#naloxone enables breathing
Text
People who use drugs deserve love and kindness.
Abstinence is not the only form of recovery. AA/NA doesn’t work for everyone. Sometimes people choose to use instead of meeting other needs, which is valid. Some people use for recreational purposes. Some people use for medicinal purposes. Some people who use have substance abuse disorder. Treatment looks different for everyone. Not everyone needs or wants treatment, for various reasons. The only thing Naloxone enables is breathing. Active use is not shameful. People who use drugs often also deal drugs. People in recovery should not shame active users. Active users deserve love. Active users deserve someone to check in on them, get them safer use supplies, and get them pizza. Active users deserve to be listened to. They deserve better than to have that be the first time anyone ever treated them as human since they began using.
Let’s care for each other.
#chronically couchbound#tw drugs#recovery#narcan#naloxone#harm reduction#harm redux#drug usage#addiction#active users#people in recovery#harm reduction saves lives#naloxone enables breathing#abstinence#alcoholism#substance use#substance addiction#safe use#safe use supplies#harm reduction is mutual aid#mutual aid#community care#narcan saves lives#AA/NA#narcotics anonymous#alcoholics anonymous
3K notes
·
View notes
Text
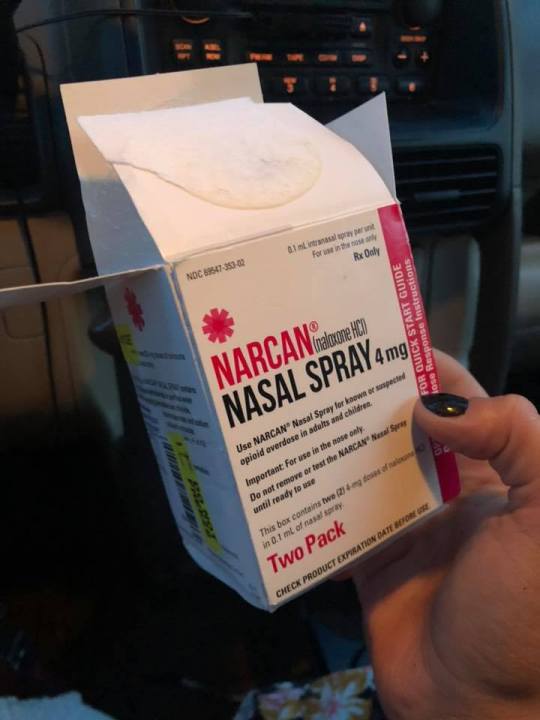
Narcan, a prescription nasal spray that reverses opioid overdoses, can now be sold over the counter, the Food and Drug Administration said on Wednesday, authorizing a move long-sought by public health officials and treatment experts, who hope wider availability of the medicine will reduce the nation’s alarmingly high drug fatality rates.
By late summer, over-the-counter Narcan is expected to be for sale in big-box chains, supermarkets, convenience stores, gas stations and online retailers.
“Today’s approval of O.T.C. naloxone nasal spray will help improve access to naloxone, increase the number of locations where it’s available and help reduce opioid overdose deaths throughout the country,” Dr. Califf said. “We encourage the manufacturer to make accessibility to the product a priority by making it available as soon as possible and at an affordable price.”
The only thing naloxone enables is breathing. Thank you to the drug users, harm reductionists, public health workers, doctors, loved ones of overdose victims, and other advocates who fought for this increased access and will continue to fight until it’s entirely free and accessible for everyone.
3K notes
·
View notes
Text
Heroin to Heroine
The Opened Narcan
As many of you know, I had to open my Narcan yesterday. A young man was found in a bathroom stall, alone and dying. He was completely slumped over, drooling, and he wasn’t breathing. By the grace of something higher (and a lot of stimulation) we brought this young man back from the brink of death. Thankfully, we happened to be in the right place at the right time. And because of that, this person is going to live another day.
The fact of the matter is that people are dropping like flies. This is an all-too-common occurrence in today’s world. We are losing dozens of people on a hourly basis because Fentanyl is wiping them out. This is the number one reason why de-stigmatizing this disease is vital. The people were losing are ALL loved by someone. They are not just “junkies” and “dope fiends”. They are sons. They are daughters. They are mothers and fathers. They are sisters, brothers, friends, spouses. And they are DYING.
Society has developed such a harsh perception of people living with addiction. We’re dealing with people that believe we should “let addicts die” because it was “their choice”. People that argue tooth and nail about the fact that “addiction is a choice” and believe that “if you stick a needle in your arm then you deserve it.” This delusional and dehumanizing perception is incredibly dangerous. It has spurred people forward into judgement and hatred. And ultimately, this stigma is killing people.
There are people out there that believe Narcan enables the addict to continue using more and without consequence. They’ve concluded that an addict doesn’t deserve to be revived based on the idea that “it condones their drug use” and that “they use more knowing they won’t die”. They say it’s a “waste”. These are the same people that believe we are nothing more than our addiction. And they are wrong. It is no one’s job to judge whether or not someone deserves to live. No matter what someone struggles with, their life still has value. The idea that Narcan drives addicts to use more is a myth. Studies have proven that the presence of Naloxone does not increase the quantity of drug use in people living with a substance use disorder.
Narcan is not made as a treatment for addiction. It is not there to take the place of inpatient or outpatient. And it is not a cure-all. But it IS a life saver. An addict cannot recover if they are dead- THAT is why we use it!! That is why it’s so vital to carry it on you! It’s not about whether or not someone is “worthy”. It’s about giving that person the OPPORTUNITY to recover!
People are losing their lives while others turn their heads in ignorance. Think about that young man’s mother. I’m sure she believes her son is worth saving. And that’s because he is! It’s unfortunate that I had to open my Narcan yesterday, but it’s also a blessing...
This young man now has the opportunity to get the help he needs. The help he deserves. An opportunity that would have disappeared had he lost his life.
PEOPLE CANNOT RECOVER IF THEY’RE DEAD!
2 notes
·
View notes
Text
Barotrauma PVP Guide

Welcome to our Barotrauma PVP Guide. Read only first 2 sections for absolute minimum minimum required knowledge. We know that there are people who have a hard time finishing the Barotrauma game. If you are one of those who find it difficult to finish the game, let's take you to our Barotrauma guide. #Barotrauma
Barotrauma PVP Guide
Read only first 2 sections for absolute minimum minimum required knowledge.
Weapons
1. Don't reload with drag and drop. If you have empty smg in slot 1, and full magazine in slot 2, press 2 on keyboard to reload without your firing stopping.
2. Stun lock is strong. Smg, shotgun, dual revolvers, and any more powerful weapons will stun lock a normal person.
3. 3 successful hits with stun rod will stun someone for 10s. 2 successful hits if the stun rod has fulgarium battery. Duel wield to stun even faster. Higher quality stun rods may stun with less hits.
4. thrown grenades can travel from within the hull to outside, but they cannot travel from outside the hull to within.
5. doors and walls shield you from explosions.
6. as of last update, dual revolvers are one of the best weapons. They have high dps, stunlocking, and accurate. Many of the pvp subs around have not adjusted to the dual revolver buff, and leaves revolvers and revolver ammo around. Use them while you can.
Meds
1. Rebind health menu to somewhere convenient (like Q).
2. Have a dedicated slot for each of the main 3 types of meds (opiates, anti-bleeding, anti-bloodloss) and have those slots rebinded to somewhere convenient (like Z,X,C) so they can be spammed.
3. Morphine and saline heal over time (10-20s); Use them right before fighting to save time.
4. Methamphetamine and hyperzine decrease stun per second for 30s. Take multiple to decrease more stun per second. Combat stimulant gives stun resist. Use any of these pre-fight to avoid stun lock.
5. steroids and hyperzine give damage resist. Use them pre-fight.
Barotrauma PVP Equipment
1. oxygenite tanks gives speed boost if breathed.
2. fire extinguishers are faster than scooters but must use hands to carry. Use fire extinguishers for travel and scooters for fights.
3. enemy turrets can be unwired with screwdriver. stun resist meds can help if the turret is manned and shooting at you.
4. enemies can see your headlights on walls. Aim with an aimable item to point headlights away from walls with enemies potentially behind them to not give away your presence.
Poisons
1. stabilozine alleviates every poison except paralysis, but multiple is required to cure advanced stages of poisoning.
2. sufforin, morbusine, cyanide all kill slow. Also, injecting someone with more than 1 dose of any of these will not kill faster.
3. hand injecting 3-4 radiotoxin will kill very fast, syringe gunning 5-7 radiotoxin will kill at about the same speed as the 3-4 hand injection. cure with antirad / multiple stabilozine
4. spam injecting opiates will kill very fast, cure with naloxone / multiple stabilozine
Communication
Mostly reminders to use common sense and contribute to your team's shared store of information. Teammates can't see what you see so you must say what you see.
1. please know your clock directions. Compared to just "top/bottom" + "left/right", the extra definition of the clock system enables the captain to communicate enemy locations beyond periscope viewing range. Gunner would be able to shoot before they see.
2. Call out enemy boarding attempts.
3. Call out enemy sub spottings (use clock system).
3. Call out reactor overloads.
4. Call out injured/unconscious teammates and where if they themselves or you have no meds.
5. If a text chat teammate's text message was obviously not read by all too busy teammates, repeat their text message in voice chat to help disseminate the message.
More Advanced Information
From this point on, it won't be minimum knowledge for pvp. Assume you are at least a knowledgeable wiki reader.
Turret Projectile Spawning Point
The projectiles of turrets spawn at variable distance from the shaft depending on the turret. This affects the level of danger of attempting to unwire the turret while it is manned and shooting.
1. Flak cannon projectiles spawn at the tip of the barrel. Being anywhere closer to the flak cannon base than the tip will render you impossible to be shot by the flak cannon. And so manned and shooting flak cannons are very easy to unwire.
2. Chaingun projectiles spawn a little beyond the tip. Very easy to unwire.
3. Pulse Laser projectiles spawn at the tip, but because the pulse laser model is short and stubby, and the fact that just 1 hit from a laser can kill or stun you for a few seconds, it is easy for the gunner to rotate the laser around to score a shot at an extremity. Because of this, pulse lasers are dangerous to unwire.
4. Coilgun projectiles spawn at the base of the barrel. It is nearly impossible to unwire it while it is manned and not be shot or mildly stunlocked. If you are willing to sacrifice health or meds to unwire the coilgun, using one or multiple meth can help with the stunlock, using one or multiple morphine right before will heal you through the procedure.
5. Railgun projectiles spawn at the base of the barrel. It is very dangerous to try to unwire one while it is manned. If you do choose to attempt to, remember that the default railgun reload time (fire rate) is 5 seconds (1 shot per 5 seconds).
6. Double coilgun projectiles spawn around the middle of the barrel. If you are closer to the double coilgun than that point, the gunner can still rotate the turret to glance one of your extremities. The ammunition is only coilgun, but there is risk of stunlock like the normal coilgun.
Barotrauma PVP Grenade Arcs
Where a grenade explodes will depend on your body's orientation when throwing, and the angle thrown. Each type of grenade will sail through the water in the same arcs, and explodes after 3 full seconds. Grenade projectiles comes from the raised hand holding the grenade.
-- if the origin is at the raised hand holding the grenade, the arcs (in water) will look like this:

Note that it is important to remember that grenade arcs and grenade projectiles come from the raised hand. since the body is about 1.6 meters long, and a body with raised hand is about 2 meters long, you should be conscious of where your body and hand is. It could mean the difference between being in the explosion radius and not:
body oriented vertical with head up and feet down, and grenade is thrown straight up (body actual size):
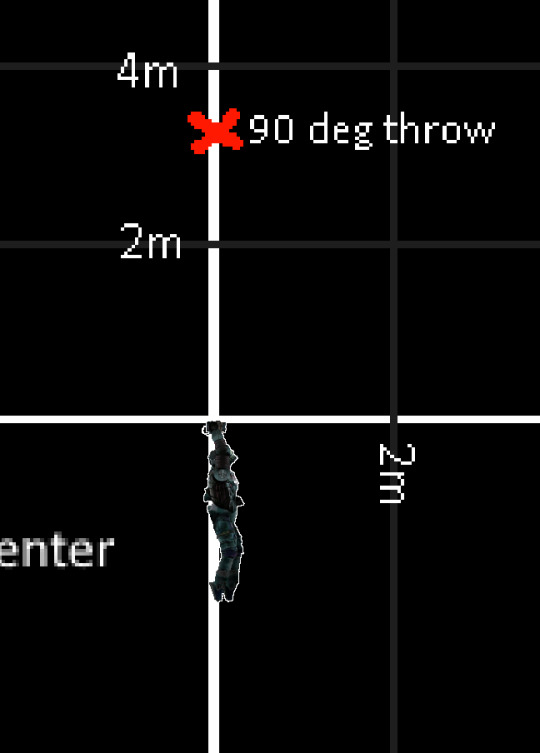
body oriented vertical with head down and feet up, and grenade is thrown straight up (notice you will be much closer to the explosion):
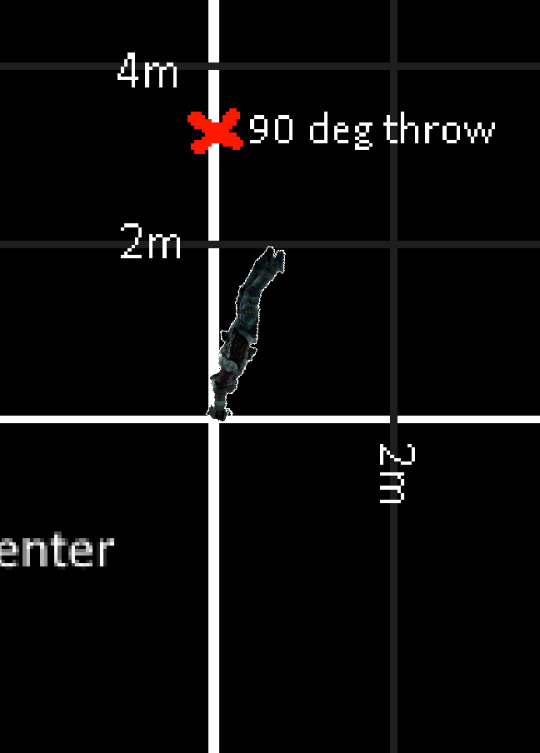
Grenades arcs will never end more than about 3.2 meters above your raised hand (the 90 deg throw), and for this reason, grenades are most useful for someone with the higher ground. Grenade arcs also can be hard to manipulate to end below you in a useful spot. The arcs are most useful when there is open space above to allow for arc movement, and submarine shells around to limit the number of possibilities an enemy has to get to you. This generally constitute fights right along submarine tops. Arcs thrown into unlit water are practically impossible to see for an enemy.
Grenades in general are most useful in two ways. 1. you know where the enemy will be in 3 seconds, and you can get a grenade there (prediction). or 2. you want the enemy to move away from somewhere, usually into another position that is also disadvantageous to him (zoning).
Prediction can be easy when the enemy has few choices as to where they can move. In chases, the enemy wants to get to you by the shortest path. You can put a grenade right in this path. If he is already quite close to you, you can arc a grenade near yourself but even nearer to him. If you arc it so that he is closer to the explosion center, you win the trade.
Volatile Explosives
For background knowledge: IC-4, Compound N, and Volatile Compound N are all volatile explosives, meaning their condition deteriorates from explosions and fires. From explosions especially, most explosions will deteriorate the condition of any volatile explosive in its radius by 50% exactly. Once condition reaches 0%, it will explode.
The profound thing is, even though explosions deal weakened damage through doors and walls against humans and walls, the effect of explosions to deteriorate volatile explosives' condition is not blocked at all by doors or walls. Each explosion will still take off 50% condition regardless.
This fact can be leveraged to create some of the most overpowered and uncounterable traps and attacks in the game:
Not all explosions can deteriorate volatile explosives. Welder bombs will not. Lithium will not. The easiest triggers that will deteriorate VE are flash powder, frag grenades, and incendium grenades. Since each explosion will take off 50% condition from the VE, it will take 2 explosions to detonate a VE. Explosions will deteriorate VE that are in your inventory, but not VE that are in your toolbelt.
Generally, you want to "prime" the VE using 1 explosion on it beforehand, so it will only take 1 more explosion to trigger it. You can keep the VE in a toolbelt until you need it, so you won't explode from stray and untimely explosions.
More Weapons Barotrauma PVP
1. Security guards and medical doctors have 110 default max vitality, while the other classes have 100.
2. Stun darts normally stun 10s after a 10s delay. However, if you are security officer or medical doctor, stun darts will only stun you for 1 second. This is because after the progressive stun from the stun dart reaches 100, it only applies 90.9 incremental stun to a character with 110 vitality, as according to the application equation of the application section of https://barotraumagame.com/wiki/Afflictions. 90.9 incremental stun will apply stuns for only 1 second.
Since stun batons also add incremental stun, it is possible to stun a security officer or medical doctor for full 10s with the 90.9 incremental stun from a stun dart + 1 more baton hit. By the way, this is also why characters with extra large amounts of vitality (from talents or something else) won't even be stunned by stun darts, and why characters with large amounts of vitality take more than 3 hits from normal quality battery cell stun rods to stun, and why those characters won't go down from just 1 dose of chloral hydrate.
3. when you shoot someone, their aim is thrown off for a fraction of a second. The slight stun from a bullet also makes it hard to rotate their body for a very slight time. In the situation of a 1v1 gunfight in the water, if you are using an smg, which mildly stunlocks, and you are shooting from behind them, they will find it very hard to rotate their body and aim at you. This strategy of shooting while swimming behind someone works for most weapons.
4. Run away from enemy shotguns. Shotguns at close range will stunlock hard. At long range they are useless. You can gun them down with almost anything by keeping a safe distance. If an enemy shotgun did catch you in his vicinity, scooter/swim away immediately to a safe distance. The scootering away will streamline your body making fewer of his shotgun pellets hit you. If you stay, you're likely to be stunlocked and killed.
5. piercing coilgun ammo pierces walls.
6. Since most subs can't slow down very fast, it is possible to predict the path of an enemy sub, and drop a depth charge to collide with that path at the right timing, and the momentum of the enemy sub will make it impossible to dodge your depth charge.
Server Style
Pvp experience will depend very much on the server's style, subs, and the items available on those subs.
1. Most common situation: they will give you the smg ammo to stun lock someone for 30 seconds, and the morphine to survive it. Whoever can spam meds the fastest or stun lock the first wins.
2. Subs with fabricators and materials to craft nuclear ammo or exploding ammo. Mostly whoever gets good shot first sweeps enemy team.
3. Subs with railguns and explosives. You need to hide from the railgun. Fabricate explosives if you can manage the crafting time and materials. Mostly whoever gets good shot first sweeps enemy team.
4. Subs with medals. Extremely overpowered. For security officer Enforcer, Beat cop, Stone wall, Implacable very OP. Electrochemist for engineer is good. Clowns tank. For captain, Inspire to battle and commander. Generally Security officer sweeps.
5. Subs with uncommon contraptions. Experience variable. Learn how they work.
6. Servers with balanced amount of medicine, and ammo, no instakill weapons, and no one dominant repeated strategy.
Read the full article
1 note
·
View note
Text
Prescription Painkiller Addiction Signs, Symptoms & Effects
Thomas says acetaminophen is a central acting drug, meaning it works centrally in the brain towards pain pathways. Though the exact mechanism of how acetaminophen works is unclear to researchers, it may work by inhibiting the COX pathway in the central nervous system. Similar to ibuprofen, aspirin is also a NSAID that inhibits the COX enzyme and prevents inflammatory prostaglandins from forming. McKnight, MD, MS, a family medicine physician and clinical assistant professor atTexas A&M College of Medicine.
His articles impress with unique research work as well as field-tested skills. He is a freelance medical writer specializing in creating content to improve public awareness of health topics. We are honored to have Ben writing exclusively for Dualdiagnosis.org.
It harnesses the power of patient stories to sway politicians, state medical boards, judges and government health regulators, emphasizing that it represents grassroots voices. In stories this year, ProPublica has detailed the close entanglements between pharmaceutical companies and groups representing doctors. Reporting showed that the positions of societies representing specialty physicians often reflected the views of their major funders. When made with Pusser's Blue Label (84 proof in the U.S.), the Painkiller weighs in at 10 percent ABV . This is nothing compared to cocktails like the martini , but sweet drinks, hot days, and summer sun can quickly get you drunker than you expect.
Joint N-11 can lead to withdrawal symptoms when stopping, such as anxiety, muscle and bone pain, diarrhea, vomiting or restless sleep. This can occur within as little as seven days of regular use. One held an over-the-counter painkiller, another an HIV drug made by another company, three contained the antipsychotic drug Seroquel, and the remainder contained other Gilead drugs. In a recent survey of physicians, most rated their knowledge about treatment of opioid dependence as only moderate. So if you are concerned that you may have become dependent, ask for a referral to a pain specialist who can help wean you off the drug and help you find other ways to help manage your pain. Behaviors can be as addicting as substances like alcohol and drugs.
During an overdose, the drug overwhelms the parts of your brain that control your respiratory and circulatory functions. Neurological signals are suppressed, leading to slowed breathing and heart rate. Sometimes, people who overdose may experience abnormal heart rhythms; sometimes they will enter full cardiac arrest.
When people refer to painkillers, they are speaking about opioid or opiate pain medications. These substances derive from opioid alkaloids found in the opium poppy, and their mechanism of action is similar to that of heroin. If you suspect someone is experiencing a painkiller overdose, it’s crucial to call 911 immediately. Timely medical attention can mean the difference between life and death. Emergency first responders are equipped with naloxone, a drug that can reverse the effects of an opioid overdose and potentially save lives. Administered via nasal spray or injectable syringe, naloxone works by blocking the opioid receptors in the brain, enabling lung and heart function to resume almost instantaneously.
Is used in combination with other chemicals and is available in prescription pain medications as tablets, capsules and syrups. Trade names include Anexsia, Dicodid, Hycodan, Hycomine, Lorcet, Lortab, Norco, Tussionex and Vicodin. Sales and production of this drug have increased significantly in recent years, as has its illicit use. There are different medications that can ease short-term or chronic pain. These drugs are also known as narcotic pain relievers and include morphine and codeine, as well as several synthetic modifications of these drugs. Some patients with chronic pain will simply not find relief with non-opioid medications or treatments like physical therapy.
#Pain Management#Back Pain Management#Chronic Pain#Chronic Pain Management#Pain Management Specialist#Interventional Pain Management#Labor Pain Management#Pain Management Near Me#Pain Management Clinic#Pain and Pain Management#Pain Management Doctors#Pain Treatment#Pain Management Specialists#Comprehensive Pain Management#Pain Management Doctors Near Me#Pain Management Without Opioids#Managing Pain
1 note
·
View note
Photo

The only thing naloxone enables is breathing, Quote medical T-Shirt
Link shirt: https://www.amazon.com/dp/B09QJLTMB3
3 notes
·
View notes
Text
Suboxone Rant
Suboxone is an opioid partial agonist = does the same thing opiates do while containing naloxone to keep patients from overdosing. Calling yourself clean or sober while taking Suboxone is inaccurate. Your addiction is managed, and by no means over. Fight me.
Normally, I'm fine with being supportive and having a "whatever works for you" mentality towards personal progress in fighting addiction, but I was addicted to Suboxone (amongst many other things.)
Stepping stones are important, but don't mistake a step in your journey for a life long answer, especially when that answer involves pharmaceutical management of addiction via taking daily narcotics. Suboxone was meant, as methadone was initially too, to be a short-term step down, only to be prescribed to those who are tapering down with a finite and time sensitive goal of getting off all opiate agonist medications.
This harm reduction model doctors have adopted, seemingly with open arms, over the past 10-15 years enables addicts to stay "acceptably addicted" under the care of providers who get a new patient pool: addicts, the most loyal of patients, people who will pay, do and/or say anything to keep getting prescribed addictive meds legally. The current substance abuse treatment model reinforces the concept that it's socially and morally ok for addicted people to be given addictive medications simply because those medications, which have the same effect as the offending narcotics and are also addictive, are labelled as recovery-assistive.
Many patients taking these medications even believe themselves to be "cured" and cite miraculous changes in their lives due to medication management (most commonly on Suboxone in particular.) I'm not saying personal progress isn't likely to be more attainable for patients while under medication maintenance, or that life victories while on these meds are anything less than praiseworthy, but I am saying that the goal should be freedom from the addictive cycle, not just legal and managable substitution of one addictive substance for another.
Regardless of whether anyone else cares to notice or say it, there's a problem when meds are administered by doctors who do not understand or do not care about the addictive mentality and physical addiction they keep going strong in their patients through long-term use of 'step down' agents such as Suboxone or methadone.
There is no magic pill, and many of the patients on these opioid replacement meds long term will never know full freedom from the addictive cycle. Why do I say that? Consider the following.
If you can't go without your narcotic medication for a few days, then you know what dependence and withdrawal are, and you may be addicted. If a doctor prescribes a med that does the same thing as the offending substance and says it's ok to take it indefinitely, are you not just dependent on a prescribed version of the same thing now? Paying a doctor to keep you in an ongoing cycle of dependence and withdrawal. You are still addicted.
There is full and complete freedom from that cycle, but it's so much easier to stay addicted to a legal prescription, and more profitable for your doctor too. I speak from my own experience when I say that most people who are truly addicted to substances (addicts) will choose never to break the addictive cycle because it's the only way they know how to live, high to high, pill to pill, feeling like they have an incurable plague, like a hole they have to fill day after day, nothing but the comfort that the euphoria brought on by use of addictive substances suffices to fill the hole. They simply do not know any other way to live, to be ok, to feel good.
So, of course replacement therapy is a highly popular alternative to sobriety from all addictive substances, and it's preferred by opiate addicts precisely because it's not alternative to the addictive cycle, it switches the addiction to something more acceptable and less risky to take. It demands no changes, it just suddenly becomes ok to be an addict once addicts admit they have a problem and start on medication management. Nothing changes except where and how they get the high, and how others treat them. When everyone around them, including society and their doctor, says it's alright, even praiseworthy, to switch addictions to a legally prescribed replacement med, why choose freedom from all substances?
Breaking the addictive cycle hurts, why else would anyone keep using addictive substances despite knowledge of their dangers, even up to and including the point of actual death. Addiction is not a choice, it is as natural and essential a process to the addict as breathing is for people without the addictive propensity. Until you take away the addictive substance entirely, I would argue, there is no sufficient chance for addicts to step back and see that a happy, meaningful, and productive life is possible without having to take any addictive substances. I know from my own experience that there's hope for a whole new kind of freedom in sobriety, but most real addicts, given the choice the harm reduction model would have us present them, will choose rather to use replacement narcotics until death than to break free of the addictive cycle altogether.
Medication management and the harm reduction model are depriving some addicts of potential lifetimes of freedom from the addictive cycle. Sometimes the truth hurts and we need a push to move forward, this goes for all humans. Especially when moving forward means changing an entire mentality and physical dependence for the chance at a better future for ourselves, as addicts, and everyone around us.
I am not without compassion, PLEASE take sobriety in steps if you need to, but don't pretend to have the answer when nothing about your relationship with addictive substances has changed. The harm reduction model would be as aptly named the freedom reduction model, from my point of view.
I'm passionate about this shit and this is a rough draft, so sue me.
0 notes
Text
Prescription Drug Abuse in Delray Beach Florida - Transformations Treatment Center
What Are Signs Of Drug Abuse
Table of Contents How To Prevent Drug Abuse In A Community Which Of The Following Is Drug Abuse? Bill Wants To Know How He Can Prevent Drug Abuse By His Adolescent Son. You Would Suggest That Bill How To Get Help For Drug Abuse What Is The Difference Between Drug Abuse And Drug Addiction How To Prevent Drug Abuse What Does Drug Abuse Mean What Is The Difference Between Drug Use And Drug Abuse
( like with some ADHD drugs) may cause heart failure or seizures. These dangers are increased when stimulants are blended with other medicines even OTC ones like cold medicines. Taking too much of a stimulant can result in a dangerously high body temperature or an irregular heartbeat. High dosages over a brief period may make someone aggressive or paranoid.
1
The dangers of prescription drug abuse can be made even worse if individuals take drugs in a manner they weren't intended to be used. Ritalin may appear safe due to the fact that it's prescribed even for youngsters with ADHD. But when an individual takes it either unnecessarily or in such a way it wasn't planned (such as snorting or injection), Ritalin toxicity can be major.
2
Individuals who abuse medications can become addicted as quickly as if they were taking street drugs. That's one reason most physicians won't restore a prescription unless they see the client they desire to analyze the client to make sure he or she isn't getting addicted. If a physician recommends a pain medication, stimulant, or CNS depressant, follow the instructions exactly.
3
How Does Drug Abuse Start
Your physician will want you to check out typically so she or he can see how well the medication is working for you and change the dosage or change the medication as required. Take down the results the drug has on your body and emotions, particularly in the first few days as your body gets used to it.
4

Keep any info your pharmacist offers you about any drugs or activities you must steer clear of while taking your prescription. Never increase or decrease the dosage of your medicine without consulting your physician's workplace initially. Lastly, never use another person's prescription. And do not permit anybody to utilize yours.
5
And if you're found providing medicine to somebody else, it's thought about a criminal activity and you might find yourself in court. Date reviewed: October 2018.
6
Why Is Drug Abuse A Problem
Prescription substance abuse is when you take a medication for a reason besides why the doctor recommended it. Experts approximate that more than 18 million individuals ages 12 and older have actually utilized prescription drugs for nonmedical reasons in the previous year. That's more than 6% of the U.S. population.
7
Many people begin by picking to take these medications. But gradually, the modifications in your brain impact your self-control and your ability to make great decisions. At the exact same time, you have intense prompts to take more drugs. The National Institute on Substance abuse states three classes of prescription drugs are often mistreated: Opioids.
8

This is partly due to the fact that of the increasing age of the U.S. population and due to the fact that more individuals are living with long-term pain. These medications handle discomfort well and can help boost your lifestyle when you follow your doctor's directions on taking them. It's possible but not common to end up being addicted to or based on opioids when you use them for a short time or under a doctor's close watch.
9
How To Prevent Drug Abuse Essay
Opioid overdose can also be lethal. If you take them with medications that work on your central nerve system-- including alcohol, barbiturates, or benzodiazepines such as alprazolam (Xanax), clonazepam (Klonopin), or diazepam (Valium)-- you have a greater possibility of breathing problems or death. Opioids can trigger a moderate cheerful sensation.
10
Injecting drugs raises your possibilities of getting illness like HIV and hepatitis C (what is the national institute on drug abuse). Central anxious system (CNS) depressants. Countless individuals in the U.S. use benzodiazepines (Ativan, Valium, Xanax) to treat anxiety and sleep disorders, consisting of insomnia. They affect a chemical in your brain called GABA (gamma-aminobutyric acid). GABA reduces brain activity, making you sleepy or calm.
11
Physicians use them for anesthesia and recommend them to deal with seizures. Taking CNS depressants for a couple of days or weeks may help you feel calm and drowsy. But after a while, you might need bigger doses to get the exact same feeling. Utilizing them with alcohol can trigger slow heartbeat, slow breathing, and death.
12
How To Do An Intervention For Drug Abuse
Stimulants. These drugs offer your body a jump-start, with a substantial boost in alertness, energy, and attention. They raise your heart rate, blood sugar level, and blood pressure. They likewise narrow your capillary and open your air passages. Physicians started utilizing stimulants to treat asthma and obesity. Today, they prescribe them for conditions such as ADHD, ADD, depression, and narcolepsy.
13
Stimulant abuse-- for instance, by taking them in greater dosages or by squashing tablets and snorting them-- can result in dependency. High doses can raise your body temperature. Misusing stimulants or utilizing them together with decongestants may trigger unequal heartbeat. Research shows that some features of you may make you most likely to abuse prescription drugs.
14
Someone who abuses opioids might have: Lightheadedness Slow or shallow breathing Distressed stomach, throwing up, or constipation Slurred speech Poor coordination Mood swings Depression or stress and anxiety Abuse of CNS depressants can trigger: Mood modifications Difficulty walking Difficulty concentrating Poor judgment Slow reflexes Slurred speech Memory issues Sluggish breathing Symptoms of stimulant abuse include: Weight loss and absence of hunger Lightheadedness Headache Insomnia Anxiousness Hypertension Uneven heart rate Paranoia Treatment for opioid dependency includes medications that can help people get control without a high possibility of dependency.
15
Why Is Drug Abuse A Social Problem
Physicians typically use it in addition to the drug naloxone (a combination that can be called Bunavail, Suboxone, or Zubsolv) to prevent relapse. If you've been taking buprenorphine in tablet kind and your body has actually gotten rid of all of the drug you were abusing, you might have another form of buprenorphine implanted under your skin.
16
It provides a continuous dosage of buprenorphine for 6 months. Buprenorphine likewise comes as a month-to-month shot called Sublocade. Other drug treatments for opiate withdrawal consist of methadone and the high blood pressure medication clonidine. Naltrexone obstructs the results of opiates and can avoid a regression. It can be taken orally (Revia) or as a month-to-month injection (Vivitrol).
17
It comes in a shot (Evzio) and a nasal spray (Narcan). Experts think that "medication-assisted treatment" with methadone, naltrexone, or suboxone and cognitive behavior modification is the very best treatment for the majority of patients who have an opioid addiction. Therapy is the most typical treatment for addiction to CNS depressants or stimulants.
18
Bill Wants To Know How He Can Prevent Drug Abuse By His Adolescent Son. You Would Suggest That Bill
The FDA uses these standards for safe prescription medication usage: Always follow the directions thoroughly. Do not raise or lower dosages without talking with your physician initially. Never stop taking a medication on your own. Do not crush or break pills, specifically if they're time-released. Make sure you know how a drug will affect your driving and other daily jobs.
19
Talk truthfully with your doctor about any personal or household history of substance abuse. Never ever enable other individuals to use your prescription medications, and do not take theirs. According to the National Institute on Drug Abuse, you should never use opioids with CNS depressants, including: Alcohol Antihistamines Barbiturates Benzodiazepines Sleep medications General anesthetics Do not use CNS depressants with other things that dull your central anxious system, such as: Alcohol Prescription opioid discomfort medications Some over the counter cold and allergy medications Be cautious utilizing stimulants in addition to other substances that trigger your nerve system, including: Antidepressants, as monitored by a doctor Non-prescription decongestant medications Some asthma medications Prescription drug abuse can have unsafe or deadly effects, particularly if you take them together with the drugs listed above: Opioids may trigger vomiting, breathing issues, a coma, or death.
20

If you stop or slow your dosage too rapidly, you could have seizures - what is drug abuse definition. Stimulant abuse may lead to high body temperature, unequal heart beat, hostility, paranoia, heart failure, or seizures. Abuse makes you more most likely to become based on or addicted to a drug. You also have a higher opportunity of devoting a criminal activity, being the victim of a criminal activity, or having a mishap.
21
What Are The Causes Of Drug Abuse
Physicians report writing more prescriptions than ever previously. Also, it's simple to find online pharmacies offering these drugs. Teens may take medication from their parents' medication cabinets for themselves or their buddies to use. A lot of young people have no idea what medications they're taking and which ones might cause serious issues-- even death-- if used with other drugs or alcohol.
22
If you think a relative or friend is abusing prescription drugs, talk with your doctor. They can refer you to drug treatment programs that may assist. You can likewise call the Drug abuse and Mental Health Solutions Administration crisis line at 1-800-662-HELP (4357 ). Speak with the person about your concerns so they understand that you know the problem.
Transformations Treatment Center
14000 S Military Trail, Delray Beach, FL 33484
FV9H+MC Delray Beach, Florida
https://www.transformationstreatment.center
Prescription Drug Abuse Rehab in Delray Beach, FL
from
https://transformationstreatment1.blogspot.com/2020/08/prescription-drug-abuse-in-delray-beach.html
from Transformations Treatment Center - Blog https://transformationstreatment.weebly.com/blog/prescription-drug-abuse-in-delray-beach-florida-transformations-treatment-center
0 notes
Note
hi I had a question about your cannabis post
i don’t know much about cannabis so sorry if I misunderstand smth
but I don’t understand what “safe” drug use implies,, how can drugs be safe? what’s safe drug use??
i probably have a very narrow view on this topic, so id like to know more
on a different note id like to thank you for your content, I feel that ive learned a lot from this account :)) thanks!!!
(feel free to ignore this)
It’s important to first recognize that more things are drugs than we normally consider: alcohol, tobacco, nicotine, caffeine, cannabis, are all drugs just as much as opiates, benzos, etc. Any medication is a drug.
Any drugs have the ability to be used properly and safely as well as the potential to be used negatively or harmfully. Drugs are morally neutral. Even addiction is morally neutral.
Alcohol can be used to cut loose with friends on the weekend, but it can also be used to cause poisoning. Tobacco can be used to calm down after an argument, but it can also cause cancer. Opiates can be used to manage severe pain, and can also cause overdose.
People have always used drugs historically, and in order to survive, people often need them. Using substances can also not just be medically or recreational, there are spiritual and cultural reasons as well. Some people need substances to manage their emotional or mental needs (especially without supports otherwise).
Any drug can be safe. It’s all in how it’s used, as well as within context.
Safe use looks different for everyone, but personally, I try to encourage methods that are harm reduction focused.
Harm reduction can look like:
• Safe supply of substances to ensure that people are getting unlaced stuff.
• Education so people know how to avoid accidental consequences of their use.
• Access to unused syringes or works to prevent blood borne infections.
• Having a designated driver or trip sitter.
• Sitting with someone while they use in case they have negative effects.
• Access to naloxone/Narcan to reverse opioid overdoses.
• Starting with a lower dose and going slow with use to ensure you’re getting the intended effects.
And harm reduction is so much more than just about substances, it’s things like seatbelts in cars and condoms and STI testing. It’s the lesser of two evils and a primary focus of harm reduction is that it keeps people alive above all else.
Some people like to say “harm reduction keeps people alive long enough to get sober” but I personally feel like sobriety isn’t always the solution for everyone, nor is it accessible to everyone.
But yeah, safe use exists, and most drugs ARE used safely every day. That’s what a pharmacist’s whole job is for.
•
I appreciate this ask, I’m always happy to talk about harm reduction. I co-founded a local harm reduction organization and have done a lot of advocacy around this— everything from reversing ODs, speaking on panels, testifying for bills with the ACLU, training communities on how to administer Naloxone, distributing safe use supplies, etc. I have a lot of personal experience with addiction and feel very passionately about this. I was tired of my friends dying and I just want to make the world a safer place.
#chronically couchbound#asks#asks answered#answered asks#harm reduction is mutual aid#harm reduction saves lives#harm redux#harm reduction#safe use#safer use supplies#safer use#naloxone enables breathing#naloxone saves lives#narcan
50 notes
·
View notes
Text
All the companies from Y Combinator’s W20 Demo Day, Part IV: Healthcare, Biotech, Fintech and Nonprofits
New Post has been published on https://magzoso.com/tech/all-the-companies-from-y-combinators-w20-demo-day-part-iv-healthcare-biotech-fintech-and-nonprofits/
All the companies from Y Combinator’s W20 Demo Day, Part IV: Healthcare, Biotech, Fintech and Nonprofits
Y Combinator’s Demo Day was a bit different this time around.
As concerns grew over the spread of COVID-19, Y Combinator shifted the event format away from the two-day gathering in San Francisco we’ve gotten used to, instead opting to have its entire class debut to invited investors and media via YC’s Demo Day website.
In a bit of a surprise twist, YC also moved Demo Day forward one week citing accelerated pacing from investors. Alas, this meant switching up its plan for each company to have a recorded pitch on the Demo Day website; instead, each company pitched via slides, a few paragraphs outlining what they’re doing and the traction they’re seeing, and team bios. It’s unclear so far how this new format — in combination with the rapidly evolving investment climate — will impact this class.
As we do with each class, we’ve collected our notes on each company based on information gathered from their pitches, websites and, in some cases, our earlier coverage of them.
To make things a bit easier to read, we’ve split things up by category rather than have it be one huge wall of text. These are the healthcare, biotech, fintech and nonprofit companies. You can find the other categories (such as B2B, consumer and robotics) here.
Healthcare and Biotech
Simple Stripes: Aims to make glucose testing cheaper and more accessible by making strips that can be read by any smartphone camera, rather than requiring a dedicated glucose meter. The company says it expects to submit its strips for FDA approval in June.
nplex biosciences: A faster, cheaper way to do the protein panels required in the development of new medications. The company says it has over $4 million in letters-of-intent in the works, including one from a major pharma company.
Healthlane: An app meant to help users in Africa communicate with their doctors, make appointments and track lab results. The company says it has already reached profitability, with a retention rate of 98%.
Breathe Well-being: A 16-week program meant to help users in India with chronic conditions (such as diabetes) in their efforts to lose weight. The company offers a one-on-one diabetes coach who helps the user with tracking things like weight/meals/activity and trains them in cognitive behavioral therapy techniques meant to reduce stress. Currently seeing an $11.2K MRR.
Dropprint Genomics: “Single cell genomics” software meant to reduce the time/financial cost of analyzing individual cell activity to enable better drug discovery. They’ve signed over $1 million in LOIs in two months.
Newman’s: A digital health clinic for men in Indonesia. They’re focusing on problems that are often seen as either embarrassing (hair loss, erectile dysfunction) or are often abandoned (quitting smoking) by making doctor visits easier, cheaper and more private by way of remote consultation. Find our previous coverage of Newman’s here.
Loop Health: Loop Health says that most health insurance in India covers “only hospital stays, not doctor visits.” They’re looking to improve this by offering unlimited access to their designated Loop Health clinics, along with app-based telemedicine.
Synapsica Healthcare: An “AI reporting assistant.” Currently focusing on spinal MRIs, the company says it saves radiologists 80% of their reporting time by automatically annotating measurements and characterizing disc degeneration. The company says it’s currently in a $100K pilot program with a radiology practice tapped by 250 chiropractic clinics.
Volumetric: Volumetric makes 3D bioprinters that create vascularized human tissue. Founded by two PhDs, Volumetric sells its photoactive tissue to pharmaceutical companies and scientists. It’s using the proceeds to move toward building bioprinters and bioinks that can generate functional tissue and even organs. Find our previous coverage of Volumetric here.
Ophelia: Ophelia replaces rehab with telemedicine for America’s 3 million opioid addicts. It lets patients do teleconferenced doctor visits, get prescribed and delivered medications like Buprenorphine and Naloxone, and access therapy without the stigma. The founder started the company after a longtime girlfriend died from opioid addiction, and Ophelia has now treated 40 patients.
Lilia: Claiming that “in the future, women will freeze their eggs upon graduation,” Lilia is an egg-freezing concierge service. The startup charges $500 for concierge, and gets another $500 when somebody is placed in a clinic. Lilia says its total addressable market is $33 billion.
Equator Therapeutics: Equator Therapeutics is developing a drug to help users burn calories without exercise. Founded by a duo of PhDs and a data scientist who worked at a company developing an anti-aging drug, Equator Therapeutics is targeting people dealing with obesity and type 2 diabetes.
Altay Therapeutics: Located inside the Bayer Collaborator in San Francisco, Altay Therapeutics has developed small molecule therapies that block disease-causing DNA-binding proteins (or transcriptional regulators). The company’s initial therapies are focused on arthritis, fibrosis, ulcerative colitis and liver cancer.
Tambua Health: Tambua Health uses an “acoustic” stethoscope and proprietary software to provide advanced imaging for lung imaging without the radiation of an x-ray.
Abalone Bio: Founded by serial life sciences entrepreneurs, Abalone Bio is using libraries of yeast cells expressing billions of antibody variants to grow specific antibodies that can activate or inhibit a drug target. Using gene sequencing, machine learning and synthetic biology, the company makes recombinant protein versions of its antibodies and confirms their efficacy in human cell assays. The company’s initial targets are drugs for pain, inflammatory diseases, rare cancer and rare kidney disease.
Felix Biotechnology: Founded by the famous Yale University researcher Paul Turner, Felix Biotechnologies is developing treatments to address antibiotic-resistant strains of bacteria and fungi. These pathogens cause more than 2.8 million infections and 35,000 deaths in the United States alone each year, according to the company. On average, someone in the U.S. dies from an antibiotic-resistant infection every 15 minutes. Researchers have warned that more people will die from antibiotic resistance than from cancer by the year 2050.
Genecis Bioindustries: Genecis Bioindustries is turning food waste into compostable plastics. Find our previous coverage on Genecis here.
Candid Health: Candid Health has developed automated billing software for the healthcare industry that follows up with insurance companies and automatically appeals denied claims. It takes a 5% cut of each payment.
Ochre Bio: Ochre says that most donated livers are discarded — despite there being a shortage — due to them containing too much fat for a successful transplant. They’re aiming to “rejuvenate livers outside the body” by finding ways to treat them prior to transplant.
Fintech
Facio: Brazil has a banking problem. An oligarchy of five banks manage the Brazilian market, and they’re slow, have terrible customer service, high APR and don’t serve SMBs. Facio wants to keep workers from falling victim to predatory debt and instead gain financial freedom with a low-priced payroll loan to employees. It integrates with the employer, deducting loans right from their payroll.
delt.ai: Delt.ai is a digital bank that handles payments, invoicing and corporate cards for poorly served SMEs and freelancers in Mexico. The startup is targeting the $50 billion+ market of business deposits in Mexico. Think of Delt.ai is a Brex or a Mercury, but focused on Latin America.
Nexu: Like many other personal financing operations in Latin America, car financing is an expensive, low-tech, arduous process. Nexu, a financing platform for Latin American car dealerships, uses dynamic credit scoring to give car buyers an approval with a turnaround of a few seconds. The founding team met as Wharton MBA candidates.
Fondeadora: Fondeadora is joining Mexico’s saturated fintech scene, with its alternative neobanking debit card. The company offers a fully mobile digital savings account run within its app. Fondeadora says it has 65,000 users and $6.5 million monthly transactions. Albo, another Mexico-focused debit card, currently owns the market share with 200,000 monthly active customers who are spending and making transactions in its platform and $26 million in capital raised. But the banking problem in Mexico is big enough that multiple startups can thrive. Out of the 130 million population of Mexico, 45% are underbanked, meaning they lack deep financial products designed to help them compound wealth through lending and savings features.
Jenfi: Loans money to small businesses in Asia — typically about $10,000 to $100,000 — based on the business’ revenue. We wrote about Jenfi previously here.
yBANQ: A collections and reconciliation system for large B2B companies in India. The company says it has found 18 customers since launching in late January, reaching a GMV of around $18K.
ZeFi: A savings account that converts USD deposits to/from “stablecoin” cryptocurrencies behind the scenes, with ZeFi lending these funds out to borrowers to gain interest.
Grain: Grain hooks your existing debit card to a “responsible” amount of credit (currently capped at $500, and based on your income/cash low), hopefully helping those with minimal/bad credit build up their credit report over time. In the three months since launch, the company says it has signed up 1,000 customers, and expects to make around $80 per customer per year.
CrowdForce: Lets local merchants in Africa act as bank branches, serving as an intermediary on transactions when a bank is too far away. The company says it made $70K in net revenue last month, making an average of $20 per year per customer.
Stark Bank: A banking API to handle B2B transactions for tech companies in Brazil. A little over a year after launch, the company says it’s seeing $12 million in monthly gross volume.
Bamboo: An online brokerage for high-wealth individuals in Africa to buy securities from around the world. The company says it already has over 2,100 investors who have traded over $1.6 million on the platform since launching roughly five months ago, currently accounting for over $10,000 in monthly revenue.
Swipe: Pitching itself as “Brex for Africa,” Swipe gives African SMBs a credit card to help cover payroll and expenses. They onboard businesses by providing them with free expensing/billing tools, then offer credit accordingly. The company says it’s currently working with 30 companies, with $200K in credit deployed.
goDutch: A payments card for splitting costs amongst groups that often share bills, such as roommates. Focusing on India. Charges are put onto one card and deducted from each group member’s account automatically.
Paymobil: Uses stablecoin cryptocurrencies to transfer money across the globe through a Venmo-style app. The founder, Daniel Nordh, notes that he previously led consumer design at Coinbase.
Karat: Karat offers banking, loans and credit cards to influencers. By using data on their popularity to manage risk, Karat has achieved 40% APR on its loans with an average repayment time of 45 days. Thanks to its founders’ experience building influencer tools at Instagram and structuring debt at Goldman Sachs, it’s already signing up stars with over 10 million followers.
Homestead: Homestead helps home owners convert their garages into rental properties at no upfront cost. Homestead pays for all the construction, tenant search and management, and then splits the rent income with the home owner. A new California law allows the state’s 8 million garages to be rented out as living spaces, creating an enormous market opportunity. Homestead’s founders met at MIT’s graduate school of architecture and city planning, and the startup has already done $1 million in sales.
Benepass: Benepass offers a benefits card for startups and small businesses. Using the Benepass debit card, employees can pay for tax-advantaged benefits and wellness perks like flexible spending accounts, childcare, commuting, fitness and education while an app tracks their buying. Free for employers, Benepass has a 6% take rate but can save thousands on income and payroll taxes. With startups desperate to compete with tech giants for top talent, Benepass could ensure employees feel supported.
GAS POS: U.S. gas station owners are racing to upgrade outside pumps with EMV technology, a global standard for credit cards equipped with computer chips. GAS POS was founded to deliver a modern point-of-sale system that will help North America’s 180,000 gas stations comply with EMV and make transactions more secure. The company has several sources of revenue, a 3% fee on processed payments, SaaS free for equipment and an offer to customers to provide next-day funding.
YearEnd: YearEnd is building tax software for the paper rich, helping startup employees file their taxes while optimizing for their equity. The startup charges $330 per year for individual users and is hoping to sell to businesses that can add YearEnd as an employee benefit.
GIGI Benefits: India’s GIGI Benefits is looking to be the benefits provider for the nation’s gig economy workers. The business takes a page from companies like last year’s hottest Y Combinator startup, Catch, or the venture-backed Trupo, to provide things like health insurance and retirement investment accounts to gig economy workers.
Easyplan: Easyplan is the Qapital or Digit for India, allowing users to seamlessly save money for certain specific goals.
Haven: Haven is a next-gen platform for servicing home mortgages, offering more modern customer interfaces, better payment modeling for lenders and more.
WorkPay: WorkPay describes itself as “Gusto for Africa” — next-gen payroll and related services targeting small and medium businesses in the region.
Spenny: Spenny is a savings tool for Indian consumers that lets customers start banking money away by rounding up their purchases.
Kosh: Kosh is an algorithmically enhanced savings and investment platform for India, allowing those with good credit to effectively vouch for friends with limited credit to help them borrow.
Nonprofit
Potential: Potential is a nonprofit that wants to connect the formerly incarcerated to jobs and resources. The company works with detention centers and employment organizations to make a more friendly hiring environment.
0 notes
Text
How Harm Reductionists Keep the Faith
It’s a bitterly cold afternoon in early March as Karen Lowe and I pick our way down the broken sidewalks of a semi-abandoned neighborhood in Statesville, North Carolina. All around us, squatter houses stretch for blocks. Every window is busted or boarded up. Thin, dirty mattresses lie on sunken porches and feral dogs scrounge in the trash-strewn yards for scraps. Some residents are huddled inside for warmth, though in most of these homes, there is no electricity.The neighborhood is a depressing sight, but it’s hard to feel blue when you’re on outreach with Karen Lowe. Co-founder of the Olive Branch Ministry, a faith-based non-profit that brings harm reduction services to the seven foothill counties of North Carolina, Karen is the embodiment of love.Harm Reduction in the Deep SouthAs I burrow into my thin jacket, Karen strolls down the middle of the street extending warm greetings to the few brave souls who venture outside. Though the pockets of her cargo pants are bursting with clean syringes, naloxone, and other supplies to prevent death and disease among people who use drugs, she doesn’t flaunt her wares.“I just want people to see me,” she explains. “It’s about building trust. They know why I’m here. If they need something, they’ll come to me.”As we walk, the 52-year-old fills me in on the colorful cast of characters who call this neighborhood home, including a man who claims he hasn’t bathed in a year and an old woman who pees on the sidewalk. Karen describes everyone with great affection.“There is a certain kind of love that goes with being an untouchable,” she says. “And [the people of this community] have it. But it’s not allowed to grow.”There certainly isn’t much growing in this neighborhood. Judging by the columned porches on every house and what looks like abandoned flower gardens, this was probably once a desirable place to live. But shifting economic winds have devastated entire cities in the South and Statesville is no exception. A small inland city—population 26,000—Statesville boasts neither North Carolina’s green mountain range nor its sparkling coastline. It’s stranded in the flatland area of the state, mostly buried under strip malls and fast food restaurants. But despite so few bragging rights, Statesville embraces its Southern pride, describing itself on its website as “a city where fish is fried (as our Lord intended they be) and a bottle of Kraft French Dressing is good enough for anybody --- so get over yourself.” Also true to its Southern roots, while Statesville has recently invested in a splash park and a $330,000 home for veterans (more than double the average price of a house in the area), the city has allowed this particular neighborhood, in which residents are almost all black, to fall into ruin. The only people who venture into this place are the churches who occasionally come evangelizing and of course, the police, who make neighborhoods like this one their second home.But Karen brings cheer to this desolate area. Twelve years ago, she was homeless herself, struggling with mental illness and depression, and searching for both a literal and metaphorical place to set down roots. She found a surrogate family and a calling in a faith-based organization in Greensboro that provides services to people living with HIV. The community welcomed Karen with open arms and she became a regular at meetings, outreach events, and retreats, which she describes as “mad love and dealing with yourself, everybody crying and snotting.”Not Your Typical Faith-Based Outreach OrganizationKaren says she knew then that her life was about to change in remarkable ways. And was it ever. A couple years into her involvement with the faith community she met the love of her life, Michelle Mathis, a woman who shared her passion for helping people in need. Though they have the same heart for harm reduction, the pair is about as opposite as two people can be. Michelle exudes elegance with a powdered face and coiffed hair that somehow survive even in the god-awfullest North Carolina humidity. Her partner is more salt-of-the-earth.“I did the make-up and heels thing when I was young…somebody should have stopped me,” Karen laughs.The yin to the other’s yang, the two married in a private ceremony in 2009 where they exchanged olive branches instead of rings, thus creating what would become their joint life’s work, The Olive Branch Ministry.Olive Branch is not your typical faith-based outreach organization—and not just because its founders are an interracial queer couple spreading the word of Jesus in the Deep South. True to the tenets of harm reduction, whose guiding philosophy is “meet people where they are at,” Karen and Michelle serve without pretense or expectation.“We say faith is why we do [this work], but it’s not what we do,” Michelle explains to me over the phone. “If someone asks us to pray for them, we will pray for people…We take the message of harm reduction to faith communities…but we don’t evangelize.”During afternoon outreach with Karen, she utters not a whisper about faith. And yet, if God’s love for others were perfume, you’d smell her coming from blocks away. Helping others comes as naturally to her as breathing. Several times during our conversation she offers to assist me personally with everything from community partnerships to my writing career, and after I mention casually I’ll be traveling abroad soon, she offers me money to buy a goat or chicken for a family in need.Morning to evening, nearly seven days a week, Karen and Michelle endure taxing commutes to bring harm reduction services to drug users in North Carolina’s hard-hit, rural areas. They ask nothing in return for their services. In fact, they seem critical of faith-based groups who use community outreach programs as a carrot to boost membership.“It’s hard to be trusted in a neighborhood like this [because people think] everyone wants to take them to church,” Karen explains, adding that this is why she maintains such a low-key presence on outreach. Instead of rolling up in a van stashed with free giveaways, she roams the streets where people can see her, offering nothing but a greeting unless she is asked.The Intersection Between Faith Communities and Harm ReductionThe Olive Branch Ministry’s approach could serve as an example for how faith-based communities and harm reduction can work together. The relationship is not always harmonious: some in the faith community accuse harm reductionists of enabling drug use or not doing enough to discourage problematic behavior. Conversely, many harm reductionists criticize faith groups for the hypocrisy of claiming to serve “the least of these” while refusing to help drug users, who belong to one of the most stigmatized and marginalized of all groups. Even when faith-based organizations do offer assistance, some peddle a strict, abstinence-only agenda or approach outreach with an attitude that appears to place more importance on gathering lost souls into the flock than on addressing people’s immediate needs.But despite the tenuous history between the groups, there is much cause for hope. Across the country, faith-based groups like The Olive Branch Ministry, Judson Memorial Church in New York City, St. Paul’s Episcopal Church in Arkansas, the national Interfaith Criminal Justice Coalition, and many more are forming active partnerships with harm reduction groups. Other organizations, including the United Methodist Church, Presbyterian Church (U.S.A.), United Church of Christ and National Council on Jewish Women have publicly proclaimed their support for harm reduction programs.The relationship between the faith community and harm reduction shows promise and room for growth. Especially in the South where faith is so important and drug users have so few services, these alliances are critical to stem the tide of deaths and disease caused by an unregulated drug supply, draconian laws, lack of sterile equipment, dearth of adequate treatment, stigma, and misunderstanding about what causes drug use to become problematic for many people.“I feel that faith communities in general think that harm reductionists are a bunch of left wing radicals,” says Michelle. “They think that we will come in and demand that the church hold drug user union meetings and do syringe exchange, but they don’t realize that we meet the congregation where they are…we figure out where they are comfortable and [decide] how to go from there.”Harm reduction groups and faith communities need to work together rather than at cross-purposes in order to reach and help as many people as possible. It's not always easy to find common ground; an olive branch is a good place to start.
from RSSMix.com Mix ID 8241841 https://www.thefix.com/how-harm-reductionists-keep-faith
0 notes
Text
How Harm Reductionists Keep the Faith
It’s a bitterly cold afternoon in early March as Karen Lowe and I pick our way down the broken sidewalks of a semi-abandoned neighborhood in Statesville, North Carolina. All around us, squatter houses stretch for blocks. Every window is busted or boarded up. Thin, dirty mattresses lie on sunken porches and feral dogs scrounge in the trash-strewn yards for scraps. Some residents are huddled inside for warmth, though in most of these homes, there is no electricity.The neighborhood is a depressing sight, but it’s hard to feel blue when you’re on outreach with Karen Lowe. Co-founder of the Olive Branch Ministry, a faith-based non-profit that brings harm reduction services to the seven foothill counties of North Carolina, Karen is the embodiment of love.Harm Reduction in the Deep SouthAs I burrow into my thin jacket, Karen strolls down the middle of the street extending warm greetings to the few brave souls who venture outside. Though the pockets of her cargo pants are bursting with clean syringes, naloxone, and other supplies to prevent death and disease among people who use drugs, she doesn’t flaunt her wares.“I just want people to see me,” she explains. “It’s about building trust. They know why I’m here. If they need something, they’ll come to me.”As we walk, the 52-year-old fills me in on the colorful cast of characters who call this neighborhood home, including a man who claims he hasn’t bathed in a year and an old woman who pees on the sidewalk. Karen describes everyone with great affection.“There is a certain kind of love that goes with being an untouchable,” she says. “And [the people of this community] have it. But it’s not allowed to grow.”There certainly isn’t much growing in this neighborhood. Judging by the columned porches on every house and what looks like abandoned flower gardens, this was probably once a desirable place to live. But shifting economic winds have devastated entire cities in the South and Statesville is no exception. A small inland city—population 26,000—Statesville boasts neither North Carolina’s green mountain range nor its sparkling coastline. It’s stranded in the flatland area of the state, mostly buried under strip malls and fast food restaurants. But despite so few bragging rights, Statesville embraces its Southern pride, describing itself on its website as “a city where fish is fried (as our Lord intended they be) and a bottle of Kraft French Dressing is good enough for anybody --- so get over yourself.” Also true to its Southern roots, while Statesville has recently invested in a splash park and a $330,000 home for veterans (more than double the average price of a house in the area), the city has allowed this particular neighborhood, in which residents are almost all black, to fall into ruin. The only people who venture into this place are the churches who occasionally come evangelizing and of course, the police, who make neighborhoods like this one their second home.But Karen brings cheer to this desolate area. Twelve years ago, she was homeless herself, struggling with mental illness and depression, and searching for both a literal and metaphorical place to set down roots. She found a surrogate family and a calling in a faith-based organization in Greensboro that provides services to people living with HIV. The community welcomed Karen with open arms and she became a regular at meetings, outreach events, and retreats, which she describes as “mad love and dealing with yourself, everybody crying and snotting.”Not Your Typical Faith-Based Outreach OrganizationKaren says she knew then that her life was about to change in remarkable ways. And was it ever. A couple years into her involvement with the faith community she met the love of her life, Michelle Mathis, a woman who shared her passion for helping people in need. Though they have the same heart for harm reduction, the pair is about as opposite as two people can be. Michelle exudes elegance with a powdered face and coiffed hair that somehow survive even in the god-awfullest North Carolina humidity. Her partner is more salt-of-the-earth.“I did the make-up and heels thing when I was young…somebody should have stopped me,” Karen laughs.The yin to the other’s yang, the two married in a private ceremony in 2009 where they exchanged olive branches instead of rings, thus creating what would become their joint life’s work, The Olive Branch Ministry.Olive Branch is not your typical faith-based outreach organization—and not just because its founders are an interracial queer couple spreading the word of Jesus in the Deep South. True to the tenets of harm reduction, whose guiding philosophy is “meet people where they are at,” Karen and Michelle serve without pretense or expectation.“We say faith is why we do [this work], but it’s not what we do,” Michelle explains to me over the phone. “If someone asks us to pray for them, we will pray for people…We take the message of harm reduction to faith communities…but we don’t evangelize.”During afternoon outreach with Karen, she utters not a whisper about faith. And yet, if God’s love for others were perfume, you’d smell her coming from blocks away. Helping others comes as naturally to her as breathing. Several times during our conversation she offers to assist me personally with everything from community partnerships to my writing career, and after I mention casually I’ll be traveling abroad soon, she offers me money to buy a goat or chicken for a family in need.Morning to evening, nearly seven days a week, Karen and Michelle endure taxing commutes to bring harm reduction services to drug users in North Carolina’s hard-hit, rural areas. They ask nothing in return for their services. In fact, they seem critical of faith-based groups who use community outreach programs as a carrot to boost membership.“It’s hard to be trusted in a neighborhood like this [because people think] everyone wants to take them to church,” Karen explains, adding that this is why she maintains such a low-key presence on outreach. Instead of rolling up in a van stashed with free giveaways, she roams the streets where people can see her, offering nothing but a greeting unless she is asked.The Intersection Between Faith Communities and Harm ReductionThe Olive Branch Ministry’s approach could serve as an example for how faith-based communities and harm reduction can work together. The relationship is not always harmonious: some in the faith community accuse harm reductionists of enabling drug use or not doing enough to discourage problematic behavior. Conversely, many harm reductionists criticize faith groups for the hypocrisy of claiming to serve “the least of these” while refusing to help drug users, who belong to one of the most stigmatized and marginalized of all groups. Even when faith-based organizations do offer assistance, some peddle a strict, abstinence-only agenda or approach outreach with an attitude that appears to place more importance on gathering lost souls into the flock than on addressing people’s immediate needs.But despite the tenuous history between the groups, there is much cause for hope. Across the country, faith-based groups like The Olive Branch Ministry, Judson Memorial Church in New York City, St. Paul’s Episcopal Church in Arkansas, the national Interfaith Criminal Justice Coalition, and many more are forming active partnerships with harm reduction groups. Other organizations, including the United Methodist Church, Presbyterian Church (U.S.A.), United Church of Christ and National Council on Jewish Women have publicly proclaimed their support for harm reduction programs.The relationship between the faith community and harm reduction shows promise and room for growth. Especially in the South where faith is so important and drug users have so few services, these alliances are critical to stem the tide of deaths and disease caused by an unregulated drug supply, draconian laws, lack of sterile equipment, dearth of adequate treatment, stigma, and misunderstanding about what causes drug use to become problematic for many people.“I feel that faith communities in general think that harm reductionists are a bunch of left wing radicals,” says Michelle. “They think that we will come in and demand that the church hold drug user union meetings and do syringe exchange, but they don’t realize that we meet the congregation where they are…we figure out where they are comfortable and [decide] how to go from there.”Harm reduction groups and faith communities need to work together rather than at cross-purposes in order to reach and help as many people as possible. It's not always easy to find common ground; an olive branch is a good place to start.
from RSSMix.com Mix ID 8241841 https://ift.tt/2UWIoWY
0 notes
Text
How Harm Reductionists Keep the Faith
It’s a bitterly cold afternoon in early March as Karen Lowe and I pick our way down the broken sidewalks of a semi-abandoned neighborhood in Statesville, North Carolina. All around us, squatter houses stretch for blocks. Every window is busted or boarded up. Thin, dirty mattresses lie on sunken porches and feral dogs scrounge in the trash-strewn yards for scraps. Some residents are huddled inside for warmth, though in most of these homes, there is no electricity.The neighborhood is a depressing sight, but it’s hard to feel blue when you’re on outreach with Karen Lowe. Co-founder of the Olive Branch Ministry, a faith-based non-profit that brings harm reduction services to the seven foothill counties of North Carolina, Karen is the embodiment of love.Harm Reduction in the Deep SouthAs I burrow into my thin jacket, Karen strolls down the middle of the street extending warm greetings to the few brave souls who venture outside. Though the pockets of her cargo pants are bursting with clean syringes, naloxone, and other supplies to prevent death and disease among people who use drugs, she doesn’t flaunt her wares.“I just want people to see me,” she explains. “It’s about building trust. They know why I’m here. If they need something, they’ll come to me.”As we walk, the 52-year-old fills me in on the colorful cast of characters who call this neighborhood home, including a man who claims he hasn’t bathed in a year and an old woman who pees on the sidewalk. Karen describes everyone with great affection.“There is a certain kind of love that goes with being an untouchable,” she says. “And [the people of this community] have it. But it’s not allowed to grow.”There certainly isn’t much growing in this neighborhood. Judging by the columned porches on every house and what looks like abandoned flower gardens, this was probably once a desirable place to live. But shifting economic winds have devastated entire cities in the South and Statesville is no exception. A small inland city—population 26,000—Statesville boasts neither North Carolina’s green mountain range nor its sparkling coastline. It’s stranded in the flatland area of the state, mostly buried under strip malls and fast food restaurants. But despite so few bragging rights, Statesville embraces its Southern pride, describing itself on its website as “a city where fish is fried (as our Lord intended they be) and a bottle of Kraft French Dressing is good enough for anybody --- so get over yourself.” Also true to its Southern roots, while Statesville has recently invested in a splash park and a $330,000 home for veterans (more than double the average price of a house in the area), the city has allowed this particular neighborhood, in which residents are almost all black, to fall into ruin. The only people who venture into this place are the churches who occasionally come evangelizing and of course, the police, who make neighborhoods like this one their second home.But Karen brings cheer to this desolate area. Twelve years ago, she was homeless herself, struggling with mental illness and depression, and searching for both a literal and metaphorical place to set down roots. She found a surrogate family and a calling in a faith-based organization in Greensboro that provides services to people living with HIV. The community welcomed Karen with open arms and she became a regular at meetings, outreach events, and retreats, which she describes as “mad love and dealing with yourself, everybody crying and snotting.”Not Your Typical Faith-Based Outreach OrganizationKaren says she knew then that her life was about to change in remarkable ways. And was it ever. A couple years into her involvement with the faith community she met the love of her life, Michelle Mathis, a woman who shared her passion for helping people in need. Though they have the same heart for harm reduction, the pair is about as opposite as two people can be. Michelle exudes elegance with a powdered face and coiffed hair that somehow survive even in the god-awfullest North Carolina humidity. Her partner is more salt-of-the-earth.“I did the make-up and heels thing when I was young…somebody should have stopped me,” Karen laughs.The yin to the other’s yang, the two married in a private ceremony in 2009 where they exchanged olive branches instead of rings, thus creating what would become their joint life’s work, The Olive Branch Ministry.Olive Branch is not your typical faith-based outreach organization—and not just because its founders are an interracial queer couple spreading the word of Jesus in the Deep South. True to the tenets of harm reduction, whose guiding philosophy is “meet people where they are at,” Karen and Michelle serve without pretense or expectation.“We say faith is why we do [this work], but it’s not what we do,” Michelle explains to me over the phone. “If someone asks us to pray for them, we will pray for people…We take the message of harm reduction to faith communities…but we don’t evangelize.”During afternoon outreach with Karen, she utters not a whisper about faith. And yet, if God’s love for others were perfume, you’d smell her coming from blocks away. Helping others comes as naturally to her as breathing. Several times during our conversation she offers to assist me personally with everything from community partnerships to my writing career, and after I mention casually I’ll be traveling abroad soon, she offers me money to buy a goat or chicken for a family in need.Morning to evening, nearly seven days a week, Karen and Michelle endure taxing commutes to bring harm reduction services to drug users in North Carolina’s hard-hit, rural areas. They ask nothing in return for their services. In fact, they seem critical of faith-based groups who use community outreach programs as a carrot to boost membership.“It’s hard to be trusted in a neighborhood like this [because people think] everyone wants to take them to church,” Karen explains, adding that this is why she maintains such a low-key presence on outreach. Instead of rolling up in a van stashed with free giveaways, she roams the streets where people can see her, offering nothing but a greeting unless she is asked.The Intersection Between Faith Communities and Harm ReductionThe Olive Branch Ministry’s approach could serve as an example for how faith-based communities and harm reduction can work together. The relationship is not always harmonious: some in the faith community accuse harm reductionists of enabling drug use or not doing enough to discourage problematic behavior. Conversely, many harm reductionists criticize faith groups for the hypocrisy of claiming to serve “the least of these” while refusing to help drug users, who belong to one of the most stigmatized and marginalized of all groups. Even when faith-based organizations do offer assistance, some peddle a strict, abstinence-only agenda or approach outreach with an attitude that appears to place more importance on gathering lost souls into the flock than on addressing people’s immediate needs.But despite the tenuous history between the groups, there is much cause for hope. Across the country, faith-based groups like The Olive Branch Ministry, Judson Memorial Church in New York City, St. Paul’s Episcopal Church in Arkansas, the national Interfaith Criminal Justice Coalition, and many more are forming active partnerships with harm reduction groups. Other organizations, including the United Methodist Church, Presbyterian Church (U.S.A.), United Church of Christ and National Council on Jewish Women have publicly proclaimed their support for harm reduction programs.The relationship between the faith community and harm reduction shows promise and room for growth. Especially in the South where faith is so important and drug users have so few services, these alliances are critical to stem the tide of deaths and disease caused by an unregulated drug supply, draconian laws, lack of sterile equipment, dearth of adequate treatment, stigma, and misunderstanding about what causes drug use to become problematic for many people.“I feel that faith communities in general think that harm reductionists are a bunch of left wing radicals,” says Michelle. “They think that we will come in and demand that the church hold drug user union meetings and do syringe exchange, but they don’t realize that we meet the congregation where they are…we figure out where they are comfortable and [decide] how to go from there.”Harm reduction groups and faith communities need to work together rather than at cross-purposes in order to reach and help as many people as possible. It's not always easy to find common ground; an olive branch is a good place to start.
0 notes
Photo

The only thing that Naloxone/Narcan enables is breath, life. Stop the nonsense, quit with the bullshit, fuck that ignorance, it enables life, period.
0 notes
Photo
What You Need to Know About Naloxone http://ift.tt/2FxmG41
The opioid epidemic in the U.S. is in full swing. In 2016 there were more deaths from drug overdoses than any other year previously, and almost two-thirds of those deaths involved opioids. Every day, there are over 100 American lives claimed by opioid overdose. In 2016, there were approximately 13,500 deaths related to heroin use, and in the four years prior, heroin-related deaths more than tripled.
What can be done about this epidemic that is sweeping across the country, affecting every demographic including all socioeconomic backgrounds? Some think that increasing access to the drug naloxone is necessary to combat the ever-rising wave of opioid overdoses.
What is Naloxone?
Naloxone is an opiate antidote. Opioids are a class of drug that includes both illegal and legal prescription drugs. Heroin and many prescription painkillers are all considered opiates. If a person is overdosing on an opioid, their breathing will slow way down, and it is very hard to arouse them from unconsciousness. Naloxone is a medication that blocks the effects of opioids and can reverse an opioid overdose.
Naloxone is not a controlled substance, and cannot be used to get high. In fact, if it is given to a person who has not had any opioids, it will have no effect on them.
How Does Naloxone Work?
If a person has opioids in their system and is given naloxone, the opioids are struck out of the brain receptors. This antidote can work even if the person has taken opioids along with other drugs or alcohol. Once a dose of naloxone is administered, the person’s breathing should begin to return to normal, and they will be reusable. Because brain damage can occur within just a few minutes of an overdose due to lack of oxygen, it is crucial that the person is given naloxone as soon as possible when overdosing. Naloxone can potentially save lives if given quickly, giving the person extra time until first responders arrive.
Naloxone is administered by intramuscular injection – in the larger muscles of the arm, thigh, or buttocks – or, more recently, by a nasal spray. Injection is the most common, but more and more U.S. cities are beginning to use the nasal spray as well. The medication typically works within the first five minutes, however, an additional dose may be needed if the person is still showing signs of overdose. About 30 minutes after the administration of naloxone, it begins to wear off and is mostly out of the patient’s system within 90 minutes. This gives the body enough time to process the opioid to the point where the patient isn’t as likely to stop breathing again.
Using naloxone will cause a person to immediately go into opioid withdrawal, which is often extremely uncomfortable, and should be monitored by medical professionals.
What is Naloxone Access Laws?
For many years, only emergency medical professionals (emergency medical technicians (EMT) and emergency room doctors and nurses) had access to naloxone. Naloxone Access Laws changed that, making it legal for anyone to have naloxone in their possession and providing legal civil and criminal amnesty for any unintended consequences when someone administers naloxone in good faith. Because naloxone has no street value and is nearly 100% harmless to healthy people, it would seem that Naloxone Access Laws would be widely accepted and enacted.
Before Naloxone Access Laws started to be enacted (only some states currently have them), some harm reduction groups circulated naloxone in at-risk areas even though it was illegal. Their common belief was that it is necessary to resort to illegal means if it was to save lives.
Should Naloxone Be Made More Available?
At first glance, increased access to naloxone seems only positive. After all, it can reverse the effects of opioid overdose quickly, it has no risks of addiction itself, and it is not dangerous if used on someone who has not ingested heroin or other opioid medications. It is undoubtedly one of the strongest tools for fighting overdose.
Even with that said, there are some concerns that have arisen regarding making naloxone access more relaxed. One of the biggest concerns is that non-medical personnel don’t have the necessary training to administer it properly. Naloxone induces immediate opioid withdrawal, and that can include serious side effects such as tachycardia (increased heart rate), vomiting, hypertension, and even hallucinations. It is thought that these side effects could be harmful to both the addict and any bystanders. Additionally, if it is given in a non-medical setting, it could lead to further complications.
Another concern shared by some medical professional and public safety officials is that the increased access and availability of naloxone may provide drug users with a false sense of security, leading to increasing opioid use and abuse and fewer people seeking treatment for opioid addiction. Despite the positive effects of naloxone – that it greatly increases chances of survival in the event of overdose – it isn’t completely foolproof. Opioid use is extremely dangerous and should not be underestimated.
Final Thoughts
Increased education about naloxone is needed. If it is to become more widely accessible, friends and family of those at risk of opioid overdose need proper training on how to administer it and the possible side effects. Users need to understand that it is not 100% guaranteed that they will be unscathed from an overdose just because they receive naloxone. It must be seen as a last-resort means to save lives, and not as something that enables further opioid abuse.
If you or a loved one is addicted to opioid drugs, your best course of action is to seek treatment for the addiction. Naloxone should not be a loophole that removes the necessity of proper treatment. If you or your loved one needs help, please contact Summit Behavioral Health. We can assist you with medical detox and addiction treatment.
The post What You Need to Know About Naloxone appeared first on Summit Behavioral Health.
February 01, 2018 at 02:38AM
0 notes
Last Seen Blogs

vietsaga-blog
Truyện dân gian Việt Nam - Vietnamese Folk Tales

drowninnoodles
DROWN IN NOODLES

hydn-jpg
how absurdly simple!

fuckyeahthisfoodrawks
This Food RAWKS!

hiddenscribe
You've Come to the Wrong Place