#this is definitely enough to constitute as a diagnosis for some kind of mental illness
Text
the latest spoke video possessed me for a bit . i also had a rough day today resulting in me writing this unreadable ramble about him on my textbook . talking about ls is literally my coping mechanism......... you might die reading this you have been warned. all the "spoke" in this refer to c!spoke btw
i have s ome very brief and short and concisely worded opinions on the new spoke video ! i want this to be some kinda character study but im not mentally capable enough to do that rn. my favourite part of spoke is his like. personality in general especially how he thinks and how he works to achieve his goals if i dont get it out of my system RIGHT NOW i will explode .
is spoke evil? well in my humble opinion his actions do come from what he thinks are correct / the right thing to do. most notably "to bring peace to lifesteal" at the end of season three. i genuinely dont think this is a lie or a smokescreen to hide his evil intentions etc. but like how bringing peace to lifesteal literally meant to kill everyone permanently, it does seem that he takes quite the radical route to do stuff every time, which caused real harm and destruction. i dont think that gets discussed enough
wiping out the entire server for peace ? whatever ill let that slide. sure . exploiting and taking advantage of the last bit of sympathy and kindness in lifesteal players by staging a fake spawn trap as bait to trick apo members wanting to rescue terry into talking? uhhhhh whatever sure. ok yea. "you can kill him if you want . you can start killing them if you want (o^^o)" blatantly saying that with a smile? "in parrots eyes this is a friendship reunited [...] however this is only one step of my true master plan."??????okay you need to be put in a padded cell immediately. actually that might be to humane you should be put on a remote island as far as possible from land . but you also did nothing wrong innocent lil dude whos just a bit silly. i think you should be put in human society and be allowed to do whatever you want
in conclusion i despise you spoke from spokeishere and i love you . i want to hug you then scream in your ears at the top of my lungs when you least expect. your awful you're evil and you're innocent and you're awesome. you treat trust from others like its nothing. you exploit other people s kindness . you always do things for the greater good. and you're spokeishere (i think thats what his name is i dont watch him that much)
in conclusion of the conclusion. did he really have to all that do achieve his goals that apparently are actually very good and good for the sever? are his goals really that honourable anymore when achieving them comes with such a hefty price tag and death toll? what if in a future event his goals aren't the morally correct thing to do in the first place, then with a passion for working towards his ideals as strong as his, wouldn't mean that he is the ultimate bad person? is he a bad guy anyway ??????my answer to that will be a resounding: "uh idk"
spoke never did anything wrong btw. aldo does anyone else think spoke sounds like hes 7 years old sometimes. not his sentences his voice, he
(the gibberish ends there)
#lifesteal#spokeishere#this is definitely enough to constitute as a diagnosis for some kind of mental illness#no actual way being this. normal ! about block lego people and their lego swords#please dont block me im normal i swear i swear i swear#what does any of this mean
15 notes
·
View notes
Text
Anders & Mental Illness
Cause someone kinda spurred this Wall of Text.
You want unpopular opinion time? Here ya go: Anders is NOT mentally ill.
So what are the symptoms that people are seeing that make them see mental illness, which, for the purposes of this post, will be a medical diagnosis concerned with neural biochemistry that can never be cured, but can be managed with the assistance of medication to help correct the body’s own imbalance.
Anders DEFINITELY has post-traumatic stress disorder. Please note, this is not considered a mental illness by way of biochemistry. It is a learned behavior and associated response, an extreme form of Pavlov’s conditioning, that can be treated through cognitive therapy, medication, and time. Why does he have PTSD? Let’s go down the list:
Because he’s been trained to hate himself since he manifested magic. Not because he did something wrong, but because of how he was born. Yay, let’s teach people to hate themselves for being born.
Because he’s been taught he’s a walking weapon.
Because his own family went from being as much a family as any other (with good and bad points) to essentially calling him a monster and throwing him out like so much garbage.
Feelings of persecution because, well, he is taken from his family, called a monster, and then locked into a tower/prison to experience little to no privacy and under constant guard where any small movement, action, or thought could be met with abuse, torture, or death.
Solitary confinement – MULTIPLE TIMES. Please note, while there is not much in canon about the type of solitary confinement used, it is generally a small cell (60-80sq ft, or a 6-8’x10’ cell). This is where everything is done – eating, drinking, sleeping, reliving oneself.
For Solitary Confinement:
There may be extreme sensory deprivation – there may or may not be light, sounds may be constant or none at all or that idle drip-drip-drip of condensation on stone. There is no actual human contact.
As if mages are dehumanized already, the combination of isolation and sensory deprivation furthers this dehumanization in that you will eventually start to question reality itself. Once you leave this sort of confinement, readjusting to the sights, sounds, and textures of the real world is a major hardship. Everything is too loud, too bright, too textured, too everything – it’s a total body sensory overload.
For someone so steadfastly opposed to being confined, who has escaped multiple times simply to be free? Solitary confinement is the WORST type of abuse. It’s throwing an arachnaphobic into a room full of spiders, or a claustrophobic in a tiny box, or an agoraphobic into an open field. It is their worst nightmare come to life. Short-term, it would excruciating, but multiple times with ever-lengthening terms? That creates a desperation that will lead to severe risk-taking, extreme levels of anxiety, a desperate need-to-please to avoid that situation again (very Stockholm Syndrome), and suicidality. But of course, the institution that does all this doesn’t care. One less mage to worry about.
From an RL-perspective, the United Nations has classified anything over 15days in solitary confinement “constitutes cruel, degrading and inhumane treatment, or torture.” For someone who is mentally ill already (again, see above), the pressures exerted on the human psyche for such extended periods of time would resolve into a complete psychological break.
Based on all of that? It’s a wonder Anders is functional at all, though we know people who have survived such things and live with PTSD and can be function. It shows a pure strength of self and major resilience. THAT we do see in Anders.
So now we’re going to look at the why so many see the shift between DAA and DA2 Anders as absolutely signs of mental illness. So DA2 was a rushed mess with a seriously unreliable narrator and essentially decided to disregard almost everything from DAA. Remarkable storytelling, there, BioWare. Good on ya. *rolls eyes*
DAA Anders. Ah, yes, the sassy, snark-driven flirt that everyone adores. It’s called OVERCOMPENSATION. Anders knows full well if this last escape attempt doesn’t work, he is, quite literally, a dead man. While he has no fucks left to give on many levels, he will fight that one tooth and nail. He would rather die than go back to solitary or be given a lobotomy. He will rail against authority, but anyone who gives him an ounce of positive reinforcement, an ounce of kindness, that is something to which he will cling with desperation and do anything to keep that positivity occurring. Especially if it can in some way prevent what he fears the most. So he flirts, is charming, is sassy, is snarky, and is HELPFUL. He may have a mouth on him, but he IS helpful. He wants to ingratiate himself. It’s also a self-defense mechanism where if he can deflect everything with wit and sass, no one will actually know what terrifies him the most and give them leverage over him. He can’t afford that vulnerability.
But he cannot hide the anger – that is there, in spades and then some. He remembers enough of his life before the Circle to know there is a better life. He is angry for everything he has felt in the Circle, for all the people who were hurt there, for how he was hurt there, for how anything resembling any sort of goodness was stripped away, beaten out, abused, or killed. They were not allowed anything truly good in their lives and he had had that, tasted it, wanted it. Knew it was there. So he is angry, furious, fighting so hard to be free and be allowed to breathe and just be him, not some monster they kept telling him he was. He didn’t feel like a monster, he didn’t want to be a monster, but he was still terrified he was one.
And so he becomes a Warden – mostly because he can and as yet another last-ditch effort (he has a lot of those) to break free from the tyranny of the Circles and his impending death sentence at the hands of the templars. The Wardens should be his escape. They are an organization beholden to NONE. Their backgrounds effectively cease to exist, for the most part. It doesn’t matter if they are rogue, warrior, thief, murderer, or mage – once they are joined, they are Wardens. And if it weren’t for the continued persecution of the templars who simply cannot stop being assholes, who knows what might have happened. He did already exhibit traits of fighting for freedom, his own if no one else’s, at this point. Justice helped him see that there were more people oppressed and made him start thinking about that.
For all the extra time he had before being taken to the Circle, Anders is still young. Though there are no canonical ages mentioned, general thought is that DAA Anders is early-20s. And the Circles are geared toward keeping mages naïve and helpless, to keep them like young children so they are, by necessity, required to rely upon their captors for survival. Anders has a bit more independence going into that environment than many, which is how he continued to fight and get himself in trouble. He’s very strong-willed with a drive for independence, but he’s still effectively in the mindset of a troubled teen.
Yet with all of that, there really isn’t any mental illness. There is the PTSD, the anxiety and paranoia, the overcompensation, all from truly legitimate and horrifying experiences that would leave multiple symptoms of lasting impact in varying extremes. Again, PTSD is a learned response to stimuli. He is reacting based on previous experiences and results. And it absolutely influences day-to-day interactions even if the experience is in the past, because the key part of PTSD is that the past is NOT the past, it is still actively influencing the present, even if those stimuli are not actively in the present.
So let’s talk DA2 Anders. This is actually my preferred Anders. Why? Because he has grown up. He’s been given the TIME to actually figure himself out to a degree outside the confines of the Circle. And do you know what he found? That is has mountains of strength and compassion to give to others. That he can say NO to some things. Do you have any idea how difficult is to say NO when you’ve been indoctrinated like that? It’s one of the hardest things in the world to do and even when you learn it and can say it, it can still be such a struggle to fight to listen to yourself and your feelings and not fall prey to that belief that it would simply be better for everyone if you said yes, no matter how horrible it may be for you to do so.
Anders in DA2 is a semi-to-mostly-functioning adult, as any adult would be after going through his life experiences, but all in all, he’s actually doing okay for himself. He’s managing. Sometimes, that is the absolute best we can manage. We find out that he merged with Justice from DAA. A lot of people will claim this, in and of itself, makes him bipolar or, at the very least, the outdated Multiple Personality Disorder (now Dissociative identity disorder), wherein there are a minimum of two distinctly separate identities that persist. On the outside? Eh, I can sorta see it…EXCEPT. Justice isn’t Anders splitting his psyche into multiple pieces. Justice is JUSTICE, a Spirit of the Fade. A personality in and of itself/himself (and this particular personification of Justice chooses to be male, so male pronouns from here on out). Justice isn’t a fragment of Anders’ personality. He is a spirit who inhabits a living form that already has a soul. YOU LITERALLY HAVE TWO SOULS IN ONE BODY. This is not a mental illness, this is spirit possession. So DID can go straight out the window on this one.
And then there’s that whole spirit/demon thing. Justice IS NOT a demon. He’s one hell of a hard ideal, in spirit form. I have an entire essay written about Fade Entities, but that’s another topic. Needless to say, Justice isn’t some cute lil cricket on Anders’ shoulder. Justice is a burning ideal in a world full of injustices. And Justice, as we can see in DAA, is actively learning about the world around him. He becomes, essentially, a very protective elder brother to Anders as you can see Justice only really breaks out and takes control in DA2 when Anders is clearly at breaking point and under severe emotional distress. Imagine Hawke going to bat for their younger sibling in times of distress and you have Justice, wielding the blue fire and lighting of the Fade. Justice allows Anders to know there is someone always looking out for him, who always has his back. He allows Anders to feel a modicum of safety and gives him that push to allow him to be who he is. He is, in a word, family. Not easy, not kind, not always loving, but he is the chosen family – the blood of the covenant, not of the womb – and that much stronger for it.
Justice gave Anders a type of companionship after years of solitary confinement that no one else could. Justice helped anchor Anders, even though he pushes him hard. Spirits can learn (Justice does, Cole does, even Wynne’s Spirit of Faith does) and they learn their environments and hosts if need be. But inhabiting the living body of someone who has experienced everything Anders has? It makes Justice very protective and very angry, but that doesn’t make him a demon. It actually makes him more human. He feels righteous fury at those who hurt his friend and continue to hurt him and others like him. He feels insulted and personally attacked whenever he is called demon because he knows Anders’ fears about himself and Justice and their merging and he would never want anything like that to hurt his friend or for he, himself, to fall to that. But he hasn’t. Justice is still Justice and still that same ideal. To warp Justice into a demon would require Justice brutalizing everything he is and warping the ideal of justice into something else entirely. And vengeance doesn’t count here – they are two sides of the same coin, which is why you often see vengeance called vigilante justice. If the order of the world dictates that those in power do not provide justice, then vigilantism is the justice they receive. I’m not even entirely sure what Justice could become if he was able to be warped enough into a demon, actually, no, I take that back, he would become Zealotry – the brute enforcement of an ideal, fanatical enforcement of an idea with no regard anything but that. And that is NOT Justice. There are much better examples of zealotry in Thedas.
Does Anders have aggressive self-defense mechanisms? Oh hell yes. He actually aggressively overacts to quite a few things to the point Hawke really should have smacked him upside the head a few times. But it goes back to that old saying where it’s not paranoia if they’re actually out to get you. And yes, they are actively and actually out to get Anders. Yet for all of this? For all that he remains hunted, for all that his very existence is hated and persecuted and reviled? He starts up a free clinic. He uses his magic to heal people without asking for anything in return, except maybe to be left alone and maybe, just maybe get a warning if the templars are too close. He has so much compassion, even after everything he has experienced. He cares enough to not want others to experience what he has experienced.
So let’s get back to mental illness. I see a lot of references to manic episodes. Now, I know that everyone who is diagnosed with BPD, I or II, experiences their own form. It’s different for everyone. I have BPD II and have only experienced medication-induced manic episodes and YIKES – I don’t know how anyone deals with those on a regular basis at all. I get the funzies of depressive episodes, sometimes so badly they will pull me under. Sometimes, so badly that yes, suicide is at the forefront of my thoughts. A lot of that has to the with the diagnosed PTSD and self-hatred that I have been trained to have. Indoctrination is a bitch. Therapy is helping, but it took years to get this shit diagnosed even after years ago, I had done enough research to kind of diagnose myself. But no one wanted to believe me when I brought it up as a possibility. People see other people functioning, to the most basic appearances, normally, and they hand-wave away the idea that there might be a problem. So that said, let’s take a look at manic episodes.
I’m going with a firm NO on this one. The closest thing I can see to manic episodes are when Anders is working almost feverishly on his manifesto. No abject risk-taking that was any more prevalent than his multiple escape attempts. The closest thing we have to that is him running a free clinic and the mage underground in Kirkwall. Hell, him breathing in Kirkwall is risk-taking. But the manifesto nights? It’s less manic and more avoidance, in my mind. I’ve done it. It’s keeping so busy that you don’t have time to think about the bad things that are constantly in your head. Keep busy, keep healing, keep writing, keep fighting and for the love of all that is good, DON’T SLEEP. Don’t let the dreams in, don’t be helpless and vulnerable. Work until you’re so exhausted and you don’t dream, then wake exhausted again and do it again. This is PTSD-anxiety at work combined with night terrors. He is terrified of going to sleep, of being vulnerable to attack, of the nightmares of not just the taint, but of dark spaces and helplessness and the Fade and memories of failures, all those he couldn’t protect. He drives himself so hard so he doesn’t have to think of those things. It’s a defense mechanism. It’s mostly utilized for anxiety and depression when dealing with PTSD or with basic extreme stress/duress and grief, and his history clearly can point to when those started.
Oh, wait, I mentioned depression up there, didn’t I? Hey, that’s a mental illness! Yes, it is. Absolutely. But you can be depressed without having the mental illness/biochemistry maladaptation. Damned genetics. ANYWAY. PTSD causes extreme reactions, stress and duress, anxiety, and yes, depression. You can’t escape the anxiety, the fear responses, the need to either work yourself to the bone or sleep away the pain. In Anders’ case, it’s working himself so he doesn’t dream. Guess what happens when you do that to yourself over and over and over again? The body isn’t designed to go without sleep and proper rest. Those of us with sleep disorders will tell you (and it’s in the medical literature if you care to research it) that that degree of sleep deprivation will cause depression. It’s not necessarily a matter of biochemistry, but that of situational body adaptations to not being able to recuperate.
So there it is in a very large nutshell – my thoughts on why Anders is NOT mentally ill. I get that some people want to see themselves in their favorite characters. I relate to Anders on many levels, but I cannot put my diagnoses on him.
#dragon age#anders#justice#daa#da2#ptsd#ptsd vs mental illness due to biochemistry#wall of text#anders - mental health
8 notes
·
View notes
Text
Why PTSD May Plague Many Hospitalized Covid-19 Survivors
https://sciencespies.com/nature/why-ptsd-may-plague-many-hospitalized-covid-19-survivors/
Why PTSD May Plague Many Hospitalized Covid-19 Survivors

While neuropsychologists Erin Kaseda and Andrew Levine were researching the possibility of hospitalized Covid-19 patients developing post-traumatic stress disorder (PTSD), they heard reports of patients experiencing vivid hallucinations. Restrained by ventilators and catheters, delirious from medication and sedatives and confused by the changing cast of medical professionals cycling through the ward, intensive care unit (ICU) patients are especially prone to trauma. For Covid-19 ICU patients, a combination of factors, including side effects of medication, oxygenation issues and possibly the virus itself, can cause delirium and semi-consciousness during their hospital stay. Kaseda says as these patients slip in and out of consciousness, they may visualize doctors wheeling their bodies to a morgue or see violent imagery of their families dying. Such instances, though imagined, can cause trauma that may lead to PTSD in patients long after they have physically recovered from Covid-19.
In addition to hallucinations during hospitalization, some Covid-19 survivors describe a persistent feeling of “brain fog” for weeks or months after recovery. “Brain fog” is an imprecise term for memory loss, confusion or mental fuzziness commonly associated with anxiety, depression or significant stress. As scientists grappled with whether such brain damage could be permanent, Kaseda and Levine warn that cognitive issues often attributed to “brain fog” may, in fact, be signs of PTSD. Kaseda, a graduate student at Rosalind Franklin University of Medicine and Science in Chicago, and Levine, a professor of neurology at the University of California Los Angeles, co-authored a study published in Clinical Neuropsychologists in October intended to alert neuropsychologists to the possibility of PTSD as a treatable diagnosis for those who survived severe illness from Covid-19.
“You have this unknown illness: there’s no cure for it, there’s high mortality, you’re separated from your family, you’re alone,” Kaseda says. “If you’re hospitalized that means the illness is pretty severe, so there’s this absolute fear of death that even if you aren’t having the delirium or the other kind of atypical experiences, just the fear of death could absolutely constitute a trauma.”
How Post-Traumatic Stress Develops in Covid-19 Patients
PTSD arises from experiencing or witnessing a traumatic event, specifically exposure to actual or threatened death and serious injury, according to the American Psychiatric Association.
Historically associated with combat veterans, PTSD was called “shell shock” or “combat fatigue” before it became a named disorder in 1980. But in 2013, the definition of PTSD broadened to include more common place traumatic experiences.
Psychiatrists are now increasingly seeing PTSD develop after traumatic stays in the ICU for any health problem, but researchers are still unsure of the scope of this issue. A paper published in 2019 in the Lancet reports that roughly a quarter of people admitted to the ICU for any health issue will develop PTSD. Another study found that between 10 and 50 percent of people develop PTSD after ICU discharge, and, in a 2016 study of 255 ICU survivors, one in ten reported PTSD within one year after discharge.
Before hospitalized patients are diagnosed with PTSD, their symptoms may be described as post intensive care syndrome (PICS). PICS can manifest as a number of physical, cognitive and mental health problems that a patient may experience in the weeks, months or years after being discharged from the ICU.
Kristina Pecora, a clinical psychologist at NVisionYou in Chicago, sees a variety of patients, including frontline medical professionals and Covid-19 survivors. Pecora was a contributing author of a brief submitted to the American Psychological Association in May describing the signs of PICS and urging psychologists to prioritize screening and referral for behavioral health problems related to hospitalization for Covid-19. At that time, some of Pecora’s patients showed signs of the lingering trauma typical of PICS within six months of their ICU discharge. Because a PTSD diagnosis can often only be made after this period, it was too early to tell then whether her patients’ PICS symptoms could be classified as PTSD. But the impact of the virus on their psychiatric health was clearly substantial.
“It becomes this gradual realization that what they’re experiencing is persisting week after week and ‘oh my goodness, this is a longer-term experience than what we thought it would be,’” Pecora says.


Restrained by ventilators and catheters, delirious from medication and sedatives and confused by the changing cast of medical professionals cycling through the ward, ICU patients are especially prone to trauma.
(Photo by Sebastian Gollnow/picture alliance via Getty Images)
A “Delirium Factory”
One major factor in whether patients develop long-term psychological effects after ICU discharge is whether or not they experience delirium during their stay. Delirium is a state of severe confusion and disorientation, often characterized by poor memory, nonsensical speech, hallucinations and paranoia. Patients who experience delirium may not be able to differentiate between real and imagined humans or events.
Side effects of sedatives, prolonged ventilation and immobilization are common factors that put many ICU patients at-risk for delirium. A study from 2017 found that up to 80 percent of mechanically ventilated people enter a hallucinogenic state known as ICU delirium.
Add isolation and the unknown cognitive effects of the virus to the mix and an ICU becomes a “delirium factory” for Covid-19 patients, as authors of a study published in BMC Critical Care in April wrote. In a different study from June, which has not yet undergone peer review, 74 percent of Covid-19 patients admitted to the ICU reported experiencing delirium that lasted for a week.
“Any time anyone is in a fearful experience and they’re isolated—they can’t have anybody in their rooms—they wake up in a strange experience or a strange place, or they know already while they’re in there that they can’t have anyone hold them or be with them. All of that is going to attribute to the emotional impact,” Pecora says.
Such intense visions and confusion about the reality of hospitalization can be especially scarring, leaving patients with intrusive thoughts, flashbacks and vivid nightmares. If such responses persist for more than one month and cause functional impairment or distress, it may be diagnosed as PTSD.
To help reduce ICU-related trauma, doctors may keep a log of the patient’s treatment to help jog their memory once they have been discharged. Having a record of the real sequence of events can help a patient feel grounded if they have hallucinations and flashbacks to their hospitalization experience.
But even for patients experiencing Covid-19 symptoms that aren’t severe enough to warrant a hospital visit, the fear of death and isolation from loved ones can be sufficiently distressing to cause lasting trauma. They may experience shortness of breath and worsening symptoms, fueling a fear that their condition will quickly deteriorate. For several days, they may avoid sleeping for fear of dying.
“Some people are more resilient in the face of that sort of trauma and I would not expect them to develop lasting psychological symptoms associated with PTSD,” says Levine. “But other people are less resilient and more vulnerable to that.”
Learning from SARS and MERS
Covid-19 isn’t the first epidemic to cause a domino effect of persisting psychiatric health problems across a population. The current pandemic has been compared to the severe adult respiratory syndrome (SARS) outbreak in 2003 and the Middle East respiratory syndrome (MERS) outbreak in 2014 in Saudi Arabia—both diseases caused by coronaviruses. In an analysis of international studies from the SARS and MERS outbreaks, researchers found that among recovered patients, the prevalence of PTSD was 32.2 percent, depression was 14.9 percent and anxiety disorders was 14.8 percent.
Much like those who fall ill with Covid-19, some patients sick with SARS and MERS developed acute respiratory distress syndrome (ARDS), which causes patients to experience similar feelings of suffocation and delirium during treatment in the ICU. Levine says that many of the people who developed PTSD during the SARS and MERS epidemics were hospitalized.
By contrast, Levine anticipates Covid-19 survivors with relatively mild symptoms may experience traumatic stress too, due to an inundation of distressing images, frightening media reports and a higher expectation of death.
For those who recover from Covid-19, their trauma may be compounded by social isolation and physical distancing practices after they are discharged from the hospital. “If you did experience a trauma, it can make it so much harder to naturally recover from that when you lack the social support from family and friends that maybe would be possible to receive in different circumstances,” Kaseda says.
Screening for PTSD in Covid-19 survivors soon after recuperation is important, Kaseda says, so that patients can receive the right treatment for their cognitive difficulties. If PTSD is treated early on, it can speed a person’s entire Covid-19 recovery.
“If we can treat the PTSD, we can see what parts of the cognition get better,” Kaseda says. “And that will give us more confidence that if problems persist even after the PTSD is alleviated, that there is something more organic going on in the brain.”
A Constantly Shifting Landscape
As more information about the traumatic effects of Covid-19 treatments become clear, neuropsychiatrists and psychologists can shift their approach to dealing with the cognitive effects of Covid-19. Scientists don’t yet have a full grasp on how Covid-19 directly affects the brain. But by maintaining an awareness of and treating PTSD in Covid-19 patients, psychiatrists and clinicians may be able to minimize some cognitive problems and focus on the unknowns.
“Part of the problem is that all of this is so new,” Pecora says. “We’ve only really been seeing this for six or seven months now and the amount of information we have gleaned, both in the medical and the psychological worlds has increased so exponentially that we have a hard time keeping up with what were supposed to be looking out for.”
Deeper understanding of which symptoms arise from brain damage and which are more psychological will help both clinicians and psychologists address patients’ needs in their practice.
“The social and emotional impact of Covid-19 hasn’t even dawned on us yet. We clinicians and doctors are certainly trying to prepare for it.,” Pecora says. “But the way this has impacted society and mental health is going to be so vast.”
#Nature
0 notes
Text
iridology definition: what is iridology
1)iridology definition from David J. Pesek, Ph.D.,
What is Iridology
"The Iris, Sclera and Pupil of the eye show the veil the soul has created, through consciousness (or forgetfulness), that reflects the illusion which prepares the soul for attaining the reality of full enlightenment."
~David J. Pesek, Ph.D., September 1988
An Introduction
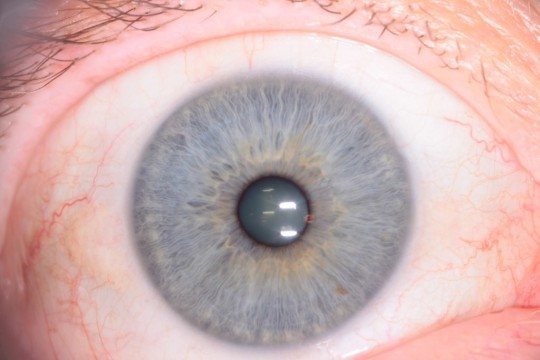
Eyes have long been referred to as the "Windows of the Soul." But few people are aware of just how true this observation is. Accurate analysis of iris structure and pigmentation provides information about you or your clients that is hard to find through other methods. This information is so valuable that Iridology deserves to become a widely practiced assessment tool in both the physical and psychological health fields. There are a multitude of factors that influence our health and personality, and many of these factors are reflected in the iris. Look closely at your eyes in a mirror, and then at the irises of those around you. You will see many different patterns of iris fibers and colors. Like fingerprints or faces, no two are exactly alike, and neither are we! The iris structure is so unique; it is now being used for security identification at ATM machines and airports. Microsoft's house of the future will use an eye scanner to identify residents and unlock the door.
http://www.iriscope.org/iridology-definition.htm
What is it?
Iridology is based on the scientific study of the iris -- the colored part of the eye. Like markings on a map, the iris reveals physiological conditions, psychological health risks, challenges and/or strengths of various organs and personality traits.
Through iridology we can get an understanding of your past, present, and potential future health conditions by assessing the various body systems. Your inherited tendencies compounded by toxic accumulations in various parts of your body are also revealed.
The Science of Iridology is based on the analogy of one of the most complicated tissue structures of the whole body - the iris.
It is a method whereby the doctor or health practitioner can tell, from markings or signs in the iris, the reflex condition of various organs and systems of the body. These markings represent a detailed picture of the integrity of the body; it's constitutional potentials, areas of congestion or toxic accumulations and inherent challenges and gifts.
The four principles that form the cornerstones of iridology are:
The condition of the nerves
The condition of the blood and lymph system
Adequate circulation
Nutrition - rest quality, breathing - state of mind
Nature has provided us with an invaluable insight into the vital status of the health of the body by transmitting this information to the eye.
The laboratory testing procedures practiced today, which are not always necessary, are expensive, time-consuming and, often, uncomfortable to the patient. With iridology, we have a simple, painless, economical and non-invasive way of looking into the body. This is not to say that it should exclude other forms of analysis. On the contrary, it may be employed in conjunction with any other system of analysis or a diagnosis that a practitioner wishes to use. Now, more than any other time in history, we are in a need of accurate and less complex means of analyzing a patient's condition.
Eighty percent of the diseases treated in this country are of a chronic nature. The tissue found in chronically afflicted patients can be monitored better in the iris of the eye than, possibly, by any other method of analysis.
Iridology gives an essential insight to the development of these chronic diseases or the diminishing of that disease or inflammation.
The Science of Iridology is based on the analysis of one of the most complicated tissue structures of the whole body-the iris. Iridology offers a unique perspective to the concept and practice of preventive health care. It involves a non-invasive diagnostic procedure, commonly used by the European practitioners and may be useful in the detection of existing conditions as well as inherited genetic weaknesses. It is known that approximately 300 thousand nerves from various parts of the body make their way to the optic nerve. Therefore, projection of systemic activity may be visible at the iris.
A Brief History of Iridology
Iridology research began in 1670 when Dr. Philippus Meyens published a paper describing the eyes of his patients when they became sick or injured. He also noticed changes in the eye that came with healing and was able to link points on the iris to specific parts of the body. By observing the eye, he was eventually able to identify areas in the body in need of support which would show up in the eye long before physical symptoms would manifest.
While eyes have been a focus in civilizations throughout the ages, "modern" Iridology got its start just over 100 years ago. In the late 1800's, a physician from Hungary and another from Sweden began observing eyes and organizing their findings. This process of observation and correlating has been slow, but it established a foundation for others to build on. The first book on Iridology in America, by an emigrated Austrian physician, was printed in 1904. This was followed by the works of N.D.s and other naturopathic oriented M.D.s.
Working with limited magnification and photography equipment, progress was difficult. Then with the emergence of the AMA and other political and economic influences and the advent of "miracle" drugs, almost all natural medicine practices declined in this country. Dr. Bernard Jensen is credited with keeping Iridology alive in North America.
In Europe, a different political and economic climate created an environment that has allowed Iridology (and other natural medicine practices) to evolve. Extensive research has been carried out in Europe and iridology is now widely accepted as a valuable preventative health care approach. Currently in the U.S. more people are showing interest in iridology as an alternative method for improving health. Now you can experience the benefits of this remarkable assessment tool/technique.
What are the benefits of Iridology?
Iridology treats the person instead of the symptoms. Through understanding your genetic vulnerabilities and reactive patterns, you can maintain balance and guard against illness. The body has its own healing wisdom, given the opportunity. Iridology offers a simple economical way to learn to care for your body.
The fundamental goal of iridology is prevention of serious degenerative processes by integrating nutritional, mechanical (chiropractic), spiritual and emotional support. Some of the benefits of iridology are:
Overall health awareness
Understanding how the organs interact
Knowing which organs are under or over active
Becoming familiar with the body's overall chemistry
Knowing the conditions of the nervous, digestive, elimination, lymphatic and structural systems of the body.
Capabilities:
Inflammation Spotting. Will show where inflammation is present.
Reveals areas in the body where acidity has or can accumulate.
Body Activity Levels. Will show if any part of your body is over active or under active.
Problem Spotting. Will show where problems are occurring in your body.
It is this tissue change that takes place in the patient that makes iridology especially valuable for those specializing in the treatment of chronic diseases.
The Health Status Equation
In order to fully appreciate what the iris reveals, let's first consider this equation:
HEALTH STATUS = PHYSICAL INHERITANCE + ENVIRONMENT (Diet, lifestyle, etc.) + EMOTIONAL/SPIRITUAL FACTORS + AGE.
We all inherit certain combinations of physical traits. We can observe some of these origins from our family tree, but how much this specifically affects you? Diet and lifestyle have a great impact on some people, but why are others able to get away with abusing their bodies? Which mental and emotional aspects significantly affect our physical health? And as we get older, we lose our resiliency at different rates.
What is our individual rate?
Iridology takes a lot of the guesswork out of these questions. Going through life without this information is like taking a trip without a map. What are your chances of arriving at your desired destination? Will you get there efficiently, or end up taking many detours along the way? And how will you know where you are heading next?
Using the road map or blueprint contained in the iris, you can find out how well you are put together (and how much abuse your body can handle), where your body will tend to get sick, (including which organ systems are at greater risk), what specific underlying reasons contribute to your symptoms (which may vary from person to person with the same symptoms), and what emotional or behavioral factors are influencing these patterns. In short, it can show you where you came from, where you are headed, what kind of body you have for a vehicle, and what type of driver you are. With this knowledge, you can more effectively approach health challenges and also identify which preventive medicine practices would be most important for you to pursue.
Iridology is dealing with one of the most basic truths of the healing arts, one that the average form of analysis has not dealt with properly.
The percentage of incorrect diagnosing is nearly as great now as it was back in the 1920s due to the increase in disease symptoms. This increase, together with the combinations of reactions due to X-ray, sulfa and other drugs, and our continued use of refined and synthesized foods, makes it difficult to diagnose accurately. Changes in living habits, pollution and the increased stress of modern times also change the manifestations of the various symptoms of disease. Based upon these facts, it is obvious that symptomology alone is often inadequate in providing the diagnostician with enough information to plan proper treatment for the patient.
Iridology offers a unique perspective to the concept and practice of preventive medicine. It is difficult to alert a person to the health problems that his or her particular body will experience, using orthodox methods of analysis and diagnosis. These methods rely upon the appearance of clinical symptoms. The iris, however, can indicate a problem in its earliest inception, long before disease symptoms are present. With this information, a health program can be developed which is tailored to the specific needs of the client, thus preventing the manifestation of disease.
Grouping a list of symptoms into a disease name, in order to identify and administer the drug that will suppress those symptoms, is not a satisfactory solution to the problem of health care and maintenance. Iridology, in its basic philosophy, stresses the treatment of the patient, not the disease. By identifying the underlying imbalances in the body that produce symptoms, it is an invaluable asset in the formulation of remedial therapies.
When one has come to fully appreciate the value of being able to determine from the outside of the body what is occurring within it, he will realize that iridology is truly a science whose time has come.
Iridology Assessment
A story unfolds in the eye that depicts a detailed picture of the body at work, in health and dis-ease. The eyes are an extension of the brain. They are the input for the brain. Through changes in the pigments and structure of the iris, abnormal conditions of the tissue in the body are revealed.
Iridology is the most effective assessment technique in the world that considers the person as a whole. Humankind must be studied as a whole since the whole is more than the sum of its parts. The most efficient response in raising the health level comes from implementing both nutrition and iris analysis. In addition to nutrition therapy, various natural therapies can be incorporated into each individual's plan of treatment.
Why Iridology Assessment? Management of your health is ultimately up to you. The wisest way to safeguard your health is to know and understand your body thoroughly. When you take care of your body, your reward is wellness. You feel and look younger. You experience more energy and enthusiasm. Iridology assessment provides you with information about your body signals and how you can respond to them. Certain conditions can be spotted before they cause serious problems, allowing you to "nip it in the bud."
If you are suffering from any of the symptoms below, iridology assessment is a highly effective tool to help you determine the cause(s):
Catarrh
Constipation
Migraine
Insomnia
Skin Eruption
Infections
Arthritis
Depression
Low Energy
Discharges
Asthma
Allergies
Colic, Diarrhea
Fevers, Cold, Flu
Chronic Fatigue
Hay Fever
The greatest feature and main advantage of Constitutional Iridology over forms of health screening is that the iris reveals potentials and tendencies that may occur if a person lives their live a certain way. Therefore, symptoms can be treated decades before they ever appear. Preventative action may be taken to improve health and avoid those diseases that might otherwise follow.
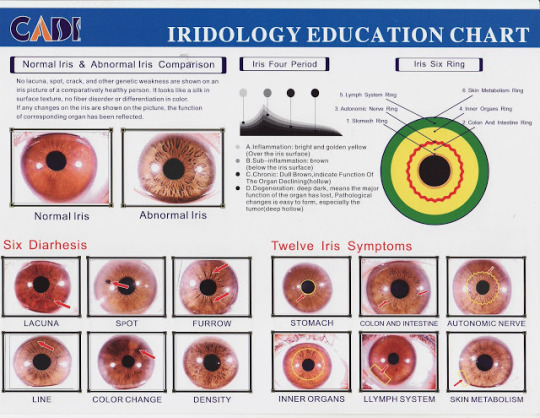
2)iridology chart meaning
IRIDOLOGY & SCLEROLOGY
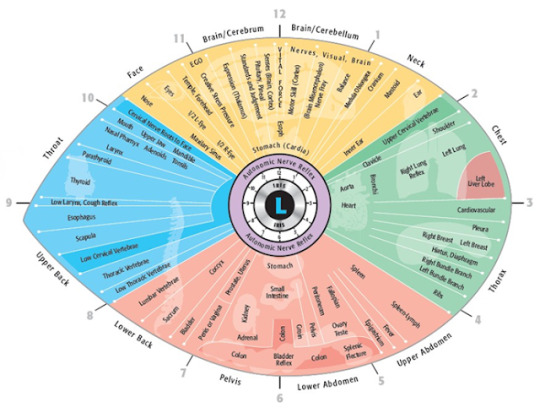
Each eye reveals different information. The left iris correlates to the organs, glands, tissues & other structures located on the left side of the body. The left side also controls the feminine, creative, conceptual & intuitive aspects of our personalities.
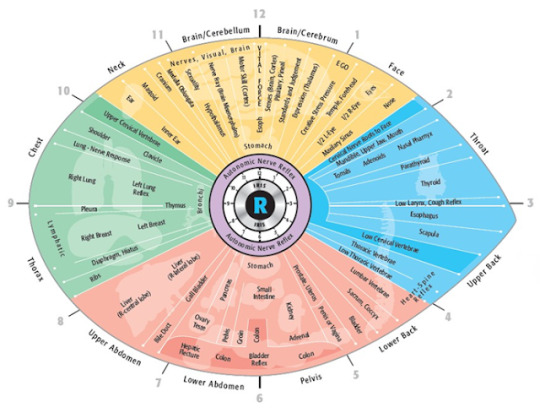
The right iris correlates to all of the anatomical structures on the right side of the body, as well as indicating the masculine, practical, analytical & logic aspects of our being.
More than just detecting the condition of present physical health & the exact location & stage of conditions, Iridology will accurately reveal potential problems twenty years or more in advance, as well as physical transitions due to toxicity, weakness or deficiency & past injuries or conditions. Emotional & mental patterns & attitudes & hereditary strengths & weaknesses also appear.
Cholesterol ring:
This sign presents as white halo around the perimeter of the iris. It may indicate a family history of heart disease.
Go for a cholesterol check.
Orange tones:
A deep orange colour surrounding the pupil can be a sign of disordered sugar metabolism.
If the eye turns a deep red & you have throbbing pain at the front, this could be iritis or — inflammation of the iris, the colored part of the eye. This is triggered by an over-reaction of the immune system, though its exact cause isn’t known. The redness tends to start at the centre of the eye & spreads in a red ring around the center within 24 to 48 hours. It doesn’t usually spread to the other eye.
A coppery-colored ring round the eye can be a sign of Wilson’s disease, a rare genetic disorder which causes too much copper to build up in the body. Untreated it can cause damage to the liver & brain.
Pupil reflex:
If a pupil does not contract when a bright light shines on to it, this indicates dulled nerve reflexes, weak adrenal glands or an overstimulated sympathetic nervous system, often from fear as a hidden, chronic condition.
Adrenal stress is indicated if the pupils begin to expand & contract repeatedly when exposed to bright light for 30 seconds.
Nerve wreath:
A strong, white & almost circular outline of the intestinal area - the nerve wreath - indicates a good condition of the autonomic nervous system.
If this outline is weak, jagged, discolored, or extends far towards the periphery or the pupil, we may assume the autonomic nervous system is in a poor condition.
The normal position of the nerve wreath is one-third the distance between the pupil & the periphery; if the nervous system is tense & overactive, the wreath is closer to the pupil & if the nervous system is relaxed & under-active it is closer to the periphery.
Nerve rings:
White circles or arcs of circles in the outer part of the iris. They indicate a tense, over-reactive, irritated nervous system.
The outermost iris zones represent the lymphatic & circulation system & bordering the sclera, the skin.
Discolored stomach area:
In a normal condition the stomach area is not visible, but if the stomach is irritated the area bordering the pupil will be whitish & distinct from the intestinal area.
A brownish discoloration of the stomach area indicates a chronic weakness.
Discolored intestinal area:
A whitish intestinal area indicates inflammation, irritation or ulcers.
If there is a mucous congestion in the head, there is a whitish or brownish discoloration in the transverse colon area, radiating towards ear & brain.
If chronically weak, this area will be dark.
Radial black lines:
When there is a serious deterioration of the intestines, strong black lines (radii solaris) will develop, starting from the pupil & radiating towards the periphery.
Organs through which these radii pass will be very weak as well.
Unusual markings:
Distinct markings may be colored brown, red or yellow. Unusual colors indicate deposits of drugs or other chemicals that settle in weak organs.
White outer ring:
A heavy white ring near the outer edge of the iris points to salt (sodium) & calcium deposits.
Bluish-white film:
A bluish-white film beginning to cover the iris from the outer rim indicates poor circulation to this area & an anemic condition.
Often this film appears in the brain area, indicating approaching senility (arcus senilis).
Dark outer ring:
A dark ring at the outer rim (scurf rim) shows the skin is inactive with accumulated wastes & needs frequent stimulation, better circulation & improved kidney & lung activities.
Lymphatic rosary:
A series of white spots near the outer rim, the 'lymphatic rosary', indicates chronic infection & congestion of the lymphatic system. Avoid especially lactose & cows milk products (except butter).
SCLEROLOGY
Sclerology is defined as the interpretation of the red lines in the whites of the eyes and their meaning for health evaluation & analysis.
The various signs, markings, shapes & colors in the sclera allow to evaluate the current state of health as well as inherited tendencies & the sings can show way before the symptoms arise or before blood test findings (up to 13 months in advance).
Sclerology may show that the function of an organ is disturbed, but not whether it is overactive or under-active.
Generally a blood vessel pointing towards a certain organ reflex in the iris indicates that there is something wrong with that organ or part of the body.
The stronger the blood vessel is visible & also the more of them are bunching together, the worse is the problem.
A bluish color of the sclera indicates under-activity.
Compare the lines to a Sclerology chart. Determine what parts of the body need attention based on the information from the chart.
The sclera can turn yellow when the body has high levels of bilirubin in it. This can be caused by blood diseases or by liver diseases.See a doctor right away, as jaundice can be a sign of several serious health problems, including liver dysfunction, hepatitis & in rare cases, pancreatic cancer.
When the sclera turns blue, it can be a sign of a syndrome called osteogenesis imperfecta, a disease that makes the bones very brittle.
Light blue sclera can be sign of lack of calcium.
Viruses or localised infections can cause the eye to redden — the problem usually starts in one eye, but can spread to both.
If they look grayish: It’s probably just a result of the natural aging process, which can make the whites of the eyes become grayer. Also there are some serious medical conditions that can turn the whites gray, including rheumatoid arthritis & brittle bone syndrome.
If one eye suddenly becomes red without any other symptoms, then it could be a subconjunctival hemorrhage — where blood leaks in the thin layer of skin at the front of the eyeball. This is very common, particularly in older people. It can be brought on by a violent coughing fit, vomiting, or if you are prone to nose bleeds or bruising. It should clear up by itself within a couple of weeks.
If they look red: Most likely, your eyes are dry. Those red squiggles you see are tiny blood vessels, which become more prominent when eyes are irritated. It can be a result of age, staring at the computer, or environmental factors, like air-conditioning.
Toxic liver.
Persistent red blotches on the whites of both eyes can be a sign of hypertension. High pressure causes the blood vessels to expand or even burst, leaving red marks across the white of the eye (but not the colored part).
Red veins on the eye whites may be sign of high blood pressure.
White discharge from the corner of the eye-could be digestive problems.
Small yellow dots,look like bits of dough,around & on the eyelids can be sign of high cholesterol or liver cirrhosis.
Red upper eyelids-gastritis.
Blind spot accompanied with flickering lights or wavy lines-Ocular migraine (may lead to loss of vision)
Bloody eye,sclera has red spots -high blood pressure, clotting disorder
Brown spots, a bump with blood vessels, often on the lower eyelid -tumor (abnormal growth which may be cancerous)
Bug eyes,bulging eyes with swollen eye tissue -It's a common sign of Grave's disease, a.k.a. overactive thyroid. In addition to the bug-eyed look, people with Grave's often experience weight loss, nervousness & a rapid or irregular pulse.
Bumpy yellowish patches,small yellow spots on the eyelid -high cholesterol
Burning eyes,stinging in the eyes with blurred vision during computer use-computer vision syndrome
Cloudy eyes,clouding of the lens with hazy vision-cataracts (may cause blindness)-the condition, which can be corrected with surgery, is most common in older people. Cataracts that arise in younger people can have a variety of causes, including tumors & diabetes, as well as side effects from certain medications.
Color confusion,reds & greens are unclear -color blindness
Crossed eyes,one or both eyes turn inwards -intra ocular tumor, neurological disorder
Double vision,seeing double images-stroke (sudden), Multiple Sclerosis
Droopy eyes,eyelids are droopy -brain tumor, neuromuscular disorder
Dry eyes,especially in 40+ women with autoimmune conditions & affecting the mouth such that absence of saliva makes chewing & swallowing difficult -Sjogren’s syndrome (immune cells damage tears & saliva producing glands).The menopause.
Golden brown or greenish yellow ring,colored ring on the cornea, surrounding the iris-Wilson’s disease (excess copper collects in tissues, may lead to liver disease)
Grey or milky-white colored ring on the cornea, surrounding the iris-which doctors call arcus senilis, often goes hand in hand with high cholesterol & triglycerides & an increased risk for heart attack & stroke. Anyone who has the condition should have a blood test to check for elevated blood lipids - especially people under age 60.
Increased eye-gunk,eyelid edges are red & itchy-dandruff, Acne rosacea
Large eye,one eye appears larger (generally in children)-glaucoma (damaged optic nerve), tumor, infection
Persistent stye,reddish lumps on the eyelid, present for more than 3 months-tumor, possibly cancerous
Pink eye,sclera is pink or light-red -conjunctivitis
Pupil size different,different size pupils & droopy eyelids -Horner’s syndrome (nervous system disorder), neck aneurysms (blood-filled bulge in blood vessel) & tumors.
Red, itchy eyes,along with sneezing, coughing, sinus congestion or runny nose -allergic reaction
Unable to close eyes or control tears ,often one side of the face is weak & droops-Bell’s palsy (facial paralysis due to dysfunctional cranial nerve VII)
Vanishing eyebrows,outer part of eyebrows disappear -thyroid disease (under active thyroid)
Yellow eyes,sclera is yellow -liver diseases such as jaundice, hepatitis & cirrhosis
Skin cancer-Basal cell carcinomas can show up in some pretty strange places, including the eyelid, where it often causes a sore that doesn't heal & the loss of eyelashes. And it's not something to be ignored. Although basal cell skin cancers are not usually fatal, they can cause severe disfigurement, blindness even death if they reach the brain through the eye socket.
3)Iridology Chart of the Right Eye Iris
Iridology Chart of the Right Eye Iris
Iridology chart on this page shows the right eye iris zones as they relate to specific tissues & organs in the body from Dr. Jenson's Iridology charting studies
The Iridology Chart below documents the right eye Iris zones related to tissues and organs in the body from Dr. Bernard Jenson's charting of Iridology zones. Our Iridologist who studied under Dr. Jensen utilizes the iridology charts to identify possible weaknesses in tissues and organs of the body.
Right Iris
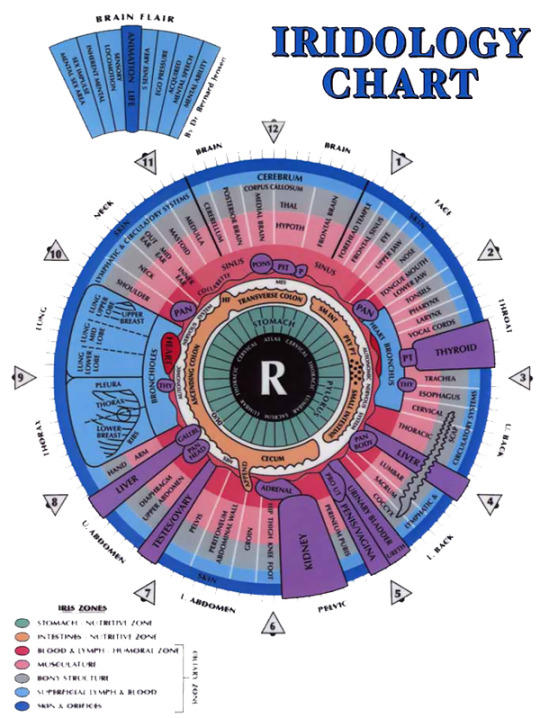
Iridology Chart of the Right Eye Iris
4)Iridology Definition
Iridology, also called iris analysis or iris diagnosis, is the study of the iris (the colored part of the eye). Iris "readings" are made by iridologists to assess a person's health picture (physical, emotional, mental, and spiritual) and guide them to take measures to improve their health.
Origins
The basic concept of iridology has existed for centuries. The medical school of the University of Salerno in Italy offered training in iris diagnosis. A book published by Philippus Meyers in 1670, called Chiromatica medica, noted that signs in the iris indicate diseases. Dr. Ignatz von Peczely, however, is generally considered the father of iridology, with the date of his discovery given as 1861. Von Peczely was a Hungarian physician. As a child, he accidentally broke an owl's leg. He observed that a black line formed in the owl's lower iris at the time of the injury. After the owl's leg healed, the young von Peczely noted that the black streak had changed appearance. As a physician, he treated a patient with a broken leg in whose eye he observed a black streak in the same location as on the injured owl's iris. Von Peczely became intrigued by the possibility of a connection between diseases and eye markings. Through observing his patients' eyes, he became convinced of this connection and developed a chart that mapped iris-body correlations. After several decades of comparative study, von Peczely mapped organs across zones identified by hours and minutes on a clock face superimposed over drawings of the eyes. In 1881, he published his theories in a book called Discoveries in the Field of Natural Science and Medicine: Instruction in the Study of Diagnosis from the Eye.
A Swedish pastor and homeopath named Nils Liljequist also developed the concept of iris-body correlations at roughly the same time but independently of von Peczely's work. He was the first iridologist to identify the effects of such drugs as iodine and quinine on the iris. Liljequist based his initial observations on changes in his own irises after illnesses and injuries, publishing writings and eye drawings during the late nineteenth century. One of his students, Dr. Henry Lahn, brought the practice of iridology to the United States. A variety of practitioners, primarily European, have sought to popularize iridology since these early works. Dr. Bernard Jensen, a chiropractor, is the best-known contemporary American advocate of iridology.
Benefits
Iridologists claim that by studying the patterns of a person's iris, they can provide helpful and accurate health and wellness information. Iridology is a holistic endeavor in that it addresses the person's whole being in the reading. The range of information gleaned encompasses physical, emotional, mental, and spiritual aspects of the person's health picture. In addition to assessing the person's general level of health, readings can reveal other data, including energy quotients; internal areas of irritation, degeneration, injury, or inflammation; nutritional
and chemical imbalances; accumulation of toxins; life transitions; and subconscious tensions. Iridologists maintain that the eyes reveal information about the person's physical and emotional constitution, such as inherited weaknesses and risks to which the person may be prone. Strengths may also be revealed, including inherited emotional tendencies from which the person derives particular talents. Cleansing and healing can be verified by changes in the iris. By looking for certain signs such as healing lines, iridologists obtain information about previous health problems and injuries and discover what may have gone wrong in the person's past.
An iridology reading reflects the causes of problems, not symptoms. It may, iridologists claim, reveal that organs or systems are overstressed or predisposed to disease before clinical symptoms even develop. By predicting future problems, iridology can be used as a preventive tool. People can use the information from iridology readings to improve their health and make better behavioral choices in the future, thereby heading off problems before they occur.
In North America, iridology is generally considered to be an assessment tool to be used in cooperation with other health specialties. Iridology is not a diagnostic tool (although it is more likely to be considered so by European iridologists) and should not be used to diagnose or name specific diseases. Not only would diagnosis represent an improper application of iridology according to many iridologists, as noted by the International Iridology Research Association (IIRA), it could also be construed in many countries as practicing medicine without a license.
Description
Iridology is generally based on the concept of neural pathways between the body and the iris. Although iridologists may differ on the exact mechanism, most maintain that the iris reflects what is happening throughout the body via nerve conduction from all parts of the body to the eye. The client's health is assessed by the iridologist, who interprets patterns, shapes, rings, colors and pigmentation markings, fibers, structures, and changes in the pupil and iris. Many iridologists also use sclerology (reading the lines in the white part of the eyes) in their health evaluation.
Iridology readings are typically performed by such holistically oriented practitioners as naturopaths, chiropractors, or nutritionists. The reading may be done using a bright light, a magnifying glass, and a notepad. The iridologist may also use various tools to better view the eye, a special camera to take pictures of the iris, and/or a computer.
Iridologists conduct their readings using charts on which each area of the iris is mapped to a specific body system or organ. Iridology charts vary, with at least 20 different ones in existence. Some charts are more widely used than others; however, many iridologists believe that there is more than one correct map and that each practitioner should become familiar with several charts. Some iridologists even develop their own charts. Differences also exist among practitioner techniques; among American, European, and other approaches; and in the interpretation of specific iris signs.
Iridology charts divide the iris into numerous zones corresponding to different parts of the body. Although the specifics may differ on each chart, all share a general pattern. The left eye is mapped to the left side of the body and the right eye to the right side. The top of the eye is mapped to the upper body (e.g., brain, face, neck, chest and heart). The center of the eye is mapped to the stomach and digestive organs, with other organs being represented by concentric circular zones moving outward toward the edge of the iris. The bottom of the eye is mapped to the legs and lower half of body. Paired organs (e.g., the kidneys) are mapped to both irises.
Using a holistic approach that considers each client as an individual with unique health patterns and concerns, behaviors, and experiences, the iridologist will examine the eyes and make a health assessment. Based on the results of that reading, the iridologist generally recommends a wellness program tailored to the individual's physical, emotional, and life situation. This program may incorporate various health improvement, maintenance, and prevention regimes. Recommendations may include vitamins, minerals, herbs, supplements, and/or diet and nutrition , among other suggestions.
Preparation
No special preparations are necessary before an iridology reading.
Precautions
An iridology reading is unlikely to cause any physical harm by itself, as it does not involve direct contact with the eye or applying eye drops of any kind. Critics of iridology, however, argue that iridology can be detrimental to health if a sick person delays treatment for a condition not suggested by the iridology reading; or that it can can cause anguish and unnecessary expense if a reading suggests a problem when there actually is none.
Research & general acceptance
Rita M. Holl, RN, PhD, states that "Within Western medicine, iridology is considered a controversial science at best and medical fraud at worst." Proponents of iridology argue that the practice is time-tested with proven results. Although critics acknowledge that certain symptoms of non-ocular disease do appear in the eyes (e.g., brain injury), there is, they argue, a lack of rigorous scientific testing and no evidence that iridology has any merit. Studies published in the Australian Journal of Optometry, the British Medical Journal, and the Journal of the American Medical Association (JAMA) have found iridologists' assessment of patients with diagnosed serious diseases including kidney and gall bladder disease to be inaccurate. Iridologists counter that the research itself was faulty, citing problems including poor-quality photos; the absence of important additional information including the ability to see/interview the client; and inappropriate expectations of diagnosing specific diseases, a task outside the parameters of iridology. A more recent study conducted to reevaluate JAMA's findings in regard to renal failure was published in the Alternative Health Practitioner. Acknowledging that the "study leaves several questions unanswered," the author reported both similarities and variations in the iridologists' readings and concluded that the iridologist's level of expertise is extremely important as well.
Training & certification
Iridologists receive training from various sources. They may learn their trade through books, tapes, correspondence courses, online classes, or live classes. According to the IIRA, "Iridology operates in a gray area in North America. In general, there are no laws defining or regulating the practice. In Europe, especially in Germany, Iridology is well recognized and routinely used by natural medicine practitioners." Also according to the IIRA, "Because Iridology has no official standards of practice, anyone can call themselves an Iridologist, often with little training or experience. There are also great differences in the Iridology information being taught, especially in North America."
Resources
BOOKS
Jackson, Adam J. Iridology: A Guide to Iris Analysis and Preventive Health Care. Boston: Charles B. Tuttle, 1993.
Jensen, Bernard. Iridology: Science and Practice in Healing Arts, Vol. II. Escondido, CA: B. Jensen, 1982.
Jensen, Bernard. What is Iridology? Escondido, CA: B. Jensen, 1984.
Jensen, Bernard and Donald Bodeen. Visions of Health: Understanding Iridology. Garden City Park, NY: Avery Publishing, 1992.
Worrall, Russell S. "Iridology: Diagnosis or Delusion?" in Science Confronts the Paranormal, ed. Kendrick Frazier. Buffalo, NY: Prometheus Books, 1986.
ORGANIZATIONS

0 notes
Text
Why We Should Call Trump a 'Narcissist'
In a Psychology Today article, Dr Allen Francis, who helped put together the DSM criteria for narcissistic personality disorder, is decrying the popular attribution of narcissism to Donald Trump. I appreciate the spirit in which these comments were offered. But the comments are also somewhat arrogant and myopic.
Two separate claims have allegedly been made. The first is descriptive; it is simply the claim that Trump is not, in fact, a narcissist. The support allegedly given for this claim is that Trump does not meet the DSM criteria for narcissistic personality disorder. The author of the comments also implies that he should know, since he is responsible for those criteria. Let’s put aside the fact that DSM categories are voted for by a committee of clinicians and academics, on the basis of empirical findings. For the sake of argument, let’s take the relevant claim from authority at face value.
The second claim is normative. It divides into both a general and a specific implication. Generally-speaking, the claim is that we should not pathologise bad behaviour. More specifically, the claim is that we should not attribute narcissism to Trump on the basis of his bad behaviour. The reasons given for this normative claim are, roughly, (i) that pathologising bad behaviour might somehow mitigate or excuse such behaviour, and (ii) that calling Trump a narcissist is unfair to narcissists, since narcissists are genuinely mentally ill and many of them are well-intentioned.
Both the descriptive claim and the normative claim are false.
The mentioned hubris emanates mainly from the first, descriptive claim. Narcissisism and narcissistic personality disorder are not the same thing. Narcissism is a personality trait that extends over a healthy range of behaviours, in addition to extending over disordered behaviours (at its extreme). Narcissistic personality disorder (NPD) is the specific diagnostic category of the DSM, which identifies a cluster of symptoms for the purposes of classification and treatment. It is simply authoritarian arrogance to conflate the two (authoritarian arrogance of precisely this kind has helped to nudge the DSM closer and closer to disrepute).
NPD is a diagnostic category that hinges entirely on a cluster of clinically observable symptoms, for the express purpose of clinical treatment. As such, NPD, like all DSM diagnostic categories, emphasises various pragmatic conditions for classification and treatment. In particular, Trump supposedly fails to meet the criteria for diagnosis, because he fails to meet the criterion of experiencing distress and dysfunction. It is claimed that Trump causes distress to others instead, as if the two were mutually exclusive. (This is called the ‘disjunction fallacy’ or, more colloquially, a ‘false dichotomy’. It is particularly aggregious in the case of NPD, whose sufferers are well-known to cause a great deal of suffering, in turn, to the people around them.) However, just as members of the public do not know enough about Trump’s personal life to genuinely diagnose him with NPD, members of the public also do not know enough about Trump’s personal life to judge that he is not experiencing distress and dysfunction, of the sort that would warrant diagnosis and treatment. The point is especially salient in the case of extreme narcissism, since it is in the nature of narcissism to do whatever it takes to hide such distress and dysfunction, especially from the eyes of the public. In fact, this alone would be a fairly good rough definition of extreme narcissism. Extreme narcissists are desperate to enforce and maintain an ideal image of themselves, and to a pathological degree. For this reason, it is often the case that only those close to the narcissist are fully aware of the true extent of his narcissism.
So that’s a non-starter. However, it probably wouldn’t matter even if it wasn’t. A great many psychological and psychiatric professionals and academics have stated publicly that they strongly believe Trump to be an extreme narcissist. Some have voiced the suspicion that he would specifically qualify for a diagnosis of NPD. This is isn’t just because of the point made above; i.e., it isn’t just because they suspect that Trump’s distress and dysfunction are hidden from the public. Rather, it is because distress and dysfunction are not even among the specific diagnostic criteria of NPD (despite the fact that Francis claims to be single-handedly responsible for these criteria). Instead, looking for distress and dysfunction in the patient and her history are peripheral guidelines for diagnosis, which remain much the same for all of the DSM diagnostic categories. Strictly-speaking, to be diagnosed with NPD, one need only have 5 of a total of 9 criteria. On this basis, it would seem that Trump more than qualifies for a diagnosis of NPD.
More important, however, is the fact that while NPD is closely related to narcissism, it is not identical to narcissism. As mentioned, narcissism is a personality trait. Typically, when it is claimed that Trump is a narcissist, the intended claim is that Trump is extreme with respect to this personality trait, and not that Trump could be diagnosed with NPD.
This brings me to the falsity of the second, normative claim. Even though mental illness is not reliably mitigating in the courts, there is a popular idea that it is nevertheless mitigating or excusing in some deeper sense. This popular idea might apply straightforwardly to those mental illnesses that used to be classified as ‘Axis I’ disorders, in the DSM. However, its applicability is not quite so clear when it comes to the personality disorders, or character disturbances (which the DSM used to collect under 'Axis II’). There is ongoing debate, among clinicians and academics, as to whether there is a genuine distinction to be made between personality disorders and the other mental illnesses. However, this debate is primarily concerned with whether there is a difference with respect to diagnosis and treatment, and not with respect to whether there is a difference in aetiology or underlying nature. E.g., if borderline personality disorder turns out to respond to all of the same treatments as type 1 bipolar disorder (it certainly responds to many of them), then it would be argued that the DSM should not distinguish between these diagnostic categories. However, this is motivated by precisely the attitude mentioned above—it is motivated by an exclusive concern with classification for the purposes of treatment, and not from a concern with aetiology or underying nature. The DSM has for a long time—and as a matter of necessity, given our relative lack of knowledge about mental illnesses—been concerned only with symptomatology and treatment.
The broader point is that there is, at least in principle, a difference of aetiology or underlying nature between personality disorders and the other mental illnesses. Personality disorders consist in pervasive dispositions or patterns of behaviour, which are difficult to distinguish from other, more profound aspects of the personality (beliefs, desires, emotions, and so on). They are difficult to distinguish from the rest of the person, both from the point of view of the clinician, *and* from the point of view of the patient herself. When a patient first presents with a personality disorder, it is highly typical for her to have originally sought help for other issues. Someone with a personality disorder typically struggles to recognise the problem with her bad behaviours at the time she is exhibiting them, and she is typically unaware of such problems until they have caused significant problems for her, or she is professionally diagnosed with a personality disorder.
The reason for stressing the distinction between personality disorders and other mental illnesses is that we are more likely to hold somebody responsible for her actions if they are seen as resulting from her personality (or from her beliefs and desires), rather than from a mental illness that is somehow separable from her personality. Indeed, what *is* being responsible for an action in the first place, other than the fact that one’s action was voluntary and deliberate? And what is the voluntariness and deliberateness of an action, other than its having been caused in the right way by one’s beliefs and desires? It is in virtue of the fact that narcissism is a personality trait that extreme narcissists *are* routinely judged to have bad intentions, despite the fact that they are mentally ill in a certain sense (i.e., in virtue of their extremity). Since extreme narcissism is a variety of personality disorder or character disturbance, the attribution of narcissism to Trump is far less likely to be seen as mitigating or excusing, in the suggested way.
Lastly, even *if* there were no distinction in aetiology or underlying nature between personality disorders and other mental illnesses, such that there was no corresponding difference with respect to mitigation, it would still be worth attributing narcissism to Trump (assuming that this attribution is appropriate). In other words, the second, normative claim fails no matter what.
It is uninformative to say that Trump merely 'behaves badly’. In contrast, an attribution of extreme narcissism constitutes an attempt to predict Trump’s specific bad behaviours, and to identify the specific causes of those behaviours. Extreme narcissism is an extreme personality trait, which predicts specific kinds of bad behaviours in specific kinds of circumstances. Thus, if an attribution of extreme narcissism to Trump is appropriate, then it is a helpful thing to do. This attribution would be predictive, and thereby allow us to anticipate and prepare for Trump’s bad behaviours; perhaps to pre-empt and avoid them; and perhaps to minimise the damage when they cannot be pre-empted and avoided. By comparison, a simple attribution of bad behaviour is no help at all; it makes little difference. It is not predictive in any useful sense.
It is not surprising that an engineer of the DSM has overlooked this useful, predictive function of personality constructs (such as extreme narcissism). The medical model has little interest in the constructs of personality, beyond their relationships to classifiable disorders and the well-defined treatments of those disorders. The predictivity of personality traits is an 'on the ground’ sort of predictivity; it is explanatory, interpersonal, and sociopolitical. It helps to inform the victims and the potential victims of bad behaviours, but does not provide any paint-by-numbers way of fixing or changing the personality traits that predict those bad behaviours. By itself, extreme narcissism does not constitute a medical-style diagnosis for the purposes of treatment. In this respect, it is unlike DSM diagnostic categories such as narcissistic personality disorder. However, it is partly in virtue of this fact that it is worth attributing extreme narcissism to Trump.
0 notes
Last Seen Blogs

teeny-tiny-moondrop
A Little Lunacy

coreuneros
Untitled

faustina1120
Bureaucrats` Matter

liamismylight
All I want to do in life is love Liam James Payne.

kacchako-week
Kacchan x Ochako Week