#doctor referred me to ob/gyn practically before even seeing me and then asked a bunch abt my porphyria and neurological history
Text
GOT7 AS: Doctors
Just some cute bullet points about what GOT7 would be like as doctors. I know almost nothing about doctors and medicine so take it easy on me with the factual accuracy.
Mark: Emergency Medicine

Mark is the stone-faced doctor who is head of the ER.
Despite the fact that the Emergency ward is always filled with people panicking, with life-or-death cases and horrifying situations, Mark always maintains a straight and calm face through it all. His ability to stay calm and composed and make rational decisions even when patients are bleeding to their death is what makes him the best Emergency medicine doctor.
He is very sweet and calm when not on duty, but his eyes flash with anger whenever one of the junior doctors get flustered while handling a patient.
Panicking at the Emergency room is unforgivable. A cool and rational decision could be the difference between someone’s life and death. Mark Tuan makes sure to drill that into every single doctor and resident that works underneath him.
But sometimes, when he has to declare a person dead and there’s nothing they can do to save them, Mark takes a moment to go into the other room and cry for a little bit. You were a junior doctor and you spotted him kneeling on the floor and crying in the on-call room one day, after a number of patients were brought in dead after a construction accident.
You realized that Dr. Mark Tuan wasn’t emotionless. He just bottled up his emotions until he had a convenient moment to release them. He was afraid that they would interfere with his work if he let them overwhelm him while he was handling the patient.
Some of the other interns and junior doctors were scared of Dr. Tuan, but he was actually quite shy and sweet. He once blushed when you brought him a coffee one morning and thanked you in a soft, shy voice. He brought you a coffee the next day in return.
You had also seen him playing with a small child when her mother was taken into the emergency room. She had been crying but Dr. Tuan let her play with her stethoscope and laughed when the large instrument wouldn’t fit properly into the toddler’s ears.
One of the nurses once told you that there Mark Tuan’s laugh was probably one of the wonders of the world. You couldn’t look at it for too long because it would dazzle you. He was probably the most popular doctor among all the female staff at the hospital because of his handsome looks.
It was really hard to find him if he wasn’t on duty, though. Dr. Tuan seemed to vanish out of thin air whenever he wasn’t on a shift and you had once spotted him practically racing to get home after he’d worked two shifts in a row.
But he worked hard, so you supposed he deserved it.
Jaebum: Neurosurgery

Dr. Im Jaebum is one of the most well-known doctors in the hospital. He’s won awards for his research in neurology and his picture is even put up in the lobby because he’s the most recommended neurosurgeon in the city.
You don’t talk to Im Jaebum before a surgery. When he’s putting his scrubs on and preparing to go into the operation theater, even a tiny unwarranted giggle from an intern will cause him to go ballistic. He once grabbed a junior doctor by the collar after surgery because the man misidentified a surgical instrument and almost handed him the wrong one. Nobody messes with Im Jaebum’s surgery.
Even though Dr. Im pretends to be extremely cold and professional, he lives for those successful surgeries when the families come to him later with tears in their eyes and thank him for saving the patient’s life. No matter how busy he is, Jaebum always takes out time to meet the patient’s family and explain exactly how the surgery is going to go/has gone.
It reminds him why he’s in this profession and it reassures him that he’s doing some good in this world.
Jaebum sometimes takes the junior doctors and interns out for drinks if they’ve worked hard and had a successful surgery. He seems a little gruff but he makes sure to give compliments just as often as he gives scoldings.
You often assisted during Jaebum’s surgeries and you thought he was extremely famous for his steady hands and steady gaze. But you once saw him turn white when he saw a little infant boy lying on the surgery table. Jaebum’s hands trembled for a little bit and he had to step out of the room for a few seconds but he returned looking calm and composed.
He is always a little bit softer with his female colleagues and it sometimes makes the male doctors in the Neurology department angry. But none of them have the guts to say anything to him about it.
Jaebum is also on the hospital’s Board. He attends meetings religiously and makes sure that all the departments are getting enough funds. He has a soft spot for Dr. Choi Youngjae, so somehow the OB-GYN department ends up with the most budget every year.
Jackson: Physical Therapy

Dr. Jackson Wang specializes in physical therapy and chronic pain.
He has a bunch of weird-looking machines and devices in his office including this enormous rubber ball. Nobody knows what all those devices are for. Even Jackson isn’t entirely sure. They’re rarely used because he mostly just recommends Pilates and yoga for common problems.
Always greets his patients with an enormous smile and asks them a bunch of random questions about their lives and day before he starts talking about their pain or what they need treatment for. You were one of his regular patients because you suffered from chronic pain due to a spinal injury some years back and Jackson always remembers his patients. Every single one.
Jackson gets a lot of old people complaining about body pains and he’s always extra sweet and smiley with them. You had once spotted an old lady who admitted to her friend that her pain wasn’t even that bad anymore, but she liked coming down to the hospital for treatment because of the ‘cute, sweet young doctor’.
A lot of his patients are sports-persons. Jackson wanted to play sports professionally once and he’s a complete fanboy, so he makes sure to take all their autographs and frames them so he can hang them up in a small corner of his office. That collection of autographs is his most prized possession.
Insists on his department being painted bright colors. It’s even more colorful than the pediatric wing.
Lives for the days when he gets children as patients. It’s not very often and Jackson is often bothering Dr. Kim Yugyeom of the Pediatric department to refer more children to physical therapy. But the one time Yugyeom did refer a little boy who had been in an accident and had his legs partially paralyzed, Jackson almost cried.
Gets a little bit hurt when people tell him he’s ‘not a real doctor’ but always forces a smile and tries not to get too angry about it.
Once an extremely rude patient called him a ‘massage therapist’ and Jackson smiled before calmly reminding him that he knew exactly which part of the patient’s body to press to make him pass out while screaming in pain.
The patient never came back for another appointment after that.
Jinyoung: Psychiatry

He’s the Departmental head of what most people call the “crazy” ward.
If you use the words crazy, retarded or anything else inappropriate around Dr. Park Jinyoung, be prepared to be kicked out of the hospital. He once fired a nurse from his department for referring to a difficult patient as ‘bat-shit’.
He likes to remind his staff that they never know when they might find themselves on the other side of the glass wall.
It’s a little bit scary because he has an almost psychotic glint in his eyes as he says it.
Dr. Jinyoung is extremely kind and understanding with his patients, and they all love him. But he can’t stand seeing parents and family who are ashamed of being found in the psychiatry ward. Once screamed at a mother who admitted that she was embarrassed of her daughter’s mental illness and wanted to take her home from the hospital.
His office is full of books on psychology. If he’s not dealing with a patient then he can be found reading in his office.
Has a slightly perverse interest in criminal psychology which also scares his staff a little bit sometimes. Jinyoung gets excited whenever he’s called in to evaluate the mental condition of a criminal, or a serial killer or something of the sort but you notice that he always looks miserable and exhausted and sort of... sad, when he returns from the evaluation.
He once admitted to you quietly that he doesn’t have a lot of faith left in humanity.
Keeps sending Dr. Kim Yugyeom reminders to come in for a psychiatric evaluation and once half-seriously diagnosed him with a mental age of 4 and a half. Dr. Yugyeom knows better than to come anywhere near the psychiatry ward.
Youngjae: Obstetrics/Gynecology
There are two beautiful sounds that one hears in the OB/GYN department.
The first is the sound of a newborn baby crying, and the second is the sound of Dr. Choi Youngjae’s laughter. Often, the two sounds can be heard simultaneously and then it’s like music to the ears.
Dr. Choi isn’t entirely sure how or why he ended up becoming an obstetrician, but he helped deliver a neighbor’s fourth child when he was still in medical school and the woman had told him that out of all the deliveries she’d had, he was the best doctor. Also, nothing made Youngjae happier than seeing new life come into this world.
He can sometimes be seen sneaking into the neo-natal unit after his shift is over and cooing at the adorable babies in their tiny little beds. You had caught him doing that once and he had blushed and tried to look professional as he walked away, but he admitted to you later that it made him feel less stressed to just look at the adorable babies.
He mainly specializes in pregnancy and childbirth but he sometimes has to deal with the ordinary gynecology department if no other doctors are available.
Once had to explain to a 13-year old girl what a period was and he got so flustered and embarrassed that he decided to stay away from ordinary gynecology and stick to the obstetrics departments where he could deal with pregnant women who thought he was adorable.
You noticed that he became extremely sad and withdrawn on the days when single mothers admitted to him that they wanted an abortion. Youngjae rarely tried to talk them out of it unless it was dangerous to their health but he told you that it made him sad. He never performs abortion procedures himself.
You once overheard a pregnant woman telling you that she had seen Youngjae’s smiling face after she’d had a c-section and since she hadn’t recovered from the anesthesia, actually thought that she was looking at a real angel.
Bambam: Ophthalmology
Specializes in illnesses and diseases relating to the eye and vision.
Tells every single female patient without exception that she has beautiful eyes in order to see whether she blushes. Sometimes even says it to the men just because.
“On a scale of one to ten, how handsome am I? Seven? Oh dear, you do need some serious treatment. Don’t worry, you’ll be able to see my devastating good looks with perfect clarity once I’m done with you.”
He’s designed his own version of the eye chart that he keeps in his office. They seem like ordinary alphabets but they actually spell out ‘Bambam is a prince’ if you read them all together. Once a Board member came by his department for inspection and forced him to take it down and replace it with the standard chart.
His department doesn’t get a lot of funds even though Bambam brings in huge money by performing lasik and other laser eye refractive surgeries. They’re cosmetic surgeries so they are extremely pricey. He likes knowing that he brings in some of the biggest money to the hospital.
Dr. Bambam can often be found pestering Dr. Im Jaebum in the cafeteria to help him get more funds for his department so that he can buy the latest technology.
Gets a lot of old people as patients, who have cataract issues and the like. Most people have to wear dark glasses after their eye surgery and Bambam only gives out really stylish ones with leopard-print designs on the frame. If you want ordinary ones they you have to spend extra money and go buy them from a pharmacy.
Is extremely chill with his colleagues and buys them all drinks when they don’t have any surgeries scheduled the next day. Once turned up to work completely hungover and wearing dark glasses so he was mistaken for a patient.
Yugyeom: Pediatrics

Dr. Kim Yugyeom is one of the best pediatricians in the city and delivers excellent results, but he can somehow never get the kids to like him. Dr. Jinyoung has a psychological theory that children have a tendency to identify Yugyeom as one of their own, which is why they don’t submit to his authority.
Dr. Jinyoung has since been banned from the pediatric ward.
People think the stuffed bear collection he keeps in his office is for the little kids to play with, but he secretly actually really likes collecting the stuffed bears and had to control his anger when a little boy ripped one of them apart once. He smiled and pretended to be fine but then told the nurse at reception to transfer the kid to a different doctor for his next appointment.
Nobody messes with Yugyeom’s bears.
He’s extremely smiley and friendly with patients and their parents. Dr. Kim Yugyeom is particularly popular with the single mothers because he’s so handsome and he always greets them with big, welcoming smiles. Some of them like to think he’s flirting with them but he just behaves like that with everyone. He tries to be polite about not giving out his personal number after one particularly lonely single mother once tried to sext him on the pretense of asking about her child’s health.
Yugyeom once had to reprimand a nurse for handling a child too roughly, but he couldn’t do it. He ended up calling in Dr, Im Jaebum to help him and the nurse somehow got fired. He still feels bad about it.
Most people think that Yugyeom is extremely innocent and harmless but the truth is, he’s most likely to be found clubbing with Dr. Bambam on weekends. The two of them like to pick up women at clubs by telling them that they’re doctors. It works like a miracle.
#got7#got7 reactions#got7 scenario#got7 scenarios#got7 fluff#got7 doctors#got7 cute#got7 imagines#got7 drabbles#got7 mark#mark tuan#got7 jaebum#im jaebum#jaebeom scenario#got7 jinyoung#park jinyoung#got7 jackson#jackson wang#got7 yugyeom#kim yugyeom#bambam#choi youngjae#got7 youngjae
1K notes
·
View notes
Text
Can Startups Save Primary Care?

By ANDY MYCHKOVSKY
Today, primary care is considered the bee’s knees of value-based care delivery. Instead of being viewed as the punter of the football team, the primary care physician (PCP) has become the quarterback of the patient’s care team, calling plays for both clinical and social services. The entire concept of the accountable care organization (ACO) or patient-centered medical home (PCMH) crumbles without financially- and clinically-aligned PCPs. This sea change has resulted in rapid employment or alignment to health systems, as well as a surge in venture capital being invested into the primary care space.
Before we get too far in the weeds, let’s first begin with the definition of primary care. The American Academy of Family Physicians (AAFP) defines a primary care physician as a specialist typically trained in Family Medicine, Internal Medicine, or Pediatrics. Some women do use their OB/GYN as their PCP, but these specialists are not traditionally considered PCPs. Now if you’ve gone to your local PCP and noticed that your care provider is not wearing a white coat with the “MD” or “DO” credentials, you are either receiving treatment from a hipster physician, nurse practitioner (NP), or physician assistant (PA). Two of the three professionals are trained in family medicine and can provide primary care services under the responsibility of an associated PCP. At least one of the three has a beard.
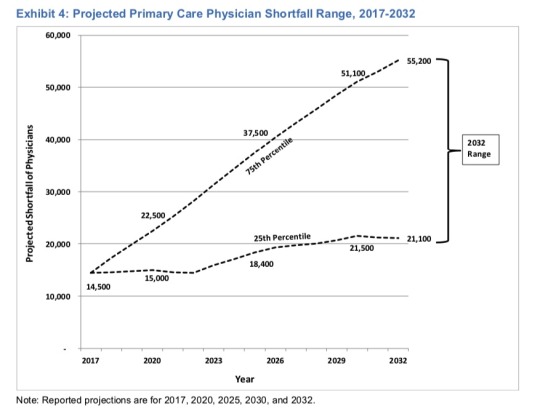
The crazy thing is, despite the industries heightened focus on the importance of PCPs, we’re still expecting a shortage of primary care providers. In April 2019, the Association of American Medical Colleges (AAMC) released a report estimating a shortage of between 21,100 and 55,200 PCPs by 2032. Given we just passed 2020, this not that far off. The primary reason for the shortage is the growing and aging population. Thanks mom and dad. Digging into the numbers will really knock your socks off, with the U.S. Census estimating that individuals over the age of 65 will increase 48% over that same time period. Like a double-edged sword, the issue is not just on the patient demand side though. One-third of all currently active doctors will be older than 65 in the next decade and could begin to retire. Many of these individuals are independent PCPs who have resisted employment by large health systems.
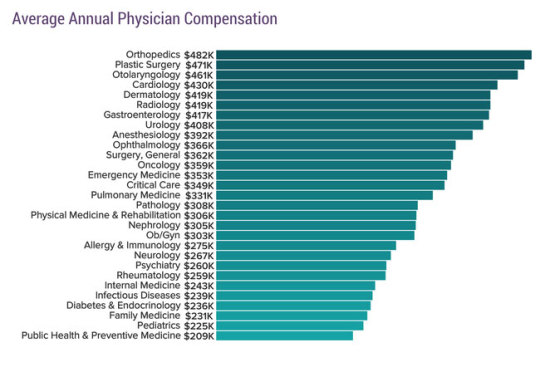
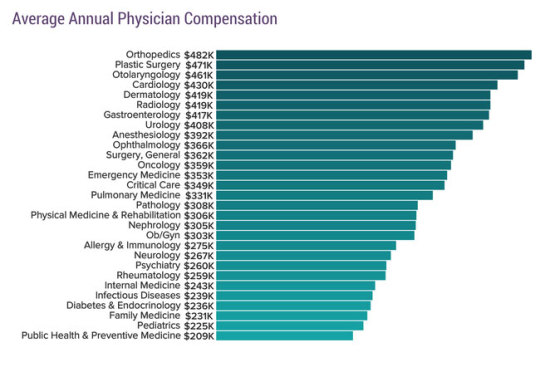
Now the easiest solution would be to wave a magic wand and dramatically increase the supply of medical students selecting primary care versus other specialties. However, in the absence of any Hogwarts-trained healthcare enthusiasts, we have to face the realities of today’s medical school situation. 75% of medical school students in the class of 2018 graduated with student debt, with the average loan debt of $196,520. With that loan balance, you’d owe approximately $2,212 a month on a standard, 10-year federal repayment plan. If you compare that with the earning potential, pediatrics and family medicine are consistently among the lowest paid specialties. According to Medscape, in 2019 PCPs earned an average of $237,000, while specialists earned an average of $341,000. That is a big difference. This all despite the fact that according to a Merritt Hawkins report estimating PCPs generated $2.1 million for their affiliated hospitals in the previous 12 months. This referral value to the hospital even exceeded Otolaryngology ($1.9 million), despite the fact the average annual physician compensation for an Otolaryngologist is $471,000.
The other important characteristic that healthcare economists and researchers have closely monitored is increase in hospital employment and alignment of PCPs versus physicians who own their own independent practices. The fear being that employed PCPs have the potential to refer testing, therapies, and services back to the mothership hospital, as opposed to independent specialists, labs, ambulatory surgical centers, or imaging centers. These hospitals charge considerably higher professional and facility fees, particularly for commercially insured patients. The crazy part of value-based care is that some of the clinically integrated network (CIN) provisions and waivers associated with primary care allow hospitals to align networks of independent PCPs and ensure they receive much higher negotiated rates. Aligning PCP networks to highly motivated and sophisticated health systems who are actively involved in significant downside risk contracts has clear benefits, but the potential for inefficiency and shoring up referral patterns does exist.
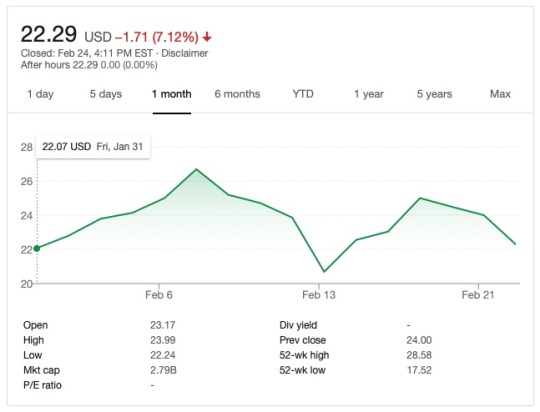
Now back to the world of healthcare startups as they relate to primary care. I’ve said it before and I’ll say it again, the successful One Medical (NASDAQ: ONEM) IPO was the single best thing for primary care startups. Yes, they focus on a particular clientele (commercially insured in urban markets). Yes, they are charging a $199 annual fee for access to their care that many Americans cannot afford. Yes, they will likely grow revenue through higher volume and negotiated reimbursement contracts by partnering with health systems, referred to as health networks. However, 3 weeks after the IPO, the company maintains a market valuation cap of $2.8 billion with nine months of net revenue equaling $199 million and $34 million is losses during the same time period. That is impressive and should be encouraging for current PCP startups.

There are a ton of other primary care focused startups and companies that should not be overshadowed. Each takes on a slightly different approach, whether they focus on a specific population (e.g., Medicare Advantage), actually employ physicians themselves, or serve as administratively- and clinically-aligned vendors for networks of PCPs. I strongly believe in the value of these organizations using technology-driven communication, remote monitoring, home care, and intensive wrap-around care management services for complex populations to offer a new model of care.
If there was ever a downside for creating the primary care-led revolution towards value-based care, I believe it would be the production of charlatans claiming to “primary care consultants” or point-solutions that only affect a sliver of the problem. I see lots of claims related to SAAS startups who utilize an AI-based, machine learning analytics program that spits out a list of high-risk patients. After many years trying to squeeze clinical and financial value out of total-cost-of-care models, that is no longer enough. In my opinion, PCPs should seek partners who can not only provide technology, but also have clinical resources and are willing to stand by their performance in terms of compensation. No guaranteed PMPMs if performance doesn’t add measurable and definitive value, unless the organization is willing to take downside risk exposure. They also need to help your PCP organization understand how to set the rules of the game in your advantage. Otherwise, you will never win regardless of performance (e.g., trend rates, minimum savings thresholds, rebasing, shared savings, etc.).
Now I’m not claiming I know everything, but my experience was borne out of helping health systems and physician groups across the country manage total-cost-of-care contracts in Medicare fee-for-service (FFS), Medicare Advantage, Commercial, and Medicaid managed care while at Evolent Health. For those unaware, Evolent Care Partners is a solution focused on enabling independent PCPs with the capital and resources needed to participate and succeed within two-sided contracts. In addition to Evolent Health, there are a bunch of other primary care startups that I appreciate. They did not pay me (although I should’ve asked before), but here are a few startups that I would research before thinking about primary care in a value-based care world.
One Medical: Provider for Commercial
Iora Health: Provider for Medicare
Oak Street Health: Provider for Medicare
ChenMed: Provider for Medicare
Privia Health: Population health management partner for primary care
VillageMD: Population health management partner for primary care / provider
Aledade: Population health management partner for independent primary care
At the end of the day, primary care still receives a pitiful amount of the total spend in healthcare. The best estimates believe only 5-7% of healthcare spending devoted to primary care. In a RAND Corporation study, researchers predicted 2.12-4.88% of total Medicare fee-for-service medical and prescription drug spending. However, the power of referral, care management, and addressing the social determinants of health (e.g., housing, food, transportation, etc.) holds the promise of a better tomorrow. I am hopeful that the trends over the past few years will continue and new startups will be developed that further innovate on the $260 billion primary care market in the U.S..
Andy Mychkovsky is the creator of Healthcare Pizza, where this article first appeared.
The post Can Startups Save Primary Care? appeared first on The Health Care Blog.
Can Startups Save Primary Care? published first on https://venabeahan.tumblr.com
0 notes
Text
Can Startups Save Primary Care?

By ANDY MYCHKOVSKY
Today, primary care is considered the bee’s knees of value-based care delivery. Instead of being viewed as the punter of the football team, the primary care physician (PCP) has become the quarterback of the patient’s care team, calling plays for both clinical and social services. The entire concept of the accountable care organization (ACO) or patient-centered medical home (PCMH) crumbles without financially- and clinically-aligned PCPs. This sea change has resulted in rapid employment or alignment to health systems, as well as a surge in venture capital being invested into the primary care space.
Before we get too far in the weeds, let’s first begin with the definition of primary care. The American Academy of Family Physicians (AAFP) defines a primary care physician as a specialist typically trained in Family Medicine, Internal Medicine, or Pediatrics. Some women do use their OB/GYN as their PCP, but these specialists are not traditionally considered PCPs. Now if you’ve gone to your local PCP and noticed that your care provider is not wearing a white coat with the “MD” or “DO” credentials, you are either receiving treatment from a hipster physician, nurse practitioner (NP), or physician assistant (PA). Two of the three professionals are trained in family medicine and can provide primary care services under the responsibility of an associated PCP. At least one of the three has a beard.
The crazy thing is, despite the industries heightened focus on the importance of PCPs, we’re still expecting a shortage of primary care providers. In April 2019, the Association of American Medical Colleges (AAMC) released a report estimating a shortage of between 21,100 and 55,200 PCPs by 2032. Given we just passed 2020, this not that far off. The primary reason for the shortage is the growing and aging population. Thanks mom and dad. Digging into the numbers will really knock your socks off, with the U.S. Census estimating that individuals over the age of 65 will increase 48% over that same time period. Like a double-edged sword, the issue is not just on the patient demand side though. One-third of all currently active doctors will be older than 65 in the next decade and could begin to retire. Many of these individuals are independent PCPs who have resisted employment by large health systems.

Now the easiest solution would be to wave a magic wand and dramatically increase the supply of medical students selecting primary care versus other specialties. However, in the absence of any Hogwarts-trained healthcare enthusiasts, we have to face the realities of today’s medical school situation. 75% of medical school students in the class of 2018 graduated with student debt, with the average loan debt of $196,520. With that loan balance, you’d owe approximately $2,212 a month on a standard, 10-year federal repayment plan. If you compare that with the earning potential, pediatrics and family medicine are consistently among the lowest paid specialties. According to Medscape, in 2019 PCPs earned an average of $237,000, while specialists earned an average of $341,000. That is a big difference. This all despite the fact that according to a Merritt Hawkins report estimating PCPs generated $2.1 million for their affiliated hospitals in the previous 12 months. This referral value to the hospital even exceeded Otolaryngology ($1.9 million), despite the fact the average annual physician compensation for an Otolaryngologist is $471,000.
The other important characteristic that healthcare economists and researchers have closely monitored is increase in hospital employment and alignment of PCPs versus physicians who own their own independent practices. The fear being that employed PCPs have the potential to refer testing, therapies, and services back to the mothership hospital, as opposed to independent specialists, labs, ambulatory surgical centers, or imaging centers. These hospitals charge considerably higher professional and facility fees, particularly for commercially insured patients. The crazy part of value-based care is that some of the clinically integrated network (CIN) provisions and waivers associated with primary care allow hospitals to align networks of independent PCPs and ensure they receive much higher negotiated rates. Aligning PCP networks to highly motivated and sophisticated health systems who are actively involved in significant downside risk contracts has clear benefits, but the potential for inefficiency and shoring up referral patterns does exist.
Now back to the world of healthcare startups as they relate to primary care. I’ve said it before and I’ll say it again, the successful One Medical (NASDAQ: ONEM) IPO was the single best thing for primary care startups. Yes, they focus on a particular clientele (commercially insured in urban markets). Yes, they are charging a $199 annual fee for access to their care that many Americans cannot afford. Yes, they will likely grow revenue through higher volume and negotiated reimbursement contracts by partnering with health systems, referred to as health networks. However, 3 weeks after the IPO, the company maintains a market valuation cap of $2.8 billion with nine months of net revenue equaling $199 million and $34 million is losses during the same time period. That is impressive and should be encouraging for current PCP startups.

There are a ton of other primary care focused startups and companies that should not be overshadowed. Each takes on a slightly different approach, whether they focus on a specific population (e.g., Medicare Advantage), actually employ physicians themselves, or serve as administratively- and clinically-aligned vendors for networks of PCPs. I strongly believe in the value of these organizations using technology-driven communication, remote monitoring, home care, and intensive wrap-around care management services for complex populations to offer a new model of care.
If there was ever a downside for creating the primary care-led revolution towards value-based care, I believe it would be the production of charlatans claiming to “primary care consultants” or point-solutions that only affect a sliver of the problem. I see lots of claims related to SAAS startups who utilize an AI-based, machine learning analytics program that spits out a list of high-risk patients. After many years trying to squeeze clinical and financial value out of total-cost-of-care models, that is no longer enough. In my opinion, PCPs should seek partners who can not only provide technology, but also have clinical resources and are willing to stand by their performance in terms of compensation. No guaranteed PMPMs if performance doesn’t add measurable and definitive value, unless the organization is willing to take downside risk exposure. They also need to help your PCP organization understand how to set the rules of the game in your advantage. Otherwise, you will never win regardless of performance (e.g., trend rates, minimum savings thresholds, rebasing, shared savings, etc.).
Now I’m not claiming I know everything, but my experience was borne out of helping health systems and physician groups across the country manage total-cost-of-care contracts in Medicare fee-for-service (FFS), Medicare Advantage, Commercial, and Medicaid managed care while at Evolent Health. For those unaware, Evolent Care Partners is a solution focused on enabling independent PCPs with the capital and resources needed to participate and succeed within two-sided contracts. In addition to Evolent Health, there are a bunch of other primary care startups that I appreciate. They did not pay me (although I should’ve asked before), but here are a few startups that I would research before thinking about primary care in a value-based care world.
One Medical: Provider for Commercial
Iora Health: Provider for Medicare
Oak Street Health: Provider for Medicare
ChenMed: Provider for Medicare
Privia Health: Population health management partner for primary care
VillageMD: Population health management partner for primary care / provider
Aledade: Population health management partner for independent primary care
At the end of the day, primary care still receives a pitiful amount of the total spend in healthcare. The best estimates believe only 5-7% of healthcare spending devoted to primary care. In a RAND Corporation study, researchers predicted 2.12-4.88% of total Medicare fee-for-service medical and prescription drug spending. However, the power of referral, care management, and addressing the social determinants of health (e.g., housing, food, transportation, etc.) holds the promise of a better tomorrow. I am hopeful that the trends over the past few years will continue and new startups will be developed that further innovate on the $260 billion primary care market in the U.S..
Andy Mychkovsky is the creator of Healthcare Pizza, where this article first appeared.
The post Can Startups Save Primary Care? appeared first on The Health Care Blog.
Can Startups Save Primary Care? published first on https://wittooth.tumblr.com/
0 notes
Text
Can Startups Save Primary Care?

By ANDY MYCHKOVSKY
Today, primary care is considered the bee’s knees of value-based care delivery. Instead of being viewed as the punter of the football team, the primary care physician (PCP) has become the quarterback of the patient’s care team, calling plays for both clinical and social services. The entire concept of the accountable care organization (ACO) or patient-centered medical home (PCMH) crumbles without financially- and clinically-aligned PCPs. This sea change has resulted in rapid employment or alignment to health systems, as well as a surge in venture capital being invested into the primary care space.
Before we get too far in the weeds, let’s first begin with the definition of primary care. The American Academy of Family Physicians (AAFP) defines a primary care physician as a specialist typically trained in Family Medicine, Internal Medicine, or Pediatrics. Some women do use their OB/GYN as their PCP, but these specialists are not traditionally considered PCPs. Now if you’ve gone to your local PCP and noticed that your care provider is not wearing a white coat with the “MD” or “DO” credentials, you are either receiving treatment from a hipster physician, nurse practitioner (NP), or physician assistant (PA). Two of the three professionals are trained in family medicine and can provide primary care services under the responsibility of an associated PCP. At least one of the three has a beard.
The crazy thing is, despite the industries heightened focus on the importance of PCPs, we’re still expecting a shortage of primary care providers. In April 2019, the Association of American Medical Colleges (AAMC) released a report estimating a shortage of between 21,100 and 55,200 PCPs by 2032. Given we just passed 2020, this not that far off. The primary reason for the shortage is the growing and aging population. Thanks mom and dad. Digging into the numbers will really knock your socks off, with the U.S. Census estimating that individuals over the age of 65 will increase 48% over that same time period. Like a double-edged sword, the issue is not just on the patient demand side though. One-third of all currently active doctors will be older than 65 in the next decade and could begin to retire. Many of these individuals are independent PCPs who have resisted employment by large health systems.

Now the easiest solution would be to wave a magic wand and dramatically increase the supply of medical students selecting primary care versus other specialties. However, in the absence of any Hogwarts-trained healthcare enthusiasts, we have to face the realities of today’s medical school situation. 75% of medical school students in the class of 2018 graduated with student debt, with the average loan debt of $196,520. With that loan balance, you’d owe approximately $2,212 a month on a standard, 10-year federal repayment plan. If you compare that with the earning potential, pediatrics and family medicine are consistently among the lowest paid specialties. According to Medscape, in 2019 PCPs earned an average of $237,000, while specialists earned an average of $341,000. That is a big difference. This all despite the fact that according to a Merritt Hawkins report estimating PCPs generated $2.1 million for their affiliated hospitals in the previous 12 months. This referral value to the hospital even exceeded Otolaryngology ($1.9 million), despite the fact the average annual physician compensation for an Otolaryngologist is $471,000.

The other important characteristic that healthcare economists and researchers have closely monitored is increase in hospital employment and alignment of PCPs versus physicians who own their own independent practices. The fear being that employed PCPs have the potential to refer testing, therapies, and services back to the mothership hospital, as opposed to independent specialists, labs, ambulatory surgical centers, or imaging centers. These hospitals charge considerably higher professional and facility fees, particularly for commercially insured patients. The crazy part of value-based care is that some of the clinically integrated network (CIN) provisions and waivers associated with primary care allow hospitals to align networks of independent PCPs and ensure they receive much higher negotiated rates. Aligning PCP networks to highly motivated and sophisticated health systems who are actively involved in significant downside risk contracts has clear benefits, but the potential for inefficiency and shoring up referral patterns does exist.
Now back to the world of healthcare startups as they relate to primary care. I’ve said it before and I’ll say it again, the successful One Medical (NASDAQ: ONEM) IPO was the single best thing for primary care startups. Yes, they focus on a particular clientele (commercially insured in urban markets). Yes, they are charging a $199 annual fee for access to their care that many Americans cannot afford. Yes, they will likely grow revenue through higher volume and negotiated reimbursement contracts by partnering with health systems, referred to as health networks. However, 3 weeks after the IPO, the company maintains a market valuation cap of $2.8 billion with nine months of net revenue equaling $199 million and $34 million is losses during the same time period. That is impressive and should be encouraging for current PCP startups.
There are a ton of other primary care focused startups and companies that should not be overshadowed. Each takes on a slightly different approach, whether they focus on a specific population (e.g., Medicare Advantage), actually employ physicians themselves, or serve as administratively- and clinically-aligned vendors for networks of PCPs. I strongly believe in the value of these organizations using technology-driven communication, remote monitoring, home care, and intensive wrap-around care management services for complex populations to offer a new model of care.
If there was ever a downside for creating the primary care-led revolution towards value-based care, I believe it would be the production of charlatans claiming to “primary care consultants” or point-solutions that only affect a sliver of the problem. I see lots of claims related to SAAS startups who utilize an AI-based, machine learning analytics program that spits out a list of high-risk patients. After many years trying to squeeze clinical and financial value out of total-cost-of-care models, that is no longer enough. In my opinion, PCPs should seek partners who can not only provide technology, but also have clinical resources and are willing to stand by their performance in terms of compensation. No guaranteed PMPMs if performance doesn’t add measurable and definitive value, unless the organization is willing to take downside risk exposure. They also need to help your PCP organization understand how to set the rules of the game in your advantage. Otherwise, you will never win regardless of performance (e.g., trend rates, minimum savings thresholds, rebasing, shared savings, etc.).
Now I’m not claiming I know everything, but my experience was borne out of helping health systems and physician groups across the country manage total-cost-of-care contracts in Medicare fee-for-service (FFS), Medicare Advantage, Commercial, and Medicaid managed care while at Evolent Health. For those unaware, Evolent Care Partners is a solution focused on enabling independent PCPs with the capital and resources needed to participate and succeed within two-sided contracts. In addition to Evolent Health, there are a bunch of other primary care startups that I appreciate. They did not pay me (although I should’ve asked before), but here are a few startups that I would research before thinking about primary care in a value-based care world.
One Medical: Provider for Commercial
Iora Health: Provider for Medicare
Oak Street Health: Provider for Medicare
ChenMed: Provider for Medicare
Privia Health: Population health management partner for primary care
VillageMD: Population health management partner for primary care / provider
Aledade: Population health management partner for independent primary care
At the end of the day, primary care still receives a pitiful amount of the total spend in healthcare. The best estimates believe only 5-7% of healthcare spending devoted to primary care. In a RAND Corporation study, researchers predicted 2.12-4.88% of total Medicare fee-for-service medical and prescription drug spending. However, the power of referral, care management, and addressing the social determinants of health (e.g., housing, food, transportation, etc.) holds the promise of a better tomorrow. I am hopeful that the trends over the past few years will continue and new startups will be developed that further innovate on the $260 billion primary care market in the U.S..
Andy Mychkovsky is the creator of Healthcare Pizza, where this article first appeared.
The post Can Startups Save Primary Care? appeared first on The Health Care Blog.
Can Startups Save Primary Care? published first on https://wittooth.tumblr.com/
0 notes
Last Seen Blogs

srednod
DONDERS

chrissy12340-blog
Untitled

artisallimgoodat
👽Tay-Tay👽


johnkatsmc5
return to the underground,the other side of music