#puberty syndrome
Text
5 notes
·
View notes
Text
Understanding Puberty Syndrome
Puberty is a natural phase of human development that marks the transition from childhood to adulthood. It is a period characterized by significant physical, emotional, and psychological changes. Understanding puberty syndrome is essential for parents, caregivers, and young individuals themselves to navigate this transformative phase with confidence and knowledge.
0 notes
Text
#alana champion#amy dunne#patrick bateman#gone girl#american psycho#mitski#puberty 2#donnie darko#black swan#jane margolis#natalie portman#kristen ritter#girl interrupted#girl interupted syndrome#franz kafka#girlblogger#girlblog#girly#waifspo#femcel#divine feminine#girlblogging#female manipulator#manic pixie dream girl#lizzy grant#sad girl#sullen girl
266 notes
·
View notes
Text
Sad Boy Hours: Billy Batson

He's trying so hard to get the screaming adults in the room to just stop screaming at each other and be reasonable.
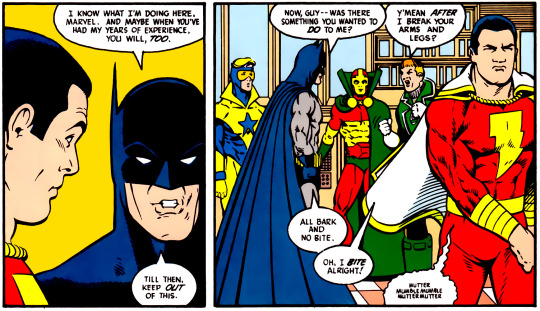
He is immediately dismissed and storms off, justifiably insulted.
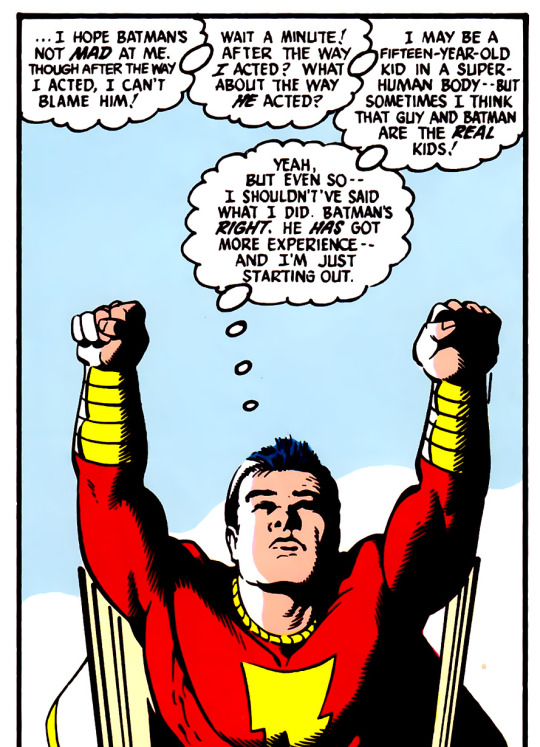
And Billy goes right back to blaming himself, trying to figure out where he went wrong, how he could have fixed things, managed the emotions of the room better--even though he is 100% correct and the adults are absolutely failing, and badly.
"Even if he's wrong...I should respect him." Honey, the thing that's eating at you is the absolute dogshit way they act and then expect you to just accept as normal. These grown-ass heroes should not be hitting each other.

And a degree, honey. Several of them.
He sounds like a teacher trying to get the class to behave and that script keeps failing him. Over and over the adults around him dismiss him for his optimism, ignore his calls for reason. And they're heroes. They're the good guys and they tear into each other regularly and viciously. And Billy is fifteen years old in a room of adults screaming at each other. The team is sometimes down right abusive, and this child is trying to keep them from falling apart.
I worry about him, ya know?
(anyway, thank you for coming to my Sad Boy Hours)
#justice league 80s#jli#justice league international#billy batson#shazam#dc captain marvel#i found so many moments of billy being an absolute sweetie pie and trying desperately to get people to get along#it kinda breaks my heart a little because he's just 15 and these are Grown Ass Adults in the MOST hostile work environment#i got a LOT of feelings about the Emotional Support Child#possibly eldest daughter syndrome but all the kids are older than you and y'all have no parents#he's literally a child soldier#kind of inspired by a fic i read the other day#and just watching billy get emotional slapped around because he Cares#sad boy hours#when the most mature person on the team is the only one who hasn't finished puberty#and i get this is kinda the joke but the sad boy hours got me so#ANGST#“its not that deep” IT IS TO ME
256 notes
·
View notes
Note

im getting you started.
Bro, the timeline in Carmen Sandiego is super finicky, and I'm pretty sure I've spent more time thinking about this than the creators intended us to, but WHATEVER. It haunts me.
Right, so the creators said Carmen is 20 at the start of the series, but as I said: that math don't math!
Season one takes place over the course of six months:

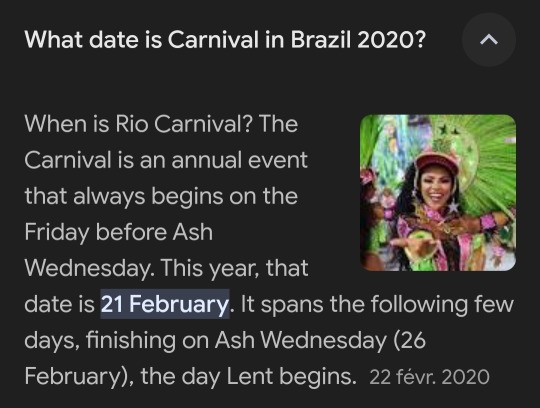
Season 2 picks up one week after season 1, in February. We know this because they're celebrating Carnival.
For the purpose of breaking down this theory, I'm going to place Carmen's birthday as March 1st, her WOEICs counterpart's official birthday.
So. At the end of season one, which would have been mid-February, Player says something about how Carmen was found on the side of the road twenty years ago, but if her birthday was in a mere matter of weeks, couldn't you theorize that he was rounding up? Maybe she's 19 turning 20.
Or, maybe, she's 20 turning 21? No!
At the end of season 2, Shadowsan says he found her twenty years ago. This is where we take a detour to discuss infant development.
In the flashbacks, we see that baby Carmen prefers crawling-- she can toddle a little bit, but not well. Children typically begin standing between 7 and 12 months, and walking between 10 and 18 months. We also see that she babbles and coos a lot, but no words. Children tend to say their first word at around 12 months. Based on this, I'd wager that baby Carmen was around seven or eight months old. We know she's a physical prodigy, so she could potentially be even younger-- the youngest recorded baby to walk was six months old.
Placing baby at 7 months when she was kidnapped, that makes Shadowsan's "I found you twenty years ago" accurate to the month. At this point, Carmen is 20 years and 7 months old.
Season three takes place in October/November. Presumably, season three picks up right after season two, putting the end of season two in October. It spans about the same length as season one.
While the word of the creators doesn't have much bearing here-- as this post is very much a "you guys are wrong and here's why" kind of post-- one of the creators did say that they imagined Carmen as being twenty by season three. That would make it impossible for her to have been twenty during season one. Too much time has passed for that to work.
Season 4 takes place sometime around February. We know this because Devineaux asks Gray what he was doing on the train to Poitiers 18 months ago. 12 months ago would have been February (start of season 2) and six months before that is August. That's eighteen months.
Going by this, I think Carmen was yoinked just after her twenty-first.
Interestingly, if my math is mathing-- and who knows, I turned a two year degree into a three year degree because I kept failing math classes, I could be talking actual nonsense right now-- this makes Player like 17/18 by season four, and that's hilarious to me because that means his parents (tried) to make him go to school for like the last semester of his senior year. Free my boy 😭
In conclusion, Carmen is 19 at the start of season one, she and Player are three years apart, and Player's parents are some cruel mfers. Thank you for coming to my TED talk.

#carmen sandiego 2019#carmen sandiego netflix#carmen sandiego#suzie speaks#asks#help girl im scrutinizing the CS timeline for the four hundred millionth time#if i missed something lmk#but i do believe my autism game was real with this one#thank you atlas for getting me started on my bullshit#also black sheep and player looked the same age#why did they make him so much younger than her#why does she longbottom puberty whereas player gets hit with that peter pan syndrome#help me im descending into insanity#cs timeline and ages will forever confound me thank you for your understanding
72 notes
·
View notes
Text
150 years ago, a boy was born to my great-great grandmother. And that was the last time that happened anywhere on my maternal line until my son was born in 2016. This is a story about intersex people.
For 150 years, the women of my family kept having daughters, who either also had daughters, or they were oddly unable to have children. Strange quirk, we assumed. No boys.
In the late 1970s, my mother’s sister had a daughter with Down Syndrome. Genetic testing was done, and it was discovered that although she looked female, she actually possessed the male XY chromosome combination. Her sister was born three years later. And because of that genetic concern, her genes were checked. And she possessed … the XY chromosomes. A third daughter, born a few years later, possessed the usual XX.
Keeping in the tradition, my mother had two daughters. Because of our cousins’ genetic conditions, my sister and I were both checked. Both of us appeared typically XX. And so for more than thirty years, it was dismissed as a quirk, and no one said the word intersex because that wasn’t a thing in 1980.
In 2016 I had a son, breaking the chain of girls. It was an interesting story! I then had two daughters, and didn’t bother to do any genetic checking.
And then in 2020 my sister became pregnant. Early genetic testing said boy, XY. Twenty week anatomy scan said girl. Definitely 100% girl. Uhhh?! As expected, she*** was born genetically male, possessing only male gonads in the form of undescended testes, but female external genitalia.
It was Androgen Insensitivity Syndrome, a genetic mutation carried on the X chromosome. See, all bodies start female. Then, when the hormonal influence of the Y chromosome kicks in, instructions on the X are supposed to detect the testosterone and create male genitalia. Except a person with AIS is non-reactive to testosterone, and the body stays, at least superficially, female. Genetic check would say boy. Presence of testes says boy. Pants check says girl. Making the question of sex (sex. Gender is something else, ok?) distinctly complicated.
If someone has a mother who is a carrier of AIS, there are 4 possibilities. Unaffected XY, and so genetically and structurally male. Affected XY, and so intersex. Affected XX, and so a female carrier. Unaffected XX female and entirely unaffected.
My grandmother was a carrier. My aunt and mother are carriers. My sister is a carrier. When my niece was born, my single non-intersex cousin and I did genetic testing. And we are both carriers as well. My son is an unaffected XY male. My niece is affected XY intersex. Both my cousin and I also have 2 daughters each. And, because it is medically and psychologically relevant, we had them tested. All XX.****
And I was ready to check one more thing: are my daughters carriers? There is a 50/50 chance. And then I stopped, because they are preschoolers, and that is their reproductive decision. They know three intersex people. And if they care, someday they can check their genes and the odds that my grandchildren will be intersex. The intersex people they know will, I hope, be able to talk to them about the beauty of their lives as one of the wonderful variations of humanity.

#***both of my adult intersex cousins identify as the female gender. For now so does my two year old niece pending future choices.#****the discovery that one is intersex is sometimes not made until puberty (doesn’t happen) or beyond.#Unusually in my family it is a part of their story from birth#intersex#androgen insensitivity syndrome
47 notes
·
View notes
Text
By: Jamie Reed
Published: Feb 9, 2023
I am a 42-year-old St. Louis native, a queer woman, and politically to the left of Bernie Sanders. My worldview has deeply shaped my career. I have spent my professional life providing counseling to vulnerable populations: children in foster care, sexual minorities, the poor.
For almost four years, I worked at The Washington University School of Medicine Division of Infectious Diseases with teens and young adults who were HIV positive. Many of them were trans or otherwise gender nonconforming, and I could relate: Through childhood and adolescence, I did a lot of gender questioning myself. I’m now married to a transman, and together we are raising my two biological children from a previous marriage and three foster children we hope to adopt.
All that led me to a job in 2018 as a case manager at The Washington University Transgender Center at St. Louis Children's Hospital, which had been established a year earlier.
The center’s working assumption was that the earlier you treat kids with gender dysphoria, the more anguish you can prevent later on. This premise was shared by the center’s doctors and therapists. Given their expertise, I assumed that abundant evidence backed this consensus.
During the four years I worked at the clinic as a case manager—I was responsible for patient intake and oversight—around a thousand distressed young people came through our doors. The majority of them received hormone prescriptions that can have life-altering consequences—including sterility.
I left the clinic in November of last year because I could no longer participate in what was happening there. By the time I departed, I was certain that the way the American medical system is treating these patients is the opposite of the promise we make to “do no harm.” Instead, we are permanently harming the vulnerable patients in our care.
Today I am speaking out. I am doing so knowing how toxic the public conversation is around this highly contentious issue—and the ways that my testimony might be misused. I am doing so knowing that I am putting myself at serious personal and professional risk.
Almost everyone in my life advised me to keep my head down. But I cannot in good conscience do so. Because what is happening to scores of children is far more important than my comfort. And what is happening to them is morally and medically appalling.

The Floodgates Open
Soon after my arrival at the Transgender Center, I was struck by the lack of formal protocols for treatment. The center’s physician co-directors were essentially the sole authority.
At first, the patient population was tipped toward what used to be the “traditional” instance of a child with gender dysphoria: a boy, often quite young, who wanted to present as—who wanted to be—a girl.
Until 2015 or so, a very small number of these boys comprised the population of pediatric gender dysphoria cases. Then, across the Western world, there began to be a dramatic increase in a new population: Teenage girls, many with no previous history of gender distress, suddenly declared they were transgender and demanded immediate treatment with testosterone.
I certainly saw this at the center. One of my jobs was to do intake for new patients and their families. When I started there were probably 10 such calls a month. When I left there were 50, and about 70 percent of the new patients were girls. Sometimes clusters of girls arrived from the same high school.
This concerned me, but didn’t feel I was in the position to sound some kind of alarm back then. There was a team of about eight of us, and only one other person brought up the kinds of questions I had. Anyone who raised doubts ran the risk of being called a transphobe.
The girls who came to us had many comorbidities: depression, anxiety, ADHD, eating disorders, obesity. Many were diagnosed with autism, or had autism-like symptoms. A report last year on a British pediatric transgender center found that about one-third of the patients referred there were on the autism spectrum.
Frequently, our patients declared they had disorders that no one believed they had. We had patients who said they had Tourette syndrome (but they didn’t); that they had tic disorders (but they didn’t); that they had multiple personalities (but they didn’t).
The doctors privately recognized these false self-diagnoses as a manifestation of social contagion. They even acknowledged that suicide has an element of social contagion. But when I said the clusters of girls streaming into our service looked as if their gender issues might be a manifestation of social contagion, the doctors said gender identity reflected something innate.
To begin transitioning, the girls needed a letter of support from a therapist—usually one we recommended—who they had to see only once or twice for the green light. To make it more efficient for the therapists, we offered them a template for how to write a letter in support of transition. The next stop was a single visit to the endocrinologist for a testosterone prescription.
That’s all it took.
When a female takes testosterone, the profound and permanent effects of the hormone can be seen in a matter of months. Voices drop, beards sprout, body fat is redistributed. Sexual interest explodes, aggression increases, and mood can be unpredictable. Our patients were told about some side effects, including sterility. But after working at the center, I came to believe that teenagers are simply not capable of fully grasping what it means to make the decision to become infertile while still a minor.
Side Effects
Many encounters with patients emphasized to me how little these young people understood the profound impacts changing gender would have on their bodies and minds. But the center downplayed the negative consequences, and emphasized the need for transition. As the center’s website said, “Left untreated, gender dysphoria has any number of consequences, from self-harm to suicide. But when you take away the gender dysphoria by allowing a child to be who he or she is, we’re noticing that goes away. The studies we have show these kids often wind up functioning psychosocially as well as or better than their peers.”
There are no reliable studies showing this. Indeed, the experiences of many of the center’s patients prove how false these assertions are.
Here’s an example. On Friday, May 1, 2020, a colleague emailed me about a 15-year-old male patient: “Oh dear. I am concerned that [the patient] does not understand what Bicalutamide does.” I responded: “I don’t think that we start anything honestly right now.”
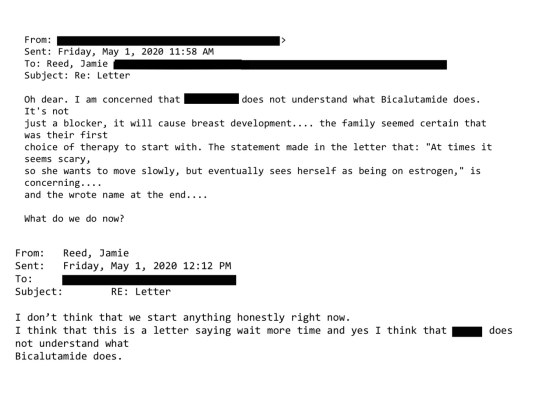
Bicalutamide is a medication used to treat metastatic prostate cancer, and one of its side effects is that it feminizes the bodies of men who take it, including the appearance of breasts. The center prescribed this cancer drug as a puberty blocker and feminizing agent for boys. As with most cancer drugs, bicalutamide has a long list of side effects, and this patient experienced one of them: liver toxicity. He was sent to another unit of the hospital for evaluation and immediately taken off the drug. Afterward, his mother sent an electronic message to the Transgender Center saying that we were lucky her family was not the type to sue.
How little patients understood what they were getting into was illustrated by a call we received at the center in 2020 from a 17-year-old biological female patient who was on testosterone. She said she was bleeding from the vagina. In less than an hour she had soaked through an extra heavy pad, her jeans, and a towel she had wrapped around her waist. The nurse at the center told her to go to the emergency room right away.
We found out later this girl had had intercourse, and because testosterone thins the vaginal tissues, her vaginal canal had ripped open. She had to be sedated and given surgery to repair the damage. She wasn’t the only vaginal laceration case we heard about.
Other girls were disturbed by the effects of testosterone on their clitoris, which enlarges and grows into what looks like a microphallus, or a tiny penis. I counseled one patient whose enlarged clitoris now extended below her vulva, and it chafed and rubbed painfully in her jeans. I advised her to get the kind of compression undergarments worn by biological men who dress to pass as female. At the end of the call I thought to myself, “Wow, we hurt this kid.”
There are rare conditions in which babies are born with atypical genitalia—cases that call for sophisticated care and compassion. But clinics like the one where I worked are creating a whole cohort of kids with atypical genitals—and most of these teens haven’t even had sex yet. They had no idea who they were going to be as adults. Yet all it took for them to permanently transform themselves was one or two short conversations with a therapist.
Being put on powerful doses of testosterone or estrogen—enough to try to trick your body into mimicking the opposite sex—-affects the rest of the body. I doubt that any parent who's ever consented to give their kid testosterone (a lifelong treatment) knows that they’re also possibly signing their kid up for blood pressure medication, cholesterol medication, and perhaps sleep apnea and diabetes.
But sometimes the parents’ understanding of what they had agreed to do to their children came forcefully:
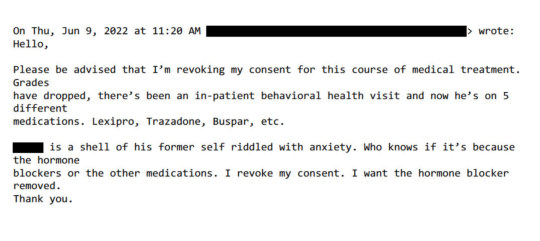
Neglected and Mentally Ill Patients
Besides teenage girls, another new group was referred to us: young people from the inpatient psychiatric unit, or the emergency department, of St. Louis Children’s Hospital. The mental health of these kids was deeply concerning—there were diagnoses like schizophrenia, PTSD, bipolar disorder, and more. Often they were already on a fistful of pharmaceuticals.
This was tragic, but unsurprising given the profound trauma some had been through. Yet no matter how much suffering or pain a child had endured, or how little treatment and love they had received, our doctors viewed gender transition—even with all the expense and hardship it entailed—as the solution.
Some weeks it felt as though almost our entire caseload was nothing but disturbed young people.
For example, one teenager came to us in the summer of 2022 when he was 17 years old and living in a lockdown facility because he had been sexually abusing dogs. He’d had an awful childhood: His mother was a drug addict, his father was imprisoned, and he grew up in foster care. Whatever treatment he may have been getting, it wasn’t working.
During our intake I learned from another caseworker that when he got out, he planned to reoffend because he believed the dogs had willingly submitted.
Somewhere along the way, he expressed a desire to become female, so he ended up being seen at our center. From there, he went to a psychologist at the hospital who was known to approve virtually everyone seeking transition. Then our doctor recommended feminizing hormones. At the time, I wondered if this was being done as a form of chemical castration.
That same thought came up again with another case. This one was in spring of 2022 and concerned a young man who had intense obsessive-compulsive disorder that manifested as a desire to cut off his penis after he masturbated. This patient expressed no gender dysphoria, but he got hormones, too. I asked the doctor what protocol he was following, but I never got a straight answer.
In Loco Parentis
Another disturbing aspect of the center was its lack of regard for the rights of parents—and the extent to which doctors saw themselves as more informed decision-makers over the fate of these children.
In Missouri, only one parent’s consent is required for treatment of their child. But when there was a dispute between the parents, it seemed the center always took the side of the affirming parent.
My concerns about this approach to dissenting parents grew in 2019 when one of our doctors actually testified in a custody hearing against a father who opposed a mother’s wish to start their 11-year-old daughter on puberty blockers.
I had done the original intake call, and I found the mother quite disturbing. She and the father were getting divorced, and the mother described the daughter as “kind of a tomboy.” So now the mother was convinced her child was trans. But when I asked if her daughter had adopted a boy’s name, if she was distressed about her body, if she was saying she felt like a boy, the mother said no. I explained the girl just didn’t meet the criteria for an evaluation.
Then a month later, the mother called back and said her daughter now used a boy’s name, was in distress over her body, and wanted to transition. This time the mom and daughter were given an appointment. Our providers decided the girl was trans and prescribed a puberty blocker to prevent her normal development.
The father adamantly disagreed, said this was all coming from the mother, and a custody battle ensued. After the hearing where our doctor testified in favor of transition, the judge sided with the mother.
‘I Want My Breasts Back’
Because I was the main intake person, I had the broadest perspective on our existing and prospective patients. In 2019, a new group of people appeared on my radar: desisters and detransitioners. Desisters choose not to go through with a transition. Detransitioners are transgender people who decide to return to their birth gender.
The one colleague with whom I was able to share my concerns agreed with me that we should be tracking desistance and detransition. We thought the doctors would want to collect and understand this data in order to figure out what they had missed.
We were wrong. One doctor wondered aloud why he would spend time on someone who was no longer his patient.
But we created a document anyway and called it the Red Flag list. It was an Excel spreadsheet that tracked the kind of patients that kept my colleague and me up at night.
One of the saddest cases of detransition I witnessed was a teenage girl, who, like so many of our patients, came from an unstable family, was in an uncertain living situation, and had a history of drug use. The overwhelming majority of our patients are white, but this girl was black. She was put on hormones at the center when she was around 16. When she was 18, she went in for a double mastectomy, what’s known as “top surgery.”
Three months later she called the surgeon’s office to say she was going back to her birth name and that her pronouns were “she” and “her.” Heartbreakingly, she told the nurse, “I want my breasts back.” The surgeon’s office contacted our office because they didn’t know what to say to this girl.
My colleague and I said that we would reach out. It took a while to track her down, and when we did we made sure that she was in decent mental health, that she was not actively suicidal, that she was not using substances. The last I heard, she was pregnant. Of course, she’ll never be able to breastfeed her child.
‘Get On Board, Or Get Out’
My concerns about what was going on at the center started to overtake my life. By spring 2020, I felt a medical and moral obligation to do something. So I spoke up in the office, and sent plenty of emails.
Here’s just one example: On January 6, 2022, I received an email from a staff therapist asking me for help with a case of a 16-year-old transgender male living in another state. “Parents are open to having patient see a therapist but are not supportive of gender and patient does not want parents to be aware of gender identity. I am having a challenging time finding a gender affirming therapist.”
I replied:
“I do not ethically agree with linking a minor patient to a therapist who would be gender affirming with gender as a focus of their work without that being discussed with the parents and the parent agreeing to that kind of care.”

In all my years at the Washington University School of Medicine, I had received solidly positive performance reviews. But in 2021, that changed. I got a below-average mark for my “Judgment” and “Working Relationships/Cooperative Spirit.” Although I was described as “responsible, conscientious, hard-working and productive” the evaluation also noted: “At times Jamie responds poorly to direction from management with defensiveness and hostility.”
Things came to a head at a half-day retreat in summer of 2022. In front of the team, the doctors said that my colleague and I had to stop questioning the “medicine and the science” as well as their authority. Then an administrator told us we had to “Get on board, or get out.” It became clear that the purpose of the retreat was to deliver these messages to us.
The Washington University system provides a generous college tuition payment program for long-standing employees. I live by my paycheck and have no money to put aside for five college tuitions for my kids. I had to keep my job. I also feel a lot of loyalty to Washington University.
But I decided then and there that I had to get out of the Transgender Center, and to do so, I had to keep my head down and improve my next performance review.
I managed to get a decent evaluation, and I landed a job conducting research in another part of The Washington University School of Medicine. I gave my notice and left the Transgender Center in November of 2022.

What I Want to See Happen
For a couple of weeks, I tried to put everything behind me and settled into my new job as a clinical research coordinator, managing studies regarding children undergoing bone marrow transplants.
Then I came across comments from Dr. Rachel Levine, a transgender woman who is a high official at the federal Department of Health and Human Services. The article read: “Levine, the U.S. assistant secretary for health, said that clinics are proceeding carefully and that no American children are receiving drugs or hormones for gender dysphoria who shouldn’t.”
I felt stunned and sickened. It wasn’t true. And I know that from deep first-hand experience.
So I started writing down everything I could about my experience at the Transgender Center. Two weeks ago, I brought my concerns and documents to the attention of Missouri’s attorney general. He is a Republican. I am a progressive. But the safety of children should not be a matter for our culture wars.
Given the secrecy and lack of rigorous standards that characterize youth gender transition across the country, I believe that to ensure the safety of American children, we need a moratorium on the hormonal and surgical treatment of young people with gender dysphoria.
In the past 15 years, according to Reuters, the U.S. has gone from having no pediatric gender clinics to more than 100. A thorough analysis should be undertaken to find out what has been done to their patients and why—and what the long-term consequences are.
There is a clear path for us to follow. Just last year England announced that it would close the Tavistock’s youth gender clinic, then the NHS’s only such clinic in the country, after an investigation revealed shoddy practices and poor patient treatment. Sweden and Finland, too, have investigated pediatric transition and greatly curbed the practice, finding there is insufficient evidence of help, and danger of great harm.
Some critics describe the kind of treatment offered at places like the Transgender Center where I worked as a kind of national experiment. But that’s wrong.
Experiments are supposed to be carefully designed. Hypotheses are supposed to be tested ethically. The doctors I worked alongside at the Transgender Center said frequently about the treatment of our patients: “We are building the plane while we are flying it.” No one should be a passenger on that kind of aircraft.
==
The U.S. gets its Tavistock. It will not be the last.
Fathers may well be some of the unsung heroes at the end of this mess. Whenever one parent is pushing for life-long medicalization of a child, it is invariably a Munchausen-by-Trans (Transhausen) possessed mother, with a father fighting against all odds and the system that favors her.
#Jamie Reed#gender ideology#queer theory#medical transition#medical corruption#medical malpractice#whistleblower#medical scandal#St. Louis Children's Hospital#ideological capture#transhausen by proxy#transhausen syndrome#medical experimentation#experimental treatment#hormone blockers#puberty blockers#wrong sex hormones#pediatric transition#woke activism#woke#wokeness as religion#cult of woke#wokeism#religion is a mental illness
41 notes
·
View notes
Text
mitski knows me better than anyone else
#mitski#girlblogging#girlblog#mitski my beloved#this is a girlblog#mitski is life#girlhood#im just a girl#hell is a teenage girl#music#me#cinnamon girl#the land is inhospitable and so are we#puberty 2#i bet on losing dogs#bury me at makeout creek#retired from sad new career in business#sullen girl#messy girl#girlblogger interrupted#girl interupted syndrome#girl interrupted#manic pixie dream girl#put me in a movie#girlposting#gaslight gatekeep girlblog#girlblogger#live laugh girlblog#girlblog aesthetic#coquette
3 notes
·
View notes
Text
will you let me, baby, lose on losing dogs?
I know they're losing and I'll pay for my place by the ring
where I'll be looking in their eyes when they're down
I wanna feel it
I bet on losing dogs
I always want you when I'm finally fine,
how you'd be over me looking in my eyes when I come
someone to watch me die
someone to watch me die
I bet on losing dogs
#girlblogging#girl interrupted syndrome#mitski#i bet on losing dogs#puberty 2#female hysteria#this is what makes us girls#crazy#baby#girl blogger#lizzie grant#be the cowboy#laurel hell#the land is inhospitable and so are we
3 notes
·
View notes
Note
Hey! Wanted to ask, are there any intersex variations that cause early puberty? We started puberty at around 3/4 years old and were further in puberty that our older sister, who was 11 at the time (and going through average puberty). We asked our mom about it, and she got incredibly defensive and upset before she said that she stopped us from eating pizza and ice cream and made us eat fresh fish, which made it stop. I don't really believe her because she lies ALOT (which my entire family is aware of), especially about things regarding my childhood. Not only that, we were poor at the time and we couldn't even afford regular fish from stores much less for fresh fish which was wayy more expensive and my siblings and I don't remember having much fish as a kids unless it was given to us by non-family memebers. And around that time, she started taking us to the doctor to get very painful shots even tho we weren't sick and had all of our vaccines already. Even with all that stuff she claims to have done puberty still didn't really stop. Quite literally, the only thing we didn't experience till we were 12 was shark week, and we started growing boobs at 3, but it stopped and started back at around 8. Apart from that, we had been experiencing everything else since we were 3. It was really difficult and painful growing up like that. People thought it was okay and acceptable to treat us like shit and also adultify us. When we were a pre-teen, certain stuff became much more noticeably masculine looking and we also think we may have hirutism (did the ferriman-gallwey thing and got 23) which also led to our parents becoming way worse to us in regard to this and to more harassment from others. Ah shit im kinda rambling sorry I hope this makes sense
(also regarding the we/our's in this, we have DID and use we/our and i/my interchangeably)
Don't worry, you're making sense! No need for apologies. Rambling is welcome on this blog and is actually very beneficial to me helping and answering your questions/concerns.
(Since you're a system, please note that when I use "you" as a collective to refer to the whole system or all the individuals who relate to or are experiencing what you sent in the ask!)
First off, I'm very sorry about all the hardships you've had to go through. That's awful, and no one deserves that. You are wonderful the way you are.
Now, to answer your questions!
Precocious puberty is the term for early puberty. This is what you experienced. There have been some studies that connect eating fish to delaying puberty, which is why I could think your mother did this.
If you were getting shots, you were likely going through GnRH analogue therapy. GnRH refers to gonadotropin releasing hormone. Gonadotropins are a hormone that affect the gonads (sex organs), gametes (sex cells), and sex horomones. Essentially, these delay development in puberty, but how effective they are and how much they work varies from person to person.
For you, I cannot say if this was medically necessary or not. It depends on the body.
Precocious puberty in itself is often a symptom of or comorbid (commonly occurring with) another condition, however pinpointing its cause is often difficult to impossible. So, basically, yes, it can be because of an intersex variation. It can be caused by or connected to thyroid, pituitary, adrenal glands, and/or ovarian issues/problems/variations, which commonly are connected to intersex conditions.
It can also be caused by brain tumors or brain injury, although I doubt that that is the case since you are still alive and fine today and didn't mention having sustained any brain injuries.
McCune–Albright syndrome is a condition that can cause precocious puberty. It is a genetic disorder that effects the bones, endocrine system, and skin. It is a mosaic condition, which means that there is a presence of more than one genetic line for a given genotype (like a given little genetic message, usually organisms are expected to only have one genotype). It is often characterized by fibrous dysplasia (disorder where bone/marrow has fibrous tissue which leads to it being weak and being susceptible to expansion), endocrine diseases, hyperpigmentation of the skin, hyperthyroidism (excessive thyroid hormones), hypophosphatemia (low phosphate levels in the blood), excess growth hormones, and very rarely Cushing's syndrome (a condition characterized by prolonged exposure to cortisol and glucocotoroid.)
Besides that and certain kinds of tumors/brain lesions, hypothyroidism is the only known cause of true precocious puberty as far as I know.
This is the only thing that could be an intersex variation for an individual that I can think of that has significantly precocious puberty as a symptom. However, I'm sure there are other intersex variations with precocious puberty as symptoms that I'm not thinking of. Many intersex variations have early or late puberty as symptoms.
Precocious puberty can also be caused by langerhans cell histiocytosis and tuber cinereum hamartoma, neither of which are related to intersex conditions as far as I know. (Other than the fact that tumors can affect development and hormonal levels.)
Now, besides all that, I'd just like to say that if you feel if your life experiences are intersex, then you are completely allowed to label as such or assert that you are intersex. Intersex is a term open to anyone who is born with or naturally develops abnormalities in their primary or secondary sex characteristics that fall outside of the understood commonly propagated binary sex model used for humans. Personally, I consider hirsutism as an inherently intersex variation all on its own. Some people believe you need a specific diagnosis to be intersex, but I am of the opinion that, if you feel it fits your life experience, then you are welcome to use it. You never need a specific diagnosis for an intersex variation to be intersex. I also think that precocious puberty can be inherently intersex if an individual knows that it gives them an intersex experience.
I hope that I managed to answer your questions and concerns well enough. Let me know if you have any other questions.
Cheers!
EDIT: Early puberty (not necessarily precocious puberty, but early puberty in general) is often associated with NCAH and LOCAH, which could make sense for you considering you have hirsutism. I talk about NCAH/LOCAH here. Thank you to @chaoticmellows for reminding me! I knew I was forgetting something major. In all actuality, NCAH/LOCAH is the most likely candidate if you did have a specific intersex variation, although you know your body best!
8 notes
·
View notes
Text
terfs activley searching out transmasc!kuina posts just to call their op's sexist. nice 👍
#like yea i probably couldve put more work into making sure it didnt show up in tag search#but also its so obvious this person was looking for posts specifically to do this lol#like girl. its one out of many interpretations of her character#i am aware of the internalized sexism and bioessensialism she is dealing with#and what her story means textually. esp for feminism#but also. a trans reading of this isnt sexist lol. transmascs also deal with puberty horror and bioessensialism and imposter syndrome in#cis-male dominated spaces. we're not 'proving' bioessensialism right for transitioning#psii.txt#she was a child who died before she could grow and figure out who she was. so much stuff happens between 'internalized sexism#/bioessentialism' and 'transmasc'#she couldve been transmasc. or a female + feminist swordswoman. she couldve been butch or fem or idfk she was a kid. im just picking one#out of the many things she couldvde been#but canonically she is dead. chill out
5 notes
·
View notes
Text
Kissing transfemmes and hormonally chaotic ovary havers gently on the mouth today (or preferred method of showing affection)
2nd (or 3rd or nth) puberty is hard but we'll get through

13 notes
·
View notes
Text
unless your supernatural journey started out of order on network television, i don't know that we have the same kind of derangement
#there are a lot of good takes from ppl who didnt get into it til the late 2010s or even in the 20s#but supernatural warped my brain before puberty completed its journey#and i was a sam girl for my first few years of spn (younger sibling syndrome)#also the first episode i ever saw if anyone was wondering was a very supernatural christmas#mer rambles#this is obviously in jest i believe something is wrong w all of us
3 notes
·
View notes
Text
A 'Strange Case of Dr. Jekyll and Mr. Hyde' movie but it's a modern day teen film adptation.
#let's discuss#dr. jekyll is going through some changes#and mr. hyde is the embodiment of puberty#and he's just Jekyll but emo#the strange case of dr jekyll and mr hyde#dr jekyll and mr hyde#the strange case of dr. jekyll and mr. hyde#or or#Jekyll is in college#and Hyde is stressed Jekyll who will snap any second#if his thesis gets lower than an A#also throw in gifted child syndrome while we're here#lil texts
19 notes
·
View notes
Text
Sorry im having a case of !woman get overlooked in health things bcs they dont believe our pain or there is no research enough about our body ???
Pure rage
#you are gonna tell me everything is puberty or anxiety or our breast are just growing#or you just have some pain without doing more reasearch???#for so many time later to hear from my sister i may have a syndrome#it sounds so right#it feels already so clear if Its really this tbh#god guys i cant#first autism and then this#the world really hate woman im so tired of this#actually autistic#autistic#asd#actually autism
0 notes
Text
Important Question
Was any Artemis Fowl book after the first one good?
#artemis fowl#I'm guessing the answer is almost certainly 'no'#Because it suffers from what I call 'Gru Syndrome'#where a villain isn't allowed o be a villain in his own story about him being a villain#Artemis hit puberty found himself crushing on a lesbian elf and couldn't commit any more t his true calling#I think I gave up by book four#or I had simply aged out of it by book four#anyone else hate mulch diggums and thought he was gross and dumb#Artemis's a rich nepo baby why the fuck did we redeem him#what was wrong with him being a selfish little shit#yeah he healed his mum but what if - here me out - she was't a nice lady but the sort of person who marries a wealth known mobster#what if his parents both sucked like the narrative framing implies#john wick stole john wick from Butler in artemis fowl and we all know it#its why that series also only has one good entry
0 notes
Last Seen Blogs

waspedits-blog
ᴡᴀꜱᴘ ᴇᴅɪᴛꜱ.

itsnotcourtney
It's Britney, bitch.

journal-sanji
Untitled

audubon-odysseys-blog-blog
wanderlusting audubon