Last Seen Blogs





Text
John Hopkins University Gender Clinic 1950-1979 Timeline
1950-1966
Around 1950 - Lawson Wilkins set up a new pediatric endocrinology clinic - doctors recognized that doctors could not tell a person’s sex just by looking at external genitalia, and in some cases recommended to the child and parents that the child’s sex be reversed. [Intersex people, for example.]
Milton Edgerton became Chief of Johns Hopkins first division of plastic surgery in 1951. Shortly afterwards he met his first transsexual: “When I went in to see the patient, who was in every outward appearance female, I began to get the request for the removal of male genitalia, and if possible, the construction of a vagina”. Patients had gone elsewhere and the surgeries oftentimes out of the country and they had been awful
John Money, who wrote his PhD thesis on hermaphrodites (the term then in use), was recruited in 1951 also by Lawson Wilkins to be professor of pediatrics and medical psychology at the newly formed Psychohormonal Research Unit (PRU) in the Pediatric Endocrinology Clinic at Johns Hopkins University. Teamed with Drs Joan and John Hampson he spent six years studying 131 intersex persons, children and adults, who had been treated at Johns Hopkins. They found persons with identical genitals and chromosomes but raised as the other gender fared equally well psychologically. On this basis, Money recommended that an intersex child be steered to a chosen gender, which was usually female as the surgery was easier, but it must be done within the first two and a half years, and that the child must not be confused by being told. Their paper won a prize from the American Psychiatric Association* in 1955. Soon afterwards, the Hampsons left to take up positions at Washington State University.
In 1958, circus performer Hedy Jo Star, after a couple of years on female hormones, presented at Johns Hopkins Hospital. The doctors in the PRU examined her for five days and then sent her home to await a letter. Three months later the letter advised her not to go ahead with surgery as she had no internal female structures. [Only interest in intersex individuals, not transsexuals.]
At about the same time however, the doctors evaluated a female-to-male patient, and in 1960 did a bilateral mastectomy on him.
In 1960 The Joneses left their private practice to become full-time faculty. Howard started doing ‘corrective’ surgery on intersex infants. Money became the director of the PRU in 1962 when Lawson Wilkins retired and died shortly afterwards. Money was awarded considerable grants by the National Institutes of Health*, and was also subsidized by wealthy trans man Reed Erickson (who also subsidized Harry Benjamin and Vern Bullough). John Money attended monthly meetings in New York with Harry Benjamin and Richard Green under the auspices of Reed Erickson’s EEF, [where the idea was raised of applying the kind of surgery being done on intersex patients to transsexuals as well.]
In 1961 Roberta White arrived without an appointment and managed to obtain an interview with John Money who admitted her for three weeks for detailed evaluation.
In 1964, a 17-year-old transsexual referred to as G.L. who had been convicted of stealing women’s clothing and $800 worth of wigs [was ordered by the Supreme Bench of Baltimore City to have sex reassignment surgery at Johns Hopkins.] Her probation officer delivered her to the Johns Hopkins Women’s Clinic where Howard Jones was to do the surgery. However the psychiatry department intervened at the last moment, and had G.L. referred to them for therapy instead.
The next year John Money pioneered the first Gender Identity Clinic in the US. He brought three postoperative patients of Harry Benjamin to meet with Howard Jones and Milton Edgerton. This was the same year that the Joneses with Edmund Novak published their gynecology textbook. That would go through several editions and in its time outsell all other such textbooks combined. Reed Erickson donated $85,000 to the Gender Identity Clinic over years, and became quite friendly with John Money. In addition he went to Johns Hopkins for a double mastectomy repair in 1965 after having had a mastectomy in Mexico and a hysterectomy in New York, and is arguably the first transsexual patient at the Johns Hopkins Gender Identity Clinic.
However the first patient is usually taken to be an African-American referred by Harry Benjamin, Phyllis Avon Wilson who was operated on by Howard Jones at around the same time. Phyllis became a dancer in New York, and on Oct 4, 1966 a gossip column in the New York Daily News carried the item: “Making the rounds of the Manhattan clubs these nights is a stunning girl who admits she was male less than a year ago and that she underwent a sex change operation at, of all places, Johns Hopkins Hospital in Baltimore.”
This caused Dr Edgerton to get a phone call from Dr Russell Nelson, president of Johns Hopkins Hospital, to find out if the story were true. Edgerton made a tactical decision and gave an exclusive to The New York Times, which ran the story on the front page on Nov 21, 1966. A press conference was called on the same day, where Edgerton and several colleagues announced at a press conference the establishment of the Johns Hopkins Gender Identity Clinic under the chairmanship of plastic surgeon John Hoopes. [To an audience of 100 reporters, the doctors defined transsexuals, “physically normal people who are psychologically the opposite sex”, explained that “psychotherapy has not so far solved the problem”, and that they had already operated on 10 patients, all of whom were happy with the outcome. Three were already married, and three more were engaged.]
This was the same year that Harry Benjamin’s The Transsexual Phenomenon had been published. Shortly afterwards, the Universities of Minnesota, Stanford, Northwestern and Washington at Seattle (headed by John Hampson) also opened Gender Identity Clinics.
Within a year, over 700 desperate transsexuals wrote and implored the doctors at the Johns Hopkins Clinic to help them. [However the Clinic would approve for surgery only those whom they unanimously deemed to be ‘good candidates’. They devised four criteria: Is the patient a candidate for psychotherapy? Is the patient authentically motivated? Is the patient psychotic? Will the patient undergo a sociocultural crisis after receiving the operation? This left much room for the doctors’ opinions, and they often chose to err on the side of wait-and-see, recommending therapy rather than progressing a patient on to surgery.]
Dr Hoopes, the chairman, recalled that [Money was often the advocate for progression: “John Money would argue very forcefully that someone was a candidate ... that he knew the patient very well and if this program was going to make any headway this patient should be accepted.”] Not surprisingly, many of the patients did not want to see a psychiatrist. This was based on previous experience with psychiatrists, in that it implied that they had a mental problem, and that they knew within themselves that what they needed was surgery. Most patients soon realized that they should read the medical literature about transsexualism and impersonate ‘textbook transsexuals’ if they wished to be progressed to the next stage.
However the doctors were willing to consider patients with what was described in 1968 as “inadequate social and moral judgment and a long history of petty and sometimes major criminal offenses”. This included transvestites, gay men and strippers, many associated with The Block, a part of downtown Baltimore with many nightclubs, bars and sex workers. The doctors realized that their patients were at risk of arrest for cross-dressing and so issued identity cards with a Johns Hopkins phone number provided by The Erickson Foundation. Dr Edgerton had several calls from police officers, and after an arrest in 1971 helped to get a female transsexual transferred to the women’s facility. Some patients dropped out during the stage where they were taking hormones. In some cases this was because they could not afford the $2,000 to $10,000 for the surgery.
1966-1979
Psychiatrist Ira Pauly had published the first aggregation study of transsexual cases in 1965, “Male Psychosexual Inversion: Transsexualism. A Review of 100 Cases". This resulted in a job offer from Johns Hopkins, but, after a pay rise, Pauly decided to stay at the University of Oregon Medical School.
One-year-old Bruce Reimer was brought to see Dr Money and surgically reassigned to female as Brenda in 1967, and continued annual visits for almost 10 years, until Brenda began to refuse, and started to change back to male as David.
The same year Barbara Dayton moved to Baltimore with wife and children, and started living as female. [The Clinic declined her application based on age, appearance and numerous tattoos. Also Barbara could not afford the fee.]
The most prominent patient in the Gender Identity Clinic was writer Dawn Langley Hall who had surgery in 1968, married an African-American the next year, and publically announced the birth of a daughter in 1971 (a claim that the Gender Identity Clinic said was “definitely impossible”).
In 1968 the Gender Identity Clinic provided surgeon Stanley Biber with diagrams on how to do sex change surgery. Renée Richards met with John Money, but at the end was told that Johns Hopkins was not accepting any more transsexual patients at that time.
In 1969, transsexual pioneer Christine Jorgensen came to Johns Hopkins for corrective surgery. Future showgirl Michelle Brinkle ran away to Baltimore intending to register at the Clinic, but never did, and ended up at Dr Burou’s Clinic in Casablanca instead. Psychiatrist Jon Meyer became chairman of the Gender Identity Clinic, and his predecessor, John Hoopes wrote: “The surgery, often considered outrageously excessive and meddlesome by the uninformed, must be undertaken regardless of the censure and taboos of present society”. Also in 1969, Richard Green and John Money co-edited Transsexualism and Sex Reassignment, with a preface by Reed Erickson, an introduction by Harry Benjamin, and published by Johns Hopkins University Press.
[John Money conducted a follow-up study of ‘17 male and seven female patients’, and found that after surgery nine patients had improved their occupational status and none declined. “Seven male and three female patients married for the first time” and “All of the 17 are unequivocally sure they have done for themselves the right thing”.]
In 1970, Dr Edgerton left for the University of Virginia, where he established a Gender Identity Clinic, and Dr Hoopes returned to Johns Hopkins to replace him as Chief of Plastic Surgery. Dr Meyer started his own study of the benefits of surgery.
[In 1972 future doctor Dana Beyer, then a student, came to the Clinic but found the intake application so off-putting that she fled before seeing a doctor.]
In 1974, 23-year-old future intersex-cum-HSTS activist Denise Tree (Kiira Triea) had surgery with Dr Howard Jones after years of therapy from Dr Money.
[In a paper with John Hoopes, Meyer wrote: “Most of the patients continue to be emotionally and socially much the same as they were in the pre-operative phase”.]
In 1975, Catholic psychiatrist Dr Paul McHugh became head of the Psychiatry department at Johns Hopkins. He later wrote that [he intended from the start to put an end to sex change surgeries which he described as “the most radical therapy ever encouraged by 20th-century psychiatrists— with perhaps the exception of lobotomies.”]
In 1976 Charles Annicello from the clinic testified in a New Jersey court on behalf of M.T., a trans woman who was suing for alimony. Louis Gooren, who would develop the Gender Clinic at the Vrije Universiteit in Amsterdam, studied at Johns Hopkins in 1976, as did Russell Reid who later became a consultant at Charing Cross Hospital.
The Joneses retired from Johns Hopkins in 1978, and became professors of obstetrics and gynecology at Eastern Virginia Medical School, where they established the first in vitro fertilization program in the United States.
[In 1979, (the same year that Janice Raymond published the transphobic The Transsexual Empire) psychiatrist Jon Meyers and co-author Donna Reter reporting to Paul McHugh, finished their evaluation of fifty post and pre-op patients they saw as still deeply disturbed. “To say that this type of surgery cures psychiatric disturbance is incorrect. We now have objective evidence that there is no real difference in the transsexual’s adjustment to life in terms of jobs, educational attainment, marital adjustment and social stability,” he said. He later told The New York Times, “My personal feeling is that surgery is not a proper treatment for a psychiatric disorder, and it’s clear to me that these patients have severe psychological problems that don’t go away following surgery.” He even referred directly to “one case”, probably Reed Erickson, “In which a woman required hospitalization for drug dependency and suicidal intentions after being changed to a man.”
John Hoopes also changed his mind: “Prior to the surgery, these patients were at least male or female, but after the surgery the males converted to females weren’t really females and the females converted to males weren’t really males. . . You’ve created a new breed. You’ve created something you don’t know what to do with. … I never saw a successful patient. For the most part they remained misfits”.
The Meyer study has not been supported by later studies. Its methodology has been strongly criticized, especially the vagueness of some of its scoring, and that it does not include any measure of personal satisfaction. None of the post-operatives regretted the operation (as Meyers and Reter acknowledged). However, citing the study, the hospital administration closed the program.
The Johns Hopkins program was never important in terms of numbers, in fourteen years they provided surgery to only thirty people (compare to Dr Biber who would do many more than that every year), but in that it was the first clinic it was felt as a loss when it closed.
Even so, Johns Hopkins' reputation was such that transsexuals continued to apply to the Hospital. They were seen in the Sexual Behaviors Consultation Unit at $150 a time, but no referrals for surgery were made after 1979.
John Money stayed at the PRU, even after 1986 when it was moved to smaller premises outside the Hospital.]
https://zagria.blogspot.com/search?q=john+hopkins#.WUfySevyvDc
0 notes


Photo

In the studio with @katehush , NYC’s reigning queen of neon
6K notes
·
View notes




Text
This Is NOT What Trans Looks Like.
This is me: Devin-Norelle an androgynous identifying, person of trans- masculine experience. My body, my transition, my passing privilege is desirable among many.
But I AM NOT what trans looks like.
I am not other trans/gnc folks who have no desire for hormones, or surgery.
I am not the person who lacks the opportunity to obtain hormones or will never be capable of embodying certain passing privileges.
I am sometimes not the non-passing gender-fluid person who is harassed on the street because of their ambiguity.
I am not a representation of all trans folx, nor will I ever be.
The trans masculine community & some of it’s visible leaders are sometimes so enthralled by cisgender conforming standards. We tend to celebrate one prosaic representation: masculine bodies, men with visible beards,and folx that pass.
But the trajectory of our individual lives, & our actual lived experiences are indefinite; each of us eclipses these materialistic standards.
My shero @lavernecox said, “We need diverse media representations of trans folks to multiply trans narratives in the media and depict our beautiful diversities.” I’d like to add the inclusion of diversity isn’t limited to just the media. Following in the footsteps of Laverne and Janet, trans-masc leaders can do more to acknowledge the abundance of gender identities & expressions Let’s transition the conversation. Uplift the narratives of those who don’t fit the definition of “normal.” Reject exclusionary dialogue of identities. It is easy to blend in. It takes strength to stand up in solidarity with folx who have no voice or lost their voice in death because they were not deemed acceptable.
Normalize non-conforming beauty standards. Include more representation for the disability community. Bring more attention to femme, trans femme & AMAB folx who are constantly victims of violence. Discuss how trans-masculine folx can elevate trans-fem folx. Hold dialogue about the shortage of hormones, especially of estrogen, & how this is violence.
Lets celebrate our diversity. Let’s celebrate our lives. Let’s celebrate our beauty. Let’s celebrate striving to be our most authentic selves, regardless of the path taken or not taken.

This^ IS what Trans look like. We are trans men. We are trans women. We are gender non-conforming. We are bigender. We are agender. We are of different ethnicities and racial backgrounds. We exists in all shapes in sizes. Our gender presentations may vary, our identities are fluid, our expressions are unique, but we are all beautiful. “Trans people are exactly who they say they are, no matter what the culture or media would lead us to believe.” -@JanetMock
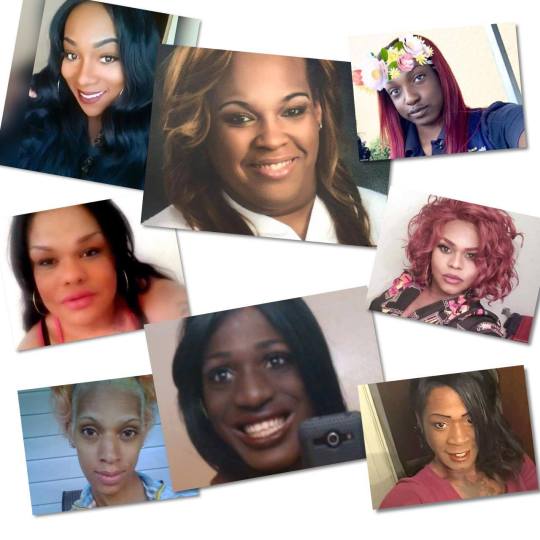
This too is what trans looks likes. Often times, trans is a story of sorrow, loss, pain and suffering. Many Trans women of color (TWOC) have lost their lives at the hands of others simply for living their truth. Their deaths are daily reminders that trans lives are not valued. Trans Women of Color in particular are subjected to such violence because they are black (or POC), are often times living below poverty, do not have access to certain health care that would help them pass, or are victims of transmisogyny (transphobia + sexism).
Several women have been killed because because of the false stereotype that they are gay men attempting to deceive straight men. The alarming rates of their deaths is also evidence that the most marginalized people of society are discriminated against for their existence. 19 Trans people have died this year, including 14 Trans women of color. The women above were killed during the summer of 2016. The deaths of these beautiful people become more difficult to read about each time, but their narratives are part of our truth and must be told.
#SayTheirNames (Above) Rest in Power Rae'Lynn Thomas, Erykah Tijernia, Skyee Mockabee, Dee Whigham, Deeniquia Dodds, Goddess Diamond, Mercedes Successful, Tyreece ‘Reecey’ Walker.
—————————————————————————————
AMAB: Assigned male at birth. (sources linked)
Trans Feminine refers to anyone with a feminine-of-center identity, especially those not assigned female at birth. This includes male-to-female transwomen, feminine-identified genderqueers, and others whose fabulousness cannot be defined. (source linked)
Trans Masculine refers to anyone with a masculine-of-center identity, especially those not assigned male at birth. This includes female-to-male transmen, masculine-identified genderqueers, and others whose fabulousness cannot be defined. (source linked)
Transmisogyny: the negative attitudes, expressed through cultural hate, individual and state violence, and discrimination directed toward trans women and trans and gender non-conforming people on the feminine end of the gender spectrum. (source linked)
6K notes
·
View notes



Photo

experimenting with a new photo style. taking photos from the Hubble Space Telescope and merging with my own land/cityscapes. follow my instagram & blog for more.
instagram
buy my artwork starting at $17 for any print
6K notes
·
View notes
Photo

Henri Cartier-Bresson coined the phrase the decisive moment to describe the instant when the action before the lens is not simply captured by the photographer, but organized in such a way as to give it power and grace, balance and form. Decisive moments are not always the same for the athletes or fans as they are for photographers. Capturing the winning touchdown, the diver’s perfect entry into the water, the power of a skier racing in the giant slalom, can establish an imagine in sports eternity, but is not necessarily decisive moment in the photographic sense. Photographers have a responsibility to satisfy their editors and the public, who often seek only the highlights of the game. However, the finest photographers are able to fulfill this responsibility and seek to make pictures that are greater than a single defining action, pictures with aesthetic qualities that last through time.
Joerg Mitter emphasizes that there is a lot of “calculated risk” in extreme sports. The athletes have to trust the photographers because everyone is together in challenging and dangerous situations. In extreme sports photography, there are no second chances. Mitter considers everything, including the backgrounds, and must preconceptualize the picture. The athletes keep their stunts real, and Mitter would also never photoshop a picture.
Joerg Mitter (Austrian, born 1980). Levi Sherwood of New Zealand performs in front of the St. Basil’s Cathedral in Moscow’s Red Square, Russia, June 24, 2010. Color photograph. Joerg Mitter // Limex Images
1K notes
·
View notes
Photo

‘When you’re dying, your life flashes before your eyes - like a rerun. It runs the risk of being very boring.’
Je me tue à le dire (2016)
Made for Seize the Night Open Air Film Festival.
4K notes
·
View notes
Text
I had sex in a graveyard and was walking around nude cause it was like 80 degrees and I was all sweaty and it was like midnight or whatever.
So this car rolls up out of nowhere and I’m stark fucken naked.
I’m also white as fuck. I glow in the dark.
I make eye contact with the dude driving.
I don’t make a move to cover up or anything because idgaf about being naked.
I see his eyes widen….
With fear.
He fucken books it out of there like a bat out of hell.
And that’s the story about how I became a ghost sighting in a small town in New England.
248K notes
·
View notes