#rsd
Text

I know people are focusing on the “I love him either way” part of this, but the “makes a lot of issues about himself” part stuck out to me.
Because a few times over the course of the show, it’s been said that Buck makes things about himself when they’re not. Like with Eddie and the fighting ring or with Red.
I had heard before about how neurodivergent people often relate their own stories to a conversation as a way to make connections and better understand things. This is Anecdotal Conversation. Autistic people and people with ADHD can do this.
I feel like this is what Buck did with Red. But with the fighting, he more so put all the blame and responsibility for it on himself. Which is also something that people with ADHD do.
(I’ve also seen @maygranted say that people with OCD can tend to catastrophise situations and put responsibility on themselves which definitely sounds like something Buck does)
#911 abc#911 on abc#911 fox#evan buckley#oliver stark#adhd!evan buckley#ocd!evan buckley#adhd#moral ocd#ocd#buddie#rsd#neurodivergent#anecdotal conversation#ryan guzman#eddie diaz#red delacroix
41 notes
·
View notes
Text
extremely unsexy of adhd to make me both very annoying and very sensitive to the concept of being perceived as annoying
#personal#actually adhd#vent post#mentat illmess strikes again smh#rsd#rejection sensitive dysphoria#kill meeeee
46K notes
·
View notes
Text
Reblog if you’re a transfem who is shy and you fear abandonment, even when you know that your friends are amazing and would never leave you.
Or if you like pizza.
5K notes
·
View notes
Text

its the little things
1K notes
·
View notes
Text

Stinky Bear motivation. Extra rolls for Initiative
#positivity#positive affirmations#dnd#rpg#tabletop rpg#mental health#trauma#cptsd#ptsd#depression#anxiety#adhd#rsd#rejection#relationships#boundaries#reminders#soft post
2K notes
·
View notes
Text
being neurodivergent is all fun and games until someone is slightly critical of you and you suddenly feel physically ill
#*not to trivialize being neurodivergent lol ik its not actually all fun and games#but it does make u hot and sexy and cool so#rejection sensitive dysphoria#rsd#neurodivergent#actually adhd#actually autistic#actually neurodivergent#eden talks
33K notes
·
View notes
Text
rejection sensitivity is so fucking lame. like boo hoo look at me i felt mildly ignored for 30 seconds and already started planning my own funeral liKE BITCH CHILL it was never that serious
665 notes
·
View notes
Text
#adhd#audhd#autism#neurodivergent#adhd things#adhdlife#adult adhd#adhd stuff#rejection#rejection sensitivity#adhd rsd#rsd#rsd things#actually rsd#actually audhd#actually adhd#actually autistic#actually neurodivergent
2K notes
·
View notes
Text
Rejection Sensitivity Dysphoria (RSD) in ADHD and Autistic People

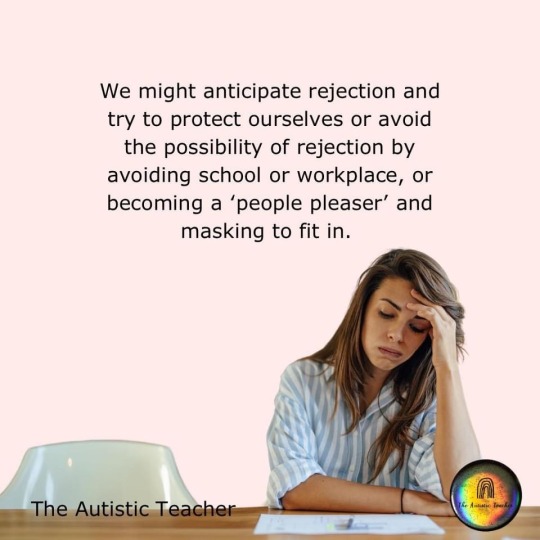
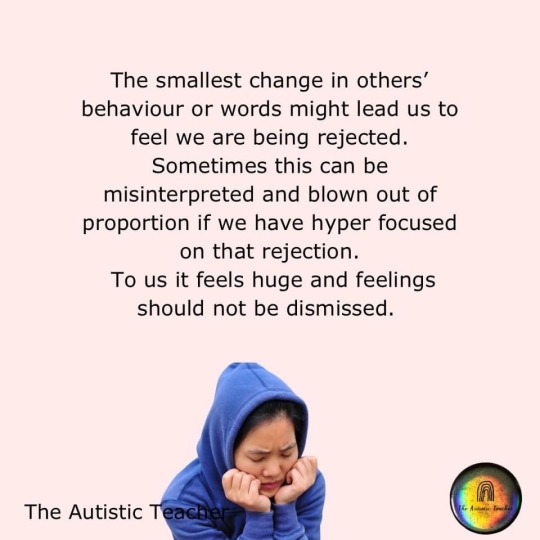

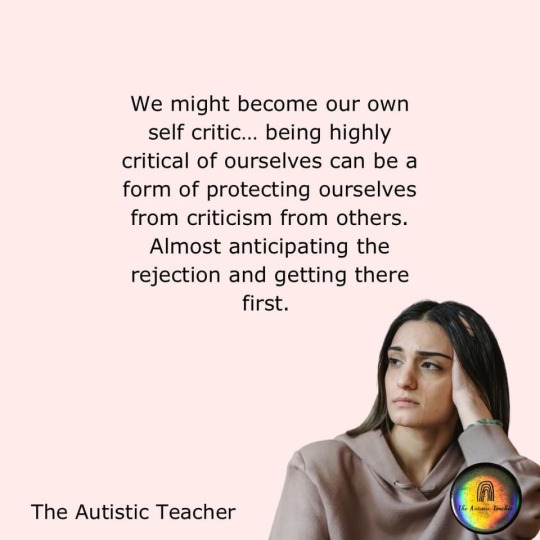
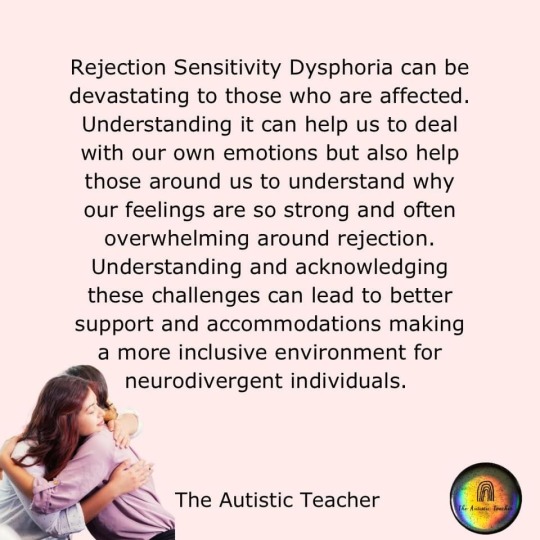
The Autistic Teacher
#autism#actually autistic#adhd#adhd post#rejection sensitive dysphoria#rsd#rsd explained#neurodivergence#neurodiversity#actually neurodivergent#feel free to share/reblog#The Autistic Teacher (Facebook)
729 notes
·
View notes
Text
youtube
Feeling a little overly perceived by Dr. Dodson right now, not gonna lie.
I'll throw a transcript under the cut, but both reading the transcript and listening to the video can be difficult as it's quite long, so here's some highlights. As always, these are the opinions of a specialist but only one specialist, so take with a grain of salt, and if you have research to add to this, please feel free to comment or reblog with it. I believe this presentation is from sometime in 2022.
ADHD appears to derive from issues in the corpus striatum in the brain. In most people, the corpus striatum filters out all but the most important input AND output; with ADHD, the things normally handled "outside of awareness" must be handled consciously.
People with ADHD don't see their emotions coming. Emotion is immediate, intense, and unfiltered, making therapies like CBT or ACT difficult, because you can learn the technique but you won't have time to employ it. Because people with ADHD have impulse control issues, expressing emotions "inappropriately" is common, leading people with ADHD to believe they can't trust themselves.
One function of ADHD-typical dysregulation is Rejection Sensitive Dysphoria, which nobody understands even a little. People who have it can't even adequately describe it to people who want to study it. It is intense, painful, and apparently impossible to control. Prevention is based in maladaptive behaviors designed to avoid it entirely (perfectionism, people pleasing, generalized withdrawal). The only currently known treatment is alpha agonist medication.
Lastly, by the age of twelve, a child with ADHD has likely received twenty thousand more "negative or corrective" messages than their neurotypical peers. (This isn't relevant to the rest, I just found it sufficiently horrifying to warrant inclusion. Fortunately for me, if I got 20,000 negative or corrective messages, I wasn't paying attention for most of them.)
Anyway, here's the transcript of the first half. I did this by copying and cleaning up the auto-transcript on YouTube, but I stopped at Question Time, so this is only the first half (the presentation). Transcription of the second half is available at YouTube.
There is suddenly a very large interest in the whole subject of emotional dysregulation and ADHD. That has been driven oddly enough by the Food and Drug Administration, which has just opened up several pathways that drug companies can study emotional dysregulation and whether or not their medications can get an FDA indication for emotional dysregulation. So it's sort of follow the money. Up until then, there was not a great deal of interest for ADHD emotional dysregulation.
We have to understand that the ADHD diagnostic criteria were not made for people like you and me, either practitioners or people who have ADHD or their families. They were designed for and made by people who do research and pretty much that's it. People who do research have to have criteria that they can physically see and count. "Little Johnny was up and out of his chair three times in the last hour," and you can write a three on your clipboard. Things which are invisible, not always there, hard to count, or even hidden by the patient, don't lend themselves to research very easily and so tend to be ignored. And so consequently this is one of the main reasons why emotional dysregulation -- until there was some other motive provided -- was pretty much ignored and disregarded.
Consequently ADHD right now, if you look at the 18 diagnostic criteria, are almost entirely behavioral criteria. What is the person doing? Not how is the person thinking, what is the patient feeling, how are they controlling their emotions, how are they sleeping. Things that are all very, very important to the person who has ADHD but which is essentially ignored by the diagnostic criteria.
Why should you care? Who really cares about this? Well, the definition of what ADHD is and isn't defines who and what will be studied. It defines who will actually get into a study and what questions will be asked. It defines who will be diagnosed with ADHD and who will not. One of the most common problems I get is with a secondary referral to me -- somebody clearly has ADHD but they're not pinging off the walls, they can sit and do their work, especially when they get into a hyperfocus, and so they're told they couldn't possibly have ADHD. When really they just have the inattentive subtype and they're not being driven by their behavior, their overt behavior. Therefore it defines who will get treatment, who will get insurance coverage for that treatment, and who will get accommodations in school when they're young and at the workplace when they're older.
Consequently we should also care because the other major components of ADHD get ignored. These are the ones that if you really stand back and look at it cause the greatest amount of impairment, the greatest amount of embarrassment, the greatest amount of just…problems in general. We're talking about cognition and thinking, that people with ADHD fundamentally think in a different way than do neurotypical people. They are able to engage with the tasks of their lives in a totally different way. Their ability to control their emotions and their behavior, control their emotional responses, tremendously affects their self-esteem and their self-definition. Who am I? What am I worth? What am I valued? Why am I valued in a certain way? What do other people think of me?
It affects tremendously the nature and healthiness of relationships. How you respond emotionally to the people in your realm makes a great deal of difference about the healthiness and gratification you get from your relationships. Being highly dysregulated in terms of your energy and emotions also affects deeply how well you sleep, how easy it is to fall asleep and awake refreshed, and of course it affects emotional dysregulation.
And this is probably, when you look at it in the long term and especially with adults, probably the most impairing part of the ADHD syndrome. The vast majority of people with ADHD have found ways around their academic and work performance, but they haven't found their way around their emotional reactions to the people and events of their lives.
At all points in the life cycle -- child, adolescent, adult, and elderly -- people who have ADHD nervous systems lead intense, passionate lives. Their highs are higher, their lows are lower, all of their emotions are much more intense. And that really is what we're talking about: not really the quality of the emotions -- people who have ADHD have the same types of emotions for the same reasons that everybody else does. What we're talking here, in terms of dysregulation, is two things: one, the expression of emotions, being able to choose whether or not you let an emotion out. And then, when you do decide to express it, how intensely that emotion is experienced and expressed by you as a unique individual.
Consequently just about everybody with ADHD, but especially little children, are always at some sort of risk of being overwhelmed by their own emotions from within themselves. This is something that needs to be really emphasized: a lot of people with ADHD grow up not being able to trust themselves.
So why is this happening, especially to people with ADHD? I think that just about everybody now would agree that ADHD is primarily a problem of insufficient inhibition, being able to slow down and keep things from happening. If you look at the mass of the human brain, 85% of all the nerves in your brain and out in your nervous system are inhibitory in function. We happen to be aware of the other 15% because we can see what happens when those nerves are used: they create movement, they create emotions, they create our experience and memory. We have to remember they are a minority of the actual mass of the human brain.
Most of what happens inside the brain occurs outside of awareness. What happens is the brain starts something, it gets it moving, and then uses inhibition to guide that toward the destination it wants. It's like shooting off a rocket -- shooting it off is the easy part, guiding it to where you want it to go is the hard part.
When you look at where stimulant class medications work, they work solely in the deep areas of the brain down in the basal ganglia, and especially in an area called the corpus striatum, which is just Latin for a "striped body". That's how it looks when you look at it -- it's got many very fine stripes in it. This area, the corpus striatum, is almost entirely inhibitory in function. What it does is that it inhibits neurological input and output to just the one piece of information or one action that happens to be most important at that time. Everything else gets handled, but it gets handled out of awareness.
Probably the easiest place to see this in action is when we're driving a car. Driving a car is the most difficult thing that the average human being ever has to learn how to do. It's a very difficult process, if anybody has ever had an adolescent learning to drive. But once we learn how to drive a car we do it largely outside of our own conscious awareness. We can drive along, talk to the person on the seat next to us, think about what we're going to have for dinner, sing along to the radio, and not really pay attention, conscious attention, to what's going on around us. But if suddenly something is out in front of the car, even before our conscious brain can process what that thing is, our corpus striatum has already handled it. Slam on the brakes, swerve to miss it, start to question that person's parentage, in the twinkling of an eye. The corpus striatum has been scanning everything, handling everything.
So basically what ADHD is, is that relative lack of inhibition that should be there. Inattention, which is a cardinal feature of ADHD, is the relative lack of the inhibition of other inputs or distractions. When we look at physiologically what's happening, we don't actually pay attention to one thing. Neurologically, we suppress every other thing we might engage with except the one thing that we want. It is maximally inefficient in that way.
Impulsivity is a relative lack of inhibition, of the expression of actions and emotions before you can think about them and make decisions about that expression. Hyperactivity is the relative lack of inhibition of physical and mental activity. When the physical activity of the hyperactive little boy who's pinging off a wall goes away in adolescence, they're still very much mentally active in their own brains.
So what? The “so what” for most of us is that when this area of the brain is not working as it should, people cannot regulate the experience and expression of their emotions. Emotions are experienced as completely unmodified and unscreened. The word that most people use is that they are raw. They come out without any modification at all, they go in without any modification at all. People can see this in hyperacusis, where somebody chewing or the conversation across the restaurant comes in loud and clear because it can't be screened out.
All this is tremendously overwhelming. We get overwhelmed by entirely too much input, and the impulse to have entirely too much output. It's exhausting, and when it does get inappropriately expressed it's embarrassing, so consequently people with ADHD must always be vigilant of themselves.
Now, when we look at the traditional therapies that have been used, or tried to be used, with ADHD, they have had very very poor track records. They're largely ineffective in helping people control the expression of what they think and feel. The reason for this is that people with ADHD don't see their own emotions, their own actions, coming. They find out about their emotions and actions the same way everybody else does: it's already out there before they even know that it's coming. Consequently they don't have the time and the warning to use the techniques and new skills that they may have learned in behavior modification therapy, or in cognitive therapy. They learned them, learned them perfectly well, but the cat’s out of the bag before they can make use of them.
Right now, as we sit here today, medications are the only thing we have to offer that have a proven track record, because they're there all the time. We have two basic groups: we have the stimulant class medications which are amphetamine, methylphenidate, et cetera, which help directly with inhibition. They help slow things down, they help inhibit both input that would distract us and output. It gives you the same two seconds that everybody else has, to see an emotion or an action coming up, to play it out in your mind. “If this happens then this will happen, then that'll happen. Oh, I don't want that to happen, I'll redirect it.”
The alpha agonist, of which we have two -- guanfacine and clonidine -- inhibit the energy driving the speed and intensity of response. Interesting enough, when we look at just clean effectiveness, when we measure how effective is this treatment, the alpha agonists are significantly more effective than are the stimulants. Usually that's kind of a false choice, because most people end up taking both classes of medication.
A very special type, I think, of emotional dysregulation is -- again a terrible technical term -- what's called Rejection Sensitive Dysphoria. We actually don't know what it is. It's much too early to tell. But it does seem to be a thing with which many people with ADHD identify. There was a brief article from ADDitude that got posted on Reddit, on their subreddit on ADHD; that particular posting got twice as many responses, in less than a month, than any other posting that had ever been put on that subreddit. It really touched a lot of people in a strong way.
In my own checklist, when I'm asking about Rejection Sensitive Dysphoria, the question I have is: “For your entire life, in other words going all the way back into childhood, have you always been much more sensitive than other people you know to rejection, teasing, criticism, or your own perception that you’ve failed or fallen short?” This is directly from a psychiatric textbook, an old one, and it's the definition of a technical term, for psychiatrists called Rejection Sensitive Dysphoria.
It's important to note, this is all a matter of degree. No one likes being rejected or criticized. Everybody hates it when we fail, we fall short, especially in front of other people. Rejection Sensitive Dysphoria is much more intense, and is much more than this universal discomfort.
When they were originally doing the research on this particular idea, 45 years ago, they wanted to get that intensity right up there in the name, and so they chose the word dysphoria -- which unfortunately happens to be Greek -- but it means “unbearable”. Because that was the description they were getting from people over and over and over again. Again, for reasons unknown, people with rejection sensitivity have trouble describing what the intense emotion is all about. They can describe its intensity -- “it's awful, it's terrible, it's catastrophic,” -- but not the quality of the mood. And so, over and over again, these research subjects would finally just tell the researcher, “Look, man, back off. I can't find words to tell you what this awful feeling feels like, but I want you to know I can hardly stand it.” And so that's where the word dysphoria came from. A researcher at Harvard who decided to put it into Greek, but that unbearable quality is very much a part of what's going on, a part of the experience of Rejection Sensitive Dysphoria.
It's extremely common in people with ADHD; my guess is that about 95% of my patients report it as a significant impairment, and about a third of my patients say that it is by far the most impairing part of their ADHD. For the majority of people, and most occurrences, it is not that particularly disruptive, but when it hits, it turns your life upside down.
So how is rejection sensitivity experienced? There's no warning. It hits out of the blue; there's no way to protect yourself from it. It happens all at once, it goes from zero to a hundred percent instantaneously. It is commonly experienced as being physically painful, as if someone just punched you in the chest or punched you in the stomach -- there's an aching in the core of your being.
Once it gets started it seems to be largely uncontrollable until it's run its course, whatever it is. The quality of the mood is indescribable. Most people struggle to find any words at all to describe this feeling, even though it's massively intense. The duration can be a few minutes to several months. It's a very potent experience and can make it very difficult to risk ever being rejected or criticized again.
If this very intense emotional reaction is internalized, it looks for all the world like an instantaneous major depression, complete with suicidal thinking. And so a lot of times people do get a diagnosis of major depression, because the clinician they're working with fails to pick up the triggered, instantaneous nature of the onset of that depressive-looking syndrome. If it's externalized, it presents as a rage that is directed at the person or situation that wounded them so terribly. In fact, being “wounded” is is a very common description. This sort of sudden trigger change, with an intense emotional response, not uncommonly leads to a misdiagnosis of borderline character organization.
So if you can't see it coming, and you can't do anything once it's happened, how do people try and protect themselves from episodes of rejection sensitivity happening in the first place? Some people use perfectionism; they try to be above reproach. They feel driven to be the very best at everything they do. These are the penultimate overachievers. It works, but it's also an absolutely terrible, driven way in which to live.
By far the most common response is that people become people pleasers. They are constantly scanning everybody around them and trying to figure out what that person wants or would approve of, and that's what they give them, so much so that it is the to the exclusion of what they want for their own lives. These are people who take care of others, please others, to the exclusion of any sort of gratification in their own lives.
Another very common way that people try to deal with this is that they give up trying anything new, giving up
anything in which they might fail or be embarrassed. I have hundreds of patients who have never been able to apply for a job or ask someone of the opposite sex out for a date. Just the imagination of being told no is so frightening, so devastating, that they just say, “No, I'm not going there. I'll sit this one out.”
One of the most effective ways of dealing with this are the alpha agonist medications, and when they work they can be almost completely effective. Alpha agonist again is a tongue twisting name, but it's not as tongue-twisting as the full name, which is alpha-2 selective adrenergic agonists. So you can see why we shorten it a bit. They were originally blood pressure medications that came on the market in the early 1980s. They worked very poorly -- when they did work, at most they lowered blood pressure about 10%, which was measurable but it still required other things that needed to be done in order to get most people's blood pressure down into a therapeutic range.
We have two of them, guanfacine which was marketed both as immediate release and extended release under the name of Intuniv, and clonidine, which was marketed under the trade name of Kapvay, both as an immediate release product and as a delayed release product. They have been used as a treatment of the hyperactive component of ADHD for more than 30 years, so these are not new medications for the field of ADHD. They're very much the treatment of choice for the “hyperactive, disruptive, and obnoxious little boy” that is what most people have in their minds when they consider the notion of “What does a person with ADHD look like?”
The exact mechanism of action of these medications both in ADHD and especially in rejection sensitivity is highly unclear. We really don't know -- we have a couple of ideas but they are very definitely theoretical. The only thing that we know for sure is that the stimulants don't work by stimulating anything, and that the alpha agonists don't work by being alpha agonists. How they do work is completely unknown.
We have two medications, they seem to work equally well, so there's nothing that would lead you to choose one over the other. The problem is that the robust response that we're looking for that really changes people's lives, is disappointingly low -- at about 30% to either molecule. Luckily that 30% is a different 30% of people, so that 30% of people get a good response to guanfacine but it's largely a different 30% that get a response to clonidine. So if the first medication tried does not work, it makes good clinical sense that that one should be stopped and the other one tried. There was an unfortunately worded sentence in an article I wrote for ADDitude several years ago that gave the impression that you could use the two medications together; they should not be used together. You try one, if that doesn't work you try the other.
The typical dose of either one is in the range of three milligrams of guanfacine per day or about three tenths of a milligram of clonidine per day. If you take all the people who get a good robust response to either one of these medications, about 80% are going to end up at these doses, so it's by far the most common dose.
There are of course side effects. Anything that's going to adjust the adrenaline system of the body is going to have the potential for sedation as a side effect, and this does occur for about 25% of people. It's usually mild and it does go away -- over a period of several months. So a person has to be fairly patient with that. It can cause dry mouth, and it's by a different mechanism then the stimulants can cause dry mouth, so the two of them together can really make your mouth cottony dry. And the third one is an accentuation of a universal experience we've all had, when we stand up quickly and suddenly and we get dizzy, get kind of a head rush, vision goes a bit gray. The technical term for it is orthostasis. And this can happen more frequently when you take the alpha agonist medications.
The benefits of the alpha agonist medications take a while to develop. When you change the dose it takes five days for the benefits to develop, so once again they're not like the stimulants where what you see is what you get at one hour. It takes a while for these medications to work and to see all that they can do.
Now just as a side note, Strattera has been looked at in two studies for emotional dysregulation and the results have been what they call mixed. If they did work it was only to a very minimal degree, almost undetectable, so Strattera does not seem to be a medication one could use and expect to have it help with emotional dysregulation.
So in summary, emotional dysregulation is a basic feature of ADHD, is almost universal in ADHD, and it should be considered as a core symptom of ADHD that ought to be evaluated in every initial evaluation. Rejection sensitivity…it's unclear yet -- this is an old concept that has only been brought up in the last couple of years. Its exact nature is still unclear. It does seem to be a specific form of emotional dysregulation, especially in regard that it does respond very well to medication. But again, how it fits into emotional dysregulation is completely unclear at this point. It does seem to be something that's really important, though. It is a thing that resonates with a large number of people with ADHD.
925 notes
·
View notes
Text
"I'm sorry I vented and took up your time with my bullshit" ❌
feeds abandonment fears, implies having needs and being helped with them are wrong, makes it all about you
"Thank you for being patient with me through that, I appreciate that you took the time" ✅
shows your gratitude, affirms your affinity, no "using up" anybody's effort, makes it about you both as equals
"I'm sorry I dumped without checking consent first. I need to act respectfully and ask for your permission before I vent" ✅
"I'm sorry I said x, that was inappropriate of me to put on you" ✅
"Was it okay when I said x the way I did?" ✅
"Would you like to place a boundary around that?" ✅
"What could I do/say instead that's healthier for us both?" ✅
correct an actual wrong, seize due accountability, consider their rights as much as yours, make amends, work to correct missteps going forward
#this is a personal callout 😍#reminders#codependency#codependent#recovering codependent#recovery#bpd#rsd#rejection sensitive dysphoria#guilt#shame#taking up space#waste of space#sorry for existing#apology#over apologizing#sorry#people pleaser#toxic#regret#remorse#gratitude#self worth#codapunk
702 notes
·
View notes
Text
I highly recommend that everyone (especially nd people who struggle w self esteem) have a collection of “proof people don’t hate me” and go look at it whenever they’re sad. I’ve compiled report card comments, stuff my friends say, all sorts of things that made me feel cared about and appreciated. And anytime I get that feeling that I’m worthless and unloved, I go through that file folder and feel better.
#chaoticbuggybitchboy#life advice#life hacks#actually adhd#rsd#adhd rsd#actually autistic#actually histrionic#mentally fucked#my posts that hit it off
242 notes
·
View notes
Text
AuDHD decided to be really funny when it made me really annoying (adhd), absolutely terrified of being perceived as annoying (rsd) and having no idea what people find annoying (autism)
#and the amazing solution to this problem is just to distance youself from your friends and stop seeing everyone!#and never leave your flat!#very fun! /j#audhd#autism#adhd#neurodivergent#rsd#ramblings
303 notes
·
View notes
Text
my favorite thing about rejection sensitive dysphoria is about how it's such bullshit that pushes you to never try anything new, or to only do it in secret.
"we can't let our loved ones know we're trying a new thing, even if it's something as minor as getting a meal we don't normally try! what if they say something slightly critical or negative about it and we spiral down into depression and then explode?"
WHEN HAS THAT EVER HAPPENED, BRAIN? NEVER, THAT'S WHEN.
but it means you try things so much less often, and you're always wanting to keep secrets, even when those secrets are fucking pointless. like "we can't let our wife know we've been trying lemon bars!"... WHO CARES? SHE DOESN'T, THAT'S FOR SURE! at most she'll go "oh you're trying those new bars?" and you'll have to say something like "yeah they're tasty" and then you'll NEVER MENTION IT AGAIN.
but no, my brain has to hate the idea of me doing things where other people might perceive me in any way!
3K notes
·
View notes
Text
You know what is just mind boggling? Neurotypical people exist. Like there are people who can just DO things and not have depression, anxiety (in every form ever), RSD, sensory overloads, and not get overwhelmed. Like there are people who can work for eight hours every day and still do things after. People who can make phone calls with no struggle. Who aren't constantly bombarded by a cacophony of thoughts both good and bad when they do things. Who have anxiety but it isn't crippling. who can spend hours, WEEKS with people and not get tired or fear that everyone there hates you. People who have no idea what Depression or intense trauma feel like. People who hear instructions and do it right first go. People who can follow a conversation without zoning out, or having to mask.
Like. Do neurotypical people actually exist?
Because I can't even imagine what it would be like to be neurotypical. Or mentally healthy. Both sound alien and foren. But like. Obviously they exist because neurodivergent people wouldn't struggle so much if not for how the world was structured for Neurotypical people but I don't know if I've ever met a neurotypical.
idk. food for thought I guess.
#neurodiverse stuff#adhd problems#childhood trauma#adhd#high functioning depression#trauma#highly sensitive people#depersonalization#toxic family#emotional abuse#neurodiversity#neurotypical#social anxiety#social issues#random thoughts#random post#idk how to tag this#relatable#rsd#adhd rsd#neurodivergent#adhd stuff#neurodivergence
925 notes
·
View notes
Text
Someone: *criticizes me*
My rejection sensitive dysphoria:
645 notes
·
View notes
Last Seen Blogs

bny83
Untitled

moonlightsmasquerade
So to hell with good intentions!

gisman68
GISMAN68

padsashtray-ao3
matt

kxcxco
Coco