#FYIMed
Photo
Advice from a Professional Doctor, Asher Nitin.
Ignore all the portrayals of life in medical school by your pre-med lecturers.
If they begin a med school narrative with, “My nephew is a doctor and he told me…,” instantly disregard it. His nephew did not tell him that. He told him much more. Those are merely the parts he wants to remember.
If it isn’t a recently-graduated doctor telling you what life in med school is like, it isn’t going to be anything like what they will tell you.
So what is it like instead? Grey’s anatomy? House, M.D.?
Neither. Med school is more like Scrubs and The Knick than it is like Grey’s Anatomy and House, M.D.
Unlike Grey’s Anatomy, you and your fellow medical students will not be that good looking. You will not sleep with each other as much. You will not cry over your patients (you’ll have a hard time remembering their full name). And you will not monkey around with barely-tested experimental procedures. Ever. If you do, it’ll probably be the last thing you do because good-bye medical school.
Unlike House, all medicine will be diagnostic. Your professors will only appear to be brilliant (it’s really just decades of specialized knowledge and experience; with their subject and with your type). Diagnosis will be algorithmic, and even that algorithm won’t be your own. But you will still get a kick out of it.
Like Scrubs and The Knick, your medical school will be your life. You will eat, sleep and dream medicine. Your entire social circle will consist of your colleagues. Your family will be the one stable point in your life. You’ll date your colleagues.
Speaking of dating, your sexy does not go up when you become a doctor. I mean this practically.
Theoretically, I’m told doctors are hot. I can see why. They undeniably have inherent value: social standing, (the promise of) money, proof of intelligence (actually, no) and actual power over life (more than you know).
But practically speaking (especially if you’re male) your dating life will not get better as a medical student. That is because the demands of medical school will swamp you. You will come home tired. Your pool of prospective partners will mostly consist of your medical colleagues. So while your newfound status as a doctor might have value in non-medical circles, it will mean nothing because you will almost never frequent those circles. But within the circle you’re in, your status as a medical student means nothing, because so what? Everyone is one too.
“But Asher!” you say, frantically gesturing at me to pause, “I’ll be smart and date outside of medical school.”
No, dummy. You’ll be a dummy if you do that because…
The more friends you have outside of med school the harder it is to excel.
Med school is about an ethos. You’re not just part of a course. You’re part of a community. This is now your primary identity. All your self worth are now belong with us, bi*ch.
There is this neurological phenomenon seen in people trying to study. When you’re focused on something, if you break off and engage with something unrelated, your brain takes up to twenty minutes to fully refocus on the original task once you return to it.
In life as well, broadly speaking, I’ve observed a similar phenomenon. I’ve known three students in med school whose circle of friends mostly lay outside of med school. One hung out with mostly dancers and choreographers. One was a socialite. One hung out with the sons of politicians. They all were (and still are as of now) the worst doctors I have ever seen. This is because they constantly take breaks from the ethos of medical life. They miss out on the rhythm of life in the world of medicine.
So you should know that…
You will leave most of your old friends behind, and you won’t even mind.
Of all the various professions, I’m told, physicians tend to default the most on school reunions. That is partly because they don’t have the time, but also because they don’t care.
It isn’t that we become arrogant or unsocial. It is that the act of medical education deeply changes you. It makes you more functionally intelligent. It makes you less prone to fake drama. It makes you calmer in crisis.
All these after-effects will permanently drive a wedge between you and many of the people you used to know. This is a surprising side-effect no one anticipates; least of all your elders. And that is an amusing paradox. They anticipate your becoming a doctor because they know medical school is elevation. They don’t realize the side effect of this elevation is you will now talk down to them.
Your most important subject in pre-med is physics.
Look, pre-med isn’t really about information continuity. The organisms you will dissect in pre-med will be phylogenetically disconnected from med school. You dissect a plant stem, a plant root, an earthworm, a cockroach, a frog, and then… a human being? See? You won’t be seamlessly connecting domains of knowledge.
Pre-med isn’t even about building a conceptual base. Many things you learn in pre-med biology will be repeated in so much greater detail in med school that your prior knowledge will only partially help.
Pre-med is about picking up mental skills you will need. Let’s talk about those.
You need to learn to form a train of thought fast.
The great thing about learning to solve problems in physics is that you learn to solve problems in general. You learn to quickly identify variables and constants. Sometimes there will be constants in the problem that would normally be variables in real life. You learn to work with those too.
Physics allows you to become mentally agile with concepts. If you get fluid mechanics, you can handle the physiology of hypovolemic shock. If you get lever mechanisms (in different orders), you can handle applied anatomy in orthopedics. If you get optics, you can handle a lot of neurology and ophthalmology.
In my experience, the students who have the hardest time in med school are the ones who didn’t learn to think on their feet within a fixed framework of time.
You hate memorizing? Actually, you don’t. It’s all about the context.
Literally none of us salivated at the prospect of memorizing taxonomies. We hated it and struggled over it and were glad when we were done with it. That was because it was something we knew we would never use.
In med school, you will do a lot of memorizing. But you will enjoy it (or at least you can, if you choose; I’m a huge nerd). Many doctors will tell you how easily drug classifications embed themselves in their brains. This is despite the fact that the latter are more complex than zoology taxonomy charts or botanical floral formulas. The difference is that your knowledge of drug classification will impact what you will say to your aunt when she confronts you over her persistent back pain over Christmas dinner (poor posture, it’s always poor posture; she sits like a potato).
So you will memorize a lot. It won’t be anything like memorizing was before. Rest easy. You will find it easy to like it.
Your persona does not matter. Caring for people and being compassionate and wanting to cure disease are the least important things in medicine.
You need to be able to meaningfully link vast amounts of information to come to a correct diagnosis as per established algorithms. You need to perform surgical procedures within a reasonable amount of time with a decent degree of success. All else is secondary.
When most of your non-doctor relatives tell you that a doctor’s personality matters, they’re doing something called argument from ignorance. You see, the world of medicine is so big and so complex that most of it is technically incomprehensible to the general public. So they latch on to the few aspects of a doctor’s life they are mentally capable of understanding (and commenting upon; remember their first reaction to meeting someone with an education superior to theirs is to give them tips). So they will talk about a doctor’s personality because it is the only part they can presume to have some expertise on. Even that they do not.
Don’t ever do stupid things like falling in love with your patients or building deep and personal relationships with your patients. You will never last in medicine. This is not because the emotional trauma of losing them will wreck you. This is because you will go bankrupt fighting lawsuits accusing you of patient preference.
You will feel the pressure in the things non-doctors will say behind a good doctors back. “He’s so boring at parties, he can only talk work stuff.” If that is your destiny, so be it. Own it. They find you boring? So what? You were not put on this earth to entertain the illiterate at parties. You were sent here to be a lifesaver; not to have a personality that appeals to the lowest common denominator.
I’m telling you it does not matter. The practice of medicine is life on the edge of reality. All personalities are welcome because medical school is a personality in itself.
The materialists among us are taught the value of wisdom and the ascetics among us learn to knot a Double-Windsor.
The atheists among us will pray frantically and the religious among us will find no time for church on Sunday.
The loudmouthed learn to whisper in the NICU and the soft-spoken learn to yell, “Stat!” in the ER.
The type-A personalities among us learn to break the news of a patient’s passing to his relatives and the type-B personalities among us learn to argue medico-legal cases.
The clumsy among us learn to suture wounds and the nimble learn to administer CPR.
Materialists.
Ascetics.
Atheists.
Theists.
Loudmouthed.
Soft-spoken.
Type-A.
Type-B.
Clumsy.
Nimble.
In medical school, we all meet in the middle.
PS: Photo not mine. Credits to the rightfully owner.
11 notes
·
View notes
Photo
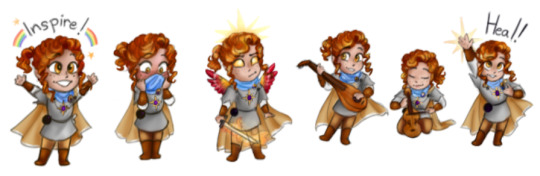


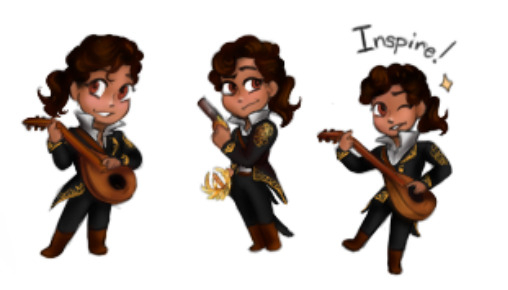






Tis the Oasis crew! I made a series of chibis of everybody’s characters which we uploaded as emojis for one of my DnD discord servers.
In order: Solas (aasmair bard/cleric. My character), Bee (changeling shadow sorcerer), Serenity (human rouge/sorcerer), Tony (human bard/fighter), Mereseja (tbh, I’m unsure of her race- fighter/warlock), Caeden (half-drow fighter/warlock), Markus (half-orc path of the beast barbarian), Taris (halfling bear totem barbarian), Fyim (human divination wizard), & Hikari (teifling rouge/fighter)
bonus:

RIP Phiris, the Eladrin Tome Warlock. (Mereseja is the player’s new character)
#Now when these characters randomly show up when I doodle stuff w/ Oasis#yall have a reference#You can tell which characters I know the most about can't cha? >w<#dnd#dnd ocs#inkwellart#swear word#one singular one#it's in the boys name I'm sorry#weapons tw#death mention tw
26 notes
·
View notes
Text
Now I’m not a BB shipper, but I know a ridiculous argument when I see one.
I hate ship wars I do & what I hate most is that nothing will never be enough to satisfy the other side.
I understand when somebody gives constructive criticism to a ship to help better improve it & make it believable. I understand there is a lot BB & BS need to work on, mostly BB now since they’re semi-canon. But there are times when at this point you’re not giving criticism & you’re not being an anti-shipper, but straight up just constantly talking shit just to talk shit.
I’m talking about RWBY YouTuber, Adel Aka.
You see Eruption Fang said he doesn’t like BB because he doesn’t like how they had to ruin a few character & dynamics to make it canon. Fair & valid.
Vexed Viewer just wants all of us to shut the fuck up. Extremely fair & extremely valid bc I too want us to shut the fuck up.
But Adel Aka? He’s not even part of the BBvsBS Ship War & Jesus H Christ he will not shut the fuck up. This is what I’m talking about. He is just constantly talking shit like he has diarrhea in his mouth to the point where none of his arguments make any type of sense.
“BB is shallow because Yang didn’t stand up for Blake” he says knowing damn well if Yang did stand up for Blake in V7 CH1 you would yell force.
“MC makes more sense than BB” More than BB, but not BS? Yes they would be better representation bc of how similar Weiss & Blake are, for both the Faunus & LGBT+, but is that it? You have your why is would be better, but not how. (FYIM, he doesn’t like MC either)
“BB shippers are getting baited.”
“BB shippers are salty”
“It’s forced.”
“There’s a lot of fluff for BB & here’s the problem.”
“It’s shippers need tumblr.”
“I mean they’re both horrible people so that’s why I like BB”
*Makes a video making fun of BB shippers evidence/arguments*
“Yang’s bike suffered so BB could be canon”
“Ilia left to make room for BB bc her representation was boring”
“Made the show worse.”
Y’all get the idea & he has in fact said this stuff in several of his videos & at this point it’s just obvious you don’t like the ship, that’s fine. You’re allowed to have your opinions on it, that’s also fine. Everybody understands that you don’t like it, why are you wasting your breathe making several videos explaining why you don’t like, shitting on it & the shippers, etc.? Dude you sound like a whiny bitch baby crying over spilled milk. BB is semi-canon get over it. You bitching about it isn’t gonna change the creators mind.
If you BB shippers want me to remove this from the BB tag just let me know & I will
Edit: It’s been removed
36 notes
·
View notes
Photo

BUY 1 GET 1 FREE🚨🚨+ FREE WORLDWIDE SHIPPING ✈️ Automatic discount code will apply at checkout! ⚡️⚡️ Crafted by professionals ⚡️⚡️ Premium Quality Metals ⚡️⚡️ Highly Detailed Designs SHOP NOW VISIT LINK IN OUR BIO!! . . . . . #skullrings #skulljewelry #rebelnation #bikerring #bikerjewelry #darkbeauty #skullface #darkfashion #alternativejewelry #customculture #kustomkulture #badassjewelry #ringsformen #signetring #skulladdicted #skulladdict #skullobsessed #ringsofinstagram #skulloftheday #ringsofig #ringoftheday #bikelife #bikerstyle #fingerrings #vrodnation #dynaholics #caferacerculture #dynanation #shovelhead https://www.instagram.com/p/COGVuJ-FyIM/?igshid=9fdhxw5j2zcf
#skullrings#skulljewelry#rebelnation#bikerring#bikerjewelry#darkbeauty#skullface#darkfashion#alternativejewelry#customculture#kustomkulture#badassjewelry#ringsformen#signetring#skulladdicted#skulladdict#skullobsessed#ringsofinstagram#skulloftheday#ringsofig#ringoftheday#bikelife#bikerstyle#fingerrings#vrodnation#dynaholics#caferacerculture#dynanation#shovelhead
0 notes
Text
Losing My Mind
"Get outta your mind!" -- Lil Jon
I had asked Sarah what is something you live by? She answered FYIP (fuck you, i’m pretty). This photo pretty much represents how I feel sometimes. The world can go to shit around but as Sarah says, “ FYIM!” Just don’t ask me to smile and we’re good. No one wants to be reminded to turn that frown upside down.
We spent a good 10- 15 minuets throwing sheet music all around Sarah while she tried to pose with out getting completely clobbered. End result above, some out takes below.
#BTS & Out takes with Sarah and Emma.
#Sarah Szeibel#thespians#the master of mess#music teacher#teacher#san francisco photographer#san francisco thespians#headshots
0 notes
Text
Wearable, Shareable, Virtual: The Demands of the Digital Health Consumer in 2018
As I wrote here in April 2017, telehealth and virtual healthcare are mainstreaming.
This week at the 2018 annual HIMSS conference, telehealth is playing a mainstream role in discussions about right-sizing and right-placing healthcare.
The evidence for telehealth’s tipping point is rooted in new research published today by Accenture on Patients + Doctors + Machines, Accentures’ 2018 Consumer Survey on Digital Health.
I sat down today with Dr. Kaveh Safavi who leads Accenture’s healthcare practice to discuss the results of this study into peoples’ atttudes toward healthcare technology and innovation.
Three in four consumers in America say technology is important to managing their health. Consumers most commonly use the following technologies to help them manage health in 2018:
56% use websites
48% mobile app
38% electronic health records
35% social media
33% wearables
27% smart scales
25% online communities, and
14% remote monitoring.
The most important advantages of virtual care have to do with cost and convenience, shown in the second chart. Half of Americans believe virtual care services can reduce medical costs to patients and accommodate patients’ schedules, and another 43% of consumers say that virtual care can provide timely services to patients. FYIm Accenture defines virtual services as video or voice transmitted by a provider either synchronously (in real-time) or asynchronously.
Patients’ views on the advantages of virtual are de-valued through consumers’ lenses on quality, engagement, and the speed of diagnoses.
There are two axes to consider when it comes to consumers’ current views on virtual healthcare options vs. in-person F2F with a clinician: those axes are trust and risk.
“When trust is high and risk is low,” Kaveh explained, “People can have asynchronous email” with their providers. “When trust is low and risk is high, we need to be in the same room. Health hasn’t offered us many options” before the emergence of the telehealth/virtual health continuum of choices, Kaveh pointed out.
We discussed other research demonstrating that the proportion of consumers who use alternatives to seeing “their” primary care provider, like telemedicine and retail clinics, is growing. A key reason these patients seek alternatives to F2F visits with their personal physicians is that they want to “get something done.” Convenience and the “Amazon Prime’ing” of consumers has come to health care underpinning consumerism.
Trust underpins health engagement, and that directly relates to the sharing of personal health information. Accenture found that 90% of consumers are willing to share health data from wearable devices with physicians and nurses, and 75% with their family. Surprisingly (to me), 72% of consumers said they’d share their health data with a health insurance plan. But only 38% would share wearable health data with an employer, and 41% with a government agency.
Here, instead of trust vs. risk, the factors to consider are trust vs. benefit, Kaveh counsels.
Accenture surveyed 2,301 U.S. adults 18 years of age and over between October 2017 and January 2018 for this survey.
Health Populi’s Hot Points: This morning, I had the honor of participating as a judge in Microsoft’s annual Health Innovation Forum. Dr. Judd Hollander of Thomas Jefferson University Health System shared his experience launching JeffConnect, which is the organization’s telehealth platform. The program provides a full continuum of healthcare access to patients both within and outside of the TJU network. “A little sick” patients can access care at the 6 o’clock point of the diagram, all the way across the patient spectrum to post-discharge and remote monitoring at home.
Dr. Hollander provided hard evidence for consumers’ embrace of telehealth based on his experience with both clinicians and patients who are using JeffConnect. My favorite of his many quotable insights was the following:
“When a patient is doing a telemedicine call for 10 minutes with a patient, she’s not hell-bent to get antibiotics. But if she waits four hours in the ER and doesn’t get antibiotics, she’ll have something to say about it.”
Thus, virtual health can drive efficiency, right-sized healthcare, and greater patient satisfaction. These are key ingredients into migrating to the Quadruple Aim.
The post Wearable, Shareable, Virtual: The Demands of the Digital Health Consumer in 2018 appeared first on HealthPopuli.com.
Wearable, Shareable, Virtual: The Demands of the Digital Health Consumer in 2018 posted first on http://dentistfortworth.blogspot.com
0 notes
Text
Wearable, Shareable, Virtual: The Demands of the Digital Health Consumer in 2018
As I wrote here in April 2017, telehealth and virtual healthcare are mainstreaming.
This week at the 2018 annual HIMSS conference, telehealth is playing a mainstream role in discussions about right-sizing and right-placing healthcare.
The evidence for telehealth’s tipping point is rooted in new research published today by Accenture on Patients + Doctors + Machines, Accentures’ 2018 Consumer Survey on Digital Health.
I sat down today with Dr. Kaveh Safavi who leads Accenture’s healthcare practice to discuss the results of this study into peoples’ atttudes toward healthcare technology and innovation.
Three in four consumers in America say technology is important to managing their health. Consumers most commonly use the following technologies to help them manage health in 2018:
56% use websites
48% mobile app
38% electronic health records
35% social media
33% wearables
27% smart scales
25% online communities, and
14% remote monitoring.
The most important advantages of virtual care have to do with cost and convenience, shown in the second chart. Half of Americans believe virtual care services can reduce medical costs to patients and accommodate patients’ schedules, and another 43% of consumers say that virtual care can provide timely services to patients. FYIm Accenture defines virtual services as video or voice transmitted by a provider either synchronously (in real-time) or asynchronously.
Patients’ views on the advantages of virtual are de-valued through consumers’ lenses on quality, engagement, and the speed of diagnoses.
There are two axes to consider when it comes to consumers’ current views on virtual healthcare options vs. in-person F2F with a clinician: those axes are trust and risk.
“When trust is high and risk is low,” Kaveh explained, “People can have asynchronous email” with their providers. “When trust is low and risk is high, we need to be in the same room. Health hasn’t offered us many options” before the emergence of the telehealth/virtual health continuum of choices, Kaveh pointed out.
We discussed other research demonstrating that the proportion of consumers who use alternatives to seeing “their” primary care provider, like telemedicine and retail clinics, is growing. A key reason these patients seek alternatives to F2F visits with their personal physicians is that they want to “get something done.” Convenience and the “Amazon Prime’ing” of consumers has come to health care underpinning consumerism.
Trust underpins health engagement, and that directly relates to the sharing of personal health information. Accenture found that 90% of consumers are willing to share health data from wearable devices with physicians and nurses, and 75% with their family. Surprisingly (to me), 72% of consumers said they’d share their health data with a health insurance plan. But only 38% would share wearable health data with an employer, and 41% with a government agency.
Here, instead of trust vs. risk, the factors to consider are trust vs. benefit, Kaveh counsels.
Accenture surveyed 2,301 U.S. adults 18 years of age and over between October 2017 and January 2018 for this survey.
Health Populi’s Hot Points: This morning, I had the honor of participating as a judge in Microsoft’s annual Health Innovation Forum. Dr. Judd Hollander of Thomas Jefferson University Health System shared his experience launching JeffConnect, which is the organization’s telehealth platform. The program provides a full continuum of healthcare access to patients both within and outside of the TJU network. “A little sick” patients can access care at the 6 o’clock point of the diagram, all the way across the patient spectrum to post-discharge and remote monitoring at home.
Dr. Hollander provided hard evidence for consumers’ embrace of telehealth based on his experience with both clinicians and patients who are using JeffConnect. My favorite of his many quotable insights was the following:
“When a patient is doing a telemedicine call for 10 minutes with a patient, she’s not hell-bent to get antibiotics. But if she waits four hours in the ER and doesn’t get antibiotics, she’ll have something to say about it.”
Thus, virtual health can drive efficiency, right-sized healthcare, and greater patient satisfaction. These are key ingredients into migrating to the Quadruple Aim.
The post Wearable, Shareable, Virtual: The Demands of the Digital Health Consumer in 2018 appeared first on HealthPopuli.com.
Wearable, Shareable, Virtual: The Demands of the Digital Health Consumer in 2018 posted first on https://carilloncitydental.blogspot.com
0 notes
Photo
Hi everyone! Here are some list of medical books we can read for aspiring doctors like us. Recommended by the website; TheMedicPortal
Ps. Photo not mine. Credits to the rightful owner.
1. Bad Science by Goldacre
- In this highly entertaining book, Ben Goldacre sheds light on how the media misunderstands science and why we are so gullible.
2. Being Mortal by Henry Marsh
- Henry Marsh, a world-renowned brain surgeon, writes a memoir of his fascinating career with painful honesty.
3. Children Act by Ian McEwan
- With a more personal outlook on medical law and ethics, you will finish this book with more perspective on those difficult ethics questions in medical interviews.
4. When Breath Becomes Air by Paul Kalanithi
- This beautiful book left me feeling truly humbled and inspired. One that every aspiring medic should read.
Check out TheMedicPortals’s website link https://www.themedicportal.com if you want to know more about them.
1 note
·
View note
Text
Wearable, Shareable, Virtual: The Demands of the Digital Health Consumer in 2018
As I wrote here in April 2017, telehealth and virtual healthcare are mainstreaming.
This week at the 2018 annual HIMSS conference, telehealth is playing a mainstream role in discussions about right-sizing and right-placing healthcare.
The evidence for telehealth’s tipping point is rooted in new research published today by Accenture on Patients + Doctors + Machines, Accentures’ 2018 Consumer Survey on Digital Health.
I sat down today with Dr. Kaveh Safavi who leads Accenture’s healthcare practice to discuss the results of this study into peoples’ atttudes toward healthcare technology and innovation.
Three in four consumers in America say technology is important to managing their health. Consumers most commonly use the following technologies to help them manage health in 2018:
56% use websites
48% mobile app
38% electronic health records
35% social media
33% wearables
27% smart scales
25% online communities, and
14% remote monitoring.
The most important advantages of virtual care have to do with cost and convenience, shown in the second chart. Half of Americans believe virtual care services can reduce medical costs to patients and accommodate patients’ schedules, and another 43% of consumers say that virtual care can provide timely services to patients. FYIm Accenture defines virtual services as video or voice transmitted by a provider either synchronously (in real-time) or asynchronously.
Patients’ views on the advantages of virtual are de-valued through consumers’ lenses on quality, engagement, and the speed of diagnoses.
There are two axes to consider when it comes to consumers’ current views on virtual healthcare options vs. in-person F2F with a clinician: those axes are trust and risk.
“When trust is high and risk is low,” Kaveh explained, “People can have asynchronous email” with their providers. “When trust is low and risk is high, we need to be in the same room. Health hasn’t offered us many options” before the emergence of the telehealth/virtual health continuum of choices, Kaveh pointed out.
We discussed other research demonstrating that the proportion of consumers who use alternatives to seeing “their” primary care provider, like telemedicine and retail clinics, is growing. A key reason these patients seek alternatives to F2F visits with their personal physicians is that they want to “get something done.” Convenience and the “Amazon Prime’ing” of consumers has come to health care underpinning consumerism.
Trust underpins health engagement, and that directly relates to the sharing of personal health information. Accenture found that 90% of consumers are willing to share health data from wearable devices with physicians and nurses, and 75% with their family. Surprisingly (to me), 72% of consumers said they’d share their health data with a health insurance plan. But only 38% would share wearable health data with an employer, and 41% with a government agency.
Here, instead of trust vs. risk, the factors to consider are trust vs. benefit, Kaveh counsels.
Accenture surveyed 2,301 U.S. adults 18 years of age and over between October 2017 and January 2018 for this survey.
Health Populi’s Hot Points: This morning, I had the honor of participating as a judge in Microsoft’s annual Health Innovation Forum. Dr. Judd Hollander of Thomas Jefferson University Health System shared his experience launching JeffConnect, which is the organization’s telehealth platform. The program provides a full continuum of healthcare access to patients both within and outside of the TJU network. “A little sick” patients can access care at the 6 o’clock point of the diagram, all the way across the patient spectrum to post-discharge and remote monitoring at home.
Dr. Hollander provided hard evidence for consumers’ embrace of telehealth based on his experience with both clinicians and patients who are using JeffConnect. My favorite of his many quotable insights was the following:
“When a patient is doing a telemedicine call for 10 minutes with a patient, she’s not hell-bent to get antibiotics. But if she waits four hours in the ER and doesn’t get antibiotics, she’ll have something to say about it.”
Thus, virtual health can drive efficiency, right-sized healthcare, and greater patient satisfaction. These are key ingredients into migrating to the Quadruple Aim.
The post Wearable, Shareable, Virtual: The Demands of the Digital Health Consumer in 2018 appeared first on HealthPopuli.com.
Wearable, Shareable, Virtual: The Demands of the Digital Health Consumer in 2018 posted first on http://dentistfortworth.blogspot.com
0 notes
Last Seen Blogs

katlyntheartist
KatlynIsDrawing

ricardoarquezlifecoach-blog
Emprende tu Destino

grimmtechnicolor
Bones

alunasky-blog
Alunasky

shitposting-hobbits-to-gallifrey
Enter Blog Title Here