#we also did some blood and urine analysis
Text
2nd day of class and we're already helping during surgeries lmaooooo
#i mean she sid warn us that they were SHORT on staff and that the sooner we help the better#i just wasn't expecting actually having to do things during surgeries lol#the cat was super super good so that made having to restrain her easy thank fuck#and then I had to do a subcutaneous injection#and the girl is already filling us on the clinics drama lmaoo#it was a simple surgery though removing a tumour#we also did some blood and urine analysis#fun day tbh
0 notes
Text
Is low kidney Function (eGFR) a Sign of kidney Failure? | Zyla Health
Our body is a complex creation with multiple processes and organs functioning altogether. From a small cell, tissues are formed, and from tissues, our organs are formed.
Each and every organ is designed to perform a particular function in our body. Lungs help in breathing, the heart pumps the blood to the whole body, and kidneys filter our blood and remove toxins from our body.

We know that all these organs are important for our survival. But have you ever wondered what will happen if even a slight change in their function will occur? All these organs are interconnected and if even one of them will not be able to function properly, your whole body can be affected.
If your body has low kidney function, it leads to the accumulation of waste in our body. As a result, these toxins and waste products can deposit in different parts of the body. This can lead to swelling and reduced functioning of other organs.
Let’s discuss how the kidney functions in your body and what will happen to your body in conditions of low kidney function. Is it a sign of kidney failure? Before jumping into low kidney function, we will try to understand what a kidney is…
What are kidneys?
Kidneys are bean-shaped organs, located in the abdomen towards the back. The kidneys are similar to water purifiers. They are the filtering system of your body. The kidneys filter blood, remove all the waste materials from your blood and excrete these waste materials in your urine.
Nephrons are the small building blocks of the kidney. They are the main filtering unit of the kidney, which performs the major functions of purifying the blood.
Did you know?
Kidneys are almost the size of your fists and each kidney has about 1 million nephrons.
Now you know how the kidney works in the filtration process which further leads to the formation of urine and excretion of the same from your body, we will now discuss the function of the kidneys in your body.
Have you taken any recent kidney function blood tests? Reach out to us at Zyla.in or the Zyla app for a comprehensive analysis of blood test reports and to keep a check on signs of kidney failure.
Functions of kidneys
1. REMOVAL OF WASTE PRODUCTS
It removes all the waste products and excess fluid from the body. It removes two major unwanted products from your body which include uric acid (a breakdown product of nucleic acid) and urea (a breakdown product of proteins).
2. REABSORPTION OF ESSENTIAL NUTRIENTS
It helps in the reabsorption of various nutrients which are essential for your body, which includes amino acids, glucose, sodium, potassium, chloride, and bicarbonate ions.
3. MAINTENANCE OF PH
In your body, a slight change in the pH is not acceptable, so maintaining an appropriate pH is very important. The kidney plays an important role in maintaining the pH of the body by absorbing or excreting the electrolytes as per the need of the body.
4. MAINTAINS HYDRATION
Your body requires a certain amount of water to function properly. Kidney keeps a check on this balance. If the water level decreases in the body it increases the water absorption from urine to prevent dehydration.

5. REGULATES
BLOOD PRESSURE
The kidneys maintain the appropriate blood pressure in your system. If the blood pressure falls below the normal range, it increases the absorption of sodium chloride (salt) and water, which increases the blood pressure.
6. RELEASE HORMONES
It produces hormones that are essential for your body. For example, Calcitriol is a hormone produced by the kidney that converts the Vitamin D taken through supplements or sunlight into an active form that can be easily absorbed.
It also produces Erythropoietin, which controls the production of Red blood cells.
You have seen that the kidney plays a vital role in your body, especially in the case of filtration. But, sometimes this filtration is affected by certain factors and if you do not keep a check on this filtration process, it can lead to some serious damage to your system.
To check the functioning of kidneys or a sign of kidney failure one of the parameters is the estimated glomerular filtration rate (eGFR). So before considering the factors and treatment, you will first learn what eGFR is!
What is the Estimated Glomerular Filtration Rate (eGFR)?
The glomerulus is a part of the nephron in the kidneys. It is the first filter of the blood that moves through the kidney.
The eGFR measures the amount of blood that is filtered by these glomeruli in a minute.
It is one of the parameters used to check the proper functioning of the kidneys.
There are several methods used to measure the eGFR, but the most common method is to calculate the eGFR with the help of creatinine levels.
Creatinine is a waste product formed by your muscles that is removed from the body through the kidneys.
Calculating the amount of creatinine eliminated by the kidneys helps in determining the eGFR.
Now that you know what eGFR is, let us look at the risk factors of low eGFR!
Risk Factors of Low Estimated Glomerular Filtration Rate
Some risk factors of low eGFR include:
1. DIABETES
In the case of some diabetic patients, blood sugar levels can increase. These high levels can clog the filtering vessels or make them narrow with time. As a result, the kidneys are not able to filter the desired amount of blood and this can result in low eGFR.
2. HYPERTENSION
Persistent high blood pressure can make the arteries around the kidney weaken, narrow, or harden. Hence, these damaged arteries are not able to deliver enough blood to the kidneys, ultimately leading to low eGFR.
3. FAMILY HISTORY OF KIDNEY FAILURE
There are more chances of low kidney function and signs of kidney failure if you have any family history of kidney failure or any chronic kidney disease.
Do you have any of the above risk factors or a family history of kidney disease? Reach out to us at Zyla.in or the Zyla app. We provide holistic personalized 24*7 preventative care for kidney health and would love to work with you to help you achieve your health goals.
We have discussed the major risk factors of low eGFR. So, in these cases, special care and precautions are suggested to be followed. Now, you will look at the causes of low eGFR, so that you can keep them in mind for better kidney function.
Causes of Low Estimated Glomerular Filtration Rate
Some of the causes of low eGFR include :
High Blood Sugar levels: If the blood sugar levels are high, over time it can affect kidney function. The elevated blood sugars can cause the blood vessels in the kidney to narrow and lead to reduced filtration.
High Blood Pressure: High blood pressure affects the blood flow to the kidneys, which leads to decreased filtration process and low kidney function.
Kidney stone: The stones in the kidneys can block the flow of urine resulting in obstruction and low kidney function.
Dehydration: It is very important for your system to maintain an adequate amount of water in your body. If you do not drink enough water, the rate of filtration slows down and this can lead to low eGFR.
Smoking: Frequent smoking can damage the kidneys over time. It harms the blood vessels and affects the flow of blood to the kidneys. It also increases the risk of developing chronic kidney disease.
Obesity: In the case of obese people, kidneys have to function more than in normal people. Over time, this extra work can lead to low eGFR.
Older age: Age is one of the major factors that influence kidney functioning. In the case of older people, kidney function normally decreases with time.
Exercise: During intense exercise, the renal blood flow is reduced because the breakdown of muscle mass increases.
For further reading on kidney health and uric acid, read our blog on the 4 risk factors of high uric acid.
We will now discuss the normal ranges of eGFR so that you can get a better idea of what to look for in order to know if our kidneys are functioning appropriately.
Normal Range of eGFR in an Estimated Glomerular Filtration Rate Test
The normal range of eGFR is mostly above 60 mL/min/1.73 m2.
If the levels are mostly below 60 mL/min/1.73 m2 for more than 3 months, then it is considered as a sign of one of the stages of Chronic Kidney Disease (CKD).
If the levels are below 15 mL/min/1.73 m2 then it is considered a sign of kidney failure and requires immediate attention.
In an estimated glomerular filtration rate test, these ranges vary from lab to lab and also change with age, weight or gender.
We have discussed the causes and risk factors of low eGFR. Let’s take a look at the symptoms of the same so that we can plan to get our eGFR checked if we experience most of these symptoms.
Symptoms of Low Estimated Glomerular Filtration Rate
The symptoms of low eGFR include:
Nausea and vomiting
Loss of appetite
Fatigue
Swelling of ankles and feet
Muscle weakness and cramps
Urinating more or less than usual
Persistent itching
Chest pain
Shortness of breath
High blood pressure
Have you experienced any of these symptoms? Reach out to us at Zyla.in or the Zyla app. We provide expert care and support 24X7 including analysis of vitals and lab reports as well as senior doctor and nutritionist consultations to create a personalized health plan for you.
After discussing the symptoms of a low eGFR, we will now throw light on some of the measures that can help us protect our kidneys and can improve their functioning.
Prevention of Low Estimated Glomerular Filtration Rate
As we all know, “Prevention is better than cure”. You will now see some of the methods to prevent low eGFR or to improve the same.
Controlling blood sugar: To prevent slow damage to kidneys with time due to high blood sugar levels, try to achieve good glycemic control. This can be achieved by a balance of medicine and lifestyle modifications.
Controlling blood pressure: As already discussed, high blood pressure can affect the eGFR, so in case of hypertension always try to keep your blood pressure under control.
Protein in diet: Avoid eating too much protein in your diet because it can increase the workload on the kidneys. Prefer protein from plant sources and be thoughtful of animal protein intake.
Keep a check on salt in your diet: Be mindful of the amount of salt in your diet, as it affects blood pressure. It is advised to avoid packaged and processed foods as they contain high amounts of sodium and other preservatives.
Smoking: We already have discussed that smoking can cause low kidney function. It is advised to take steps to quit smoking in order to protect your kidney health.
Limit the alcohol intake: Alcohol also increases the load on kidneys and the kidneys have to work more than the normal in case of alcoholic people. So, try to limit the consumption of alcohol.
Manage the medical condition: If you have any chronic disease that can affect kidney function with time, consult your healthcare professional and discuss with him the plan of early treatment or prevention methods accordingly.
Healthy weight: If you are overweight/ obese try to change your diet and lifestyle. Increase your daily physical activity, You can consult a nutritionist in order to make better dietary decisions.
For more information on kidney health, read our blog on the best treatment for high creatinine!
It is important for us to take care of each and every organ of our body. The kidney is a vital organ in the body and low kidney function can affect the quality of your life in a serious way and lead to other health conditions as well.
Therefore, it is vital to get our regular health check-ups done to prevent or catch any signs of kidney failure and critical conditions like different stages of chronic kidney disease in time. We know that “Health is wealth”, and it’s beneficial to include lifestyle changes that can improve our health as early as possible.
We strongly recommend consulting your doctor, in case of any questions or concerns regarding your health. It is important to seek medical care at the right time, in order to prevent long term health complications.
If you’re seeking help to improve your health and want to better manage your kidney health, you can download the Zyla app or visit our website Zyla.in and check out the Kidney Care Program which is tailored specifically for chronic kidney disease and low estimated glomerular filtration rate.
Zyla has a team of 50+ medical experts who can provide personalized treatment through a holistic approach. Start your health journey today!
Stay strong! Stay healthy!
Connect with us:
Subscribe to our Youtube channel: https://bit.ly/2o19OzE to watch videos on health and health-related conditions.
Find us on Facebook: https://www.facebook.com/zylahealth
Find us on Instagram: https://www.instagram.com/zylahealth/
Visit our website: https://www.zyla.in/
Talk to us on WhatsApp — https://goo.gl/kjofP
For more information, you can visit us
https://blog.zyla.in/is-low-kidney-function-egfr-a-sign-of-kidney-failure-zyla-health-28aa21feef19
0 notes
Text
scrubs - 2.
pairing: doctor!sebastian stan x biomedical scientist!reader
warnings: angst, mentions of death. if you are not comfortable with these warnings please dni.
< previous chapter
- Where are you going? - Miriam rose her head from the work bench as Y/N took her gloves and googles off, disposing of both in the yellow bin. - Y/N, where are you going? Don’t leave me alone with the trainees.
- I’m going to get dinner. No eating in the lab, remember?
- Urgh, couldn’t you have gone to dinner when Michael was here? You’re leaving me alone with the trainees ... and the ask so many questions. - she whispered the last part, afraid the trainees would hear her and hit her over the head with their very heavy portfolios. - I’m going next.
- Hour break, don’t you dare page me. - she pointed her finger menacingly at Miriam before clocking out and heading out for dinner. If they had told her during her sleepless nights spent revising for her least favourite modules the most exciting time of her shifts would be the bland food served by the hospital cafeteria, she would’ve just become a pharmaceutical researcher. Yet again, you need to start at the bottom if you want to get to the top and Y/N was more than ready to climb that moment.
She pressed the button for the lift, leaning against her own hand as she tried to wake herself up. Turns out studying and staying up all night applying for PhD projects and then coming to work at 7AM is not the way to go for energy. Luckily, the black tea she had drank this morning had managed to keep her awake, however the caffeine was starting to slowly leave her system and she still had a few more hours awaiting her. As she was about to fall asleep while waiting for the lift to make it to the lower floors, she heard her name being called out.
- Y/N? - she looked to her side to see Peter standing next to her. They’ve known each other since freshers and if there was someone who was always wide awake during twenty four hour shifts it was him. He worked currently in the clinical biochemistry laboratory, mostly coming over to visit Y/N whenever they were working on cardiac infection cases together. - I looked at the file you gave me. CRP is actually present but quite low, could be recovery phase from an infection. My guess with abdominal pain would be a UTI.
- You reckon it hit recovery phase by itself?
- Listen, some pharmacy assistant might’ve given him antibiotics. Who knows but I’d get a urine analysis, do some cultures and see how’s it going but from my point of view, it’s in recovery phase.
- You’re a superstar, Peter. - she hugged him just as the lift doors opened. - You’re going up?
- Yeah, it’s dinner time. I think they’re serving meatballs today. Exciting stuff. - the two stepped onto the lift. - Miriam said Dr. Stan came down today. You’re still giving him hell?
- I am not giving him hell. He’s just constantly sending samples either mislabelled or misplaced and he expects me to lecture his nursing staff about it.
- I don’t know, Y/N. Back at university you spent 2 hours arguing an answer with a lecturer, I just think you like arguing. - he chuckled as the doors opened onto the floor where the cafeteria was. - Or maybe you like arguing with Dr. Stan.
Before she could complain about the snide comment, Peter took to having a chat with a nurse he was particular sweet on leaving Y/N with her mouth open ready to argue and a finger pointed at him. She rolled her eyes, collecting herself as she released her hair from the ponytail which held it safely high up so her scalp could rest for a few hours before it had to go back up. Walking into the green lit cafeteria, the room was filled with half asleep medical staff digging through the bland food like mindless zombies. She did not blame them, she too sometimes would switch off her brain during breaks but lately all the free time she had was dedicated to applications after applications, despite the fact she kept getting rejections every single day.
The scientist grabbed a worn out plastic blue tray, getting a batch on weirdly shaped meatballs from the cafeteria lady as well as some odly too yellow noodles. Hey, it is food, her brain told her as she grabbed a diet Pepsi and a slice of apple pie which was the only eatable dessert around.
- Didn’t you owe me dinner?
- You almost made me drop my tray. - she gave the resident doctor a dirty look, gripping tighter onto the tray. - And I’ll be damned if I ever owe you dinner but I do have your blood culture results and we did sort out your weird infection case.
- It is not my infection case.
- Fine, your patient’s infection case. God heavens if any interns knew that you had an infection, that way they wouldn’t fawn over you. - she rolled her eyes at him, setting her tray in the first table she came over. He did the same, placing his tray right in front of hers before sitting in the metal chair with a cocky grin. - Go away, I’ll send over the report to your office.
- Have you not figured it out yet and trying to buy yourself more time? Or are you trying to escape the dinner date you set up with me?
- That might work on your interns but not on me, Stan. Besides, it is an infection.
- But there’s no worrying levels CRP besides, what about the abdominal pain? Surely CRP and white blood cells would be off the roof.
- Okay, since you probably missed Biochemistry in med school I will explain it to you. The CRP levels are high during initial phases and lower down during resolve. Your patient is probably on recovery phase already. Recovery means it is fixing itself. Do you need me to explain CRP to you?
- If you pulled that out with any other doctor, you would’ve gotten told off.
- Other doctors don’t ask me stupid questions. - she pointed her fork at him. - Dr. Mackie never sends the samples in the wrong vials.
- What about the blood cultures?
- Congratulations, Dr. Your patient is not septic. It’s most likely localised but I’d suggest ordering some X-rays if you wanna localise where it actually is. I wash my hands of your troubles. - she shrugged, wrapping her fork in the spaghetti laying on her plate. - Need anything else, Dr. Stan?
- I remember being promised a dinner date.
- You should get your ears checked, the only thing I promised you was data and you’re lucky I also gave you a data ana ... - the scientist was interrupted by her pager beeping loudly against her belt. She grumbled, looking down at her belt with a look that would scare anyone. - Duty calls.
- How convenient it went off now.
- Unlike you, Dr. Stan, I have a team to lead.
- Sounds complicated, Y/N. You sure you don’t need a babysitter?
She turned around as she was about to leave, raising his middle finger at him before rushing down the hall as her pager beeped uncontrollably. So much for not paging her during dinner time. Someone better be dying, she thought to herself as she slide her card into the door slot to get access. What she came in contact with was not what she was expecting from a laboratory of trained professionals. Miriam was holding one of the trainees head forward whose nose was bleeding all over her worktop bench.
- Miriam, what the fuck?
- Don’t look at me. Thomas ... - she squinted at the boy whose head she was holding forward. - Started bleeding when he smelled the knee aspiration.
- Oh no. - Y/N put some gloves on before walking over to the two. - Okay, Miriam call a code orange. I’ll take Thomas upstairs and get him sorted.
- It’s so stinky.
- I know. - Y/N handed them two cotton balls from the jar to her left. - Put them up your nose.
What would be a day in the laboratory if a newbie didn’t either faint or got nose bleeds from samples? Definitely not a day in her laboratory. She looked around the busy hospital grounds, trying to find any free, available nurses but they were all overworked. No wonder why, whenever midnight rolled around, people started coming in left and right from club brawls and the grounds were always a nightmare.
- What you got there, Miss Y/L/N? Is this how you lead your team?
- Fuck off, Stan. I do not have time to listen to your comments, I need to find a nurse.
- What happened, kid? - Sebastian looked to the 19 year old medical laboratory assistant holding cotton against his nose. - Lab that bad? Come on, I’ll fix you up.
- Thanks. - she mumbled, following the two men into one of the free areas. Thomas sat on the table while Sebastian pulled up a chair to sit in, Y/N remaining up on her feet.
- So kid, what happened? Y/N rough you up too much?
- He got a nosebleed from the smell of a knee fluid from an aspiration. - Y/N replied to him, much to Thomas delight who felt more than embarrassed about the situation he was in. - Is this what you’re doing now, Dr. Stan? Minor cases? Did the chief of medicine finally realised you’re unqualified?
- No. - he spoke as he pointed out his light at the trainees nose, to look for any specific damage. - One of my patient’s in critical care but it seems to have stabilised for now at least.
- Oh ... sorry. What happened to them?
- Sepsis. - he turned off the lights. - Listen kid, it’s nothing to bad. Just stay sat here and firmly pinch the soft part of your nose, just above your nostrils, for about 15 minutes. Don’t forget to lean forward and breathe through your mouth. Me or one of the nurses will come check on you after to see if it has improved but so far, so good.
- I’ll return to the lab. Page me when you’re ready to return, okay? - she gave the young starter a kind smile before pulling the curtains and letting him be. Unfortunately for her, Stan would not let her be. - Keep it.
- How weak are your staff? How are they gonna react to when they actually see infected body parts?
- I said keep it. - she crossed her arms, ready to leave and return to the laboratory until she remembered something. She turned around on her heel, passive aggressive smile on her lips as she leaned her head on her shoulder. - Also, Dr. Stan, the infected tissue samples you sent us had the wrong birthdate on them.
- C’mon Y/N.
- They’re on hold until you speak with the laboratory manager about them. Good luck.
He opened his mouth to fight with her but she had already gotten into the elevator. The rest of her shift was pretty uneventful with her and a few of her colleagues having to pick up the pace to get everything sorted before they left. Miriam and her fiance left first at 1AM leaving Y/N to count the minutes til 2 AM rolled around. Once the clock read 2AM, like a speeder, she was out of that laboratory and into the elevator before anyone could call her. Walking to her parking spot, the sky was dark, the lot light by harsh yellow barely brightening. As she walked over to the second handed baby blue Fiat 500, she noticed someone hunched over and sat on the top of a black new model Audi, smoke coming out from his cigarette. Normally, she would’ve just avoided it and gotten into her car to go home but the turquoise scrubs were much too familiar at this point.
- Dr. Stan? - her boots hit the gravel as she stood just a few meters away from him. - Do they not teach you in medical school that smoking increases the chance of lung cancer?
- Not now, Y/N. - no sarcastic remark? That was a new one. He threw the cigarette butt onto the ground once it was all over, feet rubbing it against the gravel. - Not now.
- I thought your shift finished at 1:30? Pulling overtime hours? Someone needed your assistance? Death time?
- My septic patient died. - she immediately wished she hadn’t said anything. Death was not something she particularly dealt with. Surely, some results were awful, specially in cases of ultra resistant bacteria showing up in the blood but that’s what they were, results. She didn’t see the patient, in all honesty all she would know the patient would be by a barcode number. - Sepsis quickly lead to organ failure. I don’t understand ... she was getting better.
- Sepsis is unpredictable. You did the best you could do.
- And you’d know? All you do is be in the laboratory and do tests. What would you know about it?
- Okay ... - she put her hands on her hips. - Are you on any antibiotics, prescription pain killers, sedative drugs, statins or any antidepressants?
- I don’t see the point.
- The bar nearby has a discount for hospital staff. It’s only a five minute walk and everyone else is so miserable, you don’t feel bad about being miserable.
- I’m not going to the bar in my scrubs, Y/N.
- If you’re okay wearing those ... - she pointed at his scrubs. - Then you are okay wearing them at the bar.
She was right, the bar did look miserable. Not in a miserable way which would require regulation to shut down the place but miserable in a way one would just be at home wallowing in their pity with a pint of beer and right now that was all he needed. He sat in a sticky red booth, in front of her with a pint of beer while she picked a cocktail from the menu.
- You don’t seem like the type of girl who’d come here.
- And I’m not but they sell really cheap burgers at lunchtime. - she put her hand under her chin. - Besides, I’ve done this before.
- When did you convince someone to come to the bar because their patient flat lined?
- You know Dr. Liam Watts?
- Surgery residency? I’ve heard about him before. - her lips tensed in a straight line as she leaned her head on her shoulder. - No. You’ve been here with Bucktooth Watts before?
- Yeah... even after he clearly needed support after he couldn’t save his first patient, he still decided to take me on a date here.
- I’m sorry, you dated Bucktooth Watts? - he chuckled, downing whatever was left of his pint, signalling the bartender to bring him another one.
- This is why we don’t hang out. He’s not bucktoothed.
- Sure, sure. I see the appeal, I mean over Christmas at least you have someone to cut the carrots.
The night went onwards with a bunch of maybe irresponsible drinking. Y/N was two mojitos in and she was already tipsy and giggling like a school girl, not really used to drinking. Sebastian was in the same state as her, trying not to laugh at everything as they stepped outside to grab a taxi. At least both of them were conscious enough to decide not to drive.
- No, you did not get locked in the vroom cupboard during your residency. - she held her belly as she laughed.
- I did and my senior doctor did not notice I was gone. I was stuck there for 5 hours.
- Oh god. - she held herself against the wall. - I always knew you were a clutz. You know, you’re the only doctor who hasn’t told off his nurses about the blood bottles.
- Can I tell you a secret? - he whispered mid laughter. - I am afraid of them.
- Oh my god. - she held her hand on his shoulder covering her mouth with the other one. - See, this is why I constantly argue with you. You’re soft, doctor.
- Arguing with you is the best part of my day. You look really hot when you’re telling me off.
- You look terrible when I tell you off. - the two of them stopped laughing, looking into each other eyes for the first time since they’d been out of the laboratory. Maybe it was the alcohol but at that moment, the best idea to the two of them was to lean towards each other, his hands grasping each side of her waist as they connected the space between them, getting together into a hot long kiss.
#sebastian stan#sebastian stan au#sebastian stan/reader#sebastian stan x reader#sebastian stan/you#sebastian stan x you#sebastian stan x y/n#sebastian stan/y/n#sebastian stan doctor au#doctor!sebastian stan#sebastian stan imagine
136 notes
·
View notes
Text
We have a pt who has rhabdomyolysis from taking a statin and being on the floor for 3 days. She's old, so she had muscle breakdown. The attending is Dr. Giraldo, who is really nice and awesome. He asked me what urine test you use to diagnose rhabdo and I totally forgot about myoglobinuria so I said I wasn't aware. He told me to look it up. Then after we were rounding for a bit, my brain remembered myoglobinuria! So I told him. But now I want to look up the details of diagnosing rhabdo so I can present to him tomorrow. But we also have a pt with CKD who may have kidney stones and the attending and the resident didn't realize that you can diagnose a kidney stone with a non-contrast CT. I remembered learning that last year during my emergency medicine rotation. They had ordered a KUB because they thought you would need to use contrast for the CT and so they didn't want to get the CT because the contrast would hurt the pt's kidney. But you don't use contrast to diagnose nephrolithiasis with CT. So at least I remembered something! This is from UpToDate:
●The clinical manifestations of rhabdomyolysis include myalgias, weakness, red to brown urine due to myoglobinuria, and elevated serum muscle enzymes (including creatine kinase [CK]). The degree of myalgias and other symptoms varies widely, and some patients are asymptomatic. Fever, malaise, tachycardia, and gastrointestinal symptoms may be present. Muscle swelling may occur with rehydration.
This pt was actually tachycardic in the ED. So that tracks.
●The laboratory findings that characterize rhabdomyolysis include an acute elevation in the CK and other muscle enzymes and a decline in these values within three to five days of cessation of muscle injury. The other characteristic finding is the reddish-brown urine of myoglobinuria, but this finding is often absent because of the relative rapidity with which myoglobin is cleared. The serum CK is generally entirely or almost entirely of the MM or skeletal muscle fraction, although small amounts of the MB fraction may be present.
●Other manifestations include fluid and electrolyte abnormalities, many of which precede or occur in the absence of acute kidney injury, and hepatic injury. Hypovolemia, hyperkalemia, hyperphosphatemia, hypocalcemia, hyperuricemia, and metabolic acidoses may be seen. [I think the pt also had hypocalcemia, but it wasn't true hypocalcemia because the albumin was low, so her corrected Ca2+ was in the normal range based on the lab values at the hospital; she did have acidosis too I think]. Hyperkalemia may result in cardiac dysrhythmias. Later complications include acute kidney injury (AKI), hypercalcemia, compartment syndrome, and, rarely, disseminated intravascular coagulation.
●We diagnose rhabdomyolysis in a patient with an acute muscular illness or injury based upon a marked acute elevation in serum CK; the CK is typically at least five times the upper limit of normal and is frequently greater than 5000 international units/L. Key diagnostic laboratory studies include the creatine kinase and urinalysis, including dipstick and microscopic evaluation. Myoglobinuria (present in 50 to 75 percent of patients at the time of initial evaluation) results in a positive test for blood on the urine dipstick but without red blood cells on the microscopic examination of the urine. And for this pt, the UA showed a small amount of blood, so that could have been myoglobin in the urine, but we didn't order a microscopic analysis. She also has a UTI, so that could be from the UTI as well. Also, the other day Dr. Agarwal asked how long you treat UTIs. When in the hospital, you can treat with ceftriaxone until the pt has clinically improved.
●The differential diagnosis depends upon the combination of findings present. It includes myocardial infarction, other causes of red or brown urine, inflammatory myopathy, and local causes of pain, such as deep vein thrombosis or renal colic.
The characteristic triad of complaints in rhabdomyolysis is muscle pain, weakness, and dark urine. Additional symptoms that are more common in severely affected patients include malaise, fever, tachycardia, nausea and vomiting, and abdominal pain. Altered mental status may occur from the underlying etiology (eg, toxins, drugs, trauma, or electrolyte abnormalities).
The hallmark of rhabdomyolysis is an elevation in CK and other serum muscle enzymes. The other characteristic finding is the reddish-brown urine of myoglobinuria, but because this may be observed in only half of cases, its absence does not exclude the diagnosis. Routine lab tests, including complete blood count (CBC), erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP), vary greatly depending on the underlying cause of rhabdomyolysis. Infections and crush injuries are associated with marked elevation of the acute phase reactants and peripheral white blood cell (WBC) count, while these markers of inflammation would likely be normal or only minimally raised in patients with other etiologies, such as drug-induced or electrolyte derangements.
Serum CK levels at presentation are usually at least five times the upper limit of normal, but range from approximately 1500 to over 100,000 international units/L. The mean peak CK reported for each of a variety of different causes and for patients with both single and multiple causes ranged from approximately 10,000 to 25,000 in the largest series; exceptions were the three patients with malignant hyperthermia, whose values averaged almost 60,000.
I googled the normal serum CK level:
In a healthy adult, the serum CK level varies with a number of factors (gender, race and activity), but normal range is 22 to 198 U/L (units per liter). Higher amounts of serum CK can indicate muscle damage due to chronic disease or acute muscle injury.
The CK is generally entirely or almost entirely of the MM or skeletal muscle fraction; a small proportion of the total CK may be from the MB or myocardial fraction. The presence of MB reflects the small amount found in skeletal muscle rather than the presence of myocardial disease. Elevations in serum aminotransferases are common and can cause confusion if attributed to liver disease. In one study, aspartate aminotransferase (AST) was elevated in 93.1 percent and alanine aminotransferase (ALT) in 75 percent of rhabdomyolysis cases in which the CK was greater than or equal to 1000 units/L. In only one instance was the ALT greater than the AST, although the AST declines faster than the ALT as the rhabdomyolysis resolves, such that the two may equalize after a few days.
The serum CK begins to rise within 2 to 12 hours following the onset of muscle injury and reaches its maximum within 24 to 72 hours. A decline is usually seen within three to five days of cessation of muscle injury. CK has a serum half-life of about 1.5 days and declines at a relatively constant rate of about 40 to 50 percent of the previous day's value. In patients whose CK does not decline as expected, continued muscle injury or the development of a compartment syndrome may be present.
Urine findings and myoglobinuria — Myoglobin, a heme-containing respiratory protein, is released from damaged muscle in parallel with CK. Myoglobin is a monomer that is not significantly protein-bound and is therefore rapidly excreted in the urine, often resulting in the production of red to brown urine. It appears in the urine when the plasma concentration exceeds 1.5 mg/dL. Visible changes in the urine only occur once urine levels exceed from about 100 to 300 mg/dL, although it can be detected by the urine (orthotolidine) dipstick at concentrations of only 0.5 to 1 mg/dL . Myoglobin has a half-life of only two to three hours, much shorter than that of CK. Because of its rapid excretion and metabolism to bilirubin, serum levels may return to normal within six to eight hours.
Thus, it is not unusual for CK levels to remain elevated in the absence of myoglobinuria. In rhabdomyolysis, myoglobin appears in the plasma before CK elevation occurs and disappears while CK is still elevated or rising. Therefore, there is no CK threshold for when myoglobin appears. As above, rhabdomyolysis does not occur unless CK is elevated five times or more above the upper limit of normal. Routine urine testing for myoglobin by urine dipstick evaluation may be negative in up to half of patients with rhabdomyolysis. Pigmenturia will be missed in rhabdomyolysis if the filtered load of myoglobin is insufficient or has largely resolved before the patient seeks medical attention due to its rapid clearance.
Both hemoglobin and myoglobin can be detected on the urine dipstick as "blood;" microscopic evaluation of the urine generally shows few red blood cells (RBC) (less than five per high-powered field) in patients with rhabdomyolysis whose positive test results from myoglobinuria. Such testing is not a reliable method for rapid detection of myoglobin if RBC are present or in patients with hemolysis due to its lack of specificity for myoglobin. Hemoglobin, the other heme pigment capable of producing pigmented urine, is much larger (a tetramer) than myoglobin and is protein-bound. As a result, much higher plasma concentrations are required before red to brown urine is seen, resulting in a change in plasma color.
Hypocalcemia, which can be extreme, occurs in the first few days because of entry into damaged myocytes and both deposition of calcium salts in damaged muscle and decreased bone responsiveness to parathyroid hormone. During the recovery phase, serum calcium levels return to normal and may rebound to significantly elevated levels due to the release of calcium from injured muscle, mild secondary hyperparathyroidism from the acute renal failure, and an increase in calcitriol (1,25-dihydroxyvitamin D).
Severe hyperuricemia may develop because of the release of purines from damaged muscle cells and from reduced urinary excretion if acute kidney injury occurs.
●Metabolic acidosis is common, and an increased anion gap may be present. Our pt did have an anion gap and I wondered why. I guess it's because there's more uric acid in the blood.
Acute kidney injury — Acute kidney injury (AKI, acute renal failure) is a common complication of rhabdomyolysis. The reported frequency of AKI ranges from 15 to over 50 percent. The risk of AKI is lower in patients with CK levels at admission less than 15 to 20,000 units/L; risk factors for AKI in patients with lower values include dehydration, sepsis, and acidosis. [Our pt had peed a lot and was on the floor for 2 to 3 days, so she was probably dehydrated, increasing her risk for AKI]. Volume depletion resulting in renal ischemia, tubular obstruction due to heme pigment casts, and tubular injury from free chelatable iron all contribute to the development of renal dysfunction. Reddish-gold pigmented casts are often observed in the urine sediment.
Compartment syndrome — A compartment syndrome exists when increased pressure in a closed anatomic space threatens the viability of the muscles and nerves within the compartment. Compartment syndrome is a potential complication of severe rhabdomyolysis that may develop after fluid resuscitation, with worsening edema of the limb and muscle. Lower extremity compartment syndrome can also be a cause of rhabdomyolysis, as may occur after tibial fractures.
Disseminated intravascular coagulation — Infrequently, severe rhabdomyolysis may be associated with the development of disseminated intravascular coagulation due to the release of thromboplastin and other prothrombotic substances from the damaged muscle.
EVALUATION AND DIAGNOSIS
Indications for diagnostic testing — Diagnostic testing should be performed in individuals with:
●Both myalgias and pigmenturia.
●Either myalgias or pigmenturia, with a history suggesting the presence or recent exposure to a potential cause or event.
●The absence of myalgias and pigmenturia in a clinical setting associated with increased risk for rhabdomyolysis, as symptoms may be vague or absent in up to 50 percent of patients. The diagnosis should be suspected following prolonged immobilization [like our pt who was on the floor for 2 to 3 days], in any stuporous or comatose patient, or in a patient who is otherwise unable to provide a medical history and has one or more of the following:
•Muscle tenderness
•Evidence of pressure necrosis of the skin
•Signs of multiple trauma or a crush injury
•Blood chemistry abnormalities suggesting the possibility of increased cell breakdown, such as hyperkalemia, hyperphosphatemia, and/or hypocalcemia
•Evidence of acute kidney injury
●Acute muscle weakness and marked elevation of creatine kinase (CK).
Diagnostic evaluation — We obtain the following key diagnostic laboratory studies:
●Creatine kinase – In addition to elevation of the CK, other muscle enzymes are typically elevated (eg, aldolase, aminotransferases, lactate dehydrogenase), but such testing is not usually necessary to make the diagnosis. However, elevations in aminotransferases or lactate dehydrogenase may suggest the need for CK testing if it has not been performed in a patient in whom such abnormalities may potentially be due to muscle injury rather than hepatic injury or another cause.
●Urinalysis, including dipstick and microscopic evaluation – Evidence of myoglobinuria should be sought by routine urine dipstick evaluation combined with microscopic examination. Testing of the unspun urine or the supernatant of the centrifuged urine will be positive for "heme" on dipstick if myoglobinuria is present, even if red to reddish brown urine is not evident macroscopically. The visual and microscopic examination of the sediment from a fresh urine specimen is required to exclude the presence of red blood cells (RBC) as the cause of positive testing; RBC in an older specimen may hemolyze over time, confounding the results.
In patients with persistent red to reddish-brown urine, myoglobinuria is suggested when the urine tests positive for heme by dipstick after centrifugation, while the plasma has a normal color and tests negative for heme.
Myoglobinuria lacks sensitivity as a test for rhabdomyolysis; it may be absent in 25 to 50 percent of patients with rhabdomyolysis due to the more rapid clearance of myoglobin, compared with CK, following muscle injury. Myoglobin also decreases rapidly in a similar fashion in patients with renal failure, suggesting a role for extrarenal metabolism and clearance in such patients.
We also obtain the following tests, which may help in prompt recognition of other potentially dangerous manifestations, in differential diagnosis, and in identifying the cause:
●Complete blood count, including differential and platelet count
●Blood urea nitrogen, creatinine, and routine electrolytes including potassium
●Calcium, phosphate, albumin, and uric acid
●Electrocardiography
Additional testing, such as evaluation of suspected metabolic myopathy or toxicology screening for drugs of abuse, depends upon the clinical context.
Diagnosis — We make the diagnosis of rhabdomyolysis in a patient with either an acute neuromuscular illness or dark urine without other symptoms, plus a marked acute elevation in serum creatine kinase (CK). The CK is typically at least five times the upper limit of normal, and is usually greater than 5000 international units/L. No absolute cut-off value for CK elevation can be defined, and the CK should be considered in the clinical context of the history and examination findings.
MANAGEMENT
The major issues in the treatment of patients with rhabdomyolysis include:
●Recognition and management of fluid and electrolyte abnormalities, which should be initiated regardless of renal function and which may prevent severe metabolic disturbances and acute kidney injury
●Identification of the specific causes and the use of appropriate countermeasures directed at the triggering events, including discontinuation of drugs or other toxins that may be etiologic factors
●Prompt recognition, evaluation, and treatment of compartment syndrome in patients in whom it is present
7 notes
·
View notes
Text
A Cautionary Tale? A Love Story? You Decide
It's been one of those rollercoaster weeks, one that began with a great deal of pain, which I tried to ignore at first, so as not to ruin my 17- year old’s already Corona-compromised birthday party. At some point during our 5 p.m. family Zoom celebration, I quietly left the room and went upstairs to lie down, writhe in pain, get back up, bend over, moan, repeat. This continued through the night Monday – and at one point, I remember thinking that labor wasn’t this bad and that I should probably go to the emergency room. In this new world we’re in, that thought was quickly dismissed by one word: COVID. I paced the floor at 3 a.m., alternately moaning and then bopping my head and sort of softly singing what kept running through my head, which was the chorus of The Knack’s 1979 hit song, “My Sharona.” Only my version went “My Corona.” Yes, even while suffering, I’m clever that way.
By Tuesday morning the pain had subsided. I was exhausted however, and slept throughout the day. “Tricia! Drink this! Jesus, she’s burning up.” It was the alarm in my husband’s voice that I responded to more than the command. I sat up, drank the water he was holding out to me, and when I caught my reflection in the mirror over the dresser I had the brief, feverously detached impression of someone who’d sat under a sun lamp for too long. Sun lamp, the words made me almost giggle out loud. Sun-lamp, sun-lamp, sun-lamp…Does anyone even know what that is anymore? A few hours later I had a virtual appointment with my regular GP, during which the decision was made for me to go to the office first thing Wednesday for a full exam. My instructions (my fever-addled brain again added the words “should I choose to accept them” - hehehe), for entering the building would come in the form a text.
My office exam was efficient and thorough. Upon arrival, I called the office and someone met me at a side door. As we were both masked and gloved, we nodded and murmured muffled greetings. Two PAs and an MD palpated my tender abdomen while I stifled screams. They decided that I should have a C-T scan that day, with the expectation that the offending culprit was a kidney stone. As many radiology facilities are currently closed, it took a few hours for them to locate one that would take me. My scan took place at 4:30. I was the last patient of their day.
Fast forward to 6:30 p.m. Wednesday evening. I picked up the call, which was remarkable in itself because anyone who knows me knows how irritating it is that, a) my phone is always on silent mode, and, b) I rarely answer numbers I don’t recognize. It was another doctor from Vanguard, calling to let me know that my C-T scan showed no evidence of kidney stones – “Yay!” BUT, he cut in, it did show acute appendicitis. What I needed to do, he said, was to go directly to the nearest ER.
So here’s where this story really begins, because I was about to get a reality check regarding the difference between the inconveniences of “social distancing” and quite literally, matters of life and death. For those of us who are shuffling around at home in our sweatpants, eating too much, complaining about the buffoonery of our President, laughing at all the funny memes, and who are, to one degree or another, COMPLETELY OBLIVIOUS to the fact that health care workers do not have the luxury of ANY of that, here’s the newsflash: The Corona virus has virtually SHUT down normal operations for hospitals and surgical facilities, so if you’re also laughing in the face of social-distancing guidelines, and just can’t wrap your head around the possibility of contracting this deadly disease, know this too: If you break your arm, or your spouse has a heart attack, or your child’s strange rash won’t go away and you’re just really concerned, good luck. We are NOT in Kansas anymore, peeps.
I considered doing a bit of a negative a rant on the first hospital that I went to here, but perhaps that wouldn’t be fair. “The nearest ER” for me would have been another hospital, but due to their somewhat dubious reputation, we opted to go just a bit farther away. The best thing I can say about that experience was that the safety protocols to enter the ER were impressive. Picture the scene in E.T. where the Hazmat-suited guys from the space program find out about him and “invade” the house in a tunnel of white - then picture the people standing six feet apart outside of say, ShopRite, only these people don’t look so great. They’re kind of bent over, or swaying, or leaning on someone else. Then count your blessings that your gut hurts and you’re not bleeding out…or struggling to breathe.
Three hours later, after they’d reviewed my scans and completed all of the necessary pre-op tests (blood work, EKG, urine analysis), I got the word that most of the ORs were being used as ICUs for COVID patients, and they were only doing “emergent” surgeries. They sent me home with massive doses of antibiotics, and a referral to see their staff general surgeon - outpatient.
I figured they were right, too. Must not be very serious. I was doing well with that notion until the following morning, when I heard the barely concealed shock in the voice of my regular MD.
“Did they see your scans?” his tone serving only to increase my anxiety.
“Yeah. But my appendix hasn’t exploded yet.” I said.
“Ah,” he sighed, “I know things are being handled differently in the ‘current environment,’ but last time I checked, acute appendicitis was emergent.”
Okay, pay attention now, because here’s where it gets really interesting: See if you can answer his parting questions:
“Do you have a general surgeon? Preferably one with their own facility?”
So, do you? And if you do, are you sure they’re even open right now? I sure as hell didn’t (and the name they gave me at the hospital turned out to be for a doctor whose answering machine told me he was not seeing new patients). And the idea that it was now pretty much my problem to solve was a little intimidating – especially for someone who generally needs to be told that they’re sick (enough) or in (enough) pain to seek help—but that’s another story. Now that doctor, who I respect and like a lot, said he’d be trying to find me one, but that I should do my research as well.
My husband and I made a fairly long list of people/places to call, and split it. Those we were able to reach at all offered possible solutions to my dilemma, but each dead-ended pretty quickly. I focused on the task now, trying to ignore what it might mean that the ache in my belly seemed to be spreading down my right leg.
As of this writing, I have yet to hear back from my regular GP and yet, here I sit, post-op, able to get this down mostly because of a Facebook message I sent to one of the nurses in the Belleville Public School district. The only real help I got came from her, a nurse, who responded immediately to an “in-boxed” message, and kept responding for the next hour, sending me the names and phone numbers of doctors (sometimes with their credentials!), links to possible facilities, and words of encouragement. She gave me her personal cell phone number and encouraged me to call it if I had questions and/or to let her know how it was going. I felt like she meant it, too. I also think she was responsible for the first in a series of serendipitous events that just may have saved my life. One of the names she gave me turned out to be the dad of one of my kid’s friends.
At that point, things happened pretty quickly. I called him (at home) and told him my situation. In a matter of 20 minutes, he had my scans and had booked a time slot for me for same-day surgery at Clara Maass. He’s a high-energy, outgoing kind of guy, and although I’d stood on sidelines with him and his lovely wife at many a sports event, I don’t know him well enough, nor did I think it was appropriate to laugh out loud when he laid out the plan: “With everything going on, I just really want to do you – and get you the hell out of there!”
So here I am, more grateful to him than I can possibly express and having some time to consider just how random and crazy and dangerous that whole situation was (turns out, my appendix had begun to perforate after all, and the real fun was just beginning) and how fortunate I am.
But the real heroes here - Oh, and God, aren’t we all a little sick of the “hero” thing? – well get over it, and listen up! From the minute I walked through the door of Clara Maass yesterday, my experience was the best it could possibly have been. The nurses! OMG the nurses - I was in pre-op for hours. Lucky as I was to have been squeezed in to an already crowded surgical schedule, the truth of the matter was that my presence had required a quick shifting of resources—stretchers and space and - nurses. My sudden appearance in the queue was inconvenient, possibly even annoying. And yet all of them, including the nurse who ran the OR, came by to check on me, to give me extra blankets, to chat with me, and laugh with me. A friend’s daughter-in-law, who is a nurse there, got a text from him and even she came from three floors below just to say hello and charm me with her Australian accent and tired-but-twinkling blue eyes. I swear, for me? The whole experience was a cross between a weirdly sterile spa stay, and – as mine all happened to be women - a girls’ sleepover with your best girlfriends—only these were women I'd just met (but they’d also pretty much seen me naked, so, there’s that…).
Most of them were nearing the end of a 12-hour shift. As I lay there, relaxed and warm, reading and texting, they race-walked back and forth among those of us who waited, or were recovering. I lost count of how many times one of them asked me if I was okay, or if I needed something. They ate their dinners on the move, taking bites and then sprinting off, tearing off one set of gloves, putting on another. These people Do. Not. Sit. The sink was right near my bed, so I saw a lot of hand-washing traffic too, and a lot of red, chapped, over-sanitized hands. They spoke in soothing voices to those who were waiting, and possibly scared, and loud-enough voices for those emerging from the cloud of anesthesia to understand. Sometimes they shouted good-natured complaints to one another, or teased one another – and me, as when one started repacking those bags they give you for your clothes, amusement in her voice as she yelled, “What the hell did you do here, shove it all in like a little kid? Your purse is open – Maria, come over here and see this – she’s a mess!” Hahahaha! One came by and pointed to the cover of the book I was reading entitled “The Silent Patient”, and joked “That’s the kind we like!”
I even began to wonder if what I was getting was “special treatment” reserved for those whose surgeries were personally called-in by the surgeon. Once he arrived, however, it was clear that not only did they not know he was the one who got me in, but they chided him in the same affectionate way. At a point, I said to one of them, “Doctors think they’re all that, but nurses really run the show don’t they?” She winked at me and elbowed me a little, “Like husbands, honey – they just think they’re in charge!”
I lounged, for over four hours while they stood on what had to be tired feet, hands on hips as they talked to me, telling me which part of the hospital they’d spent the morning in, or where they were headed next in this crazy, all-hands-on-deck environment. We chatted about jobs and kids, and only when the topic of this deadly disease came up did the lack of words become conspicuous. Then it was all a mime of sad shakes of the head and downward glances.
It occurs to me today that after all of this, I'm not sure I would recognize any of them tomorrow if I saw them on street – nor they me. Of course, we were all masked. But maybe I would – if I could see their eyes again. And I'm not exaggerating when I say that most of all, those eyes conveyed a profound kindness. And laughter, and concern, and compassion, and dedication—and a toughness that allows them to do it all.
I'll tell you a secret: I am a person who often has a weird response to unexpected kindness - it makes me cry. I welled up more than once yesterday afternoon. I may have been just one of many for them – this is just what they do - but for me, a bond was made. I will always remember them.
Make no mistake: it’s no hardship to be home in your sweatpants with your gel manicure looking a little ratchet, and your spouse and kids seeming more like houseguests who have overstayed their welcome. Today, I want you to feel really, really blessed and grateful, and if you’re like me, a generally healthy person who never really gave too much thought to the job that these people do, I hope I was able to convey just a little of it.
That school nurse who rescued me put it this way: “I took an oath when I graduated just as physicians do. I have followed it for 28 years and it has never let me or my patients down.” That whole oath thing is good and important and all, but the heart behind it gives it grace.
So, if you get an invitation to do one of those car processions where you beep your horn and cheer for the local health care workers as they go in to, or leave, work– get in your car and go. Or, just mail them each a check for a million dollars. Either way.
5 notes
·
View notes
Text
TAFAKKUR: Part 16
Your kidney
In the earlier issues my friends heart and stomach spoke with you and I patiently waited for my turn. I am located at the waist level to the right of the spine and my twin left kidney on the left, on whose behalf I’m also speaking now. We are truly vital organs to you. Before you say “each one of you claims that it’s vital,” let me talk a bit first, and then you decide.
In your body, which is built like a well-functioning factory, I am the most essential sanitary device. As the heart pumps blood to take food and oxygen to all your organs, you obtain the energy you need. But do you ever think about the disposal after so splendid activities are carried out in your body? If you burn a stove, you need to dispose of the smoke and the ashes if you want to keep it working. Likewise, as you burn your calorie intake, you dispose of the smoke (carbon dioxide) with your lungs and the waste with nitrate-poisonous after a certain level of intensity-thanks to my quietly and perfectly working filters. That is, I am an organ which saves your life by removing the poisonous substances in your blood. I do not only filter your blood, but also play a role at controlling the balances of the sensitive levels of water, sugar, amino acids and different minerals in your body. In short, I am a tiny but strategic laboratory.
The acid-base balance in your body and the amount of water and different salts are significant values which concern all of your bodily activities. When their balance is upset, different troubles arise in different units of your bodily mechanism. I am such a blessing, which works so sensitively to adjust the levels of water and mineral salts in your body while you don’t even realize it.
A watery environment is needed for the thousands of biochemical activities taking place in your body. In addition, activities like the contracting of the muscles and transmission of electrical stimuli between your neurons are realized with the presence of a pinch of mineral salt you don’t even give a thought about. Sometimes you sweat due to running or hot weather. The white stains on your shirt are the salts you lose after the water evaporates. When you suffer from diarrhea, you lose salt again, for the salt in the nutrients are thrown out without being absorbed. Especially when little children are concerned, this loss is of vital importance. The transfer between the blood and the liquid in the tissues is mainly realized through the concentration differences which are kept in a certain balance. If your body holds too much water, your tissues swell. You particularly feel it when you press your finger over the flesh near your shins.
I will not list all of my duties in detail in order not to confuse you. However, let me tell you one more. Since not everyone knows this duty of mine, they just see me as an organ of liquid disposal. But I also take part in controlling the blood production! Surprised? Well, I also have the duty of secreting the hormone which stimulates blood production in the bones. I must always stay alert and maintain this balance in the best way; if you start losing blood, for instance, I must increase the hormone and accelerate blood production.
Yes, I’ve told you about a few of my basic duties, but haven’t told you about how wonderfully designed I am. I am a bean-shaped organ and a single kidney like me weighs 130-160 grams on average. We are approximately 10 grams lighter in female bodies. I am surrounded by a soft but protective membrane. I need 35 grams of daily oxygen supply to survive and I use 13 % of your total body energy.
As an army is made up of individual soldiers, I am like a complex army, and a single soldier of mine is called a “nephron,” which does the real job. Thus, you can see me as a body of nephrons. Millions of these nephrons are brought together to make up one kidney.
A single nephron is a thin tubular structure with closed ends, and its length is about 3-4 cm. So the total length of my nephrons is about 50 km. The cup-like sac at the beginning of a nephron is named the “Bowman’s capsule.” The main artery bringing blood to the kidneys branch into smaller units, and one road leads to every nephron. The knot of capillaries (glomerulus) inside this double-walled capsule is more complicated than any road map you might have seen. The total length of the capillaries is nearly 25 km. The unwelcome substances in the blood are passed to the capsule thanks to blood pressure, and they proceed through the tubule. The total surface area of my tubules is about 20 m2. Within five minutes the whole of your blood passes through us. That is to say, an average of 1.2 liters of blood per minute, and 1800 liters a day are filtered by my nephrons, leaving the toxic substances in me. As this amount of blood (nearly 400 times the normal amount in your body) pass through my tubules and return to the veins they leave behind an average of 180 liters of liquid in me. In this case, you could be supposed to throw out 180 liters of urine a day. However, if you really did that, you would neither be able to find a sufficient supply of water nor salt. Fortunately, Providence granted you the mechanism to absorb back nearly 178.5 liters of this filtered substance. This way, the thickened urine throws out the toxic nitrogen-containing byproducts together with a little amount of water. Therefore, I give you back the substances you need with an amount of 1.5 liters of liquid disposal a day. This reabsorbing is realized in what you call the Henle loop. The cells in the walls of my tubules have neither intellect, nor consciousness, nor any knowledge of physiology; in spite of this, they work as if they were perfectly aware of their duty to adjust the amounts and types the substances to be kept or released. To give you an idea, you can think about the huge dialysis machines your engineers design to fulfill the job my tiny tubules do. You decide which one of us is the perfect work of engineering.
A rich network of veins surround the Heinle loop and the reabsorbed substances are released into the bloodstream. The drops to be disposed of are collected and then passed to your bladder. When the liquid in your bladder amounts to a certain value it tightens the bladder walls. The muscles blocking the way out give way and the urine is disposed of. However, know that the bladder has the capacity to expand as large as 1.5 liters when you cannot find the proper time and place.
Most people take for granted the blessings they enjoy. If you visit the nephrology service in a hospital and talk to the patients waiting to be dialyzed, you understand what I mean better. Do not forget that many people who suffer from kidney failure need that huge machine to filter the whole of their blood and they pray for a kidney suitable for transplantation to be found at once.
Incidentally, thinking of chronic kidney failure recalled various reasons which ruin me: long lasting infections, long-term use of certain medicine, different chemicals like ethylene and mercury, heavy loss of blood, high blood pressure, serious burns, and wrong blood transfers etc. In such cases I can receive irreparable damage.
Another issue which troubles me is the formation of kidney stones. The stones which form owing to failures in different metabolic processes really hurt. When excessive decrease of liquids or increases of salts in the body upset my sensitive balance, some dissolved substances remain, begin to collect, and form stones. These stones hinder urine flow and might cause infections. You may drink water abundantly to prevent these stones. Most importantly do not wait too much before going to the toilet. If you excuse me, I also strongly recommend you to urinate in sitting position; this helps emptying your bladder completely and reduces the risk of kidney stones.
I do my job properly until I lose 90 % of my working capacity. When a considerable part of me loses its capacity, the remaining good part boosts its activity to make up for the loss. When one of our twins are taken out with an operation, the other one does not complain at all; it grows a bit bigger and keeps working.
As the nature of honey depends on the nectars bees collect, the ingredients of the urine I produce depend on what’s in your body. Therefore, a urine analysis tells much in the case of illness. For example, I normally do not release valuable substances like glucose and protein in your blood into the urine, but return them to the bloodstream. As my friends cannot fulfill this function in diabetic patients, their urine analyses reveal glucose. As for medicines, I throw them out right away since they are alien substances to me.
You are young and healthy but be careful and do not get cold around the waist, otherwise I might trouble you. There’s a lot to tell you, but I do not want to confuse you. Like any other organ, I do not like being taken for granted and I just wish for you to appreciate what a blessing I am. Let me note that my perfect cooperation with the rest of your body is another wonder in itself. Anyway, the urea in your blood is increasing, so I must go help my twin now.
#allah#god#muhammad#prophet#sunnah#hadith#islam#muslim#muslimah#hijab#help#revert#convert#reminder#religion#dua#salah#pray#prayer#welcome to islam#how to convert to islam#new muslim#new revert#new convert#revert help#convert help#islam help#muslim help#convert to islam#revert to islam
1 note
·
View note
Text
One of the most rewarding things in my life became after
Studied overseas. Talking to human beings approximately my stories and sharing my tales is a lot of fun for me. I can talk for hours about the things I noticed and those I met. I advise to everyone that I meet that they should move and take a look at or journey overseas. Seeing the sites that you examine about in books, or see on TV and inside the movies. Study in Europe It is a surreal feeling whilst you are there and while you get again you get to relive it each time you see the Eiffel Tower or the Vatican.
I actually have seen extra things and been greater locations than my parents have and I know they are jealous. Also most of my friends have never been to Europe or out of this country for that matter in order that they don't understand the emotions that I actually have towards touring abroad. I begin into a story of something that came about or something I noticed and none of them can relate. This is one purpose why I think every person should go over there.
While journeying and planning to tour you can have many questions. Questions on what to do and wherein to cross, or how do I pay for this. All of those questions may be answered with the aid of the human beings which have gone earlier than you. In most cases we all know someone that has been overseas. Asking them approximately what they did and the way they did it's far the quality way to find out what you should do. People which have gone before you will help you out the maximum.
This is the cause I have made a website approximately traveling and reading abroad. I consider that my recommendations and guidelines along side my tales can help many others. I were to numerous different nations in Europe. I were to England, France, Belgium, Germany, Holland, Austria, Italy, Luxemburg, and Switzerland. Seeing most of those places within weeks was top notch but being in England for 3 weeks can not be beat. I studied abroad in Bristol England for three weeks and spent every week in Belgium with that program. After my first month overseas and my program have been over I spent every other weeks on a bus excursion of Europe. My aunt and uncle met me in London and we resulted in Paris. The last two weeks I saw more locations in a much less time than I ever imagined.
Something that I found out is that if you are going to be journeying for a protracted period of time than you need to mix up who you are visiting with. However if you know you could stand a person than you must be ok. The remaining a part of my trip I think could have been a bit bit higher if there become someone else on it with me around my age. I did make a number of knew buddies, people that I will in no way forget.
The intake of olive oil blocks the generation of oncogenic (cancerous) tissue, as defined at the first 'Worldwide Nutrition Congress' held in Barcelona through Angel Gil, an expert within the Dept. Of Biochemistry and Molecular Biology on the University of Granada.
In this recent look at, over 40% of rats fed sunflower oil died of tumors, as opposed to olive oil fed rats that scarcely produced any deaths at all. Whereas sunflower oil and animal fats promoted the creation of the three fundamental food related cancers, olive oil reduced the creation of these cancerous tumors.
While noting that this does not imply that the purchaser of sunflower oil has a greater threat of developing cancer than folks that consume olive oil, in line with Gil, there may be an influence. This is confirmed with the aid of the greater durability of people living in the Mediterranean rim countries.
2 - Expert corroborates that the consumption of olive oil increases durability -
According to an investigation reported by Jose Mataix, professor on the University of Granada, the consumption of olive oil increases sturdiness and helps maintain the frame in good running order.
According Professor Mataix: "the animals in this examine that consumed (olive oil) lived longer and, via the microscope, we understand that their systems had been better conserved than those that ate up seed oils. Also, the latter (the animals that consumed seed oils) developed extra tumors". While noting that the results aren't extrapolatable to humans 'a priori', professor Mataix added that "being as the ageing mechanisms are similar, it can be deduced that virgin olive oil maintains this correlation each in (the animals) in addition to in human beings"
3 - Olive oil, Good for nearly everything, also to save you most cancers -
A new look at confirms that (olive oil) contributes to preventing most cancers. A scientific group on the Municipal Institute of Investigative Medicine, Barcelona, studied the levels of oxidization of genetic fabric in 182 men, 20 - 60 years of age from the north, middle and south of Europe.
The examine, become published in the January 2007 version of the FASEB Journal of the Federation of American Societies for Experimental Biology.
Virgin olive oil has a better content of phenolic compounds than processed olive oil. These phenolic compounds may additionally obstruct the dangerous impact of ldl cholesterol on blood vessels. The oxidization of genetic cellular material appears related to the formation of some kinds of most cancers.
During two weeks the participants have been given a day by day dose of 25 ml. Of olive. The analysis confirmed that the excretion of oxidative residue from the DNA and RNA in the urine become higher in the regions of northern Europe when as compared to the important southern Europe.
1 note
·
View note
Text
Color Study: Blue & Yellow in 14.06
Some have already seen my red color study meta for 14.06, and it was definitely the most jarring of our themes due to the natural “stop” effect and hazard warning that comes with red to the human brain, much less how saturated it was. It started as trims, highlights, and small props before evolving into wardrobe and then overbearing lighting on one of our story effects.
Again, I emphasize. I very, very rarely get into color metas because I honestly feel they are vastly abused and set people up for misreadings and disappointments, finding addiction in finding the specific wall color or coffee mug of their choice to evoke a sentiment from a series of skewed fandom-saturated talking points and in the end, everybody bickers.
However, Richard Speight Jr executed phenomenal awareness of human psychology in what he was addressing in this episode. Red is not the only color he used to the point over over-saturation. The other cardinal colors, yellow and blue, were in thick application all around, from props, wardrobe, to lighting just the same, sometimes going so far as to directly lens flare for a color only to offset it with another impacting light later on.
I’m not calling on any-old fandom pillar of meta on this. I’m talking the pure psychology by which Richard Speight Jr decided to communicate and impact the general audience. No specific character assignments, none of that. Just pure color psychology for cinematography.
So let’s go. Blue & Yellow in 14.06
Just like in the red meta, the other themes slowly saturated us. Blue is the boldest, but instead I’m going to set up another premise that laces in both themes.
It isn’t news -- I don’t think it is, at least -- that the bunker is often yellow coded. The brick and general construct itself is beige in nature, but often the lighting is designed to give us a yellow lens of differing type. Hell, the flashback sequence and our lead in are quick to remind us of that.
So first, let’s address the base concept of yellow.
Yellow is the most luminous of all the colors of the spectrum. It’s the color that captures our attention more than any other color. It’s the color of happiness, and optimism, of enlightenment and creativity, sunshine and spring.
Lurking in the background is the dark side of yellow: cowardice, betrayal, egoism, and madness. Furthermore, yellow is the color of caution and physical illness (jaundice, malaria, and pestilence). Perhaps it’s no coincidence that the sources of yellow pigments are toxic metals - cadmium, lead, and chrome - and urine.
Although there are strong mustard yellows and deep yellow ochres, there are no dark yellows. When you add black to yellow you get gunky dirty green. Yellow is the only color that reacts badly to black: Add a little black and it becomes a sickly yellow-green.
Dull (dingy) yellow represents caution, decay, sickness, and jealousy.
Light yellow is associated with intellect, freshness, and joy.
Which kind of shows even there. Lucifer reaving out grace while everything goes to hell? Dingy, dull, green tinted. Jack having success? Fairly warm. Mood.gif in a family discussion? Half warm and lensing towards green, but not as entirely dingy. Ding ding, we have ourselves a psychological winner.
So where do we go from here?
(I do admit to tapping lightly at the contrast balance in that last frame but the saturation/color balance I left the same; the painting was there, but the shading was so subtle in the lighting I felt the point would be missed before we got through the rest of this analysis)
You may remember from my general notes and red meta that while Dean turned aside the Red Cock during the awkward flirtation, he’s mostly haunted by golden ones after that. That is, however, until there’s a very awkward timing with Jack inquiring about birds and bees, which leads Dean to promise to explain later. Here we have Red Roo but with a bold, sunny yellow right over his shoulder.
Or maybe during Jensen’s amazing Face Journey while playing good cop bad cop and teaching Jack the ropes, being called Old Man, and both the painting and lighting hugging him in that moment of maturing “discovery.”
Jack, on the other hand, sits in the backdrop of the portrait we see earlier, and hugging yellow lighting that stays warm, without turning dingy. But the thing is, this follows Jack (and often Dean) the entire episode, as below.

From walking into the warm farmy backdrop, to Jack’s communicative message in yellow reaching out against the fierce red light of their aggressor (which his presence stands against the ominous glow of all around, and even his red is the gentle scale that evokes love and kindness rather than fervor), to heading back home to the bunker, we have a variety of stronger yellows following us around by-and-through Jack.
Which is certainly fair. Jack is a good deal of warmth in their life. While we’ve talked Family Don’t End With Blood to death, Jack’s the vessel of that in our show. The communal son, everyone’s attempt at redemption in their own way, trying to pass on their better traits and raise a child as a community. Jack brings a certain warmth to their life and a rare happiness and hope. His color is yellow for far more than their eyes.
Even our preview for next week licks in yellow themes for these two.
I’m going to seem to break away abruptly now, because I have a few other things to address. Chiefly, this.
This particular cap doesn’t capture one part of it, but this is Sam sitting in a light blue truck playing with a light blue fidget spinner in front of a blue store awning.
Blue, on this branch of our story, slowly creeps forward from other elements around us just like red, and yellow, though the yellow is less abrupt. And, in the end, these paths will fuse.
So let’s briefly discuss the psychology of blue.
Blue is the color of the sky and sea. It is often associated with depth and stability. It symbolizes trust, loyalty, wisdom, confidence, intelligence, faith, truth, and heaven. However not all blues are serene and sedate. Electric or brilliant blues become dynamic and dramatic, an engaging color that expresses exhilaration. Also, some shades of blue or the use of too much blue may come across as cold or uncaring, and can dampen spirits.
It slows human metabolism and produces a calming effect.
As opposed to emotionally warm colors like red, orange, and yellow; blue is linked to consciousness and intellect. Dark blue is associated with depth, expertise, and stability.
Light blue is associated with health, healing, tranquility, understanding, and softness.
Dark blue represents knowledge, power, integrity, seriousness, intelligence and lack of emotion.
Too much blue can create feelings of melancholy, negativity, sadness, self-righteousness, and self-centeredness. Too little blue brings about qualities of suspicion, depression, stubbornness, timidity, and unreliability.
So here we are, sitting in a truck. Light blues of serenity, understanding and softness, but light while we hang in feelings of the unreliability of unhumans, and everything Charlie admits early on while the two seem to idle endlessly in this truck. Hopefully if you’re reading this, you’ve already watched the episode to understand how this lines with the color scheme you’re about to see bloom and go “wait what the fuck how did I miss this.”
So anyway the bus rolls by, one small strip of near-warning yellow and some pall glow in an otherwise blue cut=through, then heading to a blue door. I’m not even kidding. Like we leave the blue fidget spinner and awning and truck when the blue bus rolls by to head to the blue door.
We can talk to death the metaphors of this blue door for now, while knowing -- by now -- that this is all a giant metaphor both for Charlie and for everything else going on in their lives at large, which Yockey literally clobbered everyone to reflect on textually. But for now, let’s truck on.
If for some reason you thought this was pure coinkidink, not only do their lights glare blue but the entire scene is filled with consistent blue lens flares, startling electric shocks of blue tension through overbearing melancholy, negativity, and sadness in the story of the lone Musca, who abandoned his people to live alone, because he already felt alone.

It glows vividly enough we might even call it indigo at certain junctions.
The color indigo is the color of intuition and perception and is helpful in opening the third eye. It promotes deep concentration during times of introspection and meditation, helping you achieve deeper levels of consciousness.
Indigo stimulates right brain or creative activity and helps with spatial skills. It is a dramatic color relating to the world of the theater, which, during times of stress becomes the drama queen, making a mountain out of a molehill!
The negative color meaning of indigo relates to fanaticism and addiction. Its addiction encompasses everything from a need for recognized qualifications to a need for illegal drugs, from the workaholic to the religious fanatic.
Oh, so we went through the blue door and graduated towards an exploration of deeper consciousness, laced in, when not glowing damn near indigo, pure melancholy and loneliness.
I do find particular interest in the red light shining down like a bold cut out through the shocking blue with electric offsets, as if there was some sort of want, or fervor that laid unanswered right there in the pit. To read more about the use of red in this episode, just visit the red meta .
But let’s go on about Charlie and Sam’s talk, but absolutely not forget the Jack-Family-Coloring above with healthy, warm displays of yellow.
Between Sam and Charlie, as they roll along -- frankly, this would require a set of gifs I don’t have the skills to maintain -- all three colors accompany them. Melancholy and introspection sits heavily in thick blues rolling past the windows, but waves of red pass through in softer displays and lens twinkles in the distance of all three primary colors spark as she realizes the moral of this all and reconsiders taking the path of loneliness -- to not become the lone bugman, saturated in his blue melancholy and entombed in his loneliness, who abandoned his people. She considers returning, and that’s... you know, good.
Through the course of it, we see the Muscas come to reclaim their fallen. The Musca, that abandoned his people due to “self esteem issues,” has not been abandoned or forgotten by his people despite his attempt of forgetting them.
The blue rooms are carver not by blue lens flares like Charlie and Sam’s journey but a warm, soft, yellow glow as his family returns, carving through the melancholy if not entirely warding it away, centering over his body as they prepare to honor him and carry him out.
Huddled here, against grief and sadness, there is a warm, yellow, familial light in as much as a memory they still hold to honor, while Dean details the changes they can make to the world to help people and to change things. To make a difference.
Family wards away the sorrow and carries their fallen away.
Back at the bunker, Dean and Jack have their own heart to heart. And, as per the above last primary-yellow display, at first there is still warmth in the mutedness of it, but I’m going to briefly call back to this,
Yellow is the only color that reacts badly to black: Add a little black and it becomes a sickly yellow-green.
With a quickness, sickness, darkness and despair settles over the moment of warmth, and family as Dean himself blends into a motif of sickly despair and tragedy, sealing off our moment with a final collapse onto a greyed out floor.
Honestly the wardrobe piece is fantastic; his shirt is scaled so as to fuse well into the warmer yellows, dillute into the greens and still bond to the late near-greys with Jack on the floor, washing out our episode in a final moment.
So hi, yes. While it’s attractive to addict ourselves to the use of red in this episode, all cardinal colors were used with exceptional power. Red and blue sat opposite on our story ends, but yellow as a premise of family and warmth followed through, as if to bring the spirit of the bunker with it, even if by the end, the spirit of the bunker itself is falling into a pall hue.
And that’s your mindfuck for the day.
28 notes
·
View notes
Text
Exams on Astronaut and Twin Brother Spotlight Spaceflight’s Human Influence

In a landmark examine, NASA scientists performed exhaustive assessments on Scott Kelly throughout his grueling 342-day tour aboard the Worldwide House Station in 2015-2016. They usually concurrently monitored his equivalent twin brother Mark (a retired astronaut who was on Earth on the time), hoping the comparability would reveal new details about the results of long-term spaceflight on the human physique.
The outcomes of the NASA Twins Research, reported Thursday in Science, present Scott Kelly underwent various physiological changes--most of which returned to pre-flight standing after he returned to Earth. The findings may assist inform preparations for future long-term missions, corresponding to journey to Mars or stints on a moon-orbiting house station.
The examine was the primary to combine each behavioral evaluation and physiology to analyze how house influences an individual, and the primary to gather two years of such complete well being knowledge on a middle-aged Earthbound man, says co-author Brinda Rana, a molecular geneticist at College of California, San Diego.
" science at its best, in many ways, because it is leveraging something that is naturally occurring to try and understand causality," says behavioral geneticist S. Alexandra Burt, who co-directs the Michigan State College Twin Registry and was not concerned within the examine. "I think this was a unique event and they capitalized on it beautifully."
Kelly says he initially proposed the examine whereas getting ready for the ISS mission. "I said, 'Hey, if anyone asks about any studies planned with my brother Mark and I, because we're identical twins, is there any interest in that?'" he says. He was initially rebuffed, however he says NASA scientists finally spoke to a number of universities "and they found out there was actually a lot of interest." The Twins Research was a go.
For almost two years each brothers offered urine, stool and blood samples, which researchers used for 10 separate investigations involving the molecular, physiological and cognitive results of long-term spaceflight. Shut coordination among the many many investigators was important. "NASA got 10 investigators from around the country--most of whom didn't know each other--and put us in a room and got us to all cooperate and become a cohesive team to carry out this mission," Rana says. The inherent difficulties of gathering such specimens from an astronaut aboard the ISS meant the investigators needed to work with comparatively scant materials. "We had to come up with protocols where we could all do our studies effectively with one sample," Rana says. The examine additionally spurred researchers to innovate new strategies for learning physiology and genetics in house. "It's helped us drive technology to do these sorts of experiments not just for low-Earth orbit, but for future activities exploration missions," says co-author Stuart Lee, a cardiovascular scientist at KBRwyle.
Kelly had to attract his personal blood and gather his personal urine and stool. "Certainly it's more complicated to pee in a bag in space, because everything floats," he notes. "But most importantly, it takes time. Astronauts sometimes find themselves almost subconsciously trying not to be as hydrated on urine collection days because of the time it takes to pee." This was mirrored within the outcomes: researchers discovered Kelly was constantly mildly dehydrated, a standard phenomenon amongst astronauts on long-term missions--and scientists do in actual fact attribute this to astronauts' annoyance with the difficult onboard toilet.
The examine discovered Kelly was below near-constant physiological stress whereas in flight. His immune system was on excessive alert; he had adjustments in DNA expression; his carotid artery turned distended. He additionally developed "spaceflight-associated neuro-ocular syndrome," or SANS--a situation that entails adjustments to his eyes, and for which the trigger is poorly understood. And his blood, now not drawn to his legs by gravity, collected in his head. "In the beginning, it's the worst," Kelly says. "Your body adjusts to it over time, but in my experience, it never adjusts completely. I always felt pressure in my head."
Whereas in flight, Kelly's telomeres--the protecting sequences of repeating nucleotides that "cap" the ends of every chromosome like aglets on a shoelace--grew longer. "That certainly was a surprise, because going into the study we had proposed exactly the opposite," says Susan Bailey, a biologist at Colorado State College who directed the examine's telomere investigation. Telomeres shorten as we age, and an enzyme known as telomerase repairs and elongates them. Astronauts are uncovered to excessive stresses of microgravity, isolation and radiation that ought to contribute to telomere shortening, Bailey says. She suspects Kelly's extremely regimented food regimen and train program aboard the ISS might have contributed to the lengthening--or that the phenomenon might point out his cell inhabitants was altering throughout spaceflight. "Going forward, I think we will try to incorporate these telomere endpoints into some of the standard measurements that they're doing on the astronauts, so that we could actually address that question directly," she says.
After Kelly returned to Earth, a lot of the physiological, gene expression and different adjustments returned to regular inside about six months. However there was nonetheless a interval of adjustment. "When you get back to Earth all the blood just wants to pool in your legs," he says. "That lasted for me for weeks." He additionally developed rashes and hives every time his pores and skin, which had grown unaccustomed to gravity, had any stress on it. Even leaning on a desk induced a response. However he did finally readjust, a hopeful signal there could also be little lasting hazard to astronauts' well being after lengthy intervals in house. That stated, it is very important observe that touring to Mars or different long-distance explorations presents a further concern: radiation. Astronauts aboard the ISS are nonetheless considerably shielded from cosmic rays by the Earth's magnetic defend; a Mars mission would expose them to galactic radiation at a lot larger ranges, Lee says.
The examine authors warning that given the extraordinarily small pattern measurement, it's "impossible to attribute causality." They write that the examine must be "hypothesis-generating and framework-defining," with future analysis on astronauts complementing the work. "That's all true," Burt says. However she provides that having a genetically equivalent topic again on Earth permits for assuming causality far more strongly than the examine in any other case may have. Kelly agrees: "Granted, this is an experiment with an n of one," he says. "But they didn't see anything that would prevent us from going to Mars. However, he adds, "if we will transcend Mars"--requiring astronauts to stay in microgravity for years on end--"we will have to start out serious about synthetic gravity."
Read the full article
1 note
·
View note
Text
7 Reasons Why Insurance Won’t Pay for Functional Medicine
Functional medicine focuses on getting to the root cause of your problem instead of just treating the symptom.
We are living in one of the worst chronic disease epidemics of all time with 1 in 2 Americans living with a chronic disease (CDC, 2017) caused by preventable lifestyle factors, like nutrition and sleep, and a projected 100,000 doctor shortage by 2030 (Association of American Medical Colleges, 2017).
The solution? If you’re looking to insurance, you may be waiting awhile, at least if you want an option other than the current model, like Functional Medicine or a holistic doctor.
Practitioners who take an “unconventional approach” to medicine by addressing the roots of disease, as opposed to managing symptoms like the norm.
Sound Familiar?
If you’ve ever been to the doctor, you’ve probably experienced the healthcare rabbit hole.
1st Step: Feel sick.
2nd: Step Call the doctor to make an appointment.
3rd Step: Wait 1-4 weeks to get seen.
4th Step: Go to see the doctor. Wait in the waiting room. Chat briefly.
5th Step: Walk out with a prescription or go down a rabbit hole to see another specialist or schedule another appointment.
We ALL know that rabbit hole:
The Rabbit Hole of Healthcare
In the traditional healthcare system, it takes an average of121 minutes each time a person seeks medical care just to get seen. The total includes 37 minutes of travel time, as well as 87 minutes at the doctor’s office or clinic—most of that spent waiting in the waiting room. (Ray et al, 2015)
In fact, the average person only spends 15 minutes of “talk time” with the doctor in a visit (Tai-Seale et al, 2007).
Couple this with the projection tha,t by 2030, America will have a 100,000 doctor shortage (Association of American Medical Colleges, 2017)—unable to meet the “demands” of the, now, 1 in 2 Americans who has a chronic disease (CDC, 2017) and, Houston…we have a problem!
I’ve been there, got the t-shirt.
The Scene: Healthcare & Current Insurance Inefficiencies
I had waited 3-months for the appointment with a local doctor in town.
Nothing unusual—as the “average” wait time to see a doctor nowadays—especially a specialist—is an average of 24-52 days (Merritt Hawkins, 2017). And, not for anything crazy—just an annual “Well Woman” check up.
So there I was in a conventional outpatient clinic, after 3-months of waiting to see the doctor, and here’s what went down under my conventional health insurance…
What Traditional Health Insurance DOES Cover
1. OVERBOOKED APPOINTMENTS:
Traffic was shut down to one lane on I-35 in Austin and I was running right on time to the appointment (not early). I called the office on my way to inform them of the situation, to which they said to still come in.I managed to park in the lot right at 8:35 a.m. and race upstairs for my 8:30 a.m. appointment.
Once checking in with the staff, she told me she’d have to call back to the doctor’s staff (which they had already done) to verify I could get “in.” 10-minutes later, confirmation was given—I could go back to the waiting room.
2. DISORGANIZATION:
However, before being released to the waiting room, ANOTHER hurdle…
Front Desk: “Oh wait a second..you can’t see the doctor, you have an HMO plan,” the front desk girl said.
Me: “My doctor faxed it over 3-months ago when I made the appointment.”
Front Desk: “You will need to fax it again if you want to keep the appointment,” the girl said.
(I quickly texted my doctor—one of my colleagues and now friends—and the situation was resolved).
3. A SYMPTOM-BASED APPROACH:
As I sat in the waiting room, I was asked to complete a one-page form.The only thing the form asked me about was…my symptoms, my brief health history (surgeries, family diseases), if I smoke or drank, and the date of my last period.
That’s it.
No exploration around my current diet, sleep habits, what work I had already done around my gut health, my health goals, my physical activity patterns, food intolerances and beyond.
4. CHRONIC DISEASE SYMPTOMS:
Initially, it only took about 15-minutes once I was in the waiting room to go back to the clinic room. The nurse was very nice and did her routine thing: blood pressure, weight check, heart rate and body temperature. She also asked me the SAME questions on my health form. She was shocked to hear how I had NO diseases whatsoever. My ONLY complaint was chronic constipation. (Apparently she was used to hearing ALOT more).
5. LONG 2-HOUR WAITS:
After our check in, the nurse left me be…for 2 hours.
At one point in my waiting, she actually asked if she could “pull me” out of my room for “about 10 minutes” to go back to the waiting room in order to see another patient.
So I went back to the waiting room where I waited another 45-minutes…
6. NO APPOINTMENTS:
I had booked a 10:30 am appointment with a client of mine—allotting for my 8:30 a.m. doctor visit that morning, thinking I’d have plenty of time in between. 10:20 a.m. rolled around and I was STILL in the waiting room. To say the least, I did not get seen, and the nurse told me she’d call back that evening to reschedule…which did not happen.
The Solution?: People Want to Take Their Health Into Their Own Hands
Many people are looking to take their health into their own hands—with at least 80% of all people seeking out advice on search engines like Google alone (Pew Research Center, 2013).
Others are looking for OTHER options (like holistic doctors, health coaches and functional medicine providers).
According to a report from the National Institute for Health in 2015 alone, researchers found that about 1 in 3 Americans were utilizing some sort of alternative or holistic care out of mainstream medicine (Stussman et al, 2015).
Fast forward to today, and there is no doubt that those numbers are consistent—if not more—with the job outlook for all allied healthcare providers expected to go up by 2026 according to the Bureau of Labor Statistics (including occupational therapy, physical therapy, personal fitness training, health coaching, life coaching, acupuncture, chiropractic care and naturopathic or functional medicine).
However, this doesn’t mean these alternative providers are always covered by health insurance.
A common question we as functional medicine practitioners are asked is:
Patient: “Do you take insurance?”
Functional Medicine Provider: To which we most often reply, “No.”
Although many holistic doctors and functional medicine practitioners CAN submit superbills, and SOME CAN reimburse partially for visits or lab testing, generally most holistic doctors and functional medicine practitioners are cash pay.
Why?!
Let me give you 7 reasons.
7 Reasons Why Insurance Doesn’t Cover Holistic Doctors & Functional Medicine
1. Insurance is NOT Patient-Centered.
Functional Medicine is patient-centered. Instead of focusing on numbers-centered or about getting more people in the door, wee typically take time to review your chart well before your appointment.
2. Insurance is NOT Big on Taking Time with Patients.
Functional Medicine takes time. We don’t rush to get you through our churn mill. Typically, you will spend 1-2 hours for your first appointment so your practitioner can truly get to know your story. The doctor will assess your health struggles and your goals.
3. Insurance is NOT Focused on the Whole Body.
Functional Medicine is a “Whole Body Medicine,” taking into consideration all aspects of your health and life. Those that contribute to how you feel and the presentation of disease. It’s different from an endocrinologist who just looks at your hormones and thyroid, an ENT doc who just looks at your ears, nose and throat, or a psychologist who just focuses on your mental health. Functional Medicine acknowledges a respect and awareness of how ALL body systems impact one another, including:
Gut Health
Brain Function
Hormone Health
Detoxification Pathways
Mindset/Mentality
Cardiovascular Health
Immunity
Thyroid & Metabolic Health
Mineral & Vitamin Status
4. Insurance Does NOT Address the Roots of Disease.
Functional Medicine does. Instead of looking to suppress or manage symptoms from the top down, we take a “bottom up” approach. We find and address the triggers and root causes of any disease or symptoms a patient is experiencing. These include bacterial overgrowth and SIBO (connected with skin conditions, chronic headaches, metabolic dysfunction, and GI disturbances), or cortisol imbalances (connected with insomnia, anxiety, blood sugar imbalances, and GI disturbances).
5. Insurance is NOT Focused on Prevention.
Functional Medicine focused on preventing disease, or further decline of health from happening by using laboratory reference ranges (blood work, urine, stool analysis, etc.) that reflect the progression of disease (in order to help reverse it early). We also integrate lifestyle medicine FIRST to support our clients health as a whole. Through a holistic care plan that includes nutrition, supplement, lifestyle healing and stress busting strategies, and physical activity.
6. Insurance Views Functional Medicine as “Quack” Medicine.
Contrary to popular belief, Functional Medicine isn’t about “woo woo” or “voo doo.” Functional Medicine acknowledges the latest in research to influence and support care. In fact, Functional Medicine is simply an approach to medicine. Healthcare says, “Hey guys, let’s address lifestyle factors FIRST and consider all aspects of health—not symptoms—before turning to medicines or negating other factors of our patients’ modern day lifestyles.”
Functional medicine acknowledges science, reason and research for modes of healing and treatment protocols. If anything, is a compliment to the ever-evolving research in traditional medicine.
For example, with the past 3 years of research on the gut microbiome alone (more than 8,000 studies in PubMed), we know that our gut health definitely influences other aspects of our health, including our mood and anxiety levels (Clapp et al, 2017), our metabolism (Boulange et al, 2016) and brain health (Li et al, 2017). In practice, Functional Medicine is more readily able to address gut healing for all types of conditions and diseases.
Another example: when TIME Magazine leaked the “big news” that the sugar industry paid off the FDA to hide evidence that sugar—not saturated fat—was the driver of all disease, Functional Medicine practitioners could further educate their patients as to why butter, bacon and egg yolks are NOT bad. Mainstream medicine on the other hand? Still preaching that saturated fat and high cholesterol are the number one drivers of heart disease. Nevertheless, insurance companies DON’T always look for the research on their own.
7. Insurance is Stuck in the Good Ol’ Days.
If you’ve ever simply tried to call or fax something to your insurance provider, you know the never-ending hold times. In addition, inefficiencies of modern day health care (seemingly stuck in 1961). Whereas, functional medicine is now integrating more and more tele-health, “biohacking” (alternative therapies and healing supports, like infrared saunas, hot-cold therapy, coffee enemas and herbal supplements), and high-tech EMR’s (medical record systems), Insurance still has you on a “brief hold”and is comfortable doing things they’ve always done.
Bio:
Dr. Lauryn Lax is a Doctor of Occupational Therapy, Nutritional Therapy Practitioner, Functional Medicine Practitioner, author and speaker, with over 20 years of clinical and personal experience specializing in gut health, intuitive eating, disordered eating, anxiety, hormone balance and women’s health. She’s based in Austin, Texas, and operates a virtual Nutrition & Functional Medicine practice, Thrive Wellness & Recovery, LLC, working with clients and patients around the world. In addition, Dr. Lauryn is a published journalist and speaker. Her works have been featured in Oxygen Magazine, Women’s Health, Paleo Magazine, Breaking Muscle, CrossFit Inc, USA Today, ABC and CBS News. Ultimately, she loves nothing more than helping others “quiet the noise” in the health food and fitness world.
The post 7 Reasons Why Insurance Won’t Pay for Functional Medicine appeared first on Meet Dr. Lauryn.
Source/Repost=>
https://drlauryn.com/wellness-knowledge/insurance-wont-pay-functional-medicine/ ** Dr. Lauryn Lax __Nutrition. Therapy. Functional Medicine ** https://drlauryn.com/
2 notes
·
View notes
Text
Guns for Hire
Ramsay Bolton x Reader
Part 1 of the Bastard’s Boys series
Ao3
Chapter 2: Wolves at the Door
"When did you find out?" Ramsay asked, arms crossed, leaning against the door frame as you peed on the fourth pregnancy test.
"Only this morning." You said with a sigh, replacing the cap and setting it next to the other three that all read positive. "I was hoping to tell you at dinner tonight. But..." You added, giving your husband a frown.
He pushed off the door frame and watched, for the fourth time, the lines read positive.
It was hard to tell what was going through his head. Was he mad? Excited? Scared? Happy?
"Who all knows?" He asked, glancing over at you as you washed your hands.
"Just you baby." You said, reassuringly, drying your hands off.
Ramsay nodded. "You're making a doctor's appointment first thing in the morning." With that he left you alone in the bathroom.
You were a bit afraid. It wasn't that he had shown no emotion, it was that you didn't know the emotion he had etched on his face. It was foreign and unknown to you. Was he making you set up an appointment for an abortion? The thought made your stomach hurt.
You let out a yawn and crawled into bed. You had been so ready for bed after sex, but then Ramsay demanded going and buying pregnancy tests.
Kira raised her head off the floor a bit when you entered the bedroom. You gave her a loving nudge with your toe before climbing into bed, heaving a deep sigh as you sunk into your squashy pillow.
A few moments later Ramsay came to bed. What happened next made you want to cry in happiness. Once under the covers he pulled you into him, nuzzled your neck, and placed his hand protectively over your stomach.
"I love you, baby girl." He whispered.
You let a small smile tug your lips, "I love you too, baby."
×××
The smell of bacon and coffee woke you. You looked around through bleary eyes and stifled a yawn. The clock on the bedside table read 8:17.
You sat up, running your hand through your hair, casting around for your bathrobe. You slid out of bed and opened the closet door. No bathrobe hanging up.
'Laundry room.' You thought with a sigh, grabbing the silk robe instead.
It was really too cold as the cold December air seemed to seep into your hardwood floor. You shrugged into your robe and made your way to the kitchen.
The table was set with a plate of eggs, toast, and bacon. A cup of coffee waiting for you. Ramsay was nowhere to be found. He must have been outside smoking.
You sat in the chair and tucked into your food. Once you had eaten your fill you looked around the spotless kitchen, thinking back to the night before. You sipped your coffee, absentmindedly running your hand over your stomach.
Ramsay came into the kitchen, whistling. You looked up and offered a small smile. He narrowed his eyes and gave you a sweet smile back.
"Go get ready. We have a doctor's appointment at eleven thirty." He said, clapping his hands together, and taking your plate away.
"Uhm, okay, love." You said, rising from your chair.
"I need to go into the office after, so one of the guys will bring you home. We have dinner reservations at six."
You smiled to yourself walking into the bathroom and turning the shower on. It had been weeks since your husband had taken you out to eat, and you were excited. Though, you were also nervous about the appointment in three hours.
"How cold is it outside?" You called from your closet.
"Cold enough." Ramsay called back.
You nodded to yourself grabbing a sweater and pair of skinny jeans. After dressing you pulled on your boots and walked back to the bathroom to fix your hair and make up.
"Come on baby girl, let's go!"
"Coming!" You called from the bathroom, finishing up your hair.
Ramsay held out your coat and purse when you reached the front door.
×××
You felt extremely out of place in this waiting room. You felt way over dressed as you looked around at the women in the room. Ramsay sat, impatiently tapping his foot until the nurse opened the door and called your name.
Ramsay possessively grabbed your hand and pushed you forward to walk in front of him as the nurse led you back.
"Good morning, Mrs. Bolton." The nurse said kindly, as she indicated you to step on the scale.
"Good morning!" You said brightly, as she took down your weight.
"So what are we doing today?" The nurse asked, leading you to an empty room.
"Well, yesterday five pregnancy tests informed me that I'm pregnant." You said, as Ramsay helped you up onto the examination bed.
"First?" The nurse asked, making a note.
"Yes." You breathed in excitement, cheeks flushing.
The nurse smiled kindly, "can you tell me the last day of your cycle?"
You frowned, trying to remember. "Uh...."
"Second week of September." Ramsay spoke up.
Nothing slipped past him. In a weird way it was like he knew everything. Especially when it came to you.
The nurse nodded, writing another note. She then smiled at you again.
"Alright, let's get some blood drawn and a urine analysis and then Doctor Stark will be with you and we'll see what we can see."
You nodded, sliding off the table and following the nurse. You glanced back at Ramsay who looked uncomfortable with letting you leave without him.
Five minutes later the nurse returned you to your room and you sat nervously on the examination bed while Ramsay sat in a chair, stared out the window. Every so often he would glance down at his watch and jiggle his foot.
Finally there was a knock on the door and the doctor entered as Ramsay stood quickly, taking his place beside you.
The doctor was a lovely looking woman, who was maybe old enough to be your mother. She had kindly blue eyes and deep auburn hair.
She held her hand out to shake Ramsay's hand.
"I'm Doctor Stark. But feel free to call me Cat." She took a seat on her stool and glanced down at the clipboard she was holding.
"So, I believe a congratulations are in order. Mother's urine sample and blood shows she is in perfect health and baby will do just fine. And this is your first?"
"Yes ma'am." You said, unable to keep the grin off your face.
"Never had any miscarriages before?" The doctor questioned.
You shook your head, "no. But I've been trying for a couple years. Was about ready to give it up as a lost cause. But here we are."
"Here we are." Doctor Cat echoed, writing more things on her clipboard. "Okay, well, you seem healthy, your weight is good, I want you to start taking prenatals, and we will get the Doppler in here to see if we can hear a heartbeat."
You chewed your lip and gave a nod.
You held back tears, gripping Ramsay's hand as the tiny heartbeat came through the speaker of the Doppler.
Ramsay clenched his jaw and fought back a grin.
"I would say we are about eight to nine weeks. Next appointment we will get an ultrasound done, and see exactly how well the little one is doing." Doctor Cat said, with a smile.
The woman at the front desk handed you a slip of paper with your next appointment. You thanked her, smiling brightly, as Ramsay led you from the office. Your smile faltered slightly as you saw Damon's car parked next to yours.
"I won't be long." Ramsay said, pressing a kiss to your temple and then stepping into Damon. "She will get home safe or even Satan himself will have pity on you." He growled so threateningly it made your blood run cold.
"Y-yes, of course." Damon trembled, opening the door for you.
You said nothing as Damon wound his way out of the downtown. You didn't like him. Something about him made you uneasy. But he was Ramsay's right hand. He had more brains than some of the men Ramsay had employed.
"You hungry, ma'am?" Damon asked, waiting on the stoplight to turn green.
"No. Thank you though." You said, watching a group of people hurry across the street, bundled against the harsh December wind and laden with shopping bags.
×××
You were curled up on the couch, under a blanket, reading when both dogs sat up and growled at the front door. You peered at them in interest as the doorbell rang.
You hurried to the door as the dogs barked. Peering out the peep hole you saw two men in suits standing on your door step.
Slowly you opened the door.
The taller of the two, a auburn haired man gave you a smile, while the sandy haired man gave you a nod.
"Mrs. Bolton?" The auburn haired man asked, flashing a badge.
Your stomach dropped, but you put on a sweet smile, "Yes. May I help you gentlemen?"
"We have a few questions for you. I'm detective Stark and this is my partner Detective Greyjoy."
"Yes, of course. Please, come in out of the cold." You said opening the door wider. Kira and Willow on your heels, emitting low, rumbling growls. You snapped your fingers and the dogs reluctantly retreated across the room to their beds, but never taking their eyes off the men.
You motioned to the empty love seat and the two detectives sat down.
"Can I offer you gentlemen anything to drink? Tea, coffee, water?" You asked taking your seat, and folding your blanket up.
"No thank you." Detective Greyjoy said, eyeing you up and down.
Your phone lit up on the coffee table.
[Ramsay: 5 min]
"If you'll excuse me a second." You said, picking your phone up and hitting call.
'Yes baby doll?' Ramsay said on the other end.
"Hey, wanted to finish up that cake for your father. Can you bring home some sugar?" You said, looking down at the coffee table.
'Of course, baby. See you soon. I love you.'
"Be careful. I love you too." You said, hanging up and turning back to the detectives. "Sorry, I just wanted to catch him before he got home. Really don't wanna be out in this cold."
'Bring home some sugar' was your code phrase to let Ramsay know unexpected company had shown up.
"Not a problem at all. But, last night a man was murdered behind the bar you work at. Reports say you were the last one to see him." Detective Stark said, pulling a picture from his jacket pocket and laying it on the coffee table and sliding it towards you.
You picked up the photo with trembling fingers and taking in a sharp gasp. "Oh my god." It was a picture of Dogbait Farlan as he was known at the bar. You looked up from the picture, trying to remember yesterday. You had been feeling ill and were only half there.
"What... what happened?" You asked, looking between the two men.
"Stabbed to death it seems." Greyjoy spoke, glancing around your house. "Awfully nice place for someone who works at a bar."
His partner gave him a scowl.
You bristled, "I've been working at the bar since I was eighteen. The customers love me and tip me well. Besides i co-own it, if you must know. And my husband works at the bank. We don't hurt for money, thank you."
"Please forgive my partner's rudeness. He's having a bad day it seems." Stark spoke up quickly.
You pursed your lips and turned your gaze to the red head, "is your mother the OBGYN at the place down town?"
The man nodded.
"I saw her today. She confirmed my pregnancy." You said, making small talk. If you could keep them talking until Ramsay got home you'd feel better.
"Congratulations. You must be excited."
You nodded, smiling. Glancing up as Ramsay entered the house, looking rather goofy with a bag of sugar. He gave you a quick look and then ran his eyes over the detectives.
Both men stood, pulling their badges. Ramsay gave a nod. You watched him take an interest in the Greyjoy man
"Has my wife done something I should know about? Money laundering? Murder? Grand theft auto, perhaps?" Ramsay asked, dropping the sugar on the coffee table and taking a seat beside you.
Detective Stark gave a laugh, putting his badge away, and sitting down again. "No, sir. But we had information that she was the last one to speak to our murder victim last night before we was found dead behind the bar.
From the corner of your eye you saw Ramsay narrow his slightly.
Bastard. You knew it. It was him. It had to be.
"So, what can you tell us?" Greyjoy asked.
"Well, I mean, it was a slow evening. Just the regulars. I left early. I wasn't feeling well and had a date with my husband. But by the time I got home I was feeling too bad to go out. But as far as the bar... Nothing out of the ordinary, honestly. Farlan was my last customer before clocking out, yes. He ordered a beer, drank it, and left. He wasn't with anyone that I know of, and he didn't seem distressed in any way. He was telling me about his new litter of hounds and was just regular ol' Farlan. Sorry if I'm not much help. I can't believe... I mean... He was a good guy." You said, playing up emotion at the end. Ramsay draped his arm around your shoulders and gave you a small squeeze. To let you know you were playing your part wonderfully.
"No enemies? He didn't owe anyone any money or favors?" Stark asked.
You frowned, shaking your head. "Not that I'm aware of. He was a pretty quiet man. After him and his wife divorced he kept himself to himself mostly."
The detectives exchanged looks, telling you they were back to square one. Stark sighed and rose from his seat.
He held his hand out to you and Ramsay in turn.
"Thank you for your time. If you hear anything, please give us a call."
"Of course. Good luck." Ramsay said, politely showing the men to the door.
Once they were gone, Ramsay clicked the lock and watched as they drove away. He then walked over to the chair they sat in and pulled all the cushions and pillows, examining every inch.
He stood back up and turned to you.
You grinned at him, picking up the bag of sugar. "We may have more sugar than anyone in the world now. When the apocalypse happens we can make our fortune selling sugar." You giggled.
Ramsay snorted, following you to the kitchen.
"Did you do it?" You asked casually, glancing at your husband over your shoulder as you placed the bag of sugar on a shelf in the pantry.
"No. Wasn't us. We were across town."
You frowned, crossing your arms. "Then who? I mean, who'd want to kill that man? Everyone loved him."
Ramsay shrugged, stepping into you and pulling you into him.
"Go get ready for dinner."
"I didn't like that one detective. He was rude." You said, slipping your dress on and pulling your hair aside so Ramsay could zip it.
He kissed along your bare skin before pulling the zipper up.
"Rude, how?" He asked, placing a diamond necklace around your neck and clasping it.
You fingered the new necklace and stared at it in the mirror.
"Rams, this is beautiful." You whispered.
"Thought my little momma might like it when I saw it in the window. Now, tell me about the detective." Ramsay said, kissing your cheek.
You turned to face him, "he was just all like, 'this is an awfully nice place for someone who works at a bar.' Fucking rude ass."
You saw the gears turning behind your husband's eyes.
"Don't do anything stupid, please." You added quickly.
Ramsay smirked, "I would do no such thing, baby girl."
"Liar." You whispered, pressing your lips to his.
His grin widened against your lips, but said nothing as he kissed you back.
#ramsay bolton x reader#ramsay bolton#ramsay bolton imagines#game of thrones#game of thrones imagines#mafia au#ao3fic#ao3 writer#guns for hire#kee_theyoungwolf#kee-writestrash#modern ramsay bolton#ramsay is his own warning#game of thrones au#game of thrones fic#archiveofourown
32 notes
·
View notes
Link
“These twelve dubious concepts promote conflict, cruelty, suffering and death rather than love and peace.
1. Chosen People –The term “Chosen People” typically refers to the Hebrew Bible and the ugly idea that God has given certain tribes a Promised Land (even though it is already occupied by other people). But in reality many sects endorse some version of this concept. The New Testament identifies Christians as the chosen ones. Calvinists talk about “God’s elect,” believing that they themselves are the special few who were chosen before the beginning of time. Jehovah’s witnesses believe that 144,000 souls will get a special place in the afterlife. In many cultures certain privileged and powerful bloodlines were thought to be descended directly from gods (in contrast to everyone else).
Religious sects are inherently tribal and divisive because they compete by making mutually exclusive truth claims and by promising blessings or afterlife rewards that no competing sect can offer. “Gang symbols” like special haircuts, attire, hand signals and jargon differentiate insiders from outsiders and subtly (or not so subtly) convey to both that insiders are inherently superior.
2. Heretics – Heretics, kafir, or infidels (to use the medieval Catholic term) are not just outsiders, they are morally suspect and often seen as less than fully human. In the Torah, slaves taken from among outsiders don’t merit the same protections as Hebrew slaves. Those who don’t believe in a god are corrupt, doers of abominable deeds. “There is none [among them] who does good,” says the Psalmist. Islam teaches the concept of “dhimmitude” and provides special rules for the subjugation of religious minorities, with monotheists getting better treatment than polytheists. Christianity blurs together the concepts of unbeliever and evildoer. Ultimately, heretics are a threat that needs to be neutralized by conversion, conquest, isolation, domination, or—in worst cases—mass murder.
3. Holy War – If war can be holy, anything goes. The medieval Roman Catholic Church conducted a twenty year campaign of extermination against heretical Cathar Christians in the south of France, promising their land and possessions to real Christians who signed on as crusaders. Sunni and Shia Muslims have slaughtered each other for centuries. The Hebrew scriptures recount battle after battle in which their war God, Yahweh, helps them to not only defeat but also exterminate the shepherding cultures that occupy their “Promised Land.” As in later holy wars, like the modern rise of ISIS, divine sanction let them kill the elderly and children, burn orchards, and take virgin females as sexual slaves—all while retaining a sense of moral superiority.
4. Blasphemy – Blasphemy is the notion that some ideas are inviolable, off limits to criticism, satire, debate, or even question. By definition, criticism of these ideas is an outrage, and it is precisely this emotion–outrage–that the crime of blasphemy evokes in believers. The Bible prescribes death for blasphemers; the Quran does not, but death-to-blasphemers became part of Shariah during medieval times.The idea that blasphemy must be prevented or avenged has caused millions of murders over the centuries and countless other horrors. As I write, blogger Raif Badawi awaits round after round of flogging in Saudi Arabia—1000 lashes in batches of 50—while his wife and children plead from Canada for the international community to do something.
5. Glorified suffering – Picture secret societies of monks flogging their own backs. The image that comes to mind is probably from Dan Brown’s novel, The Da Vinci Code, but the idea isn’t one he made up. A core premise of Christianity is that righteous torture—if it’s just intense and prolonged enough–can somehow fix the damage done by evil, sinful behavior. Millions of crucifixes litter the world as testaments to this belief. Shia Muslims beat themselves with lashes and chains during Aashura, a form of sanctified suffering called Matam that commemorates the death of the martyr Hussein. Self-denial in the form of asceticism and fasting is a part of both Eastern and Western religions, not only because deprivation induces altered states but also because people believe suffering somehow brings us closer to divinity.
Our ancestors lived in a world in which pain came unbidden, and people had very little power to control it. An aspirin or heating pad would have been a miracle to the writers of the Bible, Quran, or Gita. Faced with uncontrollable suffering, the best advice religion could offer was to lean in or make meaning of it. The problem, of course is that glorifying suffering—turning it into a spiritual good—has made people more willing to inflict it on not only themselves and their enemies but also those who are helpless, including the ill or dying (as in the case of Mother Teresa and the American Bishops) and children (as in the child beating Patriarchy movement).
6. Genital mutilation – Primitive people have used scarification and other body modifications to define tribal membership for as long as history records. But genital mutilation allowed our ancestors several additional perks—if you want to call them that. In Judaism, infant circumcision serves as a sign of tribal membership, but circumcision also serves to test the commitment of adult converts. In one Bible story, a chieftain agrees to convert and submit his clan to the procedure as a show of commitment to a peace treaty. (While the men lie incapacitated, the whole town is then slain by the Israelites.)
In Islam, painful male circumcision serves as a rite of passage into manhood, initiation into a powerful club. By contrast, in some Muslim cultures cutting away or burning the female clitoris and labia ritually establishes the submission of women by reducing sexual arousal and agency. An estimated 2 million girls annually are subjected to the procedure, with consequences including hemorrhage, infection, painful urination and death.
7. Blood sacrifice – In the list of religion’s worst ideas, this is the only one that appears to be in its final stages. Only some Hindus (during the Festival of Gadhimai) and some Muslims (during Eid al Adha, Feast of the Sacrifice) continue to ritually slaughter sacrificial animals on a mass scale. Hindu scriptures including the Gita and Puranas forbid ritual killing, and most Hindus now eschew the practice based on the principle of ahimsa, but it persists as a residual of folk religion.
When our ancient ancestors slit the throats on humans and animals or cut out their hearts or sent the smoke of sacrifices heavenward, many believed that they were literally feeding supernatural beings. In time, in most religions, the rationale changed—the gods didn’t need feeding so much as they needed signs of devotion and penance. The residual child sacrifice in the Hebrew Bible (yes it is there) typically has this function. Christianity’s persistent focus on blood atonement—the notion of Jesus as the be-all-end-all lamb without blemish, the final “propitiation” for human sin—is hopefully the last iteration of humanity’s long fascination with blood sacrifice.
8. Hell – Whether we are talking about Christianity, Islam or Buddhism, an afterlife filled with demons, monsters, and eternal torture was the worst suffering that Iron Age minds could conceive and medieval minds could elaborate. Invented, perhaps, as a means to satisfy the human desire for justice, the concept of Hell quickly devolved into a tool for coercing behavior and belief.
Most Buddhists see hell as a metaphor, a journey into the evil inside the self, but the descriptions of torturing monsters and levels of hell can be quite explicit. Likewise, many Muslims and Christians hasten to assure that it is a real place, full of fire and the anguish of non-believers. Some Christians have gone so far as to insist that the screams of the damned can be heard from the center of the Earth or that observing their anguish from afar will be one of the pleasures of paradise.
9. Karma – Like hell, the concept of karma offers a selfish incentive for good behavior—it’ll come back at you later—but it has enormous costs. Chief among these is a tremendous weight of cultural passivity in the face of harm and suffering. Secondarily, the idea of karma can sanctify the broad human practice of blaming the victim. If what goes around comes around, then the disabled child or cancer patient or untouchable poor (or the hungry rabbit or mangy dog) must have done something in this or a previous life to bring their position on themselves.
10. Eternal Life – To our weary and unwashed ancestors, the idea of gem encrusted walls, streets of gold, the fountain of youth, or an eternity of angelic chorus (or sex with virgins) may have seemed like sheer bliss. But it doesn’t take much analysis to realize how quickly eternal paradise would become hellish—an endless repetition of never changing groundhog days (because how could they change if they were perfect).
The real reason that the notion of eternal life is such a bad invention, though, is the degree to which it diminishes and degrades existence on this earthly plane. With eyes lifted heavenward, we can’t see the intricate beauty beneath our feet. Devout believers put their spiritual energy into preparing for a world to come rather than cherishing and stewarding the one wild and precious world we have been given.
11. Male Ownership of Female Fertility – The notion of women as brood mares or children as assets likely didn’t originate with religion, but the idea that women were created for this purpose, that if a woman should die of childbearing “she was made to do it,” most certainly did. Traditional religions variously assert that men have a god-ordained right to give women in marriage, take them in war, exclude them from heaven, and kill them if the origins of their offspring can’t be assured. Hence Catholicism’s maniacal obsession with the virginity of Mary and female martyrs. Hence Islam’s maniacal obsession with covering the female body. Hence Evangelical promise rings, and gender segregated sidewalks in Jerusalem and orthodox Jewish women wearing wigs over shaved heads in New York.
As we approach the limits of our planetary life support system and stare dystopia in the face, defining women as breeders and children as assets becomes even more costly. We now know that resource scarcity is a conflict trigger and that demand for water and arable land is growing even as both resources decline. And yet, a pope who claims to care about the desperate poor lectures them against contraception while Muslim leaders ban vasectomies in a drive to outbreed their enemies.
12. Bibliolatry (aka Book Worship) – Preliterate people handed down their best guesses about gods and goodness by way of oral tradition, and they made objects of stone and wood, idols, to channel their devotion. Their notions of what was good and what was Real and how to live in moral community with each other were free to evolve as culture and technology changed. But the advent of the written word changed that. As our Iron Age ancestors recorded and compiled their ideas into sacred texts, these texts allowed their understanding of gods and goodness to become static. The sacred texts of Judaism, Christianity and Islam forbid idol worship, but over time the texts themselves became idols, and many modern believers practice—essentially—book worship, also known as bibliolatry.
“Because the faith of Islam is perfect, it does not allow for any innovations to the religion,” says one young Muslim explaining his faith online. His statement betrays a naïve lack of information about the origins and evolution of his own dogmas. But more broadly, it sums up the challenge all religions face moving forward. Imagine if a physicist said, “Because our understanding of physics is perfect, it does not allow for any innovations to the field.” Adherents who think their faith is perfect, are not just naïve or ill informed. They are developmentally arrested, and in the case of the world’s major religions, they are anchored to the Iron Age, a time of violence, slavery, desperation and early death.
Ironically, the mindset that our sacred texts are perfect betrays the very quest that drove our ancestors to write those texts. Each of the men who wrote part of the Bible, Quran, or Gita took his received tradition, revised it, and offered his own best articulation of what is good and real. We can honor the quest of our spiritual ancestors, or we can honor their answers, but we cannot do both.
Religious apologists often try to deny, minimize, or explain away the sins of scripture and the evils of religious history. “It wasn’t really slavery.” “That’s just the Old Testament.” “He didn’t mean it that way.” “You have to understand how bad their enemies were.” “Those people who did harm in the name of God weren’t real [Christians/Jews/Muslims].” Such platitudes may offer comfort, but denying problems doesn’t solve them. Quite the opposite, in fact.
Change comes with introspection and insight, a willingness to acknowledge our faults and flaws while still embracing our strengths and potential for growth. In a world that is teeming with humanity, armed with pipe bombs and machine guns and nuclear weapons and drones, we don’t need defenders of religion’s status quo—we need real reformation, as radical as that of the 16th Century and much, much broader. It is only by acknowledging religion’s worst ideas that we have any hope of embracing the best.”
Valerie Tarico is a psychologist and writer in Seattle, Washington.
https://valerietarico.com/2015/01/20/religions-dirty-dozen-12-really-bad-religious-ideas-that-have-made-the-world-worse/
384 notes
·
View notes
Text
Is Western Puppet Navalny a Drug Fiend Who Overdosed on Lithium and Benzo? Has He Been Messing With Mr. Prescription High?
— John Helmer | 29 October, 2021

How did eye drop medicine get into his hair? Eye drop medicine that doesn’t enter the bloodstream topically but is in Russia and Italy injected by adventurous people seeking a good time
German clinical evidence of Alexei Navalny’s chronic use of lithium and benzodiazepine drugs before his sensational collapse last year is being withheld and covered up by the Berlin doctors who obtained the evidence from testing a sample of Navalny’s hair.
The significance of the hair testing was identified this month by an expert toxicologist employed by the British government. “[It] would be interesting,” he said, requesting his name not be released, “to see the hair test as this will reflect only the drugs given up to six days and more earlier in Russia.”
Dr Kai-Uwe Eckardt, the head of the team of German doctors treating Navalny in Berlin’s Charité University Hospital, reported publicly last December that “a hair sample obtained on day 4 confirmed the presence of several of the compounds detected in blood and urine.” Day-4 in Berlin meant August 24, four days after Navalny alleges he was poisoned in Tomsk by Novichok on orders of the Kremlin. Navalny’s allegation was endorsed by the German, British and US governments on the evidence, they said at the time, of Navalny’s tests in Germany.
This allegation was repeated last week at the Organisation for the Prohibition of Chemical Weapons (OPCW) in The Hague. According to an October 5 statement by a group of OPCW member governments, “it is now more than a year since Mr Alexei Navalny was poisoned with a nerve agent whilst travelling in Russia. The OPCW Technical Secretariat confirmed, following a Technical Assistance Visit to Germany, that Mr Navalny was exposed to a nerve agent from the Novichok group. This is a matter of grave concern.”
Led by Germany, the UK and US, the governments also charged that “the Russian Federation has not yet provided a credible explanation of the incident that took place on its soil.”
The Russian Foreign Ministry responded two days later, on October 7, charging the accusers of “inconsistencies, contradictions, misinformation, shady developments that have yet to be clarified, insinuations at the highest political level and outright lies professed by the West… a provocation, crudely planned and coarsely executed by the special services of some Western countries.”
The significance of the hair sample testing by the German doctors is that the results corroborate lithium and benzodiazepine drug use in Navalny’s blood and urine found on his arrival in Berlin.
An independent British toxicologist adds that the levels of the drugs in the hair testing would also confirm Navalny’s dependence on these drugs in Russia, well before he arrived in Tomsk and long before the Novichok “incident” alleged at OPCW last week.
“Without seeing the actual hair analysis report, we are guessing which specific drugs and compounds were common to the blood and urine and hair. The hair ones are all pre-attack compounds. If ‘several’ drugs were in the hair, as the Berlin report says, then Navalny would be described as a chronic abuser. That, plus his multiple bacterial infections the Berlin report also identifies, would make the trained professional clinician looking at the data believe that the patient was a down-at-heel street person with a serious drug problem and mental health issues.”
Medical psychiatrists and toxicologists acknowledge that the “cocktail” combination of drugs Navalny had been taking before he collapsed on August 20 may explain his subsequent symptoms and the cause of his collapse. Lithium, according to the British government toxicologist reporting last week, “would not be detected by normal drug screening and must have been indicated for some reason to cause them [the Charité hospital doctors] to carry out as a special, targeted test. It would be interesting to know why it was tested for and the blood concentration – were the Russians treating [Navalny] for a bipolar disorder?”
Eckardt was asked to explain his reason for testing Navalny for lithium and benzodiazepines. He was also asked what specific compounds were detected in the Day-4 hair sample testing he directed. Eckardt refused to answer, or to provide what OPCW called last week “a credible explanation”.
Last December, Eckardt, co-author David Leindl, and twelve other German doctors signed a clinical report on the Navalny case, which was published by The Lancet.

Dr Kai-Uwe Eckardt, identified publicly and thanked by Navalny as head of the team treating him. According to the published paper, Eckardt and Leindl “wrote the first draft of the report, coordinated internal revision, and prepared the submitted version….[They] had unlimited access to all clinical data and reports.” These reports, according to Eckardt and Leindl, included reports from the German Bundeswehr Institute of Pharmacology and Toxicology in Munich “who did repetitive measurements of…cholinesterase status and gave toxicological advice”.
Attached to the Navalny case report was what Eckardt and Leindl called a “Supplementary Appendix”. This comprises four separate clinical data summaries. Read them all here.
Appendix S2 says it reports the results of testing of Navalny’s blood and urine samples “on the arrival of the patient at Charité – Universitatsmedizin Berlin (day 3). Day 3 was August 22, 2020. For telltale analysis of each of the compounds identified, read this. For an independent medico-psychiatric diagnosis of the pattern of drug- taking revealed.
Supplementary appendix
This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Steindl D, Boehmerle W, Körner R, et al. Novichok nerve agent poisoning. Lancet 2020; published online Dec 22. http://dx.doi.org/10.1016/S0140-6736(20)32644-1.
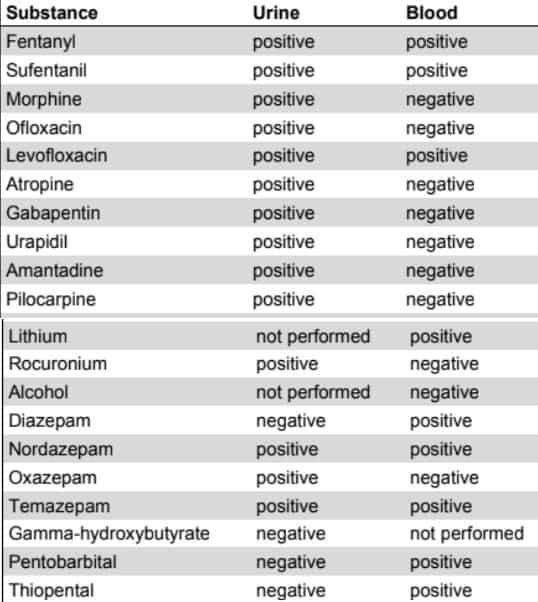
Appendix S2: Results of local toxicology and medication tests in blood and urine samples obtained on arrival of the patient at Charité - Universitätsmedizin Berlin (day 3). A hair sample obtained on day 4 confirmed the presence of several of the compounds detected in blood and urine and, in addition, revealed the presence of Tropicamide. Results of toxicology analyses conducted in a special laboratory of the armed forces are not included
From: https://drive.google.com/file/d/1zYD6nPDhmpuTsu6r-BReHaI-wVLiXzoh/
The British government toxicologist requested to review this and the three other appendices commented:
“[this is] an interesting cocktail and as far as I can see, most drugs administered to him (perhaps under guidance from medics experienced at treating OP [organophosphate] poisoning elsewhere in the world). Fentanyl [was] certainly given in air ambulance – not sure about sufentanil although it’s mentioned in the Lancet paper and was probably also given in the ambulance. It is interesting that a lot of propofol and midazolam was administered but neither reported (detected). How good is the [Berlin] tox testing? Would be interesting to see the hair test as this will reflect only drugs given up to 6 days and more earlier in Russia.”
“[I am] surprised about lack of atropine in blood – Russians must have stopped it or testing insensitive. Barbiturates & rocuronium consistent with intubation and forced ventilation but odd that no barbs in urine while blood positive. Also odd that rocuronium negative in blood (when used in UK you find it for weeks afterwards, so again I wonder about quality of [the Berlin] tox?).”
The scientific research literature reveals that lithium concentrations can be measured in hair samples from six to twelve months before the hair is tested. Hair sampling is also a standard procedure used by police for evidence of illegal purchase and consumption of benzodiazepines.
“Hair has been identified as a good analytical specimen and probative evidence for chronic drug use. Results obtained from the analysis of hair specimens provide sufficient evidence of previous drug usage as well as information on the duration for which the drug was used, depending on the growth rate of hair (approximately 1 cm/month), and thus can serve as key evidence in legal decisions.”
Of the benzodiazepine drugs recorded in Navalny’s body in Berlin, temazepam (brand name Restoril) is relatively short-lasting; diazepam (Valium), nordiazepam (CalmDay) and oxazepam (Serax) will be found in hair testing for up to 90 days. Concentrations of these drugs are still measurable in hair samples after 10 months.
An independent British toxicologist who specializes in the organophosphates found in fertilizers and chemical weapons commented that “anything found in the hair sample must be 21 days [since ingestion] or even further back in time.” That means 21 days before August 24, 2020 – August 3, 2020.
It was midsummer in Russia at the time, and Navalny has advertised daily publicity photographs of himself in brimming health, secure and unthreatened. On Sunday, August 2, 2020, Navalny was at a distance running event in Moscow. On Monday, August 3, 2020, and Tuesday, August 4, he published an Instagram of himself in his office. On Wednesday, August 5, he was at his dacha outside the city. On Friday, August 7, he was waterboarding on a Moscow region river.




Top Left: Alexei Navalny tweets from an outdoor run in Moscow, August 2, 2020. Top Right: Navalny in his Moscow office on August 4, 2020. Bottom Left: Navalny and his wife Yulia Navalnaya at their dacha on August 5, 2020. Bottom Right: Navalny in a river waterboading video clip he made behind a speedboat, Moscow August 7, 2020.
The hair sample testing reported in Berlin on August 23, 2020, revealed the drugs which Navalny was consuming on the days of the published photographs. These hair test results have been withheld by the Charité hospital doctors, although Eckardt and Leindl acknowledge knowing what they were.
“The German doctors say ‘several’ of the blood and urine-detected drugs were also found in Navalny’s hair,” the non-government British expert said last week. “I don’t see any logical reason in giving a comprehensive blood and urine report, and not do the same with hair. Without seeing the actual hair analysis report, we are guessing which specific drugs and compounds were common to blood/urine and hair.” What is medically certain, however, according to the British toxicologist, is that “the hair ones are all pre-attack compounds.”
“Alcohol use/abuse is perhaps the most common type of hair test,” according to this source. “You can keep off the booze for a day or two, but the hair does not lie. Ethyl glucuronide is the ethanol metabolite which is present in hair. Again, four weeks and older is the history [in the hair test]”.
The Eckardt-Leindl report in The Lancet describes in detail many types of tests for Navalny, including “toxicological analysis and drug screening in blood and urine samples obtained on admission”; “cranial CT and MRI scans”; “analysis of cerebrospinal fluid”; “skin swabs obtained on admission”; “laboratory analyses [of blood] plasma”; and the “hair sample obtained on day 4”.
The only test results not precisely identified by Eckardt and Leindl from this list were from the hair sample test. Instead, they noted the “presence of several of the compounds detected in blood and urine” – without identifying what they were. “In addition,” Eckardt and Leindl claim, their hair testing “revealed the presence of Tropicamide.”
The British experts query why Eckardt and Leindl specified tropicamide but omitted the other compounds. Tropicamide is an atropine-type drug typically used in the form of drops for eye treatment. Navalny has required eye treatment since 2017, when he was attacked. On the other hand, in Russia and Italy, according to published medical research, tropicamide is used intravenously to achieve highs in combination with alcohol and opiates. When tropicamide is combined in overdose, the “medical effects of tropicamide misuse include slurred speech, persistent mydriasis [dilation of the eye pupil], unconsciousness/unresponsiveness, hallucinations, kidney pain, dysphoria, ‘open eye dreams’, hyperthermia, tremors, suicidal feelings, convulsions, psychomotor agitation, tachycardia and headache.” In 2017, this report on drug abuse in Russia noted that tropicamide was the “latest street drug”.
An internationally recognized European eye surgeon comments that tropicamide is a fast-acting topical application whose effect to relax the eye muscles and dilate the pupils disappears within two hours. He believes the drug does not enter the body’s biochemical system, so it would not register on blood or hair tests. Testing of biomedical system responses to tropicamide drops in the eye, such as heart rate and blood pressure, shows no effect. Once Eckardt and Leindl discovered the tropicamide in Navalny’s hair sample test, they recognised that Navalny had taken the drug for a non-medical purpose.
According to this review of the medical research on tropicamide abuse, “acute tropicamide intoxications can lead to anticholinergic syndrome, hyperthermia, tremors and convulsions. Chronic tropicamide-related problems include cardiovascular toxicity, psychosis, renal or liver failures, severe weight loss and infections.” For the layman, the commonest cause of “anticholinergic syndrome” is poisoning from drug overdoses.
Reporting on Navalny, the Berlin doctors led by Eckardt and Leindl said that “based on clinical and laboratory findings, severe cholinesterase inhibition was diagnosed.” But Eckardt and Leindl also say they did not measure this themselves at their Berlin hospital. Nor do they claim to have found Novichok in any of the Navalny samples they tested.
Instead, they report that it was the “Bundeswehr [German Army] Institute of Pharmacology and Toxicology (IPTB] in Munich, Germany, who did repetitive measurements of butyrlcholinesterase, aceltycholinesterase in red blood cells, and cholinesterase status and gave toxicological advice.” For more on this military unit and its role in the Navalny Novichok operation, read this and this .
The principal medical doctor responsible for the IPTB testing in Munich was Horst Thiermann. He claims to have detected nerve agent poisoning in Syria, Iraq, Japan and Malaysia. In November 2018 Thiermann gave a speech to a trade fair in Dusseldorf selling medical technology to NATO and other armies; Thiermann’s speech was entitled “bedside diagnostic and biomedical verification of exposure to chemical warfare agents”.

Left: Dr Horst Thiermann.
Next month, on November 15, 2021, Thiermann will appear again at the same Dusseldorf trade fair, selling his advice on “therapy & verification of poisoning by organo-phosphorus compounds”. This will be Thiermann’s first public appearance since his role in authorizing the Novichok allegation was revealed by Eckardt and Leindl in The Lancet.

For attendance at Thiermann’s presentation on November 15 for journalists and “interested parties”, fill in this application to the organisers, Medica Dusseldorf.
The British government toxicologist and the British organophosphorus expert have called into question why Eckardt and the Charité hospital in Berlin failed to test and measure Navalny’s cholinesterase indicators, and why they relied instead on Thiermann and the German Army. Said the second of these sources:
“The Berlin hospital relying on the Army or any outside lab to perform the Acetylcholine esterase [AChE] assay makes no sense at all. Berlin seemed to have no issues in measuring Butyrylcholine esterase, but not the more relevant AChE. Take the example of a German farmer accidentally poisoning himself with OP [organophosphorus] pesticide. Would the Berlin hospital really have to rely on the Army? The AChe assay is simple, straightforward. AChe is the most critical assay, yet it was ‘sent out’ to an Army lab. What was the reason?”
Eckardt and Leindl were contacted by email at their Charité hospital office, and asked to clarify the medical evidence which they have published in The Lancet under their names.
From: "John Helmer"
To: "nephro-intensiv" «[email protected]>
Sent: 08/10/2021 11:08:08
Subject: Attn: Prof Kai-Uwe Eckardt & Dr David Leindl
Independent expert toxicological review of your case report and your data presentation in the supplementary appendices notes that the hair sample testing "will reflect only drugs given up to 6 days and more earlier in Russia". Published clinical research papers with which you are familiar confirm that hair samples may indicate lithium and benzodiazepines for at least 21 days after ingestion, and that there are many types of testing for these drugs in standard use. For example, I refer to: https://pubmed.ncbi.nlm.nih.gov/1576379/ The independent toxicology expert also states that lithium, which you record as positive in the blood in Appendix 52, "would not be detected by normal drug screening and must have been indicated for some reason to cause them [Charite] to carried out as a special, targeted test." In light of these fresh observations I request you to say - (1) what reason was there for you to carry out the special targeted test for lithium? - (2) what specific compounds were detected in the Day-4 hair sample testing? In the event that you refuse to answer these questions, it will be reported that you refuse; that the independently sourced evidence will stand that lithium and the four benzodiazepines identified in your Appendix 52 were identified in Mr Navalnys hair sample; and that by refusing to disclose, report or comment on the Day-4 hair sample testing you undertook, you intend to withhold these data from scientific analysis.
Eckardt and Leindl have not replied. They refuse to respond to the evidence analysis provided by the British experts.
After this report was published, Eckardt and Leindl were asked to read it and to respond to the medical evidence casting “doubt on the veracity of the case report you signed”. Noting Novichok in the headline of their Navalny case report and tropicamide in Appendix S2, Eckardt and Leindl were asked “whether you believe withholding clinical results of Mr Navalny’s hair tests in the context of your Lancet case report is professionally appropriate.” CASE REPORT.
Novichok nerve agent poisoning
David Steindl, Wolfgang Boehmerle, Roland Körner, Damaris Praeger, Marcel Haug, Jens Nee, Adrian Schreiber, Franziska Scheibe, Katharina Demin, Philipp Jacoby, Rudolf Tauber, Sven Hartwia, Matthins Endres, Kai -LAve Eckardt
Eckardt and Leindl refuse to answer.
— Source: Dances With Wolves
0 notes
Text
Does It Have an Effect?
New Post has been published on https://depression-md.com/does-it-have-an-effect/
Does It Have an Effect?

High blood pressure, or hypertension, can lead to serious health concerns like a heart attack or stroke. But because hypertension doesn’t typically cause symptoms, many people who have it don’t even know. That’s why it’s so important to regularly check your blood pressure.
If you have hypertension, you may have heard that cannabidiol (CBD) can help lower blood pressure. Here’s what the research says, plus tips for finding a few products to explore.
Blood pressure is defined as the pressure of blood against the walls of the arteries. While it’s normal for blood pressure rates to rise and fall over the course of a day, consistently high blood pressure levels are an issue.
There are two kinds of hypertension:
Primary hypertension is the most common. It develops gradually with no discernible cause, but it may be linked to genetics, physical changes in the body, or high body weight.
Secondary hypertension comes on quickly and can be more serious. It has a number of causes, including kidney disease, congenital heart defects, thyroid issues, alcohol consumption, and certain medications and stimulants, like cocaine and amphetamines.
Since hypertension is often a silent condition, you may not experience symptoms until the condition has developed in severity. At that point, symptoms may include:
headaches
nosebleeds
shortness of breath
dizziness
chest pain
flushing
changes in vision
blood in the urine
If you’re experiencing these kinds of symptoms, it’s important to seek medical attention right away.
CBD is one of the active compounds in the cannabis plant. Unlike tetrahydrocannabinol (THC), it doesn’t have intoxicating properties or produce a “high.” Instead, much focus is on the potential therapeutic benefits of CBD. It may be helpful for everything from pain relief and improved sleep to anxiety, and even addiction.
CBD is available in a few different types: full-spectrum, broad-spectrum, and isolate.
While full-spectrum and broad-spectrum both contain other compounds from the cannabis plant — like flavonoids, terpenes, and other cannabinoids — full-spectrum CBD is the only type that contains some THC (usually less than 0.3 percent).
CBD isolate is pure CBD. But it’s important to know that any type of CBD may contain trace amounts of THC that could show up on a drug test.
These three forms of CBD are made into a variety of products, including:
Oils and tinctures. These liquids have been infused with CBD. You can either place them under your tongue or add them to food and drinks.
Edibles. Sometimes, CBD is added to foods like gummies or drinks like teas. Edibles are among the most popular methods of consumption because they’re discreet and easy to dose.
Capsules. CBD can be taken in pill or capsule form.
Topicals. Topical CBD is applied directly to the skin for targeted relief.
Vape juices. These products are designed to be inhaled using a vape pen. Effects are very fast, but there have been reports of lung injuries associated with vaping. At this time, we don’t know if vaping CBD poses the same risks.
CBD interacts with the body’s endocannabinoid system (ECS), a complex system that helps regulate a number of processes in the body.
While our understanding of the ECS is still unfolding, we know it’s made of three components:
endocannabinoids, which are molecules made in the body
endocannabinoid receptors, which are found throughout the body; the main receptors are called CB1 and CB2 receptors
enzymes, which break down endocannabinoids once they’ve completed their function
At this time, researchers believe the primary role of the ECS is maintaining homeostasis in the body. The ECS is linked to a number of processes in the body, including:
appetite and digestion
metabolism
pain
mood
sleep
motor control
Cannabinoids, including THC and CBD, interact with the ECS by binding to the receptors in the same manner as endocannabinoids.
While THC can bind to both CB1 and CB2 receptors, researchers don’t yet understand how CBD interacts with the ECS. One theory is that CBD prevents endocannabinoids from being broken down, giving them a greater effect on the body. Another theory is that CBD binds to a receptor that researchers haven’t identified yet.
There is research from 2011 that suggests taking both THC and CBD, along with the other compounds in the cannabis plant, may be more effective than using a single cannabinoid alone. This theory is called the entourage effect, and it’s why some people say full-spectrum CBD works better than broad-spectrum or isolate.
There is evidence that CBD products could help lower blood pressure, but research is somewhat contradictory.
A 2017 study of nine male participants found that a single dose of CBD in healthy participants lowered blood pressure for those at rest and those who were under stress.
Another 2017 study in mice found that CBD significantly reduced stress-induced increases in blood pressure and heart rate.
But a 2020 study in rats found that CBD wasn’t effective in lowering blood pressure, though it did have an antioxidant effect. Another 2020 study was more promising, with results demonstrating that CBD could reduce blood pressure in patients who were stressed.
Researchers acknowledge the beneficial effects of CBD for cardiovascular disorders, but note that additional studies are needed to fully understand how it might contribute.
Both the Food and Drug Administration (FDA) and the World Health Organization (WHO) acknowledge the potential benefits of CBD.
A 2017 WHO report describes CBD as generally well-tolerated with a good safety profile and no effects that might indicate the potential for misuse or dependence.
The FDA notes that more research is needed, and it points out that there are many unanswered questions about CBD’s safety. Furthermore, it notes that some CBD products are inaccurately labeled and of questionable quality.
If you do decide to try CBD, know that some people experience side effects, including:
diarrhea
changes in weight or appetite
fatigue
Research from 2012 on cannabinoids and anxiety suggests that some cannabinoids may have a biphasic effect, meaning they produce different effects depending on the dose you take.
For high blood pressure specifically, a 2011 study found that THC alone or in combination with CBD sometimes resulted in an increase in blood pressure, and sometimes in a decrease.
Finally, it’s crucial to keep in mind that CBD may interact with some medications, including those used for hypertension. If you’re considering using CBD to help manage high blood pressure, talk with a doctor first.
While CBD comes in many forms, the best option for high blood pressure is likely an oil or tincture rather than a topical or edible. Oils tend to offer higher bioavailability, which means a greater absorption rate for more efficacy. Sublingual products also have a full-body effect.
The FDA doesn’t regulate CBD products the same way they do supplements and medications, which means consumers must be careful about the brands they use. To find a quality CBD product, it’s important to check for a few things.
Certificate of analysis
Avoid purchasing CBD products that don’t have a certificate of analysis (COA). A current COA means a product has been tested for safety and purity by a third-party lab. Many brands make these reports available via a QR code on the product packaging or on the website.
When you review the COA, check to see if the amount of CBD and THC that the lab found matches what’s being advertised. Also, look at the contaminant testing results to be sure there aren’t unsafe levels of pesticides, heavy metals, or molds.
FDA warning letters and lawsuits
If a CBD company is making unverified health claims, the FDA will send a warning letter. You can check online to see whether a company has been the recipient of such a letter, as well as whether it’s been involved in any lawsuits. If you see that a company has received one, they may be best to avoid.
Customer feedback
Look for customer feedback on both the company and the product you’re considering to get an idea of efficacy. Keep in mind, though, that some brands may:
only publish positive reviews on their sites
remove reviews that mention specific health conditions in order to comply with FDA rules
Transparency
Always peruse the website of any brand you’re interested in. Some brands will be very up front about where they get their CBD from, as well as how they make their products. These are the brands you’ll want to buy from.
Don’t rely on CBD alone to lower blood pressure. It’s important to talk with a doctor and follow what they prescribe. This may include medication.
There are also home remedies that can help manage the condition. A nutritious diet rich in fruits, vegetables, whole grains, and lean proteins is important, along with managing weight and exercising regularly. Maintaining a low sodium diet is also advised.
Stress management is also key. Things like meditation, massage, yoga, and even deep breathing are worth exploring to reduce stress.
Finally, smoking can also have an effect on blood pressure. Chemicals in tobacco smoke are damaging to tissues in the body and harden the walls of blood vessels. Alcohol can also raise blood pressure, so limiting your intake can help.
Before trying CBD to help manage high blood pressure, it’s important to speak with a doctor. Regular checkups are also a good idea, as symptoms of high blood pressure don’t often begin until the condition is more severe.
If you’re noticing symptoms, or you can’t remember the last time your blood pressure was taken, it’s a good idea to talk with a doctor.
High blood pressure can be dangerous, and it’s a condition that may not be noticeable until it’s serious. Fortunately, there are medications and lifestyle changes that can help, and there is some evidence that CBD is another option worth exploring. Before you do, however, consult a doctor.
Jessica Timmons has been working as a freelance writer since 2007, covering everything from pregnancy and parenting to cannabis, chiropractic, stand-up paddling, fitness, martial arts, home decor, and much more. Her work has appeared in mindbodygreen, Pregnancy & Newborn, Modern Parents Messy Kids, and Coffee + Crumbs. See what she’s up to now at jessicatimmons.com.
Source link
0 notes
Text
Best Weight Loss Tips That Lower Your Diabetes Risk | Eat This Not That
New Post has been published on https://weightlosshtiw.com/best-weight-loss-tips-that-lower-your-diabetes-risk-eat-this-not-that/
Best Weight Loss Tips That Lower Your Diabetes Risk | Eat This Not That

Having diabetes is a lot like being in the middle of the ocean and dying of thirst. You’re surrounded by something your body desperately needs, but ingesting it will kill you. With diabetes, that toxic substance is sugar.
Sugar—derived from the various healthy fruits and vegetables we eat—is what our bodies run on; we can’t function without it. But when you suffer from diabetes, that very same substance can wreak havoc.
Your digestive system turns brunch into glucose—the form of sugar your body uses for energy—and sends it into the bloodstream. Zap! You got energy. But glucose is actually toxic when it lingers in the bloodstream, so when the glucose hits, your pancreas—a large gland located near your stomach—produces insulin, a hormone, and sends that into the bloodstream as well. Insulin is your body’s air traffic controller: It takes command of all your glucose and directs it into your cells, where it can be used for rebuilding muscle, for keeping your heart pumping and your brain thinking, for exercising, or even singing or dancing.
But overeating on a consistent basis—or taking in too many calories too quickly, like when we eat sweets or drink sweetened beverages—turns insulin into the boy who cried wolf. Eventually your body’s insulin receptors—the docking stations where insulin parks glucose—begin to ignore insulin’s instructions. That’s a condition known as insulin resistance. After several years, the pancreas gets fed up with producing all that ineffective insulin and begins to produce less than you need. This is called type 2, or adult-onset, diabetes.
Glucose builds up in the blood, turning toxic and damaging the blood vessels, which is why diabetes can result in blindness, impotence, amputation, and other horrible afflictions. But remember, the body needs that glucose, which is now overflowing from the bloodstream and passing out through the urine. So at the same time too much sugar is killing you, you don’t have enough sugar in your cells to keep your body functioning. You feel fatigue and unusual thirst, and you begin losing weight for no apparent reason. You get sick more often, and injuries are slow to heal because your body is losing its ability to maintain itself.
More than 10% of the American population has diabetes, and more than a third of us have elevated blood sugar levels. Several studies indicate, though, that belly fat is strongly correlated with risk factors such as insulin resistance, which sets the stage for type 2 diabetes. Reducing belly fat via exercise and a healthy diet are two of the best ways to prevent and manage the disease.
To help you out, here are the best weight loss tips that will help lower your diabetes risk. And for more healthy changes, try out any of these 21 Best Healthy Cooking Hacks of All Time.
There’s a reason why omega-3 fatty acids are one of the core nutrients. Considered “essential” because the body does not produce them naturally, omega-3s boast a number of health benefits, including helping to reduce the risk of type 2 diabetes. A study by the University of Eastern Finland found that men with the highest intake of omega-3 fatty acids had a 33% reduced risk for this type of diabetes, compared to men with the lowest intake. Oily fish like wild salmon, rainbow trout, sardines, and mackerel are among the best sources of omega-3s. The American Heart Association recommends eating two 3 1/2-ounce servings of fatty fish per week.
Circuit train your belly away.
Aerobic exercise is known to prevent type 2 diabetes, and combining a heart-pumping cardio session with muscle-strengthening exercises is even better. A study published in the journal PLOS Medicine found that women who engaged in at least 150 minutes per week (about 20 minutes per day) of aerobic activity and at least 60 minutes per week (three 20-minute sessions) of muscle-strengthening activities reduced their risk of diabetes by 33% compared with inactive women.
Get your Greek on.
A Mediterranean diet may help to guard against obesity and consequently reduce your risk of diabetes by up to 21%, according to research presented at the American College of Cardiology’s 63rd Annual Scientific Session. The researchers’ conclusion comes from the analysis of nineteen original research studies that followed more than 162,000 participants for an average of five and a half years. While there is no set Mediterranean diet, it commonly emphasizes fresh fruits and vegetables, beans, nuts, fish, olive oil, and even a regular glass of red wine.
Hit the trail mix.
A study at the University of North Carolina at Chapel Hill found that people who consumed the most magnesium from foods and from vitamin supplements were about half as likely to develop diabetes over the next 20 years as people who took in the least magnesium.
Large clinical trials testing the effects of magnesium on diabetes risk are needed to determine whether a causal relationship truly exists, but researchers have found that as magnesium intake rose, levels of several markers of inflammation decreased, as did resistance to the effects of the key blood-sugar-regulating hormone insulin. Higher blood levels of magnesium also were linked to a lower degree of insulin resistance.
So what should you stock up on? Pumpkin seeds and dark chocolate are two of the best food sources of magnesium.
Eat the whole thing.
Simply choose a whole apple instead of a glass of apple juice, and not only will you dodge a ton of added sugar and additives, but you may also lower your risk for diabetes, according to a study by the Harvard School of Public Health. Researchers found that people who ate at least two servings each week of certain whole fruits—particularly blueberries, grapes, and apples—reduced their risk for type 2 diabetes by as much as 23% in comparison to those who ate less than one serving per month.
Conversely, those who consumed one or more servings of fruit juice each day increased their risk of developing type 2 diabetes by as much as 21%. Swapping three glasses of juice a week with three servings of whole fruit was associated with a 7% risk reduction! The high glycemic index of fruit juice—which passes through the digestive system more rapidly than fiber-rich fruit—may explain the results.
Don’t load up on acid.
A study of more than 60,000 women found that an acid-promoting diet, one that includes more animal products and processed foods than fruits and vegetables, causes a number of metabolic problems including a reduction in insulin sensitivity. According to the study, women with an “acid load” in the top quartile had a 56% increased risk of developing type 2 diabetes compared with the bottom quartile. Foods that promote an alkaline body environment—vegetables, fruits, and tea—counter acidity.
Bad news for people who love going back for seconds at the cookout: Researchers at the University of Singapore found that a small increase in red meat (we’re talking half a serving per day) was associated with a 48% elevated risk for type 2 diabetes over the course of four years. The good news is that you can undo some of the damage by reducing your red meat intake. (And for more help getting you lean for life, try out this 14-day flat belly plan.)
This content was originally published here.
0 notes
Last Seen Blogs

jgxkyfkhgihtghjj
Untitled

kazookazoo
suede supremacist

chocolatesauce-blog-blog
Malachai

papperish
Just It

liebro
To young age