#trisomy 18
Text
A Texas woman who had sought a legal medical exemption for an abortion has left the state after the Texas Supreme Court paused a lower court decision that would allow her to have the procedure, lawyers for the Center for Reproductive Rights said Monday.
State District Judge Maya Guerra Gamble last week had ruled that Kate Cox, a 31-year-old mother of two from Dallas, could terminate her pregnancy. According to court documents, Cox's doctors told her her baby suffered from the chromosomal disorder trisomy 18, which usually results in either stillbirth or an early death of an infant.
As of the court filing last week, Cox was 20 weeks pregnant. According to the Center for Reproductive Rights, which brought the lawsuit, Cox left the state because she "couldn't wait any longer" to get the procedure.
"Her health is on the line," said Center for Reproductive Rights CEO Nancy Northup. "She's been in and out of the emergency room and she couldn't wait any longer."
In response to Gamble's decision, Texas Attorney General Ken Paxton warned a Texas medical center that it would face legal consequences if an abortion were performed.
In an unsigned order late Friday, the Texas Supreme Court then temporarily paused Gamble's ruling.
On Monday, after Cox left the state, the state Supreme Court lifted the pause and ruled against Cox's request, dismissing it as moot.
According to court documents, Cox's doctors had told her that early screening and ultrasound tests suggested her pregnancy is "unlikely to end with a healthy baby," and due to her two prior cesarean sections, continuing the pregnancy puts her at risk of "severe complications" that threaten "her life and future fertility."
The lawsuit alleges that due to Texas' strict abortion bans, doctors have told her their "hands are tied" and she would have to wait until the fetus dies inside her or carry the pregnancy to term, when she will have to undergo a third C-section "only to watch her baby suffer until death."
The lawsuit was filed as the state Supreme Court is weighing whether the state's strict abortion ban is too restrictive for women who suffer from severe pregnancy complications. An Austin judge ruled earlier this year that women who experience extreme complications could be exempt from the ban, but the ruling is on hold while the all-Republican Supreme Court considers the state's appeal.
In the arguments before the state Supreme Court, the state's lawyers suggested that a woman who is pregnant and receives a fatal fetal diagnosis could bring a "lawsuit in that specific circumstance."
According to the Center for Reproductive Rights, Cox v. Texas is the first case since the overturning of Roe v. Wade to be filed on behalf of a pregnant person seeking emergency abortion care. Last week, a woman in Kentucky who is 8 weeks pregnant filed a lawsuit challenging the state's two abortion bans.
#us politics#news#cbs news#2023#abortions#abortion bans#reproductive rights#reproductive health#Reproductive healthcare#bodily autonomy#texas#texas supreme court#Center for Reproductive Rights#Judge Maya Guerra Gamble#trisomy 18#Nancy Northup#Kate Cox#Ken Paxton#Cox v. Texas
94 notes
·
View notes
Text
21 notes
·
View notes
Text
A reminder that Republicans reserve the right to police reproductive systems.
A Texas woman who had sought a legal medical exemption for an abortion has left the state after the Texas Supreme Court paused a lower court decision that would allow her to have the procedure, lawyers for the Center for Reproductive Rights said Monday.
State District Judge Maya Guerra Gamble last week had ruled that Kate Cox, a 31-year-old mother of two from Dallas, could terminate her pregnancy. According to court documents, Cox's doctors told her her baby suffered from the chromosomal disorder trisomy 18, which usually results in either stillbirth or an early death of an infant.
As of the court filing last week, Cox was 20 weeks pregnant. According to the Center for Reproductive Rights, which brought the lawsuit, Cox left the state because she "couldn't wait any longer" to get the procedure.
"Her health is on the line," said Center for Reproductive Rights CEO Nancy Northup. "She's been in and out of the emergency room and she couldn't wait any longer."
In response to Gamble's decision, Texas Attorney General Ken Paxton warned a Texas medical center that it would face legal consequences if an abortion were performed.
In an unsigned order late Friday, the Texas Supreme Court then temporarily paused Gamble's ruling.
On Monday, after Cox left the state, the state Supreme Court lifted the pause, dismissing it as moot, and overturned the lower court ruling that had granted Cox's request.
Fortunately Ms. Cox had the option of traveling to another state to have the procedure. A future US Supreme Court packed with MAGA judges could further restrict abortion nationally.
ALL of the current GOP candidates for president would choose anti-abortion judges for the US Supreme Court. And a GOP Senate would confirm them. Remind anybody considering voting for an impotent third-party candidate who has no chance of winning.
#abortion#a woman's right to choose#texas#kate cox#trisomy 18#texas supreme court#republicans#anti-abortion extremists#the far right#the sanctity of reproductive freedom#election 2024
19 notes
·
View notes
Link
Their baby was diagnosed with Edwards’ syndrome at their first scan. Edwards’ syndrome, also known as Trisomy 18, is a genetic condition that means the child is unlikely to survive for very long outside of the womb — although in some cases, people with Edwards’ syndrome have been known to survive to adulthood.
Jessica was offered abortions but said, “as he was still alive, I couldn’t do it”.
Jessica was able to connect with online support groups and managed to find lots of other positive stories of children being born alive.
She explained, “This gave me hope and the confidence to give him a chance to be born. I’m so glad I went ahead. At least we had Oaken and a positive experience”.
To raise awareness of baby loss and Edwards’ syndrome, and to fundraise for the charity that has got them through this experience, Jessica has had her 11-year-old dreadlocks chopped off.
The money raised will go toward the family’s local children’s hospice Martin House, who supported them throughout baby Oaken’s life and are now providing them with counselling.
The hospice cares for children with life-limiting illnesses. They allowed the family to prepare themselves for the expected short time they’d be able to share with baby Oaken.
107 notes
·
View notes
Text
My children, pt. 3, Jessica-Joy
Time passed and we were doing okay. I kept on working as a secretary at Cornerstone Counselling Centre, Henry at the church. I went with him to youth group meetings, church, etc., wherever I was allowed to go. It was not easy. The youth were not unfriendly by any means. It was my own hang-ups. I had always been socially awkward and making small talk was never something I could do. Plus, I felt…
View On WordPress
0 notes
Text
Edwards Syndrome
Edwards syndrome is a very rare condition caused by an abnormal amount of chromosomes in the cells of the body. Babies are normally born with 46 chromosomes, which are arranged in 23 pairs.
0 notes
Photo

NIPT Test screens for Trisomy 21 (Down Syndrome), 18 (Edward Syndrome), and 13 (Patau Syndrome) as early as 10 weeks of pregnancy. The test possesses no risk to the mother or the baby. Request your test now for a blissful pregnancy.
For more details, Call us at 18001214030 or drop us an email at [email protected] for an Appointment
To know more visit. https://t2m.io/DTjoF2P
#NIPT #NIPTTest #Pregnancy #NonInvansive #Trisomy18 #Trisomy21 #ChromosomalMicroarray #Chromosomal #PregnancyTest #AntibodyTest #Sequencing #PregnantWomen #Genes2Me #GeneticTesting #RTPCRTest #Antigen #AntigenTest
0 notes
Text
Trisomy 18 and Microdeletion 18p Mosaicism: A case report and literature review by Chao-Chun ZOU in Journal of Clinical Case Reports Medical Images and Health Sciences

ABSTRACT
The trisomy 18 syndrome is a common chromosomal disorder due to the presence of an extra chromosome 18, either complete, mosaic trisomy or partial trisomy 18q. The mosaic trisomy 18 patients’ phenotype was extremely variable, from the absence of dysmorphic features to complete trisomy 18 syndrome. The phenotype of 18p deletion syndrome is variable and almost all survived. A 2-year-old girl was referred to our hospital due to growth delay. Mild dysmorphy including thin hair, frontal bossing, low set ears, broad-flat nose, nostrils slightly upward, downturned corners of the mouth, dysplasia teeth, small hands and fingers bilaterally was observed. The karyotype of peripheral leukocyte showed 46,XX, psu idic (18)(p11.2)[55]/46,XX, del (18)(p11.2)[45]. We report this case to add to our knowledge of the trisomy 18 and microdeletion 18p mosaicism.
Keywords: Trisomy 18, mosaic;18p microdeletion; Psychomotor retardation; Karyotype
INTRODUCTION
The trisomy 18 syndrome was first reported by Edwards et al in 1960, also known as Edwards syndrome. It is the second most common autosomal chromosomal disorder after trisomy 21(Down’s syndrome)due to the presence of an extra chromosome 18, which has three basic types: complete, mosaic and partial type (Edwards et al., 1960, Cereda and Carey, 2012,Mudaliyar and Mudaliyar, 2017). The syndrome presents a recognizable pattern of major and minor anomalies, significant psychomotor and cognitive disability are associated with high neonatal and infant morbidity and mortality. The estimated overall prevalence of trisomy 18 in live born is approximately 1/6, 000 to 1/8, 000 while the incidence in fetus is much higher, the difference is caused by fetal loss and pregnancy termination after prenatal diagnosis (Cereda and Carey, 2012, Rasmussen et al., 2003). The mosaic trisomy 18 usually means having more than one cell line in the individual, and it occurs in approximately 5 percent in all trisomy 18 patients (Fitas et al., 2013). The phenotypic manifestations are highly variable, from the absence of dysmorphic features to the complete trisomy 18 syndrome (Tucker et al., 2007). Since the clinical outcomes of complete and mosaic trisomy 18 can be different, it is of vital importance to achieve a correct diagnosis because of implications in medical management and genetic counselling. 18p deletion was first described by de Grouchy and colleagues in 1963 and was estimated to occur in approximately 1/50, 000 live born, which results from deletion of a part or full of the short arm of chromosome 18(Turleau, 2008). The mostly reported clinical features include cognitive impairment, congenital heart defects, small stature, minor facial dysmorphy, and skeletal deformities(Turleau, 2008, Xiao et al., 2019, Hasi-Zogaj et al., 2015, Yi et al., 2014)
Typical facial features include hypertelorism, ptosis, strabismus, broad–flat nose, micrognathia, and low-set big ears. Holoprosencephaly may be seen in approximately 10–15% of patients(Turleau, 2008). In addition, speech and language difficulties, pituitary abnormalities, generalized seizures, dystonia, and autoimmune diseases have also been described(Turleau, 2008, Rao et al., 2001, Graziadio et al., 2009, McGoey et al., 2011). However, these non-specific features are easily overlooked clinically. The clinical phenotype severity is related to the size and location of deletion region. In this report, we present a 2-year-old girl of mosaic trisomy 18 and 18p microdeletion with mild psychomotor retardation, cognitive impairment and language developmental disability.
CLINICAL DESCRIPTION
A 2-year-old female second child of non-consanguineous parents was admitted to our hospital due to growth delay. Her mother and father were 34 years old and 38 years old when giving birth to her. She was born at full-term with uncomplicated gestation, her birth weight was 3.35 kg and the length was about 50 cm. No feeding difficulty and complications were referred in the neonatal period. She had a motor retardation of autonomous walking until 22-months old and intelligence disability and language disability. She only knew a few simple words like ”mama“, not ”baba“, and she cannot communicate clearly with others though she was willing to speak to strangers. Gesell Developmental Schedules performed in local hospital indicated mental developmental delay in motor behavior, language behavior, adaptive behavior and personal-social behavior at age of one year and 8 months old. The height of her father, mother and 15
years old sister were 165cm, 161cm, and 155cm, respectively. No similar history was noted in her family.
On physical examination, she had a height of 81.4 cm below -3SD and a weigh of 11.6 kg below -1SD. Mild craniofacial dysmorphy was present, including thin hair, frontal bossing, low set ears, broad-flat nose, nostrils slightly upward, and downturned corners of the mouth while other craniofacial anomalies were not obvious (Fig.1A). Her hands were small especially her fingers, but the fingernails are normal (Fig.1B). Her teeth were dysplasia (Fig.1C). The echocardiography revealed patent foramen ovale (ϕ 2.96 mm) while no murmur was present. The muscle tension was normal and no other organ abnormality was detected in our patient.
Laboratory examinations (urine, liver, kidney, thyroid hormone, GS/MS and blood glucose analyses) were all normal. Insulin-like growth factor-1 was 72.5 ng/ml (normal range, 55-327 ng/ml).
MANAGEMENT AND OUTCOME
Ten months ago, the child was brought to a local hospital with developmental delay, the peripheral leukocyte karyotype was taken and revealed two abnormal cell lines, the result was 46,XX, psu idic (18)(p11.2)[55]/46, XX, del (18)(p11.2)[45] . She was then referred to another hospital to take the whole-exome sequencing demonstrating a deletion at 18p11.32-p11.22 (GRch37/hg19, chr18:158679 9708482del) and a duplication at
18p11.21-q23(GRch37/hg19, chr18:12012132 78005255dup). She was diagnosed mosaic trisomy 18 syndrome.
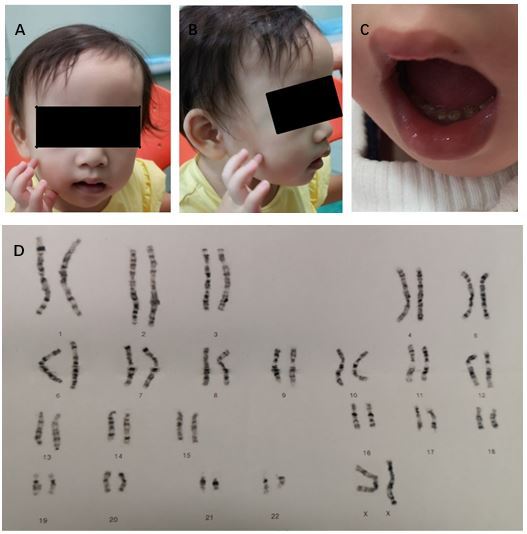
Figure 1: Clinical manifestation and karyotype of our patient. (A and B) thin hair, frontal bossing, low set ears, broad-flat nose, nostrils slightly upward, downturned corners of the mouth, small hands and fingers bilaterally; C) dysplasia teeth; (D) Karyotype shows 46,XX, psu idic (18)(p11.2)[55]/46,XX, del (18)(p11.2)[45]
DISCUSSION
The first reported patients with trisomy 18 syndrome were initially described by Edwards et al and Smith et al in 1960s, while the first case of mosaic trisomy 18 was reported in 1965. Less than 5% portion of patients have mosaicism of trisomy 18, and Banka et al reminded that routine karyotype from lymphocyte culture may not be sufficient to diagnose mosaicism if practitioners suspect a diagnosis of mosaic trisomy 18, karyotype from skin fibroblasts should be considered. Since then over 40 cases of mosaic trisomy 18 have been described, Tucker et al reviewed 33 reported individuals of mosaic trisomy 18 and added 2 more cases in 2007. Their clinical manifestations are extremely variable from complete trisomy 18 syndrome with early death to near totally normal. Some physical features are relatively more common and included brachydactyly, high arched palate, microcephaly, delayed bone age, frequent respiratory infections and otitis media, heart defect, 5th finger clinodactyly, micrognathia, and hypotonia. The most common heart defect is ventricular septal defect in mosaic trisomy 18. Our case has mild craniofacial dysmorphy and patent foramen ovale, and no other physical anomalies were observed.
Trisomy 18 mosaicism usually indicates the existence of more than one cell line in the individual. The peripheral leukocyte karyotype demonstrates pseudodicentric chromosome substituting a normal chromosome 18 in 55 cells and chromosome 18 missing the end of the short arm in 45 cells. The skin fibroblasts karyotype was not taken. Furthermore, there is no correlation between the physical and intellectual findings and the percentage of trisomy 18 cells in either peripheral leukocytes or skin fibroblasts. Besides, there is no correlation between the percentage of trisomic cells in peripheral leukocytes and brain, gonads, or other key organs. The variety of mosaic trisomy 18 may be related to the percentage of trisomic cells in different key organs of the body.
For complete trisomy 18 patients, approximately 50% of infants live longer than one week and about 5-10% of children survive beyond the first year. In overall, trisomy 18 mosaicism patients usually survive longer when compared to complete trisomy 18. This does not mean that all the mosaic trisomy 18 patients have a longer survival, some died a few hours after birth. For normal or mild phenotypical mosaic trisomy 18 cases, some were diagnosed due to recurrent miscarriages or giving birth to a child with trisomy 18 while others may never be identified. 18p deletion syndrome, also called monosomy 18p and De Grouchy syndrome type Ⅰ, which means a deletion of full short arm of chromosome 18 or a microdeletion of the short arm of chromosome 18. Some researches showed that nearly half of patients have breakpoints in the centromeric region and the rest scatter in the short arm, and approximately half of the deletions occur on the maternal chromosome 18 no matter where the breakpoint locations are. Our case’s breakpoint is at the 18p11.32-p11.22. Approximately two thirds of patients’18p deletion are de novo; the rest may be due to a de novo unbalanced translocation or malsegregation of parental chromosome rearrangement or a ring chromosome. The patient’s height and weight is 81.4 cm below -3SD, 11.6 kg below -1SD, respectively. It may be a prodrome of small stature, but her insulin-like growth factor-1 was normal. It also could be contributed to feeding problem. More follow-up work needs to be done to figure it out. Some reported cases show that growth hormone replacement treatment is efficient in growth hormone deficiency patients.
Our case has trisomy 18 and microdeletion 18p mosaicism simultaneously. The possibility of meiotic chromosomal nondisjunction of the ovogonia/spermatocyte was increased because of her parents’ advanced maternal age, some women may have higher a risk for nondisjunction. More possible mechanism may be a de novo unequal recombination occurring in early embryonic mitosis. Some deletions are from the parents, there is no way to figure her mutation mechanism out since we can not get her parents’ consent to analysis. The phenotype of our case combines two syndromes’ typical features, including common psychomotor retardation, cognitive impairment and congenital heart defect, characteristic small stature and language impairment of 18p deletion syndrome. Our case’s uncharacteristic craniofacial features also combine two syndromes.
In a conclusion, mosaic trisomy 18 and 18p deletion syndrome both are chromosomal disorders which has a variety of clinical manifestations. If an individual has untypical phenotypical anomalies and psychomotor and cognitive disability, chromosome disorder should be considered and cytogenic analysis is needed.
Acknowledgements: We thank the patient and his parents for permitting us to use the data.
For more information: https://jmedcasereportsimages.org/about-us/
For more submission : https://jmedcasereportsimages.org/
#Trisomy 18#mosaic#18p microdeletion#Psychomotor retardation#Karyotype#trisomy 18 syndrome#Chao-Chun ZOU#jcrmhs
1 note
·
View note
Text
Air
When I was in college I took a music appreciation class. I’ve always loved music. This class gave me an opportunity to explore various genres of music. For instance, we listened to quite a lot of classical music. Through this experience I gained an appreciation for the classical composer, Johann Sebastian Bach. One piece in particular of his that I enjoy is “Air on the G String.”
I heard this…

View On WordPress
#babies#Disability#doctors#faith#foster care#hospital#Illness#infection#love#nurses#patience#prayer#trisomy 18
0 notes
Text
Reminder that your life matters even if you are disabled or diagnosed with a terminal condition.
198 notes
·
View notes
Text
Giving Life: How does for and to look? The Fight Scavenger Hunt 1.2 - Guest Blog by Chrissy L Whitten
Giving Life: How does for and to look? The Fight Scavenger Hunt 1.2 – Guest Blog by Chrissy L Whitten
First, I want to thank every single person during 2010 and beyond during our time with The Children’s Hospital at Saint Francis in Tulsa, OK. We appreciate each of them for being patient, kind, hardworking, and loving to our family. We went into the unknown at Saint Francis Hospital, scared—walking into darkness. Our first daughter’s life expectancy projection was that her first breath could be…

View On WordPress
#Chrissy Whitten#From Giving to Building#God#scavenger hunt#The Fight#trisomy 18 Edward&039;s Syndrome
0 notes
Text
A woman with two children gets pregnant. She wants another child. Unfortunately, during pre-natal checks, it's discovered that this pregnancy has Trisomy 18, a rare condition which is nearly always fatal. Even in the rare cases where it is not fatal, it can cause severe pregnancy complications and the child that results will require full time care for however long they live.
This woman decided, in consultation with her doctors, that she would prefer not to go through a pregnancy whose overwhelmingly likely result is simply a dead fetus or infant and even whose ideal outcome would result in a substantially reduced ability to parent her other children. Moreover, she still wants another child and does not wish to risk the possible damage to her body and fertility that may come as a result. For this reason she chose to abort the pregnancy.
I think most of us, even a large number of those who consider themselves pro-life, can accept this result. It's not the ideal circumstance any of us would prefer, but the decision is reasonable given the situation.
Unfortunately, this woman lives in Texas and Texas has taken a hard line on its abortion ban, arguing that abortion can only be performed in case of immediate threat to the life of the mother. This position has been taken both by the Attorney General and the Supreme Court of the state, meaning that this is the way the law will be enforced.
Many people who celebrated the end of Roe v. Wade tried to say that this type of situation would never come to pass, that their abortion bans would always be enacted and enforced with an eye toward mercy and care for women. It's been about a year and a half since Dobbs and it's become increasingly clear that this is not the case.
Perhaps there are legal guardrails that should be put around the procedure of abortion, I'm certainly open to the possibility and discussion. But what I think is clear at this point is that the type of people who push for blanket bans on the procedure cannot be trusted to enforce them in any way that is consistent with how the majority of Americans view compassion, mercy, and care for women and families, not to mention medical science. Anyone who continues to argue otherwise is lying to try to get you to enact their extreme agenda.
157 notes
·
View notes
Text
"Just google it" activism has so many issues and inherent hostility to it and i would argue likely pushes people away from a movement and like,, research is a learned skill that i KNOW half the internet doesnt have based on the credibility of the "sources" they cite and im thinking about this again because i looked up what trisomy 18 is out of genuine curiosity and got the texas right to life website so can we maybe stop acting like people asking us genuine questions are always maliciously ignorant
2K notes
·
View notes
Note
Anencephaly, major heart defects, major lung defects, trisomy 13, holoprosencephaly, hydranencephaly, renal agenesis, thanatophoric dysplasia, and triploidy. These aren't "disabilities" ; they are death sentences. You are for forcing women who find out a heart breaking truth to know for months they won't be able to have a baby. You are for forcing an infant into the world only to know torture and agony and pain.
You are a monster, full stop. This is not freedom, this is torture.
Allowing a mother to spend every moment she can with her dying child and also giving her the comfort that she did everything she could rather than the guilt of knowing she had her child killed - that’s what you think is torture?
No family should go through this alone, and there are great resources for perinatal hospice that should be made available to parents.
Also, the number of times doctors have been wrong about a diagnosis or survival chance…
Not to mention new options for correcting issues by performing surgery on a baby in utero to save lives:
Heart surgery for Trisomy 13 and 18, surgery for spina bifida, Renal Anhydramnios Fetal Therapy for renal agenesis, placenta-derived stem cell therapy for spinal bifida, just to name a few
My husband’s parents were told he wouldn’t survive. They were told to abort, and they refused. They planned to say goodbye to him in the hospital after he was born. All the family came. He was born, baptized by his grandpa, and rushed to surgery.
As you probably figured out, he survived (since he is now my husband). He has no lingering effects of the condition that doctors said would kill him, except that he only has one kidney (and doctors now say he has normal kidney function because his single kidney grew to compensate).
Doctors aren’t omniscient. Conditions that were death sentences 20 years ago are now treatable. New surgeries and procedures are constantly being developed.
We’re not going to sentence babies to death because a doctor says they’re going to die. Sorry not sorry.
493 notes
·
View notes
Text
Republicans are thrashing around trying to get themselves out of the abortion ban they have tried to win for so many decades.
Senator Lindsey Graham (R-SC) was the first. In the fall of 2022, just months after the Supreme Court struck down Roe v. Wade, he proposed legislation calling for a national abortion ban after 15 weeks. So far, this bill has gone nowhere. Then, in 2023, gubernatorial candidate Glenn Youngkin of Virginia put the 15-week abortion ban at the center of his campaign to help the GOP take full control of the Virginia legislature. Rather than holding one house and picking up the other, he lost both. Recently, former President Donald Trump—who often brags about appointing the three Supreme Court justices who made possible the repeal of Roe v. Wade—offered his own way out of the thicket by applauding the fact that states now can decide the issue for themselves. And in Arizona, the Republican Senate candidate, Kari Lake, is trying to rally the party around the notion of a 15-week ban instead of the 1864 near total ban their court just affirmed, even though she’s facing criticism for this on the far right. Meanwhile, the Wall Street Journal came out with a poll showing that abortion was the number one issue—by far—for suburban women voters in swing states.
In each instance (and there will be more) we find Republicans desperately trying to find a position on the issue that makes their base and the other parts of their coalition happy.
It doesn’t exist, and here’s why—abortion is an integral part of health care for women.
Since 2022, when the Supreme Court eviscerated Roe in the Dobbs case, we have been undergoing a reluctant national seminar in obstetrics and gynecology. All over the country, legislators—mostly male—are discovering that pregnancy is not simple. Pregnancies go wrong for many reasons, and when they do, the fetus needs to be removed. One of the first to discover this reality was Republican State Representative Neal Collins of South Carolina. He was brought to tears by the story of a South Carolina woman whose water broke just after 15 weeks of pregnancy. Obstetrics lesson #1—a fetus can’t live after the water breaks. But “lawyers advised doctors that they could not remove the fetus, despite that being the recommended medical course of action.” And so, the woman was sent home to miscarry on her own, putting her at risk of losing her uterus and/or getting blood poisoning.
A woman from Austin, Texas had a similar story—one that eventually made its way into a heart-wrenching ad by the Biden campaign. Amanda Zurawski was 18 weeks pregnant when her water broke. Rather than remove the fetus, doctors in Texas sent her home where she miscarried—and developed blood poisoning (sepsis) so severe that she may never get pregnant again. Note that in both cases the medical emergency happened after 15 weeks—late miscarriages are more likely to have serious medical effects than early ones. The 15-week idea, popular among Republicans seeking a way out of their quagmire, doesn’t conform to medical reality.
Over in Arkansas, a Republican state representative learned that his niece was carrying a fetus who lacked a vital organ, meaning that it would never develop normally and either die in utero or right after birth. Obstetrics lesson #2—severe fetal abnormalities happen. He changed his position on the Arkansas law saying, “Who are we to sit in judgment of these women making a decision between them and their physician and their God above?”
In a case that gained national attention, Kate Cox, a Texas mother of two, was pregnant with her third child when the fetus was diagnosed with a rare condition called Trisomy 18, which usually ends in miscarriage or in the immediate death of the baby. Continuing this doomed pregnancy put Cox at risk of uterine rupture and would make it difficult to carry another child. Obstetrics lesson #3—continuing to carry a doomed pregnancy can jeopardize future pregnancies. And yet the Texas Attorney General blocked an abortion for Cox and threatened to prosecute anyone who took care of her, and the Texas Supreme Court ruled that her condition did not meet the statutory exception for “life-threatening physical condition.”
So, she and her husband eventually went to New Mexico for the abortion.
Obstetrics lesson #4—miscarriages are very common, affecting approximately 30% of pregnancies. While many pass without much drama and women heal on their own—others cause complications that require what’s known as a D&C for dilation and curettage. This involves scraping bits of pregnancy tissue out of the uterus to avoid infection. When Christina Zielke of Maryland was told that her fetus had no heartbeat, she opted to wait to miscarry naturally.
While waiting, she and her husband traveled to Ohio for a wedding where she began to bleed so heavily that they had to go to an emergency room. A D&C would have stopped the bleeding, but in Ohio, doctors worried that they would be criminally charged under the new abortion laws and sent her home in spite of the fact that she was still bleeding heavily and in spite of the fact that doctors in Maryland had confirmed that her fetus had no heartbeat. Eventually her blood pressure dropped, and she passed out from loss of blood and returned to the hospital where a D&C finally stopped the bleeding.
These are but a few of the horror stories that will continue to mount in states with partial or total bans on abortion. As these stories accumulate, the issue will continue to have political punch. We have already seen the victory of pro-choice referenda in deep red conservative states like Kansas, Kentucky, Montana, and Ohio; and in swing states like Michigan and in deep blue states like California and Vermont. In an era where almost everything is viewed through a partisan lens, abortion rights transcend partisanship.
And more referenda are coming in November. The expectation is that at least some, if not most, of the pro-choice voters likely to be mobilized by the abortion issue will help Democrats up and down the ballot. As a result, Democratic campaigns are working hard to make sure the public knows that Republicans are responsible.
46 notes
·
View notes
Photo
Non-Invasive prenatal testing (NIPT) is a blood screening test can assess the risk of a fetus will be born with certain genetic abnormalities. The testing analyses small amounts of fetal cell free DNA that is in the mother’s bloodstream. NIPT is a screening test that can determine whether the fetus is at higher or lower risk for a condition. Book your Genes2Me NIPT test now!
#NIPT #NIPTTest #Pregnancy #NonInvansive #Trisomy18 #Trisomy21 #ChromosomalMicroarray #Chromosomal #PregnancyTest #AntibodyTest #Sequencing #PregnantWomen #Genes2Me #GeneticTesting #RTPCRTest #Antigen #AntigenTest
For more details, Call us on 18001214030 or drop us an email at [email protected] for an Appointment
To know more visit. https://t2m.io/DTjoF2P
0 notes
Last Seen Blogs

incelsss
CEO of Weirdos

dreamsofknighthood
I will be a knight, Python. Just you watch!

doing-t0m-daley-blog
Go on shake it up what you got to lose ?
glitternymph
demi devil

jamesjanzen
Nurturing ministry for artists and churches