every day. In this article, we’ll explore the top 10 health benefits of dark chocolate, backed by scientific research and expert opinions.
Top 10 Benefits of…

View On WordPress
#added sugars#antioxidant status#antioxidants#blood pressure#brain function#cocoa#cognitive functions#coronary vasomotion#dark chocolate#dietary intake#endothelium-dependent vasodilation#Exercise#flavanols#health benefits#healthy diet#healthy treat#heart health#high-quality brands#hypertension#insulin resistance#lipid metabolism#lipid profile#minimal processing#moderate intensity cycling#organic cocoa beans#platelet reactivity#scientific research#type 2 diabetes#visual functions#weight loss
0 notes
Text
Difference Between Endothelium and Epithelium
The main difference between epithelium and endothelium is that the epithelial cells usually line the pathway that opens into the external environment i.e, the respiratory system or digestive tract. On the other hand, endothelial cells line the closed pathways like those of the vascular system.
0 notes
Photo

Endothelium by Vincenzo Lamolinara
This artist on Instagram
546 notes
·
View notes
Text
the question
what is the difference between a machine and an angel?
ask gabriel, judge of hell, and he'll say, soul.
what is the difference between a machine and an angel?
ask gabriel, apostate of hate, and he may not answer you.
for machine and angel are not so different. both are creatures with metal skin to hide and hold their fleshy, bloody selves. organs churn, gorgeous tunica externa, media, interna of rubber and flesh, twist and wind like rope choking the throat of the nonbelievers, endothelium, venous valve of copper direct precious blood to power the chassis, the body, of life. both must fight to keep their life from spilling out onto the floor. to lose, even once, is death. both yield weapons to do it. both think, move, kill. the better question then, is this:
what happens to an angel who loses its soul?
#ultrakill#gabriel ultrakill#v1 ultrakill#my writing#ficlet#im having thoughts about 'we all bleed the same' and machines being full of flesh again#check the rbs for the ao3 link
44 notes
·
View notes
Text
Human and rodent placentation is hemochorial, the fetomaternal interaction between the two blood circulations involving direct physical interaction between maternal blood and the chorionic trophoblasts.
The mechanism by which cells are exchanged across the placental barrier is unclear. Possible explanations include deportation of trophoblasts, microtraumatic rupture of the placental blood channels or that specific cell types are capable of adhesion to the trophoblasts of the walls of the fetal blood channels and migration through the placental barrier created by the trophoblasts. Intervillous thrombi containing mixed maternal and fetal cells occur in the fetal placenta/labyrinth.44,45 Histological defects in the continuity of the trophoblasts lining the vasculature of the placenta are also reported.46,47 Together these observations suggest the possibility that fetomaternal hemorrhage within the fetal placenta/labyrinth may allow exchange of cells between the fetal and maternal circulation. Microtraumatic dislodgment of trophoblasts from the trophoblast-lined blood channels through which the maternal blood passes may also explain why trophoblasts appear in maternal circulation. The microtraumatic hypothesis of cell exchange does not appear consistent with the hypothesis that fetomaternal microchimerism may be of adaptive value to the fetus but fits well with the hypothesis that fetomaternal microchimerism is an epiphenomenon of pregnancy with potential pathological consequences.
An alternative hypothesis is that cells cross the placental barrier by mechanisms akin to the active adhesion and transmigration that occurs across high endothelial venule (HEV) endothelium in peripheral lymph nodes and at the blood-brain barrier (BBB).48 Intriguingly, in the mouse at least some of the fetal cells that enter the mother are also capable of crossing the blood brain barrier into the brain.35,49
Fetomaternal microchimerism appears to occur with great frequency following human pregnancy. It has been suggested that fetomaternal traffic occurs in all pregancies.14 Moreover fetal cells are reported to persist in the mother for decades. Male cells have been found in maternal blood even decades after pregnancy,7,77 including in one case in which the women was last pregnant with a male child 27 years earlier.7 Fetal cells also may persist for even longer after engrafting maternal bone marrow14 and perhaps other organs. By engrafting into niches such as the bone marrow, fetal cells may also be able to proliferate and reinfiltrate blood or other tissues later. There is strong evidence that fetal cells with the characteristics of mesenchymal cells do engraft the bone marrow. Male DNA was detected in 48% of CD34-enriched apheresis products from nonpregnant female marrow donors.1 Male cells were also detected in all bone marrow samples from women who had previously been pregnant with males, including one woman who was last pregnant with a son 51 years earlier.14
The absence of Y chromosome markers in samples from women who had never born sons in some studies14 strongly supports the argument that the male cells observed originate from the fetus. However, it is important to note that there are crucial caveats in the use of the Y chromosome alone as a marker for fetomaternal microchimerism that may have led to over estimation of the incidence and persistence of fetomaternal microchimerism in humans. Male cells have been found in the blood of women without sons.78,79 Male cells may occur in the blood of as many as 8–10% of healthy women without sons and no known history of abortion.79 It has been speculated that the male cells arise from unrecognized spontaneous abortions, vanished male twins, an older brother transferred by the maternal circulation, or sexual intercourse. However, a history of unrecognized spontaneous abortions or sexual intercourse cannot explain all cases of the presence of male cells in females as another study detected the presence of the Y chromosome in normal liver from seven of eleven female fetuses and five of six female children.80 Such microchimerism may be best explained, by fetofetal transfer from an undetected vanishing male twin or maternofetal transfer of male cells harbored by the mother. Estimates of the frequency of vanishing twins range from 3.7–100% of pregnancies81 however not all twins share connected placenta vasculature, especially at the early stages of development at which many twins disappear. Maternofetal transfer to the mother may also have occurred if the mother's mother had a history of blood transfusion, transplantation or previous pregnancy with a male fetus. It is difficult to estimate how frequently male cells in females could arise as a result of fetofetal or maternofetal transfer. Although one might expect such events to be rare, the incidence may be high enough to have biased estimates of the incidence of fetomaternal microchimerism in humans. While the possibility that the Y chromosome could also enter the mother via microchimerism as a consequence of previous blood transfusion or transplantation has been considered in most studies, the possibility that male cells detected in the mother may have arrived via fetofetal or maternofetal transfer to the mother in utero has not be systematically excluded. Conclusive proof of fetomaternal microchimerism in humans would require the use of other paternal markers that differentiate between the father of the fetus and the father of the mother. One scenario might be to investigate cases where the mother and the mother's father share a genetic mutation or polymorphism not carried by the father of the fetus. In such cases, evidence of genetic markers derived from the father of the fetus in the mother could provide more conclusive evidence of fetomaternal microchimerism in humans. If the genetic mutation or polymorphism caused disease the presence of fetal cells in the diseased tissue could also offer evidence of the potential of fetomaternal tissue repair.
37 notes
·
View notes
Photo
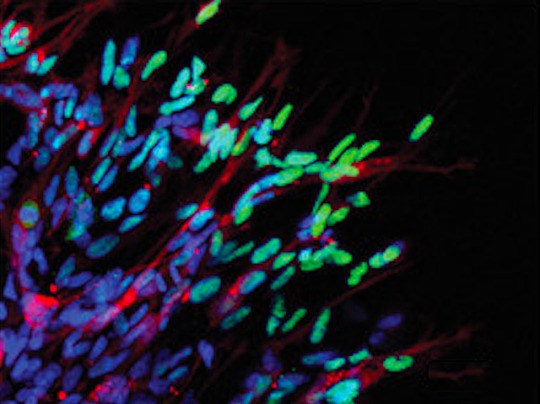
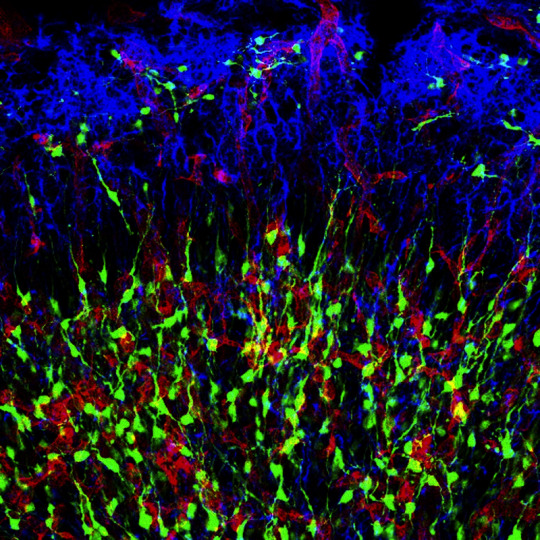
No Safe Haven
Like a city’s sewers safely harbouring the monster’s eggs at the climax of a disaster film, primed for chaos in the inevitable sequel, there’s a cosy nook inside certain tumours where a pool of cancerous stem cells lurk, refuelling the cancer even after initial treatment. In glioblastomas, aggressive brain cancers, the perivascular niche is this safe haven. Past research has been unable to pinpoint how cells of the niche support the stem cells, but researchers have developed a new platform for testing. Their model includes lining cells (endothelium) and neural support cells (astrocytes). In experiments, all three cell types flourished, and the stem cells (red) released characteristic markers of activity (green), showing the platform was a useful proxy for real-world tumours. Further study showed the endothelial cells and astrocytes boosted cancer stem cell invasiveness and persistence, and showed the platform’s potential for deeper interrogation and future treatment development.
Written by Anthony Lewis
Image from work by Emmanuela A. Adjei-Sowah and colleagues
School of Biological and Health Systems Engineering, Arizona State University, Tempe, AZ, USA
Image originally published with a Creative Commons Attribution 4.0 International (CC BY 4.0)
Published in Advanced Science, May 2022
You can also follow BPoD on Instagram, Twitter and Facebook
#science#biomedicine#cancer stem cells#stem cells#cancer#tumours#oncology#glioblastoma#endothelium#astrocytes#neuroscience#immunofluorescence
13 notes
·
View notes
Text
Me actually writing a fanfic on ao3? I’d never.
Anyways this is the link to it :D
#Apollo#hyacinthus#apollo and hyacinthus#hyacinthus x apollo#apollo x hyacinthus#fanfic#ao3 fanfic#first ao3 fanfic?! WOAH!
14 notes
·
View notes
Text
Propaganda!
The endothelium is a single layer of squamous endothelial cells that line the interior surface of blood vessels and lymphatic vessels. The endothelium forms an interface between circulating blood or lymph in the lumen and the rest of the vessel wall. Endothelial cells form the barrier between vessels and tissue and control the flow of substances and fluid into and out of a tissue.
A progenitor cell is a biological cell that can differentiate into a specific cell type. Stem cells and progenitor cells have this ability in common. However, stem cells are less specified than progenitor cells. Progenitor cells can only differentiate into their "target" cell type. The most important difference between stem cells and progenitor cells is that stem cells can replicate indefinitely, whereas progenitor cells can divide only a limited number of times.
32 notes
·
View notes
Text
Lumen
-- the lumen is the central opening of a blood vessel
-- the lumen is surrounded by a wall of three layers
Layers:
Tunica Intima
-- inner layer facing the blood
-- inntermost layer is the endothelium
-- the endothelium is simple squamous epithelium
-- the endothelium is surrounded by connective tissue
Tunica Media
-- the middle layer
-- made of smooth muscle
-- has some elastic fibers
Tunica Adventitia
-- the outer layer
-- made of connective tissue
#medblr#studyblr#notes#my notes#medical notes#med notes#medblr notes#anatomy and physiology#anatomy#physiology#anatomy notes#physiology notes
15 notes
·
View notes
Text
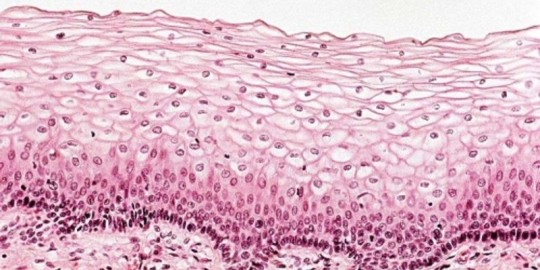
The Different Types of Epithelial Tissue
Epithelial tissue can be classified into several types based on its structure and function. Here are some of the different kinds of epithelial tissue:
Simple Squamous Epithelium:
Features a single layer of flattened cells.
Found in areas where diffusion and filtration occur, such as the lining of blood vessels (endothelium) and air sacs of the lungs (alveoli).
Simple Cuboidal Epithelium:
Consists of a single layer of cube-shaped cells.
Found in areas involved in secretion and absorption, such as kidney tubules and glands.
Simple Columnar Epithelium:
Composed of a single layer of column-shaped cells.
May contain specialized cells, such as goblet cells that secrete mucus.
Found in the lining of the digestive tract, where it aids in absorption and secretion.
Pseudostratified Columnar Epithelium:
Appears stratified but is actually a single layer of cells of varying heights.
Often contains cilia and goblet cells.
Found in the respiratory tract, where it helps in moving mucus and trapping foreign particles.
Stratified Squamous Epithelium:
Comprises multiple layers of flattened cells.
Provides protection against abrasion and forms the outer layer of the skin (epidermis) and lines the oral cavity, esophagus, vagina, and anal canal.
Transitional Epithelium:
Features multiple layers of cells that change shape when stretched.
Found in organs that undergo stretching, such as the urinary bladder, allowing it to accommodate varying volumes of fluid.
Stratified Cuboidal and Stratified Columnar Epithelium:
Less common types of epithelium.
Stratified cuboidal epithelium consists of two or more layers of cuboidal cells and is found in some ducts.
Stratified columnar epithelium consists of two or more layers of columnar cells and can be found in certain parts of the male urethra and large ducts of some glands.
These are just a few examples of the diverse epithelial tissues in the body. Each type is specialized for specific functions and locations within various organs and tissues.
2 notes
·
View notes
Text
My idea is that cDNA libraries of the mRNA from humans of different ages, eg 1 year, 5 years, 10 years, 15 years, 22 years, 30 years, 40 years, 55 years, 70 years and 85 years (but practically it would be necessary to just take the samples that became available!) could be constructed or acquired. They could also be acquired from specific “aging critical” tissues/organs eg endothelium, cardiac, pulmonary, kidney, brain etc. The cDNA libraries could be compared by constructing microarrays (that is my dated knowledge but today it could probably be done computationally).
What would that give us? By the differences in the transcriptome between the different age cohorts it would show the difference between aged tissues and young tissues.
Of course, how these differences arose is AS a result of the epigenetic processes, but the differences themselves ARE the results of the epigenetic processes and (in some way which I am not able to imagine right now) may lead to approaches to discover more about the epigenetic processes themselves, which is your interest. Please forgive me if I am telling you things that are already second nature to you, but there is more to my proposal which is in fact quite simple really although very broad in scope and ambitious in outcome.
The differences mentioned above would be either the absence of specific mRNA in older tissues that is present in younger tissues, or vice versa, or quantitative differences in levels of mRNA.
That then gives a series of mRNA targets to investigate, both upstream, in terms of regulation of transcription such as transcription factors and silencing, and downstream in terms of identifying and characterising the protein product of the mRNA, its structure, binding sites, effects etc. That as you said before is quite a considerable body of work and would require many teams of researchers.
As far as intervention to promote health is concerned, discovering the epigenetic processes which cause the changes would be one pathway to treatments; other pathways could be pharmaceutical, perhaps based on transcription factors, and gene-therapy based approaches.
I think that the approach I have outlined is slightly different to that of the Yamanaka factors, which reset some cells to pluripotent stem cells, as my approach is intended to make differentiated cells youthful but still basically differentiated, as in the functioning young
adult.
I have heard of a researcher called Jaoa de Magalhaes who was said to be doing something like what I suggest (and he has now moved to Birmingham University in Britain) but I do not see mention of it on his website, he talks about long lived species, another interesting approach. An academic in Cambridge told me that she had heard of something like this that I propose being done in Singapore, but did not know the name of the researcher. So, although this approach is not truly novel, I believe it is still new ground.
#longevity#bioscience#biology#ageing#anti-ageing#molecular biology#research#scientific research#research proposal#DNA#mRNA
4 notes
·
View notes
Last Seen Blogs
solarexplosion
Idk What To Write Here

summerscramble-event
SUMMER SCRAMBLE

pimpan-fern-blog
Fern Fern

avissimming
Avis Sims

mzambitious
Ambitious Girl...