#cdc corruption
Text
CDC Releases Paper on Myocarditis After COVID Vaccination, and EVERY WORD Is Redacted in 148 page report. 🤔
#pay attention#educate yourselves#educate yourself#knowledge is power#reeducate yourself#reeducate yourselves#think about it#think for yourselves#think for yourself#do your homework#do some research#do your own research#ask yourself questions#question everything#fda#cdc corruption#fda corruption#government corruption#lies exposed#news#you decide
799 notes
·
View notes
Text
Here’s the proof on the Death Sticks. The Conspiracy Realists are crushing it the past 3 years. It’s got to be at least 18-0.
https://expose-news.com/2023/10/30/24-year-lifespan-reduction-c19-vaccination/
#common sense#truth#msm is the enemy#big pharma#globalist playbook#vaccine#deep state#globalist#cdc#cdc corruption#anthony fauci#fauci#fauci lied#Fauci lied people died#conspiracy realist
111 notes
·
View notes
Text
I apologize, I forgot to put a trigger warning before. I do mention suicide.
As a chronic pain patient/advocate who is newish but oldish to the game, I have learned that the argument of addiction is the reason people in pain are not getting proper pain relief. And if you are lucky to get pain relievers, it comes with a big, red scarlet sticker saying the medication “can cause dependency” on the bottle... well, think about it: if you have daily pain, you will need daily relief if you hope to live a normal life.
But there is a major difference between addiction & dependency:
Addiction is an insatiable desire for the medications immediate “euphoric” effects, aka “chasing the dragon” which typically lasts all day. The patient may end up over using/taking much more or all of the prescribed amount within a shorter time period.
Dependency is when the person needs the medication to sustain a decent quality of life. The patient is taking their prescribed medications as directed so that their body can function properly.
An example of dependency is a diabetic patient needing insulin so that they can live.
The problem is that addiction is in everyone, and everyone has some form of addiction that is waiting to be ignited. It is a basic human condition to “want more” and it can be a result of MANY things including a traumatic experience, or even the dreaded “peer pressure” during a high-school party. It can happen with gambling, sex, exercising, even food… It is a spectrum. And it is up to the person to determine their path.
We have reached a new stage of our awful human evolution. Being thin is a societal influence, something that people will kill them-selves for, and we now have everyday people using the diabetic prescription drug “ozempic” as a way to lose weight.
Diabetic patients who are dependent on this type of drug are unable to fill their prescriptions because of the high numbers of non-diabetic people using this drug for their personal gain- pun noted.
To be blunt or a bit dramatic, we could say they are abusing or misusing a diabetics drug.
A person in pain asking for medical attention is shamed, mocked, reported, harassed, and some extraordinary nurses have even taken it far enough to record their rejected “drug seekers” walking out from the hospitals as they’re laughing in the background.
We have been waiting for justice for what seems forever, and some pain warriors have even decided death is better than endless pain… there are so many. It’s not just pain patients either, an ER doctor Dr. Steve Ortiz committed suicide, because he was unable to help his patients. He was continually harassed by the ones who made these fucking rules. He wanted to bring light to the corruption with his death, leaving behind his wife and children in hopes for justice.
And now pain patients everywhere get to watch our society do exactly what they claim to hate us for: abusing someone else’s medication…
Self reflection is free, and everyone should use it daily.
#pain warrior#pain pain pain#pain pain go away#chronic pain#invisible disability#chronic illness#chronically ill#ozempic#cdc corruption#propaganda#social issues#idk what else to tag#long reads#please stop#lets be friends#lost light#be kind#i am healing#live and let live#ramblings#pain suffering etc#pain suffering agony#i hate this#i am so tired#i am going insane#triggering content
71 notes
·
View notes
Text
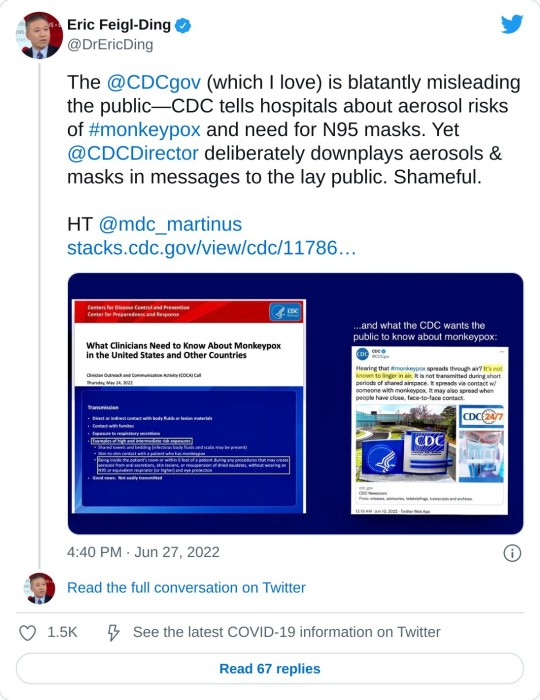
>2) Sometimes in life you have to call the CDC out and admit that the beloved world renowned public health agency you grew up loving, @CDCgov, is a mere shadow of its former self.@CDCDirector cannot tell lay public one thing & then tell clinicians something else on #monkeypox


#twitter#eric feigl ding#monkeypox#mkpx virus#mkpx#cdc corruption#gaslighting#pandemic#monkeypox pandemic#masking#world health organization
68 notes
·
View notes
Text
COVID isn't over, and this is an action you can take to remind the CDC of that. People still need help, and ignoring the problem isn't the way to address it.
#covid19#covid isn't over#action alert#community care#cdc corruption#public health emergency#disability justice
10 notes
·
View notes
Text
CDC: Child Deaths Started Skyrocketing in 2021
The U.S. Centers for Disease Control and Prevention (CDC) has admitted that official data shows that deaths in children aged 1-14 have skyrocketed since 2021.
#CDC#cdc corruption#vaccine deaths#child deaths#crimes against humanity#biontech#big pharma#depopulation agenda#crimesagainsthumanity#depopulationagenda#child murder#child death#vaccine wars#mrna vaccine#vaccines#covid vaccine
1 note
·
View note
Text
1 note
·
View note
Text

These kinds of tweets may seem innocuous, but they are very intentional. These optics are designed to boost bosses pushing workers back into unsafe offices during an ongoing pandemic. This is manufactured consent: If the CDC is doing it, then everyone can.
#all infected in covid outbreak at cdc conference were vaccinated#cdc corruption#cdc#manufactured consent#chattel slavery#wage slavery#slaves#slavery#slave#neoliberal capitalism#capitalist dystopia#usa#america#ausgov#politas#auspol#tasgov#taspol#australia#fuck neoliberals#anthony albanese#albanese government#working class#class warfare#class war#classism#classwar#workers rights#amazon workers set to walk out for three days this weekend amid pay row#workers of the world unite
1 note
·
View note
Text

Investigate Instutionalized Tyranny
#knowledge#a conspiracy of truths#liberation#revolution#strange world#mkultra#1950s#usamriid#cdc corruption#who#white coat#cia#artichoke#project#central intelligence agency
1 note
·
View note
Text
Amish did NOT follow a single guideline from the CDC. 🤔
#pay attention#educate yourselves#educate yourself#knowledge is power#reeducate yourself#reeducate yourselves#think for yourself#think for yourselves#think about it#do your homework#question everything#ask yourself questions#medical system#medical lies#medical corruption#cdc corruption
1K notes
·
View notes
Text
You don’t say…that’s shocking…NOT!
#truth#common sense#msm is the enemy#globalist playbook#big pharma#vaccine#cdc corruption#cdc lies#fda corruption#fda lied#nih corruption#nih lies#world health organization#United Nations against America#deep state
17 notes
·
View notes
Text
Doctors take an oath to do no harm.
Choosing not to help someone…
isn’t that doing more harm?
#chronic illness#chronic pain#i am scared#lost light#i need a doctor#sos from Canada#i need heeeeelp#ramblings#pain warrior#i am working on it#i am in pain#i am insane#stop it#stop the war#please stop#cdc corruption
14 notes
·
View notes
Text
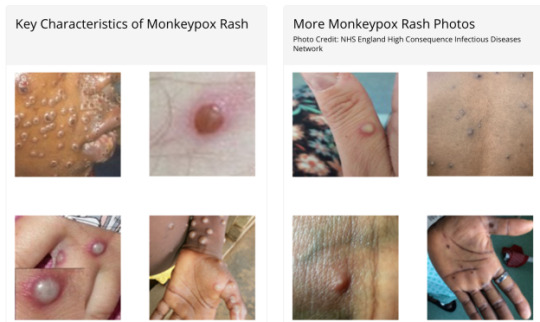
Medical experts and some pundits are raising alarm about the spread of monkeypox, a far more containable disease than Covid. But apparently because the public has been told to get used to endemic Covid, it’s supposed to resign itself to endemic Covid. A fresh report from IM Doc illustrates how appalling state of public health in America.
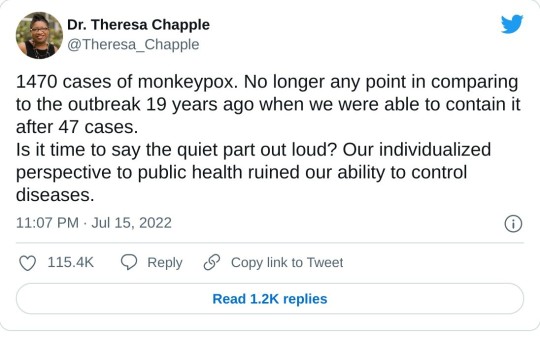
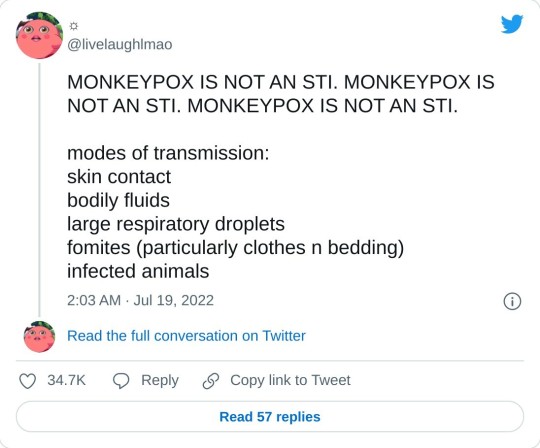
A little background courtesy Twitter:
From IM Doc at the start of the week:
Today a gay patient in his 30s showed up in the office. He is healthy and very athletic. He is a “boy” to another older gay man.
They travel the world and are into serious gay fetish play. Spanking, bondage, discipline etc.
Patient has had fever and chills and horrible headache for 3 days. A reticulonodular rash has developed but no vesicles yet. They have been playing in clubs, parties, and orgies in 4 major cities the past 2 weeks.
There are so many things in that diagnostic differential but of course monkeypox is right up there.
And of course NO TESTING IS AVAILABLE. I called all levels of health department and even CDC today. The CDC is voice mail hell. Never talked to a human. It took several hours for a health dept human but by then the patient was already gone potentially spreading the wealth everywhere. They are acting as if I was talking about the Martian Flu. Again, we have known about this two months now, and it was like I was asking for the Holy Grail. Testing? “I need to call so and so……not sure…..but I’ll get right back to you……..”. And don’t get me started about their handling of the quarantine.
I have no idea if he is really a case. Multiple tests are pending. But not monkeypox. There is apparently no blood test for that. You have to swab the vesicles. But what if we do not have vesicles yet? Or if a patient may be past the vesicular stage? Crickets.
I would like to think there is a baseline competence. But that is too much an ask right now.
Again two months all over the news and this is what we have.
We are a completely unserious nation.
Remember that IM Doc is in a wealthy destination in Flyover. Apparently the local public health officials not only think that monkeypox is exclusively a gay STD, but also that they can’t have it locally because there are no gay men in their part of the world. Did they miss Brokeback Mountain? Or the private jet landing schedule?
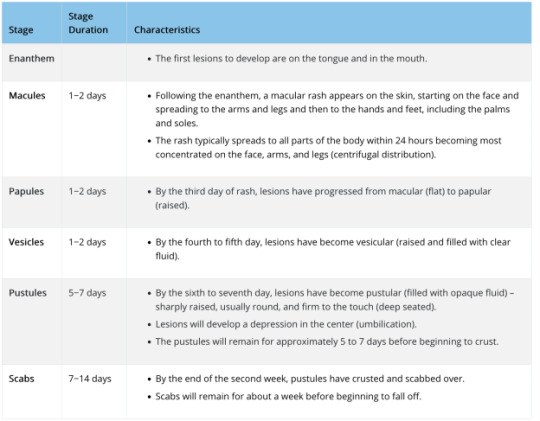
On top of that, the local public health officials appear unable to use a search engine. In fact, there are monkeypox tests, but as IM Doc did correctly infer, they can’t be used before the vesicles stage, which is 2-4+ days after lesions start forming. Oh, and monkeypox patients are contagious as soon as they start having lesions and potentially also during the prodome period, before rash starts.
From the CDC:
Persons with monkeypox will develop an early set of symptoms (prodrome). A person may sometimes be contagious during this period.
The first symptoms include fever, malaise, headache, sometimes sore throat and cough, and lymphadenopathy (swollen lymph nodes).
Lymphadenopathy is a distinguishing feature of monkeypox from smallpox.
This typically occurs with fever onset, 1–2 days before rash onset, or rarely with rash onset.
Lymph nodes may swell in the neck (submandibular & cervical), armpits (axillary), or groin (inguinal) and occur on both sides of the body or just one.
And the disease progression:
So let us return to IM Doc’s predicament. Yes, the CDC has been announcing that various labs are now testing for monkeypox. For instance, from a July 13 press release:
Starting today, Quest Diagnostics will begin testing for monkeypox. The company has developed a real-time polymerase chain reaction (PCR) test that uses patient swab specimens to qualitatively detect non-variola orthpoxviruses and monkeypox virus DNA. The test is now available to healthcare providers nationwide (except in New York)*….
Quest will offer monkeypox virus testing at the company’s advanced laboratory in San Juan Capistrano, Calif. and can accept specimens from anywhere in the country.* Quest’s testing will continue to increase the current capacity provided through CDC’s Laboratory Response Network (LRN), Labcorp, and Mayo Clinic Laboratories, providing testing capacity of up to 60,000 specimens per week by the end of July.
On June 22, HHS announced that five commercial laboratory companies would soon begin offering monkeypox testing. Since then, CDC has shipped the tests to the laboratories and their employees have been trained on their administration, among other steps.
Anyone with a rash that should talk to their healthcare provider about whether they need to get tested, even if they don’t think they had contact with someone who has monkeypox. Healthcare providers can order monkeypox virus testing from Quest as they normally would order other tests. People seeking testing for monkeypox must consult with their healthcare provider first; they cannot separately go to a Quest lab, submit a specimen, and request testing
This sounds easy-peasy, right? Except it isn’t. From the CDC Monkeypox: Preparation and Collection of Specimens (boldface ours):
Effective communication and precautionary measures between specimen collection teams and laboratory staff are essential to maximizing safety when manipulating specimens suspected to contain monkeypox virus….
Procedures and materials used for collecting specimens may vary depending on the phase of the rash (i.e., swab of lesion surface or crust from healing lesion).
For initial laboratory testing of monkeypox virus specimens at Laboratory Response Network (LRN) laboratories or authorized commercial laboratories, the recommended specimen type is skin lesion material. Specifics on the acceptable specimen type accepted within these laboratories may vary.Please contact the appropriate public health department or commercial laboratory to determine acceptable specimens.
For further characterization of the specimen at CDC, dry swabs of lesion material, swabs of lesion material in VTM, or crusts are acceptable. To ensure specimens are stored and shipped within the required timeframe, consultation with the CDC is suggested.
Personnel who collect specimens should use personal protective equipment (PPE) in accordance with recommendations for healthcare settings. Specimens should be collected in the manner outlined below. When possible, use a plastic, sterile, leak-proof container rather than glass materials for specimen collection.
Two swabs from each lesion should be collected for testing. Using two sterile synthetic swabs (including, but not limited to polyester, nylon, or Dacron) with a plastic, wood, or thin aluminum shaft, swab the lesion vigorously to collect adequate DNA. Do not use cotton swabs. It is not necessary to de-roof the lesion before swabbing. Break off the end of each swab’s applicator into a 1.5-or 2-mL screw-capped tube with O-ring or place the entire swab in a sterile container that has a gasket seal and is able to be shipped under the required conditions. Two swabs from each lesion should be collected, preferably from different locations on the body or from lesions which differ in appearance. Swabs and other specimens should each be placed in different containers. If using transport media, only VTM is accepted at CDC at this time; do not use universal or other transport media.
Specimen collection, storage, and shipping of human specimens is subject to CLIA restrictions. Specimens being sent to CDC for testing should be stored refrigerated (2-8°C) or frozen (-20°C or lower) within an hour of collection. CDC 50.34 form must be included for each specimen. When possible, ship specimens on dry ice. Specimens received outside of acceptable temperature ranges will be rejected.
Laboratory testing has indicated that the current monkeypox outbreak is associated with the West African clade of monkeypox virus. The U.S. government does not consider the West African clade of monkeypox virus as meeting the definition of Category A infectious substance under the Hazardous Materials Regulations (HMR). Therefore, specimens and material suspected or confirmed to contain the West African clade of monkeypox virus can be shipped as UN 3373 Biological Substance, Category B. See U.S. Department of Transportation’s (DOT) Transporting Infectious Substances Safely and Managing Solid Waste Contaminated with a Category A Infectious Substance (pg. 94) for further guidance.
Refer to the Poxvirus Serology test on the CDC Test Directory for further specimen storage, packaging, and shipping instructions.
For current information on the Molecular Detection test, please contact the CDC at [email protected] for details on collection, storage, packaging, and shipping of specimens.
Now perhaps this sort of specimen collection and shipment is routine for many small hospitals like IM Doc’s. But the repeated “Call the CDC for instruction” suggests otherwise. So even if IM Doc’s patient had monkeypox-looking pustules that could have been sampled and tested, neither the CDC nor the local health department did a damned thing to help.
From a later message, after I had informed IM Doc that there were monkeypox tests, but only of vesicles (as he’d inferred):
Is it not a sad state of affairs that you are able to find this and the public health dept did not know the first thing about this?
I am thinking they are probably able to assist now after this incident yesterday, but it is the total lack of preparedness that is very disturbing. They did not know the first thing about testing.
And from what I am told this PCR testing is on the vesicle swabs only. My questions remain. What if the patient is in a prodrome of fever and rash but no vesicles? What if the patient has already convalesced through the vesicles? What do we swab in those instances? Are we certain that every single monkeypox patient will have vesicles? What do we do when this is highly suspected and the patient is already having a high fever and pain and rash but no vesicles? And most importantly, should any of the examples above be placed into quarantine until further notice? The fact that none of these questions could be answered and still are not today, especially the quarantine of highly suspected patients, is of the most concern to me. These are simple obvious issues that any clinician would raise and it is as if they have never been thought of before.
The patient from yesterday, for example, has been reported. Multiple blood tests for many other things done. Most of which are pending. I still do not know for sure his diagnosis, and he has no vesicles when I followed up with him today. And there is no quarantine at all.
This just does not jive well in my opinion with the level of fear they are exhibiting about this getting out of control.
This is what I have been talking about for the past two years. In the past, the CDC would have been all over making sure every primary care doctor in the USA knew exactly what the protocol was. I have heard or seen nothing. I go over my email daily. I have found nothing on their website that is more than simple platitudes. Certainly nothing that would guide me through the above questions. And to my disappointment, the health department personnel were in no better shape than I was. Just like Ebola, COVID, and West Nile virus, monkeypox is something no one of us has ever handled. I would have expected after two months for the entire system to be on the ball, and after our first scare in my area, it is clear we are nowhere near prepared. Acute public health issues like this are only as strong as the weakest link, and we failed yesterday.
This departure from past behavior from the CDC has been the most difficult for us old docs to stomach.
And to add an additional point: the fact that there is a monkeypox test of some sort suggests that the CDC is in mission accomplished mode and isn’t pushing for the development of a blood test, which would enable clinicians to find the infection earlier (and perhaps later) than the skin-sampling ones do, and would also be less nasty to administer from the patient and practitioner perspective.
So we are well on the way to having monkeypox be as bad as it could be. Scientist GM added:
We actually have no idea how bad monkeypox is right now.
Notice that there are no statistics released on how many of the cases are hospitalized, how many in ICU, etc. We had that reporting system fairly quickly with COVID back in 2020. And it is being rolled back now, with the move to weekly reporting in many places, likely to be followed by no reporting at all eventually (other than some quarterly or annual retrospective summaries)
So the lessons – that if you don’t control infections, you need to control information – have been learned.
And it is very much possible that people have died of monkeypox in the West but it is not reported yet.
So far 3 people have officially died of monkeypox in the last two months, all in Africa. And Africa has reported very few cases in that period, i.e. the CFR there is in line with what it has been historically.
Now it is certain that they have always missed cases there, but I also have doubts it is the same undercount ratio that it is for COVID, as monkeypox is a rather visible disease that drags for longer than COVID and the pain is serious.
Which means that we have the following possibilities:
1) Mortality is low in western hospitals but high in Africa where hospitals are less well equipped. That sounds attractive on the surface, but if you think about it, it doesn’t really make that much sense – it would if there were a lot of people in ICU on their death bed and we in the West are doing miracles to save them that they don’t have the resources for in Africa. But we are not hearing about that.
2) The people it is hitting right now are a lot less susceptible to dying. I doubt that though, as this isn’t a disease known to exhibit drastic differences in CFR across different populations….
3) The virus has mutated on its way to the growing pandemic outside Africa and is less pathogenic now. Meanwhile those 3 people who died in Africa got the ancestral Nigerian strain (with the 3-4% CFR, while the Congo strain with the 10% CFR hasn’t been exported at all) and this is why they died
4) We aren’t told the truth.
We will unfortunately know more in the coming months. Once schools reopen and community-wide transmission has ramped up even more, there should be massive outbreaks in children, from where it will infect parents, etc. And then there will be serious pressure on hospitals. This will likely coincide with yet another major COVID wave and your guess is as good as mine about what will happen then…
Remember that GM’s gloomy-seeming calls on Covid most of the time weren’t pessimistic enough. So take that as a warning.
And while we are at it, CDC delanda est.
#mkpx#mkpx virus#monkeypox#monkeypox pandemic#center for disease control and prevention#cdc corruption#cdc#naked capitalism
12 notes
·
View notes
Text
CDC Aware of Hundreds of Safety Signals for COVID Jab
In September 2022, The Epoch Times asked the U.S. Centers for Disease Control and Prevention to release its Proportional Reporting Ratio (PRR) data mining results. The CDC refused. A Freedom of Information Act (FOIA) request has now forced the release of these data, and they are stunning The CDC’s PRR monitoring has identified several hundred safety signals, including for Bell’s palsy, blood clots, pulmonary embolism and death. In individuals aged 18 and older, there are 770 safety signals for different adverse events, and more than 500 of them have a stronger safety signal than myocarditis and pericarditis In the 12- to 17-year-old age group there are 96 safety signals, and in the 5- to 11-year-old group there are 66, including myocarditis, pericarditis, ventricular dysfunction, cardiac valve incompetency, pericardial and pleural effusion, chest pain, appendicitis and appendectomies, Kawasaki’s disease and vitiligo The proportions of deaths, which were only provided for the 18-plus age group, was 14% for the COVID jabs compared to 4.7% for all other vaccines The FDA is also required to perform safety monitoring, using empirical Bayesian data mining. The Epoch Times asked the FDA to release its monitoring results in July 2022 but, like the CDC, the FDA refused, only to admit in December 2022 they’d confirmed the Pfizer shot was linked to pulmonary embolism
0 notes
Photo
“THE CDC - THEY’RE LYING AND THEY KNOW THEY’RE LYING” -Tucker Carlson
The CDC complained about our segment on the Covid vaccine being required for kids to attend school. We stand by what we said. Here's our response.
CDC openly lies to the nation repeatedly & here they do it again when they say it is up to the states to implement the 15-0 vote to place COVID gene injections on child immunization schedule
CDC knows that there are US states that follow the CDC's immunization schedule & will implement, of course BLUE states & parents if you want your child not harmed & at no risk of death, say NO! Tucker
https://palexander.substack.com/p/cdc-openly-lies-to-the-nation-repeatedly
https://twitter.com/TuckerCarlson/status/1582895910295855104
download mp4; https://icedrive.net/s/k1F5gVSQwDj1AuDvjTTVQa8PkygT
see also; Must Read Article on CDC By A Midwestern Doctor “Bribes” Are Illegal, but Bill Gates, Big Pharma, and Politicians Can Still Buy Influence at the CDC https://mathewaldred.substack.com/p/must-read-article-on-cdc-by-a-midwestern
0 notes
Last Seen Blogs
scruplepossum
ScruplePossum

nightaxel
Was your life worth dying for?

quaexsanguinis-blog
Of Blood

bloodievamp
Untitled
akkoeln
Anarchistisches Kollektiv Köln