#image case journal
Text
Medical Image Journal: Journal of Medical Images

Medical Image Journal: Journal of Medical Images publishes medical image articles, images in medical science, imaging in medical journal, imaging in medical science journal, images in clinical medicine journal, images in medical research, imaging in medical research, image case journal etc. Journal allows for the peer-reviewed communication and archiving of Clinical and Medical Research, as well as applications, focused on medical imaging, a field that continues to benefit from technological improvements and yield biomedical advancements in the early detection, diagnostics, and therapy of disease as well as in the understanding of normal conditions.
Journal Homepage: https://www.literaturepublishers.org/
Manuscript Submission
Authors are requested to submit their manuscript by using Online Manuscript Submission Portal:
(or) also invited to submit through the Journal E-mail Id: [email protected]
Medical Image Journal: Journal of Medical Images provides a forum for the dissemination of new research results in the field of Medical and Clinical Image Journal, with special emphasis on efforts related to the applications of computer vision, virtual reality and robotics to biomedical imaging problems. Medical Image Journal: Journal of Medical Images publishes the highest quality, original papers that contribute to the basic science of processing, analyzing and utilizing medical and biological images for these purposes. Medical Image Journal: Journal of Medical Images is interested in approaches that utilize biomedical image datasets at all spatial scales, ranging from molecular/cellular imaging to tissue/organ imaging. While not limited to these alone, the typical biomedical image datasets of interest include those acquired from.
The types of papers accepted include those that cover the development and implementation of algorithms and strategies based on the use of various models (geometrical, statistical, physical, functional, etc.) to solve the following types of problems, using biomedical image datasets: representation of pictorial data, visualization, feature extraction, segmentation, inter-study and inter-subject registration, longitudinal / temporal studies, image-guided surgery and intervention, texture, shape and motion measurements, spectral analysis, digital anatomical atlases, statistical shape analysis, computational anatomy (modelling normal anatomy and its variations), computational physiology (modelling organs and living systems for image analysis, simulation and training), virtual and augmented reality for therapy planning and guidance, telemedicine with medical images, telepresence in medicine, telesurgery and image-guided medical robots, etc.
#Medical Image Journal: Journal of Medical Images publishes medical image articles#images in medical science#imaging in medical journal#imaging in medical science journal#images in clinical medicine journal#images in medical research#imaging in medical research#image case journal
0 notes
Text

Post Gremloblin Accident
Blank version under the cut

Feel free to use!
(Tag me if you do, I am excited to see your editions!)
#gravity falls#ford pines#fiddleford mcgucket#stanford pines#gravity falls memes#fiddleford h mcgucket#fiddauthor#if you want to read it that way#Guess who procrastinates going to sleep by making shitty memes again#right it's me#gf meme#meme template#meme#id in alt#if you read this leave a note if it's relevant to you if pictures have image descriptions or not#I think I will continue with them just in case#young fiddleford#journal 3
180 notes
·
View notes
Text
Original tweet, more information.
#brazil#brazilian politics#politics#environmental justice#indigenous rights#journalism#dom phillips#bruno araujo pereira#mod nise da silveira#image description in alt#°'everyday i wake up brazilian + just another case of the mondays amirite' intensify°
28 notes
·
View notes
Text
im literally in the trenches im going to war im being exploded im being war crimed u have no idea what im going thru u dont understand
5 notes
·
View notes
Text
The New York Times, however, does have rules and norms. Schwartz had no prior reporting experience. Her reporting partner Gettleman explained the basics to her, Schwartz said in a podcast interview on January 3, produced by Israel’s Channel 12 and conducted in Hebrew.
Gettleman, she said, was concerned they “get at least two sources for every detail we put into the article, cross-check information. Do we have forensic evidence? Do we have visual evidence? Apart from telling our reader ‘this happened,’ what can we say? Can we tell what happened to whom?”
Schwartz said she was initially reluctant to take the assignment because she did not want to look at visual images of potential assaults and because she lacked the expertise to conduct such an investigation.
This is stunning.
The fear among Times staffers who have been critical of the paper’s Gaza coverage is that Schwartz will become a scapegoat for what is a much deeper failure. She may harbor animosity toward Palestinians, lack the experience with investigative journalism, and feel conflicting pressures between being a supporter of Israel’s war effort and a Times reporter, but Schwartz did not commission herself and her nephew to report one of the most consequential stories of the war. Senior leadership at the New York Times did.
Schwartz said as much in an interview with Israeli Army Radio on December 31. “The New York Times said, ‘Let’s do an investigation into sexual violence’ — it was more a case of them having to convince me,” she said. Her host cut her off: “It was a proposal of The New York Times, the entire thing?”
“Unequivocally. Unequivocally. Obviously. Of course,” she said. “The paper stood behind us 200 percent and gave us the time, the investment, the resources to go in-depth with this investigation as much as needed.”
The whole piece is quite long, please go read it yourself, it's quite definitive.
11K notes
·
View notes
Text
Retinal and choroidal vascular drop out in a case of severe phenotype of Flammer Syndrome. Rescue of the ischemic-preconditioning mimicking action of endogenous Erythropoietin (EPO) by off-label intra vitreal injection of recombinant human EPO (rhEPO) by Claude Boscher in Journal of Clinical Case Reports Medical Images and Health Sciences

Journal of Clinical Case Reports Medical Images and Health Sciences
ABSTRACT
Background: Erythropoietin (EPO) is a pleiotropic anti-apoptotic, neurotrophic, anti-inflammatory, and pro-angiogenic endogenous agent, in addition to its effect on erythropoiesis. Exogenous EPO is currently used notably in human spinal cord trauma, and pilot studies in ocular diseases have been reported. Its action has been shown in all (neurons, glia, retinal pigment epithelium, and endothelial) retinal cells. Patients affected by the Flammer Syndrome (FS) (secondary to Endothelin (ET)-related endothelial dysfunction) are exposed to ischemic accidents in the microcirculation, notably the retina and optic nerve.
Case Presentation: A 54 years old female patient with a diagnosis of venous occlusion OR since three weeks presented on March 3, 2019. A severe Flammer phenotype and underlying non arteritic ischemic optic neuropathy; retinal and choroidal drop-out were obviated. Investigation and follow-up were performed for 36 months with Retinal Multimodal Imaging (Visual field, SD-OCT, OCT- Angiography, Indo Cyanin Green Cine-Video Angiography). Recombinant human EPO (rhEPO)(EPREX®)(2000 units, 0.05 cc) off-label intravitreal injection was performed twice at one month interval. Visual acuity rapidly improved from 20/200 to 20/63 with disparition of the initial altitudinal scotoma after the first rhEPO injection, to 20/40 after the second injection, and gradually up to 20/32, by month 5 to month 36. Secondary cystoid macular edema developed ten days after the first injection, that was not treated via anti-VEGF therapy, and resolved after the second rhEPO injection. PR1 layer integrity, as well as protective macular gliosis were fully restored. Some level of ischemia persisted in the deep capillary plexus and at the optic disc.
Conclusion: Patients with FS are submitted to chronic ischemia and paroxystic ischemia/reperfusion injury that drive survival physiological adaptations via the hypoxic-preconditioning mimicking effect of endogenous EPO, that becomes overwhelmed in case of acute hypoxic stress threshold above resilience limits. Intra vitreal exogenous rhEPO injection restores retinal hypoxic-preconditioning adaptation capacity, provided it is timely administrated. Intra vitreal rhEPO might be beneficial in other retinal diseases of ischemic and inflammatory nature.
Key words : Erythropoietin, retinal vein occlusion, anterior ischemic optic neuropathy, Flammer syndrome, Primary Vascular Dysfunction, anti-VEGF therapy, Endothelin, microcirculation, off-label therapy.
INTRODUCTION
Retinal Venous Occlusion (RVO) treatment still carries insufficiencies and contradictions (1) due to the incomplete deciphering of the pathophysiology and of its complex multifactorial nature, with overlooking of factors other than VEGF up-regulation, notably the roles of retinal venous tone and Endothelin-1 (ET) (2-5), and of endothelial caspase-9 activation (6). Flammer Syndrome (FS)( (Primary Vascular Dysfunction) is related to a non atherosclerotic ET-related endothelial dysfunction in a context of frequent hypotension and increased oxidative stress (OS), that alienates organs perfusion, with notably changeable functional altered regulation of blood flow (7-9), but the pathophysiology remains uncompletely elucidated (8). FS is more frequent in females, and does not seem to be expressed among outdoors workers, implying an influence of sex hormons and light (7)(9). ET is the most potent pro-proliferative, pro-fibrotic, pro-oxidative and pro-inflammatory vasoconstrictor, currently considered involved in many diseases other than cardio-vascular ones, and is notably an inducer of neuronal apoptosis (10). It is produced by endothelial (EC), smooth vascular muscles (SVMC) and kidney medullar cells, and binds the surface Receptors ET-A on SVMC and ET-B on EC, in an autocrine and paracrine fashion. Schematically, binding on SVMC Receptors (i.e. through local diffusion in fenestrated capillaries or dysfunctioning EC) and on EC ones (i.e. by circulating ET) induce respectively arterial and venous vasoconstriction, and vasodilation, the latter via Nitrite oxide (NO) synthesis. ET production is stimulated notably by Angiotensin 2, insulin, cortisol, hypoxia, and antagonized by endothelial gaseous NO, itself induced by flow shear stress. Schematically but not exclusively, vascular tone is maintained by a complex regulation of ET-NO balance (8) (10-11). Both decrease of NO and increase of ET production are both a cause and consequence of inflammation, OS and endothelial dysfunction, that accordingly favour vasoconstriction; in addition ET competes for L-arginine substrate with NO synthase, thereby reducing NO bioavailability, a mechanism obviated notably in carotid plaques and amaurosis fugax (reviewed in 11).
Severe FS phenotypes are rare. Within the eye, circulating ET reaches retinal VSMC in case of Blood-Retinal-Barrier (BRB) rupture and diffuses freely via the fenestrated choroidal circulation, notably around the optic nerve (ON) head behind the lamina cribrosa, and may induce all pathologies related to acute ocular blood flow decrease (2-3)(5)(7-9). We previously reported two severe cases with rapid onset of monocular cecity and low vision, of respectively RVO in altitude and non arteritic ischemic optic neuropathy (NAION) (Boscher et al, Société Francaise d'Ophtalmologie and Retina Society, 2015 annual meetings).
Exogenous Recombinant human EPO (rhEPO) has been shown effective in humans for spinal cord injury (12), neurodegenerative and chronic kidney diseases (CKD) (reviewed in 13). Endogenous EPO is released physiologically in the circulation by the kidney and liver; it may be secreted in addition by all cells in response to hypoxic stress, and it is the prevailing pathway induced via genes up-regulation by the transcription factor Hypoxia Inducible Factor 1 alpha, among angiogenesis (VEGF pathway), vasomotor regulation (inducible NO synthase), antioxidation, and energy metabolism (14). EPO Receptor signaling induces cell proliferation, survival and differentiation (reviewed in 13), and targets multiple non hematopoietic pathways as well as the long-known effect on erythropoiesis (reviewed in 15). Of particular interest here, are its synergistic anti-inflammatory, neural antiapoptotic (16) pro-survival and pro-regenerative (17) actions upon hypoxic injury, that were long-suggested to be also indirect, via blockade of ET release by astrocytes, and assimilated to ET-A blockers action (18). Quite interestingly, endogenous EPO’s pleiotropic effects were long-summarized (back to 2002), as “mimicking hypoxic-preconditioning” by Dawson (19), a concept applied to the retina (20). EPO Receptors are present in all retinal cells and their rescue activation targets all retinal cells, i.e. retinal EC, neurons (photoreceptors (PR), ganglion (RGG) and bipolar cells), retinal pigment epithelium (RPE) osmotic function through restoration of the BRB, and glial cells (reviewed in 21), and the optic nerve (reviewed in 22). RhEPO has been tested experimentally in animal models of glaucoma, retinal ischemia-reperfusion (I/R) and light phototoxicity, via multiple routes (systemic, subconjunctival, retrobulbar and intravitreal injection (IVI) (reviewed in 23), and used successfully via IVI in human pilot studies, notably first in diabetic macular edema (24) (reviewed in 25 and 26). It failed to improve neuroprotection in association to corticosteroids in optic neuritis, likely for bias reasons (reviewed in 22). Of specific relation to the current case, it has been reported in NAION (27) (reviewed in 28) and traumatic ON injury (29 Rashad), and in one case of acute severe central RVO (CRVO) (Luscan and Roche, Société Francaise d’Ophtalmologie 2017 annual meeting). In addition EPO RPE gene therapy was recently suggested to prevent retinal degeneration induced by OS in a rodent model of dry Age Macular Degeneration (AMD) (30).
CASE REPORT PRESENTATION
This 54 years female patient was first visited on March 2019 4th, seeking for second opinion for ongoing vision deterioration OR on a daily basis, since around 3 weeks. Sub-central RVO (CRVO) OR had been diagnosed on February 27th; available SD-OCT macular volume was increased with epiretinal marked hyperreflectivity, one available Fluorescein angiography picture showed a non-filled superior CRVO, and a vast central ischemia involving the macular and paraoptic territories. Of note there was ON edema with a para-papillary hemorrage nasal to the disc on the available colour fundus picture.
At presentation on March 4, Best Corrected Visual Acuity (BCVA) was reduced at 20/100 OR (20/25 OS). The patient described periods of acutely excruciating retro-orbital pain in the OR. Intraocular pressure was normal, at 12 OR and 18 OS (pachymetry was at 490 microns in both eyes). The dilated fundus examination was similar to the previous color picture and did not disclose peripheral hemorrages recalling extended peripheral retinal ischemia. Humphrey Visual Field disclosed an altitudinal inferior scotoma and a peripheral inferior scotoma OR and was in the normal range OS, i.e. did not recall normal tension glaucoma OS (Fig. 1). There were no papillary drusen on the autofluorescence picture, ON volume was increased (11.77 mm3 OR versus 5.75 OS) on SD-OCT (Heidelberg Engineering®) OR, Retinal Nerve Fiber (RNFL) and RGC layers thicknesses were normal (Fig. 2). Marked epimacular hypereflectivity OR with foveolar depression inversion, moderately increased total volume and central foveolar thickness (CFT) (428 microns versus 328 OS), and a whitish aspect of the supero-temporal internal retinal layers recalling ischemic edema, were present (video 1). EDI CFT was incresead at 315 microns (versus 273 microns OS), with focal pachyvessels on the video mapping (video 1). OCT-Angiography disclosed focal perfusion defects in both the retinal and chorio-capillaris circulations (Fig. 3), and central alterations of the PR1 layer on en-face OCT(Fig. 4).
Altogether the clinical picture evoked a NAION with venous sub-occlusion, recalling Fraenkel’s et al early hypothesis of an ET interstitial diffusion-related venous vasoconstriction behind the lamina cribrosa (2), as much as a rupture of the BRB was present in the optic nerve area (hemorrage along the optic disc). Choroidal vascular drop-out was suggested by the severity and rapidity of the VF impairment (31). The extremely rapid development of a significant “epiretinal membrane”, that we interpreted as a reactive - and protective, in absence of cystoid macular edema (CME) - ET 2-induced astrocytic proliferation (reviewed in 32), was as an additional sign of severe ischemia.
The mention of the retro-orbital pain evoking a “ciliary angor”, the absence of any inflammatory syndrome and of the usual metabolic syndrome in the emergency blood test, oriented the etiology towards a FS. And indeed anamnesis collected many features of the FS, i.e. hypotension (“non dipper” profile with one symptomatic nocturnal episode of hypotension on the MAPA), migrains, hypersensitivity to cold, stress, noise, smells, and medicines, history of a spontaneously resolutive hydrops six months earlier, and of paroxystic episods of vertigo (which had driven a prior negative brain RMI investigation for Multiple Sclerosis, a frequent record among FS patients (33) and of paroxystic visual field alterations (7)(9), that were actually recorded several times along the follow-up.
The diagnosis of FS was eventually confirmed in the Ophthalmology Department in Basel University on April 10th, with elevated retinal venous pressure (20 to 25mmHg versus 10-15 OS) (4)(7)(9), reduced perfusion in the central retinal artery and veins on ocular Doppler (respectively 8.3 cm/second OR velocity versus 14.1 mmHg OS, and 3.1/second OR versus 5.9 cm OS), and impaired vasodilation upon flicker light-dependant shear stress on the Dynamic Vessel Analyser testing (7-9). In addition atherosclerotic plaques were absent on carotid Doppler.
On March 4th, the patient was at length informed about the FS, a possible off label rhEPO IVI, and a related written informed consent on the ratio risk-benefits was delivered.
By March 7th, she returned on an emergency basis because of vision worsening OR. VA was unchanged, intraocular pressure was at 13, but Visual Field showed a worsening of the central and inferior scotomas with a decreased foveolar threshold, from 33 to 29 decibels. SD-OCT showed a 10% increase in the CFT volume.
On the very same day, an off label rhEPO IVI OR (EPREX® 2000 units, 0,05 cc in a pre-filled syringe) was performed in the operating theater, i.e. the dose reported by Modarres et al (27), and twenty times inferior to the usual weekly intravenous dose for treatment of chronic anemia secondary to CKD. Intra venous acetazolamide (500 milligrams) was performed prior to the injection, to prevent any increase in intra-ocular pressure. The patient was discharged with a prescription of chlorydrate betaxolol (Betoptic® 0.5 %) two drops a day, and high dose daily magnesium supplementation (600 mgr).
Incidentally the patient developed bradycardia the day after, after altogether instillation of 4 drops of betaxolol only, that was replaced by acetazolamide drops, i.e. a typical hypersensitivity reaction to medications in the FS (7)(9).
Subjective vision improvement was recorded as early as D1 after injection. By March 18 th, eleven days post rhEPO IVI, BCVA was improved at 20/63, the altitudinal scotoma had resolved (Fig. 5), Posterior Vitreous Detachment had developed with a disturbing marked Weiss ring, optic disc swelling had decreased; vasculogenesis within the retinal plexi and some regression of PR1 alterations were visible on OCT-en face. Indeed by 11 days post EPO significant functional, neuronal and vascular rescue were observed, while the natural evolution had been seriously vision threatening.
However cystoid ME (CME) had developed (video 2). Indo Cyanin Green-Cine Video Angiography (ICG-CVA) OR, performed on March 23, i.e. 16 days after the rhEPO IVI, showed a persistent drop in ocular perfusion: ciliary and central retinal artery perfusion timings were dramatically delayed at respectively 21 and 25 seconds, central retinal vein perfusion initiated by 35 seconds, was pulsatile, and completed by 50 seconds only (video 3). Choroidal pachyveins matching the ones on SD-OCT video mapping were present in the temporal superior and inferior fields, and crossed the macula; capillary exclusion territories were present in the macula and around the optic disc.
By April 1, 23 days after the rhEPO injection, VA was unchanged, but CME and perfusion voids in the superficial deep capillary plexi and choriocapillaris were worsened, and optic disc swelling had recurred back to baseline, in a context of repeated episodes of systemic hypotension; and actually Nifepidin-Ratiopharm® oral drops (34), that had been delivered via a Temporary Use Authorization from the central Pharmacology Department in Assistance Publique Hopitaux de Paris, had had to be stopped because of hypersensitivity.
A second off label rhEPO IVI was performed in the same conditions on April 3, i.e. approximately one month after the first one.
Evolution was favourable as early as the day after EPO injection 2: VA was improved at 20/40, CME was reduced, and perfusion improved in the superficial retinal plexus as well as in the choriocapillaris. By week 4 after EPO injection 2, CME was much decreased, i.e. without anti VEGF injection. On august 19th, by week 18 after EPO 2, perfusion on ICG-CVA was greatly improved , with ciliary timing at 18 seconds, central retinal artery at 20 seconds and venous return from 23 to 36 seconds, still pulsatile. Capillary exclusion territories were visible in the macula and temporal to the macula after the capillary flood time that went on by 20.5 until 22.5 seconds (video 4); they were no longer persistent at intermediate and late timings.
Last complete follow-up was recorded on January 7, 2021, at 22 months from EPO injection 2. BCVA was at 20/40, ON volume had dropped at 7.46 mm3, a sequaelar superior deficit was present in the RNFL (Fig. 2) with some corresponding residual defects on the inferior para central Visual Field (Fig. 5), CFT was at 384 mm3 with an epimacular hyperreflectivity without ME, EDI CFT was dropped at 230 microns. Perfusion on ICG-CVA was not normalized, but even more improved, with ciliary timing at 15 seconds, central retinal artery at 16 seconds and venous return from 22 to 31 seconds, still pulsatile (video 5), indicating that VP was still above IOP. OCT-A showed persisting perfusion voids, especially at the optic disc and within the deep retinal capillary plexus. The latter were present at some degree in the OS as well (Fig. 6). Choriocapillaris and PR1 layer were dramatically improved.
Last recorded BCVA was at 20/32 by February 14, 2022, at 34 months from EPO 2. SD-OCT showed stable gliosis hypertrophy and mild alterations of the external layers (video 6).
Figure 1: Humphrey visual field at baseline on March 7th 2019, showing an altitudinal central scotoma, an inferior peripheral scotoma with a normal and symmetrical foveolar sensitivity threshold, and a normal visual field OS
Figure 2: Retinal Nerve Fiber (RNFL ) evolution from normal at baseline on March 2019 7th, to development of a superior sequellar deficit that remained stable on last follow-up.
Figure 3: OCT-Angiography at baseline on March 7th 2019, showing perfusion voids OR in the superior superficial retinal plexus and in the choriocapillaris.
Figure 4: OCT en face at baseline on March 7th 2019, showing PR1 layer deficits OR (artefacts in the superior half) compared to OS.
Figure 5: Humphrey visual field follow-ups : at follow-up 1 eleven days after rhEPO intra vitreal injection showing resolution of the altitudinal central scotoma and decrease of the inferior scotoma, and at last visual field follow-up on January 20th 2021, showing residual defects corresponding to the RNFL ones on Figure 2.
Figure 6: OCT Angiography performed on January 7th 2021, at 22 months from EPO injection 2, showing persisting perfusion voids, especially at the optic disc, and within the deep retinal capillary plexus, that were present at some degree in the OS as well.
Video 1 : SD-OCT video mapping OR at baseline on March 7th 2019, showing epiretinal hyperreflectivity and epiretinal membrane with foveolar depression inversion, ischemic edema in the internal and temporal to the disc superior retinal layers, and focal choroidal Haller pachyvessels with reduction in chorio-capillaris/Sattler layers.
Vedio: https://jmedcasereportsimages.org/articles/JCRMHS_1231_Vedio_1.mov
Video 2: SD-OCT video mapping OR at follow-up 1 eleven days after rhEPO intra vitreal injection on March 18th, showing epiretinal hyperreflectivity and epiretinal membrane with foveolar depression inversion, ischemic edema in the internal and temporal to the disc superior retinal layers, and development of central cystoid macular edema.
Vedio: https://jmedcasereportsimages.org/articles/JCRMHS_1231_Vedio_2.mov
Video 3 : Indo Cyanin Green-Cine Video Angiography OR, performed on March 23, i.e. 16 days after the rhEPO IVI, showing a persistent drop in ocular perfusion: ciliary and central retinal artery perfusion timings were dramatically delayed at respectively 21 and 25 seconds, central retinal vein perfusion initiated by 35 seconds, was pulsatile, and completed by 50 seconds only.
Vedio: https://jmedcasereportsimages.org/articles/JCRMHS_1231_Vedio_3.mov
Video 4 : Indo Cyanin Green-Cine Video Angiography OR, performed on August 19, i.e. by week 18 after EPO 2, showing greatly improved perfusion, with ciliary timing at 18 seconds, central retinal artery at 20 seconds and venous return from 23 to 36 seconds, still pulsatile. Capillary exclusion territories were visible in the macula and temporal to the macula after the capillary flood time that went on by 20.5 until 22.5 seconds.
Vedio: https://jmedcasereportsimages.org/articles/JCRMHS_1231_Vedio_4.mov
Video 5: Indo Cyanin Green-Cine Video Angiography OR, performed on January 7th, 2021, at 22 months from EPO injection 2: perfusion was not normalized, but even more improved, with ciliary timing at 15 seconds, central retinal artery at 16 seconds and venous return from 22 to 31 seconds, still pulsatile.
Vedio: https://jmedcasereportsimages.org/articles/JCRMHS_1231_Vedio_5.avi
Video 6 : SD-OCT video mapping at 34 months from EPO 2, showing stable gliosis hypertrophy and mild alterations of the external layers.
Vedio: https://jmedcasereportsimages.org/articles/JCRMHS_1231_Vedio_6.avi
DISCUSSION
What was striking in the initial clinical phenotype of CRVO was the contrast between the moderate venous dilation, and the intensity of ischemia, that were illustrating the pioneer hypothesis of Professor Flammer‘s team regarding the pivotal role of ET in VO (2), recently confirmed (3)(35), i.e. the local venous constriction backwards the lamina cribrosa, induced by diffusion of ET-1 within the vascular interstitium, in reaction to hypoxia. NAION was actually the primary and prevailing alteration, and ocular hypoperfusion was confirmed via ICG-CVA, as well as by the ocular Doppler performed in Basel. ICG-CVA confirmed the choroidal drop-out suggested by the severity of the VF impairment (31) and by OCT-A in the choriocapillaris. Venous pressure measurement, which instrumentation is now available (8), should become part of routine eye examination in case of RVO, as it is key to guide cases analysis and personalized therapeutical options.
Indeed, the endogenous EPO pathway is the dominant one activated by hypoxia and is synergetic with the VEGF pathway, and coherently it is expressed along to VEGF in the vitreous in human RVO (36). Diseases develop when the individual limiting stress threshold for efficient adaptative reactive capacity gets overwhelmed. In this case by Week 3 after symtoms onset, neuronal and vascular resilience mechanisms were no longer operative, but the BRB, compromised at the ON, was still maintained in the retina.
As mentioned in the introduction, the scientific rationale for the use of EPO was well demonstrated by that time, as well as the capacities of exogenous EPO to mimic endogenous EPO vasculogenesis, neurogenesis and synaptogenesis, restoration of the balance between ET-1 and NO. Improvement of chorioretinal blood flow was actually illustrated by the evolution of the choriocapillaris perfusion on repeated OCT-A and ICG-CVA. The anti-apoptotic effect of EPO (16) seems as much appropriate in case of RVO as the caspase-9 activation is possibly another overlooked co-factor (6).
All the conditions for translation into off label clinical use were present: severe vision loss with daily worsening and unlikely spontaneous favourable evolution, absence of toxicity in the human pilot studies, of contradictory comorbidities and co-medications, and of context of intraocular neovascularization that might be exacerbated by EPO (37).
Why didn’t we treat the onset of CME by March 18th, i.e. eleven days after EPO IVI 1, by anti-VEGF therapy, the “standard-of-care” in CME for RVO ?
In addition to the context of functional, neuronal and vascular improvements obviated by rhEPO IVI by that timing in the present case, actually anti VEGF therapy does not address the underlying causative pathology. Coherently, anti-VEGF IVI : 1) may not be efficient in improving vision in RVO, despite its efficiency in resolving/improving CME (usually requiring repeated injections), as shown in the Retain study (56% of eyes with resolved ME continued to loose vision)(quoted in (1) 2) eventually may be followed by serum ET-1 levels increase and VA reduction (in 25% of cases in a series of twenty eyes with BRVO) (38) and by increased areas of non perfusion in OCT-A (39). Rather did we perform a second hrEPO IVI, and actually we consider open the question whether the perfusion improvement, that was progressive, might have been accelerated/improved via repeated rhEPO IVI, on a three to four weeks basis.
The development of CME itself, involving a breakdown of the BRB, i.e. of part of the complex retinal armentorium resilience to hypoxia, was somewhat paradoxical in the context of improvement after the first EPO injection, as EPO restores the BRB (24), and as much as it was suggested that EPO inhibits glial osmotic swelling, one cause of ME, via VEGF induction (40). Possible explanations were: 1) the vascular hyperpermeability induced by the up-regulation of VEGF gene expression via EPO (41) 2) the ongoing causative disease, of chronic nature, that was obviated by the ICG-CVA and the Basel investigation, responsible for overwhelming the gliosis-dependant capacity of resilience to hypoxia 3) a combination of both. I/R seemed excluded: EPO precisely mimics hypoxic reconditioning as shown in over ten years publications, including in the retina (20), and as EPO therapy is part of the current strategy for stabilization of the endothelial glycocalix against I/R injury (42-43). An additional and not exclusive possible explanation was the potential antagonist action of EPO on GFAP astrocytes proliferation, as mentioned in the introduction (18), that might have counteracted the reactive protective hypertrophic gliosis, still fully operative prior to EPO injection, and that was eventually restored during the follow-up, where epiretinal hyperreflectivity without ME and ongoing chronic ischemia do coincide (Fig. 6 and video 6), as much as it is unlikely that EPO’s effect would exceed one month (cf infra). Inhibition of gliosis by EPO IVI might have been also part of the mechanism of rescue of RGG, compromised by gliosis in hypoxic conditions (44). Whatever the complex balance initially reached, then overwhelmed after EPO IVI 1, the challenge was rapidly overcome by the second EPO IVI without anti-VEGF injection, likely because the former was powerful enough to restore the threshold limit for resilience to hypoxia, that seemed no longer reached again during the relapse-free follow-up. Of note, this “epiretinal membrane “, which association to good vision is a proof of concept of its protective effect, must not be removed surgically, as it would suppress one of the mecanisms of resilience to hypoxia.
To our best knowledge, ICG-CVA was never reported in FS; it allows real time evaluation of the ocular perfusion and illustration of the universal rheological laws that control choroidal blood flow as well. Pachyveins recall a “reverse” veno-arteriolar reflex in the choroidal circulation, that is NO and autonomous nervous system-dependant, and that we suggested to be an adaptative choroidal microcirculation process to hypoxia (45). Their persistence during follow-up accounts for a persisting state of chronic ischemia.
The optimal timing for reperfusion via rhEPO in a non resolved issue:
in the case reported by Luscan and Roche, rhEPO IVI was performed on the very same day of disease onset, where it induced complete recovery from VA reduced at counting fingers at 1 meter, within 48 hours. This clinical human finding is on line with a recent rodent stroke study that established the timings for non lethal versus lethal ischemia of the neural and vascular lineages, and the optimized ones for beneficial reperfusion: the acute phase - from Day 1 where endothelial and neural cells are still preserved, to Day 7 where proliferation of pericytes and Progenitor Stem Cells are obtainable - and the chronic stage, up to Day 56, where vasculogenesis, neurogenesis and functional recovery are still possible, but with uncertain efficiency (46). In our particular case, PR rescue after rhEPO IVI 1 indicated that Week 3 was still timely. RhEPO IVI efficacy was shown to last between one (restoration of the BRB) and four weeks (antiapoptotic effect) in diabetic rats (24). The relapse after Week 3 post IVI 1 might indicate that it might be approximately the interval to be followed, should repeated injections be necessary.
The bilateral chronic perfusion defects on OCT-A at last follow-up indicate that both eyes remain in a condition of chronic ischemia and I/R, where endogenous EPO provides efficient ischemic pre-conditioning, but is potentially susceptible to be challenged during episodes of acute hypoxia that overwhelm the resilience threshold.
CONCLUSION
The present case advocates for individualized medicine with careful recording of the medical history, investigation of the systemic context, and exploiting of the available retinal multimodal imaging for accurate analytical interpretation of retinal diseases and their complex pathophysiology. The Flammer Syndrome is unfortunately overlooked in case of RVO; it should be suspected clinically in case of absence of the usual vascular and metabolic context, and in case of elevated RVP. RhEPO therapy is able to restore the beneficial endogenous EPO ischemic pre-conditioning in eyes submitted to challenging acute hypoxia episodes in addition to chronic ischemic stress, as in the Flammer Syndrome and fluctuating ocular blood flow, when it becomes compromised by the overwhelming of the hypoxic stress resilience threshold. The latter physiopathological explanation illuminates the cases of RVO where anti-VEGF therapy proved functionally inefficient, and/or worsened retinal ischemia. RhEPO therapy might be applied to other chronic ischemia and I/R conditions, as non neo-vascular Age Macular Degeneration (AMD), and actually EPO was listed in 2020 among the nineteen promising molecules in AMD in a pooling of four thousands (47).
For more information regarding our Journal: https://jmedcasereportsimages.org/about-us/
For more artices: https://jmedcasereportsimages.org/archive/
0 notes
Text
Love and Deepspace men x fem!reader slightly unhinged HCs
I started Love and Deepspace yesterday so please have my slightly unhinged HCs for the men so far. And minors don’t you dare interact
Part 2

Rafayel
He’s a biter. Leaves you covered in marks from your neck all the way down your thighs.
Plans a date where he’s laid out a huge canvas on the floor of his studio, puts your fave color paint on your hands and his favorite color on his hands, plus several globs of the two colors across the canvas, and then proceeds to have the wildest three rounds of sex on that canvas as it gets progressively more covered in paint. Sells the painting for 6 figures a few weeks later and uses it as an excuse that you need to make more of them.
Tells you his best masterpiece is painting your body with his cum—got really into it once and dipped the paint brush into your cunt to collect his cum and then painted it across your breasts
Has a secret sketch book that’s nothing but pictures of you. Lots of them are of you sleeping when he can study your features but there’s still quite a few he drew from memory.
Made you lay down naked with your legs spread and be still so he could draw the most detailed image of your pussy you could possibly imagine. It’s his personal fave that no one besides him will ever see.
Sees shibari as a beautiful art form and likes to practice with you—has a whole album in his phone just of pics of you tied up all pretty for him
Rarely gets soft in a serious way, he much prefers the teasing back and forth you two usually have.
Xavier
He’s definitely broken into your room Edward Cullen style and watched you sleep
His favorite dates are taking you into the forest at night to watch the stars and moon together. Bonus points if you come across a wanderer and get to fight together.
Clingy after you become his, always wants to be touching you and doesn’t let you out of his sight (and yes that means sometimes he’s following you but it’s just because you’re brave and reckless and he worries)
When he eats you out, he holds both your hands in his for you to hold on to and does it with no hands—makes you cum more times on his tongue than you could fathom (and yes, he’s eating you for his pleasure)
Downloaded a tracker into your watch so he can know where you are at all times
Gets horny when he watches you fight and has def pulled you aside during a mission for a quickie in which you end up having your cunt stuffed with cum for the remainder of the mission
Such a cuddler but like a cat where he only wants to cuddle if he wants to—falls asleep nearly instantly in your arms like the cute sleepyhead he is
Zayne
Finds it so cute the first time he comes to your apartment and sees all the little snow creatures he’d made you sitting in a windowsill together. Makes you so many more after that. Sends you a bouquet of flowers made from his ice too (#Elsa)
Has food delivered to you at lunch on days he knows you’re super busy so you don’t forget to eat since you often forget to take care of yourself (he doesn’t mind too much since he likes that you let him take care of you)
Prefers kisses over hugs, except when he’s sad because of a patient (then he likes the warm comfort of your hugs)
Moves his glasses to the top of his head and rubs the bridge of his nose when he gets really stressed
Brings you a mild painkiller after blowing your back out, a smug but tiny smile on his lips, and tells you, “I was a bit rough so humor me and take this medicine. I don’t want you in excess pain because of me.”
Loves when you want to lay on his chest when he’s reading through cases and medical journals at night. He’ll read them out loud until you fall asleep and then finish them quietly as you snore softly into his chest
Calls you before a difficult surgery because your voice instantly calms him down
Into bondage—specifically he likes to tie you up so you can’t escape when he starts to overstimulate you. He really can’t help it, you just make such pretty noises for him when he gets you to that point that he has to keep going
Tags: @adaurielle @luffysprincess @seraphofthesimps
#love and deepspace#love and Deepspace HCs#zayne love and deepspace#Zayne HCs#zayne x reader#rafayel#rafayel love and deepspace#rafayel HCs#rafayel x reader#Xavier x reader#xavier love and deepspace
4K notes
·
View notes
Text

Case Report of Coronary Artery Disease Journal publishes surgery in Coronary Artery Diseases journal, images in Coronary Artery Disease, journal of Coronary Artery Disease case reports, Coronary Artery journal etc. Case Reports in Coronary Heart Disease is peer reviewed worldwide reputed medical cardiology journal.
#Case Reports in Coronary Heart Disease#Case Report of Coronary Artery Disease Journal#surgery in Coronary Artery Diseases journal#images in Coronary Artery Disease
0 notes
Text
Case Report Journal of Cardiovascular Medicine publishes imaging in Cardiovascular Medicine, case reports in Cardiovascular Medicine, videos in Cardiovascular Medicine case reports journal etc. This is further assessment and peer-reviewed by the editors of Cardiovascular Medicine Journal.
#Journal of Cardiovascular Medicine#Case Reports in Cardiovascular Medicine#Case Report Journal of Cardiovascular Medicine#case reports in Cardiovascular#Medicine images#Cardiovascular Medicine images
0 notes
Text
I swear to God if you wrote something like this into a political satire like Spitting Image, it’d be called too on-the-nose.
995 notes
·
View notes
Text
Medical Image Journal: Journal of Medical Images publishes medical image articles, images in medical science, imaging in medical journal, imaging in medical science journal, images in clinical medicine journal, images in medical research, imaging in medical research, image case journal etc. Journal allows for the peer-reviewed communication and archiving of Clinical and Medical Research, as well as applications, focused on medical imaging, a field that continues to benefit from technological improvements and yield biomedical advancements in the early detection, diagnostics, and therapy of disease as well as in the understanding of normal conditions.
Journal Homepage: https://www.literaturepublishers.org/
Manuscript Submission
Authors are requested to submit their manuscript by using Online Manuscript Submission Portal:
(or) also invited to submit through the Journal E-mail Id: [email protected]
#medical image articles#images in medical science#imaging in medical journal#imaging in medical science journal#images in clinical medicine journal#images in medical research#imaging in medical research#image case journal
0 notes
Text
a little ink - C.S


summery - y/n is journaling in bed but chris gets bored of his phone and begins to play around with y/n's stationary.
notes - fluff <33333, chris is so boyfriend, i thought the fandom needed more fluff, short
a/n - hey yall, this is an apology gift because ive been bad on being active and writing so enjoy this lil thing i whipped up.
——————————————————————————
——————————————————————————
i stationed myself on my side of the large bed with a little tray table on top of my bare legs. my shorts barely covered up to my mid thigh so the vent near me was absolutely chilling. i begin to go slowly when i'm trying to write a title for my next page, i began to journal when my boyfriends brother and my therapist recommended it to me, despite how simple matt’s was, I thought i could take it up a notch and make it a little cutesy.
my pencil case was jam packed with highlighters, colourful pens and high quality markers, my concentration stays strict on the page in front of me, i tried to keep my penmanship neat while i'm trying to write something in cursive. a warm hand wraps around my ankles as i look down beside me seeing chris look at me with want in his eyes. “hi chris,” i simply say looking at the boy while i put the cap back onto my brush tip marker.
“hi baby,” he looks up at me with a beaming bright smile, he just radiates good energy and love. he drops his phone beside him now playing a song instead of the various audios from tiktok.
his hand sneaks up into my pencil case grabbing a yellow marker from it. he uncaps it and i feel the light pressure of it press down onto my skin, the yellow marker glides along my scar, he continues to draw past it to make a star out of the previously hurt skin. chris knew i was self conscious about my scars, it was a permanent reminder of the pain i went through in highschool.
he didn’t care though. he continued to draw random doodles on my leg, moving on to my arms where more scars lay hurt, he switched out his marker for a different colour the more he explored. little hearts, stars and chris’ signature riddle my legs and arms, i feel his writing getting a bit faster. It looks like a sentence but i couldn’t quite read it.
i stopped what i was doing a long time ago, now just admiring what he was doing. he was so focused on writing his signature on the larger line of a scar i had on my arm using the line from my body to represent the line through the dollar sign he always made whenever he wrote his name.
he does a very magnificent heart beside his name, filling it in still trying to be very soft on my skin as the ink seeps in. he plants a fulfilling kiss onto the scar now covered in orange ink, he looks up at me with a little bit of a knowing look painted on his face. “im sorry, it was only meant to be a little ink but your scars are beautiful, as is the rest of you.” his finger underlines the sentence imprinted on my skin as he reads it out.
“chris i'm gonna cry oh my gosh. you are so cute, you know that?” i saw trying to hold back a sob.
a chuckle escapes his smiley lips “i love you so much y/n” his lips make contact with the star that started the rest of the pseudo tattoos. i wish i could keep this image in my head forever, because this was a moment too precious to let go of.
taglist - @westwiing13 @comet235 @mayhem73
#sturniolo triplets#syn speaks#chris sturniolo#christopher sturniolo#sturniolo fanfic#sturniolo x reader#Spotify
315 notes
·
View notes
Text
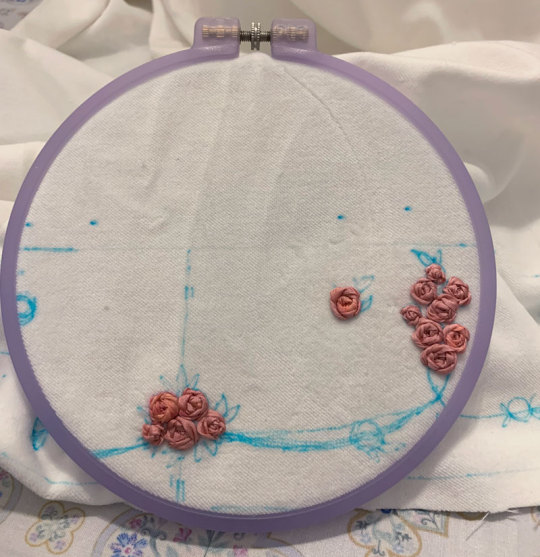
Rose Ribbon Embroidery "Mini" Projects (for BABY NYFW) Part 2: Embroidered Bonnet
I decided semi-last minute to attend BABY's fashion show at NYFW!
BABY had mentioned in their NYFW brand description that their newest collection would be a return to their origins, as well as presenting archival items.
You have to dress to impress for NYFW, right? So of course, I had to pull out all the stops and wear my Rose Ribbon Embroidery.
Also at the last minute, I decided to make a few extra complementing items...
A matching RRE kumya JSK, and a bonnet.




What follows is more of a sew-along/journal rather than a tutorial or guide, mainly for my own memory's sake. But if you enjoy looking at my process (sometimes sloppy), I'm happy!
Also feel free to take a look at the more romantic process video I edited.
Part 1: Kumya JSK
Part 2: Bonnet (you are here)
This post will be my process pictures and notes for the bonnet, as well as a matching mask as a bonus.
I don't believe BABY released matching headwear for Rose Ribbon Embroidery, although I've seen an unknown velveteen headbow with rose lace sold with RRE before.
BABY usually coords RRE with the bunny ear bonnet since Ichigo wears it this way in Kamikaze Girls.



I do own this because I wanted to wear an Ichigo-like outfit at some point, but for this occasion I decided to do something different and make a "matching" embroidered bonnet.
I originally wanted to make a hard bonnet with a very defined brim that could show off the embroidery clearly as I don't really like soft bonnets, but when looking at existing BABY bonnets as a reference, it doesn't look like hard bonnets were a thing back in 2004 (and as it is, BABY rarely releases hard bonnets). So to keep with the oldschool theme, the bonnet is a soft one, although I later make some decisions to make it slightly more structured.
The next decision to make was full bonnet vs half bonnet. The bunny ear bonnet is a full bonnet and I think this is technically more "period accurate", but I am not a fan of how they look like a weird hood from the back so I opted for half (plus, that makes construction and patterning easier for me).
I still used my own bunny ear bonnet as a reference for approximate brim dimensions!
The kumya JSK was a little easier to carelessly sketch out and embroider since I was copying 1:1 from an existing design, but I felt I needed to do at least a bit more careful planning for the embroidery on this. I'm quite bad at creating embroidery designs from scratch, but with the mental image of the rose clusters and swags of vine, as well as referencing the embroidery from the film, I came up with this:

I wanted to emulate the embroidery style of the Momoko's (well, in reality likely the embroidery designer Onoe Megumi--unclear if she did the actual embroidery, but it's likely) embroidery, which I figured wouldn't be too difficult if I was also embroidering by hand.
For material, I am using the same velveteen I used for kumya's JSK. Not my first choice and I actually purchased some thicker looking 100% cotton velvet that I thought would be more similar to the original JSK material, but was worried it wouldn't arrive in time and wanted this project out of the way in case things went wrong/took longer than I expected (it did arrive about a week before the event, but it was totally wrong IRL so I'm glad I just went with this acceptable option). I also bought some more torchon lace, so I used that and another lace from my stash.
The colours of the embroidery in the film also seem to be quite different than BABY's dress. I'm not sure if the pink of the roses has faded over the years, but it has a slight salmon tone whereas the film's roses seem to be more of a pale cool/neutral pink (hard to tell with the yellow tint of the entire film) with some variegation. I love the colour scheme of the film's embroidery, but to keep things coordinated I try to opt for the same colours as the actual dress I have.
I only have white silk ribbon in the width I wanted, so I opted to attempt to dye it to match. Previously I have used alcohol markers to colour the embroidery afterwards, but I find the colour hard to control and it tends to bleed into the fabric. I've also tried colouring the ribbon with the marker before embroidering, but without heat setting the colour transfers onto the fabric as well (and it seems like trying to do so with the amount of ribbon I need would be a waste of ink).
I don't have a lot of experience with it, but since the ribbon is silk, acid dyeing seemed like the way to go.

Very interesting photo of ribbon in pot (the pink ribbon gets eaten up by pinwheel roses much faster than I expected so this is the second batch I had to dye--not ideal as they are definitely slightly different in colour but it's not too noticeable). In total, I think I had to dye 3 batches of ribbon and 4 for the pink ribbon as I just barely ran out near the end, and they are all slightly different colours. Thankfully the undertone is the same so it's difficult to tell unless you are really comparing up close.
I thought I would take this opportunity to use the "peach" acid dye that I bought years ago for another project, but this ended up being a mistake as the colour was totally off (maybe the red dye was too expired). I ended up using my regular fiber reactive procion dyes (with heat/acid), because I have many more colours I could mix together, and that was much better. I really should have done this from the start as I wasted perfectly good silk ribbon by making it too dark/off for my purposes (I ended up overdyeing it in pink so it's a usable colour now, but not for this project).
The silk seems to take on dye extremely fast--even just heating up the dyebath will colour it. In some cases I removed the ribbon before adding any acid at all because I felt the ribbon was already getting too dark.

I managed to get a fairly usable mossy green colour for the leaves and vines, however the pink still ended up being a little off/dark compared to whatever BABY used. It's not too bad here as one strand of ribbon, but when many layers are on top of each other in a rose it seems pretty dark. While not ideal, I think it's still okay, especially considering the embroidery colours used in kumya's JSK match nothing else (many pinks will be going on in this coord).
After dyeing and drying, the ribbon is super wrinkled so I ironed it and wound it on some spare card so it's ready to use.
And now I can start the arduous process of embroidery.
Like before, I mainly use a combination of ordinary ribbon stitches, pinwheel roses, and french knot roses. However, this time I try harder to duplicate, or at least evoke the appearance of the embroidery of the film.
It's interesting how plain and somewhat boring the roses look on their own, especially with this monotone colouring. The varied colours of the film's embroidered roses are lovely, but I decided against it here because the BABY dress has monotone ribbon roses.

The roses definitely seem to just be pinwheel style which is very easy and doable, however I am a bit more confused about the leaves. They look like a number of straight stitches in various lengths and directions that fill in a leaf-like shape. I have no idea if this technique has a name and if there is a proper method for it, because I am a silly beginner who is very uneducated in embroidery.
Anyway I do my best and hopefully I got close enough. Ribbon embroidery is really all about the texture, which is really lovely to look at. Except I have trouble looking at my own work for too long because I start nitpicking all the mistakes I made...

Adding the green and leaves really helps the embroidery come to life.
I took even fewer pictures of the embroidery process than kumya's JSK this time because it's not that interesting. I was definitely getting sick of doing the same pinwheel over and over...

I stupidly decided that aside from embroidering the front of the brim, I also wanted a little bit of embroidery on the back of the brim for interest, as well as on the side.
The designs I drafted out for these two pieces is much simpler, but still, more work....

Almost ready for construction! Hopefully a lot faster with the handwork out of the way.

I iron on some interfacing onto the back brim panel and the bonnet band for slight extra stiffness.
The bottom part of the brim is plain cotton sateen because I was worried that the part that touches the head would get dirtier more quickly it if was velveteen.

I wanted some lace gathered around the brim and an extra velveteen ruffle on the back of the band, so I prepare that now. The lace is gathered with a single gathering thread and sewn down before sandwiching between the two brim panels.

Brim sewn and topstitched (and band is ready for attachment).
The upper flowers ended up a little closer to the top of the band then I intended, but I think it's okay.

Gathering brim and attaching it to band. Because the velvet fabric is so thick, the usual "sew one line of stitching with a wide stitch length" not only made the fabric incredibly difficult to gather, but the thin polyester thread also continually broke when trying to do so. Therefore, I opted for an alternative method I think I'd remember seeing in my sewing machine manual of all things--a zigzag carefully stitched over a central gathering thread. This worked much better, although I probably should have used a thicker/extra strong thread as the central gathering thread because it did break the second time I had to gather the brim due to a mistake.

I also add a bit of lace to the inside of the brim. I think this adds some luxury and frilliness between the head and the bonnet's brim, so I wanted to add a small width. I probably could have used even more of the lace's width since it turned out very subtle when worn. But I still think it adds a small amount of interest to the innermost part of the brim and was worth adding.
Unfortunately here after sewing on both brim parts I realize that I gathered both using an incorrectly marked centre line, so I had to rip it out and do it again ;_;

Next, I can carefully align and pin the bottom of the brim to the bonnet and sew it down. I tack this down by hand because I'm not skilled/accurate enough with a sewing machine to topstitch both sides nicely at once (look closely, and my messy stitching is quite visible...)

I also fold in the raw edges and finish the sides of the brim by hand, leaving some openings for ribbon ties.
At this point I spray almost the whole bonnet with water to disperse and fade my markings. Unfortunately, some of the earlier batches of ribbon that I dyed (Can you tell the variance in the 3 dye batches I needed to do?) were probably not washed well after dying and seem to have bled into the fabric from the water...but hopefully it's not too noticeable.
Next I topstitched all around the brim and attached the ribbon ties.

I bought some double sided velvet ribbon in my last minute supplies shipment and made some bows from it. I think the material is a little thick and petersham would have worked alright as well, but the consistent velvet material feels more luxurious, doesn't it? I also think as an added benefit (?) the ribbon being plush and double sided made the bows more puffy looking.
I add some clips to the sides and a toupee clip to the top for security. I opted for a toupee clips because I think it's really the way to go if you don't want the head item to move at all, no matter how thin or slippery your hair.

Finished.
Bonus 1: rose accent pin

I was in a bit of a rush at this point as it was near the end of the week coming up to the show, so I didn't take any photos of the process here but the technique and templates I used were identical to my handmade faux rose rosettes I made for UM (and the bonus corsages). I have a post with all the details of this sitting in my drafts that I will post eventually, and I will update this post when that happens.
The brooch was just meant to add a bit of 3D faux flower accent to the bonnet, bringing in the rose motif even more. Partially inspired by the faux flowers BABY adds to their bonnets sometimes, like on Milk Tea Doll.
The fabric was "custom dyed" with the same fiber reactive dye I used for the silk. The fabric was further starched, cut out by hand, and shaped with flower iron tools before gluing together.


Bonus 2: matching embroidered mask

I wasn't sure about whether or not I wanted to wear a matching mask, but decided to do so for situations when I would want my face at least half-covered in public. I didn't really expect to be visible in fashion show pictures as someone in the back, but just in case. (I think this decision was worth it, although my makeup transferred all over the thing and in most pictures my face was even more unflattering. eh well)

I forgot to take a lot of pictures of my process for this, but it's very uninteresting and not dissimilar from every other mask sewalong from 2020. I draft out a design similar to the bonnet motifs on both of my mask panels (cotton sateen), and embroider.
I should have embroidered closer to the centre of the mask because when worn the embroidery is not very visible/covered by my hair at the sides. What can I do since the panels were already cut though...oh well!
The lining material is some Japanese CLEANSE Ex fabric I had bought previously to make masks during the pandemic. It's supposed to be antibacterial and antiviral, as well as washable, but I have no idea how well supported those claims are.
Sew together normally on both upper and lower sides, turn inside out, add a channel for nose wire and side channels for elastic.
I also have some mask elastic on hand so I use that.
And the finished outfit again with all my items~

Thank you for reading! If you ever feel inspired to take up a similar project, such as the kumya JSK, I'd love to see it!
222 notes
·
View notes
Text

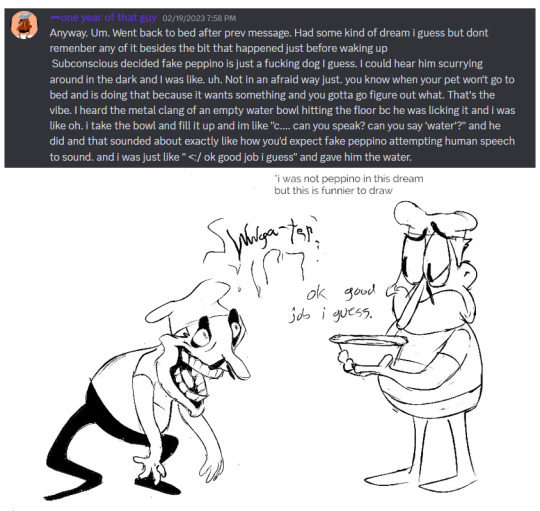


a year!!! as of today i have now been drawing these funny little pizza freaks, to the exclusion of almost everything else, for!!! an entire year!!! i wanted to do a nice group shot/lineup of everybody to compare to when i first started trying to draw them because oh boy were they bad. i never even posted most of them anywhere because they were so bad. but im posting them here, now, to see how everything's changed/evolved.
this is probably the hardest time i've ever had trying to figure out how to work with a style, but we got there eventually; i'm pretty happy with the handle i've got on everybody now...dont let ur memes be dreams. lots of unimportant journaling and idle thoughts abt it below.
older pics
the first one is the VERY first time i drew them, before i thought i was going to actually have any interest in drawing them [lmao]; it was just the one isolated image, for my friendserver, to illustrate the funney message, so there was no attempt to make it Good or actually understand anything going on w/ the designs or style.
second is the original run of practices sketches to start trying to figure them out for real; done after i started having ideas for the comics and such and realized oh god maybe i am actually gonna draw fanart for this. [again, lol, and lmao.]
third one is the first pt art thing i posted on here. there were a couple weeks of sprite studies between this one and the previous image. the one on the top right wasn't part of that post i just threw it on as space filler; i'd intended to shift to doing Sprite Redraws But Stylized to explore tings more, but that was the only one i did. ¯\_(ツ)_/¯
individual characters
peppino: by far the hardest dear god. bro what ARE your shapes how DOES your face work. jesus christ. everything i have trouble with this style for, peppino has it in excess. i draw in polygons! i need consistency! and that is the last thing this kind of style is concerned with. they are made of squarshy clay and i do not understand how to mold them. i was really hoping trying to learn this game's style would GIVE me that kind of flexibility for fun exaggerated facial expression but i don't think much came of it in the end 😔. anyway on the bright side all this means once i got peppino figured out a little bit everybody else clicked way easier.
fake peppino: honestly i never did anything with him on purpose except for how his eyes work + the perma-smile thing. i figured ok hes supposed to look weird and off model so whatever happens with him happens. and it did. and it kept happening. it is still, in fact, happening.
noise/ette: somehow, for every bit that peppino was the least natural thing i've ever tried, these two worked pretty much right off the bat. i still don't understand it, seeing as pretty much all the things at play for peppino are also at work for them. i think the new sketches are actually a little worse than older ones but not enough that i care.
gustavo: really funny bc i drew him on model twice and just went 'okay, cool nice, easy, um. he doesn't have any fucking legs?' fortunately he was the only one i had a strong idea for how to stylize him [square] and it worked exactly as i was hoping so wahoo.
brick: is an animal and therefore 5000x easier and more natural for me to draw/stylize than anything else in the cast. that is Just a rat bro. i can draw a rat.
gerome: i think the funniest one here. the most drastic and least necessary change imo. i was gonna have him be really small at first, like smaller than the noises, but then i just... didn't. he's just peppino-sized now. also i gave him like. actual human facial structure, which is funny bc in most cases i'd do anything to avoid, but it works well for his being A Rock to give him some angles and definition like that+ to differentiate his vibe from the rest of the cast who are all very squishy. also since he is essentially Just A Head it's good to emphasize that too ig.
john: i only drew john a couple times but he gets to be here because i like him. and because most of the stuff i applied to gerome was readily applicable to john, though i did try to keep him a little more uncanny because he is a Huge And Lanky Freak. i hate that he is barefoot btw but idk how to make his color balance look right with shoes.
pizzahead: i did not want to put him on here honestly but i Have drawn him a handful of times and more importantly i didn't know what i was gonna do with john's pose if i didn't have him there to be glared at. the only thing that's different with him is giving him wider-bottomed pants, which i got from when i tried to draw these guys in clone high style [i never posted that one either][i will eventually]
snick: he gets to be here because 1. he's like 6 lines 2. i like him and 3. ive scribbled him a few times offhand and it went pretty well
misc
there are some guys missing because those are guys i didn't draw enough [or at all] to have gotten comfortable with them. sorry
i would have Liked to shade these but for the time being i have accepted that my grasp of light/shadow has decayed to the point im not going to be happy with anything i try there, so For Now i am working on my presentation with flats i guess. gerome has a shadow only because he's shaded like that ingame and looks naked without it
anyway if you are still reading [hi?] i get to shamelessly plug now. i'm over the hill of my pizza run now, and while i still have plenty of things i want to make here, most of the bigger more in-depth ones have passed. pizza tower was the first thing in THREE YEARS to get me out of my oc groove to doing fanart, and once i am done with my ideas here i will be going right back to it. if you like my art or how i write characters/interactions you should check out my oc/webcomic blog @jamverse . i can't promise people who like pizza stuff will be terribly into my designs, but i can guarantee i treat my guys with the exact same sort of tone i handle the pt guys with. and hell, i've mentioned it a few times before, but like 70% of my characterization for fake pep is just copied off one of my characters, so if u are going to miss him... he will still be there in spirit >;p
and if you dont care about any of that and are still reading thank you anyway. actually making these comics + seeing how shockingly well-received they've been has done a lot for my confidence, and for seeing that my kind of stuff IS something people enjoy :')
#pizza tower#peppino spaghetti#fake peppino#gustavo and brick#the noise#noisette#pizzahead#arting#pizzaposting
178 notes
·
View notes
Text
Sleepless nights
╰⇢ 9. Good shit
Warnings: just yuta being in denial again?? (no surprise tho)
note: THERE’S WRITING AFTER THE FIRST 10 IMAGES you don’t wanna miss it :] also thank you for all the support?! i never thought there would be many people who would want to read this series. but i’m thankful for all of you <3




“Alright. So how about we all split up into pairs while we go around the mall?” Nobara took a sip of her drink as you all began leaving the food court.
“That would probably be easier.” Yuta nodded.
“But there’s seven of us.” You added.
“You guys will just have to be in a group of three.” Maki slung her arm over Nobara’s shoulder, giving a sly grin to the black haired boy.
“I don’t think-” Yuta tried to protest.
“Perfect! Inumaki, you’ll come with us!” You interjected, taking a hold of the boy’s hand.
Maki watched with an amused look as Yuta glared at her. He knew exactly what she was trying to do, but it’s not like he could do anything about it.
“Let’s go then!” You began dragging the two boys away.
The three of you then began strolling through the mall, pointing at windows and looking inside the stores. You did most of the dragging, pulling Yuta and Inumaki into whatever store caught your eye.


“Look at this!” You smack Yuta’s arm to get his attention. The three of you were currently stationed at the front counter of an antique shop, looking at all the various trinkets that were displayed behind the glass barrier.
In this case, you were focused in on a simple silver ring. The obviously well-loved wedding band sat in a velvet box, practically begging for attention. You couldn’t help but stare at it.
Small engravings ran through the material, creating intricate designs across the entire surface. A truly beautiful piece of jewelry. It almost drew you in, in some way. Like a magnet.
“I’m almost scared to ask how much that is.” Yuta chuckled.
“It can’t be as bad as you think.” You smile. “How much is this ring?” You ask the old lady behind the counter, pointing at the silver ring.
“That one? It’s 50 dollars. But for a young one like yourself, I’ll let you have it for 40.” She smiled.
As much as you appreciated the kindness, you politely declined. Not because you felt bad, but because you simply couldn’t afford it. It was times like this when you really wished you had a job.
“I can pay for it.” Yuta offered.
“No way! I’d actually feel bad if you payed for this. 40 bucks is a lot even for you!” You immediately shut him down.
It’s true, 40 dollars is a lot for broke high school students, even if they have jobs. You couldn’t allow Yuta to spend that kind of money on you.
“You sure? You’ve been eyeing that ring for a solid 15 minutes while we looked around the store.”
“Positive.” You gave the ring one more glance before forcing yourself to leave the store. “Let’s go. Any more staring and I’ll regret not having enough money.”
“Alright, I just want to look at some of those old journals before we go, just wait outside for me.” Yuta shooed you away.
You roll your eyes with a smile, turning your attention to Inumaki as the two of you walked out. “I bet he’s gonna take a long time.”
The two of you found a bench to wait for Yuta, sitting down side by side, the two of you sat in silence. It wasn’t long before Inumaki pulled out his phone, swiping to a game and started playing.
“What are you playing?” You lean over and watch the boy tap away on his screen. He angled his phone to you, displaying a familiar game layout. “Oh! You play Genshin?”
The boy gives you a simple not. It was obvious he wasn’t much of a talker, but that didn’t bother you.
“That’s cool. I don’t really play but I really like watching this one streamer play.” You started going on about the game. “If I’m annoying you, just tell me, okay?”
“You’re not bothering me. Keep going.” He mumbled.
It was the first time you ever heard him actually speak to you. His voice was low, lower than Yuta’s at least. A little husky from the lack of use. But soft at the same time.
You couldn’t help but smile. It was like the next step in your already growing friendship. You continued to watch the boy play, leaning on his shoulder as time went on.
Masterlist | Next
fun facts:
— even though she’s all for the chaos, maki does genuinely want yuta to be happy and confess his feelings
— inumaki has his phone always on do not disturb because of the amount of notifications he gets
— the original monster energy drink is yuta’s favourite because he rarely drinks them (you try to get him to try different flavours but he just doesn’t like them)
taglist:
@sur-i-ki @aespaforlifersyall @camilo-uwu @butterflyqueen234 @shinsukeee @tanchosanke @emii4evr @lees-chaotic-brain @you-always-made-me-blush @jayathelostdragon @chilichopsticks @polarbvnny @instantmusico @sad-darksoul @hellyyy06 @rosieandthethorns @zellwa @iluv-ace @h3xi2g0n3 @morgyyyyyyy @bellaabee082
Bold means I for some reason can’t tag you! I don’t know why :[
#jujutsu kaisen#jujutsu kaisen x reader#jujutsu kaisen imagines#jujutsu kaisen smau#jjk#jjk x reader#jjk imagines#jjk smau#yuta okkotsu#okkotsu yuuta#yuta x reader#okkotsu x reader#toge inumaki#inumaki toge#toge x reader#inumaki x reader#yuta x you#inumaki x you#smau#modern au#strawberri-elixir
268 notes
·
View notes
Text
We have a serious problem
Michael Laidlaw, MD: I'm a board-certified endocrinologist, practicing in private practice for the last 16 years. I've been studying and publishing in this area for the last 5 years, including peer reviewed journals such as Journal of of Clinical Endocrinology and Metabolism, and others. I also have a patient who is a detransitioner.
I think it's important to note that studies are shown that desistance, or growing out of this condition, of children by adulthood is very high. It's some 50-98%.
I want to be sure before I give someone a very powerful hormone like Insulin that they in fact have diabetes.
What about cancer? Before we give any powerful agents such as chemotherapeutics or surgeries, we certainly want to have physical evidence of this problem, such as biopsies or imaging.
Now, the gender affirmative therapy treatment proposed by WPATH gives very powerful hormones and surgeries on what basis? Where can we find the gender identity to be certain that these children will not desist by adulthood? Can we use imaging of the brain or blood tests, genetic testing, are there other biomarkers to ensure that we are correct? There is no such thing.
Julia Mason, MD: The Endocrine Society put out guidelines in 2017, and they were very careful in the guidelines. One, to point out that the evidence was of low and very low quality. And they also said in the guidelines that they have no idea how you identify which kids are trans and require this treatment.
And then the American Academy of Pediatrics the next year just leapt into that void and said, oh, oh, we'll tell you how you know which kids. You ask them.
Prior to 2018 I had maybe one trans patient. But then there was another one. And another one. And another one.
It wasn't until later that I started asking questions like, wait, every single kid I send to the gender clinic gets put on puberty blockers or cross-sex hormones. Just, it was happening immediately.
Patrick Hunter, MD: This affirmative model of care has spread wildly in the last 8 years. Now we have objective, unbiased systematic reviews. These systematic reviews tell us the evidence for youth transition is poor quality, and with very low certainty for benefit.
In JAMA Pediatrics, there was a study reported from Northwestern University in Chicago. Patients ranged in age from 13 to 24 years. The authors concluded that mastectomy was beneficial and should not be delayed in youth. What lead them to that conclusion? The finding that 3 months after surgery, the 36 patients were happy with their flat chests. They lost 9% of their surgical cases to follow-up. Nine percent. In 3 months.
It is absurd, meaningless to draw any conclusions after 3 months.
This paper is indicative of the quality of research we have in this field, published in our most prestigious journals.
We have a serious problem.
#gender ideology#queer theory#medical transition#desistance#detrans#sex trait modification#genderwang#detransition#trans identity#cross sex hormones#wrong sex hormones#puberty blockers#poor research#medical malpractice#medical scandal#medical corruption#endocrinology#low quality#ideological capture#ideological corruption#religion is a mental illness
912 notes
·
View notes
Last Seen Blogs

noithatcodientcd-blog
Nội Thất Cổ Điển Tân Cổ Điển

daisyinagunbarrel
tuntematon

edkra
Ed Kra

borderlinegirly
Borderline 🖤🤍

thecrusadercomrade
It ain't much, but it's honest work