#abortion services
Text
ABORTION AND LGBTQ+ INDIVIDUALS: UNIQUE CONSIDERATIONS AND SUPPORT

Diverse Challenges: LGBTQ+ individuals may face unique abortion challenges due to societal attitudes, discrimination, and limited healthcare understanding.
Inclusive Healthcare Access: Crucial for LGBTQ+ individuals, inclusive healthcare should address specific needs like gender-affirming care during abortion.
Legal Protections Awareness: Vital for a safe experience, LGBTQ+ individuals must understand their rights and protections during the abortion process.
Specialized Counseling: LGBTQ+ individuals benefit from counseling services acknowledging their unique experiences and concerns.
Community Guidance: Use LGBTQ+ community resources for support during abortion. Community organizations provide valuable information and connections.
Affirming Language: Healthcare providers should use inclusive language for a supportive environment during abortion services for LGBTQ+ individuals.
Cultural Competency Training: Healthcare professionals need training to provide respectful care, addressing LGBTQ+ individuals' specific needs during abortion.
Mental Health Recognition: Recognize potential mental health impacts for LGBTQ+ individuals during abortion, offering essential support for additional stressors.
Privacy Assurance: Crucial for LGBTQ+ individuals, ensuring privacy and confidentiality addresses concerns about disclosing sexual orientation or gender identity.
Advocacy and Awareness: Vital for creating supportive environments, advocating for LGBTQ+ inclusive healthcare policies, and raising awareness about unique considerations during abortion.
#abortion services#telehealth abortion services california#ABORTION AND LGBTQ+#abortion#hersmartchoice
6 notes
·
View notes
Text
Microsoft, Amazon, Meta, Apple, Google, JP Morgan Chase and Dicks Sporting Goods will all pay for abortion services for their employees
https://www.rawstory.com/big-tech-companies-will-cover-travel-expenses-for-employees-medical-procedures-including-abortion/
7 notes
·
View notes
Text
Since working at Planned Parenthood I’ve definitely learned some new things, especially regarding abortion.
1. No governmental funding goes towards covering abortion costs. None. Zero. I don’t know why people think that. Donations are what primarily cover those services, but depending on what a persons insurance is, it’s still about $775 for the medical (pill) or surgical option. This might vary by location (and the amount of donations they’ve received) or if your insurance defection or has been met.
At the one I work at, any sort of Medicaid combo (state insurance) covers all services. So if someone has state insurance they could get an abortion at no cost. I feel like this is why people think that the government is funding abortion services (although who the fuck cares if they were tbh).
2. We cannot offer abortion services if someone is less than 6 weeks pregnant. This is also what’s so infuriating about the bills/laws that are banning abortions past 6 weeks - not everyone realizes they’re even pregnant at that time and Planned Parenthood wouldn’t even be able to perform an abortion before then.
The medication abortion (the pill) can be used anywhere between 6-10 weeks. The surgical can be done between 6-13 weeks and 6 days. Anything after 13 weeks we have to refer the person out to a different place. We do not perform abortions after 13 weeks.
I am not a medical professional, but I welcome any questions anyone has regarding Planned Parenthood and the services we offer.
0 notes
Text
PSA
1 note
·
View note
Text
on March 14th 2023, a Polish abortion activist Justyna Wydrzyńska was sentenced to eight months of community service for helping a woman in an abusive relationship access abortion pills
Poland has one of the strictest abortion laws in Europe.
if you can, please consider donating to ADT, the organisation that helps people in Poland access abortion!
edit: i see this post got reblogged into the terf teritory. ADT is trans friendly. please just donate and be quiet <3
#luckily they still can appeal and it's better than jail still but like.#it's so stupid that so much time is wasted on those absurd trials#i know that community service doesn't sound that bad comparing to some other things happening around the world#but still at first she was told she could face up to 3 years in jail#idk those women are heros and make me feel much more safer and less stressed living in Poland#because I know if I ever needed an abortion they would be there to help me#and also 5 dollars is almost an equivalent of a minimum hourly wage in Poland#polish currency is weaker so even 2 dollars count a lot!#and the judge was a woman! same as the leader of the constitutional tribunal that made abortion more illegal#feminism#abortion#poland#human rights#reproductive rights
2K notes
·
View notes
Text
One time I was at work at a place that had a copy center, etc. I was making some copies for a little pig faced white lady for her lil' church group event or whatever. Now, I don't remember which church it was, as my city had many, but what I do remember is that it was a white church. I remember because that's important for context of this conversation with this also white customer.
She begins the conversation. I actually am multitasking multiple jobs and didn't intend to talk to her. She was a regular and she knew how this worked. But, she starts this conversation inviting me to the event. I kindly decline, mind you, this was during one of my church phases. Even when I was "in church," city's pretty segregated and the few times I'd been to one of their churches, it wasn't for me.
Then, she tells me that the event is specifically designed to stop abortions. And I'm a different person at the time. I'm a person with poor views on this matter from being youngish and being religiously conditioned + by this time I've had, I believe 2 miscarriages, but I'm not positive.
So, I guess with that, I say either, "Oh, that's nice" or something, idk. And this woman says to me, somebody she only knows from making copies of fliers and ringing her up when done...
"You really should get involved in these efforts. You would not believe how many young Black women are there, denying beautiful Black babies the right to live." And now, I'm done with customer service, because Idek if I replied to her. But, I look at these damn fliers and they are the white saviorest fliers about Black abortion that I have ever seen.
I'm ringing this bitch up, and she's talking about what her church teaches about life before the womb, circa the book of Jeremiah, etc. I say, "Yeah, they teach the Bible in my church too," and I told her the total.
She reaches for her checkbook, and instead of writing the check starts asking ME, the lady from the copy center/cashier/asst manager of a local supplies store, if I have ever been pregnant or if I have kids. I say, since we so cozy and I actually want her uncomfortable, "No kids, just miscarriages." And smile.
Do you know this heffa, without missing a beat, tells me, "More of a reason for you to care about these Black babies!"
I repeat the total. She starts finally writing her check and my manager walks up. Fellow Black woman, and the homie at work. "Tenesha, I need you to go cut soem butcher paper in art supplies." I go.
After the woman leave, Michelle says to me, "Now, I don't know WHAT that woman was saying to you, but I know that look on your face that you had and you looked like you was gettin ready to get her. So, I stepped in."
There really is no message or purpose or nothing of me telling this story. It just popped into my mind. But, for what it's worth, this was a perfectly normal conversation for this person to have. Some white lady at a church that was predominantly white, if not all white, with her save the Black babies from them abortions fliers and chit-chat. With a Black woman at least 20 years younger than her, I'm guessing from looks. Tbh, I can never tell how old they are because they... you know they age differently. And to have this conversation while I, apparently look so disgruntled my manager sent me away from the transaction?
They're just a trip. That's the point, I guess.
14 notes
·
View notes
Text
.
#just saw a post that was like 'if you have religious or moral objections that stop you from providing certain types of medical care maybe#you shouldn't work in healthcare' (paraphrased) and...#what a way to look at the world tbh#like. they're talking about me i think - i am a conscientious objector when it comes to euthanasia#(which granted has come up exactly twice and both cases in a theoretical capacity only this is not a frequent request to me)#and... i am also a good doctor#last week i told someone that her weight doesn't matter to her health with receipts to prove it and she cried#no one had ever told her that before#and that was something that came from me specifically. that was something i would not trust all of the GPs in my practice - a practice of#excellent and compassionate GPs! - to say#i am verifiably doing good in my job that is coming from specifically who i am as a person#i cannot put that down when it comes to issues i care deeply about#fundamentally the fact that i cannot put it down is what makes me a good doctor#i think that's what i'm trying to get at#the reason that i do well by my patients is that i practice out of my values and my ethics#if i did not stand on that core i would not stand at all#so you can't have it both ways. you can't have engaged and active and compassionate healthcare providers without sometimes those engaged an#active providers having things they do not feel comfortable doing#and it is to everyone's service if they are up front about it and do not try to hide (i am suspicious of people who try to hide this)#i am literally figuring this all out as i type hence the v long tag ramble and also being nowhere near the post that started this train#(honestly in med school we talked so much about ethics as like. abortion! euthanasia! trans rights! and the ethics in practice is the littl#things. do you apologise when you mess up. how do you manage a consult with your patient with paranoid dementia and her child in the same#room at one time - or one by one bc that's fraught too. (that one's on top i had one of those today.) how do you act with grace when#you're a bit stressed and your patient is a bit stressed and the nurse wants to add five more things to your book. the day to day ethics is#SUCH a bigger thing when you come to actual practice.)#this is obviously entirely about me and leans on the fact that i largely do think i am doing a good job i am really feeling my own way#to a Thought. but i think to a certain extent it is generalisable
9 notes
·
View notes
Text
Access Free Abortion Pills | Her Smart Choice
Her Smart Choice East Los Angeles Women’s Health Center provides safe and accessible abortion services, including free abortion pills. We offer compassionate and confidential care to empower women to make informed decisions about their reproductive health. for more information, visit our website!

#hersmartchoice#womenshealth#freeabortionpills#abortion services#healthcaredecisions#losangeles#healthcare
0 notes
Text
Planned Parenthood Action Fund emphasized that abortion is still legal in most of the country and directed people who need care to abortionfinder.org, a website that lists abortion service providers.
6 notes
·
View notes
Text
This is Idaho
And this is also Idaho
And so is this
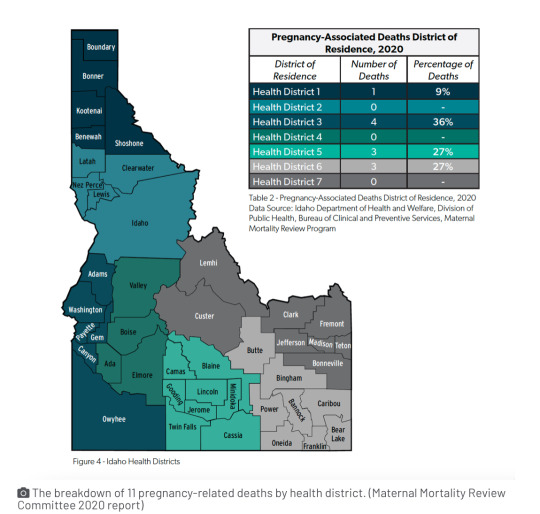
#Idaho#USA#reproductive rights#access to reproductive resources#Abortion access#maternal care#labor and delivery services#Maternal death rates
49 notes
·
View notes
Text

#us politics#2022#us supreme court#scotus#dobbs v. jackson women’s health organization#roe v. wade#planned parenthood v. casey#taxes#tax returns#irs#internal revenue service#us government#abortions#abortion bans#income tax returns#fetal viability#personhood#reproductive health#reproductive rights
344 notes
·
View notes
Text
A ‘twisted’ experience: How KY’s abortion bans are depriving pregnant patients of health care
BY ALEX ACQUISTO
On the way to her 20 week ultrasound, Amy English texted her family group chat inviting guesses on her baby’s biological sex.
“Baby boy English muffin!” her father in-in-law texted.
“I thought boy at first but I’m thinking girl now,” her sister-in-law said. “My official guess is a girl :).”
It was December 28. Earlier that morning, Amy, 31, her husband David, and their 20-month-old daughter Annie had celebrated a belated Christmas at their house in Louisville with family visiting from out of state.
Amy and David had planned this pregnancy, and it was, in a way, perfectly timed. Their baby’s due date was five days after Annie’s birthday. Her children would be two years apart almost exactly to the day — a reality Amy was “ecstatic about.”
Sitting in a fluorescent-lit room inside Baptist Health Louisville, Amy looked for familiar shapes on the screen as an ultrasound tech probed her abdomen. Familiar with radiology in her career as a physical therapist, she has a baseline understanding of how to read ultrasounds: gray shapes usually indicate fluid, and bone shows up as white.
Amy remembers seeing her baby’s arms, legs and the curve of its back. But there was no recognizable outline where the skull should be.
“I couldn’t see the top of my baby’s head,” Amy said in an interview with the Herald-Leader. “I kept waiting for the tech to move the probe in a way where we could see what we should be seeing. I could tell she was searching for it, too.”
Amy had also learned in school about anencephaly, a severe fetal birth defect impacting the brain and skull. A lack of folic acid early in pregnancy increases the likelihood of this happening. This possibility flashed in her mind but she quickly batted it down; she’d been taking her prenatal vitamins, rich in folic acid, for months even before discovering she was pregnant.
The tech paused, then spoke.
“What we’re looking for here is an outline of the baby’s head, and right now I’m not really seeing that,” the woman explained before calling in Amy’s longtime OBGYN.
Over the next few minutes, Amy remembers the room blurring as she heard her doctor use the word “acrania,” which is when a fetus matures through pregnancy without ever developing parts of its skull. It can spur anencephaly, when the brain, too, is underdeveloped and partially missing. Pregnancies with either of these conditions are nonviable.
Amy’s baby, which they learned was a boy, had both. He would not survive into childhood, likely not beyond a few minutes after birth.
This, alone, was devastating news. Her dismay was compounded the next day when she learned that terminating her nonviable pregnancy, even by way of an early induction — a commonplace and provider-recommended method of treatment for such a diagnosis — couldn’t happen.
Even though Amy’s baby would never survive outside her womb, the pregnancy still had a fetal heartbeat — a technicality, considering the diagnosis. Coupled with the lack of immediate threat to her health, her doctors explained they couldn’t induce labor, much less give her an abortion. Kentucky laws forbade it, they said.
“I don’t know what was more shocking: to find out the baby had anencephaly, or that I would have to go out of state to get this care,” Amy said.
Kentucky’s abortion bans do not legally permit the standard of care treatment for a nonviable pregnancy like Amy’s. As a result, doctors must refer patients needing otherwise medically-recommended terminations out of state in droves, along with people desiring elective abortions, according to interviews with seven providers across four hospital systems. Providers who terminate pregnancies in violation of the trigger law can be charged with a felony in Kentucky.
Though this scenario is increasingly common statewide, it’s one arbiters of the state’s laws have yet to remedy, and one lawmakers are not publicly working to resolve.
Kentucky’s trigger law, enacted in late June 2022, criminalizes abortion except to prevent a “substantial risk of death,” or to “prevent the serious, permanent impairment of a life-sustaining organ of a pregnant woman.” The fetal heartbeat law also includes these exceptions but otherwise bans abortion except in a “medical emergency” once fetal cardiac activity begins, usually around six weeks.
Any time a pregnancy is terminated, each law requires a provider to document in writing why it was necessary to, in the case of the six-week ban, “prevent the death of the pregnant woman or to prevent a serious risk of the substantial and irreversible impairment of a major bodily function of the pregnant woman.”
The law permits the Cabinet for Health and Family Services to audit any licensed health care facility to make sure its abortion reporting requirements are “in compliance” with the law.
Both bans allow physicians to use their “reasonable medical judgment” when deciding whether pregnancy terminations are medically necessary. But providers interviewed for this story said that guidance is antithetical with the rest of the law’s limits, which only permit terminations in medical emergencies. There are no exceptions for fetal anomalies, or for the gamut of conditions that may make a pregnancy nonviable but don’t pose an immediate or emergent health risk to a pregnant person.
Moreover, the lack of uniform guidance from the state on what’s considered an emergency means definitions across hospitals sometimes vary, the Herald-Leader found. This has created a legal thicket for health care institutions. As a result, the final say on some critical medical decisions affecting pregnant patients is falling not to medical experts, but to hospital attorneys and administrators, who are worried about legality, liability and reputation.
The Herald-Leader asked the University of Kentucky, UofL Health and Baptist Health for insight into how their respective risk management teams and providers are navigating the laws. None responded to multiple questions about respective protocols for deciding when terminations are legally defensible, or how risk management teams, administrators and providers go about deciding.
“Clinicians have a responsibility to provide compassionate, evidence-based care and counsel to their patients, and also comply with the law,” Baptist said in a statement.
“UofL Health is committed to provide comprehensive health care to all its patients and their families,” UofL said in a statement. “In the case of a nonviable pregnancy that poses a health risk to the mother, we explain options for care while complying with all state and federal laws.”
“Although we cannot discuss when or how our legal counsel gives advice,” UK HealthCare said, “in Kentucky, state law prohibits the University’s physicians and staff from performing abortions except when the mother’s life is in danger. In the case of a nonviable pregnancy, our health care staff work with patients to determine the best course of care for the patient that is consistent with state and federal law.”
‘WE COULD NOT PROVIDE THIS SERVICE HERE’
The morning after Amy learned her baby likely had a fatal birth defect, the diagnosis was confirmed at a second ultrasound with a high-risk specialist. The buoyancy and excitement of the prior day was replaced with dread and grief. Amy remembers the quietness of the room during the second ultrasound, the hollow clicking of the keyboard keys and the intermittent clicking of the computer mouse.
Baptist Health refused to make Amy’s doctor available for an interview. But their conversation was outlined in Amy’s medical records, which were provided to the Herald-Leader.
“I discussed this finding with the patient and offered my sincerest condolences — that this was not compatible with life and that I am so sorry she and her husband are in this situation,” the doctor wrote in her notes. “She was understandably tearful.”
Amy listened as her provider explained her two options: Amy could carry her son to term and deliver him via C-section. He would immediately be taken to palliative care, where he would live a few minutes, maybe hours. Grief counselors would be on standby.
Her second option was to terminate the pregnancy early by way of an abortion or preterm induction. “Choosing not to continue the pregnancy: we discussed that this is also a loving choice for a baby that will certainly not survive,” her doctor wrote.
Pre-trigger law, termination under these circumstances would’ve happened in a hospital, and Amy’s health insurance likely would’ve covered it.
“No part of me wanted to be pregnant anymore,” Amy said. “Every flutter and kick he gave felt like a literal gut punch reminder that I would never get to take him home.”
Strangers were already approaching her at the grocery to ask to touch her stomach. Her patients at work often asked how far along she was. It seemed emotionally unthinkable to continue subjecting herself to a life where, at any moment, she would be forced to repeat that her growing body was nurturing a baby that wouldn’t live, she said.
Termination was what Amy wanted. She erupted into sobs when her doctor told her that under her current circumstances (her life wasn’t immediately threatened, and there was still a fetal heartbeat) it wasn’t an option.
“We discussed that due to our current Kentucky laws, we could not provide this service here,” her doctor wrote in her records.
“I’m sorry, I’m sorry, I’m so sorry,” Amy remembers the specialist saying.
She gave Amy a list of hospitals and clinics in surrounding states that might be able to terminate her pregnancy. Her doctor recommended calling Northwestern Memorial Hospital in Chicago, or another clinic in Illinois, where abortion is widely available.
“Am I just supposed to Google the number, call the front desk and ask, ‘How do I get an abortion at your hospital?’” Amy remembered thinking.
Over the next few days, she, her husband and sister-in-law cold-called a handful of clinics to request a dilation and evacuation abortion, common in the second trimester. But a combination of abortion restrictions in Indiana and Ohio, including gestational limits on when abortion is legal — Amy was 21 weeks along at this point — left her with few options.
Then, Amy’s sister, a nurse anesthetist at Northwestern Medicine Kishwaukee Hospital in Dekalb, west of Chicago, stepped in. Her hospital lacked the equipment for a D&E, but they agreed to induce Amy.
On January 4, after driving close to 400 miles, Amy was induced and gave birth to a son she and her husband named Solomon Matthew. He didn’t cry. His heart beat for about two minutes before it stopped.
‘NOT KNOWING WHAT TO DO’
The Republican-led General Assembly has made no moves to amend or further clarify either abortion ban since both took effect seven months ago, even though the combined impact has harmed patients, doctors have told lawmakers.
The Kentucky Supreme Court still hasn’t issued a preliminary opinion on whether either law infringes on a person’s constitutional right to bodily autonomy and self-determination. Deciding so would temporarily block one or both bans from being enforced. Convened for a regular session through March, the Republican supermajority has yet to file any bills related to reproductive health care access and likely won’t until the high court weighs in.
In the meantime, there’s disagreement about whether or not either ban infringes on providers’ ability to dole out the standard level of care to pregnant patients.
Kentucky Supreme Court Justice Michelle Keller and former Deputy Chief Justice Lisabeth Hughes raised this point during November oral arguments in the pending court case from the state’s two outpatient abortion clinics challenging the constitutionality of both laws.
The trigger law “doesn’t recognize an exception for women who are under the care of a physician who tells them that the standard of care would be to terminate the pregnancy,” Hughes told Solicitor General Matt Kuhn, arguing on behalf of the Attorney General’s office.
As a result, “What’s really happening is physicians in (hospitals) all over the commonwealth are calling the risk managers and attorneys for the hospitals not knowing what to do,” Keller added. “You’re obfuscating what this trigger statute says. There isn’t a strict life of the mother exception.”
The law’s proponents, including Republican Attorney General Daniel Cameron, have cited the provision in the law that allows for use of “reasonable medical judgment” as protecting doctors’ autonomy, and that any challenge to that fact is overblown.
“The law has an explicit health exception, (which) depends on a ‘reasonable medical judgment’ from physicians,” Kuhn told Kentucky Supreme Court Justices that day. There’s been “a lot of misinformation” suggesting the law doesn’t adequately protect a pregnant person’s health, he said, citing two advisories Cameron’s office has issued since both measures took effect. Both clarify that in vitro fertilization, and abortions as treatment of miscarriages, preeclampsia and ectopic pregnancies don’t violate the law.
As for the host of other conditions not mentioned, “we are continuing to work with Kentucky doctors giving guidance on that,” Kuhn said.
But no written evidence of that guidance appears to exist. In response to an open records request from the Herald-Leader, Cameron’s office said this week it had no written or electronic records of communication between the Attorney General’s office and licensed health care facilities or providers regarding the trigger law or six week ban.
‘AN UNNECESSARY PHYSICAL AND PSYCHOLOGICAL RISK’
It was mid June when Leah Martin, 35, discovered she was pregnant with her second child.
Pregnancy at ages 35 and above is considered geriatric. Aware that her age meant she faced a heightened risk, she opted for genetic testing early on to gauge any abnormalities.
Her first ultrasound didn’t raise any alarm. At just over nine weeks, Leah took a prenatal genetic test. The results a week later showed “low fetal fractal numbers,” she said in an interview.
That result, her OBGYN told her, could mean there hadn’t been enough material collected to show a clearer result. It could also signal an abnormality.
Leah, wanting to be judicious, got a more exact genetic test just before 12 weeks. She quickly learned her fetus had triploidy, a rare condition that causes the development of 69 chromosomes per cell instead of the regular 46. It causes not only severe physical deformities, but triploidy stunts development of crucial organs, like the lungs and heart. It means a fetus, if it even survives to birth, will likely not live beyond a few days.
What’s more, Leah was also diagnosed with a partial molar pregnancy, which causes atypical cells to grow in the uterus and, as Leah’s doctors told her, could lead to cancer.
It was mid-July, and Kentucky’s trigger law and six week ban had been in effect for barely two weeks. Leah was familiar enough with what both laws restricted and assumed that because her pregnancy could cause her cancer and was nonviable, she would lawfully qualify as an exception.
So, she weighed her options with her doctors at Baptist Health Lexington, who included Dr. Blake Bradley, her longtime OBGYN.
Similar to Amy’s diagnosis, Leah’s doctors told her that even if she opted to carry the pregnancy to term, her baby “would live a short life in palliative care, most likely never leaving the hospital. It would really be a quite painful existence,” she said.
“I have a 2-year-old at home, and I’m 35, weighing how I would like to expand my family. It seemed like the safest option for me and the compassionate choice for my unborn child was to terminate the pregnancy,” she said.
Like Amy’s, a medically-necessary abortion under these circumstances would typically take place at a hospital, doctors interviewed for this story said. Leah’s health insurance had already agreed to cover it. It was also the quickest way to help Leah to her end goal: getting pregnant again in order to birth a child that would survive.
It was July 21 and Leah was just over 12 weeks pregnant when she learned that Baptist’s legal counsel had blocked her doctors from giving her a dilation and curettage abortion.
“I was told the hospital refused to perform the procedure while the case was being litigated. I was dumbfounded,” Leah said. Hospital lawyers cited an ongoing lawsuit from Kentucky’s two outpatient abortion providers that’s pending before the Kentucky Supreme Court.
According to Leah, hospital providers, relaying the message from administration and risk management, reportedly said if her fetus died on its own, doctors would be able to terminate her pregnancy. But their hands were tied as long as it had a heartbeat.
“People minimize that pregnancy, even under its best circumstances, is associated with life-threatening risks, life-altering risks and emotional impacts,” Bradley told the Herald-Leader. “So, to compel a woman to continue a pregnancy that is by everyone’s assessment, doomed, by definition places that woman at an unreasonable and unnecessary physical and psychological risk, period.”
Baptist Health refused to make Leah’s high-risk doctor available for an interview.
The following Monday, July 25, Leah had an ultrasound at the hospital to confirm what she already knew. As an ultrasound tech probed her abdomen, a wheel of dizzying emotions spun in her head: she desperately wanted a baby, but she didn’t want to birth a child into a painful existence.
Already faced with a gutting dilemma, she felt further burdened by having such an intimate choice ripped from her. And she was furious at now being forced to remain pregnant despite there being no chance for survival, despite the risks continuing such a pregnancy posed to her own body.
She remembers staring at the ultrasound screen waiting to hear the muffled heartbeat of her fetus, racked with guilt because she hoped she wouldn’t.
“It was such a twisted experience being pregnant with a baby I desperately wanted, lying there hoping its heart had stopped,” she said shakily. “It was horrible to have to wish for that in order to receive care. It just felt so unsafe and cruel.”
Leah had already arranged to drive to Chicago to get an abortion when a Jefferson Circuit judge issued a preliminary injunction on July 22, temporarily blocking the state from enforcing both bans. She immediately called EMW Women’s Surgical Center in Louisville — one of the plaintiffs in the lawsuit against the state — and made an appointment.
On Wednesday, July 27, almost 13 weeks pregnant, Leah paid $950 out of pocket for her abortion. Her insurance wouldn’t cover it, since it was considered elective. The following Monday, the Kentucky Court of Appeals overturned the circuit court injunction, reinstating both abortion bans.
After Leah’s abortion, she sent a message to her high-risk doctor. Her doctor responded the following day. Leah shared that correspondence with the Herald-Leader.
“You’ve been on my thoughts a lot,” her doctor wrote. “Words cannot express the dismay I feel right now. I’ve spent my whole adult life learning how to care for mothers in heart wrenching or dangerous situations like yours, and the politics now make it not only impossible, but to work to take care of patients like they deserve — with compassion and science — in these horrible situations is wrong and immoral.”
“I hope your procedure yesterday was smooth, though I know it was hard,” her doctor wrote. “I’m so sorry we could not (were not allowed, rather) to take care of you here.”
#us politics#news#Kentucky Herald-Leader#2023#abortions#Abortion bans#anencephaly#acrania#nonviable pregnancies#kentucky#fetal heartbeat laws#Cabinet for Health and Family Services#dilation and evacuation abortions#Kentucky Supreme Court#Daniel Cameron#triploidy#palliative care#dilation and curettage abortions#Kentucky Court of Appeals#reproductive rights#bodily autonomy
68 notes
·
View notes
Text
Every time Catha was minding her business yesterday, @justabiteofspite would hear initiative roll followed by me going, "OH SHI- Don't worry about it." Then suddenly appearing after Astarion and Gale murder hoboed someone.
The only person left alive Act 1 so far has been Gandrel 😭
We have exactly two traders we can currently visit until we make it to the Duergar. We do not have Volo as one bc Catha got her eye gouged out.
Like this is so fucking funny. It's been a GREAT playthrough especially with my ADHD ass running Astarion around like he has the zoomies. Catha and Shadowheart are like lesbian moms and Astarion is their hyperactive vampire child that is constantly on a child's harness and leash bc otherwise he'll go scavenge rotten food and fill Shadowheart's inventory with it OR find someone to eat.
Astarion is SO good at hunting/gathering that he has the most supplies but he also keeps. Picking up the rotten food and handing it over like "This is similar to a rat, you could eat it in a pinch."
#bat plays bg3#astarion act 1 still doesnt care abt the consequences of his actions#he's starting to think about it since Gale said he doesnt like who he is around Astarion#but now Gale is smitten and Astarion doesnt care again#so he was mean to mayrina and she and connor attacked#so now astarion is going around performing abortion services across the sword coast#him and gale will retire together and open an apoe#an apothecary together#jk this is a god gale/ascended astarion run they're so bad for each other
8 notes
·
View notes
Text
ah yeah it's saturday and the school year's started. explains the protesters on my way to the metro station
#i passed someone holding a 'washington commits infanticide' side and i was just like. ah sidewalk prayer is back on again yeah?#*lives next to a planned parenthood#*school has a regular and well-attended 'sidewalk prayer' event on saturdays where people go and pray the rosary/protest outside it#happened during the summer too but attendance massively ticks up when students are on campus#pp posts up volunteers outside with hi vis 'escort' vests to help people Trying To Get Healthcare avoid too much harassment every week#i guess the people who just show up to pray are annoying but not disruptive. the people with angry signs and shouting suck ass though#it's annoying that they all treat pp like an abortion factory still though when that place does literally so many other things#they have a big banner out front advertising primary care services#and they'll see you for migraines. internal medicine. stuff like that. not just reproductive health although of course that's important#like honestly of i didn't already have an appointment booked across the city i'd probably move to seeing doctors there#hell of a lot more convenient. even if you have to deal with the demonstrators outside. but at least they're usually constrained to saturday#i wanna talk about me
10 notes
·
View notes
Last Seen Blogs
unbelievabelle
if heaven is full of people

hippoggriff
the pain of water is infinite.

as-is-above-so-below
Batfam & COD Enthusiast|Amateur Fanfic Writer

smaqib
Untitled

calliesissy
sissy lcrossdresser