#by junell
Text
NaNo Day 17!!
Words Added" 2,010
Words Total: 50,011
100%
I have completed my first National Novel Writing Month goal, and rest assured. It is only my first. The Lady Junelle has reached the word goal, but the story is not quite finished. I am going to start edits and sending chapters to my wonderful betas @kaleighkarma and @blazingorchid, and go from there!
#talking teleia#nanowrimo#fairy tail nalu#fairy tail#nalu#natsu dragneel#current wip#lucy heartfilia#natsu x lucy#lady junelle#Nanowrimo complete#creative writing#ao3 fanfic#archive of our own#ao3#fairy tail fanfic
14 notes
·
View notes
Text
birth control made me grow the mustache of a 19th century oil tycoon. new gender achievement unlocked
#i could build a financial empire but Rockefeller couldn’t live with endometriosis so who’s the real tycoon here#(it’s me)#junel slay#endometriosis#my posts
3 notes
·
View notes
Text

The children certainly ran the home of Alynne & Jezyk.
Somewhere in the hills, and even along the countless oxbow lakes, one of their brood was making their way into some of their people's homes, visiting and choosing to make friends with all the little ones, barging in at the Randolph Bakery, and watching the Randolph cousins and Clea bake and sneak little treats to them.
It only encouraged them to think they were welcome everywhere they went.
Alynne beamed as Junelle shared a vibrant story of sharing a few fresh baked rolls with some young wolves.
"The wolfies did not want to mama, but I told them it was good for them, like you and 'Da tell me and..." and sighed theatrically with a roll of her eyes, "Ros, Evie, even Julien! Ula, too! And then they did!"
Alynne laughed softly, peering into her daughter's eyes, "That means you have the touch."
Junelle touched her mother's face, "Are you healed now?"
Alynne smiled and kissed her nose, "Yes, Junie, I am."
#alynne thea skye#junelle adair skye cantaville#the stony hills & oxbow lakes#the skyes#the third generation
1 note
·
View note
Text
Song of the day: “Season of the Witch” by Donovan. Dark Winds used it. :D
I’m going to try to post personal updates more on Sundays lol. On Hailey Fe now. I miss Junel Fe, except Hailey comes with iron instead of sugar pills. Hailey is keeping my skin clearer than Lo Loestrin Fe did.
Speaking of PCOS, Delicate Condition is the first book I’ve read where a character has that. :D She doesn’t show up until the ending, though. There are some characters I headcanon as having polycystic ovaries. They’re just that: headcanons.
After hearing how Angelica Ross was treated on-set, I’m even more pissed by American Horror Story: Delicate’s casting. Despite the novel’s anti-misogyny, -racism, and -ageism messages… Well, those first two could have used some more work. Editing wasn’t great. Anna came off as an out of touch rich woman more than once. (Like this season’s cast.)
I felt horrible for her publicist, who was fired due to misunderstandings. It’s understandable why Anna thought she was being stalked. It’s the whole point of the book. But poor Emily never gets an explanation, much less an apology. Siobhan also claims resurrecting the dead is unnatural. Being part of an immortal coven capable of body hopping/genetic memory à la Dune isn’t??
Long story short, there are already reviews that remind me of The VVitch. Protagonist joins a coven that hurt her. Some fans claim female empowerment. Siobhan’s coven isn’t malevolent. But Anna was left ignorant that magic was being performed on her, which was the cause of her pain and hallucinations.
Danielle Vega did a great job at exploring ageism with number1crush’s attitude toward Anna. That has to be said. Fan (or anti-fan) entitlement is a pet peeve.
I haven’t read Rosemary’s Baby in a while and haven’t seen the movie, but the doctor’s name was also Hill. Dr. Carla Hill makes me think of Carl Hill from Re-Animator.
Right now I’m reading the Joe Leaphorn series after watching Dark Winds. Also, the Rev. Clare Fergusson Mysteries and almost done with Dr. Ruth Galloway. Mysteries are more my cup of tea book-wise.
#Tawney talks#PCOS#polycystic ovary syndrome#Hailey Fe#Junel Fe#Lo Loestrin Fe#Delicate Condition#Angelica Ross#American Horror Story#AHS#American Horror Story: Delicate#Delicate Condition spoilers#Delicate#Dune#The VVitch#The Witch#The Witch 2015#Danielle Vega#Rosemary’s Baby#Rosemary’s Baby 1968#The Witch: A New-England Folktale#Joe Leaphorn#Dark Winds#Clare Fergusson#Ruth Galloway#Donovan
2 notes
·
View notes
Text
when i was a really angry teenager who also felt a lot worse about my gender than i do now i had this pet "theory" (theory is a strong word idk what else to call it) that vriska had to feed her lusus roughly once per month and that this ritual of blood was an allegory for menstruation in that both were a monthly punishment for the sin of persisting as a teen girl at all
#in retrospect this is ridiculous and also because i didnt get put on birth control for debilitating cramps until i was 16#homestuck-inflected musings on suffering and the inherent cruelty of puberty decreased by like 90% after junel fe#ITS HARD BEING A KID AND GROWING UP. ITS HARD AND NOBODY UNDERSTANDS. etc.
1 note
·
View note
Text
Perimenopause Panic: Ultimate Guide | Dr. Kelly Culwell | MomCave LIVE
Hold on to your hot flashes, folks! We’ve got the amazing Dr. Kelly Culwell in the MomCave, where the coffee is strong, and sanity is on a coffee break. Dr. Kelly, not just your typical doctor—she’s the OBGYN rockstar with a prescription for laughter and a cure for the chaos that is perimenopause. Buckle up for a rollercoaster of hormones, hilarious anecdotes, and maybe a few tips on how to…
View On WordPress
#birth control and menopause symptoms#birth control diaphragm#birth control during perimenopause#birth control junel#birth control perimenopause symptoms#birth control sprintec#birth control without hormones#perimenopause bloating#perimenopause dizziness#perimenopause fatigue#perimenopause joint pain#perimenopause missed period#perimenopause quiz#perimenopause symptoms#taking birth control during perimenopause
0 notes
Link
The Benefits and Risks of Loestrin Contraceptive Pills In this comprehensive guide, we'll delve into the world of Loestrin, a widely used contraceptive medication. Whether you're considering Loestrin as your birth control option or just curious about its effects, we've got you covered. We'll explore its uses, potential side effects, dosages, and important considerations to help you make an informed decision. [caption id="attachment_63774" align="aligncenter" width="686"] Loestrin[/caption] What Is Loestrin? Loestrin is a prescription medication primarily used for birth control. It belongs to a class of drugs known as combination hormonal contraceptives. These medications contain both estrogen and progestin and work by preventing ovulation, thickening cervical mucus, and altering the uterine lining. By doing so, Loestrin effectively reduces the chances of pregnancy. Uses and Benefits of Loestrin Loestrin is prescribed not only for contraception but also for managing other health conditions. Some of its uses include: Birth Control: Loestrin is highly effective in preventing pregnancy when taken as directed. It offers a convenient and reversible form of contraception. Menstrual Cycle Regulation: Loestrin can help regulate irregular menstrual cycles, reducing heavy bleeding and painful periods. Acne Treatment: Some formulations of Loestrin are approved by the FDA for treating moderate acne in females aged 15 and older. Hormone Replacement Therapy: In certain cases, healthcare providers may recommend Loestrin as hormone replacement therapy for women experiencing menopausal symptoms. Potential Side Effects and Considerations While Loestrin is generally well-tolerated, it's essential to be aware of potential side effects and considerations, including: Common Side Effects: These may include nausea, breast tenderness, headache, and breakthrough bleeding. These symptoms often improve after the initial adjustment period. Serious Side Effects: Although rare, Loestrin can lead to severe complications such as blood clots, stroke, heart attack, and high blood pressure. It's crucial to discuss your medical history and risk factors with your healthcare provider. Interactions: Some medications, supplements, and herbal products may interact with Loestrin, reducing its effectiveness or increasing the risk of side effects. Always inform your healthcare provider about all the medications you're taking. Considerations for Smokers: Smoking while using hormonal contraceptives like Loestrin can increase the risk of cardiovascular problems. If you smoke, discuss alternative birth control methods with your healthcare provider. Dosages and Administration Loestrin is available in various formulations, each with its specific dosages and administration instructions. Your healthcare provider will determine the most suitable option for you based on your medical history and individual needs. Common dosages may range from low-dose options to higher-dose formulations. It's essential to follow your healthcare provider's guidance carefully to ensure the medication's effectiveness. Loestrin and Birth Control Effectiveness Loestrin is highly effective when taken correctly, but it's essential to understand how to maximize its contraceptive effectiveness. This section can cover topics such as: The importance of taking Loestrin at the same time each day. What to do if you miss a dose and backup contraceptive methods. The timeframe in which Loestrin becomes effective (usually after seven days of consistent use). Choosing the Right Loestrin Formulation Loestrin comes in various formulations, each with slightly different hormone levels. Discussing the considerations for choosing the right formulation based on individual needs, such as addressing specific menstrual symptoms, acne, or contraceptive goals, can be beneficial. Loestrin and Your Health This section can delve into how Loestrin may impact various aspects of health, including: Bone Health: Discuss the potential impact of Loestrin on bone density and the importance of calcium and vitamin D intake. Emotional Well-being: Addressing how hormonal contraceptives can sometimes affect mood and emotional health and when to seek medical advice if experiencing mood changes. Regular Check-ups: Encouraging regular check-ups with a healthcare provider to monitor health while on Loestrin. Alternatives to Loestrin Not all individuals may be suitable candidates for Loestrin or may prefer alternative contraceptive methods. Discussing other birth control options, such as intrauterine devices (IUDs), implants, or barrier methods, can provide valuable information. Frequently Asked Questions What is the primary mechanism of Loestrin in preventing pregnancy? Loestrin primarily prevents pregnancy by inhibiting ovulation (the release of eggs). Can Loestrin be used as an emergency contraceptive? No, Loestrin is not intended for emergency contraception. It should be taken regularly as prescribed. Are there age restrictions for using Loestrin? Loestrin is typically prescribed to women of reproductive age. Consult with a healthcare provider for suitability. Does Loestrin protect against sexually transmitted infections (STIs)? No, Loestrin does not protect STIs. It's essential to use barrier methods, such as condoms, to reduce the risk of STIs. How long can I use Loestrin as a contraceptive? The duration of Loestrin use can vary based on individual needs and plans for family planning. Discuss with your healthcare provider. Are there dietary restrictions when taking Loestrin? There are no specific dietary restrictions while taking Loestrin. However, maintaining a balanced diet is always recommended for overall health. Can I use Loestrin while breastfeeding? Certain formulations of Loestrin may be suitable for breastfeeding mothers. Consult with a healthcare provider for guidance. What should I do if I experience persistent side effects with Loestrin? If you experience severe or persistent side effects, contact your healthcare provider. They may recommend adjusting your medication. Is Loestrin available over-the-counter (OTC)? No, Loestrin is available by prescription only and should be obtained from a healthcare provider. How quickly can I expect my menstrual cycle to return to normal after discontinuing Loestrin? The return to a regular menstrual cycle can vary from person to person. It's normal for some variation initially. Conclusion: In the concluding section, summarize the key points discussed in the article, reiterate the importance of consulting with a healthcare provider before starting or discontinuing Loestrin, and encourage readers to make informed decisions about their contraceptive options.
#birth_control#birth_control_pill#contraception#contraceptive#contraceptive_pill#ethinyl_estradiol#Gildess#hormonal_contraception#hormone_pill#Junel#Larin#Microgestin#Minastrin#oral_contraceptive#prescription_medication
0 notes
Text
original (c. late 2019-early 2020)

redraw (today)

proud of how my grip on anatomy has improved over the years! there are a couple things i still need to improve on but it's doubtless i've gotten better.
0 notes
Text
I need to go back through june tags and add a juniper/fengling specific ship tag so I can look at all my silly little posts and feel all my silly little feelings about them with one click of a button
#I've DONE this with elyss and june and it's GREAT but fengling stuff usually just goes into juniper insp tag with everything else in there#Fengling's player after last night's session: I've been thinking about what the ship name would be-- Juneling? or Feyniper?#me: oh no those are both cute agajdkfsh#FRANKLY I don't always go in for portmanteau ship names but. those are both cute and fun to say lol#personally I'm inclined toward Feyniper because adding the Y to clarify pronunciation also alludes to both their ties to the fey 👀#(also it sounds cuter)#ANYWAY I'm still just so! no thoughts head empty hehe dnd ship go brrr and I want Content#but the only content there IS is whatever has been made by me or stephen and whatever else I may have reblogged while thinking about em :')#well and listening to the ship playlist on repeat. you know.#about me#my OCs#juniper#fengling and june
0 notes

Text
Update with Snippet!
Nano Update
Nano Day 8!!
Words Added: 3,133
Word Total: 17,491
35%
Chapters 1-5 are done!
Have a Snippet! <3
/\/\/\/\/\/\/\/\/\/\/\
“Nah. Magic makes us brave,” he said. “And if they aren’t mages, then they aren’t your peers,” he said with a shrug. “Magic makes ya brave, and strong. Even a weak mage is stronger than they realize, because it takes a lot of heart, and a strong soul, to learn magic. That’s what Gramps says anyway.”
Lucy reached into the pouch she kept strapped to her thigh and drew out a golden key. She stroked her finger over the cerulean lines that decorated it. “I like that a lot,” she murmured.
Natsu admired the way light and love filled her face as she looked at the key.
“Show me,” he prompted, nodding to the key when she cocked her head curiously.
She blushed slightly. “I’ve never introduced anyone to her before… I’m not sure how well she would react. She can be difficult on the best of days.” She took a deep breath when he looked undeterred. “All right, but I warned you.”
Natsu chuckled and watched her slide down to the lower ledge of the rock where she could reach the water. Dipping the key’s tip into the water, she called out, “Open, Gate of the Water Bearer. Aquarius.”
She sat back and braced herself. A flash of golden light momentarily illuminated the area and Aquarius appeared with her arms crossed under her bust.
“What could you possibly want from me?” she asked, glaring down at the girl. “I’m busy, so I don’t have time to play with you today.”
Lucy smiled up at her from the rock. “I’m glad to see you, either way,” she said.
Natsu shifted into his squat again and grinned. “That was awesome! Where did she even come from?”
Aquarius’s eyes snapped up to him, then back to Lucy. “That’s not your fiancé. Boyfriend?” she asked teasingly.
Lucy huffed. “I’m married now. And he’s my bodyguard.”
“And friend,” he interjected, grinning at the blush that filled her cheeks.
#talking teleia#wip wednesday#nanowrimo#nanowrimo wip#fairy tail#ao3 fanfic#archive of our own#fairy tail fanfic#fairy tail nalu#creative writing#ao3#lucy heartfilia#natsu dragneel#natsu x lucy#writeblr#Lady Junelle
12 notes
·
View notes
Text

(apologies if this is a bit hard to read) here are all the contestants! all characters and those who created them will be under the cut! i will update when round one is ready to be posted with some advance notice!
some general rules for this bracket:
please keep things civil! this is purely for fun, no need to get personal.
propaganda is now allowed to be posted! @ me or send it in the dms for it to be reblogged!
if you did not get in, please don't fret! they either didn't meet an aspect of the guidelines or i could not find your blog. you're free to try again with another oc or an image next time the bracket is open.
here are the round one competitors:
neirum stardancer (@fagdykes) vs. elijah kalt-yaharam (@petulant-poet)
sigma octantis (@identityquest) vs. gabriel (@bloodyodyssey)
junelle (@browzerhistory) vs. angel (@slenderverse)
charles equilla (@bjdeogame) vs. first dewdrop of morning, fifth sunrise (@klugpuuo)
isabelle davis (@ratnukegenius) vs. katia (@cactus-zombie)
dawn automato (@flannelfloofs) vs. valentina minh (@riotontheward)
chicken noodle (@sammisafetypin) vs. fabian levine (@4usrhacidae)
carius (@starbowdream) vs. laridae marlin (@grand-arcanist-wynslow)
konpieto (@yakiattaki) vs. nobody (@dino--draws)
coral (@sim-ant) vs. vera hoffman (@bubblelovewaltz)
competitors introduced in round two:
vali (@blookisses)
davey (@bandtrees)
hironobu shirahama (@notoriousmasc)
sir wulfington scudworth (@wulfums)
nekiyah (@queefzillah)
okona (@roakkaliha)
78 notes
·
View notes
Text
spent the night in the ER. As we all may or may not know, I got an IUD placed in Oct when I was 4 months postpartum.
I've been bleeding ever since. Not "spotting," but bleeding. Heavily. I've had ultrasounds to check on the position - it's in place. at 6 months of bleeding, I was put on Junel Fe to see if it would calm down. Nope. I started getting cramping so bad, I thought I had another cyst burst. I was getting really big clots/tissue.
Back to the doctors, I'm taken off Junel and put on doxycycline bc I guess it can slow the bleeding? and an ultrasound is scheduled for the first week in June, where, after imaging, I'd most likely have it taken out.
well, 3 days later and I'm bleeding so heavily and passing tissue like I've given birth. I bled through a heavy overnight pad in 3 hours, and left a blood pool on my cough 6 inches wide. the tissue I passed was like the size of my palm. I called the on-call midwife and she told me to go to the ER.
So, new pants, fresh pad (heavy flow overnight ~guaranteed 10 hours!~, I go to the ER and I'm ofc crying bc I didn't know wtf is going on and I hate leaving Aidan. I think I sat in the waiting room for less than 2 hours, getting up twice to get vitals and bloodwork done. When i got up to be wheeled to ultrasound, I realized I had bled through my pad and my pants again. Badly. I told the attendant while holding up my blood covered hand and he just went "oh. I'm sorry" LOL K
The tech tells me to get undressed and get on the table etc and I'm like "um, I'm bleeding like really really bad.." she was just like "it's fine" and left. I'm crying a little, and I pull down my underwear and I shit you not, felt clots and blood just gush out and splatter on the floor.
Now I'm sobbing bc there's nothing for me to clean it up, I can't find a trash can, and I just keep bleeding anyways, so I put some paper towels over the murder scene on the floor and lay on the bed, covering my face with my arm unable to stop crying. the tech is a cold bitch as usual and then I'm told to get dressed (in my bloody clothes thanks!) and sit in the wheelchair to be picked up.
the attendant. brings me back. to the waiting room. WHICH HAS BEEN PACKED WITH PEOPLE BY THE WAY! I'm crying still, and I get out if the chair and go to the desk to be like "hi I'm bleeding through my clothes??" but the male nurse grabbed and was like "THERE YOU ARE! I've got a room ready for you! I tried to call ultrasound but they didn't answer. what were you looking for?" and I just mumbled that I didn't want to get blood on the furniture as I followed him.
he had the nurse get me mesh underwear and pads and it was the first time I felt like someone empathize with me. he said "it's gonna be ok" with a reassuring look, and left.
I waited a while in there. listening to the ridiculous chaos that they were dealing with, all definitely more acute than me - esp bc my bloodwork showed I wasn't bleeding out or anything. a man with dementia was being aggressive with the staff even though he had broken ribs and a pneumothorax and had been dosed with fentanyl. he kept trying to dismantle his bed, almost broke his foot, and I was just waiting for one of the nurses to get hurt.
I got a pelvic exam, and the doctor used about 12 gigantic swabs trying to get all the clots he saw. he said "yeah i see what you mean, it's a slow constant ooze" wow, I feel sexy.
ultrasound was apparently clear, and he asked if I preferred to go home for the night or stay -bc he wanted me to be seen by obgyn within 2 days. I chose to go home. it was after midnight. I asked for scrubs to go home in and thankfully got some.
my ultrasound showed my right ovary was fine, no torsion,cyst etc. then "suboptimal view of left ovary due to secondary location"
sorry What. also my uterus is LARGE and my endometrium is thickened to 11mm AND THATS AFTER 7 MONTHS OF BLEEDING THAT i KEPT GETTING TOLD WAS My UTERINE LINING THINNING OUT BC THATS THE IUD'S JOB
all I can think is endo/adenomyosis/cancer.
so I'm getting this thing (the iud) taken out. I want my hormones checked. and the dr im seeing already said i can get a hysterectomy or my tubes tied or whatever. and I can't stop thinking of my aunt who died of ovarian cancer bc they failed to catch it in time despite her going to doctors constantly with symptoms.
I'm really scared,actually. my history of medical trauma is on hyperdrive. I feel like I'm failing my kid. I'm not capable of being the mom I want to be. I feel betrayed and sabotaged by my body again. I also can't think straight whatsoever so I could be misunderstanding the meanings of things.
just don't kill me you piece of shit meatsack. not now that I've been trying to actually stay alive.
3 notes
·
View notes
Text
🧿 HAPPY AUTUMNAL EQUINOX. BEHOLD MY VISAGE. 🧿
Actually, the equinox was last week. Enjoy this post-shower, mid-bathroom cleaning, pre-harvest festival selfie. (Ended up hitting another one the next day. I love fall.)
Got a SlimpySwampGhost “Sisters of the Ever Sharpening Blade” t-shirt as an early b-day present for myself. Pale blue is pretty.
I want to update my wardrobe to include more ghostly spooky stuff instead of mainly bones and celestial objects. Also thinking of getting detached sleeves so I can wear t-shirts in winter (under jackets and hoodies).
When your primary care moves offices. ლ(ಠ_ಠლ) For some reason my new doc prescribed me larger pills than usual, so I’ve been splitting them in half. So I guess that’ll make it easier to eventually wean myself off Lexapro? If the halves are smaller than usual?
Speaking of pills, I gotta get back on Junel Fe, too. I CAN FEEL THE TESTOSTERONE COURSING THROUGH MY LIFEBLOOD. PCOS IS A BITCH.
Excess testosterone = texcessterone?
Watching as much Gotham as possible before they take it off Netflix. Then I will borrow the DVDs. Butch, Penguin, Jerome, and Mr. Sionis can get it. In that order.
Song of the Day: “Why Not” by Ghostface Playa. Want to read Treasure Island before watching the Soviet ‘toon. And the Muppets one. I liked studying Dr. J and Mr. H, so I’ll probably like the book.
#Tawney talks#mirror selfie#goth#goth girl#goth woman#minors do not interact#goth chick#PCOS#Trevor Henderson#Treasure Island#Alice in Wonderland#Disney#Gotham#DC#casual goth#equinox#Hot Topic#Robert Louis Stevenson#Junel Fe#Ghostface Playa#TSCODJAMH#Muppets#SlimpySwampGhost#polycystic ovary syndrome#Lexapro#escitalopram#GAD#fall equinox#autumn equinox#September equinox
12 notes
·
View notes
Text
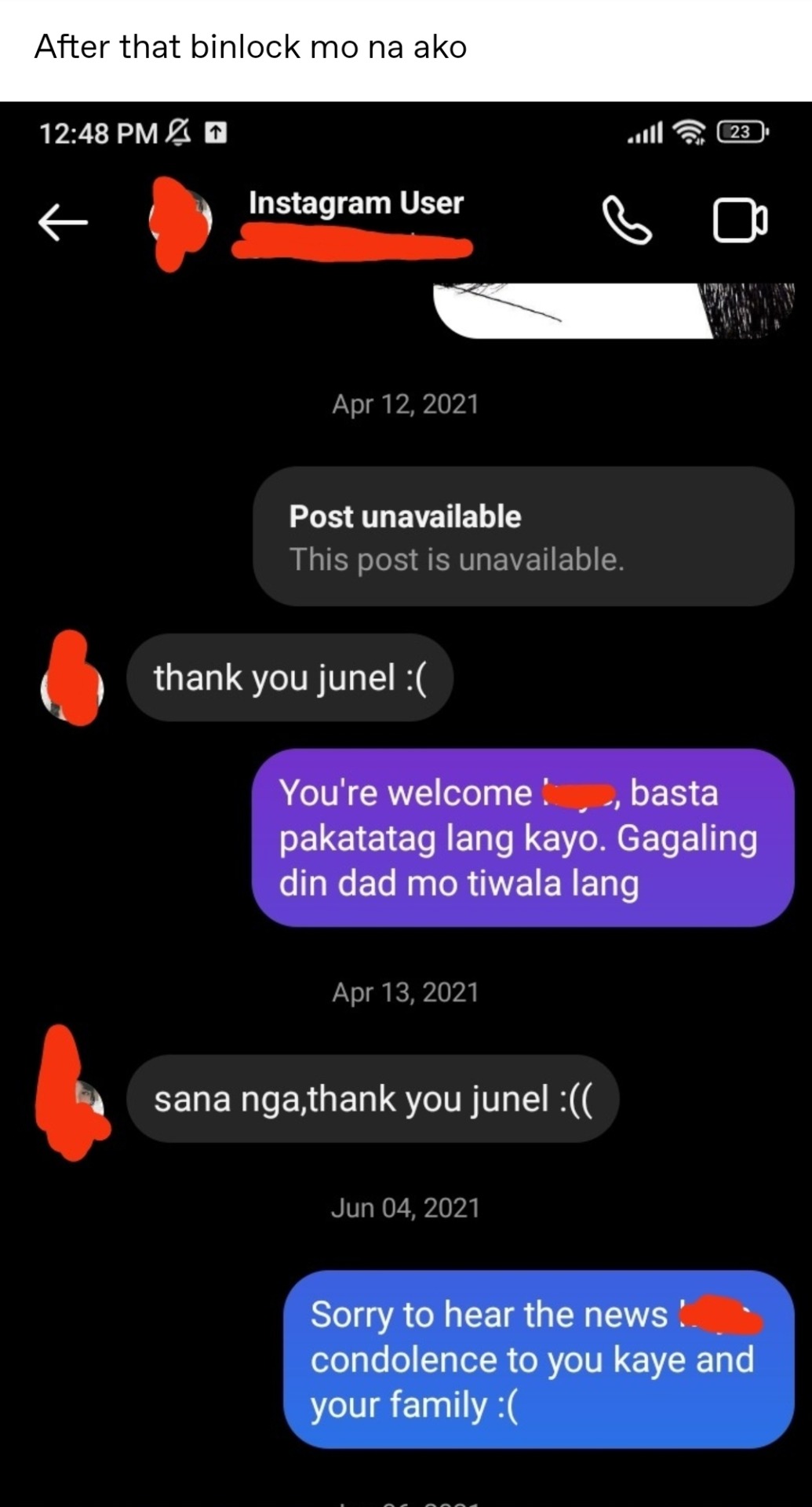

@iamhappygoth09
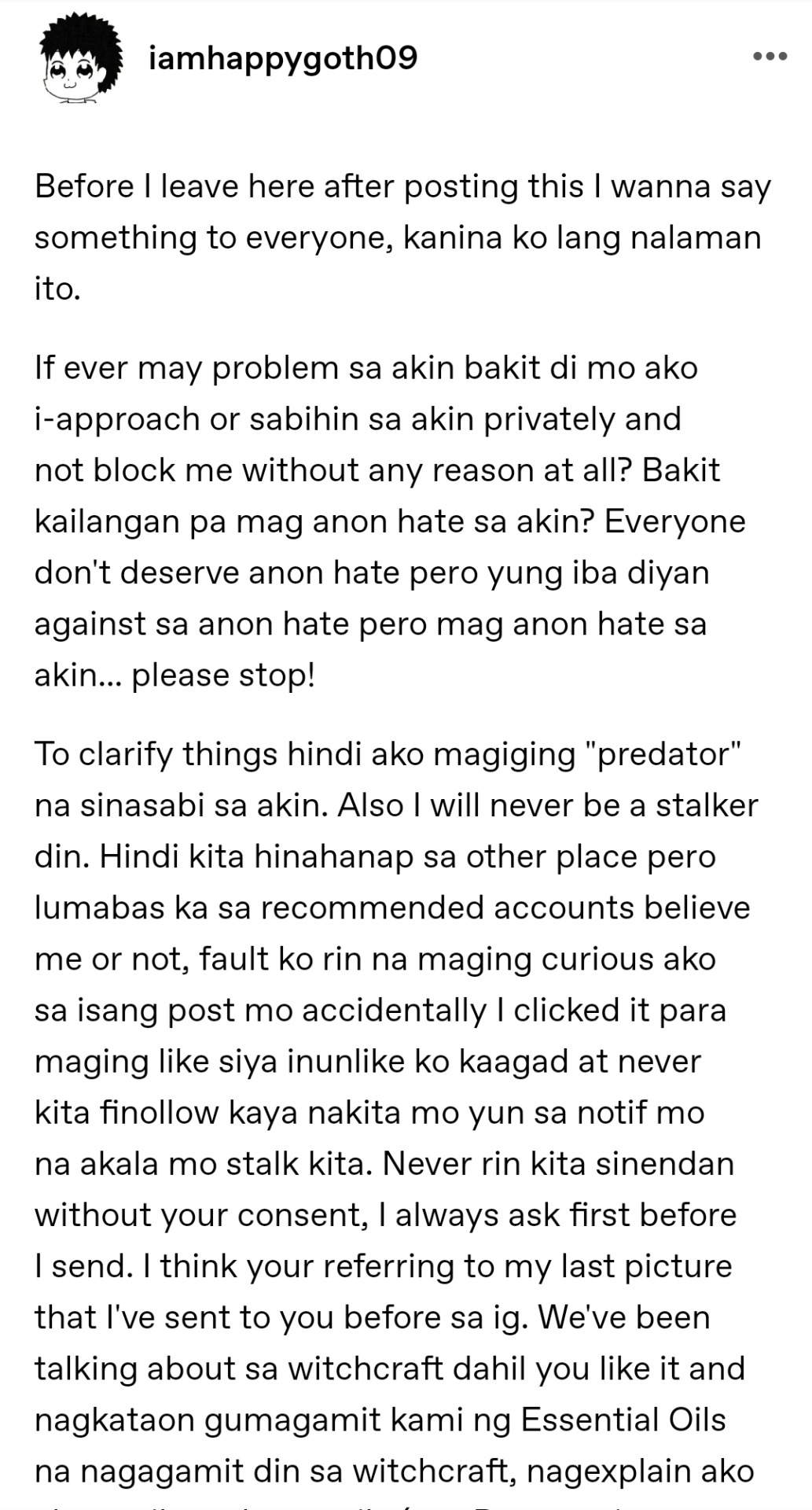
1. I'm allowed to simply block you once di na ko komportable sayo. We are NOT and have never been friends in real life for me to owe you any explanations. It is NOT my obligation to tell you kung anong mali mo at ayaw ko sayo. You are just a guy I met on Tumblr that I mistakenly befriended only to find out na sobrang creepy mo pala and kept taking advantage of the fact that I was so nice and friendly to you. I was dating somebody so I chose to cut off whatever friendship or connection we had because it's simply not that deep. And not to mention, you are MARRIED. So the sane thing to do would be to fucking stop and just move on. Easy. I don't owe you anything. And I value my own comfort and my past relationship more than you. I'm allowed to block you because you started making me feel uncomfortable. It's that simple. You are turning 36. You are a grown ass man. I'm 25. When somebody blocks you, your instinct should be to stay the fuck away and accept that the person cut you off. NOT keep posting about me—full name and all, and how much you're crushing on me and posting my photos without my permission and even my photos that were either not posted in public platforms, OR photos that were on my very old, long deactivated blog pa (deactivated in 2018). I was literally your FRIEND and I chose to cut you off and you continued doing those things. Hindi ba weird para sayo? Ang tanda mo na, simply accept that I cut you off and move on. Need ko pa talaga sabihin yan sayo? Ikaw sa tanda mong yan? Ikaw na may asawa? Di mo naisip na "ay wag na lang pala tigilan ko na lang siya." Like ?????
2. What do these screenshots prove? That I treated you like a friend? Like a real friend? Tapos ikaw ano trato mo sakin, like I'm some public figure na kapag nagcut off na ko sayo, di mo pa rin irerespect yung privacy at boundaries ko? Na ipopost mo pa rin ako at information ko? That you will still try to stalk my accounts everywhere?
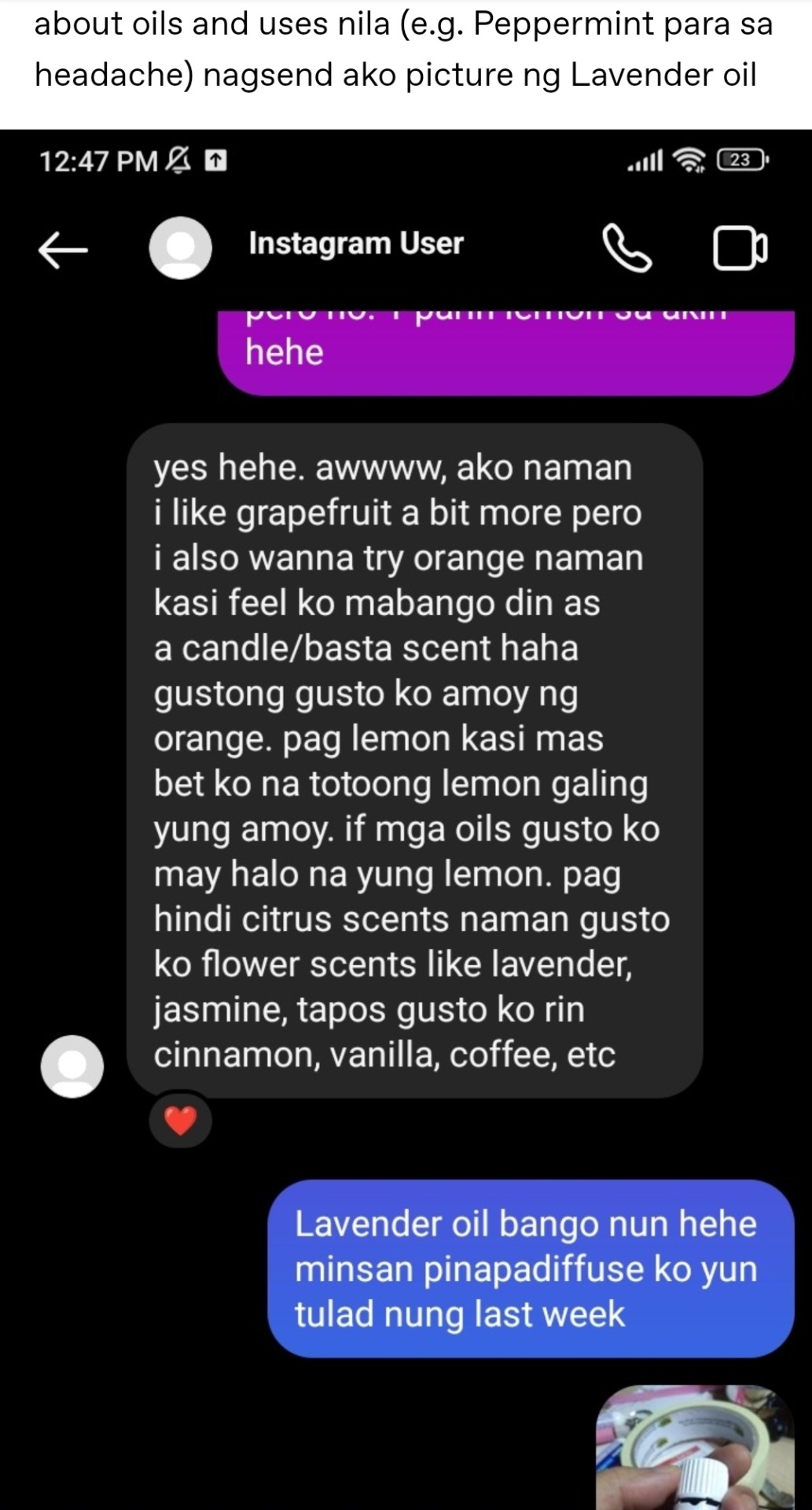
3. You claim na di ka predator, but let's be real, the first time you ever befriended me you did send me unsolicited nudes. Sa TG back in 2018, remember? Nung di pa tayo close? Kasi puro ka lang jakol. I was too nice and polite to say anything to you because we shared mutual followers. Even some mutual tumblr friends. Ang iniisip ko, friend ko si J*shy (remember her?) at nakita kong kinakausap at kaibigan mo rin kaya hinayaan na lang kita kaysa gumawa ng issue when friend mo rin kaibigan ko. Saka lang kita kinaibigan talaga nung 2019, I gave you another chance kasi iniisip ko sila J*shy.
ALSO. Kaya ko to binibring up DAHIL may isa pang blogger na lumapit sakin and shared the same experience she had with you. Ganon din. Kinaibigan mo tapos dinala mo sa TG tapos sinendan mo ng unsolicited nudes. So ngayon mo sasabihin na di ka predator? Kahit pa makaibigan at makuha mo loob namin, isip-isipin mo rin naman intensyon mo sa "pakikipagkaibigan" mo sa mga tao dito at saka mo sabihin sa sarili mo na malinis intensyon mo at hindi ka naghahanap lang ng target at pagjajakulan at papatol sayo dahil mabait yung tao. Ako, personally, I'm not that pressed about it sa interactions natin noong late 2018 nung minemessage mo ko sa TG kaya i don't care too much. Maybe pinatulan pa nga kita. It's not that deep for me I mean I did give you another chance to be my friend. Pero knowing na even until recently ganyan ka? Sa ibang mga tao? Unsolicited nudes? Really Junel? Ngayon mo sasabihin di ka predator o wala kang predatory tendencies? You? 36 and married? Approaching women younger than you on Tumblr and befriending them for the sake of getting/sending nudes na minsan sobrang unsolicited pa? Without mentioning you have a wife? That's not predatory? Sure ka na talaga final answer?
4. You will never be a "stalker" pero todo parinig ka about sa pagpunta mo sa las piñas na ang lapit mo sakin at sana madatnan mo ko? According to one of your posts sa SM Southmall pa nga yung isang beses na sinabi mo yan. Sana "masilayan" mo ko. At pinagkwekwento mo ko sa mga tao na ako si crush na taga las piñas na binlock ka?

Kahit pa sabihin mo na di ka "stalker" does it really matter what you say at this point? What matters is from MY, and everyone else's point of view, sobrang creepy ng mga pahiwatig mo tungkol sa pagpunta kung nasaan ako. Do you even hear yourself? Kahit pa sabihin mong di mo ko balak sundan in real life. The MERE FACT THAT YOU BEHAVE LIKE THIS ABOUT SOMEONE YOU DON'T PERSONALLY KNOW AND SOMEONE WHO CHOSE TO CUT YOU OFF AND DISTANCE FROM YOU. IT IS DISTURBING.
5. Yeah, you are only sorry you were caught. Kahit pa sabihin mong lumabas lang ako sa recommended mo. Anong magagawa natin eh nahuli kitang naglike at umaaligid sa account ko? After everything you've said and done about me. Who wouldn't be disturbed to find out you're still spying on me? When nung una tinolerate lang kita kahit sobrang creepy mo na. Tapos biglang ayan ka pala nastalk sa kabago-bago kong account? TAPOS magkukunwari kang walang nangyari THEN ifafollow mo ko gamit yung b&w photography instagram mo as if di ako aware na ikaw yun eh kaso lang di ako tanga?
So ano? You want to talk? Ngayon ka pa iimik ng "handling things privately" when you never respected my privacy. Pero kung gusto mong mag-usap GOW LANGZ IM DOWN IM OPEN. Wanna toss in your wife too?
8 notes
·
View notes
Text
I'm on OB rotation again. I asked the attending what are things the PCP should know about prenatal and postpartum pts. Stuff we discussed:
SSRIs can be continued during pregnancy. I often see patients on Zoloft during pregnancy if they need an antidepressant. In fact, I just started a prenatal patient on Zoloft the other day in clinic. It is safe to continue SSRIs during pregnancy because you should treat the patient's depression. Babies can come out sort of jittery because of the SSRI, but that goes away.
Postpartum patients will have bleeding somewhat similar to a menstrual period right after giving birth. It starts to decrease and becomes like a brownish color and can last up to 6 weeks postpartum. Any bleeding beyond that point is abnormal.
There is some evidence that if you have estrogen-containing birth control, it can decrease milk supply. Actually, I had a patient in clinic recently who was seen by an attending and he started her on a progesterone only birth control so that it would not affect her milk supply. Estrogen decreases the patient's milk supply, so patients who plan to breast-feed should not be started on estrogen-containing birth control. Right after giving birth, your body has increased amounts of estrogen, so you would not start estrogen containing birth control until at least 6 weeks postpartum anyway. Increasing estrogen immediately postpartum increases risk of blood clots. For patients who plan to breastfeed and want to be on an oral contraceptive, use progesterone only oral contraceptives until she stops breastfeeding.
If the mother is breastfeeding at least every 4 hours, then this can be used for contraception. It's about 80% effective. Once baby starts sleeping through the night or once baby starts feeding more than every 4 hours, this method won't work! If you go more than 4 hours without breastfeeding, breastfeeding will not protect you from pregnancy! You can also ovulate before your menstrual period returns, so you can't say you can't get pregnant because your period has not returned yet!
I asked the attending I worked with today about how she goes about prescribing birth control. She said she will usually start with Sprintec. It's usually covered by insurance and if it's not covered, it's pretty affordable. She also said Junel is pretty well tolerated. Certain progestins in certain brands of birth control may work better for certain things like acne control, but she didn't have as much knowledge on that. I'll ask another attending again about that. I usually start people on Sprintec as well.
PCP should know that alkaline phosphatase is high in pregnant patients. It comes from the placenta. So don't be freaked out by that.
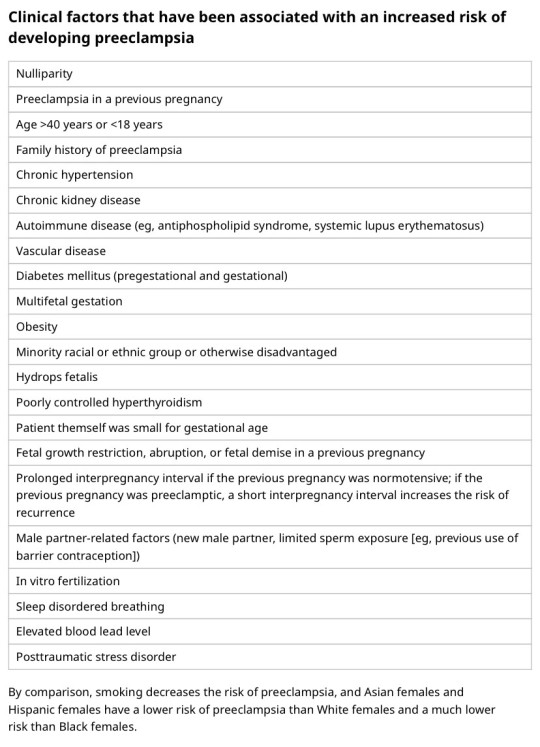
You should know HTN in pregnancy and preeclampsia workup. High BP is 140/90. Severely high BP is 160/110. Swelling occurs in many pregnant pts, but that should also alert you to start preeclampsia workup.
[Preeclampsia w/u from UpToDate:
Diagnostic evaluation
•Laboratory – Patients with suspected preeclampsia should have a complete blood count with platelets, creatinine level, liver chemistries, and determination of urinary protein excretion.
•Fetal status – Fetal status is assessed concurrently or postdiagnosis, depending on the degree of concern during maternal evaluation. At a minimum, a nonstress test or biophysical profile is performed if appropriate for gestational age. Ultrasound is used to evaluate amniotic fluid volume and estimate fetal weight, given the increased risk for oligohydramnios and growth restriction.
•Consultation with the neurology service is generally indicated in patients with neurologic deficits/abnormal neurologic examination, which may include ocular symptoms or a severe persistent headache that does not respond to initial routine management of preeclampsia.]
An important thing to review is physiology of pregnancy. Blood volume increases during pregnancy, so there are lots of new RBCs and that will throw off a HgbA1c reading, therefore HgbA1c is not measured during pregnancy and will not be accurate! My attending today told me there was a midwife who offered pts either HgbA1c or oral glucose tolerance tests to screen for gestational DM. The HgbA1c is not accurate in pregnancy, so this should not be done. That would be bad to miss a diagnosis of gestational diabetes. You have to wait until 3 months postpartum to measure HgbA1c to get an accurate reading. Had a pt who did not have a PCP prior to getting pregnant, was on insulin during the pregnancy, and after giving birth, still needs to establish with PCP for diabetes f/u. After you give birth, you insulin needs drastically change, so you don't need as much as you did when you were pregnant. So I stopped her insulin and advised that she f/u with her new PCP for diabetes care.
I still need to review fetal heart tracings. The attending today said the first thing to look at is the baseline (the baseline HR should be about 160 beats/min), then the variability, then look for accelerations and decelerations. If more than 32 weeks GA, accelerations are 15 beats/min above the baseline lasting at least 15 seconds. Early decelerations are representative of compression of the fetal head, which is normal during labor as baby moves down the pelvis/birth canal. Variable decelerations look sharper like a "V" and can represent compression of the umbilical cord. Late decelerations represent placental insufficiency.
ACOG has very helpful practice bulletins.
I can't take screen shots on my work laptop, so I'm just going to summarize gestational HTN w/u from UpToDate:
Gestational HTN: New onset of systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg on at least 2 occasions 4 hours apart after 20 weeks of gestation in a previously normotensive individual
And:
No proteinuria
No signs/symptoms of preeclampsia-related end-organ dysfunction (eg, thrombocytopenia, renal insufficiency, elevated liver transaminases, pulmonary edema, cerebral or visual symptoms)
Preeclampsia: New onset of systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg on at least 2 occasions at least 4 hours apart after 20 weeks of gestation in a previously normotensive individual. Patients with systolic blood pressure ≥160 mmHg and/or diastolic blood pressure ≥110 mmHg should have blood pressure confirmed within a short interval (minutes) to facilitate timely administration of antihypertensive therapy.
And:
Proteinuria (≥300 mg per 24-hour urine collection [or this amount extrapolated from a timed collection], or protein:creatinine ratio ≥0.3, or urine dipstick reading ≥2+ [if other quantitative methods are not available]).
In a patient with new-onset hypertension without proteinuria, the diagnosis of preeclampsia can still be made if any features of severe disease are present.
Preeclampsia with severe features: In a patient with preeclampsia, presence of any of the following findings are features of severe disease:
Systolic blood pressure ≥160 mmHg and/or diastolic blood pressure ≥110 mmHg on 2 occasions at least 4 hours apart (unless antihypertensive therapy is initiated before this time)
Thrombocytopenia (platelet count <100,000/microL)
Impaired liver function as indicated by liver transaminase levels at least twice the normal concentration or severe persistent right upper quadrant or epigastric pain unresponsive to medication and not accounted for by alternative diagnoses, or both
Progressive renal insufficiency (serum creatinine concentration >1.1 mg/dL [97 micromol/L] or doubling of the serum creatinine concentration in the absence of other renal disease)
Pulmonary edema
Persistent cerebral or visual disturbances
Eclampsia: A generalized seizure in a pt with preeclampsia that cannot be attributed to other causes.
HELLP syndrome: hemolysis, elevated liver enzymes, low platelets. Hypertension may be present (HELLP in such cases is often considered a variant of preeclampsia).
Chronic (pre-existing) hypertension: hypertension diagnosed or present before pregnancy or on at least 2 occasions before 20 weeks of gestation. Hypertension that is first diagnosed during pregnancy and persists for at least 12 weeks postpartum is also consider chronic hypertension.
Blood pressure criteria during pregnancy are:
Systolic ≥140 mmHg and/or diastolic ≥90 mmHg
Prepregnancy and 12 weeks postpartum blood pressure criteria are:
Stage 1 – Systolic 130 to 139 mmHg or diastolic 80 to 89 mmHg
Stage 2 – Systolic ≥140 mmHg or diastolic ≥90 mmHg
Chronic HTN with superimposed preeclampsia*:
Any of these findings in a patient with chronic hypertension:
A sudden increase in blood pressure that was previously well-controlled or an escalation of antihypertensive therapy to control blood pressure
New onset of proteinuria or a sudden increase in proteinuria in a patient with known proteinuria before or early in pregnancy
Significant new end-organ dysfunction consistent with preeclampsia after 20 weeks of gestation or postpartum
*Precise diagnosis is often challenging. High clinical suspicion is warranted given the increase in maternal and fetal-neonatal risks associated with superimposed preeclampsia.
Chronic hypertension with superimposed preeclampsia with severe features:
Any of these findings in a patient with chronic hypertension and superimposed preeclampsia:
Systolic blood pressure ≥160 mmHg and/or diastolic blood pressure ≥110 mmHg despite escalation of antihypertensive therapy
Thrombocytopenia (platelet count <100,000/microL)
Impaired liver function as indicated by liver transaminase levels at least twice the normal concentration or severe persistent right upper quadrant or epigastric pain unresponsive to medication and not accounted for by alternative diagnoses, or both
New-onset or worsening renal insufficiency
Pulmonary edema
Persistent cerebral or visual disturbances
A reduction in blood pressure early in pregnancy is a normal physiologic occurrence. For this reason, women with chronic hypertension may be normotensive at their first few prenatal visits. Later in pregnancy, when their blood pressure returns to its prepregnancy baseline, they may appear to be developing preeclampsia or gestational hypertension if there are no documented prepregnancy blood pressure measurements.
BP: blood pressure.
* Blood pressure should be elevated on at least two occasions at least four hours apart. However, if systolic pressure is ≥160 mmHg or diastolic pressure is ≥110 mmHg, confirmation after a short interval, even within a few minutes, is acceptable to facilitate timely initiation of antihypertensive therapy.
¶ The onset of preeclampsia and gestational hypertension is almost always after 20 weeks of gestation. Preeclampsia before 20 weeks of gestation may be associated with a complete or partial molar pregnancy or fetal hydrops. Postpartum preeclampsia usually presents within two days of delivery. The term "delayed postpartum preeclampsia" is used for signs and symptoms of the disease leading to readmission more than two days but less than six weeks after delivery.
Δ Significant proteinuria is defined as ≥0.3 g in a 24-hour urine specimen or protein/creatinine ratio ≥0.3 (mg/mg) (34 mg/mmol) in a random urine specimen or dipstick ≥1+ if a quantitative measurement is unavailable.
◊ Almost all women with the new onset of hypertension and proteinuria at this gestational age or postpartum have preeclampsia, but a rare patient may have occult renal disease exacerbated by the physiologic changes of pregnancy. An active urine sediment (red and white cells and/or cellular casts) is consistent with a proliferative glomerular disorder but not a feature of preeclampsia. Women with chronic hypertension who had proteinuria prior to or in early pregnancy may develop superimposed preeclampsia. This can be difficult to diagnose definitively, but should be suspected when blood pressure increases significantly (especially acutely) in the last half of pregnancy/postpartum or signs/symptoms associated with the severe end of the disease spectrum develop.
§ Photopsia (flashes of light), scotomata (dark areas or gaps in the visual field), blurred vision, or temporary blindness (rare); severe headache (ie, incapacitating, "the worst headache I've ever had") or headache that persists and progresses despite analgesic therapy; altered mental status. Seizure occurrence upgrades the diagnosis to eclampsia.¥ The differential diagnosis of preeclampsia with severe features includes but is not limited to:
Antiphospholipid syndrome
Acute fatty liver of pregnancy
Thrombotic thrombocytopenic purpura (TTP)
Hemolytic uremic syndrome (HUS)
The laboratory findings in these disorders overlap with those in preeclampsia with severe features. (Refer to table in the UpToDate topic on the clinical manifestations and diagnosis of preeclampsia.) The prepregnancy history, magnitude and spectrum of laboratory abnormalities, and additional presence of signs and symptoms not typically associated with preeclampsia help in making the correct diagnosis, which is not always possible during pregnancy.
In addition, a variety of medical disorders may be associated with hypertension and one or more of the signs and symptoms that occur in women with preeclampsia with severe features. These patients can usually be distinguished from patients with preeclampsia by taking a detailed history, performing a thorough physical examination, and obtaining relevant laboratory studies.‡ In contrast to preeclampsia, gestational hypertension is not associated with end-organ involvement, so neither proteinuria nor the symptoms or laboratory findings of preeclampsia are present.
#OB#OBGYN#birth control#gestational HTN#preeclampsia#eclampsia#breastfeeding#gestational diabetes#fetal heart tracing#FHT
2 notes
·
View notes
Last Seen Blogs

otherpeoplsheartache
Previously On Other People's Heartche...
andyhoneybee
Untitled

bitter-anxiety
BUBBLEGUM BOY

sarajocasta
Sara's Shameful Secrets

rocketwerks
Rocket Werks