#i have delusions and paranoia and hallucinations but it’s not like. super severe which is why i don’t really do anything about it
Text
psychosis is not “bad person disorder” it’s not a moral failing it’s not a quirk or “evil” or a plot device or an insult and im so sorry to psychotic people who have to deal with that stigma on the daily. you all deserve so much better
#psychosis#i might be psychotic#i have delusions and paranoia and hallucinations but it’s not like. super severe which is why i don’t really do anything about it#or take that label for myself#i haven’t been diagnosed either or done much research so#i do my best to stay in my lane#but hearing people demonize those symptoms 😬#text post#top posts#4k#5k#10k
11K notes
·
View notes
Text
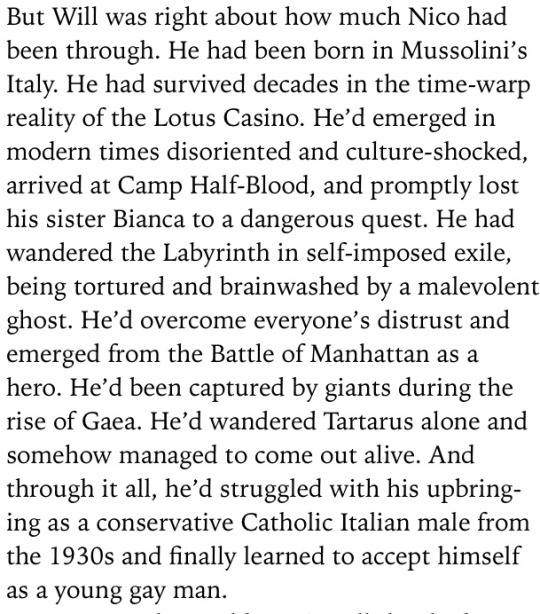
Schizophrenic Nico, here's why I think it's possible:
I want to start off by saying these are just my thoughts, there is no one way to be schizophrenic or to have schizophrenia. It's also important to note that many of the schizophrenic symptoms overlap with other mental illnesses/nuerodivergences like ADHD, Autism, Depression, and OCD which I know many people who head canon Nico as having. I'm not arguing schizophrenic Nico is more correct, more canon, or more right, but to explain some thoughts on why I think it's possible/very likely he does so I can use this for future reference in various thing.
I am using the term schizophrenia as a catchall for all "types" of schizophrenia, but not for schizoaffective disorder which I would say Nico probably doesn't have.
Children born in the winter/those who were "sickly" as babies are more likely to develop schizophrenia. It may also be possible if your mother was sick while pregnant with you, or having a father who was significantly older when he had you.
A stressful life, especially trauma, are more likely to develop schizophrenia or schizoaffective disorder. It likely has something to do with excessive dopamine production, but it may also have something to do with the same genes that control the sleep-wake cycle. Schizophrenia is more common with other mental illnesses or with other nuerodivergences or developmental delays.
Common symptoms include:
Hallucinations
Delusions
Disorganized thinking
lack of motivation
slow movement
change in sleep patterns
poor grooming or hygiene
changes in body language and emotions
less interest in social activities
Now what does this mean for Nico, and why do I think it's likely he has Schizophrenia?
Let's start with Nico's childhood, "children born in the winter/those who were "sickly" as babies are more likely to develop schizophrenia". Although Rick proposed two birthdays for Nico, the fandom generally accepted the January date more fully. We also know that Nico is described as small when he was younger, smallness is common in children who grow up sickly, but it is also common in children who's mother was ill while pregnant with them. We obviously don't know if Nico was sick as a kid, or if Maria was sick while pregnant with him, but again being born in the winter makes these things more likely, as well as consideration for the time period Nico grew up in and the larger variety of illnesses going around at the time. (He is vaccinated against some things though).
Trauma and Nico... do I really have to go into super detail on this one? He spent his childhood growing up in a fascist country that was extremely racist/anti-Semitic/homophobic/etc, his mom died when he was a child- in front of him, his father intentionally gave him amnesia, his sister died when he was a child, he then proceeded to become homeless living/spending lots of time with Minos who verbally (and possibly physically) abused him, becoming aware of his past memories, becoming aware of the fact that many people hated him because of his father and because they thought he was joining the other side (therefore, he was "bad"), he fought in many battles as a child, fought monsters alone, was often faced with life or death situations, went to Tartarus alone (where the goddess of misery told him he was "perfect"), was trapped in a hostage situation with little/no air for a long time while people debated whether or not to save him, was outed against his will, was freed only to travel again fighting monsters and then win a battle, was eventually made to quest with Apollo despite still having lots of healing to do in ToN. So stressful life? Fuck yeah, that doesn't being to cover it.
Genetic factors, obviously nothing here is confirmed so I'm speculating a little bit again, but the common idea in regards to Hades children through the series is that they are "bad". Mental illnesses have been stigmatized for hundreds, if not thousands of years, and often mentally ill people were made out to be weird/bad/etc. It's more than possible there is some sort of genetic factor taking place, also "having a father who was significantly older when he had you". Although I doubt godly genes work the same as mortal ones (trust me I have lots of thoughts on how god genetics/DNA work, but that's not the point right now), I think Hades being the oldest out of all his brothers and having a reputation for having "questionable" children says something... We have no information on Maria's family history at all.
As for schizophrenia often occurring with other mental illnesses and/or neurodivergences: Nico canonically is implied to have either ADHD and/or Autism, and is canonically stated to have PTSD. I think most people would agree that saying Nico has or has had depression isn't a stretch in the slightest.
So canonically we can all agree Nico has severe trauma and coinciding mental health issues/neurodivergences, so out of 4 possible issues I’ve first presented we guaranteeably have two. If I wanted to stretch this a little I would give myself a half point for him being born in the winter and a half point for the aspect of Hades genetics but I won’t do that.
On top of that schizophrenia usually appears during teenage and young adult years in people who receive diagnosis; most people live with mental illness for a few months or a few years in some cases before they're able to receive a diagnosis. Nico being 15 (16 by the end of ToN/shortly following the end of ToN) is about the age that schizophrenia would start to make an appearance. It's also more likely to be found in men, with men also noticing the appearance of schizophrenia appearing early in their lives, and experiencing more negative symptoms in comparison to the higher commonality of affective symptoms in women. That's a really complicated explanation to basically say there's 3 more things that would make Nico having schizophrenia make more sense.
Alright, let’s go back to the list of symptoms I provided:
Hallucinations
Delusions
Disorganized thinking
lack of motivation
slow movement
change in sleep patterns
poor grooming or hygiene
changes in body language and emotions/behavior
less interest in social activities
Once again, some of these are not solely related to schizophrenia and can be the result of other mental health issues, I’m just going to go down the list and add in some moments from the books in which Nico shows some of these traits/behaviors.
Delusions/Hallucinations (more later)
Our best chances for understanding Nico's thought process is in Blood of Olympus where he has a P.O.V... Sometimes Nico's thoughts do derail, or sometimes they get a little confusing, but not always, and when talking to others he is consistent and aware of what he's saying, as well as blunt. Anything "off" about his thought patterns to me just seems like ADHD..
Dietary changes (whether or not you think he has an eating disorder) are behavioral changes (I personally think Nico has AFRID)
Within House of Hades Nico's poor sleep patterns are constantly referenced, and I'll give him a pass on poor hygiene because he's in the middle of a quest but still..
I have extremely complicated feelings on what Will says here, it's possible Nico is an extremely unreliable narrator (unlikely, it seems many people are bothered by him and only maybe a handful aren't), I've also thought at many points this was Rick trying to backtrack some stuff with Nico because he realized he'd made his story a little too harsh for a kids book, it could also be Will's trauma kicking in and that happening... I'm not counting it as full proof about Nico disliking social interactions, but Nico does try to leave even after this conversation and isn't convinced to stay until the last chapter, so maybe there's something to be said about people's dislike of him for being a Hades kid- but I think it's fair to say Nico also dislikes people at least some because he doesn't have interest in trying to befriend anyone either, and is quick to assume all people dislike him (paranoia/low self esteem/and some other possible stuff). There's lots of discussions to be had about this quote and other similar ones, and I don't think a broad brush approach of "Nico good everyone else bad" is accurate it's more, "Nico is good but he fails to try and you have to work on your own mental health everyone won just go to you, and also people dislike Nico for silly reasons and need to get over themselves and make an effort too". (I'm extremely oversimplifying my thoughts and feelings to keep it brief.)
More on delusions and hallucinations:
Now I want to state that lots of schizophrenia symptoms share a lot of commonalities with ADHD and with depression, so although I might include some moments you think are just ADHD/depression I wouldn’t necessarily disagree with you but they could also be schizophrenia or coexisting mental health issues/divergences. I also went through the DSM-5 for schizophrenia (the DSM-5 is just this big book with lists and it’s how doctors diagnose any mental health issue/divergence), I also looked through the DSM-IV (an older book from before DSM-5 which is no longer really used) and the differences between the diagnosis was fairly minimal but they quit categorizing types of schizophrenia and instead rely more on a couple of word descriptions that seem more in line with a spectrum rather than a checkable box.
In order to receive a schizophrenia diagnosis, two (or more) of the following, each present for a significant portion of time during a 1-month period (or less if successfully treated), and at least one of these symptoms must be (1), (2), or (3):
Delusions
Hallucinations
Disorganized speech (frequent derailment or incoherence)
Grossly disorganized or catatonic behavior
Negative symptoms (i.e., diminished emotional expression or avolition).
It’s important to note that only one of these need to be checked off/true if the patient has voices which narrate their actions/behaviors/thoughts or if the person has more than one voice conversing with each other.
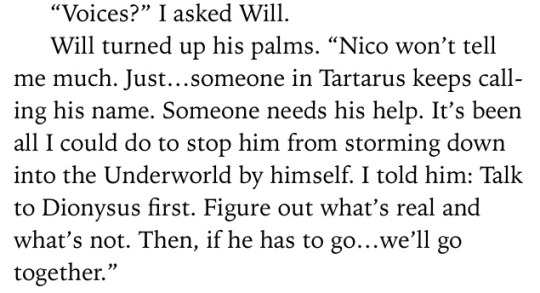
Nico deals with auditory hallucinations (2), he believes the voice belongs to Bob, his titan friend he left in Tartarus:
However this isn’t and immediate diagnosis because Bob’s voice doesn’t talk to another voice(s) in Nico’s head, and we don’t know if Nico has voices running commentary on his behaviors/thoughts.
The reason I state we are unaware if Nico has commentary isn’t because Nico hasn’t said anything, but because many people with schizophrenia before their diagnosis believe the narrative voices are just their thoughts and are a normal internal monologue- usually patients don’t realize anything is wrong until the voices start providing commentary on their actions so instead of “washing the dishes now” the voice(s) might say “wash the dishes now, you’re so lazy you can’t do anything, idiot” during a period of psychosis which may help them acknowledge that the voice(s) isn’t the way most people experience internal voice(s). It is very possible Nico is unaware he is experiencing narrative thoughts and simply assumes that his experience is something most people have, but I won’t use this to argue my point because it’s not confirmation of anything.
Returning now to Bob, Nico knows he is hearing Bob’s voice but he believes Bob is calling to him from Tartarus. Now, Nico says the voices are calling to him from Tartarus but there’s no confirmation of this anywhere… What I think is happening is Nico has a guilty conscience. He feels bad for “using” Bob to get out of Tartarus and various other things, so he feels bad that he is still down there. However, we don’t really know if Bob is calling to him or if Bob is able to do that- what I personally think is happening here is Nico’s brain is convincing Nico that Bob needs him because Nico is upset with himself for not helping Bob more, but also because Nico has never “sat still” before without a quest. Nico has also always felt the want to be needed/important...
It very well could be a delusion.
Schizophrenic patients often experience delusions which make them think they are destined for greatness, or that they have some divine/high force calling out to them for help that only they can provide. It’s an extremely common thing in individuals who experience delusions, and is in fact one of the most common delusions experienced. So although Bob could really be calling out to Nico, I don’t think he is, it doesn’t entirely make sense and there’s lots of little things which point to it being not entirely real- like the fact that nobody else knows about it? Or how absolutely sure Nico is that he need to return to Tartarus? It seems like a mixture of PTSD, delusions, and trauma response (returning to the trauma), working against him. I’ll say delusion is very likely (1).
Using these two factors alone there’s sufficient evidence for diagnosis, but let’s keep going just to see.
For disorganized speech (3) this isn’t something Nico seems to struggle with, and even if he did “derailing” could be ADHD or Autism, so I don’t think this symptom pertains to him.
Changes in behavior (4), seem to all be explainable via depression and/or PTSD- he has begun to express emotion again in Tower of Nero upon learning of Jason’s death he is said to be upset by Will and he walks off to be alone, seems like depression to me. Emotional/Behavior changes from schizophrenia tend to relate more to bipolar disorder rather than a depressive disorder, so I would say if Nico has schizophrenia he probably doesn’t have emotional or behavioral changes from it. If he did he might have some catatonic behavior, but this seems to be clearing up some in Tower of Nero so I’m not super sure on that, maybe during bad periods of psychosis behavioral changes occur, but I would lean more towards this isn’t a symptom Nico personally deals with. Negative symptoms (5) tie into this same idea, it’s possible it’s schizophrenia, but it’s more likely PTSD or depression at work.
So why do I care so much about the possibility of Nico being schizophrenic?
I feel like canonically/fanonically making Nico schizophrenic does a few things, firstly schizophrenic rep in media is extremely extremely awful- can you think off the top of your head of a schizophrenic character who isn't from a horror film/a murder/a villain in their own story? Maybe, but personally I can only think of one which is Charlie from Perks of Being a Wallflower- and even then? That's not canon, it's only implied- and it might not even be true
Schizophrenic media representation always paints schizophrenic people as bad, scary, and evil, and although the horror genre is extremely well known for being super ableist, transphobic, racist, homophobic, and misogynistic (just the final cherry on top) having one of the first- if not the first openly confirmed schizophrenic characters in children's media not only be someone who has lots of character development, and isn't a stereotype, but also be someone people have grown up with, cared for, and sympathized with- would be extremely monumental.
People with schizophrenia and other related disorders aren't something to be scared of or to think of as bad, and often times they're more bothered by whatever they're experiencing than you are.
I don't have schizophrenia or schizoaffective disorder or anything like that, but I have various undiagnosed mental health issues which often lead to me questioning reality, or having to set aside time to convince myself that no there isn't a man living in my wall... Having a character have to question those things, work through those feelings, and learn to trust themselves and care for themselves even with those difficulties would be really great to see in media, not just for people with schizophrenia but also for people with similar/related disorders who might share symptoms see parts of their own struggles in a good, educative way.
I have to finish this in two parts because tumblr keeps breaking because there's too many words in my post lmao (2nd part here)
197 notes
·
View notes
Text
Wat up, I'm here to bitch about stuff.
A good 90% of my life is straight pain and struggle right now. I spend every day trying to distract myself from how I'm feeling, whether that's through sitting on facebook watching slime videos for hours, doing schoolwork for even more hours, or doing regular things and pretending everything is fine. I try to make myself believe that I'm ok. Not say I'm never going to be ok, but I'm having a hard time dealing with all the shit life is throwing at me; has been throwing at me, for years.
I took off that mask yesterday, and I feel like I've been emotionally flayed. I'm raw and feeling all those little fragments of emotion I was protecting myself from, all at once. I've been in bed for the past 3 hours or so, thinkin about life and what mine is trying to teach me. Writing helps and I'm really open abt my mental health struggles, so I figured I'd pour it all out on here so maybe it could help someone or something.
A lot of my stressors include other people, so for their privacy, I'm going to use aliases.
Have you ever done something completely against your values/beliefs and wondered what underlying causes made you (re)act that way? I try to think about that often bc it tends to give new perspective and shed light on information necessary for changing those behaviors.
I had a tough childhood and now that I'm older, I can see the impact it's had on me for so long. Even things I can barely remember are reflected in my emotional responses and conscious decisions if I pay enough attention. Bc of the trauma and inconsistent relationship I had with my parents, I have varying degrees of trust issues, problems with relationships (platonic, familial, and romantic), and mental illnesses. I've struggled with behavioral problems for a long, long time. At one point, it was thought I had ODD because of the severity of some of my outbreaks.
Fortunately, some of my more unusual symptoms started showing up as early as 7. I had been placed in the custody of close family a couple years before that, who sought professional help when my depression and visual hallucinations first appeared. I was in counseling from that point on and began seeing psychiatrists at the age of 13, all of that lasted until I turned 19 and lost my medicaid.
Shortly after I started experiencing various mental health problems, I went into sort of a "dark age" and I don't remember much, like there's a big blind spot in my memories. There are some memories that survived and I've clung to, because I don't have much left from that time period. It lasted until about when I started taking psychiatric medications. And about that time, I started to experience extreme mood swings which resulted in damn near anything, from self harm and suicide attempts to violent outbursts and severe paranoia and delusions. These only increased in intensity until I was kicked out at the age of 17.
*I was hurt by that for a long time which fueled poor decision after poor decision, but I have forgiven both myself and my family bc all that anger and pain and guilt was doing was holding me back. I appreciate everything my family has done for me and I hold them very dear to my heart, especially in times of hardship.*
That's some back story for ya. A lot has happened since then, and maybe I'll talk about it some other time, but I'd really like to focus on the present.
My biggest source of pain currently is the fact that my daughter, Acacia, is in one state and I'm in another. I miss her terribly and every day I sit and think about how I've failed her. I want to be a source of joy for her, but right now she's hurting because her mother is gone and she doesn't understand why. We facetime, but she tells me that she doesn't like me and she's sad. It breaks my heart that she's dealing with such big emotions and I can't even be there to comfort her. But I'm also very grateful she's surrounded by people who love her and we can talk every day. It's really hard, and I'm usually in a lot of pain after we hang up, but I will always be there for her. I have to be the mother she needs me to be so I'm going to have to make some tough decisions. I'm not going to talk abt this anymore bc it's too much for me right now.
I'm in another state living with my husband, Onyx, and I feel utterly and completely alone. We left bc we were evicted back home and the only place we could go was his parents'. He shut me out a long time ago, but the homesickness is amplifying my feelings of isolation. Due to some of the toxicity in our relationship, I burned many bridges with friends and family, and aside from my 2 best friends (who I rarely talk to anymore) I have no one. Many days I beg Onyx for affection or communication or some semblance that he still loves me, but my efforts are futile. Weve been having the same fight for nearly half a year. I bring up something that's bothering me, and he becomes angry and says "it's always something", in some form or another I try to remind him that we have to work on the issues in our relationship at some point if we want things to get better, this is where he usually gets defensive and says something something along the lines of "I always need 'more or too much'". From that point, I've learned to just be quiet bc our problems are suddenly my fault and he will do everything in his power to deflect and shame if I try to get him to own up to his negative behaviors that hurt me almost every second.
I saw the red flags a long time ago, but I had hope. Hope that has now completely withered away bc I know he won't change, at least not anytime soon. I can see it in his face when I try to have any form of an adult conversation with him. The way he just barely squints his eyes while I'm talking, the smirk that I try to convince myself isn't real bc it's so slight, the overall look of complete apathy.
I've tried leaving before, several times and one period of 5 months, but I wanted to make things work bc we got married this year. He told me it would make me more consistent and I wouldn't feel like leaving all the time, but let me tell you, I feel like leaving all the time. I've told him about my plans to go back home, without him. I've told him I would stay if he would be a part of this relationship too bc I can't be with someone who is the source of so much of my pain. You know that saying, "you can't make someone love you if they don't want to"? It's true, fucking painfully true. I've found myself holding on to tiny shreds of hope here and there, making myself believe that he'll try in small gestures like a kiss or laying his head on me. But I've been doing that for too long. I have made sacrifices for him over and over to the point where I don't recognize myself anymore. I've stopped talking to wonderful ppl bc it made him uncomfortable. I'll admit it, I kissed a guy back the night after we decided to be mutually exclusive. I talked to an ex love interest for a period of time abt how I was struggling in my relationship w Onyx. But I apologized, owned up to those behaviors, and made changes. I don't deserve for those things to be held over my head and brought up in almost every fight bc yes, I fucked up, but I did what I had to do to fix things. At a certain point, you have to be accountable for how you let your hurt and anger manifest.
So now I'm leaving bc I have to get back to my daughter and get in a better environment, but I don't know how or when. Like I said earlier, I ruined a lot of relationships try to preserve the one that was ruining me. But I'm really stuck out here, I've never been able to hold a job in my working career, and even if I could, I'm also taking several online college classes (that's been a bitch too) so I can't work more than part time and even that would jeopardize my mental health. I'm really stuck and so frustrated and I'm sorry that this has been a super long post. Like I said, I'm just bitching about life. I know the most sucky situations bring about the most growth.
For those of you who are curious, my diagnoses are PTSD, atypical OCD, and persistent depression w mood incongruent psychotic features.
Also: Besides being a good talker, I'm also a great listener. If you're struggling right now, I'm here for u.
#mental illness#mental health#life sucks#real life#sorry#beenthrushit#parental seperation#OCD#psychosis#growth#opportunity#depression#hard times#strength#inner power#self love#self preservation#do what you gotta do#potential#background#back story#bad day#no friends#love yourself#see the good
1 note
·
View note
Link
In 2005, there were an estimated 81,600 prisoners in solitary in the US; this month’s Senate Subcommittee Hearing puts the numbers at about the same. That’s 3.6 per cent of the 2.2 million presently incarcerated, many of whom, like King, were put in there for random acts of non-violent rule-breaking. Some, like him, shuttle in and out of solitary; others remain locked up for decades. Prison authorities in every state are running a massive uncontrolled experiment on all of them. And every day, the products of these trials trickle out on to the streets, with their prospects of rehabilitation professionally, socially, even physiologically diminished. The Box, as psychologists and psychiatrists have been saying for decades, damages the mind. But evidence from neuroscience increasingly suggests that it is irrevocably harming the brain, too.
In the fall of 1982, the forensic psychiatrist Stuart Grassian visited Walpole State Penitentiary, Massachusetts’s only maximum-security prison at the time. He went there at the behest of a legal aid attorney, who wanted him to evaluate the mental health of the inmates in the prison’s segregation unit. He spoke to 14 young men who’d been in isolation for several months, each in a 6ft x 9ft cell with a barred inside gate, and a steel door with a voice box and a dirt-stippled glass panel the width of his face. Grassian expected to hear fantastically exaggerated claims from prisoners looking to dupe their way out of the unit, but each vociferously denied that anything was the matter. ‘Solitary doesn’t bother me,’ one told him. ‘Some of the guys can’t take it, I can,’ said another. With close questioning, Grassian wrote later in the American Journal of Psychiatry, the second prisoner ‘came to describe panic, fears of suffocation, and paranoid distortions while he had been in isolation’, while the first had recently slashed his wrists because he ‘figured it was the only way to get out of here’.
They suffered a range of symptoms: stupor, delirium, hallucination, and a loss of ‘perceptual constancy’ – the ability to recognise the sameness of things when viewed from different distances and angles. Many had painfully sharpened senses. One lived in dread of prisoners on the tier above turning on the faucet, sending water clinking and whooshing down the pipes. ‘It’s too loud, gets on your nerves. I can’t stand it – I start to holler,’ he told Gassian. ‘Are they doing it on purpose?’
Half of them hallucinated constantly. They heard whispers and muttered sounds, which took on menacing meanings: prison guards conferring about amputating a prisoner’s leg, someone getting beaten up with sticks. One prisoner – the disconsolate historian of Sartre’s Nausea brought to life – was haunted by the inconstancy of objects. ‘Melting, everything in the cell starts moving,’ he told Grassian. ‘Everything gets darker, you feel you are losing your vision.’ Another had Alice in Wonderland-like visions, featuring pancakes of diminishing sizes delivered to his gate. Four had extended bouts of amnesia. They said they felt narcotised, and couldn’t concentrate on anything.
‘These people were very sick,’ recalls Grassian. He thought it resembled anoxic brain injury – the result of an oxygen-starved brain – or delirium tremens, suffered by dipsomaniacs in the throes of alcohol withdrawal. But the symptoms also recalled a curious set of Cold War-era experiments that Grassian had read about years before.
Through the 1950s and ’60s, researchers in America and Canada were investigating the effects of ‘sensory deprivation’ or ‘perceptual isolation’, both analogues of solitary. This work was largely bankrolled by the CIA, which was interested in developing more efficient techniques of interrogation and ‘mind control’. The Canadian neuropsychologist Donald O Hebb proposed that dramatically reduced stimuli – such as in narrow windowless cells with single beds – might be one way to impair a prisoner’s alertness, and lay the ground for ‘the implantation of new or different ideas’.
To test this hypothesis, Hebb’s colleagues at McGill University confined college students to isolation units, where ear pillows muffled their hearing, and plastic visors restricted their sight. Within 24 hours, they couldn’t think or concentrate, and experienced powerful sensorial hallucinations: they had strange visions of rocks, eyeglasses, babies, their skin crawled, and they heard choirs trilling in ‘full stereophonic sound’. They experienced spatial disorientation whenever they left their cell.
Meanwhile, researchers on a Californian army base confined soldiers to soundproof isolation chambers for four days, after which they observed that their test subjects became hyper-attentive to stimuli. ‘After the dearth of sensory experience imposed by isolation,’ they wrote, ‘[the prisoner] seems to become more responsive to any dynamic stimulus energy in his environment, actively seeking and better tolerating stimuli that are normally inadequate to attract and maintain attention.’
With this research at the back of his mind, Grassian headed to the library to search for clinical parallels of what he’d just seen, and also to research the history of solitary – something he hadn’t encountered before. ‘I saw that similar symptoms had first been seen in poliomyelitis patients in iron lungs, in spinal traction patients, or those who’d had eye-patch surgery, polar explorers…’ he told me. All these situations were analogous to solitary confinement, by reducing sensory inputs or creating isolating circumstances. But what Grassian found most staggering was his discovery that America was the earliest adopter of solitary confinement, despite its reputation as ‘the world leader in social progress’. The English philosopher Jeremy Bentham might have been the first to design the ‘Panopticon’ – a structure of remotely observed solitary cells that enforced discipline through the threat of being watched – at the tail end of the 18th century. But these ideas first found shape in stone and mortar with the opening of the Eastern State Penitentiary in Philadelphia in 1829.
The ‘separate system’ was regarded a rational, humane replacement for the dark legacies of colonial law: punishments that consigned offenders to the gallows, the stock, or the public cage, which used pain and shame as deterrence. As its name and its vaulted, sky-lit cells suggested, the Philadelphia penitentiary intended to reform prisoners by enforced monkish solitude, repentance and rehabilitation. Inmates ate, slept, and worked in individual cells. They exercised in a private yard once a day, and were given a single book to read: the Bible.
The ‘separate system,’ as it became known, had impassioned admirers and critics, who battled it out in pamphlets (the message boards of the day). Charles Dickens visited the prison in 1841, and thought its ‘slow and daily tampering with the mysteries of the brain… immeasurably worse than any torture of the body’. In the same year, Reich, a clinician in southwest Germany, observed a distinct psychic malady developing among some isolated prisoners awaiting trial. ‘The prisoner becomes silent, chary of words, lost in brooding,’ he wrote in 1871. ‘He observes little of what goes on about him and remains motionless in one spot. His face takes on an astonished expression, the gaze is vacant and indefinite.’ With prolonged isolation, the condition worsened. ‘Consciousness becomes more and more clouded, soon illusions, hallucinations, and delusions appear… Simultaneously [the patients] complain about all kinds of bodily sensations.’ Reich called this twilit fugue state ‘prison paranoia’.
In 1890, the testimony of James J Medley, an isolated prisoner on death row in Colorado, inspired a landmark decision by Supreme Court Justice Samuel Freeman Miller, who subsequently released the prisoner. In his judgment, Justice Miller observed: ‘A considerable number of the prisoners fell, after even a short confinement, into a semi-fatuous condition, from which it was next to impossible to arouse them, and others became violently insane; others still, committed suicide; while those who stood the ordeal better were not generally reformed, and in most cases did not recover sufficient mental activity to be of any subsequent service to the community.’
Yet, just as Grassian was researching the history of solitary and its associated ills, the US prison system was strengthening its faith in this form of incarceration, building, in every state, multimillion-dollar citadels composed of single-cell ‘control units’: super-maximum-security prisons, or supermaxes, for short.
Supermaxes are high-tech panopticons built to fulfil the Benthamite objectives of ‘punishing the incorrigible’ and ‘reforming the vicious’ or, in contemporary policy-speak, ‘managing risks efficiently’. Constructed after a decade of riots and prison-guard slayings, these free-standing facilities entirely composed of single-cell units are designed to minimise contact between prison guards and inmates. Of the 81,600 prisoners in solitary today, approximately 25,000 are in supermaxes. While the majority of America’s isolated prisoners are routinely moved in and out of the solitary confinement wards of regular prisons, supermaxes are entirely given over to the long-term containment of a specific set of prisoners: those on death row, and those deemed violent, disruptive or given to escape attempts. In the press, such prisoners are typically described as ‘untameable’ (by popular conservative commentator George Will in 1997), ‘predatory, problematic and influential’ (by three prison wardens in the Wisconsin State Journal), and ‘the most devious and manipulative’ violent offenders (by Gerald Berge, a supermax warden, for the journal Corrections Today in 2001).
Supermaxes embody a transition in prison policy over the past 30 years, from rehabilitation to a punitive ideology that emphasises stricter regulations, harsher punishment, and tougher sentences. They are carceral citadels that recall army bases with their remote locations and soaring electrified perimeter fences, and they star in a kind of security theatre intended to make the public feel safer. Inside, cells are typically laid out in narrow rows radiating from a central tower. From these eyries, correctional officers control the doors, lights, and temperatures of every unit. Prisoners spend 22.5 hours a day in 8ft x 10ft windowless isolation units, with 1.5 hours’ recess by themselves in a small concrete pen. Verbal communication takes place over an intercom system, and moments of contact are fleeting and often brutal: prisoners are put in security restraints or subjected to ‘cell extractions’, forced out of their cells by officers in riot gear and shock shields, armed with tasers and pepper spray.
America got its first proto-supermax in 1934. This was Alcatraz Federal Penitentiary, a military prison-turned-maximum security facility on an island in the San Francisco Bay, intended to house ‘the worst of the worst’. In 1941, the warden designated Block D, an isolation unit, for troublemakers inside the prison, the worst of the worst of the worst. When ‘the Rock’ shut shop in 1963, United States Penitentiary Marion was opened in southern Illinois to ‘confine not only some of the incorrigibles from Alcatraz but several hundred other difficult, escape-minded young inmates’. In 1973, ‘control units’ were built for the most violent of these ‘incorrigibles’. After two inmates stabbed and killed two prison guards on 22 October 1983, the prison was put on ‘lockdown’ for 23 years. Prisoners were isolated in their cells for 23 hours a day, and they were denied exercise and communal dining. This sparked off the ‘Marionisation’ of prisons around the country, and effectively turned USP Marion into the country’s first supermax facility.
In 1989, a sprawling concrete bunker started to take shape in California, amid a stand of redwoods near the state’s coastal border with Oregon. Bounded by an electric perimeter fence, Pelican Bay State Prison was the country’s first official supermax, intended for California’s ‘most serious criminal offenders’. States across the country followed suit. Between 1995 and 2000, the number of prisoners in supermax beds soared by 40 per cent nationally, to 20,000 – almost 1.8 per cent of the number of prisoners serving more than a year’s sentence in both state and federal prisons. This upward tick was mirrored in the number of prisoners being consigned to solitary. Between 1995 and 2000, according to a report by the Bureau of Justice Statistics, the number of prisoners in ‘restrictive housing’ also soared by 40 per cent nationally, outstripping the overall growth rate of the prison population, which increased by 28 per cent in the same period. By 2004, 44 states had some form of supermax housing, and the number of inmates in them had risen to its present-day tally of 25,000.
The numbers are notoriously difficult to track. Not all supermax-type facilities are classified as such, and in prisons and jails, solitary confinement goes by various appellations. Inmates can be sent to ‘disciplinary segregation’, which is incurred whenever a hearing officer from the Department of Corrections judges that an inmate has committed a disciplinary infraction. ‘Administrative segregation’ is the prison official’s destination of choice for gang members and the politically active. ‘Protective custody’ is ostensibly for prisoners’ protection, but it’s otherwise indistinguishable from the other categories. ‘Suicide watch’ can be worse than other types of isolation, because prisoners are stripped down to their shorts and put in a kind of padded mini-Box (known in California as the ‘rubber room’). ‘Keep-lock’ is confinement that takes place amid the general population, usually before being consigned to the Box for a rule violation, or before a transfer to another correctional facility.
In the public imagination, these sentences are handed to ruthless mass-murderers on death row, not a humble stoner such as King, or the perpetrators of the kinds of offences enumerated in inmate misbehaviour reports: collecting too many stamps; possessing ‘contraband’ such as phone cards or nail varnish, or condiments such as pepper or curry powder; refusing to return a food tray; declining to submit to a urine analysis test; spitting on a correctional officer; erecting a makeshift ‘privacy curtain’ in order to perform ablutions out of a bunkmate’s sight; inflicting self-harm.
As heterogeneous as supermax facilities are, they have a few things in common. They all cost two or three times as much to construct and maintain as maximum-security prisons, and prisoners released directly from them – and restricted housing circumstances in general – are found to have an elevated chance of finding their way back, particularly through violent recidivism. One judicial report in 2012 quoted the University of Albany criminologist Hans Toch, who said that prisoners ‘may become the “worst of the worst” because they have been dealt with as such’.
In recent years, supermaxes have incited a number of lawsuits for being dirty, dangerous, and for having inadequate mental health services. Terry Kupers, an Oakland-based forensic psychiatrist, has evaluated the psychological conditions of hundreds of isolated prisoners for several such lawsuits filed by the American Civil Liberties Union (ACLU) against prison authorities. A recent case involving death row inmates in Unit 32, a supermax facility in Mississippi State Penitentiary at Parchman, sparked off a change of heart among prison officials, and something of a national trend. When Kupers evaluated the residents in Unit 32 in 2002, which reeked of malfunctioning toilets, he found that about 100 of them had severe undiagnosed or misdiagnosed mental illnesses. They hallucinated, threw faeces at the guards, and howled through the night; in response, they received punishment, not treatment. After listening to the accounts of inmates who described the facility as a hellhole and insane asylum, the prison authorities gradually reduced the segregated population from 1,000 to 150, upon which violence plummeted by 70 per cent.
The Mississippi experience led to a re-examination of the rationale behind solitary confinement in Colorado, Illinois, Maine, Ohio and Washington. Maine cut its segregated population by almost 60 per cent, and made it onerous to keep a prisoner in confinement for more than 72 hours. The Colorado prison authorities reviewed their segregation practices and, in 2012, announced the closure of a 316-bed administrative segregation unit that will save the state $13.6 million this year. This January, prison authorities in Illinois closed down its notoriously repressive supermax, Tamms Correctional Center, which cost the state $26 million annually, or about $64,800 per inmate per year to run.
In June 2012, in a packed hearing held before the Senate Subcommittee on the Constitution, Civil Rights and Human Rights, Senator Richard Durbin of Illinois spoke out against solitary confinement, and engaged in a fiery debate with the director of the Federal Bureau of Prisons. The Senate was shown a life-size replica of a 7ft x 10ft SHU, and heard the testimony of former isolated inmates and prison officials in Mississippi. In February 2013, the Federal Bureau of Prisons announced that it was undertaking an audit of the practice; by November, it had announced it would visit 13 isolation units during 2014. This February, following a lawsuit by the New York Civil Liberties Union on behalf of three inmates who’d been in solitary, New York state agreed to curb the widespread use of isolation in the case of prisoners who were pregnant, or developmentally disabled, or under the age of 18. As this essay is published a second Senate Committee Hearing on solitary confinement is in motion.
‘Half the successful suicides in prison happen in solitary,’ Kupers told me over a Skype interview, despite only 3 to 6 per cent of the prison population being held in isolation. ‘It is such a stunning correlation that it is difficult to not conclude that there’s something about solitary confinement that exacerbates suicidal tendencies.’ This finding was replicated in a study published in the American Journal of Public Health this month, in which the correctional psychiatrist Fatos Kaba and colleagues analysed about 244,699 jail admissions New York City between 2010 and 2013, and found that although 7.3 per cent of prisoners admitted during this period were consigned to solitary, this group accounted for 53.3 per cent of acts of self-harm, and 45 per cent of potentially fatal acts of self-harm.
In a 2008 study in Psychiatric Services, the psychiatrists Raymond Patterson and Kerry Hughes analysed admissions between 1999 and 2004 in the California state prison system – the largest in the country – and found that nearly half of successful suicides occurred in single cells in administrative segregation or ‘secure housing units’, while another 12 per cent took place in mental health crisis beds. That chimes with a 1997 study by psychologists Holly Miller and Glenn Young which found that prisoners’ symptoms of mental distress rose in concert with the severity of their segregation. It also echoes a 2008 study in Criminal Justice and Behavior by David Lovell, who found that nearly half of all isolated prisoners in a Washington State supermax prison had serious mental illness or brain damage.
Such studies still leave important questions unanswered: does solitary draw in an especially vulnerable subgroup of prisoners? Does isolation damage or transform the brain? Or both?
Grassian is convinced that both are true – the first, from his research, and the second, from his experiences visiting hundreds of prisoners in isolation units across the country. ‘Punish him, punish him, punish him: that’s the only thing the correctional system knows to do,’ he told me. But the kind of prisoners who tend to be in solitary don’t respond to a rational calculus of means and ends and ‘that paradigm holds valid for an exceedingly small fraction of the prison population.’ His research and observations have lent strength to several important federal court decisions, including the landmark 1995 case Madrid v Gomez, in which the court called for the removal of prisoners with psychiatric problems from isolation, and the judge conceded that the conditions in SHUs ‘may well hover on the edge of what is humanly tolerable for those with normal resilience’.
In 1999, Grassian went on a tour through the SHU of Attica, a maximum-security prison in upstate New York, which brought that message home especially forcefully. In cell after cell, there emerged characters who belonged in a Romantic painter’s depiction of a madhouse: ‘Some guys were masturbating openly. Some guys were screaming,’ Grassian told me. He remembers turning on his companion, a lawyer for the Department of Corrections, and ‘growling’ at him: ‘You’re looking at the population of a state psychiatric hospital. This isn’t the “worst of the worst”. This is the sickest of the sick!’
160 notes
·
View notes
Last Seen Blogs

ironfistd-2
Untitled

lesbian-of-nine
Cause I’m her kind of boy and also her girl.

princesschubbi
🩷 Princess Chubbi is still here 🩷


jujustrawberry2001
XOXO