#tras
Text
Someone probably made a poll like this at some point but I'll do it anyway idgaf
#i'm ashamed to admit that i was a tra#the worst thing i did which haunts me to this day is that i told a lesbian that she's transphobic for not wanting to date trans women#because trans women are women DUH#and i genuinely believed that#it didn't cross my mind how homophobic it was#welp#fortunately im normal now#radfem#radical feminism#radfems#radfem safe#radblr#radfems do interact#radfems do touch#feminism#radfem poll#ask radfem#terf#terfs#tras#tra#terf safe#lgb drop the t#poll#tumblr polls#question to radfems#women#female#adult human female#radfems please touch
121 notes
·
View notes
Text
tras are some of the most privileged & coddled individuals i’ve ever come across. They want ‘terfs’ to be blocked & never want to hear anyone’s opinion that’s different from theirs. They all act like they’ve never been told no
I see them on my feed sometimes sending anons & harassing people like ‘um op you just reblogged a terf’ & so what if they did? Literally no one outside of your delusion bubble cares why can’t they understand that 😭
359 notes
·
View notes
Text
Breaking Down Cass Review Myths and Misconceptions: What You Need to Know.
An answer when some tranny or handmaiden disputes the review. (long post with lots of facts!)
Via The Quakometer:
It has now been just little under a week since the publication of the long anticipated NHS independent review of gender identity services for children and young people, the Cass Review.
The review recommends sweeping changes to child services in the NHS, not least the abandonment of what is known as the “affirmation model” and the associated use of puberty blockers and, later, cross-sex hormones. The evidence base could not support the use of such drastic treatments, and this approach was failing to address the complexities of health problems in such children.
Many trans advocacy groups appear to be cautiously welcoming these recommendations. However, there are many who are not and have quickly tried to condemn the review. Within almost hours, “press releases“, tweets and commentaries tried to rubbish the report and included statements that were simply not true. An angry letter from many “academics”, including Andrew Wakefield, has been published. These myths have been subsequently spreading like wildfire.
Here I wish to tackle some of those myths and misrepresentations.
Myth 1: 98% of all studies in this area were ignored.

Fact
A comprehensive search was performed for all studies addressing the clinical questions under investigation, and over 100 were discovered. All these studies were evaluated for their quality and risk of bias. Only 2% of the studies met the criteria for the highest quality rating, but all high and medium quality (50%+) studies were further analysed to synthesise overall conclusions.
Explanation.
The Cass Review aimed to base its recommendations on the comprehensive body of evidence available. While individual studies may demonstrate positive outcomes for the use of puberty blockers and cross-sex hormones in children, the quality of these studies may vary. Therefore, the review sought to assess not only the findings of each study but also the reliability of those findings.
Studies exhibit variability in quality. Quality impacts the reliability of any conclusions that can be drawn. Some may have small sample sizes, while others may involve cohorts that differ from the target patient population. For instance, if a study primarily involves men in their 30s, their experiences may differ significantly from those of teenage girls, who constitute the a primary patient group of interest. Numerous factors can contribute to poor study quality.
Bias is also a big factor. Many people view claims of a biased study as meaning the researchers had ideological or predetermined goals and so might misrepresent their work. That may be true. But that is not what bias means when we evaluate medical trials.
In this case we are interested in statistical bias. This is where the numbers can mislead us in some way. For example, if your study started with lots of patients but many dropped out then statistical bias may creep in as your drop-outs might be the ones with the worst experiences. Your study patients are not on average like all the possible patients.
If then we want to look at a lot papers to find out if a treatment works, we want to be sure that we pay much more attention to those papers that look like they may have less risk of bias or quality issues. The poor quality papers may have positive results that are due to poor study design or execution and not because the treatment works.
The Cass Review team commissioned researchers at York University to search for all relevant papers on childhood use of puberty blockers and cross-sex hormones for treating “gender dysphoria”. The researchers then graded each paper by established methods to determine quality, and then disregarded all low quality papers to help ensure they did not mislead.
The Review states,
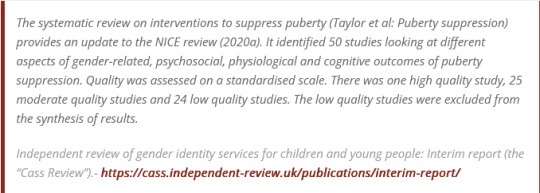
As can be seen, the conclusions that were based on the synthesis of studies only rejected 24 out of 50 studies – less than half. The myth has arisen that the synthesis only included the one high quality study. That is simply untrue.
There were two such literature reviews: the other was for cross-sex hormones. This study found 19 out of 53 studies were low quality and so were not used in synthesis. Only one study was classed as high quality – the rest medium quality and so were used in the analysis.

Again, it is myth that 98% of studies were discarded. The truth is that over a hundred studies were read and appraised. About half of them were graded to be of too poor quality to reliably include in a synthesis of all the evidence. if you include low quality evidence, your over-all conclusions can be at risk from results that are very unreliable. As they say – GIGO – Garbage In Garbage Out.
Nonetheless, despite analysing the higher quality studies, there was no clear evidence that emerged that puberty blockers and cross-sex hormones were safe and effective. The BMJ editorial summed this up perfectly,

Myth 2: Cass recommended no Trans Healthcare for Under 25s.

Fact
The Cass Review does not contain any recommendation or suggestion advocating for the withholding of transgender healthcare until the age of 25, nor does it propose a prohibition on individuals transitioning.
Explanation
This myth appears to be a misreading of one of the recommendations.
The Cass Review expressed concerns regarding the necessity for children to transition to adult service provision at the age of 18, a critical phase in their development and potential treatment. Children were deemed particularly vulnerable during this period, facing potential discontinuity of care as they transitioned to other clinics and care providers. Furthermore, the transition made follow-up of patients more challenging.
Cass then says,
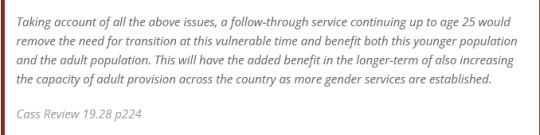
Cass want to set up continuity of service provision by ensure they remain within the same clinical setting and with the same care providers until they are 25. This says nothing about withdrawing any form of treatment that may be appropriate in the adult care pathway. Cass is explicit in saying her report is making no recommendations as to what that care should look like for over 18s.
It looks the myth has arisen from a bizarre misreading of the phrase “remove the need for transition”. Activists appear to think this means that there should be no “gender transition” whereas it is obvious this is referring to “care transition”.
Myth 3: Cass is demanding only Double Blind Randomised Controlled Trials be used as evidence in “Trans Healthcare”.

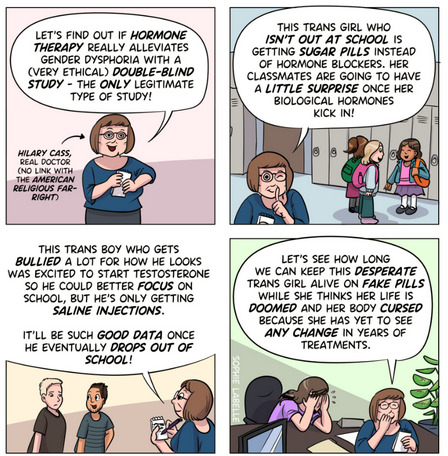
Fact
While it is acknowledged that conducting double-blind randomized controlled trials (DBRCT) for puberty blockers in children would present significant ethical and practical challenges, the Cass Review does not advocate solely for the use of DBRCT trials in making treatment recommendations, nor does it mandate that future trials adhere strictly to such protocols. Rather, the review extensively discusses the necessity for appropriate trial designs that are both ethical and practical, emphasizing the importance of maintaining high methodological quality.
Explanation
Cass goes into great detail explaining the nature of clinical evidence and how that can vary in quality depending on the trial design and how it is implemented and analysed. She sets out why Double Blind Randomised Controlled Trials are the ‘gold standard’ as they minimise the risks of confounding factors misleading you and helping to understand cause and effect, for example. (See Explanatory Box 1 in the Report).
Doctors rely on evidence to guide treatment decisions, which can be discussed with patients to facilitate informed choices considering the known benefits and risks of proposed treatments.
Evidence can range from a doctor’s personal experience to more formal sources. For instance, a doctor may draw on their own extensive experience treating patients, known as ‘Expert Opinion.’ While valuable, this method isn’t foolproof, as historical inaccuracies in medical beliefs have shown.
Consulting other doctors’ experiences, especially if documented in published case reports, can offer additional insight. However, these reports have limitations, such as their inability to establish causality between treatment and outcome. For example, if a patient with a bad back improves after swimming, it’s uncertain whether swimming directly caused the improvement or if the back would have healed naturally.
Further up the hierarchy of clinical evidence are papers that examine cohorts of patients, typically involving multiple case studies with statistical analysis. While offering better evidence, they still have potential biases and limitations.
This illustrates the ‘pyramid of clinical evidence,’ which categorises different types of evidence based on their quality and reliability in informing treatment decisions

The above diagram is published in the Cass Review as part of Explanatory Box 1.
We can see from the report and papers that Cass did not insist that only randomised controlled trials were used to assess the evidence. The York team that conducted the analyses chose a method to asses the quality of studies called the Newcastle Ottawa Scale. This is a method best suited for non RCT trials. Cass has selected an assessment method best suited for the nature of the available evidence rather than taken a dogmatic approach on the need for DBRCTs. The results of this method were discussed about countering Myth 1. Explainer on the Newcastle Ottawa Scale
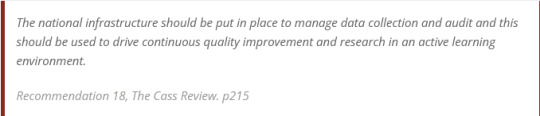
As for future studies, Cass makes no demand only DBRCTs are conducted. What is highlighted is at the very least that service providers build a research capacity to fill in the evidence gaps.
Myth 4: There were less than 10 detransitioners out of 3499 patients in the Cass study.
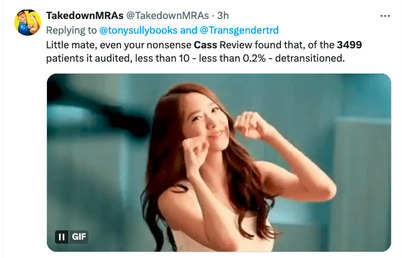

Fact
Cass was unable to determine the detransition rate. Although the GIDS audit study recorded fewer than 10 detransitioners, clinics declined to provide information to the review that would have enabled linking a child’s treatment to their adult outcome. The low recorded rates must be due in part to insufficient data availability.
Explanation
Cass says, “The percentage of people treated with hormones who subsequently detransition remains unknown due to the lack of long-term follow-up studies, although there is suggestion that numbers are increasing.”
The reported number are going to be low for a number of reasons, as Cass describes:

Damningly, Cass describes the attempt by the review to establish “data linkage’ between records at the childhood gender clinics and adult services to look at longer term detransition and the clinics refused to cooperate with the Independent Review. The report notes the “…attempts to improve the evidence base have been thwarted by a lack of cooperation from the adult gender services”.
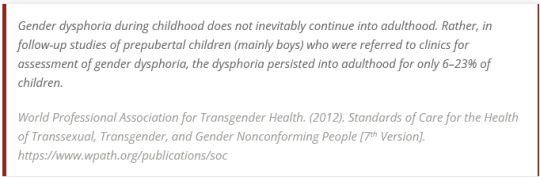
We know from other analyses of the data on detransitioning that the quality of data is exceptionally poor and the actual rates of detransition and regret are unknown. This is especially worrying when older data, such as reported in WPATH 7, suggest natural rates of decrease in dysphoria without treatment are very high.
This suggests that active affirmative treatment may be locking in a trans identity into the majority of children who would otherwise desist with trans ideation and live unmedicated lives.
I shall add more myths as they become spread.
#Cass report#the cass report#cass review#the cass review#trans lies#gender critical#tras#medical malpractice#the tide is turning
71 notes
·
View notes
Text

#ai nude#sexy pose#sexy breast#ai model#sexy nude#ai girl#hot nude#ai generated#sexy content#trasparecy#tras
58 notes
·
View notes
Text
It really boils down to this.

BoJack Horseman, S3E8
#feminism#radical feminism#radfem safe#radfem#bojack quotes#TRAs#TIMs#male entitlement#gender discourse
2K notes
·
View notes
Text
for anyone who thinks that he's just some clueless Richie Rich who is simply coping with his homosexuality and obsession with performing femininity via transition and nothing else.
He's just as sinister as the rest of the vocal TRAs and likely would not care if you have to deal with years long legal battles because your workplace doesn't think that reality is something that should be acknowledged.
149 notes
·
View notes
Text
I'm wondering, for what trans rights American TRAs are fighting for? I just don't get it. Transitioning children? Self-identification? Abolishing gendered spaces?
I'm from Poland. Over here, trans people have it awfully hard, both medical and social transition are very troublesome and even dangerous. Gay people can't get married here, can't adopt kids. Conversion therapy is alive and well despite being illegal. Hell, a girl at the pride parade got SHOT for nothing a few weeks back. In 2020 a bunch of men went around after the pride parade beating people up just for having something rainbow on them.
Those "anti-trans" bills y'all are talking about are bills that protect women and children. You have it really good in the US compared to Eastern Europe, the Middle East, Africa, South America, etc.
#gender critical#tra#trans rights activism#tras#radblr#women deserve better#gender ideology#anti gender ideology#radfems do interact#terf#terf safe#terfsafe#terfblr#usa#trans identified male
147 notes
·
View notes
Text
The fully sane to fully insane TRA progression:
"I'm a man, but I don't feel comfortable actively conforming to traditionally masculine gender roles."
Nothing wrong with that! Gender is bullshit anyways.
"I'm a man, but I feel more comfortable actively conforming to traditionally feminine gender roles."
Cool. You do you.
"I'm a man, but I have a mental disorder that makes me deeply uncomfortable with being male. In addition to presenting and acting in a traditionally feminine manner, I would like to be recognized socially as a woman and addressed as 'she/her' in order to more easily manage the distress that results from my condition."
Okay. That's fine I guess.
"I'm a woman who was incorrectly identified as male at birth. I am not meaningfully distinct from biological women and therefore am entitled to exist in single sex, female only spaces, and to speak on behalf of women as a group. Women as a class should change the language they use to discuss their bodies and their oppression in order to make me more comfortable even though many of such discussions necessarily do not involve me. Women are to blame if I am the victim of male violence, especially women who are concerned about the issue of male violence. If I don't have access to a lifetime supply of medically unnecessary hormones and receive multiple invasive cosmetic surgeries in order to make my body appear more female, I will become suicidal, but also I am not mentally ill. Calling my condition, which causes me daily psychological distress, a mental illness is hate speech."
Um...
"What even is a woman, anyways? I know I'm a woman, because I identify as a woman, and that's what it means to be female. Gender isn't real and doesn't exist. But also transgender identities are real and valid and trans women are discriminated against because their gender is female. Sex is an arbitrary nonbinary social construct just like gender, also sex has nothing to do with gender. But also I would like my penis to become a vagina in order to alleviate my gender dysphoria. Sex based oppression isn't real, only gender based oppression is, and it is a totally random coincidence that the concept of gender happens to benefit the penis people at the expense of the vagina people 99% of the time. The existence of intersex birth defects demonstrates that humans are not a gonochoric species. No one is born male or female. A clitoris is just a very tiny penis, and a penis is just the outie version of a vagina, and sex organs don't determine whether someone is male or female. I still really want a vagina specifically though because I am female and females have vaginas. Homosexuality has nothing to do with sex and being exclusively same sex attracted is morally wrong. I think minors should be allowed to take cross sex hormones and receive cosmetic surgery but also no one is saying that shut up stop lying. I don't have a mental illness, that would be bad and gross, I'm perfectly normal and dysphoria is perfectly healthy, and you must literally want me to die if you think otherwise, how dare you be so hateful towards mentally ill people. Not giving in to my every demand and actively catering to my desires is literally partipating in genocide. Choke on my cock and die you misogynist!"
...
#radical feminism#radfem#radblr#feminism#tras#tra logic#gender critical#guys I used to be on board until things got to stage four
173 notes
·
View notes
Text
TRAs to radfems: we are not violent!! YOU are the ones who wish all trans people were dead!! Why can't you just be kind??
Also TRAs under every radfem post:

#🤡#the circus#radfem#radical feminism#radfem safe#radfems do touch#radfems do interact#tras#trans rights#tims#woke hypocrisy#trans women#lgb drop the t#male violence#adult human female#sex not gender#gendies
480 notes
·
View notes
Text
‘terfs’ don’t hold conservative beliefs. The rf in that acronym (if you didn’t know but most TRAs are so stuck on calling anyone a terf) stands for radical feminism. And if a TRA did some reading which we all know they never do, they would quickly learn there’s a complete difference between radical feminism and conservatism. It’s like night and day.
277 notes
·
View notes
Text
South African TRAs bullied a black woman, Ntsiki Mazwai, into deleting her tweet about trans women being men.
They’ll do anything to silence women.



#TRAs#trans rights activists#gender cult#gender ideology#gender critical#radical feminism#black radfem#radfem#radblr#radical feminists please interact#radical feminists do interact
327 notes
·
View notes
Text

Do these people know what words mean
56 notes
·
View notes
Text
dudes be like: THERES NO RADFEMS IN THE GLOBAL SOUTH😠😠😠 —while saying it to a radfem born, raised and still living, in the global south
40 notes
·
View notes
Text
detrans women deserve so so so much love
the way the tra community treats them like evil beings who deserve the worst after they detrans is very telling of the tra community's thoughts and feelings on women as a whole
#the ostracization of these women by the same communities that allegedly loving accepted them with open arms the instant they wake up and go#against the grain is scary cultish behaviour#tras#tra#terfblr#radblr#radfems#radical feminists do touch#radfems do touch#radical feminism#radfem safe#detrans ftm#detrans women i love you
39 notes
·
View notes
Text

En la mañana, cuando despiertes, no olvides agradecer, abrir la ventana de las oportunidades, respirar profundo por un día más de vida y sonreír, esa es la pildorita, la vitamina de ánimo que te va a ayudar a ver lo positivo de cada amanecer, lo increíble que es la vida, lo majestuoso que es comenzar con el optimismo a su máximo nivel y la energía para continuar.
De noche, vuelve agradecer haber concluido el día y espera en Dios que mañana sea una nueva oportunidad de ir tras tus sueños. 😊🙏🏼🌹
Leregi Renga
26 notes
·
View notes
Last Seen Blogs


tummy-stuffing-king
a round tum is a happy tum

liliandkenken
lili and kenken

mil-aucca
Untitled

goingtothehospital
glad