#lupinepublishersllc
Text
Lupine Publishers| Strength Improvement and Interface Characteristic of Dissimilar Metal Joints for TC4 Ti Alloy to Nitinol NiTi alloy

Lupine Publishers| Modern Approaches on Material Science
Abstract
Laser welding of TC4 Ti alloy to NiTi alloy has been applied using pure Cu as an interlayer. Mechanical properties of the joints were evaluated by tensile tests. Based on avoiding the formation of Ti-Ni intermetallics in the joint, three welding processes for Ti alloy-NiTi alloy joint were introduced. The joint was formed while the laser was acted on the Cu interlayer. Experimental results showed that Cu interlayer was helping to decrease the Ti-Ni intermetallics by forming Ti-Cu phases in the weld. The average tensile strength of the joint was 216 MPa.
Keywords: Ti alloy; NiTi alloy; Cu interlayer; Laser welding; Microstructure; Tensile strength
Introduction
TiNi alloy has shape memory and pseudo-elastic properties, excellent corrosion resistance and good biocompatibility, it provides promising solutions to solve the problems in various applications such as aerospace, atomic energy, microelectronics, and medical equipment [1,2]. As we all know, the successful application of any advanced material depends not only on its original properties, but also on its development [3]. People are more and more interested in the combination of TiNi alloy and other materials, especially for the development of devices with different mechanical properties and corrosion resistance. Ti alloy has excellent comprehensive properties, such as high specific strength, high specific modulus, hardness, corrosion resistance and high damage resistance [4,5]. It is widely used in aerospace, marine industry, biomedical engineering, and military industry. The composite materials of TiNi alloy and Ti alloy can not only meet the requirements of heat conduction, conductivity, and corrosion resistance, but also meet the requirements of high strength but light weight [6]. Therefore, it will be widely used in aerospace, instrumentation, electronics, chemical industry, and other fields. Compared with single material property, this material can use the performance and cost advantages of each material to select the best material for each structural component [7]. However, the weldability of dissimilar materials also limits the wide application of these alloys. This leads to the formation of brittle-like intermetallic compounds (IMCs) in the weld zone. For example, Ti2Ni, NiTi, Ni3Ti [8]. The formation of Ti-Ni IMCs in the weld makes the weld brittle, and the mismatch of the thermal expansion coefficient of the two materials, it will lead to the formation of transverse cracks in the weld and the deterioration of mechanical properties [9-11]. In fact, TiNi alloy-Ti alloy joint is one of the most direct and effective methods to increase the use of TiNi alloy, Ti alloy and other lightweight materials in the field of aerospace and engineering manufacturing and to use structural lightweight design to achieve structural optimization, energy saving, environmental protection and safety [12]. Therefore, the effective connection between TiNi alloy and Ti alloy becomes an urgent problem.
At present, the most commonly used method is to insert an intermediate layer to improve the microstructure of the joint, which can improve the mechanical stability between TiNi alloy and Ti alloy and lead to the formation of other phases except for Ti-Ni IMCs [13]. This is because the addition of intermediate layer can reduce the fusion ratio of TiNi alloy and Ti alloy in the joint. This effect reduces the content of Ti and Ni in the weld metal, thus reducing the probability of the formation of Ti-Ni IMCs in the weld metal [14,15]. Elements such as niobium, zirconium, molybdenum, tantalum, and vanadium are recommended interlayers for dissimilar welding of Ti-based alloys, since they do not react with titanium [16]. However, due to the high price and unavailability of these elements, Ag, Cu and Ni are usually used as the interlayer for the welding of these two materials, among which Cu is the most widely used interlayer in the field of dissimilar materials welding [17]. These elements will react with Ti and may form new IMCs, but in a case that the hardness of the new phases are less than that of the primary intermetallic phases formed between base metals elements (Ti-Ni IMCs in here), so it is reasonable to use these metals as the interlayer. Compared with TiNi alloy and Ti alloy, Cu has higher ductility and lower melting point, so it can reduce the influence of thermal stress mismatch caused by solidification of welding pool during welding [18]. In addition, copper is much cheaper than Zr, Ta, Mo, Ni, V and other elements, and is easy to obtain. On the other hand, according to the research of Bricknell et al. [19] on ternary shape memory alloys of Ti-Cu-Ni, nickel atoms can be substituted with copper atoms in lattice structure of NiTi. This substitution leads to the formation of Ti (Ni, Cu) ternary shape alloy at different transition temperatures. Therefore, Cu has a good compatibility with NiTi.
Experimental Procedure
Materials
The base materials used in this experiment were TC4 Ti alloy and TiNi alloy. There are large differences in thermal conductivity and linear expansion coefficient between the two base materials, which would lead to large temperature gradient and thermal stress in the joint during welding process. The base materials were machined into 50 mm×40 mm×1 mm plate, and then cleaned with acetone before welding. 0.3 mm thick Cu sheet (99.99 at. %) were adopted as interlayer and placed on the contact surface of the base material fixed in fixture.
Welding Method
CW laser was used with average power of 1.20 kW, wavelength of 1080 nm and beam spot diameter of 0.1 mm. Schematic diagram of the welding process is shown in (Figure 1). Schematic diagram of the welding process is shown in (Figure 1), where a good fitup between the TC4-Cu-NiTi was required to prevent gaps and ensure adequate heat transfer to form a joint. Laser welding for joint. During welding, laser beams were focused on the centrelines of the Cu interlayer (Figure 1). According to the thickness of the Cu interlayer to adjust welding parameters. At the same time can adjust parameters to change the fusion ratio of the base material. Laser offset for weld of joint was defined as 0 mm. The welding process parameters were: laser beam power of 396W, defocusing distance of +5 mm, welding speed of 650mm/min. Argon gas with the purity of 99.99% was applied as a shielding gas with total flow of 20L/min at top of the joint. Supplementary gas protection device covering the melted zone has been used to minimize the risk of oxidation.
Figure 1: Sketch of hydro-power plant.
Characterization Methods
The cross sections of joints were polished and etched in the reagent with 2ml concentrated HNO3 and 6 ml concentrated HF. The microstructure of joints was studied by optical microscopy (Scope Axio ZEISS), scanning electron microscope SEM (S-3400) with fast energy dispersion spectrum EDS analyzer, and selected area XRD (X’Pert3 Powder) analysis. Vickers microhardness tests for the weld carried out with a 10s load time and a 200g load. Tensile strength of the joints was measured by using universal testing machine (MTS Insight 10 kN) with cross head speed of 2mm/min.
Results and Discussion
Characterization of Joint
According to the previous research results, the microstructure, and mechanical properties of NiTi alloy/Ti alloy joint can be improved by adding appropriate interlayer materials, but the formation of brittle and hard Ti-Ni intermetallic compounds in the weld cannot be avoided. To further improve the mechanical properties of NiTi alloy/Ti alloy joint, the design idea of laser welding of NiTi alloy and Ti alloy assisted by metal transition layer is proposed in this paper. The purpose is to avoid the metallurgical reaction between Ti and Ni and improve the microstructure and mechanical properties of NiTi alloy/Ti alloy joint.
Macro-Characteristics
The optical microscopy image of the cross section of the joint is shown in (Figure 2a). The joint can fall into three parts: the fusion weld formed at the Ti alloy side, unmelted Ti alloy and the diffusion weld formed at the TiNi-Ti alloy interface. The fusion weld did not form Ti-Fe intermetallics due to the presence of unmelted Ti alloy. The average width of fusion weld, unmelted Ti alloy and diffusion weld was 1.8 mm, 0.35 mm and 0.17 mm, respectively. Because the microstructure of the fusion weld is quite different from that of the diffusion weld, the diffusion weld becomes black after corrosion. (Figure 2b) presents the optical image before corrosion of the diffusion weld. It does not present such defects as pores and macro-cracks. The unmelted part of Ti alloy acted as a heat sink absorbing a significant amount of energy from the welding pool and transferring it to the TiNi alloy side [20]. Hence, the filler metal of TiNi-Ti alloy interface had a high temperature during welding although it was not subjected to laser radiation. The temperature was high enough to promote atomic interdiffusion. This meets the temperature requirement for diffusion welding. Moreover, the local heating of the Ti alloy side caused uneven volume expansion and thermal stress was produced, which helped to obtain an intimate contact between the TiNi alloy, Cu-based fillers and Ti alloy surface. The high temperature and the intimate contact at the TiNi-Ti alloy interface provided favourable conditions for atomic (Cu, Zn, Ti, Ni) interdiffusion. Therefore, a diffusion weld was formed originated from atomic (Cu, Zn, Ti, Ni) interdiffusion at the Ti alloy-filler metal and filler metal-TiNi alloy interface. Additionally, the unmelted Ti alloy was beneficial to relieve and accommodate the thermal stress in the joint, which could help to improve the mechanical properties of the joints.
Figure 2: Macroscopic feature of the joint: (a) optical image of the cross section of the joint; (b) optical image before corrosion of the Ti alloy-TiNi alloy interface.
Microstructure Analysis
The optical image of the fusion weld is shown in (Figure 3a), and no defects were observed in it. SEM image of the fusion weld is shown in (Figure 3b). The fusion weld mainly consists of acicular structure. The optical image of the diffusion weld at NiTi-Ti alloy interface is shown in (Figure 3c). It can be observed that, the diffusion weld contained three zones marked as Ⅰ, Ⅱ and Ⅲ sorted by their morphologies and colours. (Figures 3d, 3e and 3f)correspond to the three zones in (Figure 3c), respectively. The compositions of each zone (denoted by letter A-C in (Figure 3)) were studied using SEM-EDS. EDS analysis was applied to these zones to measure the compositions of the reaction products and the results are listed in Table 1. Based on the previous analysis, the microstructure of the diffusion weld was mainly composed of Cu-based fillers. The chemical composition of zone Ⅰ was consistent with the Cu-based fillers. Based on the EDS analyses results and Cu-Zn phase diagram, the main microstructure of zone Ⅰ was defined as β-CuZn phase. When the laser beam was focused near the Ti alloy-filler metal interface, the element diffusion occurs immediately between the base materials and filler metal and causes its component to deviate from the original component. The interdiffusion of Cu, Zn, Ti and Ni elements occurred at diffusion welding interface (Ti alloy-filler metal and filler metal-NiTi alloy). At this moment, the dissolution of Ti and Ni into the filler metal occurred under the high concentration gradient, which formed solid-phase reaction layer, and this reaction layer exists only in the smaller region of the NiTi-Ti alloy interface. As shown in, zone Ⅱ and zone Ⅲ were reaction layers formed by element diffusion. Based on Ti-Cu-Ni phase diagram, the microstructure of zone Ⅱ was defined as TiCu2+NiZn. Based on Cu-Ti-Zn phase diagram, the microstructure of zone Ⅲ was defined as Ti3Cu4+Ti2Zn3. Therefore, the main microstructures of diffusion weld were TiCu2+NiZn, β-CuZn and Ti3Cu4+Ti2Zn3.
Table 1: The chemical composition of each phase in joint C (wt.%).
Figure 3: Microstructures of the joint : (a) optical image of fusion zone; (b) SEM image of fusion zone; (c) optical image of the diffusion weld; (b) SEM image of the zone I in Fig. 3c; (c) SEM image of the zone II in Fig. 3c; (d) SEM image of the zone III in Fig. 3c.
Figure 4: Vickers microhardness measurements at semi-height of joint (zero point situated in the center of joint).
Tensile Tests and Fracture Analysis
The maximum tensile strength of the joint was about 256 MPa (Figure 5a). The joint fractured in Ti alloy side of the diffusion weld during tensile tests (Figures 5b, 5c)shows fracture surface of the joint exhibiting typical brittle characteristics. Moreover, as shown in (Figure 5d), XRD analyses of fracture surface detected Ti3Cu4 and Ti2Zn3 phases. This confirmed the presence of Ti-Cu and Ti-Zn intermetallics at fracture surfaces. It should be noted that there was no Ti-Ni intermetallics in the brazed weld. Reaction layer at Ti alloy side in diffusion weld became the weak zone of the joint, which led to the failure in the tensile test.Based on the above results, the formation of Ti-Ni intermetallic compounds is avoided due to the presence of unmelted Ti alloy in the joint. Only a small amount of Ti-Cu intermetallic compounds is formed in the reaction layer at the NiTi-Ti alloy interface. Due to the rapid heating and cooling speed of laser welding, the holding time at high temperature is short, and it is easy to form a narrow reaction zone at the NiTi-Ti alloy interface. In addition, higher cooling rate inhibited the growth of dendrite structure in the reaction zone. Therefore, it is easy to obtain fine microstructure in the reaction zone, which is conducive to reducing the brittleness of the reaction layer. The results show that the formation of narrow reaction layer and fine metallurgical structure at the interface is one of the main reasons to improve the joint strength.
Figure 5: Tensile test results of joint: (a) Tensile test curve; (b) Fracture location; (c) SEM image of fracture surface; (d) XRD analysis results of fracture surface.
Conclusion
The possibility of welding processes for connect TC4 Ti alloy to NiTi alloy with Cu-base filler metal was studied. The main conclusions are presented below. without filler metal, For joint with a laser beam offset of 1.2 mm for Ti alloy, the unmelted Ti alloy was selected as an barrier to avoid mixing of the NiTi alloy and Ti alloy which eliminated the formation of brittle Ti-Ni intermetallic in the joint . A diffusion weld was formed at the NiTi alloy-Ti alloy interface with the main microstructure of TiCu2+NiZn, β-CuZn and Ti3Cu4+Ti2Zn3. A great amount of atomic diffusion occurs at the NiTi-Ti alloy interface during welding, and the thickness of diffusion weld can reach hundreds of micrometres. The tensile resistance of the joint was determined by diffusion weld. The maximum tensile strength of joint was 256 MPa.
For more Lupine Publishers Open Access Journals Please visit our website:
wt u have given that link add For more Modern Approaches on Material Science articles Please Click Here:https://lupinepublishers.com/material-science-journal/
#lupinepublishers#lupinegroup#lupinepublishersLLC#materialSciences#Modern Approaches on Material Sciences
0 notes
Text
Lupine Publishers | Bioactivity, Biocompatibility and Biomimetic Properties for Dental Materials: Clarifying the Confusion?
Lupine Publishers | Journal of Oral Healthcare
Abstract
Often in the profession of dentistry, a new or novel instrument, material, technique, and/or “system” is introduced which can incur a “state-of-the-art” status without necessarily being subjected to the rigors of clinical testing or longitudinal patient-based studies prior to receiving the stamp of approval or the moniker of “standard of care”. Recently, provocative terminology surrounding the field of dental materials has been publicized through the literature, promoting exciting claims and possible long-term advancements for patient care. In this “new era” of evidence-based restorative dentistry; conservative interdiction, i.e. “informed” removal of diseased tissue with concurrent substitution considering form and function, esthetics, and the interaction of the physical and mechanical properties of the replacement materials with living, dynamic structures found in the human tooth, has been of paramount importance.
Abbrevations: ACP: Amorphous Calcium Phosphates, MTA: Mineral Trioxide Aggregate, PVPA: Poly Vinyl Phosponic Acid, PAA: Polyacrylic Acids
Introduction
The progression or evolution of dentistry has occurred, to a great degree, in concert, with the development of material technology [1]. During the last two decades, the categorization of dental materials, specifically, adhesive systems and composite resins have included the term “nanotechnology” into the lexicon of scientific literature [2]. Nanotechnology involves the science and engineering of functional molecules at the nanoscale (onebillionth of a meter) level [2]. As applied to dentistry, this innovative approach promotes the incorporation or interaction of nanostructured materials together with the complex arrangement of organic/inorganic molecular-level constituents comprising living tooth structure, allowing for a myriad of possible preventive and therapeutic applications [2]. Owing to this progression of material development, the assignments of additional revolutionary dimensions have included the origination of the concepts of biocompatibility or bioactivity into dental science.
As a possible expansion of nanotechnology applied to dental materials: the terms biocompatible, bioactive, bioinduction, and biomimetics can be defined independently; however, have often been characterized synonymously [3]. Biocompatible is simply a term to describe a substance or material that will do no harm to existing living structures, that is non-mutagenic and noncytotoxic. The term “bioactivity” was first described in 1969 by Hench, whereby a “bioactive material is one that elicits a specific biological response at the interface of the material which results in the formation of a bond between the tissues and the material” [4]. Furthermore, the definition was refined and updated to include two categories based upon intent and procedure, originally pertaining, specifically, to bone tissue:
a) Class A: A material that elicits an intracellular and extracellular response (osteoproductive);
b) Class B: Materials eliciting an extracellular response only (osteocontuctive) [5].
Accordingly, a bioactive material can have “the effect on, or eliciting a response from living tissue, organisms, or cells”, thus contributing to the formation of a new substance or creation of a living, compatible system [3]. A bioinductive property is defined as “the capability of a material for inducing a response in a biologic system”[3]. Biomimetics is the “study of formation, structure, or function of biologically produced substances and materials and biological mechanisms and processes for the purpose of synthesizing similar products by artificial mechanisms that mimic natural substances”[3,6]. So, although these terms seem to imply different connotations, what can a dental practitioner conclude, deduce, and/or apply for everyday use? Any substance, arrived from by any process (bioactive, bioinduction, biomimetic) should exhibit attributes of being biocompatible. It appears that both a bioactive and biomimetic substance can include the process of bioinduction and that a biomimetic substance could possibly be produced through bioactive activities.
Bioactive materials and processes are probably the most applicable for endodontics and restorative dentistry based upon current uses: luting cements, pulp capping agents, root repair materials, permanent restorations, hard tissue remineralization (fluoride, calcium, and phosphate ions) and bone regeneration properties, and treatment of dentinal hypersensitivity[1,3,7-13]. In order for these materials to become biocompatibily active or retain characteristics of bioactivity; bactericidal and bacteriostatic (inhibits bacterial growth and biofilm formation) properties for the stimulation of reparative dentin formation and maintenance of pulpal vitality must be achieved and maintained [3]. Examples include fluorides for remineralization, antibacterial resins and cements (Reactimer bond™ Shofu Dental Corp., Kyoto, Japan; ABF™ Kuraray, Kurasiki, Japan), restoratives (Active™ BioACTIVE, PULPDENT Corp., Watertown, MA, USA) releasing fluorides and containing amorphous calcium phosphates [ACP], medicaments (mineral trioxide aggregate [MTA] and bioaggregate; Biodentine™, Septodont, Lancaster, PA, USA; TheraCal™, Bisco Dental Products, Schaumburg, ILL, USA; and Endosequence root repair [RRM]™, Brasseler USA, Savannah, GA), and luting cements (Ceramir Crown & Bridge, Doxa Dental Inc., Chicago, ILL, USA) that induce healing and/or for creation of new tooth structures[1,3,7,8,10-14]. Biomimetic substances include the usage of polyvinylphosponic acid (PVPA) polyacrylic acids (PAA) as calcium phosphate matrix protein analogues for remineralization purposes [7,15].
Conclusion
Although these materials are in their infancy, with long-term efficacy based on improvements of mechanical and physical properties pending, future materials will hopefully create circumstances for increased tooth-like attributes due to properties of adhesion, remineralization, and integration [1,3,7].
For more Lupine Publishers Open Access Journal please click: http://lupinepublishers.us/
For more Journal of Oral Healthcare articles please click here: https://lupinepublishers.com/dental-and-oral-health-journal/index.php
To know more about Open Access Publishers please click on Lupine Publishers
Follow on Linkedin : https://www.linkedin.com/company/lupinepublishers
Follow on Twitter : https://twitter.com/lupine_online
0 notes
Text
Lupine Publishers | Martial Arts as a Mindfulness in Motion: A Neurocognitive View
Lupine Publishers | Clinical Microbiology Reviews

Introduction
Mindfulness programs have given high visibility to bring the impact of the practice through a well-structured protocol that can be replicated over the years offering many clinical benefits as well as a greater understanding of neurophysiological mechanisms from immediate and long-term practice [1-5]. Since then, several protocols have been created to give specificity to the public suffering from mental health problems such as depression and anxiety (MBSR, MBCT), addicts (MBRP), eating disorders (MBEAT), pain and chronic illness (MBPM). With this, Mindfulness has gained great popularity for a healthy population [6].
Thus, many studies have emphasized the structures and neurophysiology that Mindfulness practice promotes [7-9]. Based on these results, new protocols have been studied through body movement. The basis is that the body becomes an excellent anchor for maintaining attention, inasmuch attentional flexibility develops, the attentional process becomes faster and more natural [10]. An important factor in this finding is the main point that Mindfulness neurophysiology integrates different areas at different times of practice [11]. In the case of focused attention practice, attentional neural networks are present until distraction occurs, where more medial networks (default mode network) become more prominent [12,13]. As this distraction comes out, a deeper network (salience network) begins to activate so you can then decide to return to the focused object [14,15].
This neural flow became known as the neurocognitive model [11,14] that develops (neuroplasticity) throughout the training (hours/year of practice) [16].
Therefore, Mindfulness is no longer understood only as a practice of meditation or protocol but becomes a cognitive skill or mental training that develops as these neural networks adjust [17]. Then, body awareness is the starting point in the development of Mindfulness due to sensory experience improves the focus [18]. Thus, studies based on martial arts have been studied using Mindfulness neurophysiology as a major aim [19,20]. Studies using the Tai Chi Chuan [21] and Chi Kung [22] Mindfulness attitude had a great impact on research, showing important neurophysiological changes that corroborated with current findings that posterior areas (parietal cortex) of the cortex play a key role in practitioners’ development [23-25]. Conscious movements have become a practical way of training Mindfulness, while martial arts have been an important way of maintaining these practices, considering the synchronization of movement with the Mindfulness attitudes described above.
Karate studies, for example, have gained prominence as training develops cognitive aspects such as attention, working memory, decision making [17,26,27]. The repetition of the movement seems to be an important way to manage the cognitive skill in this learning process, which is associated with a subtle recognition of the movement [26] with lower activity of the brainpower [28,29] and improved body balance [30]. Moreover, studies have shown improvement in cognitive processing speed in older practitioners [31] which related to neural efficiency [28,32]. More studies are necessary to explore the efficacy of martial arts training in the cognitive aspects, whereas Mindfulness has shown an important factor to link the physical activity into cognitive abilities.
For more Lupine Publishers Open Access Journal please click: http://lupinepublishers.us/
For more Clinical Microbiology Reviews Articles please click here: https://lupinepublishers.com/biotechnology-microbiology/index.php
To know more about Open Access Publishers please click on Lupine Publishers
Follow on Linkedin : https://www.linkedin.com/company/lupinepublishers
Follow on Twitter : https://twitter.com/lupine_online
0 notes
Text
Lupine Publishers | Post-Traumatic Stress Disorder: Symptoms, Screening and Treatment
Lupine Publishers | Microbiology Articles
Abstract
Sometimes, as a result of experiencing or witnessing a distressful/traumatic event, there are changes in the brain leading to an anxiety disorder called as Post Traumatic Stress Disorder (PTSD). In the present article, symptoms of PTSD have been described which may be categorized into four different categories viz. flashbacks, avoiding behaviour, unusual alertness and negative feelings. Person with PTSD has mental problems like depression, phobias and anxiety. Person when feels that distressful event is occurring again or recalls in the memory, there may be increased heart beats, high blood pressure etc. Here, screening for PTSD has also been described. On MRI of brain, patient has difference in the size of hippocampus compared to normal person. There are changes in the levels of certain hormones involved in stress conditions also. Mostly doctors recommend counselling, psychotherapy, medicines or combination of these.
Keywords: Post traumatic stress disorder; Traumatic events; Flashbacks; Depression; Anxiety; Hippocampus
Introduction
If a person experiences or witnesses a traumatic event which is shocking, life threatening, humiliating, distressful and feels helpless, these conditions may happen in situations like crimes, fire, accident, death of a very loved person, sexual or physical abuse in some form, rape, terrorist attack, ragging in the college/ hostel etc. It causes changes in the brain leading to disturbance in thinking and emotional process leading to an anxiety disorder called as posttraumatic stress disorder (PTSD).
As per an estimate, nearly 45 million people worldwide are suffering from PTSD. This number may be even more since many people do not go to a doctor since they do not realize about the seriousness of the situation or due to shame or societal fear. It has also been predicted that women are more prone to PTSD than men since men are generally more able to tolerate [1,2]. Generally, person gets shocked and suffers from stress disorder within short span of the distressful event, however, in some cases, symptoms develop at a later stage. It has been found that with time, person instead of feeling better, he/ she feels worse and becomes more anxious and fearful. In the present article, symptoms of the disease have been discussed. Besides, clinical screening for diagnosis and various treatment therapies and medicines available are discussed including present trend of research for PTSD.
Symptoms of PTSD
Generally, symptoms are visible within three months of a distressful event, sometimes, it takes longer. The symptoms of PTSD may be categorized into following four categories, and one may develop either of these or jointly more than one category.
Flashbacks/Intrusion
i. The person has upsetting memories of the distressful event and generally sees the event in nightmares feeling that the same event is occurring with him/her.
ii. Person always feels as the traumatic (distressful) event will occur with him/her again.
iii. Person feels unusual body reactions like increased heart beats, high blood pressure when he/ she feels that distressful event is occurring again or recalls in the memory.
Avoiding behaviour
i. Person avoids to go the place, or to meet the person(s), which reminds him/ her of that distressful event. ii. Person avoids to discuss the event with anyone.
Unusual alertness
i. Person behaves abnormally, for example, on ringing the telephone, he/ she starts jumping or running towards the telephone.
ii. Person develops the tendency to cause harm to himself/ herself or sometimes even develops suicidal behaviour.
iii. Person remains irritated all the time, unable to sleep properly, not able to concentrate on any work.
Negative feelings
i. Person feels unsafe everywhere.
ii. Person develops persistent negativity and blames to himself/ herself for the distressful event.
iii. Person feels isolated/ detached from everyone.
iv. Person feels reduced interest in life.
v. Person has mental problems like depression, phobias and anxiety.
Although, it is usual to feel anxiety immediately after the traumatic event but normally there is healing with time. If healing did not occur with time and increased with time, then these may be symptoms of PTSD.
American Psychological Association (APA) has also formulated the guidelines for detecting symptoms of PTSD. According to these guidelines, person has been exposed to death or threatened death, serious injury or sexual violence whether directly, through witnessing it, by it happening to a loved one, or during professional duties. Besides, APA has also described more or less the same symptoms as stated above [3,4]. It is advisable that if a person got witnessed or suffered a distressful/ traumatic event and finds the persistent symptoms as stated above for a longer time, he/she must visit expert doctor for checkup.
Physical Symptoms
Besides, person suffering from PTSD may also have following physical symptoms:
a) observed that if behaviour changes persist for a longer time, person has problems at work and in the When person is not able to sleep properly, he/ she may feel much tiredness and other problems like body ache.
b) Sometimes, person gets frequent infections. It is due to weakened immune system.
c) Besides, person may feel chest pain, stomach cramps/ pain, headache, dizziness etc.
It has also been marital relationship. Person starts drinking more alcohol or taking drugs. Under the circumstances, it is advisable to get check up by an expert doctor.
In case of children who suffer sexual abuse, may have following visible symptoms:
a) They generally have low self-confidence.
b) They try to hurt themselves.
c) Mostly appear sad, anxious, feared and prefer to stay in isolation.
d) Sometimes become habitual for alcohol and/or drugs.
e) They mostly behave aggressively.
f) Sometimes, depending upon the age, show unusual sexual behaviour.
g) Sometimes, depending upon the age, feel guilt and think, why he/ she did not resist during the traumatic event; and afterwards have the feeling of taking revenge.
h) Sometimes, children exhibit reflection of the traumatic event in paintings, plays, stories etc. They feel nightmares of traumatic event and get disturbed. Due to fear, they hesitate to go to school or are not able to behave properly with the friends. Sometimes, even are not able to study properly.
If even a few symptoms are visible in a child who has witnessed or suffered any sex abuse or other stressful event, parents without much delay must carry the child to an expert doctor.
Screening for PTSD
Doctors generally give a screening test in order to confirm whether he/ she is suffering from PTSD. If symptoms of PTSD get faded or disappear after a few weeks or a couple of months, it may be acute stress disorder and not PTSD. If person suffers from PTSD, symptoms are much severe and mostly appear after few months of the distressful event. In case of PTSD, patient is likely to recover within a year or so [5-7]. However, in some cases, patient suffers for years with visible symptoms.
It has been observed that some people suffer from PTSD after experiencing or witnessing a traumatic event while others don’t.
There are number of factors which increase the chances of PTSD like:
a. If person does not get social support from the family or friends.
b. If person in the past had some mental problems.
c. If in the past, person experienced sexual abuse.
d. If person’s physical health is weak.
e. If after the tragedy, person got other problems too like firing from the job or loss of some beloved one.
On the other hand, there may be conditions which help in not developing PTSD. These are:
a. If person has emotional support from the friends/ family members.
b. If person is having the quality to face the odd situations boldly.
c. If person has the quality to cope up even under much traumatic conditions.
According to some reports, genetic factors also influence the condition by increasing depression, anxiety etc.
On MRI of brain, it has been found that people with PTSD have difference in the size of hippocampus compared to normal individual since this part of the brain is involved in processing emotions and memories which may affect the flashbacks.
It has also been reported that levels of hormones which are released under adverse conditions/ stress, has also been found to be different in persons with PTSD compared to normal person.
Treatment
Mostly doctors recommend counselling, psychotherapy, medicines or combination of these.
It is recommended that if talks are done repeatedly about the traumatic event and about the fear present in the patient in a safe environment, it may help to control the adverse thoughts. This therapy is called Exposure Therapy. However, in this therapy, there is always a risk that instead of improvement, condition of the patient may be worse.
Besides, person is convinced to think the whole event in a new way. Psychotherapy may help in controlling the stress and fear.
Medicines
No patient must take any medicine without consulting a doctor. If above mentioned treatments, exposure therapy and/or psychotherapy do not work, Doctors normally prescribe selective serotonin reuptake inhibitors (SSRIs) like paroxetine. The SSRIs help in reducing depression, anxiety and sleep problems, symptoms mostly present in PTSD. However, sometimes, antidepressant medicines have adverse effects like patient may think to suicide. Some doctors also prescribe benzodiazepines for anxiety, sleep problems, irritation etc. It is pertinent to mention that generally it must be preferred not to give any medicine (unless there is a severe problem) since these medicines only subsidize visible symptoms and person may become habitual of taking these antidepressants.
Other Therapies
1. Specialist asks the patient to recall the traumatic event after making a specific type side to side eye movement. This therapy helps in reducing the stress level for patients of PTSD and also helps in developing positive emotions, thoughts, behaviour etc. This therapy is called as eye movement desensitization and reprocessing.
2. It has also been suggested that if cortisol hormone therapy is given to the patient just after the distressful event, it may help in reducing the risk of PTSD.
3. Some doctors prefer to prescribe a recreational drug which affects the memories more positively by encouraging a feeling of safety.
All these therapies are not proven therapies and require more research.
Sareen [8] discussed important advances in PTSD considering much increase in the number of patients of PTSD after many highprofile traumatic events like wars in Iraq and Afghanistan, terrorist attacks of September 11 on the World Trade Center. He reviewed the advances in the diagnosis of PTSD, inclusion of its diagnosis in the Diagnostic and Statistical Manual of Mental Disorders, impact of PTSD in the community, risk factors, assessment and treatment.
Bisson et al. [2] emphasized on the need to know about PTSD. According to them, responses to traumatic events vary depending upon the individual and most of the persons do not suffer with any mental disorder after traumatic event. Nearly 3% adults suffer from PTSD at any one time and ranging from 1.9 to 8.8% people suffer lifetime. They also reviewed diagnosis and treatment for the disease. They identified Cochrane and other relevant systematic reviews, meta-analyses and other research papers. They also used evidences from meta-analyses of randomized trials in writing the review research article.
Shalev et al. [9] reviewed the clinical status of PTSD. According to them, more than 70% humans experience a traumatic event at some or other time in their lives, and 31% experience four or even more traumatic events. PTSD is the most common psychopathological condition which has been evidenced after experiencing traumatic events. They discussed symptoms of PTSD, status of diagnosis, neurobiologic characters, treatments available and clinical implications of the knowledge.
Dopfel et al. [4] reported individual variability in behaviour and functional networks and mentioned that differences in vulnerability to PTSD is due to predisposition or trauma exposure, is not clear. They measured pre-trauma brain-wide neural circuit functional connectivity, behavioural and corticosterone responses to trauma exposure, and post trauma anxiety by using the predator scent model of PTSD in rats and a longitudinal design. They showed that pre-existing circuit function can predispose animals to differential fearful responses to threats.
Corbett et al. [3] showed that sphingosine-1-phosphate receptor 3 in the medical prefrontal cortex of rats regulates resilience to chronic social defeat stress. They also showed that sphingosine-1- phosphate receptor 3 mRNA in blood of veterans with PTSD gets reduced when compared with the combat exposed control subjects. They also negatively correlated the expression of sphingosine-1- phosphate receptor 3 mRNA with the severity of the symptoms. On the basis of results, they concluded that sphingosine-1-phosphate receptor 3 is a regulator of stress resilience and sphingolipid receptors are important substrates of relevance to stress related psychiatric disorders.
Holmes et al. [5] showed that synaptic loss and deficits in functional connectivity may be considered as symptoms for major depressive disorder (MDD) and PTSD. They also mentioned that synaptic vesicle glycoprotein 2A can be used to index the number of nerve terminals and that is an indirect estimate of synaptic density. They showed that lower synaptic density is associated with the severity of depression and network alterations. They claimed that their study is the first to show in vivo evidence correlating lower synaptic density with depression severity and network alterations. This study may be helpful in treating depression.
Iribarren et al [6] reviewed the current knowledge of PTSD. They emphasized for the role of allostasis in fundamental research on PTSD. They also argued in support about the future of clinical and translational research in PTSD and supported systematic evaluation of the research evidence in treatment of the disease. They showed a strong correlation of novel sleep EEG coherence markers with diagnosis and severity of PTSD. For this, they collected overnight polysomnography data containing EEG across sleep and wake states of many veterans with PTSD and without PTSD (for control). They calculated brain coherence markers from EEG signals using a novel approach. They showed that EEG based brain coherence markers can be used as an objective means for determining the presence and severity of PTSD [10,11].
Conclusion
Post-traumatic stress disorder (PTSD) is a mental disease which changes the life of the person. After some distressful event, if a person’s behaviour changes and does not revert back within reasonable time, person must consult a specialist doctor and proper treatment must be taken. Although therapy commonly given may not cure completely, patient’s condition may improve. There is requirement of more research on PTSD.
Acknowledgement
Author acknowledges the facilities of the Department of Biotechnology, Ministry of Science and Technology, Government of India, New Delhi (DBT) under the Bioinformatics Sub Centre as well as M.Sc. Biotechnology program used in the present work.
For more Lupine Publishers Open Access Journal please click: http://lupinepublishers.us/
For more Biotechnology & Microbiology Articles please click here: https://lupinepublishers.com/biotechnology-microbiology/index.php
To know more about Open Access Publishers please click on Lupine Publishers
Follow on Linkedin : https://www.linkedin.com/company/lupinepublishers
Follow on Twitter : https://twitter.com/lupine_online
0 notes
Text
Lupine Publishers | The Nutritional Status of the Children with Severe- ECC Comparison with the Nutritional Status of Children without Caries Aged 3-5-Years-Old and with the Caregiver’s Demographics in a Kenyan Hospital
Lupine Publishers | Dentistry Open Access Journals
Abstract
Severe early childhood caries (Severe-ECC) is an aggressive, infectious and preventable form of dental caries that affects very young children. The survey purposed to examine any differences in the severity of poor nutrition in children without decay and those children with dental decay in the age group between thirty-six and sixty months. Sampling was purposeful and 196 children aged between 3 to 5 years for this study. The study was hospital-based where eighty-one children with severe dental decay who had attended the Nyanza Provincial General Hospital (NNPGH). Similarly, one hundred and fifteen children who were caries free were chosen from amongst the children attending the maternal child health clinic at NNPGH over a period of three months. Odds Ratio (OR) and 95% Confidence Interval (CI) were used to estimate the strength of association between Severe ECC and nutritional status. The mean dmft for the children with severe Early Childhood Caries (ECC) was 7.5±19. The prevalence of malnutrition was reported among both groups of children with severe ECC and without decay as 28 (14.3%) underweight, wasting 5(2.5%), and stunting 9(4.6%). The malnutrition in children with, Severe-ECC was observed as 27(14%) underweight; 10(4.9%) of the children were wasted, and 5(2.5%) were stunted. However among the children without caries 26 (13.9%) were underweight while 5 (2.6% were wasted, and 12 (6.1%) were stunted. Both children those with severe ECC and those with decay, however, the children who were likely to be underweight at 1.23 times were those affected with severe ECC at 1.23 times compared to the children without decay. Hence other factors may be playing a role in malnutrition of children aged 3-5year old.
Keywords: Severe-ECC; Nutritional status; Caregivers demographics
Introduction
Early childhood caries (ECC) is defined as the presence of one or more decayed (non-cavitated or cavitated lesions), those missing (due to caries), or filled tooth surfaces in any primary tooth in a child 71 months of age or younger. Severe Early Childhood Caries reported in children below three years of age as smooth surface caries1. One or more cavitated, missing teeth due to caries has been associated with age s 3-5years.The filled smooth surfaces in primary maxillary anterior teeth or a decayed, missing or filled a score ≥ 4 for age 3years, a score of ≥ five is associated with 4years while cavitation, restored tooth and missing due to caries a score of ≥6 is for children in the 5-year-old group. All these scores constitute Severe – ECC [1].
Disadvantaged groups have been found to be vulnerable to ECC in both developed and developing countries and even within a single country disparity by social standing there exist, differences due to diet, fluoride use, and social empowerment. Disparities in social empowerment may persist due to lack of access to dental care and inadequate utilisation of dental care even when available [2]. Untreated caries and associated infections can cause pain, discomfort, reduced intake of foods because eating is painful
[3]. Pain may also because the child refuses the caregiver from maintaining good oral hygiene for the child. There is a paucity of literature on the prevalence of Severe -ECC in Kenya. However, a study conducted in nursery school children in Nairobi on the on dental caries and dietary patterns reported a prevalence of 63.5% among 3-5 years old [4]. A survey conducted in Kiambaa division in Kiambu County, a peri-urban population, reported ECC prevalence in 3 - 5-year-olds of 59.5% [5]. Several studies on nutritional status and dental caries have reported variable results. A retrospective survey on the body mass index was done in the United States of America, and it involved two hundred and ninety-three children aged two to five years with Severe - ECC receiving dental treatment under general anaesthesia. In the study, the weight groups were defined by being assigned the CDC body mass index about on age and gender of the children. Results showed that the distribution of subjects by percentiles and the children who were underweight were 11%; of the study sample. However the children whose weight was normal weight 67%; at risk of overweight 9%; overweight 11%. This study concluded that significantly, more children in the sample were underweight than in the reference population [6]. However comparative research on the nutritional status and dental caries among a large sample of four and five-year-old South African children found no significant association between the prevalence of caries and stunting or wasting. However, a relationship was found between decayed, missing and filled surfaces and wasting [7]. This study, therefore, aimed to compare the nutritional status of children aged 3 – 5 years with Severe-ECC and the nutritional status of those aged 3-5 years without caries.
Severe ECC is also associated with oral Microbiota, and in particular anaerobic bacteria of the species Scardovia Wigggsiae and others have been found in abundance in severe ECC lesions [8]
Materials and Methods
One hundred and ninety-six children aged between 3 to 5 years were recruited for this study. Purposive sampling was done to select Eighty-one children with Severe - ECC was chosen from amongst the patients who had sought dental treatment at the dental clinic at the Nyanza Provincial General Hospital (NNPGH). However, 115 children who were caries free were selected from amongst the children attending the maternal child health clinic at NNPGH over a period of three months. Inclusion criteria were: the child was 3 – 5 years of age, was medically healthy, and the parent or caregiver was willing to consent. A semi-structured questionnaire was administered to the caregiver in a face to face interview, and information was collected on the socio-demographic background of the children. There gathered data included education level, age, gender, and the caregiver’s, occupation, and area of residence of the caregivers. The Intraoral examination was carried using dental mirrors and a Michigan O dental probe under natural light as the child sat on an ordinary chair facing the light. Severe ECC was defined as decayed, missing or filled a score of ≥ 4 (age 3), ≥ 5 (age 4), ≥ 6 (age 5). Before dental caries diagnosis, each tooth was dried using a piece of sterile gauze. WHO 1997 caries diagnosis criteria were used, and dental caries was diagnosed when there was a clinically detectable loss of tooth substance and when such damage had been treated with fillings or extraction [9]. Anthropometric measurements were determined to assess the nutritional status of the children and height of the children were obtained by measuring the child standing when standing erect and barefoot, using a measured with a standard height board to the nearest 0.5cm. Weight for age was measured using a Salter scale to the nearest 0.1kg. Each parameter of height and weight had three measurements taken, and an average of each was then recorded. The Cut-offs +2 standard deviations (SD) were used to identify children at significant risk for either delayed (<-2SD) or excessive (>+2SD) growth. The indicators were weight-for-age (WAZ), height-for-weight (HAZ), weight-forheight (WHZ) based on the World Health Organisation(WHO) 2005 recommended reference standard [10]. The collected data collected were coded, cleaned and analysed using SPSS version 17.0 (SPSS Inc, Chicago Illinois, USA) for Windows and Microsoft Office Excel 2007. Nutritional data was analyzed using Epi-Nutri program of Epi-Info version 3.5.1. Descriptive statistics such as proportions were used to summarize categorical variables while measures of central tendency such as mean, standard deviations and ranges were used to summarise continuous variables. The strength of association was established between categorical values using a Pearson’s Chi-square tests. Odds Ratio (OR) and 95% Confidence Interval (CI) were used to estimate the strength of association between independent variables and the dependent variable. The multivariate analysis was done using binary logistic regression at a statistical significance set at p≤0.05. The relevant research and ethics approving institutions approved the study.
Results
A total of 196 children aged 3-5 years were recruited into the study, eighty-one children with S - ECC (41.3%) and 115(58.7%) without caries. The study group had a mean age of 4.1 + 0.6years, and it ranged from 3- 5 years with a high proportion of the children (62.2%) aged four years. There was a statistically significant difference in age distribution among children with Severe ECC and children without caries (χ2=28.36, d.f=2, p<0.001). The majority of the children with caries were aged four years (84.0%) compared to those without caries (47.0%).Gender distribution was comparable with boys slightly more (51.0%) than girls (49.0%).
Sixty-five children (33.2%) lived in the rural community, and 131(66.8%) lived in the urban area. The differences in the area of residence were significant with a Pearson chi square=13.36, df=1, p≤0.001) for the children with severe ECC and those children without decay. It was noted that sixty-six (81.5%) out of 81 children with Severe ECC lived in an urban setting when compared to children who were caries- free who had 65 (56.5%) out of 115 children who were caries free. Some sixty-eight caregivers had had primary school education of whom 24 (29.6% had severe ECC while 44 (38.3%)) were caries free. However, 103 caregivers had secondary school education of whom 43 (53.1% had severe-ECC and60 (52.2%), while 21 (10.7%) their caregivers had tertiary education and 14 (17.3%) and seven 6.1% were caries free. Also, children whose caregivers had a primary level of education had the highest prevalence of severe-ECC followed by those whose caregivers had secondary education. The differences in the severecares prevalence were significant with a Pearson Chi-square =9.41 d.f 3, p≤0.024 Table 1 & 2.
Table 1: Age and gender distribution of children with Severe - ECC and children without caries.
Table 2: Level of education, demographics for the caregivers, place of residence, level of education, and occupation.
The mean dmft of 7; 5±1.9 d was observed among children with Severe – ECC, and it ranged from 5 to 12 scores. Scores. However, the mean dmft for the males was 7.5±1.8 and for females (7.5±2.0), which was statistically insignificant difference found between the two groups (t=0.15, p=0.88). The mean dmft score for children aged three years was 6.9 ± 2.2, four years was 7.6 ± 1.9, and for five-year-olds was 7.2 ±1.2 and all the dmft ranged from 5-12. The dmft progressively increased with age and peaked at age four years. There were no statistically significant differences found between the age groups (t=1.59, p=0.248). Figure 1.
Figure 1: Distribution of decayed, missing, and filled teeth by age and gender.
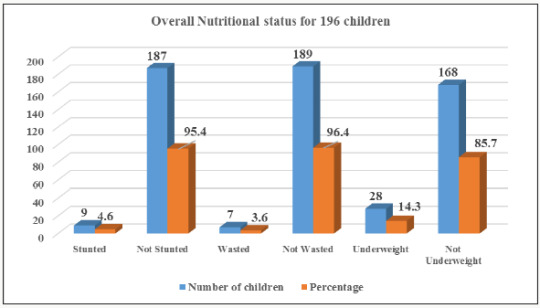
Overall the decayed component of the dmft contributed 92.3%. The missing and filled component of the dmft contributed 7.4% and 0.3% respectively. The overall prevalence of underweight for acute malnutrition, stunting, and wasting for chronic malnutrition was 14.3%, 4.6%, and 3.6% respectively. There were more females 17(17.7%), 4 (4.2%), and 5 (5.2%) who were underweight, wasted and stunted respectively when compared to males, but this difference was not statistically significant Pearson Chi-square respectively for underweight, stunted and wasted were 1.80,df=1, p=0.180 ; 0.19,d. f=1, p=0.660 and 0.16, d.f=1, p=0.686 Figures 2 & 3.
Figure 2: Prevalence of malnutrition for children aged 3-5 n=196.
Figure 3: Nutritional status by gender distribution.
Table 3: Underweight among children with caregivers place residence, level of education, and occupation.
When the caregiver’s residence, level of education, and occupation were considered the children who lived in the rural areas had higher prevalences of were underweight 10(15.4%), when compared to the children in the urban areas 18(13.7%) resided in urban areas. Sixty-eight children had caregivers whose education was of a primary level, and 11(16.2%) of the children were underweight while 57 (83.8%) had normal weight for age. Children whose parents had a secondary education were 103 of whom 14 (13.6% were underweight, and 89 (86,4%) had normal weight for an age while caregivers who had higher education were eighteen of whom 3(14.3%) were underweight, and 15( 85.7%) had normal weight. There were more underweight children 24(15,7) out of 153 when weight for age was examined about the caregivers who were informally employed, However, the differences in the children who were underweight with the caregiver’s various demographics were not significant Table 3.
According to the educational level, the children who were stunted and whose parents had a primary education were four (9.3%)), secondary 6(8.8%), and higher education were 5(7.7%). The caregivers who had formally employed were from the urban area while those who were informally employed and had primary school education were from the rural areas Table 4. There were statistically insignificant differences in the caregiver’s place of residence, the level of education, and occupation among children who stunted and those who were not stunted.
Table 4: Stunting among children about caregivers place of residence, level of education, and occupation.
For the children who were wasted five 7.4% of the caregivers lived in the Urban area and had a primary level of education; also 6(3.9%) of the caregivers had informal employment, and 2(3.1%) resided in rural areas Table 5. There statistically insignificant differences in the caregiver’s place of residence, the level of education, and occupation among children who wasted and those who were not wasted.
Table 5: Wasting among children about caregivers place of residence, level of education, and occupation.
There was a slightly higher prevalence of underweight 14’8% for the children suffering from severe ECC compared with children without decay 13.9%. Although there were differences in the nutritional status of children with severe- ECC and children without caries the differences were insignificant for stunting with p=0.311; also underweight was insignificant with p=0.859 while wasting had p=0.451). A child identified with Severe- ECC at risk 1.08 more times likely to become underweight when compared to a child who did not have decay odds ratio lower and upper limits of 0.48 and 2.4 at 95% CL Table 6.
Table 6: Comparison of the nutritional status of children with Severe ECC and children without caries.
Multivariate analysis was done to determine the relationship between underweight and Severe- ECC among the participating children. Five factors associated with underweight and Severe- ECC at P≤0.05 during bivariate analysis were considered for multivariable analysis upon fitting the factors using binary logistic regression. Adjusting for child’s age in years, child’s oral hygiene status, child feeding on demand, place of residence and caregiver’s level of education, the occurrence of S-ECC was not significantly associated with underweight (AOR=1.23; 95% CI: 0.45 – 3.35; p=0.689). However, a child with S – ECC was 1.23 times more likely to have low weight for an age when compared to a child who was caries – free. However adjusting for other factors, age three years was found to be statistically significantly associated with underweight with an Adjusted Odds Ratio value =2.83; 95% CI: 1.15 – 6.96; p=0.023 Table 7. A child aged three years was 2.83 times more likely to be underweight when compared to one aged four years.
Table 7: Logistic Regression Predicting underweight using caries status, Child’s age in years, Child’s oral hygiene status, Child feeding on demand, Place of residence and Caregivers level of education.
Discussion
In the current study found that children with severe ECC were mainly from urban areas in comparison to children who were caries free. The finding of a high prevalence of severe –ECC in the urban children is similar to other studies in Kenya and elsewhere that have shown that children residing in urban areas have a higher caries experience than their rural counterparts [4,5,11,12]. The mean dmft of children with severe ECC in the present study was 7.5+1.9 which is comparable to a study carried out among preschool children of low socioeconomic status in India which reported a mean dmft of 8.9 [13]. Studies in the USA, and Canada among preschool children found mean dmft scores of 9.6±3.6 and 10.5 respectively [13-15]. The differences in the mean dmft may be due to variations in dietary practices among different populations. Also, decayed component accounted for 92.3% of the dmft, and this finding was similar to a study in South Africa [14]. Untreated tooth decay reflects a low utilisation of oral health services or lack and inaccessibility of preventive and curative dental services to the caregivers, or if the facilities are available, they are too costly.
Higher caries experience was observed in the children from the urban areas when compared to their rural counterparts [11]. The mean dmft of children with severe ECC in the present study was 7.5+1.9. The caries experience for severe-ECC in the present study is comparable to a study carried out in a low social, economic status in India among preschooler and reported a mean dmft of 8.9[112]. Studies in the USA, and Canada among preschool children have reported mean dmft scores of 9.6±3.6 and 10.5 respectively [13,14]. The differences in the dmft could be due to variations in dietary practices among different populations. The decayed component in the current study accounted for 92.3% of the dmft, which similar to other studies elsewhere [14]. Untreated tooth decay reflects a low availability and accessibility of preventive and curative dental services.
In this study, there were more females were underweight, stunted, and wasted when compared to males when referenced on the WHO reference standard. However, the differences were insignificant. The WHO child growth standards reference was used to evaluate nutritional status. The WHO growth reference provides a scientifically reliable yardstick of children’s growth achieved under desirable health and nutritional conditions and establishes the breastfed infant has been used as a reference against whom other alternative feeding practices are measured to and compare to regarding growth, health, and development of in children [9]. The children with severe-ECC who were underweight were 4.9%, stunted 2.5%, and those who were wasted were 14.8%. The presence of underweight, stunting, and wasting may be associated with the inability of the children with severe-ECC to chew the available food and absorb enough nutrients resulting in faltering nutritional status. In comparison a study carried out in Italy among 2- 6 years old found that 11% were e underweight, 11.11% overweight and 22.2% to be at risk of overweight [15]. A study in the USA reporting on the BMI of children with severe ECC noted those who were underweight as 11.%, overweight 11%, and those who were at risk of overweight were nine %6. These findings were insignificant may be due to differences in cultural, dietary practices and the primary determinants of nutritional status among the different populations. In Kenya, the primary determinants of nutritional status among children under five years of age include poverty, hunger, and drought [16]. The low weight for age observed with urban children is similar to previous research from other countries where children with high prevalence with severe-ECC had low weight for age [17].
Children who were malnourished were also noted to have severe ECC compared to children who were caries free. There are high levels of malnutrition in Nyanza as reported in the Kenya Demographic and Health Survey 2008-2009 where 19%, 2%, and 14%of the children under five years were underweight, wasted and stunted respectively [18]. Considering the caregiver’s demographic factors children who had low weight for age, wasting and stunted, resided in rural areas. Also, their caregivers had informal employment and had a primary level of education.The finding may be related to the low socioeconomic status and affect access to health care, food security and hence changing overall nutritional status [16,17].
The differences in the nutritional status of the children with ECC and those without ECC was insignificant. South African children aged between four and five years reported similar findings as what has been observed in this study. Njoroge et al. reported 60% in a study population of 338 children aged five years and below[4]. The most affected dentition were the upper central incisors however the severity of decay increased with age and the first and the second deciduous molars had the highest prevalence ranging between 57% -66%. In this study, the caregivers knew the importance of good oral hygiene and significance of snacks about caries formation. However, the infant feeding habits and the weaning practices were not reported on in this study [19,20].
The South African Study found no relationship between the prevalence stunting or wasting with dental caries. However, they reported an association between Wasting with the decayed, missing and filled tooth surfaces [7]. Children with severe ECC were 1.23 times more likely to be underweight when compared to children without caries. Severe ECC may affect general health and development because a toothache associated with caries may affect food intake and sleep [1]. Poor oral health associated with pain may interfere with the intake, mastication digestion of food and nutrients which may lead to decrease in good nutritional health and reduced quality of life for a child [1].
In summary, the difference in the nutritional status of children with severe ECC and children without caries and stunting was insignificant p=0.311, Underweight p=0.859 and wasting p=0.451. However, children with Severe ECC were 1.23 .times more likely to be underweight than children without caries.
For more Lupine Publishers Open Access Journal please click: http://lupinepublishers.us/
For more Dentistry Open Access Journal articles please click here: https://lupinepublishers.com/dental-and-oral-health-journal/index.php
To know more about Open Access Publishers please click on Lupine Publishers
Follow on Linkedin : https://www.linkedin.com/company/lupinepublishers
Follow on Twitter : https://twitter.com/lupine_online
0 notes
Last Seen Blogs
ubq1973
Uhuru

quagsireunaware
ス ポ ッ ト ラ イ ト!

stinky-dirty-white-boys
Stinky Dirty White Boys

brouwn
Untitled

ladylouuuuuu
I Am Small Potato