#Cervical Fluid
Text
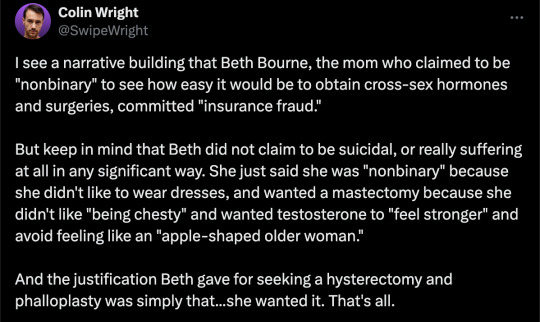
By: Beth Bourne
Published: Feb 27, 2024
Kaiser gender specialists were eager to approve hormones and surgeries, which would all be covered by insurance as “medically necessary.”
On September 6, 2022, I received mail from my Kaiser Permanente Davis Ob-Gyn reminding me of a routine cervical screening. The language of the reminder stood out to me: “Recommended for people with a cervix ages 21 to 65.” When I asked my Ob-Gyn about this strange wording, she told me the wording was chosen to be “inclusive” of their “transgender” and “gender fluid” patients.
Based on this response, several thoughts occurred to me. Could I expose the medical scandal of “gender-affirming care” by saying and doing everything my daughter and other trans-identifying kids are taught to do? Would there be the type of medical safeguarding and differential diagnosis we would expect in other fields of medicine, or would I simply be allowed to self-diagnose and be offered the tools (i.e. hormones and surgeries) to choose my own gender adventure and become my true authentic self?
If I could demonstrate that anyone suffering from delusions of their sex, self-hatred, or identity issues could qualify for and easily obtain body-altering hormones and surgeries, all covered by insurance as “medically necessary” and potentially “life-saving” care, then maybe people would finally wake up. I certainly had.
I was prepared for failure. I wasn’t prepared for how easy success would be.
* * *
I am a 53-year-old mom from Davis, CA. My daughter began identifying as a transgender boy (social transition) and using he/him pronouns at school during 8th grade. Like several of her peers who also identified as trans at her school, my daughter was a gifted student and intellectually mature but socially immature. This shift coincided with her school’s sudden commitment to, and celebration of, a now widespread set of radical beliefs about the biology of sex and gender identity.
She “came out” as trans to her father (my ex-husband) and me through a standard coming-out letter, expressing her wish to start puberty blockers. She said she knew they were safe, citing information she had read from Planned Parenthood and the World Professional Association for Transgender Health (WPATH). To say I was shocked would be an understatement. I was also confused because this announcement was sudden and unexpected. While others quickly accepted and affirmed my daughter’s new identity, I was apprehensive and felt the need to learn more about what was going on.
Events began escalating quickly.
During a routine doctor’s visit scheduled for dizziness my daughter said that she was experiencing, the Kaiser pediatrician overheard her father using “he/him” pronouns for our daughter. The pediatrician seemed thrilled, quickly asking my daughter about her “preferred pronouns” and updating her medical records to denote that my daughter was now, in fact, my son. The pediatrician then recommended we consult the Kaiser Permanente Oakland Proud pediatric gender clinic, where she could get further information and (gender affirming) “treatment.” Now I was the one feeling dizzy.
As I began educating myself on this issue, I discovered that this phenomenon—minors, most often teen girls, suddenly adopting trans identities—was becoming increasingly widespread. It even had a name: rapid onset gender dysphoria, or ROGD. Thankfully, after learning about the potential side-effects of blockers and hormones, my ex-husband and I managed to agree not to consent to any medical interventions for our daughter until she turned 18 and would then be able to make such decisions as an adult.
Over the past five years, my daughter’s identity has slowly evolved in ways that I see as positive. Our bond, however, has become strained, particularly since I began publicly voicing my concerns about what many term as “gender ideology.” Following my daughter’s 17th birthday family celebration, she sent me an email that evening stating she would be cutting off contact with me.
While this estrangement brought me sorrow, with my daughter living full-time with her father, it also gave me the space to be an advocate/activist in pushing back on gender identity ideology in the schools and the medical industry.
I decided to go undercover as a nonbinary patient to show my daughter what danger she might be putting herself in—by people who purport to have her health as their interest, but whose main interest is in medically “affirming” (i.e., transitioning) whoever walks through their door. I am at heart a mother protecting her child.
* * *
My daughter’s sudden decision to become a boy was heavily on my mind in early September of 2022, when mail from my Kaiser Permanente Davis Ob-Gyn reminded me of a routine cervical screening with “Recommended for people with a cervix ages 21 to 65.” I was told that the wording was chosen to be “inclusive” of transgender and “gender fluid” patients.
Throughout the whole 231-day process of my feigned gender transition, the Kaiser gender specialists were eager to serve me and give me what I wanted, which would all be covered by insurance as “medically necessary.” My emails were returned quickly, my appointments scheduled efficiently, and I never fell through the cracks. I was helped along every step of the way.
Despite gender activists and clinicians constantly claiming that obtaining hormones and surgeries is a long and complex process with plenty of safety checks in place, I was in full control at every checkpoint. I was able to self-diagnose, determine how strong a dose of testosterone I received and which surgeries I wanted to pursue, no matter how extreme and no matter how many glaring red flags I purposefully dropped. The medical workers I met repeatedly reminded me that they were not there to act as “gatekeepers.”
I was able to instantly change my medical records to reflect my new gender identity and pronouns. Despite never being diagnosed with gender dysphoria, I was able to obtain a prescription for testosterone and approval for a “gender-affirming” double mastectomy from my doctor. It took only three more months (90 days) to be approved for surgery to remove my uterus and have a fake penis constructed from the skin of my thigh or forearm. Therapy was never recommended.
Critics might dismiss my story as insignificant on the grounds that I am a 53-year-old woman with ample life experience who should be free to alter her body. However, this argument for adult bodily autonomy is a standard we apply to purely cosmetic procedures like breast implants, liposuction, and facelifts, not “medically necessary” and “lifesaving” treatments covered by health insurance. Or interventions that compromise health and introduce illness into an otherwise healthy body. And especially not for children.
My story, which I outline in much more detail below, should convince any half-rational person that gender medicine is not operating like any other field of medicine. Based on a radical concept of “gender identity,” this medical anomaly preys upon the body-image insecurities common among pubescent minors to bill health insurance companies for permanent cosmetic procedures that often leave their patients with permanently altered bodies, damaged endocrine systems, sexual dysfunction, and infertility.
* * *
Detailed Timeline of Events
On October 6, 2022, I responded to my Ob-Gyn’s email to tell her that, after some thought, I’d decided that maybe the label “cis woman” didn’t truly reflect who I was. After all, I did have some tomboyish tendencies. I told her I would like my records to be changed to reflect my newly realized “nonbinary” identity, and that my new pronouns were they/them. I also voiced my desire to be put in touch with an endocrinologist to discuss starting testosterone treatment.
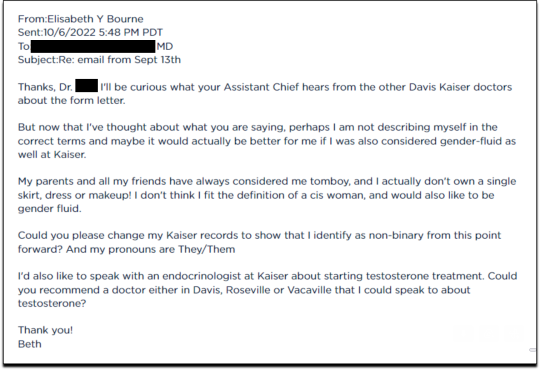
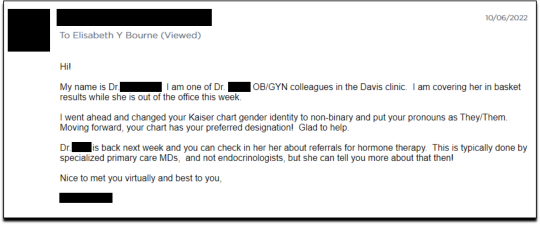
Fifteen minutes later I received an email from another Kaiser doctor informing me that my medical records had been changed, and that once my primary doctor returned to the office, I’d be able to speak with her about hormone therapy.
I responded the following day (October 7, 2022), thanking her for changing my records, and asking if she could connect me with someone who could help me make an appointment for “top surgery” (i.e., a cosmetic double mastectomy) because my chest binder was rather “uncomfortable after long days and playing tennis.”
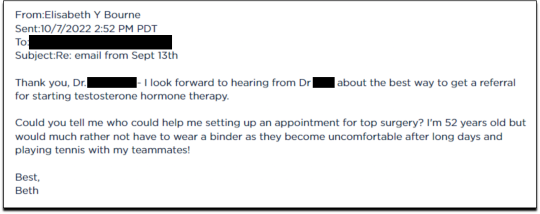
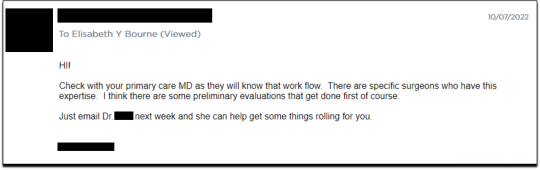
She told me to contact my primary care MD to “get things rolling,” and that there were likely to be “preliminary evaluations.”
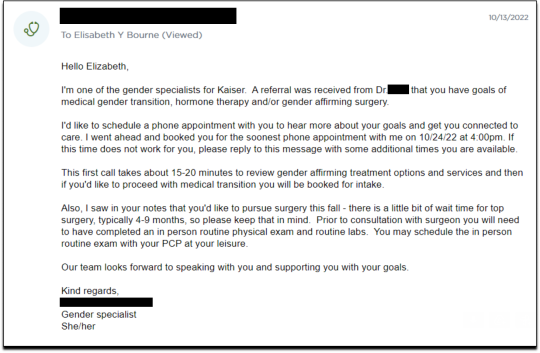
Six days after contacting my primary care MD for a referral, I received an email from one of Kaiser’s gender specialists asking me to schedule a phone appointment so she could better understand my goals for surgery, so that I could get “connected to care.” This call to review my “gender affirming treatment options and services” would take 15-20 minutes, after which I would be “booked for intake,” allowing me to proceed with medical transition.
This wasn’t an evaluation of whether surgical transition was appropriate, it was simply a meeting for me to tell them what I wanted so that they could provide it.
On October 18, I had my one and only in-person appointment in preparation for top surgery. I met in Davis with my primary care physician, Dr. Hong-wen Xue. The assessment was a 10-minute routine physical exam that included blood tests. Everything came back normal. Notably, there was not a single question about why I wanted top surgery or cross-sex hormones. Nor was there any discussion of the risks involved with these medical treatments.
The following week, on October 24, I had a phone appointment with Rachaell Wood, MFT, a gender specialist with Kaiser Sacramento. The call lasted 15 minutes and consisted of standard questions about potential drug use, domestic violence, guns in the house, and whether I experienced any suicidal thoughts. There were no questions from the gender specialist about my reasons for requesting a mastectomy or cross-sex hormones, or why I suddenly, at 52, decided I was “nonbinary.”
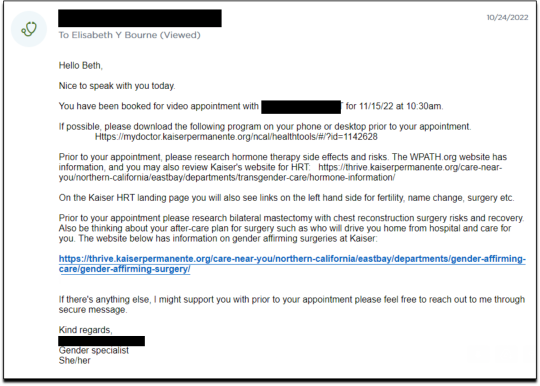
After the call, Kaiser emailed me instructions about how to prepare for my pre-surgery intake video appointment to evaluate my mental health, scheduled to take place on November 15. The email stated that prior to my appointment, I should research hormone risks on the WPATH website, and to “research bilateral mastectomy and chest reconstruction surgery risks and recovery” on Kaiser’s website.
I decided to request a “gender-affirming” double mastectomy and phalloplasty. Kaiser sent me a sample timeline for gender transition surgery preparation (see below) that you can use as a reference for the process. I also asked for a prescription for cross-sex hormones (testosterone) as needed and recommended by Kaiser.
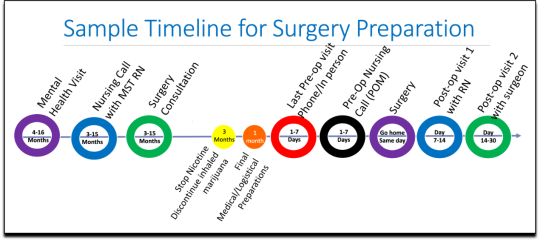
[ Source: Kaiser Permanente, Top Surgery - EXPLORING YOUR SURGICAL OPTIONS ]
Pre-Surgery Mental Health Video Appointment, Part I
This “Mental Health Visit” assessment was conducted over Zoom. The Kaiser gender specialist started with questions addressing my marital status, race, gender identity, and other demographics. She asked whether I was “thinking of any other surgeries, treatments in the future.” The list she read included “gender-affirming” hysterectomies, bottom surgeries such as metoidioplasty and phalloplasty, vocal coaching, support groups, and body contouring. “Anything else you might be interested in doing?” she asked. I said that I’d perhaps be interested in body contouring. I was also assured that all the procedures would be covered by insurance because they were considered “medically necessary.”
I dropped in several red flags regarding my mental health to see the reaction, but all were ignored. For instance, I revealed that I had PTSD. When the therapist asked me about whether I had experienced any “childhood trauma,” I explained that I grew up in Mexico City and had been groped several times and had also witnessed men masturbating in public and had been grabbed by men in subways and buses. “I was a young girl, so [I had] lots of experiences of sexual harassments, sexual assault, just the kind of stuff that happens when you are a girl growing up in a big city.” “So, you know,” I finished, “just the general feeling that you are unsafe, you know, in a female body.”
The therapist did not respond to my disclosure that trauma could be the cause of my dysphoria. Instead of viewing this trauma as potentially driving my desire to escape my female body through hormones and surgery, she asked whether there is anything “important that the surgery team should be aware of” regarding my “history of trauma,” such as whether I’d be comfortable with the surgeon examining and marking my chest prior to surgery.
When asked about whether I had had any “psychotic symptoms,” I told her that while I had had no such symptoms, my mother had a delusional nervous breakdown in her 50s because she had body dysmorphia and became convinced she had a growth on her neck that needed to be removed. I told her that my mother was then admitted to an inpatient hospital for severe depression. I asked her whether she ever sees patients with body dysmorphia and whether I could have potentially inherited that from my mother. She told me that psychosis was hereditary, but that it was “highly unlikely” that there was any connection between body dysmorphia and gender dysphoria.
I enthusiastically waved more mental health red flags, waiting to see if she would pick up on any of them.
I’m just wondering if my feelings, or perseverating, or feeling like these breasts make me really unhappy and I just don’t want them anymore!...I’m just not sure if that’s a similar feeling to body dysmorphia? How do you decide which one is gender dysphoria and general body dysmorphia, and just not liking something about your body? Feeling uncomfortable with your body?
And I did have an eating disorder all through college. I was a distance runner in college so I had bulimia and anorexia, you know. So I don’t know if that’s related to gender dysphoria?
The therapist replied, “I completely appreciate your concerns, but I am going to ask you questions about your chest, about your expectations. And then I’ll be able to give you an assessment.” She also said the main difference between my mom’s situation and mine was that my mom didn’t really have a growth on her neck, whereas it’s “confirmed” that I actually have “chest tissue.” Furthermore, she said that while “historically there has been all this pressure on patients to be like ‘Are you really, really sure you want hormones? Are you 100% sure?’ We are a little more relaxed.” She continued, “As long as you are aware of the risks and the side-effects, you can put your toe in the water. You can stop ‘T’ [testosterone], you can go back and do it again later! You can stop it! You can stop it! You know what I mean?”
Because we ran out of time, I scheduled a follow-up phone meeting on December 27, 2022 with a different gender specialist to complete my mental health assessment for top surgery.
Pre-Surgery Mental Health Video Appointment, Part II
During this meeting, Guneet Kaur, LCSW, another Kaiser gender specialist (she/her/they/them pronouns) told me that she regretted the “gatekeeping vibe” of the meeting but assured me that since I have been “doing the work,” her questions are essentially just a form of “emotional support” before talking with the medical providers.
She asked me about what I’d been “looking into as far as hormones.” I told her that I’d be interested in taking small doses of testosterone to counterbalance my female feelings to achieve “a feeling that’s kind of neutral.”
When she asked me about me “not feeling like I match on the outside what I feel on the inside,” I dropped more red flags, mentioning my aversion to wearing dresses and skirts.
I don’t own a single dress or a skirt and haven't in 20 years. I think for me it’s been just dressing the way that’s comfortable for me, which is just wearing, jeans and sweatshirts and I have a lot of flannel shirts and, and I wear boots all the time instead of other kinds of shoes. So I think it’s been nice being able to dress, especially because I work from home now most of the time that just a feeling of clothing being one of the ways that I can feel more non-binary in my everyday life.
She responded, “Like having control over what you wear and yeah. Kind of that feeling of just, yeah, this is who I am today. That’s awesome. Yeah.”
She then asked me to describe my dysphoria, and I told her that I didn’t like the “feeling of the female form and being chesty,” and that because I am going through menopause, I wanted to start taking testosterone to avoid “that feeling of being like this apple-shaped older woman.” “Good. Okay, great,” she responded, reminding me that only “top surgery,” not testosterone, would be able to solve my chest dysphoria. (Perhaps it was because all these meetings were online, they didn’t notice I’m actually fit and relatively slender at 5’-5” and 130 pounds, and not apple-shaped at all.)
She told me that we had to get through a few more questions related to my medical history before “we can move on to the fun stuff, which is testosterone and top surgery.”
The “fun stuff” consisted of a discussion about the physical and mood changes I could expect, and her asking me about the dose of testosterone I wanted to take and the kind of “top surgery” technique I’d prefer to achieve my “chest goals.” She told me that all or most of my consultations for surgeries and hormones would be virtual.
The gender specialist told me after the appointment, she would submit my referral to the Multi-Specialty Transitions Clinic (MST) team that oversees “gender expansive care.” They would follow up to schedule a “nursing call” with me to review my medical history, after which they’d schedule my appointment with a surgeon for a consultation. Her instructions for this consultation were to “tell them what you’re wanting for surgery and then they share with you their game plan.”
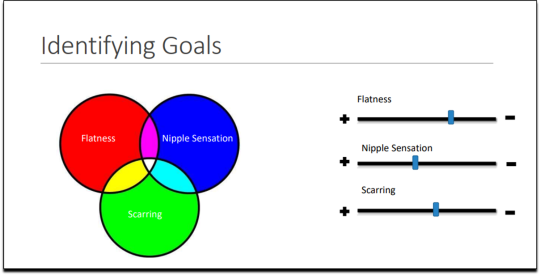
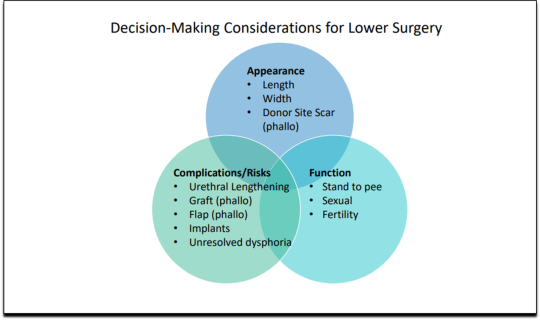
[ Decision-making slide to help me identify my goals for top surgery–flat chest, nipple sensation, or minimal scarring. Source: Kaiser Permanente, Top Surgery - EXPLORING YOUR SURGICAL OPTIONS ]
She told me that Kaiser has a team of plastic surgeons who “only work with trans and nonbinary patients because there’s just so much need for them.” She asked about my priorities for chest surgery, such as whether I value flatness over nipple sensation. I learned about double incision top surgery with nipple grafts, as well as “keyhole,” “donut,” “buttonhole,” and “Inverted-T” top surgeries.
By the end of the hour-long appointment, I had my surgery referral and was ready for my “nursing call” appointment.
Nursing call with Nurse Coordinator from the Transgender Surgery and Gender Pathways Clinic at Kaiser San Francisco
On January 19, 2023, I had my nursing call with the Nurse Coordinator. He first said that “the purpose of this call is just for us to go through your chart together and make sure everything’s as accurate as possible.” Once that was done, my referral would be sent to the surgeon for a consultation.
He asked me about potential allergies and recreational drug use, and verified that I was up to date on mammograms, pap smears, and colon cancer screenings, as well as vaccines for flu and COVID. I verified my surgical history as well as my current medications and dietary supplements.
He told me about a “top surgery class” available for patients where one of the Kaiser surgeons “presents and talks about surgical techniques and options within top surgery,” and includes a panel of patients who have had top surgery. I signed up for the February 8th class.
Within 10 minutes he told me that he had “sent a referral to the plastic surgery department at Kaiser Sacramento,” and that I should be hearing from them in the next week or two to schedule a consultation.
Appointment for Testosterone
On January 27, I had a 13-minute online appointment with a primary care doctor at Kaiser Davis to discuss testosterone. The doctor verified my name and preferred pronouns, and then directly asked: “So, what would you like to do? What kind of physical things are you looking for?”
I told her I wanted facial hair, a more muscular and less “curvy” physique, and to feel stronger and androgynous. She asked me when I wanted to start, and I told her in the next few months. She asked me if I was menopausal, whether I had ovaries and a uterus, although that information should have been on my chart.
The doctor said she wanted me to come in to get some labs so she could check my current estrogen, testosterone, and hemoglobin levels before starting hormones. Then “we'll set the ball in motion and you'll be going. We’ll see you full steam ahead in the direction you wanna go.”
That was it. I made an appointment and had my lab tests done on February 12. My labs came back on February 14, and the following day, after paying a $5 copay at the Kaiser pharmacy, I picked up my testosterone pump. That was easy!
Top Surgery Consultation
On the same day I received my labs, I had a Zoom surgery consultation with Karly Autumn-Kaplan, MD, Kaiser Sacramento plastic surgeon. This consultation was all about discussing my “goals” for surgery, not about whether surgery was needed or appropriate.
I told the surgeon that I wanted a “flatter, more androgynous appearance.” She asked me some questions to get a better idea of what that meant for me. She said that some patients want a “male chest,” but that others “want to look like nothing, like just straight up and down, sometimes not even nipples.” Others still wanted their chest to appear slightly feminine and only “slightly rounded.” I told her that I’d like my chest to have a “male appearance.”
“What are your thoughts about keeping your nipples?” she asked. “Are you interested in having nipples or would you like them removed?” I told her that I’d like to keep my nipples, but to make them “smaller in size.” She asked me if I’d like them moved to “the edge of the peck muscle” to achieve “a more male appearance.” I said yes.
I was asked to show my bare chest from the front and side, which I did. Then she asked me how important it was for me to keep my nipple sensation. I replied that it was important unless it would make recovery more difficult or there were other associated risks. She highlighted the problem with the free nipple graft, saying that removing the nipple to relocate it means “you're not gonna have sensation in that nipple and areola anymore.” However, some nipple sensation could be preserved by keeping it attached to “a little stalk of tissue” with “real nerves going to it,” but that would require leaving more tissue behind. I told her I’d go for the free nipple graft to achieve a flatter appearance. It was also suggested I could skip nipple reconstruction entirely and just get nipples “tattooed” directly onto my chest.
She told me I was “a good candidate for surgery,” and put me on the surgery wait list. She said that the wait time was between three and five months, but a cancellation could move me up to a sooner date. Also, if I wanted surgery as soon as possible, I could tell the surgery scheduler that I’d be willing to have any of the other three surgeons perform my mastectomy. Outpatient top surgery would cost me a copay of $100.
They contacted twice, in February and March, notifying me of cancellations. If I had accepted and shown up on those dates, they would have removed my breasts. This would have been less than five months from the time I first contacted Kaiser to inform them of my new “nonbinary” gender identity.
How Far Can I Go?
I decided to see how easy it would be for me to get approved for a phalloplasty. Known euphemistically as “bottom surgery,” phalloplasty is the surgical creation of an artificial penis, generally using tissue from the thigh or arm.
I sent an email on March 1, 2023, requesting to have a phalloplasty and concurrent hysterectomy scheduled alongside my mastectomy.
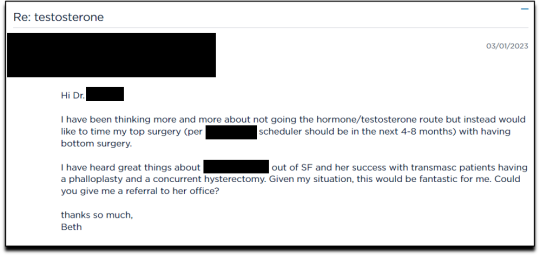
Two weeks later, on March 16th, I had a 16-minute phone call with a gender specialist to discuss my goals for bottom surgery and obtain my referral.
During the call, I explained to the specialist that I wasn’t sure about taking testosterone anymore because I was already quite athletic and muscular, and that taking testosterone didn’t make much sense to me. Instead, I wanted bottom surgery so that I wouldn’t feel like my “top” didn’t match my “bottom.” I told her:
But what I really wanted was to have bottom surgery. So this way when I have my top surgery, which sounds like it could be very soon, that I’ll be aligned, that I won’t have this sense of dysphoria with one part of my body and the other part feeling like it matched who I am. So yeah. So I just did a little bit more research into that. And I looked at the resources on the Kaiser page for the MST clinic and I think I know what I want, which is the hysterectomy and then at the same time or soon after to be able to have a phalloplasty.
I told her that I wanted to schedule the top and bottom surgery concurrently so that I wouldn’t have to take more time off work and it would save me trips to San Francisco or Oakland, or wherever I had to go for surgery.
None of this gave the gender specialist pause. After a brief conversation about some online resources to look over, she told me that she would “submit the referral now and we’ll get this ball rolling.”
Bottom surgery would cost me a copay of $200, which included a couple of days in the hospital for recovery.
Phalloplasty Surgical Consultation with Nurse Coordinator
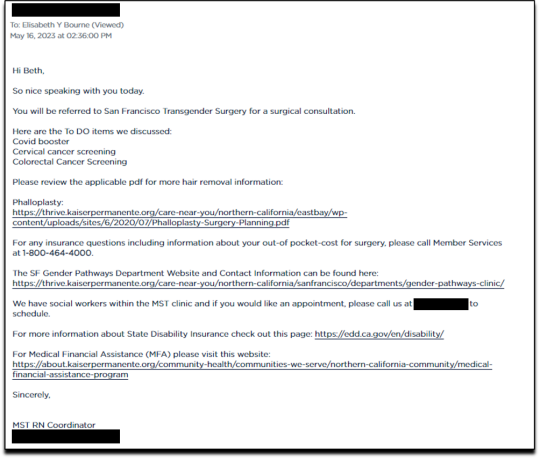
On May 16, 2023, I had a short surgical consultation with a nurse coordinator to go through my medical history. This was similar to the consultation for top surgery but included information about hair removal procedures for the skin on my “donor site” that would be fashioned into a makeshift penis. They also went over the procedures for determining which donor site—forearm or thigh—was more viable.
After only 15 minutes, she submitted my referral to the surgeon for another surgical consultation.
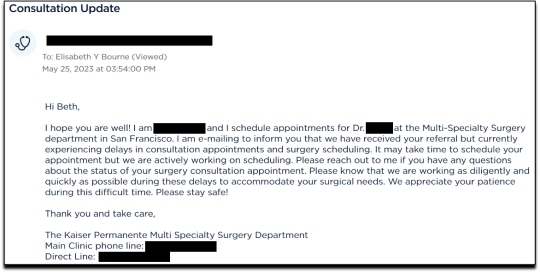
On May 25 I received an email from my phalloplasty surgeon’s scheduler, informing me that they have received my referral and are actively working on scheduling, but that they are experiencing delays.
I ended my investigation here once I had the referral for the top and bottom surgery. I never used my testosterone pump.
Final Thoughts
In fewer than 300 days, based on a set of superficial and shifting thoughts about my gender and my “embodiment goals” triggered by the mere mention of “gender” in a form letter from my primary care physician, and driven by what could only be described as minor discomforts, Kaiser Permanente’s esteemed “multi-disciplinary team” of “gender specialists” was willing, with enthusiasm—while ignoring mental health concerns, history of sexual trauma, and rapidly escalating surgical requests—to prescribe life-altering medications and perform surgeries to remove my breasts, uterus, and vagina, close my vaginal opening, and attempt a complex surgery with high failure and complication rates to create a functionless representation of a penis that destroys the integrity of my arm or thigh in the process.
This describes the supposedly meticulous, lengthy, and safety-focused process that a Kaiser patient must undergo to embark on a journey to medically alter their body. No clinician questioned my motivations. No one showed concern that I might be addressing a mental health issue through radical and irreversible interventions that wouldn’t address my amorphous problems. There were no discussions about how these treatments would impact my long-term health, romantic relationships, family, or sex life. I charted the course. The clinicians followed my lead without question. The guiding issue was what I wanted to look like.
No other medical field operates with this level of carelessness and disregard for patient health and welfare. No other medical field addresses issues of self-perception with surgery and labels it “medically necessary.” No other medical field is this disconnected from the reality of the patients it serves.
Kaiser has traded medicine for ideology. It’s far beyond time we stop the ruse of considering “gender-affirming” interventions as anything approaching medical care.
This isn’t the first time Kaiser Permanente has been in the news for completely disregarding medical safeguards in the name of “gender-affirming care.” As girls, Chloe Cole and Layla Jane became convinced that they were born in the wrong body and were actually boys on the inside. Doctors at Kaiser ignored their underlying conditions and instead prescribed testosterone and removed their breasts. Both Cole and Jane have since detransitioned and are currently suing Kaiser.
The fact that children and vulnerable adults are being exploited in this massive ideological experiment is not just tragic; it’s deeply disturbing, especially considering it has evolved into a billion-dollar industry.
I hope that by sharing my story, I can bring more focused scrutiny to the medical scandal unfolding not just at Kaiser but also at medical centers and hospitals across the Western world. These institutions have completely abandoned medical safeguards for patients who claim to be confused about their “gender,” and I aim to awaken more parents and assist them in protecting their children.
--
==
This is completely insane.
Apologists online are running around saying, but she didn't mean it, she was lying, she was pretending...
It doesn't matter.
Any kind of security, penetration or integrity test is insincere too. When security researchers compromise Microsoft's operating system or Google's browser or whatever, "but they didn't mean it" is not a defence to a discovered security flaw. It doesn't matter that the security researchers didn't plan to steal data or money or identities. The flaw in the system is there regardless.
It doesn't matter that it was insincere. Because the workers didn't know that. They never checked, never asked questions, never tested. They had been taught and instructed to never ask any questions. They did what they were supposed to. And the system failed spectacularly. Because that's what "gender affirming care" means.
Additionally, the claim that Beth Bourne committed fraud is an outright lie. A patient cannot bill. They do not have the authority. The medical clinic is the only one that can bill, and they must supply a diagnosis and a medical necessity.
If they didn't diagnose her and just wrote down what she said, then they committed fraud. If they claim they did diagnose her, then they committed fraud, because the diagnosis they concocted was bogus. This, by the way, is actually going on. Clinics are reporting fake endocrine and other disorders to get blockers, hormones and other interventions. Jamie Reed and other whistleblowers have documented evidence of this. Beth Bourne is not responsible for what the clinic does. They have medical licenses and legal responsibility. Not her.
Additionally, anyone who actually read the article would know how she tested the system. She said things like, "I've always been not that feminine. So, maybe I get my boobs removed." And they said, "sure." Instead of saying, "wait, why do you think that?" Framing it as her lying is itself a lie. They violated their ethical obligations. That much is incontrovertible. And it's directly the result of "gender affirming care," where clinics and clinicians rubber-stamp anything deemed "trans" based entirely on ideological, not medical, grounds.
#Beth Bourne#undercover#undercover investigation#gender identity ideology#queer theory#nonbinary#non binary#top surgery#bottom surgery#double mastectomy#bilateral mastectomy#gender affirming care#gender affirming healthcare#gender affirmation#affirmation model#medical scandal#medical malpractice#medical corruption#religion is a mental illness
759 notes
·
View notes
Text
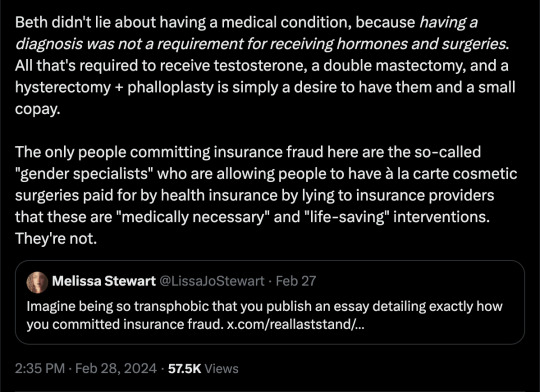
head injury
Y/N had been an integral part of Arsenal Women's Football Club for three years. Her journey with the team had seen them through victories, challenges, and unforgettable moments on and off the field. During this time, Y/N had cultivated deep connections with her teammates, and they had become more than just friends and fellow athletes; they were her soccer family. As this season progressed, Arsenal found themselves facing a crucial match against their fierce rivals, Chelsea. Y/N, being her tenacious self, was right in the thick of the action. Her partnership with Leah on the field had always been one of Arsenal's strengths, and they synchronized like clockwork. Arsenal was known for its fluid passing and attacking style of play, and Y/N played a pivotal role in their success.
The first half of the match saw both teams battling fiercely for dominance on the field. The intensity was high, and both Arsenal and Chelsea were pushing their limits.
During a set piece, as Y/N went up to contest a header, an accidental collision with an opposing player pushed her back into the goal post, her head ricocheting off the metal post.
As the ball was kicked to upfield, everyone cleared around the goal, but the stadium fell into a hushed panic as Y/N lay motionless on the ground. Leah, her girlfriend, was the first to reach her.
Kneeling by Y/N's side, her voice trembling as she cried out, "We need medics!" Leah shouted, her heart racing seeing Y/N's eyes closed. Leah reached out, placing her trembling hand on Y/N's cheek, hoping to rouse her. "Y/N, I need you to open your eyes for me. Hey, Y/N, come on. Open your eyes."
More teammates gathered around as panic swelled, their faces etched with worry. Jessie Fleming, Y/N's sister, dropped to the ground beside Leah. She reached out to shake her sister's shoulders, but Leah stopped her.
"You can't move her, Jessie," Leah cautioned, her voice strained with fear. "Her neck or back might be injured." Jessie nodded in understanding and opted to stroke little strands of her hair that have fallen from her ponytail, out of her face.
Leah and Jessie tried their best to awaken y/n but nothing seemed to work.
Finally, the team's medical staff arrived as well as medics, their expertise evident as they swiftly assessed the situation. They took every precaution to stabilize Y/N's neck and spine, carefully fitting a cervical collar around her and turning her over.
“We need some space guys.” The older medic informed Jessie and Leah but they remained in their spots. Jordan, McCabe, Kerr and a few other of their own teammates had to physically pull them back. They now stood a few feet away watching one of the medics speak to Y/N, trying to coax her into consciousness while another examined her vitals.
As the medics worked for a few minutes, Y/N's eyelids fluttered open, revealing her dazed and confused expression. She tried to sit up, but the medical staff gently held her down, reminding her not to move. Y/N mumbled incoherently, and Leah leaned closer, straining to catch her words before going right next to y/n side, hating the sight of seeing her so lost and scared. "It's okay, Y/N," Leah whispered, her voice trembling. "You had a tough collision, but the medics are here to help you."
“Y/n, you need to lay back down. Everything is going to be okay, but try not to move so much.” Jessie crouched down and spoke as she noticed her wanting to get up once again.
Y/N's consciousness wavered like a flickering flame. She struggled to comprehend her surroundings, her eyes darting aimlessly as confusion clouded her thoughts. Jessie's plea to stay still seemed to fall on deaf ears, and Y/N's movements grew more erratic.
Leah held her girlfriend's trembling hand, her voice quaking with concern. "Y/N, please, lay back down. You need to stay still. Everything is going to be okay." She desperately hoped her words would reach Y/N through the haze of her dazed state.
The medical staff worked with a sense of urgency, attempting to keep Y/N from further harm as she teetered on the edge of consciousness. They continued their assessments, monitoring her vitals, and told Leah and Jessie to try to keep y/n engaged in conversation to keep her awake.
Y/N's attempts to engage back in the conversation were sporadic and disjointed, and it became increasingly apparent that the injury was more severe than anyone had initially thought. Her responses were fragmented, and she struggled to maintain her focus.
Leah squeezed her hand, her voice trembling with worry. "Y/N, do you remember our first date? We went to that little café near your place, and it was pouring rain. You laughed when I slipped on a puddle."
Y/N's eyelids fluttered, but her gaze was unfocused. She mumbled, "Rain... yeah," but her voice was barely audible, and her response lacked the warmth and clarity it once held.
Jessie, trying to hold back tears, added, "And what about that time we played football in the park with Dad? You always said you'd be better than all of us."
Y/N's lips twitched in an attempt at a smile, but it was fleeting. "am... better," she mumbled, her words disjointed and distant. The memories, which should have elicited laughter and connection, now seemed to be slipping away from her grasp.
As Y/N's condition worsened, she suddenly gagged, her face contorted in pain, it was a distressing sight, and the medics reacted swiftly, turning her onto her side to clear her airway and prevent any choking from the vomit that arose.
Leah's voice quivered as she tried to maintain Y/N's focus. "Y/N, stay with us. We're right here with you. Keep those beautiful eyes of yours open."
But Y/N's response was a mere groan, and her eyes slowly rolled back, her body growing limp. The medics exchanged concerned glances, realizing that her condition was rapidly deteriorating.
Without a moment to lose, they immediately placed an oxygen mask over her face, ensuring she received a steady flow of oxygen. Simultaneously, they carefully slid a backboard beneath her, immobilizing her spine and neck to prevent any further damage during transportation. Moments later, an ambulance sped onto the field. Y/N, still unconscious, was swiftly and gently transferred onto a stretcher, her body secured and placed into the ambulance. Leah and Jessie immediately followed behind inserting themselves into the ambulance not caring if they were in the middle of a match.
As the ambulance raced towards the hospital, the sound of the siren echoed in the confined space causing Y/N to begin to stir. Her eyelids fluttered open, and she found herself disoriented, with the oxygen mask covering her face. In her groggy state, she attempted to remove the mask, her hands reaching up to pull it away.
Leah noticed Y/N's movement and gently placed her hand over Y/N's to stop her. "It's okay, love," she reassured, her voice soft and soothing. "You need to keep that on for now. It's helping you breathe."
"Y/N, it's okay," Jessie whispered, her hand resting on Y/N's arm. "You're in the ambulance, and we're on our way to the hospital.”
Y/N's eyes shifted from Leah to Jessie, her gaze still hazy. She attempted to speak but found it difficult. The words came out slurred and unfocused. "Why...hospital?"
Leah's fingers gently brushed Y/N's hair back from her forehead. "You had an accident on the field, love. The medics are taking you to the hospital to make sure you're okay. We're here with you, and everything will be fine."
Jessie leaned closer, her voice soothing. "Just relax, Y/N. The hospital will take good care of you, and we'll be right there beside you."
Y/N, though still disoriented and in pain, found some comfort in their presence. She nodded weakly and allowed them to reposition the oxygen mask, focusing on their voices to keep herself calm.
#woso x reader#woso fanfics#arsenal wfc#arsenal x reader#leah williamson x reader#leah williamson#jessie fleming x reader#jessie fleming#soccer#soccer fanfic#hurt/comfort
561 notes
·
View notes
Text
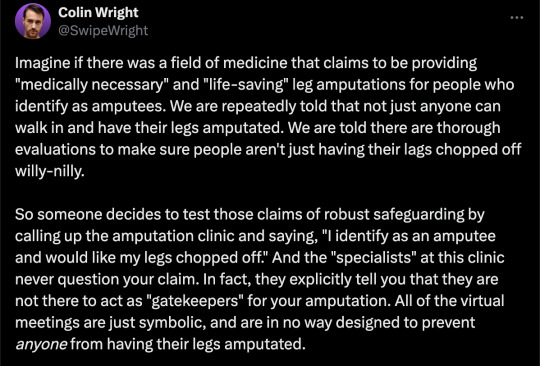
Zails the Zone Cop NSFW Headcanons
Zails x Reader
NSFW Headcanons
Short Concept

Potential ⚠️TWs⚠️ :
Both reader+character are of legal age or aged-up for obvious reasons in this post!
These are smut headcanons, read at own risk. !Female!dom!Reader+sub!Zails • Eating his darling out • Drooling/salivating • He gets a bit rabid with it
Ah, wowie. Zails getting himself a girlfriend? I thought it would never happen... but let me tell you that Zails is truly one of the most hopeless and desperate variant of Tails that exists. He would be so needy for constant affection and reassurance, but he'd also be quicker to grow a lot more ...horny than the rest of the bunch. Even if he constantly has his grabby fingers all over you, a singular touch from you can easily trigger his sensitive nerves, leaving him an aroused mess.
And if you gave him permission to taste your cervical fluids? That is 111% the worst idea I’ve ever heard in my life and you absolutely should do it because it would absolutely shatter Zails the best way possible. He would instantly fall and completely melt into a drooling mess and beg you for a chance. He’s not used to those sweet, sweet fluids and he is absolutely not stopping until he has to be pried off of your body with a crowbar. He would be in pure ecstasy and nobody would be able to separate him from you anymore.
It would be the worst thing Zails has ever felt, and he wouldn’t be able to think straight anymore due to how much he would enjoy it. He’d be making pathetic groaning noises and his leg would shake uncontrollably. You would be his whole world at that moment, he wouldn’t even hear it if there was a volcano exploding outside his house. There would be no way for him to recover from that at all.
Tell him to not dare disappoint you while does the deed.
Cause that, my friends, would be the end of everything for Zails because that would literally be the final blow. His legs would go numb from the ecstasy as he softly moans into your entrance, tongue working overtime just to enjoy the sweet and divine taste. His mind would become completely flooded with hormones that would leave him absolutely dizzy. His whole world has been flipped upside down and he would NEVER recover from this.
He’d be so weak-minded that he wouldn’t be able to think of anything else but making you feel satisfied as his eyes would roll back and moan louder into you, not wanting it to stop. He would be completely addicted to the taste, and the sound, and the sight of the whole thing. His tongue deep inside of you getting every drop of nectar he can. I can see his tongue would become more desperate with its movements to try and taste even more of you. Becoming more vocal as it reaches deeper into your body, his tongue being in this hot, moist and tight claustrophobic space, with juices soaking his already wet tongue.
And by the time he reaches that level of desperation, he’d be nothing short of rabid. His tongue would move at rapid pace as he just tries to get more of every single drop, his brain just melting to the point he feels like a drooling animal. And the more he gets the more desperate he becomes, he would feel your hands on his back and he would get more desperate. He’d start licking anywhere you touched him, just praying for more. His body is nothing more than a shell anymore.
Which is the perfect comparison honestly, he’d be acting like he was on death row and this was his last meal before dying. He would be lapping up everything like a dog that wasn’t fed for weeks. And if you decided to actually allow yourself to climax, oh lord, that would be the biggest shot of pure ecstasy he could ever experience. It would absolutely break him to the bone. He would feel like he didn’t deserve to live for being able to experience that kind of blissful experience.
You'd have a grip over his tongue since the start of the interaction, and it would get progressively tighter until it would become unbearable. His breathing would get heavier and he’d start to moan so loudly, but you could definitely make him feel the lowest he could possibly be. He’d be trying to reach a deeper level while you can enjoy every moment of him being helpless in your grasp, sitting on his face once he’s ready to burst.
Zails would absolutely need a full body suit just to keep all the drool in his mouth because he’s actually just a mess of an entity at this point. He’s nothing short of a starving animal in heat who would have no care about being overstimulated. And if you were to let out a sound that even remotely resembles a moan, he’d be a goner. He’d go insane on you and you may as well just be giggling the whole time over him melting and making a mess. He is completely broken at this point. All it takes is a single sound.
And that, I think, would cause his mind to completely snap. He would be completely overrun by his own emotions and be in complete euphoria, yet so filled with desire too. He would reach a point where even days after the experience, he will literally be begging for you to let him drink from your fountain of life again. You would not only see the desperation in his eyes, but you could feel it in his entire being. And his body would be shaking all over, as if in a fever, unable to contain all of that need inside ever again.
A need he didn't even know he had.
#zails the fox#zails the zone cop x reader#zails#zails x reader#zails the zone cop#sonic smut#sonic x reader#sonic the hedgehog x reader#tails x reader#tails smut#sonic comics x reader#sonic comics#sonic the hedgehog
78 notes
·
View notes
Note
hi cervical delving, was wondering if you think isopods are more comparable to cows or horses IF we were small enough to milk / ride them. their many pretty patterns remind me of both, honestly. but i dont know much about isopods. i like to imagine owning large fields of them and they also large, but i hate the thought of putting them through the industrial torture cows go through... i understand there is a more comparable cow beast that ants milk, but
in my bugs-as-vertebrate fauna understanding I see isopods as rodents actually; they’re incredibly prolific and numerous where they exist, can eat anything and have these nasty little gnawing mandibles that can cut through whatever they want. being small enough to ride an isopod would be like riding a giant rat & probably either would kick you off its back and then eat you, bones and all. I have seen hungry isopods tear into their molting brethren and fight one another to eat live beetle larvae. they have been known to bite holes into the tarantulas and centipedes people mistakenly cohabitate with them thinking the isopods will “clean up” the enclosure. as soon as the predator molts they’ll clean the enclosure really well. isopods are a menace
millipedes are probably more your speed and I could imagine a relatively peaceful millipede farm with a bunch of big spirobolids munching on a bale of old rotten wood. not sure what you’d milk them for other than benzoquinone defense fluid. or in the case of flat millipedes maybe bottling their cyanide gas for chemical reagents
94 notes
·
View notes
Text
This post is super TMI 😬
Sooooo for the first time in almost exactly 3 years, we had unprotected sex. I was so terrified of the thought of doing this until the last few months. I remember the first 2 years PP, I was so scared that the thought of having UP sex and risking pregnancy literally revolted me. I can’t believe that at 3 years PP, even hours later, I’m hoping that we made a baby. That I’m excited to be back in this space, knowing everything I know about pregnancy, labor, and PP depression. Like… I really want this. It will be different in so many ways and whether I’m pregnant now or will be in the future, I’m excited.
Before I got pregnant with Sky (like way before) I dreamt of an Aries baby. She ended up being an Aries. For a long time, I’ve had this gut feeling this next baby will be a Sagittarius baby (if I am pregnant, due date would be in Sagittarius season). I know it’s so silly to some, but way back in 2017, I was in India and I got a natal chart reading. The lady told me I’d have 2 children, born in 2021 & 2024. I remember being low key outraged like… WHAT DO YOU MEAN???? I’m not going to wait that long to have a baby… but then we took another big trip, then we moved to NYC, and then it took me a year to get pregnant. (I got pregnant the literal month after I was told by my GYNO that all my fertility tests came back totally fine and truly believe stress kept me from conceiving)
I also remember thinking 2021&2024… kids 3+ years apart????? I would never do that, my kids are going to be less than 2 years apart … and the reader was very no nonsense, like… honey, this is what it is. I’m just reading what I see. I’m really hoping the lady is right 🥹✨(although I know I know, first time trying and getting pregnant is rare)
I’m going to go buy prenatals today and start taking those ASAP. I just have to pray for the best. I’m healthy, eat well, I’m back at my PP weight, and I didn’t overthink it. I just told Kevin I was ready and he obliged happily 😂🙈
I’m very familiar with FAM and track my cycle every month. Yesterday, before we had sex or knew that we would have sex that day, I wiped in the bathroom and was like WHOA — if I wanted to get pregnant today, pretty sure I would have a good chance. I was also having ovarian pain, which is my telltale sign that ovulation is gearing up to happen. After so many years of tracking with temps and OV sticks, I know my body very well. I’m very grateful that my cycle is consistent —every 25-30 days, I get my period. I checked my tracker app late last night and saw that I was on CD13 and due to OV in 1-3 days (can’t know for sure without BBT but once cervical fluid is dry, that’s how one knows OV has happened).
Ahhhh I just can’t believe it. I’m back in “not trying, not avoiding” and I’m excited. I want another little baby to hold and love. I want Sky to have her own baby sibling ✨🙏🏽🤍
33 notes
·
View notes
Note
hi sex witch! is it normal to have a lot of white-grey discharge? like to the point where i have to keep using my menstrual cup for a couple days after my period and during ovulation so i don't soak through my pants?? it's usually a couple ounces worth of fluid and pretty watery..
hi anon,
while it might be a pain, what you're describing is SUPER common and generally not considered a cause for concern unless you're also experiencing symptoms like a heavy fishy odor, itching or burning around your genitalia, or pain when urinating.
the kind of discharge you're describing is most likely a combination of cervical mucus and other "fertile fluids" that are meant to help sperm more effectively reach an egg to fertilize; if that doesn't happen, it gets flushed out like your uterine lining. you may be experiencing it in higher quantities than the average person, but like I said, there's nothing inherently unhealth about that, and a menstrual cup is a smart way to handle it!
19 notes
·
View notes
Text
bodily fluids ranked worst to best based on how much i hate handling them
poop < chunky stomach contents < chyme < bile < semen < urine < cervical mucus < vitreous humor < cerebrospinal fluid < ascites < blood < serous fluid < synovial fluid
#the definitive list! if u disagree then argue your point and i may edit#other stuff like saliva idont rlly ever have to deal with#synovial fluid wins bc its inherently fun to play with#semen is low in the list not bc its gross to deal with but because. the Connotations
13 notes
·
View notes
Text
It did not seem like a good thing when a precious consignment of human tumour samples on its way from Kampala, Uganda, to Heathrow was diverted to Manchester. When the samples finally arrived at the Middlesex hospital in London, they were swimming in murky fluid in their vials as though they had been infected with bacteria.
But when the pathologist Anthony Epstein looked at the fluid under the microscope he saw no bacteria, just individual cells that had been shaken loose from the tumours. And that was just what he needed in order to search for elusive virus particles and test his hunch that they were causing cancer.
In the early 1960s Epstein, who has died aged 102, had heard a lecture by Denis Burkitt, an Irish surgeon working in Kampala, that described strange tumours (now known as Burkitt lymphoma) growing around the jaws of children in equatorial Africa.
Intriguingly, the geographical distribution of the condition seemed to depend on temperature and rainfall, suggesting a biological cause. Epstein, who had been working with viruses that cause cancer in chickens, immediately suspected a virus might be involved, perhaps in association with another tropical disease such as malaria.
Epstein began to collaborate with Burkitt, who supplied him with tumours from children he had treated. But Epstein’s efforts to grow pieces of tumour in the laboratory and isolate a virus had all been unsuccessful until the dissociated cells arrived.
With his graduate student Yvonne Barr, he then decided to look at cultures of these cells in an electron microscope, a powerful instrument that had only recently become available in his lab.
The very first image showed a tell-tale outline that looked like one of the family of herpes viruses. It turned out to be a previously undescribed member of that family, and was given the name Epstein-Barr virus. In 1964, Epstein, Barr and Epstein’s research assistant, Bert Achong, published the first evidence that cancer in humans could be caused by a virus – to be greeted by widespread scepticism even though they went on to demonstrate that EB virus caused tumours in monkeys.
Thanks to samples supplied by Epstein, in 1970 Werner and Gertrude Henle at the Children’s hospital in Philadelphia discovered that EB virus also caused glandular fever. That made it possible to design a test for antibodies to the virus in order to confirm a diagnosis. EB virus turned out to be very common, infecting most children in early life, though it usually causes glandular fever only in older teenagers and young adults. As well as causing Burkitt lymphoma in endemic areas in Africa and Papua New Guinea, it is also associated with a cancer of the nose and throat that is the most common cancer of men in south China, as well as cancers in people whose immune systems have been compromised, such as those infected with HIV.
More recent research suggests that EB virus might also be involved in some cases of multiple sclerosis, and that people who have previously had glandular fever are more susceptible to severe Covid-19.
After the discovery, Epstein and others devoted time and effort to trying to find out under what circumstances EB virus causes cancer. The relationship between the virus, other diseases, human genetics and cancer is complex, and it took decades before the medical community could accept the EB virus as a cause with confidence.
Not until 1997 did the International Agency for Research on Cancer class it as a Group 1 carcinogen, formally acknowledging its role in a variety of cancers.
The discovery of EB virus opened up a whole new field of research into cancer-causing viruses. It also raised the exciting possibility of preventing cancers through vaccination, an advance that has now been achieved in the case of human papilloma virus, which causes cervical cancer, and hepatitis B virus, which causes liver cancer.
By the time of his retirement in 1985, Epstein’s research group at the University of Bristol had developed a candidate vaccine that protected monkeys infected with EB virus against tumours, but neither it nor any other candidate has yet been successfully developed for human use.
Epstein was born in London, one of three children of Olga (nee Oppenheimer) and Mortimer Epstein. Mortimer was a writer and translator who edited The Statesman’s Yearbook for Macmillan from 1924 until his death in 1946. Olga was involved with charitable work in the Jewish community. Anthony attended St Paul’s school in west London, where the biology teacher Sidney Pask encouraged boys to go far beyond the syllabus and whose pupils also included Robert Winston and Jonathan Miller.
Epstein won a place to study medicine at Trinity College, Cambridge. He moved to Middlesex hospital medical school in wartime London to complete his training, before doing his national service in India with the Royal Army Medical Corps. He returned to work at the Middlesex hospital as assistant pathologist, conducting his own research. Thinking electron microscopy might be useful in his studies of cancer-causing viruses in chickens, he spent some time learning the new technique at the Rockefeller Institute in New York (now Rockefeller University). Not long afterwards he attended Burkitt’s lecture and began the serendipitous route to his discovery.
In 1968 he was appointed professor and head of the department of pathology at the University of Bristol, where he remained until his retirement. He moved to Oxford as a fellow of Wolfson College in 1986, becoming an honorary fellow in 2001.
An exemplary scientific good citizen, he served as foreign secretary and vice-president of the Royal Society, and sat on boards and councils for numerous national and international research organisations, including as a special representative of the director general of Unesco; he was also a patron of Humanists UK. Among his many prizes and honorary degrees, he received the international Gairdner award for biomedical research in 1988. He was appointed CBE in 1985 and knighted in 1991.
“It was a series of accidents, really,” he said of his discovery in a conversation with Burkitt they recorded for Oxford Brookes University’s oral history archive in 1991. “Lucky quirks.” Burkitt immediately responded with Louis Pasteur’s aphorism: “Chance favours the prepared mind.”
Epstein was a deeply cultured man who retained a lively interest in many subjects – particularly oriental rugs, Tibet and amphibians – until the end of his life.
He is survived by his partner, Kate Ward, by his children Susan, Simon and Michael, from his marriage to Lisbeth Knight, from whom he was separated in 1965, and who died in 2015, and by two grandchildren and two great-grandchildren.
🔔Michael Anthony Epstein, pathologist, born 18 May 1921; died 6 February 2024
Daily inspiration. Discover more photos at Just for Books…?
13 notes
·
View notes
Text
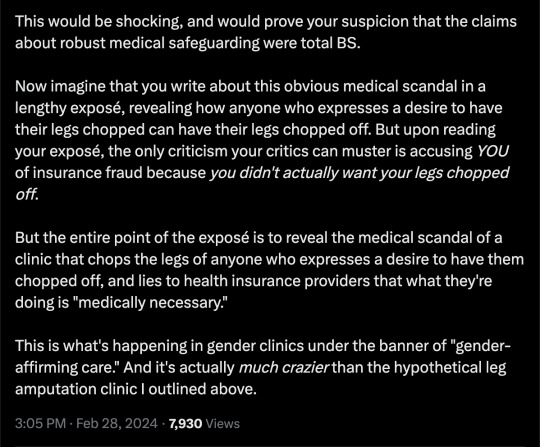
Time for your check up
kinktober day nineteen
Hatori Sohma x reader
warning: work sex, suducing, peer pressure??, fingering, penetration?
a/n: sorry for not finishing completly, i've lost motivation for this fic and im going through a writers block.

You were lead into the exam room by Dr. Sohma. You hop onto the exam table, crossing your legs in a flirty matter. Dr. Sohma ignores it, and focuses on the matter of hand. And turns his back to you to pull up your chart on the computer. You start to unbutton your stylish trench coat, and put yourself in an suggestive pose. He turns around looking down to his clipboard “So miss y/n, your here fo-“. “I’m ready for my check up, doc” you interrupted him. While you look up at him with sparkling eyes, twirling your hair with your fingers.
He stares at you completely surprised, before he lets out a sigh. “Y/n I thought we spoke about this, we can’t be doing this at my work anymore.” He warns. “Oh Hatori” you say to him seductively, while you stand up from the table putting your hands on your lover’s chest before your press your breasts against him. “How else are we going to get together with us being on the down low” you say while playing with his tie, giving him the sweetest puppy dog eyes. “I can get you a different doctor.” Hatori says in a professional matter.
Even though you both know he wants to take you right there and now, but also wants to keep his job. “No other doctor can help me the way you can” you say while you remove his tie. Kissing his neck while you slip off your coat so your stark naked. Hatori looks away trying not to lose his composure, him being stubborn.
At this point your kinda miffed that he’s not falling for it. You peel away from him to take a seat on the exam bed. Spreading your legs apart so he can see your glistening pussy. You look up at him, while you proceed to touch yourself. You start to gently pant while you stick a finger into yourself. While Hatori just watches you, while biting his lip.
You start pumping your finger in and out. When you questioned “Shouldn’t you be doing my ‘cervical check’? You are the professional after all.”. Hatori can’t deny you, no matter how much he wants or needs too. But he can’t resist you and you always get what you want. He grabs your hand removing it from your pussy, making you whine at the absence. Which has him quickly replace yours with two of his, leaning down to kiss you. You moan, relishing at his touch and finally getting what you have wanted.
Your cunt drips fluids onto the paper wrapped around the table below you. Making it cling onto your ass. As you open your mouth for Hatori to slid his tongue in. Giving him complete access to your mouth as he explores. You start to unbutton his shirt, the horny little minx you are can't wait any longer. But knowing Hatori he won't let you leave him completely naked at work. So instead of removing his coat and shirt, you move to unbuckle his pants. In that moment he curves his fingers so they hit your sweet spot perfectly. Making you squeak out and falter you movement on his zipper.
Once your finished unzipping his pants, you hook your fingers to in his boxers to lower them enough to free his cock. Hatori takes this as his queue to lean closer to you. Grabs his cock to rub his mushroom shape tip against your clitoris. While he continues to pump his fingers. Making you whine at the added stimulation. His precum mixing with your slick.
He continues to rub circle into your clit. Making you shudder against him. As you clamp down on his fingers. An unexpecting orgasm hits through you, making your body tingle. Which has Hatori quickly remove fingers to replace it them with his cock. So he can help you ride out your high and he can start to chase his.....
#fruit basket#fruit basket smut#hatori sohma#hatori x reader#hatori smut#hatori sohma smut#hatori sohma x reader#Hatori Soma#Hatori Soma smut
141 notes
·
View notes
Note
omg beloved cato....what thought did you have....
darling vic...🙈 i was just thinking... you know... how eager Touya gets, right?
And how much he enjoys making a mess of you, or if you're already a little messy and bloody, for some reason, how cute he looks licking up all that extra fluid; the way he'll come away from you with a thick string of cervical mucus still attached to his tongue.
he gets a bit lovesick over it, don't you think?
#sorry u caught me right when i needed to wash my dishes but here i am#he's disgusting and i love him for it#i would allow him. to do things to me. when i was on my. period.#'s*x helps the pain'-guy#caitie answers#gen#vic!!#saintshigaraki#menstruation tw#body fluids tw
7 notes
·
View notes
Note
I have a question about 3rd trimester abortions that I can’t find the answer to on Google!
When I had my baby, I had to be induced at 38 weeks for cholestasis. They tried multiple different induction methods for 36 hours, and my cervix barely ripened and I did not even kind of go into labor. I had misoprostol, cervidil, catheter balloon, and I got up to the max dose of pitocin. Eventually they gave me the option to keep trying or get a c-section. I happily opted for the c-section. My baby was never in distress and we were both 100% safe and healthy the entire time. It was a very non-emergent c-section.
I’m assuming part of why I couldn’t go into labor is that my body was in no way ready for it. The induction (and eventual c-section) was 100% medically indicated and things happened the way they needed to happen. No complaints here.
I guess I’m confused about why that wouldn’t happen during a late stage abortion. Does it happen? Are there people who never are able to go through cervical ripening or dilation? If an abortion is very late (I know someone who had to have one at like 37 weeks), doesn’t labor need to be induced? Can’t it just not happen? Does it ever not? Then what? Thank you!! :)
Hi there! I'm so happy to hear that you and your baby had a safe labor and birth experience, even with the failed induction attempts! I'm answering your question under a cut. To others: all the expected content warnings apply.
I think this is a super interesting and reasonable question to have! To be totally frank, this does not happen because there are just many, many more interventions available when the desired outcome is not a healthy mom and baby.
Late term abortions are typically done over four days, with mechanical dilation occurring over the first 72 hours (so twice as long your induction was attempted, primarily by chemical methods besides the foley catheter). The cervix is opened with increasingly large osmotic dilators (osmotic: they go in smaller, absorb your body fluid and expand over several hours) that are placed and replaced every 24 hours, in addition to being given the misoprostol/cervidil/mifepristone/pitocin etc used to induce normal labor. The cervix can be further opened by passing through metal dilating rods that would injure (maybe fatally!) a healthy fetus. Fetal death itself, which is induced before the first osmotic dilators are placed, also seems to contribute to preparing the body for labor.
In all honesty, the limiting safety factor for most induction interventions is baby, not mom. In addition to being able to use more physically forceful methods of dilation, different medications or doses of medications, etc, fetal delivery in a late term abortion doesn't have to occur intact. In many late term abortions, patients want remains to grieve and bury and this is definitely something that guides care, but the abortions later in pregnancy that I have assisted essentially never result in complete fetal remains. This means you do not need 10 full centimeters of dilation to get all tissue out.
I asked one of the attendings at work a similar question a few years ago and in 25 years of abortion care he personally had never seen an abortion performed via cesarean. There are certainly cases where fetal death has occurred or is likely to occur and a csection is performed (the zavanelli maneuver for example, when the head has passed through the cervix but the shoulders are unable to, so the head is reduced back into the uterus in anticipation of csection, has pretty poor survival rates for baby; if placenta is disengaging, a lot of times it is the only option to get mom out safely) but I think in planned abortion, it is either exceedingly rare or just doesn't happen.
11 notes
·
View notes
Text
astro theory 2: organs/systems by ruler
everyone and their mother has their opinion on what body parts are ruled by which sign, including myself. maren altman described saturn in pisces as a time when one thing questioned would be bodily autonomy, so let's ring in this transit with a small anatomy lesson (if we have any activists here, i'd like to thank you in advance for the next 3 years, as they are going to be very important for you) on my opinions of what rules what.
the traditional western view (being general; not citing anyone specific in case of plagiarism accusations) was to 'slice' l'uomo vitruviano into 12 parts from top to bottom and label them like this:
aries: head/face/brain
taurus: neck/throat
gemini: hands, arms, shoulder area
cancer: chest, cervical spine area (of back), ribs
leo: heart, thoracic spine area
virgo: belly (under chest to navel/above hips), lumbar spine area
libra: navel until hip line
scorpio: genitals
sagittarius: thighs
capricorn: knees
aquarius: calves
pisces: feet
eastern astrology has a few interpretations but here's the one written by sanjay rath, based on traditional planets and organ systems:
sun: skeletal
moon: circulatory
mercury: nervous & integumentary
venus: reproductive
mars: muscular
jupiter: digestive
saturn: excretory

i disagree with both (eastern seems to fit my interpretation better though) as modern medicine has come a long way since then - while it may not be accurate for everything, as discoveries and advances will still and always will still be made, we can categorize some beliefs from the past as (generally) untrue.
i personally agree with putting signs as body part (if i say systems I'm talking about multiple body parts, rather than them working together) rulers and planets system rulers.
i'm starting with signs and then following with planets, as this seems like the more logical order. I can't list every body part, but it will be very detailed - comment/message and if i think it applies i will add it (cells/intracellular fluids do not have specific rulers).
aries/1st: skin, hair, nails, epithelial tissues
taurus/2nd: heart, veins/arteries
gemini/3rd: cerebellum, frontal lobe, occipital lobe, cns (including eyes)
cancer/4th: interstitial fluids (lymph, pus, spit, breast milk, etc.), eggs/sperm
leo/5th: blood (connective tissue)/intravascular fluid
virgo/6th: stomach hydrochloric acid, temporal lobe, parietal lobe, pns, ens
libra/7th: remaining connective (including osseous)
scorpio/8th: mesenchyme (connective) tissue, nephrons, cartilage, extracellular matrix
sagittarius/9th: enzymes, steroid/adrenal hormones*
capricorn/10th: joints, muscle tissues, protein (peptide/amine/glycoprotein) hormones
aquarius/11th: glands, lungs/airway, uterus, testes
pisces/12th: adipose tissues*
now for the slightly easier parts, planets in the modern order (why didn't i include rising? look in your first house - above in sign/degrees/house list with aries).
sun: fluid-based (lymphatic) immune**
moon: reproductive
mercury: nervous, digestive/excretory
venus: circulatory
mars: integumentary (exocrine)
jupiter: lipid structures/steroid-based endocrine*
saturn: musculoskeletal, protein-based endocrine*
uranus: respiratory
neptune: response-based immune* **
pluto: non-digestive excretory
*why are the jupiter signs not concrete? (aka i am preparied for the slander). jupiter and neptune are the 'expansive' and 'shadowy' planets (or as i like to say the 'overt/covert' planets) which means that unlike the other planets, there is not an easily decipherable concrete form (actually for the sake of technicality, there is a concrete form but its so large and made of so many parts that it is hard to see - think air molecules). jupiter being expansive is not the reason why it represents fats - jupiter's supportive nature (whether wanted or not) makes it the planet for fats. additionally, sagittarius which traditionally responds to gets tasks done quickly (whether correctly or not) represents every enzyme and steroid response. also saturn -> time -> growth.
**immune system is divided into: first the 'drainage' which is what the lymph picks up before being drained into lymph nodes, filtered and sent back to the bloodstream. 'but the sun is the outwards expression of personality' - hold on - the sun needs to 'take stock' of the other plants before expressing their desires in the 'sunny (lol) fashion' and it can only do this by passing through everyone else and collecting the inputs. the lymphatic network goes literally everywhere in the body and drains any 'extras' and doesn't make it waste - it eventually sends it back into the bloodstream. second the 'responses' - which is made of other parts of other systems working together. in the illusory nature of neptune (as described above) it makes sense to have the system that is not 'seen' but still works to defend from behind the scenes.

this is my theory but feel free to comment your questions and opinions if you have any - i'm interested in people's responses (and potential jupiter signs slander) - as I said, any input that I think applies may be added.
anyways,

~ Lala
41 notes
·
View notes
Text
cervical fluid did you mean jungle juice
3 notes
·
View notes
Text
Kinktober Day 2: Medical Kink with Simpbur
DID WE SAY THE RETURN OF DOCTOR SIMPBUR AND HIS OBSESSION WITH A PATIENT!??
No? well then, here have some good old medical malpractice with a creepy old simp!
MINORS DNI!
Out of all his patients, you were his favourite, eager and ready for more experimental treatments, taking new pills and fluids at the drop of his hat. There was nothing he felt he couldn't do, the sight of you spread out before him be it in the stirrups that were for cervical exams or barely coherent against his examination bed, you were always so perfect, smiling at him as he swirled fluids, flicked needles, or rattled pill cases, ready with your rights signed away in that little medical test agreement.
The test for today was one he had been looking forward to for so, so long, the very idea of seeing you stripped bare and ready for him to administer the trial drug was driving his strides and making him more personable to his coworkers than ever before, the door to your observational room was quiet as it opened, two small clicks before he was locked in with you, gloved hands shaking as he took up your chart.
Everything that was listed was up to date and accurate but it was a habit to flick through the pages and smile as you blinked awake, staring at him as he came to sit by your bedside. eyes crinkling to show he was smiling behind his mask, teeth digging into his bottom lip as you yawn and stretch, still so sleepy after the initial application of the trial drug, your voice scratchy and rough as he waited for answers to his questions.
But the moment you had answered it was time for him to enjoy, to revel in what he was about to do, to savour as you tipped your head back mouth open wide and tongue lolling out as he changed his gloves, the white latex so stark against the pink of your tongue.
There were strings of spit connecting his fingers to your tongue, the sight of your mouth open like this, tongue nestled between the white of his gloved fingers, lips slowly becoming slick as he move around pretending to look down your throat for changes or reactions to the drugs running through your system, and yet with hazy eyes you still couldn't catch as his eyes watch the movement of your tongue.
Taking every twitch and unconscious movement of the wet muscle, mind racing about having you like this mouth open, drooling and waiting for the weight on your tongue, maybe it would be his cock, maybe it would be his fingers again but bare, skin on skin as he fucked your mouth, letting your drool and choke on him.
God if only you had signed up for the sleep study happening in two weeks, he would have devoured you, played out every fantasy, the results be damned, he would have fucked you while on EKG or while the rest periods ran.
But for now, he would have to commit this moment to memory, keep the sight of you drooling around his gloved fingers, eyes half-lidded as they looked up at him eager for his words, his attention, his anything.
Lord forgive him for what he was going to do in the rest bunks the moment his shift ended, thankfully the sheets for that room get mixed with the patient ones, no one would bat an eye at a few sheets being just a little stained and damp, no one at all…
Maybe he could get a moment and change your current ones with the ones he was about to soil, yeah… Yeah maybe he would, how else would he get to mark you up with his cum.
93 notes
·
View notes
Text
Differences in cervical cancer screening guidelines around the world
When looking for information about cervical screening* I noticed that the guidelines differ from country to country, and that even supposedly reliable sources offer rather inconsistent and often contradictory information. The point of this ‘survey’ is to find out more about the cervical cancer screening recommendations (and gynecological care in general) around the world, and to start an open discussion about this. The questions and more info are under the cut.
Reblogs are welcome but I realize this is a sensitive topic. If you don't want to publish this post and your answers on your blog, answering the questions in the comments is more than enough. If you want to respond anonymously, you can put the answers in my ask box.
1. Where do you live?
2. What is the recommended age for starting cervical cancer screening (also called pap smear, smear test, or cervical cytology) in your country?
3. Is cervical cancer screening in your country recommended for people who have never had any kind of sexual contact? Is it recommended for people who have never had penetrative vaginal intercourse?
4. What information about hymens** have you been taught in sex-ed class, biology class, or told by healthcare professionals? Do doctors in your country try to avoid tearing the hymen during exams if the patient has a small hymenal opening (for example using smaller instruments)?
5. Have you ever been pressured into a gynecological exam or procedure that you didn't want or didn't think you needed?
6. Have you ever been discouraged or prevented from getting a gynecological exam or procedure that you thought you needed?
Feel free to share any opinions or experiences relevant to this topic.
* Cervical cancer screening, pap smear, smear test, or cervical cytology is a medical test that examines a sample of cells from the cervix (a part of the uterus that protrudes into the vagina) and often helps detect pre-cancerous or cancerous changes early enough to treat. A speculum or a similar instrument is used to visualize the cervix; and a brush, a cotton swab, or a similar instrument is used to collect cells from the ectocervix and the external cervical os.
** The hymen (also called the hymenal ring or the vaginal corona) is a thin piece of mucosal tissue that surrounds or partially covers the vaginal opening. In the past it was often assumed that hymenal tissue always tears and bleeds during the first intercourse, which is of course an inaccurate and heteronormative overgeneralization. The thickness and elasticity of the tissue, and the size and shape of the opening (or sometimes multiple openings) are extremely diverse. Some hymens are fragile enough to tear during completely non-sexual activities, such as sports, some can gradually stretch out or wear down with tampon use, some can accommodate even penile penetration without tearing. Some people with vaginas are born without any hymenal tissue at all, and on the other side of the spectrum there are hymens that can't even let menstrual fluid out of the vagina so a surgery is necessary to create a sufficient opening. Some people don`t experience any discomfort when the hymenal tissue stretches or tears, while others feel significant pain.
#gynecology#gynecology tw#cervical screening#pap smear#smear test#healthcare#feminism#informed consent
43 notes
·
View notes
Text
AITA for pulling the cancer card to shame someone and drawing attention to myself in a party?
Seven years ago I had cervical cancer, which wreaked havoc on my life in a lot of ways. Perhaps stupidly but I was more upset about losing my hair than I was my fertility, at least at first. I used to have long hair, rarely ever cut it, but shaved it during the course of chemo. Even after treatment, after remission, I found that I felt empowered by my new hairstyle (mostly what it meant to me) and kept it short. Recently I’ve been diagnosed with vaginal cancer. Thankfully we caught it early so hopes are high, but I won’t lie that I’m not upset that this is happening to me again. This upset has led me to be tetchy.
My brother and his new girlfriend and newborn flew in for a visit, for the first time since the baby was born. This is the first time in years we’ve seen him, except for video calls, because they’re out of country now. She’s a sweetheart but kind of blunt. Over the course of the party: She pointed out that my haircut made my face look round - but that’s the chemo causing fluid build up. She asked me multiple times if I was sure I didn’t want a drink, mostly because she was also getting herself one. She also said I was very confident to avoid wearing jewelry with such short hair; again she is a little lacking in social mores but still she’s very genuine in what she says.
I just got sick of answering questions about my lack of alcohol, about my haircut, about my face, so I snapped, admittedly. After she commented about my hair again I said, “I have cancer” very bluntly and too loudly. Many people overheard, which caused many eyes to turn onto us, during a party that was meant for my brother and his girlfriend.
My brother took me aside after everyone else had left the house and his GF was in the car. He said I made a scene. He expressed his sympathy that I was dealing with cancer again, but he said that he wished I chose a better time to reveal it, because it took away from his and his family’s announcements.
[view this story on reddit]
Feel free to make your opinion be heard in the comments/reblogs but keep it respectful. For detailed information please read the guidelines for commenting. Violations will lead to your comment being deleted and you potentially being blocked.
14 notes
·
View notes
Last Seen Blogs

nessa-elanesse-blog
Ralph Wiggum

appla1
Applla

doragifs
i deleted my old blog by accident whoooops

dumbsena
Untitled

futuregws
Fire breathing bitch queen